
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 07 December 2023
Sec. Viral Immunology
Volume 14 - 2023 | https://doi.org/10.3389/fimmu.2023.1277793
 Oskar Ayerdi1Rafael Benito2Diego Ortega3Antonio Aguilera4Natalia Montiel5Ilduara Pintos6Alberto Díaz de Santiago6Begoña Baza1Vicente Soriano7*Carmen de Mendoza6 on behalf of the Spanish HTLV Network
Oskar Ayerdi1Rafael Benito2Diego Ortega3Antonio Aguilera4Natalia Montiel5Ilduara Pintos6Alberto Díaz de Santiago6Begoña Baza1Vicente Soriano7*Carmen de Mendoza6 on behalf of the Spanish HTLV NetworkBackground: HTLV-1 infection is a neglected disease, despite estimates of 10 million people infected worldwide and producing life-threatening illnesses in 10% of carriers. Sexual transmission is the main route of contagion. However, HTLV-1 is not listed among sexually transmitted infections (STIs).
Methods: Serum from all consecutive individuals who had attended six STI clinics across Spain during the last 12 months were tested for HTLV antibodies using a commercial enzyme immunoassay (EIA). Reactive samples were confirmed by immunoblot.
Results: A total of 2,524 samples were examined. The majority (1,936; 76.7%) belonged to men, of whom 676 (34.9%) were men who have sex with men (MSM) receiving HIV pre-exposure prophylaxis. Although native Spaniards predominated (1,470; 58.2%), up to 593 (23.5%) came from Latin America and 139 (5.5%) were African. A total of 26 individuals were initially EIA reactive and immunoblot confirmed 5 as HTLV-1 and 7 as HTLV-2. All but one HTLV-1+ case came from Latin America. Three were men and two were women. Among Latin Americans, the HTLV-1 seroprevalence was 0.67%. In contrast, all seven HTLV-2+ were native Spaniards and former injection drug users, and all but one were HIV+.
Conclusion: The rate of HTLV infection among individuals with STIs in Spain is 0.5%, which is greater than in the general population. These results support the introduction of universal HTLV screening in persons who attend clinics for STIs.
HTLV-1 infection is a neglected disease, despite infecting around 10 million people worldwide (1, 2) and producing life-threatening illnesses in roughly 10% of carriers (3). HTLV-1 infection is highly endemic in parts of Latin America, Equatorial Africa, and Southern Japan (4, 5). Sexual transmission is the most frequent mechanism of contagion (6). Transmission may also occur following parenteral exposure among injection drug users or recipients of contaminated blood or solid organ transplants (7, 8). In endemic regions, vertical transmission of HTLV-1 from mother to child, especially throughout breastfeeding, is also common (9).
Globally, more than 80% of new HTLV-1 infections are estimated to be acquired during adulthood (10, 11). Sexual transmission is more frequent from men to women than vice versa (12). Neutralizing antibodies and a weak local immune response to the infection most likely explain the limited ability of HTLV transfer via cervicovaginal secretions (13). In contrast, the seminal fluid milieu enhances HTLV replication (14). Despite all these facts, HTLV-1 is not listed among sexually transmitted infections (STI) (15). Information on the relative risk of HTLV-1 transmission in persons with multiple sexual partners or in men who have sex with men (MSM) is scarce (16, 17). Herein, we report the results of the first large cross-sectional survey of HTLV antibodies in consecutive individuals who attended clinics for STIs in Spain.
A nationwide HTLV-1 register was created in Spain in 1989. The main demographics, clinical symptoms/signs, and laboratory findings are collected for each new HTLV-1 case at baseline and longitudinally using a standardized case report form. A biological repository of specimens stores patient samples when possible. Members of the Spanish HTLV Network cover most of the lab facilities nationwide where this virus can be diagnosed, including public or private microbiology labs or blood banks (18). From the coordination center, all members of the network were invited to participate in the current study during the year 2021.
Serum specimens collected from consecutive individuals who attended six clinics across Spain and with a diagnosis of at least one STI during the last 12 months were tested for HTLV antibodies. A commercial enzyme immunoassay (EIA) was used for screening for HTLV-1/2 antibodies (HTLV Abbott). The sensitivity and specificity of this test have been evaluated previously and are considered reliable for screening purposes (19). Reactive samples were then confirmed by immunoblot (Inno-Lia HTLVI/II, Fujirebio). Given its good performance and easy interpretation, this test has replaced classical Western blot assays as confirmatory and discriminatory of serum HTLV-1 and HTLV-2 antibodies (20). Demographics (age, gender, and country of origin) and STI diagnoses were recorded for all patients.
Figures are given in absolute numbers and percentages. Quantitative and qualitative variables are described as medians with interquartile ranges, means with standard deviations, or proportions. Bivariate comparisons of quantitative variables were performed using the Chi2 test.
All statistical analyses were performed using the IBM SPSS package for Windows v25.0 (IBM Corp, Armonk, NY). All tests were two-tailed, and only p-values <0.05 were considered significant.
The study was designed as a multicentre and retrospective collection of anonymized and consecutive clinical data associated with serum HTLV-1 antibodies. It was approved by the Puerta de Hierro University Hospital ethics committee (ref. PI 185/21).
A total of 2,524 samples were analyzed. The majority (1,936; 76.7%) belonged to men, of whom, 676 (34.9%) were MSM receiving HIV pre-exposure prophylaxis (PrEP). The median age of the study population was 37 (IQR, 18) years old. Although native Spaniards predominated (1,470; 58.2%), up to 593 (23.5%) came from Latin America and 139 (5.5%) were Africans. The most prevalent STIs diagnosed within the last 12 months were syphilis (43.2%), gonorrhea (20%), HIV (19.7%), Chlamydia trachomatis (17.9%), and hepatitis B (8.6%).
A total of 26 individuals were initially reactive for HTLV antibodies on the EIA screening. Using immunoblot, 5 were confirmed as HTLV-1 and 7 as HTLV-2, 2 were indeterminate, and 12 were negative.
The overall seroprevalence for HTLV-1 was 0.2% and for HTLV-2 was 0.28%. As shown in Table 1, all but one of the HTLV-1-positive patients came from Latin America (2 Colombia, 1 Brazil, and 1 Peru). Three were men and two were women. All men were MSM, of whom two were HIV-positive and another was under PrEP. The only native Spaniard was a 77-year-old woman who had been tested for HTLV-1 following a diagnosis of hepatitis B. The most frequent STIs, along with HTLV-1, in these five cases were syphilis (3), HIV-1 (2), Chlamydia trachomatis (2), and hepatitis B (1). Among Latin Americans with STIs, the HTLV-1 seroprevalence was 0.67%.
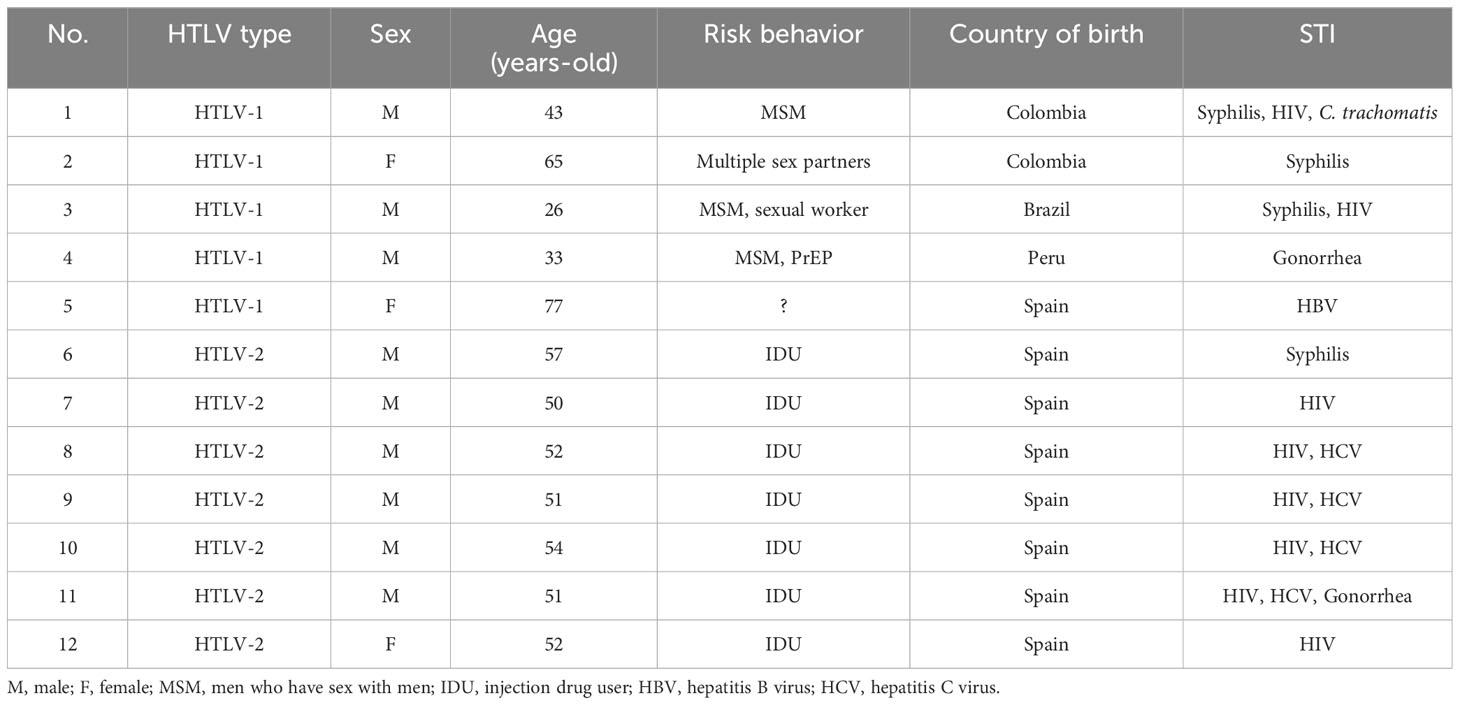
Table 1 Main features of individuals with HTLV infection and sexually transmitted diseases in Spain.
All seven HTLV-2 cases were native Spaniards and all had been injection drug users. The most frequent STIs diagnosed within the last 12 months, along with HTLV-2, were HIV-1 (6), hepatitis C (4), Neisseria gonorrhoeae (1), and syphilis (1). The overall HTLV-2 seroprevalence among native Spaniards with STIs was 0.48%.
A rebound in STIs following the relief of social isolation measures taken to curb the COVID-19 pandemic has been noticed worldwide (21, 22). Even before, STIs had been on the rise along with a loss of fear of acquiring HIV, as a compensatory effect of the widespread use of PrEP (23–26). More than 400 million new STIs occur each year worldwide. Four agents are the predominant etiologies, namely syphilis, gonorrhea, chlamydia, and trichomoniasis. However, there are many more, including HIV, papillomavirus, herpes simplex, hepatitis B, etc.
Despite infecting roughly 10 million people worldwide and causing neurological disease and/or lymphoproliferative disorders in 10% of carriers, HTLV-1 infection remains a neglected disease (2). In endemic regions of Japan, following the implementation of HTLV-1 antenatal screening, vertical transmission decreased drastically. However, HTLV-1 infection in adolescents and adults through sexual contact has replaced vertical transmission as the main route for transmission. In Japan, which has a population of 125 million, roughly 3,000 new HTLV-1 infections occur annually (27).
Persons engaged in high-risk HIV behaviors who receive antiretrovirals to prevent HIV acquisition are recommended to be tested periodically for distinct STIs. Specifically, certain MSM groups have fueled outbreaks of hepatitis A (28), hepatitis C (29), and more recently, mpox (30). When acute infections are symptomatic, the etiology can be excluded and preventative measures implemented. However, when acute infections are asymptomatic, following HTLV-1 exposure, new carriers may establish a silent population reservoir from which the virus can spread unnoticed.
Although HTLV-1 is nowadays a predominantly sexually transmitted agent, testing is not mentioned in HIV pre-exposure guidelines (31). A recent study conducted in England examined the rate of HTLV infection in this population. Although none of the 2015 HIV PrEP users were infected, the authors cautioned that up to 75% were men of white ethnicity born in Europe. Hence, persons from HTLV-1 endemic regions were poorly represented (32).
In our survey, we examined 2,524 individuals attending STI clinics in Spain, and we found five cases of HTLV-1 and seven cases of HTLV-2 infection. All HTLV-1 male cases were young Latin Americans. The two women were 65 years old or older. One was a former Latin American sex worker. Another was an older Spaniard woman for whom we could not find any potential source of HTLV-1 infection. Two of the HTLV-1-positive men were coinfected with HIV-1. Both acknowledged multiple sexual partners, some of whom were using PrEP. The possibility of the use of antiretrovirals to protect against both HIV and HTLV infections warrants further consideration (33). At this time, it is unclear to what extent the use of antiretrovirals to treat or prevent HIV contagion might protect against sexual transmission of HTLV-1 infection (34). In vitro data support that cabotegravir may halt HTLV-1 transmission (35) and long-acting formulations of this drug are increasingly being used by persons engaged in high-risk sexual behaviors. Our findings highlight the convenience of adding anti-HTLV testing to the screening of individuals presenting with or at risk of any STI.
All seven HTLV-2-positive individuals identified in our STI study were native Spaniards and former injection drug users. Moreover, all but one were HIV-positive and four had hepatitis C. Several studies in Europe and North America have highlighted the occurrence of a large-scale spread of HTLV-2 during the 1980s and 1990s among injection drug users (36, 37). This explains the frequent identification of coinfection with HIV and hepatitis C. Interest in HTLV-2, however, has been lower than in HTLV-1 because evidence to date has only occasionally demonstrated human pathogenicity, with only anecdotal cases of myelopathy or neuromuscular disease (38, 39).
Our study has several limitations. First, we should acknowledge that 14 out of 26 initially reactive EIA specimens were disregarded since HTLV immunoblot was either negative (n=12) or indeterminate (n=2). We did not test these samples using molecular techniques such as polymerase chain reaction. Prior studies have unveiled HTLV-2 proviral gene sequences mainly in HIV-coinfected individuals (40, 41). Therefore, our figures for HTLV-2 could underestimate to some extent the real number of HTLV-2 infections in our study population. Second, individuals tested in our study population should not be considered representative of the STI population in Spain, as we included a disproportionate number of MSM and of the subset under PrEP. However, in our experience, most of the individuals who attend STI clinics in Spain are engaged in high-risk practices for HIV and are familiar with the healthcare system. In contrast, other individuals occasionally presenting with gonorrhea and/or syphilis are generally attended to by general practitioners. Accordingly, this group escaped our testing, which focused on those who attend STI clinics.
Estimates from hospital discharges (42), clinical presentation (43), and the HTLV national register (18) have concluded that HTLV-1 is an orphan disease in Spain, meaning that it affects less than 5 per 10,000 citizens. In our study, the overall seroprevalence of HTLV infection among individuals with STIs in Spain was 0.5%, significantly greater than in the general population. The rate of HTLV-1 infection among individuals with STIs from Latin America approached 0.7%. Altogether, our results support the introduction of universal HTLV screening in all individuals who attend clinics for STIs in Spain. It would be worth collecting information from similar studies conducted in other non-endemic countries with significant migrant flows from HTLV-endemic regions.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving humans were approved by the Ethics committee of Puerta de Hierro University Hospital ref. PI 185/21. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
VS: Conceptualization, Formal analysis, Funding acquisition, Methodology, Supervision, Writing – original draft. OA: Investigation, Writing – review & editing. RB: Data curation, Writing – review & editing. DO: Data curation, Writing – review & editing. AA: Data curation, Writing – review & editing. NM: Formal analysis, Writing – review & editing. AD: Formal analysis, Writing – review & editing. BB: Data curation, Writing – review & editing. CM: Data curation, Funding acquisition, Investigation, Methodology, Writing – review & editing. IP: Data curation, Writing – review & editing.
E. Calderón (Hospital Virgen del Rocío & CIBERESP, Sevilla); M. Rodríguez-Iglesias, N. Montiel & T. Trujillo (Hospital Universitario Puerta del Mar, Cadiz); I. Viciana (Hospital Virgen de la Victoria, Málaga); T. Cabezas (Hospital Torrecárdenas, Almería); A. Lozano, E. Fernández-Fuertes & J.M. Fernández (Hospital de Poniente, Almería); F. Garcia and M. Alvarez (Hospital Universitario Clínico San Cecilio, Granada); R. Benito, S. Algarate & M. Ducons (Hospital Clínico Universitario Lozano Blesa, Zaragoza); D. Ortega (Hospital Miguel Servet, Zaragoza); C. Cifuentes, V. Fernández-Baca & J.V. Fernández-Montero (Complexo Hospitalario Universitario de Santiago-CHUS, Santiago de Compostela); M.D. Maciá (Hospital Son Espases, Mallorca); A. Hernández-Betancor & A.M. Martín (Hospital Insular Hospital Universitario, Las Palmas de Gran Canaria); M.J. Pena (Hospital Universitario Dr. Negrín, Las Palmas de Gran Canaria); M. Hernández, A.M. López-Lirola & J.L. Gómez-Sirvent (Hospital Universitario La Laguna, Tenerife); R. Copado (Hospital Dr. José Molina Orosa, Lanzarote); M.E. Cano (Hospital Universitario Marqués de Valdecilla, Santander); S. Rojo (Hospital Clínico Universitario, Valladolid); J.M. Eirós (Hospital Rio Hortega, Valladolid); M. Rodríguez (Hospital del Bierzo, Ponferrada); C. Gómez-Hernando (Complejo Hospitalario Virgen de la Salud, Toledo); A. González-Praetorius (Hospital Universitario, Guadalajara); A. Rando (Hospital Vall d’Hebrón, Barcelona); L. Force (Hospital General, Mataró); E. Miró (Hospital Santa Creu i Sant Pau, Barcelona); A. Cebollero (Clilab Diagnostics, Barcelona); J.F. Delgado (Hospital Universitario Parc Taulí, Sabadell); G. Rodríguez & L. Fernández-Pereira (Hospital San Pedro de Alcántara, Cáceres); A. Aguilera & S. Pereira (Hospital Conxo-CHUS, Santiago); J. García and R. Arcay (Complexo Hospitalario de Ourense); M. Trigo, J. Diz & M. García-Campello (Complejo Hospitalario, Pontevedra); S. Cortizo, S. Pérez & L. Morano (Hospital do Meixoeiro, Vigo); G. Reina (Clínica Universidad de Navarra, Pamplona); M. Arazamendi & Y. Salicio (Hospital Donostia, San Sebastián); E. Ugalde, M.C. Nieto & P. Liendo (Hospital Universitario de Basurto); A.J. Goikoetxea (Hospital Universitario de Cruces, Baracaldo); M.D. Ocete (Hospital General Universitario, Valencia); J.M. Ramos & I. Escribano (Hospital Universitario, Alicante); S. Sauleda & M. Pirón (Banco de Sangre & Tejidos, Barcelona); R. González, A. Richart & L. Barea (Centro de Transfusiones, Madrid); A. Jiménez & L. Blanco (Centro de Hemoterapia y Hemodonación de Castilla y León, Valladolid); L. Navarro (Centro de Transfusiones de la Comunidad Valenciana, Valencia); O. Ayerdi, B. Baza, C. Rodriguez & J. del Romero (Centro Sanitario Sandoval, IdISSC, Madrid); A. Galar, T. Aldamiz, M. Valeiro & L. Pérez (Hospital Gregorio Marañón, Madrid); I. Rodríguez-Avial (Hospital Clínico San Carlos, Madrid); L. Martín-Carbonero (Hospital Universitario La Paz, Madrid); M. Fernández-Ruiz, P. Parra, N. Redondo & T. Ruiz-Merlo (Hospital Universitario 12 de Octubre & CIBERINFEC, Madrid); M.J. Pozuelo (Universidad CEU-San Pablo, Madrid); P. Barreiro (Enfermera Isabel Zendal Emergency Hospital, Madrid); A. Treviño, F. de Jesús, O. Corral & V. Soriano (UNIR Health Sciences School, Madrid); I. Pintos, V. Moreno-Torres, M. Blanco, A. Huertas, J.A. Vargas-Núñez & C. de Mendoza (IIS Hospital Universitario Puerta de Hierro, Majadahonda).
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded in part by grant UNIR-itei 005/23, Fondos Feder-Instituto de Salud Carlos III (FIS-PI-21/1717) and Fundación Mutua Madrileña (AP-174112020).
Members of the Spanish HTLV Network.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gessain A, Cassar O. Epidemiological aspects and world distribution of HTLV-1 infection. Front Microbiol (2012) 3:388. doi: 10.3389/fmicb.2012.00388
2. Legrand N, McGregor S, Bull R, Bajis S, Valencia BM, Ronnachit A, et al. Clinical and public health implications of HTLV-1 infection. Clin Microbiol Rev (2022) 35:e0007821. doi: 10.1128/cmr.00078-21
3. Hirons A, Khoury G, Purcell D. HTLV-1: a lifelong persistent infection, yet never truly silent. Lancet Infect Dis (2021) 21:e2–e10. doi: 10.1016/S1473-3099(20)30328-5
4. Gessain A, Ramassamy JL, Afonso P, Cassar O. Geographic distribution, clinical epidemiology and genetic diversity of the human oncogenic retrovirus HTLV-1 in Africa, the world’s largest endemic area. Front Immunol (2023) 14:1043600. doi: 10.3389/fimmu.2023.1043600
5. Sampaio G, Ribeiro J, de Almeida C, Boa-Sorte N, Galvão-Castro B, Grassi M, et al. HTLV-1 global prevalence associated with the human development index: systematic review with meta-analysis. AIDS Res Hum Retroviruses (2023) 39:145–65. doi: 10.1089/aid.2021.0230
6. Caswell R, Manavi K. Emerging sexually transmitted infections: review of HTLV-1 disease. Int J STD AIDS (2022) 31:92–9. doi: 10.1177/0956462419886940
7. Oliveira-Filho A, Araújo A, Souza A, Gomes C, Silva-Oliveira G, Martins L, et al. HTLV-1 and -2 among people who used illicit drugs in the state of Pará, northern Brazil. Sci Rep (2019) 9:14750. doi: 10.1038/s41598-019-51383-7
8. Toro C, Rodés B, Poveda E, Soriano V. Rapid development of subacute myelopathy in three organ transplant recipients after transmission of HTLV-1 from a single donor. Transplantation (2003) 75:102–4. doi: 10.1097/00007890-200301150-00019
9. Percher F, Jeannin P, Martin-Latil S, Gessain A, Afonso P, Vidy-Roche A, et al. Mother-to-child transmission of HTLV-1: epidemiological aspects, mechanisms and determinants of mother-to-child transmission. Viruses (2016) 8:E40. doi: 10.3390/v8020040
10. Satake M, Iwanaga M, Sagara Y, Watanabe T, Okuma K, Hamaguchi I. Incidence of HTLV-1 infection in adolescent and adult blood donors in Japan: a nationwide retrospective cohort analysis. Lancet Infect Dis (2016) 16:1246–54. doi: 10.1016/S1473-3099(16)30252-3
11. Nunes D, Boa-Sorte N, Grassi MF, Taylor G, Teixeira M, Barreto M, et al. HTLV-1 is predominantly sexually transmitted in Salvador, the city with the highest HTLV-1 prevalence in Brazil. PloS One (2017) 12:e0171303. doi: 10.1371/journal.pone.0171303
12. Stuver S, Tachibana N, Okayama A, Shioiri S, Tsunetoshi Y, Tsuda K, et al. Heterosexual transmission of HTLV-1 among married couples in south western Japan: an initial report from the Miyazaki Cohort Study. J Infect Dis (1993) 167:57–65. doi: 10.1093/infdis/167.1.57
13. Zunt JR, Dezzutti CS, Montano SM, Thomas K, Alarcón J, Quijano E, et al. Cervical shedding of human T cell lymphotropic virus type I is associated with cervicitis. J Infect Dis (2002) 186:1669–72. doi: 10.1086/345364
14. Moriuchi M, Moriuchi H. Seminal fluid enhances replication of human T-cell leukemia virus type 1: implications for sexual transmission. J Virol (2004) 78:12709–11. doi: 10.1128/JVI.78.22.12709-12711.2004
15. Martel M, Gotuzzo E. HTLV-1 is also a sexually transmitted infection. Front Public Health (2022) 10:840295. doi: 10.3389/fpubh.2022.840295
16. Goudsmit J, de Wolf F, van de Wiel B, Smit L, Bakker M, Albrecht-van Lent N, et al. Spread of human T-cell leukaemia virus (HTLV-I) in the Dutch homosexual community. J Med Virol (1987) 23:115–21. doi: 10.1002/jmv.1890230204
17. Calderón EJ, Gómez-Lucia E, Aguado I, Pineda JA, Essex M, Leal M. Absence of HTLV-I and HTLV-II infection in prostitutes in the area of Seville, Spain. Eur J Clin Microbiol (1991) 10:773–5. doi: 10.1007/BF01972509
18. de Mendoza C, Caballero E, Aguilera A, Requena S, de Lejarazu R, Pirón M, et al. Human T-lymphotropic virus type 1 infection and disease in Spain. AIDS (2017) 31:1653–63. doi: 10.1097/QAD.0000000000001527
19. Guiraud V, Crémoux F, Leroy I, Cohier J, Hernandez P, Mansaly S, et al. Comparison of two new HTLV-I/II screening methods, Abbott Alinity i rHTLV-I/II and Diasorin LIAISON® XL murex recHTLV-I/II, to Abbott architect rHTLVI/II assay. J Clin Virol (2023) 164:105446. doi: 10.1016/j.jcv.2023.105446
20. Okuma K, Kuramitsu M, Niwa T, Taniguchi T, Masaki Y, Ueda G, et al. Establishment of a novel diagnostic test algorithm for human T-cell leukemia virus type 1 infection with line immunoassay replacement of western blotting: a collaborative study for performance evaluation of diagnostic assays in Japan. Retrovirology (2020) 17:26. doi: 10.1186/s12977-020-00534-0
21. de Mendoza C, Carrizo P, Sauleda S, Richart A, Rando A, Miró E, et al. The slowdown of new infections by human retroviruses has reached a plateau in Spain. J Med Virol (2023) 95:e28779. doi: 10.1002/jmv.28779
22. Soriano V, Blasco-Fontecilla H, Gallego L, Fernández-Montero JV, Mendoza C, Barreiro P. Rebound in sexually transmitted infections after the COVID-19 pandemic. AIDS Rev (2023) 26:127–35. doi: 10.24875/AIDSRev.23000015
23. Zheng Y, Yu Q, Lin Y, Zhou Y, Lan L, Yang S, et al. Global burden and trends of sexually transmitted infections from 1990 to 2019: an observational trend study. Lancet Infect Dis (2022) 22:541–51. doi: 10.1016/S1473-3099(21)00448-5
24. Fu L, Sun Y, Han M, Wang B, Xiao F, Zhou Y, et al. Incidence trends of five common sexually transmitted infections excluding HIV from 1990 to 2019 at the global, regional and national levels: results from the Global Burden of Disease Study 2019. Front Med (Lausanne) (2022) 9:851635. doi: 10.3389/fmed.2022.851635
25. Peters R, Chico R, Rowley J, Low N. Estimating the global burden of sexually transmitted infections. Lancet Infect Dis (2022) 22:1112–3. doi: 10.1016/S1473-3099(22)00415-7
26. Soriano V, del Romero J. Rebound in sexually transmitted infections following the success of antiretrovirals for HIV/AIDS. AIDS Rev (2018) 20:187–204. doi: 10.24875/AIDSRev.18000034
27. Sagara Y, Nakamura H, Satake M, Watanabe T, Hamaguchi I. Increasing horizontal transmission of HTLV type 1 in adolescents and young adults in Japan. J Clin Virol (2022) 157:105324. doi: 10.1016/j.jcv.2022.105324
28. Andani A, Bunge E, Kassianos G, Eeuwijk J, Mellou K, Van Damme P, et al. Hepatitis A occurrence and outbreaks in Europe over the past two decades: A systematic review. J Viral Hepat. (2023) 30:497–511. doi: 10.1111/jvh.13821
29. Huang M, Chen G, Sun H, Chen Y, Su L, Ho S, et al. Risky sexual practices and hepatitis C viremia among HIV-positive men who have sex with men in Taiwan. J Microbiol Immunol Infect (2023) 56:566–74. doi: 10.1016/j.jmii.2023.01.006
30. de Vries H, Götz H, Bruisten S, van der Eijk A, Prins M, Oude Munnink B, et al. Mpox outbreak among men who have sex with men in Amsterdam and Rotterdam, the Netherlands: no evidence for undetected transmission prior to May 2022, a retrospective study. Euro Surveill. (2023) 28:2200869. doi: 10.2807/1560-7917.ES.2023.28.17.2200869
31. Calabrese S, Krakower D, Willie T, Kershaw T, Mayer K. US guideline criteria for HIV pre-exposure prophylaxis: clinical considerations and caveats. Clin Infect Dis (2019) 69:884–9. doi: 10.1093/cid/ciz046
32. Bradshaw D, Khawar A, Patel P, Tosswill J, Brown C, Ogaz D, et al. HTLV seroprevalence in people using HIV pre-exposure prophylaxis in England. J Infect (2023) 86:245–7. doi: 10.1016/j.jinf.2023.01.033
33. Machuca A, Rodés B, Soriano V. The effect of antiretroviral therapy on HTLV infection. Virus Res (2001) 78:93–100. doi: 10.1016/S0168-1702(01)00287-8
34. Bradshaw D, Taylor G. HTLV-1 transmission and HIV pre-exposure prophylaxis: a scoping review. Front Med (2022) 9:881547. doi: 10.3389/fmed.2022.881547
35. Schneiderman B, Barski M, Maertens G. Cabotegravir, the long-acting integrase strand transfer inhibitor, potently inhibits HTLV-1 transmission in vitro. Front Med (2022) 9:889621. doi: 10.3389/fmed.2022.889621
36. Soriano V, Vallejo A, Gutiérrez M, Tuset C, Cilla G, Martínez-Zapico R, et al. Epidemiology of human T-lymphotropic virus type II (HTLV-II) infection in Spain. HTLV Spanish Study Group Eur J Epidemiol. (1996) 12:625–9. doi: 10.1007/BF00499462
37. de la Fuente L, Toro C, Soriano V, Brugal M, Vallejo F, Barrio G, et al. HTLV infection among young injection and non-injection heroin users in Spain: prevalence and correlates. J Clin Virol (2006) 35:244–9. doi: 10.1016/j.jcv.2005.06.006
38. Lehky T, Flerlage N, Katz D, Houff S, Hall WH, Ishii K, et al. Human T-cell lymphotropic virus type II-associated myelopathy: clinical and immunologic profiles. Ann Neurol (1996) 40:714–23. doi: 10.1002/ana.410400507
39. Blanco S, Barile ME, Frutos MC, Vicente ACP, Gallego SV. Neurodegenerative disease in association with sexual transmission of human T-cell lymphotropic virus type 2 subtype b in Argentina. Trans R Soc Trop Med Hyg (2022) 116:622–7. doi: 10.1093/trstmh/trab173
40. Bassani S, Toro C, Jiménez V, Rodés B, Soriano V. Can the level of immunosuppression in HIV -infected patients affect the reliability of human T-cell lymphotropic virus type 2 serological diagnosis? Clin Vaccine Immunol (2006) 13:160–1. doi: 10.1128/CVI.13.1.160-161.2006
41. Campos K, Santos F, da Silva Brito V, Gonçalves N, Araujo T, Galvão-Castro B, et al. Line immunoassay for confirmation and discrimination of Human T-Cell Lymphotropic Virus infections in inconclusive Western blot serum samples from Brazil. J Clin Microbiol (2019) 58:e01384–19. doi: 10.1128/JCM.01384-19
42. Ramos JM, de Mendoza C, Aguilera A, Barreiro P, Benito R, Eiros JM, et al. Hospital admissions in individuals with HTLV-1 infection in Spain. AIDS (2020) 34:1019–27. doi: 10.1097/QAD.0000000000002508
Keywords: HTLV-1, sexually transmitted infections, syphilis, HIV, transmission
Citation: Ayerdi O, Benito R, Ortega D, Aguilera A, Montiel N, Pintos I, Díaz de Santiago A, Baza B, Soriano V and de Mendoza C (2023) HTLV infection in persons with sexually transmitted diseases in Spain. Front. Immunol. 14:1277793. doi: 10.3389/fimmu.2023.1277793
Received: 15 August 2023; Accepted: 13 November 2023;
Published: 07 December 2023.
Edited by:
Nilu Goonetilleke, University of North Carolina at Chapel Hill, United StatesReviewed by:
Tesfaye Gelanew, Armauer Hansen Research Institute (AHRI), EthiopiaCopyright © 2023 Ayerdi, Benito, Ortega, Aguilera, Montiel, Pintos, Díaz de Santiago, Baza, Soriano and de Mendoza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente Soriano, vicente.soriano@unir.net
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.