 Lucianne Righeti Monteiro Tannus*
Lucianne Righeti Monteiro Tannus* Karla Rezende Guerra DrummondEliete Leão da Silva ClementeMaria de Fátima Bevilacqua da MattaMarilia Brito Gomes on behalf of the Brazilian Type 1 Diabetes Study Group (BrazDiab1SG)
Karla Rezende Guerra DrummondEliete Leão da Silva ClementeMaria de Fátima Bevilacqua da MattaMarilia Brito Gomes on behalf of the Brazilian Type 1 Diabetes Study Group (BrazDiab1SG)- Unit of Diabetes, Department of Medicine, State University Hospital of Rio de Janeiro (UERJ), Rio de Janeiro, Brazil
Cardiovascular disease (CVD) is the leading cause of mortality in patients with type 1 diabetes (T1D). The cardiovascular autonomic neuropathy (CAN), although considered as an independent risk factor for CVD, remains underdiagnosed. The aim of this paper was to determine the prevalence, predictors of CAN in patients with T1D and its association with other chronic complications of diabetes. Patients with T1D underwent a clinical-epidemiological survey, had blood and urinary samples collected, performed ophthalmoscopic and clinical neurological examination and cardiovascular reflex tests. One hundred and fifty one patients with T1D, 53.6% female, 45.7% Caucasian, mean age of 33.4 ± 13 years, diabetes duration of 16.3 ± 9.5 years, and glycated hemoglobin levels of 9.1 ± 2% were evaluated. The prevalence of CAN in the studied population was 30.5%. CAN was associated with age (p = 0.01), diabetes duration (p = 0.036), hypertension (p = 0.001), resting heart rate (HR) (p = 0.000), HbA1c (p = 0.048), urea (p = 0.000), creatinine (p = 0.008), glomerular filtration rate (p = 0.000), urinary albumin concentration (p = 0.000), LDL (p = 0.048), free T4 (p = 0.023), hemoglobin (p = 0.01) and presence of retinopathy (p = 0.000), nephropathy (p = 0.000) and diabetic neuropathy (p = 0.000), the following symptoms syncope (p = 0.000), post prandial nausea (p = 0.042), early satiety (p = 0.031), sexual dysfunction (p = 0.049), and gustatory sweating (p = 0.018). In logistic regression model, it was observed that only resting HR, diabetic neuropathy, and retinopathy were independent associated with CAN. In conclusion, CAN is a common chronic complication of T1D affecting about 30% of the studied population and is associated with the presence of other chronic complications. Indicators of CAN included age, diabetes duration, hypertension, resting HR, diabetic neuropathy and retinopathy, and symptoms suggestive of autonomic neuropathy. This study confirms the importance of systematic and early screening for CAN.
Introduction
Type 1 diabetes (T1D) is the most common endocrine disorder of childhood and adolescence affecting about 10–20 million people worldwide (1). Poor glycemic control is associated with the development of micro and macrovascular chronic complications leading to a major impact on morbidity and mortality (2). Cardiovascular disease (CVD) is the leading cause of mortality in patients with T1D (3–5).
Cardiovascular autonomic neuropathy (CAN) although considered a common diabetic chronic complication (6) and associated with increased cardiovascular morbidity and mortality, remains underdiagnosed (6, 7).
Depending on the methodology and diagnostic criteria, the prevalence of CAN ranges from 2.6 to 90% among patients with diabetes and its prevalence increases with age, diabetes duration, and inappropriate glycemic control (8, 9) and may be associated with peripheral neuropathy (up to 62.5% of cases) and the presence of other cardiovascular risk factors, such as hypertension, dyslipidemia, diabetic nephropathy and retinopathy, arterial stiffness, left ventricular hypertrophy, and diastolic dysfunction (9, 10).
Cardiovascular autonomic neuropathy has been identified as a strong predictor of CVD in both patients with T1D and type 2 diabetes (T2D). Patients with diabetes and CAN have 5-year mortality rates ranging from 16 to 53%, depending on its severity (8).
In the DIAD study (Detection of silent myocardial ischemia in asymptomatic diabetic subjects) conducted in patients with T2D, the presence of CAN, determined by abnormal Valsalva ratio, was a strong predictor of silent myocardial ischemia, regardless of the presence of traditional cardiovascular risk factors such as hypertension, age, sex, and smoking (11–13).
Data from the Action to Control Cardiovascular Risk in Diabetes (ACCORD) study showed that patients with CAN presented mortality rate approximately 1.55–2.14 times higher than patients without CAN (14).
Unfortunately, clinical symptoms of CAN appears late in the course of the disease, which makes the use of cardiovascular reflex tests critical for CAN diagnosis (15–17). However, the presence of symptoms suggestive of dysautonomia as syncope, postprandial hypotension, exercise intolerance, resting tachycardia, gastroparesis, diarrhea, urinary incontinence, and erectile dysfunction may suggest the presence of CAN and these patients should be investigated (7).
According to Toronto Consensus, the analysis of heart rate variability (HRV) using the variation of RR intervals of the electrocardiogram are sensitive and specific methods used for the early detection of CAN and seven parameters can be used to assess the presence of CAN: the three spectral analysis frequency bands [very low frequency (VLF), low frequency (LF) and high frequency (HF)] and four tests proposed by Ewing [heart rate (HR) response to the Valsalva maneuver, to deep breathing, and to standing and the blood pressure response to standing] (17, 18).
The consensus of Diabetic Neuropathy Conference held in San Antonio in 1992 (15), of the Toronto Diabetic Neuropathy (17, 18), and the Study Group on the Diabetic Neuropathy Italian Society of Diabetology (16), advocates the use of cardiovascular reflex tests (deep breathing test, orthostatic test, OH test, and Valsalva test) as the gold standard tests for the diagnosis of CAN.
The time and frequency-domain HRV parameters seem to be more sensitive and changes in HRV may occur earlier than alterations on cardiovascular reflex tests. Tannus et al. (19) showed that short-term spectral analysis of HRV (VLF, HF, and LF) despite being a low cost, non-invasive, easy to perform, and does not require active cooperation of patients, demonstrated poor reproducibility (20–24) being thus considered as additional tests for the diagnosis of NAC (15–17).
Considering the paucity of data in the literature on the prevalence of CAN in the Brazilian population with T1D, this study aimed to determine the prevalence of CAN in Brazilian patients with T1D and to identify clinical and laboratory factors associated with the presence of CAN.
Materials and Methods
This study is a cross-sectional study conducted in patients with T1D attended in the diabetes unit of State University of Rio de Janeiro. Written informed consent for the study was obtained from all of the patients aged 18 years or older or from the parents or guardians of the patients younger than 18 years. The study was approved by each local center’s ethics committee.
The inclusion criteria were patients with T1D, defined by a physician based on the criteria of American Diabetes Association (ADA) and Brazilian Diabetes Society (BDS), which include age less than 40 years old at diagnosis, typical clinical presentation (weight loss, polyuria, polydipsia), or history of diabetic ketoacidosis or ketonemia and need to use insulin without interruption since the diagnosis; age ≥13 years and diabetes duration ≥5 years. Exclusion criteria were pregnancy, lactation, chronic alcoholism, congestive heart failure, cardiac arrhythmias, acute respiratory failure or severe obstructive lung disease, infections, and acute complications of diabetes.
The following clinical and demographic data were obtained through an interview during a clinical visit: sex, age (years), weight (kg), height (m), body mass index [BMI (Kg/m2)], systolic (sBP) and diastolic blood pressure [dBP (mmHg)], HR, ethnicity, age at diagnosis (years), duration of diabetes (years), smoking status, alcohol consumption, daily insulin dose, use of other medications, and associated diseases.
Body mass index was calculated by dividing weight (kg) by height squared (m2). Individuals aged ≥18 years and BMI ≥25 and 30 kg/m2, were considered as overweight and obesity respectively and in subjects <18 years overweight was defined if BMI ≥85th percentile and obesity if BMI ≥95th percentile, according with growth charts from Center for Disease Control CDC), respectively (25).
Hypertension was defined as sBP ≥140 mmHg and/or dBP ≥90 mmHg or on therapy for hypertension (26) and in subjects <18 years as sBP and/or dBP >95 percentile according to sex, age, and height (27).
The following laboratory variables were performed: fasting plasma glucose (FPG), postprandial glucose (PPG), glycated hemoglonin (HbA1c), total cholesterol, high density lipoprotein (HDL), triglycerides, uric acid, plasma creatinine, plasma urea, sodium, potassium, liver enzymes [aspartate (AST) and alanine aminotransferase (ALT)], creatine phosphokinase (CPK), thyroid stimulating hormone (TSH), free T4, cyanoconalamin, and C-reactive protein (CRP). The low-density lipoprotein (LDL) was calculated using the Friedewald formula (LDL = total cholesterol − HDL + Triglycerides/5), when the values of triglycerides did not exceed 400 mg/dl (28).
Screening for retinopathy by fundoscopy and nephropathy by albuminuria and determination of glomerular filtration rate (GFR) was performed.
The diagnosis of micro and macroalbuminuria was established by urinary albumin concentration of respectively 17–173 mg/dl and ≥174 mg/dl, at least two random urine specimen (29). The GFR was calculated from the chronic kidney disease epidemiology collaboration (CKD-EPI) (30) equation in patients aged >16 years and the Schwartz equation for children and adolescents and was considered normal if GFR >60 ml/min/1.73 m2 (31, 32).
Screening for sensory motor neuropathy was performed by the neuropathic disability score (NDS) and neuropathic impairment score (NIS) (33, 34).
The evaluation of CAN was performed according to the protocol described elsewhere (19). Briefly, the subjects were instructed to refrain from drinking alcohol- or caffeine-containing beverages and to engage in smoking cessation for a minimum of 8 h prior to testing and to refrain from strenuous exercise for at least 24 h preceding the examination. The exclusion criteria were fever in the last two days, emotional distress on the day before the autonomic tests and arrhythmias.
Autonomic tests were performed in the morning. Subjects were instructed to assume the supine position in a metabolic unit with a controlled temperature (23°C) after an overnight fast or at least 2 h after a light meal (containing a total of 300 Kcal) standardized by a dietitian.
After 5 min of rest in the supine position with the head elevated 30° and after 5 min of breathing spontaneously, an electrocardiogram (EKG) was recorded for 300 s using a computer. The EKG was analyzed by a mathematical algorithm (fast Fourier transform) and expressed in a diagram of oscillation amplitude (HR variations per second) versus frequency (Hz).
The autonomic tests are described below. After each test, a resting period of 1 min was scheduled to prevent influences by the previous tests.
Deep Breathing Test
The subject was kept in the supine position for at least 1 min and then invited to start the test with a deep inspiration to the maximum total lung capacity for 5 s, which was followed by a forced expiration down to the residual volume for 5 s. The time to alternate the respiratory cycle is signaled directly to the patient by the operator. Such a respiratory cycle was repeated three times. The expiration:inspiration ratio (E:I ratio) was determined by the ratio between the longest and shortest RR intervals obtained during the expiration and inspiration cycles, respectively, and the highest E:I ratio was considered (16).
Valsalva Maneuver
Without taking a deep breath beforehand, the subject, who was in the supine position, was invited to blow with an open glottis into a mouthpiece connected to a manometer and to maintain a constant expiratory effort equivalent to an intraoral pressure of 40 mmHg for 15 s. This test induces a physiological tachycardia, which persists for a maximum of approximately 14 s. After this period, the expiratory straining is suddenly released, and the subject should breathe regularly and remain silent and motionless until the end of the test. An EKG was continuously recorded for 70 s, when the physiological bradycardia is observed. The Valsalva ratio was determined by the ratio between the longest and shortest RR intervals. The occurrence of facial flushing, plethora, and neck vein engorgement testify to the correctness of the maneuver (7, 24). The test was performed twice, and the highest Valsalva ratio was considered.
Orthostatic Test
After lying in the supine position for at least 5 min, the subject was invited to stand up quickly but remain relaxed with their arms at rest alongside the body and without speaking or moving until the end of the test (180 s after standing up). The 30:15 or maximum:minimum (max:min) ratio was determined by the ratio between the longest (maximum bradycardia at approximately the 30th beat) and shortest (maximum tachycardia at approximately the 15th beat) RR intervals.
Orthostatic Hypotension Test
After at least 5 min of supine rest, the blood pressure was measured at baseline and after 3 min of standing. A drop in the systolic blood pressure that was higher than or equal to 20 mmHg was considered abnormal (7, 24).
The diagnosis of incipient and defined CAN was considered in the presence of one and two abnormal cardiovascular reflex tests, respectively (17, 35).
Statistical analysis
The statistical analysis was performed using Statistical Package for Social Sciences (SPSS) for Windows (version 13.0). The data are presented as mean ± SD and median (minimum–maximum). Comparison between numeric variables was performed using t-test and Mann–Whitney test for variables with normal or skewed distribution, respectively. The chi-square test was used to compare the frequencies of two categorical variables. A Pearson’s correlation coefficient was calculates when applicable. Adjustments were made for potential confounders. A binary logistic regression was performed with diagnosis of CAN (yes/no) as the dependent variable. The following independent variables were included: sex, age, diabetes duration, pulse pressure, resting HR, BMI, hypertension, presence of micro or macroalbuminuria, presence of diabetic neuropathy and retinopathy, HbA1c, urea, creatinine, LDL cholesterol, and hemoglobin. Odds ratios with 95% confidence intervals (CI) were performed when indicated. A two-sided p-value less than 0.05 was considered significant.
Results
One hundred and fifty-one patients with T1D were evaluated. Clinical and demographic data for the study population are presented in Table 1.
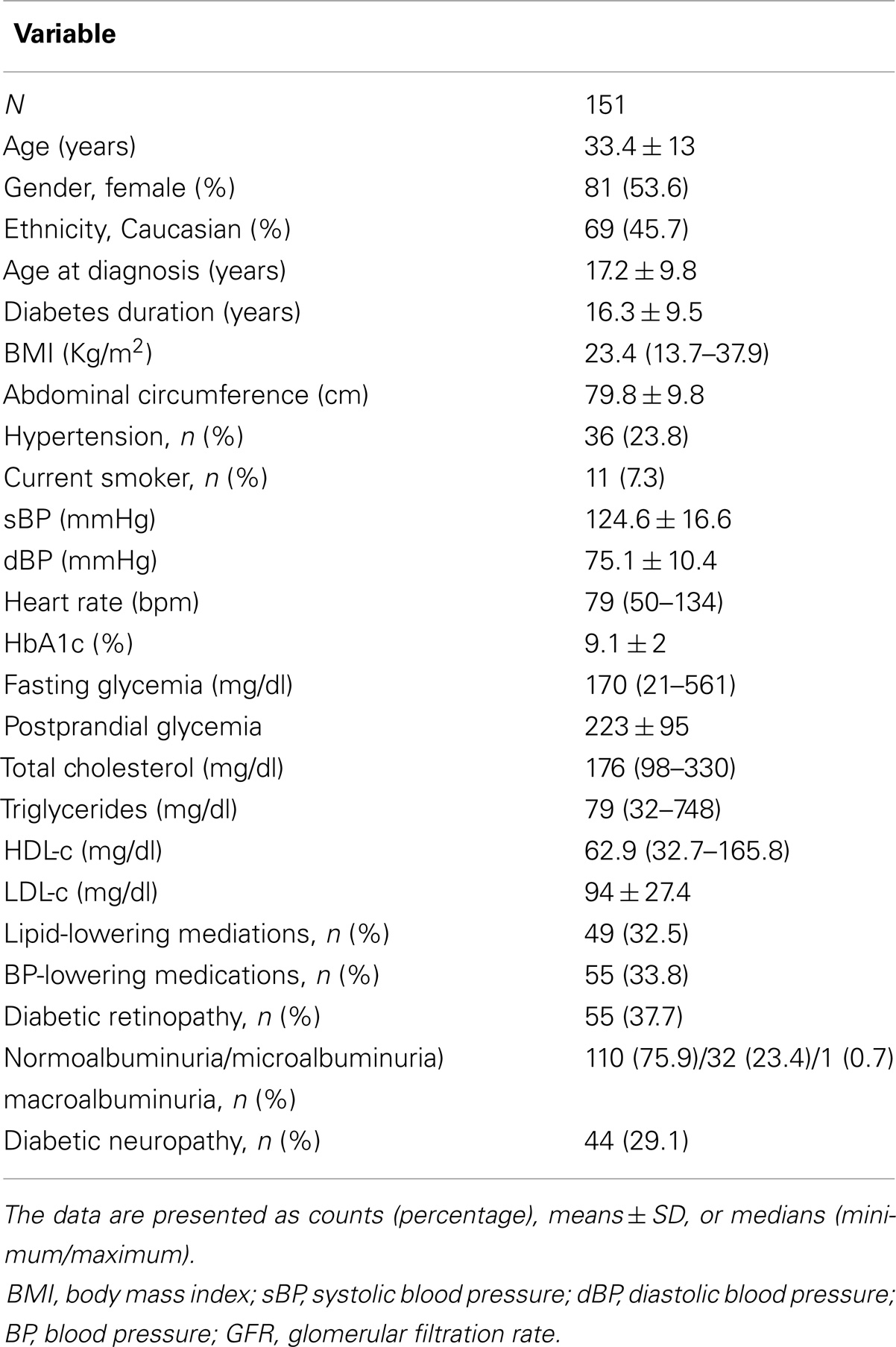
Table 1. Clinical and demographic data of the studied population.
Table 2 presents the variables used for assessment of CAN in the study population and in subgroups of patients with and without CAN. The prevalence of CAN as assessed only by HRV (spectral analysis) was higher than the prevalence of CAN assessed by cardiovascular reflex tests and showed moderate agreement (kappa = 0.44/p = 0.074). Data about the prevalence of CAN according to the diagnostic criteria are shown in Table 3.
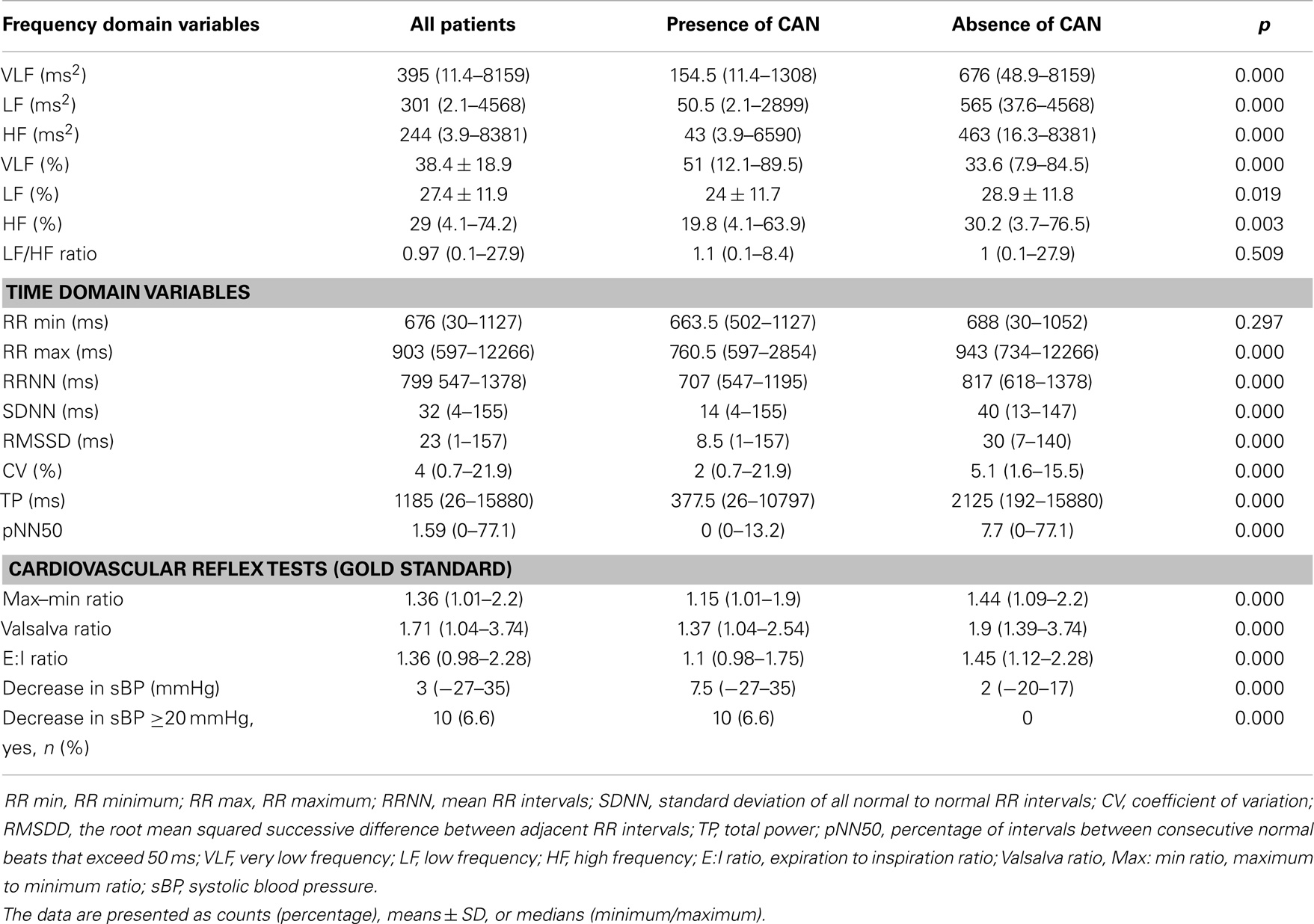
Table 2. Variables used for assessment of CAN.
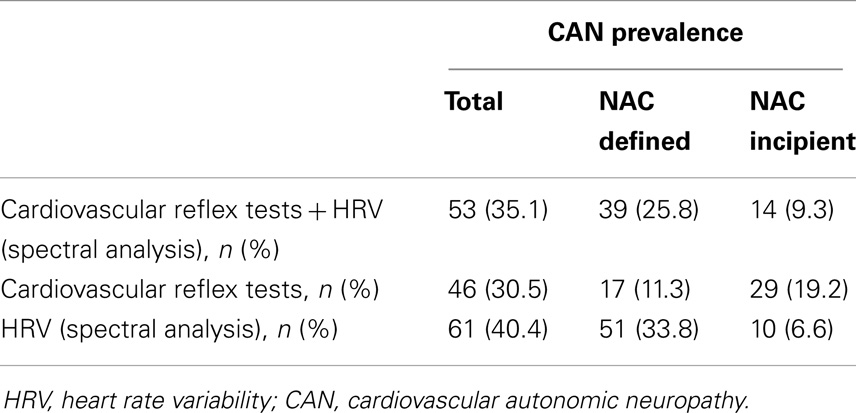
Table 3. Prevalence of CAN according to the diagnostic criteria.
The prevalence of autonomic symptoms in the general population, in patients with and without CAN is shown in Table 4. Symptoms associated with the presence of CAN were syncope (p = 0.000), postprandial nausea (p = 0.042), early satiety (p = 0.031), sexual dysfunction (p = 0.049), and gustatory sweating (p = 0.018).
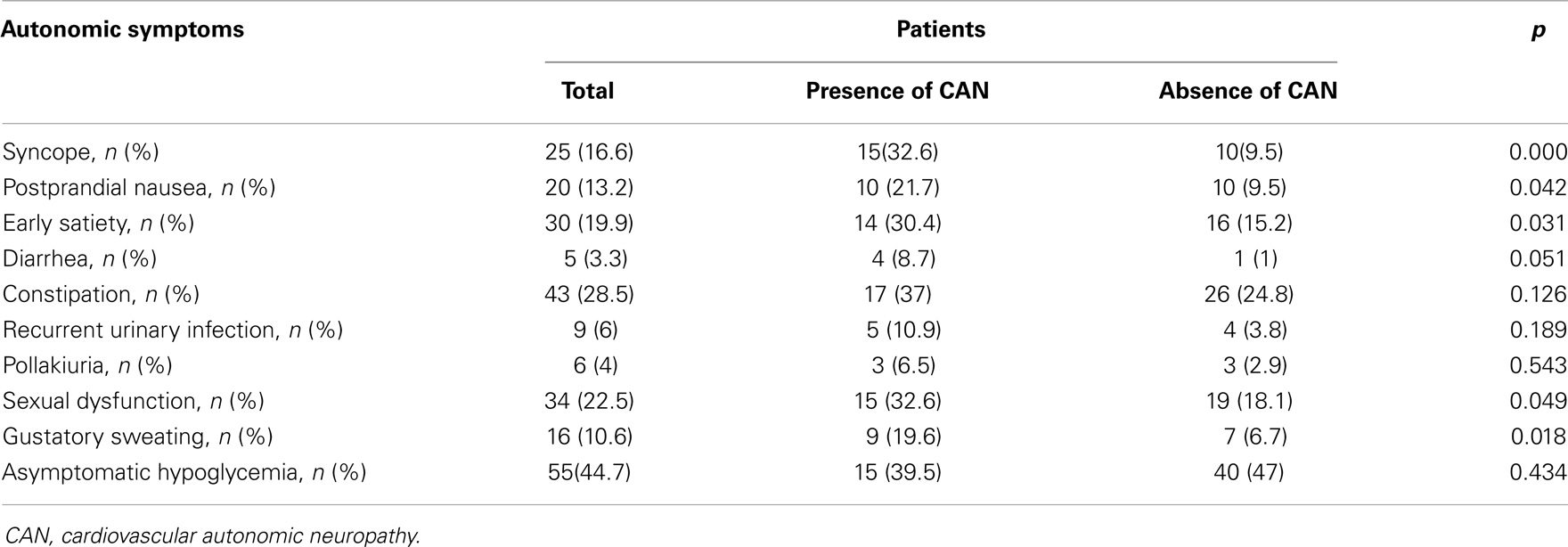
Table 4. Prevalence of autonomic symptoms in patients with and without CAN.
The clinical and laboratory predictors of CAN found in the studied population were age (p = 0.01), diabetes duration (p = 0.036), hypertension (p = 0.048), resting HR (p = 0.000), HbA1c (p = 0.048), urea (p = 0.000), creatinine (p = 0.008), GFR (p = 0.000), urinary albumin concentration (p = 0.000), LDL-cholesterol (p = 0.048), free T4 (p = 0.023), and hemoglobin (p = 0.01) (Table 5). All microvascular chronic complications were related to the presence of CAN (Table 5). Only 1 (2.2%) patients with CAN presented levels of HbA1c lower than 7% compared with 18 (17.2%) in patients without CAN (p = 0.011).
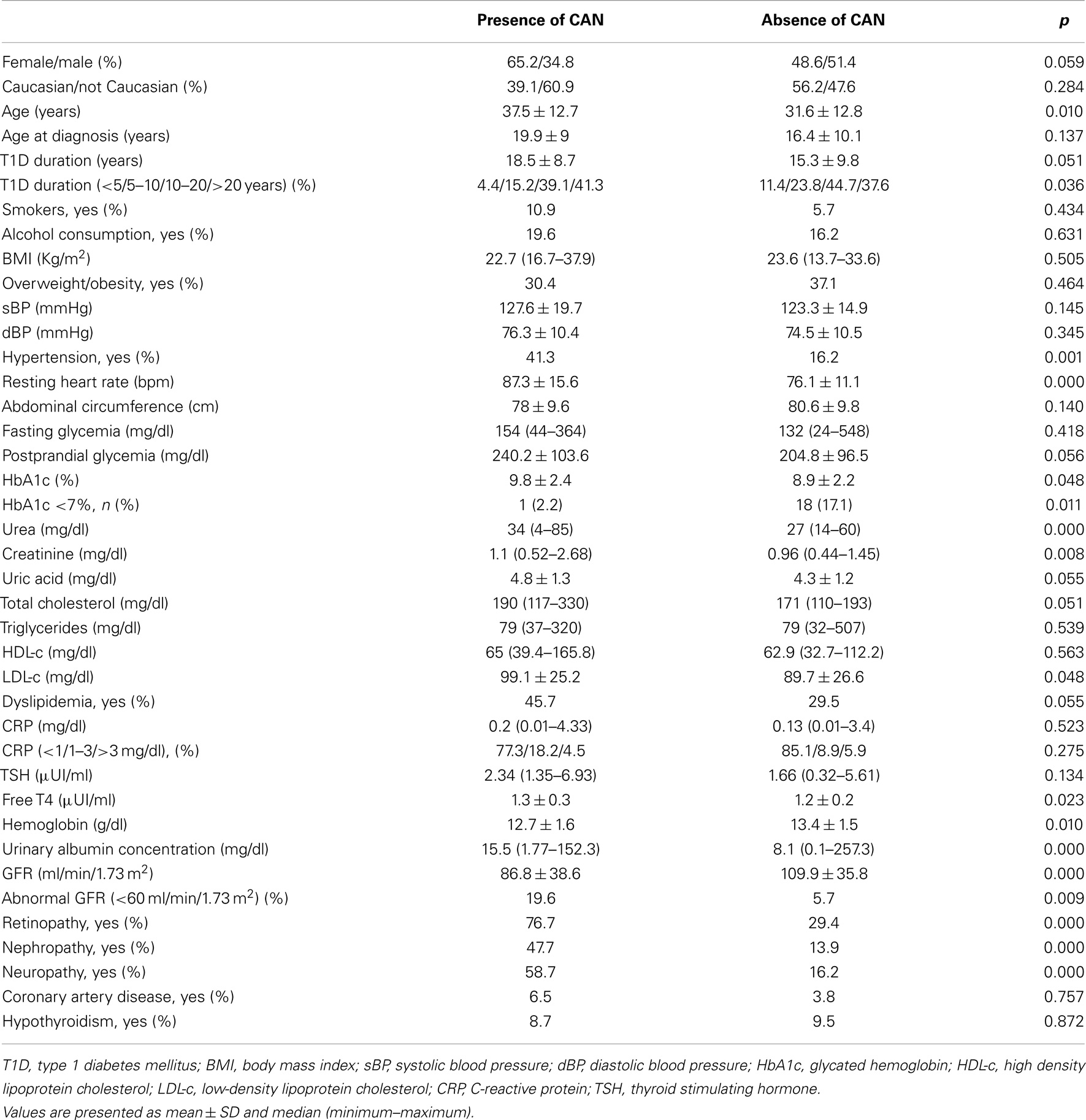
Table 5. Predictors of CAN in the studied population.
After logistic regression model using diagnosis of CAN by cardiovascular reflex testes as a dependent variable and sex, age, diabetes duration, pulse pressure (calculated as the difference between the sBP and dBP), resting HR, BMI, hypertension, albuminuria, presence of diabetic neuropathy and retinopathy, HbA1c, urea, creatinine, LDL, and hemoglobin as independent variables, it was observed that only resting HR, presence of diabetic neuropathy and retinopathy were significantly independent variables associated with the diagnosis of CAN (Table 6).
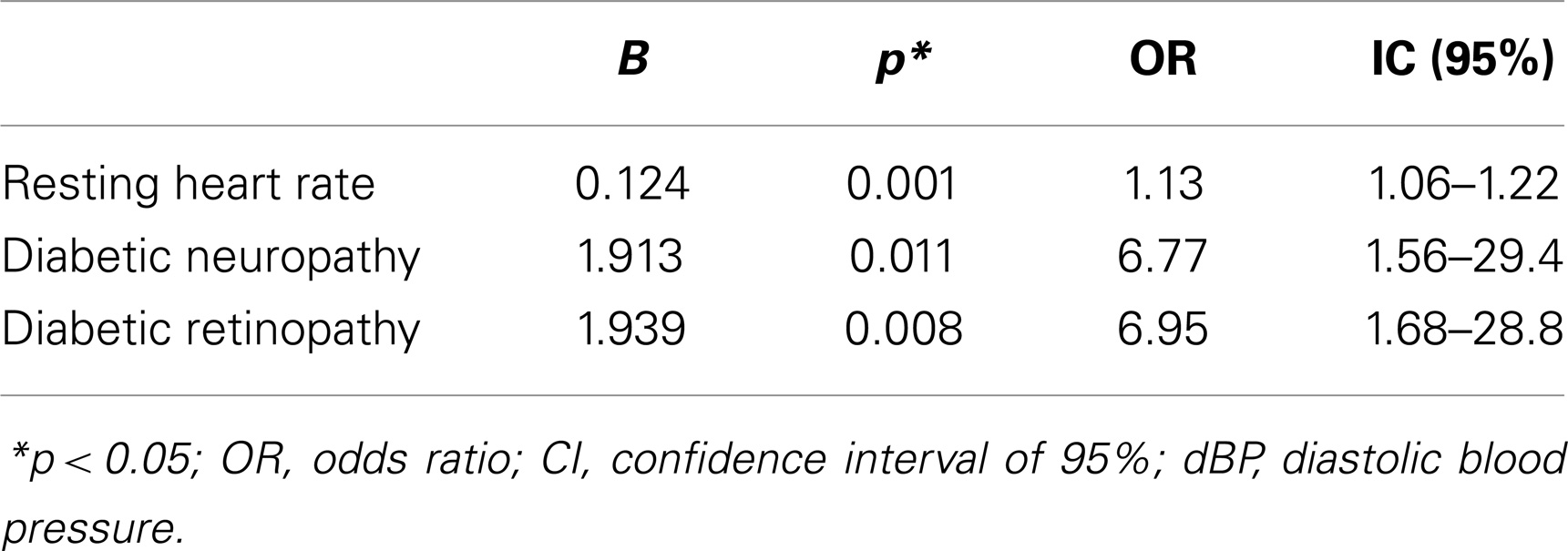
Table 6. Logistic regression with the diagnosis of cardiovascular reflex tests as the dependent variable.
Discussion
In the present study, the prevalence of incipient, defined, and total CAN in patients with T1D and T1D duration ≥5 years was 19.2, 11.3, and 30.5%, respectively when used only cardiovascular reflex tests; 6.6, 33.8, and 40.4% when using the HRV parameters (spectral analysis) and 9.3, 25.8, and 35.1% when used both criteria. The prevalence of CAN assessed by cardiovascular reflex tests was lower than the prevalence reported in the literature (11.3 versus 25%), but quite similar when using cardiovascular reflex tests associated with the HRV parameters (spectral analysis) (25.8 versus 25%). As we can see, the prevalence of CAN defined by HRV (spectral analysis) was superior to cardiovascular reflex tests, which could corroborate the data from the literature regarding the sensitivity and early detection of cardiovascular autonomic dysfunction by this diagnostic criterion. However, the diagnosis of CAN based only on spectral analysis must be carefully considered since previous study from our group (19) demonstrated that the assessment of HRV by spectral analysis (VLF, LF and HF) showed low reproducibility.
The agreement of CAN diagnosis for the two diagnostic methods (cardiovascular reflex tests versus spectral analysis) was moderate. Therefore, analysis of CAN using only frequency-domain HRV analysis should be considered an additional tool for CAN diagnosis according to other studies (16–18, 36).
The incidence of CAN increases with age, diabetes duration and poor glycemic control. (7,8) In this study, clinical and laboratory predictors of CAN were age, T1D duration >10 and 20 years, hypertension, resting HR, HbA1c, LDL-c, urea, creatinine, free T4 and hemoglobin, and the presence of retinopathy, nephropathy and diabetic peripheral neuropathy. Slightly higher levels of free T4, even within the normal range were found in patients with T1D and CAN, possibly suggesting a sympathovagal imbalance (16).
Some studies showed that CAN can reduce the renal release of erythropoietin probably by renal denervation, leading to the development of anemia (37, 38). In our study, we observed that patients with T1D and CAN had lower hemoglobin levels, corroborating the above mentioned data. Patients with T1D and proteinuria may have anemia by erythropoietin deficiency, even in the absence of changes in GFR (38).
However, it is difficult to differentiate whether the anemia was a result of CAN or diabetic nephropathy since these two diabetic complications are frequently associated.
Several studies have suggested a causal relationship between CAN and diabetic nephropathy (39, 40). Forsen et al (39) evaluated the prevalence of microalbuminuria and CAN after 14 years of follow-up and observed that CAN precedes the development of albuminuria in patients with T1D. In patients with T1D and CAN, the sympathovagal imbalance (assessed by abnormal E:I ratio) promotes increase in nocturnal BP (reduction of parasympathetic activity) with consequent overnight increase in intraglomerular pressure, and daytime reduction in intraglomerular pressure as a result of postural hypotension (39, 41). CAN appears to be a permissive factor for the development of persistent microalbuminuria (39). In our study urinary albumin concentration and GFR were associated with the presence of CAN, corroborating the association of these two complications. This study was a cross-sectional study and could not establish a causal relationship between diabetic nephropathy and CAN.
Inflammatory markers such as CRP and IL-6 have been correlated with abnormal HRV (6). One study evaluated 611 healthy subjects and showed an inverse correlation between CRP levels and HRV parameters (42). Ridker et al (43, 44) have shown an association of CRP levels >3 mg/dl with high cardiovascular risk. In the current study, we found no statistically significant association between CRP levels and CAN, which could be explained by the fact that only 8 patients had CRP levels ≥3 mg/dl.
Autonomic symptoms, although disabling, appears in more advanced stages of CAN, have low sensitivity and specificity and have low association with abnormal cardiovascular reflex tests (6, 17, 18). Symptoms associated with CAN in this study symptoms were syncope, postprandial nausea, early satiety, sexual dysfunction and gustatory sweating. Therefore, autonomic symptoms did not seems to represent sensitive indicators for early diagnosis of CAN (16).
This study is one of the first studies that evaluated the prevalence of CAN assessed by the gold standard cardiovascular reflex tests as recommended by the ADA in the Brazilian population, thus allowing the identification of patients with T1D and increased cardiovascular risk. Moreover, this study allowed the identification of some clinical factors that might suggest the diagnosis of CAN.
The study had some limitations. Because this was a cross-sectional study we could not establish a causal relationship between the predictors and the diagnosis of CAN. Another limitation is related to data collection on hypoglycemia. Patients self-reported the number and severity of hypoglycemic episodes in the last month. It was not possible to obtain data through the glucometer of all patients, which could underestimate the prevalence of hypoglycemia.
In conclusion, CAN is a common chronic complication of T1D affecting about 30% of the studied population and is associated with the presence of other chronic complications of T1D. Indicators of the presence of CAN included age, duration of diabetes, presence of hypertension, resting HR, presence of diabetic neuropathy and retinopathy and symptoms suggestive of autonomic neuropathy. This study confirms the importance of systematic and early screening for this complication.
Author Contributions
Lucianne Righeti Monteiro Tannus and Marilia Brito Gomes researched data, drafted the manuscript. Karla Rezende Guerra Drummond, Eliete Leão da Silva Clemente, and Maria de Fátima Bevilacqua da Matta contributed to the conception of the work and the acquisition of data for the work. Lucianne Righeti Monteiro Tannus and Marilia Brito Gomes reviewed the manuscript and contributed to the discussion. The writing group takes final responsibility for the paper and is the study guarantor.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Elisangela Santos for her technical assistance. This work was supported by grants from Farmanguinhos/Fundação do Amparo à Pesquisa do Estado do Rio de Janeiro, and Conselho Nacional de Desenvolvimento Científico e Tecnológico do Brasil (5637532010/2).
References
1. American Diabetes Association. Diabetes statistics for Youth. American Diabetes Association (2004). http://www.niddk.nih.gov/news/research-updates/Pages/Rates-of-Diabetes-Increasing-in-U-S--Youth.aspx
2. DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. NEJM (1993) 329:977–86. doi: 10.1056/NEJM199309303291401
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
3. Libby P, Nathan DM, Abraham K, Brunzell JD, Fradkin JE, Haffner SM, et al. Report of the National Heart, Lung, and Blood Institute; National Institute of Diabetes and Digestive and Kidney Diseases Working Group on Cardiovascular Complications of Type 1 Diabetes Mellitus. Circulation (2005) 111:3489–93. doi:10.1161/CIRCULATIONAHA.104.529651
4. Zgibor CJ, Piatt GA, Ruppert K, Orchard TJ, Roberts MS. Deficiencies of cardiovascular risk prediction models for type 1 diabetes. Diabetes Care (2006) 8:1860–5. doi:10.2337/dc06-0290
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Laing SP, Swerdlow AJ, Slater SD, Burden AC, Morris A, Waugh NR, et al. Mortality from heart disease in a cohort of 23,000 patients with insulin-treated diabetes. Diabetologia (2003) 46:760–5. doi:10.1007/s00125-003-1116-6
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. Vinik AI, Erbas T, Casellini CM. Diabetic cardiac autonomic neuropathy, inflammations and cardiovascular disease. J Diabetes Investigat (2013) 4:4–18. doi:10.1111/jdi.12042
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
7. Rolim LCS, Sá JR, Chacra AR, Dib AS. Diabetic cardiovascular autonomic neuropathy: risk factors, clinical impact and early diagnosis. Arq Bras Cardiol (2008) 90:e23–31. doi:10.1590/S0066-782X2008000400014
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Schmid H. Impacto cardiovascular da neuropatia autonômica do diabetes mellitus. Arq Bras Endocrinol Metabol (2007) 51:232–43. doi:10.1590/S0004-27302007000200012
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
9. Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation (2007) 115:387397. doi:10.1161/CIRCULATIONAHA.106.634949
10. Prince CT, Secrest AM, Mackey RH, Arena VC, Kingsley LA, Orchard TJ. Cardiovascular autonomic neuropathy, HDL cholesterol, and smoking correlate with arterial stiffness markers determined 18 years later in type 1 diabetes. Diabetes Care (2010) 33:652–7. doi:10.2337/dc09-1936
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
11. Frans JTH, Wackers FJT, Young LH, Inzucchi SE, Chyun DA, Davey JA, et al. For the detection of ischemia in asymptomatic diabetics (DIAD) investigators. Detection of silent myocardial ischemia in asymptomatic diabetic subjects. Diabetes Care (2004) 27:1954–61. doi:10.2337/diacare.27.8.1954
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
12. Wackers FJT, Chyun DA, Young LH, Heller GV, Iskandrian AE, Davey JA, et al. For the detection of ischemia in asymptomatic diabetics (DIAD) investigators. Resolution of asymptomatic myocardial ischemia in patients with type 2 diabetes in the detection of ischemia in asymptomatic diabetics (DIAD) study. Diabetes Care (2007) 30:2892–8. doi:10.2337/dc07-1250
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
13. Wackers FJT, Chyun DA, Young LH, Heller GV, Iskandrian AE, Davey JA, et al. For the detection of ischemia in asymptomatic diabetics (DIAD) investigators. Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes. JAMA (2009) 15:1547–55. doi:10.1001/jama.2009.476
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
14. Pop-Busui R, Evans G, Gerstein H, Fonseca V, Fleq JL, Hooqwerf BJ, et al. The ACCORD study group. Effects of cardiac autonomic dysfunction on mortality risk in the action to control cardiovascular risk in diabetes (ACCORD) Trial. Diabetes Care (2010) 33:1578–84. doi:10.2337/dc10-0125
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
15. American Diabetes Association and American Academy of Neurology: Consensus Statement. Report and recommendations of the San Antonio conference on diabetic neuropathy. Diabetes Care (1988) 11:592–7.
16. Spallone V, Bellavere F, Scionti L, Maule S, Quadril R, Bax G, et al. On behalf of the Diabetic Neuropathy Study Group of the Italian Society of Diabetology. Recommendations for the use of cardiovascular tests in diagnosing diabetic autonomic neuropathy. Nutrit Metab Cardiovasc Dis (2011) 21:69–78. doi:10.1016/j.numecd.2010.07.005
17. Tesfaye S, Boulton AJM, Dyck PJ, Freman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. On behalf of the Toronto Diabetic Neuropathy Expert Group. Diabetes Care (2010) 33:2285–93. doi:10.2337/dc10-1303
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
18. Spallone V, Ziegler D, Freeman R, Bernardi L, Frontoni S, Pop-Busui R, et al. On behalf of the Toronto Consensus Panel on Diabetic Neuropathy. Cardiovascular autonomic neuropathy in diabetes: clinical impact, assessment, diagnosis, and management. Diabetes Metab Res Rev (2011) 27:639–53. doi:10.1002/dmrr.1239
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Tannus LRM, Sperandei S, Junior RMM, Carvalho VR, Pedrosa HC, Félix MT, et al. Reproducibility of methods used for the assessment of autonomous nervous system’s function. Autonom Neurosci Basic Clin (2013) 177:275–9. doi:10.1016/j.autneu.2013.05.444
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
20. O’Brien IAD, O’Hare P, Corrall RJM. Heart rate variability in healthy subjects: effect of age and the derivation of normal ranges for testes of autonomic function. Br Heart J (1986) 55:348–54. doi:10.1136/hrt.55.4.348
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
21. Kowalewski MA, Urban M. Short and long term reproducibility of autonomic measures in supine and standing positions. Clin Sci (2004) 106:61–6. doi:10.1042/CS20030119
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
22. Lobnig BM, Maslowska-Wessel E, Bender R. Repeatability of heart rate variability measured via spectral analysis in healthy subjects. J Clin Basic Cardiol (2003) 6:29–33.
23. Gerritsen J, TenVoorde BJ, Dekker JM, Kingma R, Kostense PJ, Bouter LM, et al. Measures of cardiovascular autonomic nervous function: agreement, reproducibility, and reference values in the middle age and elderly subjects. Diabetologia (2003) 46:330–8. doi:10.1007/s00125-003-1032-9
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
24. Ziegler D, Laux G, Dannehi K, Spuler M, Mayer P, Gries FA. Assessment of Cardiovascular Autonomic Function: age related normal ranges and reproducibility of spectral analysis, vector analysis and standard tests of heart rate variation and blood pressure responses. Diabet Med (1992) 9:166–75. doi:10.1111/j.1464-5491.1992.tb01754.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
25. de Onis M, Habicht JP. Anthropometric reference data for international use: recommendations from a World Health Organization Expert Committee. Am J Clin Nutr (1996) 64(4):650–8.
26. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension (2003) 42(6):1206–52. doi:10.1161/01.HYP.0000107251.49515.c2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
27. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics (2004) 114(Suppl 2):555–76.
28. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem (1972) 14:492–9.
29. Leitão CB, Canani LH, Bolson PB, Molon MP, Silveiro SP, Gross JL. Que valores devem ser adotados para o diagnóstico de microalbuminúria no Diabete Melito? Arq Bras Endocrinol Metab (2006) 50:322–6. doi:10.1590/S0004-27302006000200018
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med (1999) 130(6):461–70.
31. Schwartz GJ, Muñoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, et al. New equations to estimate GFR in children with CKD. J Am Soc Nephrol (2009) 20(3):629–37. doi:10.1681/ASN.2008030287
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl (2013) 3:1–150.
33. Moreira RO, Castro AP, Papelbaum M, Appolinário JC, Ellinger VC, Coutinho WF, et al. Tradução para o Português e Avaliação da Confiabilidade de Uma Escala para Diagnóstico da Polineuropatia Distal Diabética. Arq Bras Endocrinol Metab (2005) 49:944–50. doi:10.1590/S0004-27302005000600014
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
34. Young MJ, Boulton AJM, Macleod AF, Williams DRR, Sonksen PH. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia (1993) 36:150–4. doi:10.1007/BF00400697
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
35. Boulton AJM, Vinik AI, Arezzo JC, Bril V, Feldman EL, Malik RA, et al. Diabetic neuropathies. A statement by the American Diabetes Association. Diabetes Care (2005) 28:956–62. doi:10.2337/diacare.28.4.956
36. Rolim LC, Souza JST, Dib SA. Tests for early diagnosis of cardiovascular autonomic neuropathy: critical analysis and relevance. Front Endocrinol (2013) 4:173. doi:10.3389/fendo.2013.00173
37. Thomas MC, MacIsaac RJ, Tsalamandris C, Molyneaux L, Goubina I, Fulcher G, et al. Anemia in Patients with Type 1 Diabetes. J Clin Endocrinol Metab (2004) 89:4359–63. doi:10.1210/jc.2004-0678
38. Bosman DR, Osborne CA, Marsden JT, Macdougall IC, Gardner WN, Watkins PJ. Erythropoietin response to hypoxia in patients with diabetic autonomic neuropathy and non-diabetic chronic renal failure. Diabet Med (2002) 19:65–9. doi:10.1046/j.1464-5491.2002.00634.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
39. Forsén A, Kangro M, Sterner G, Norrgren K, Thorsson O, Wollmer P, et al. A 14-year prospective study of autonomic nerve function in Type 1 diabetic patients: association with nephropathy. Diabet Med (2004) 21:852–8. doi:10.1111/j.1464-5491.2004.01255.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
40. Sundkvist G, Ljlia B. Autonomic neuropathy predicts deterioration in glomerular filtration rate in patients with IDDM. Diabetes Care (1993) 16:773–9. doi:10.2337/diacare.16.5.773
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
41. Lafferty AR, Werther GA, Clarke CF. Ambulatory blood pressure, microalbuminuria, and autonomic neuropathy in adolescents with type 1 diabetes. Diabetes Care (2000) 23:533–8. doi:10.2337/diacare.23.4.533
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
42. Thayer JF, Fischer JE. Heart rate variability, overnight urinary norepinephrine and C-reactive protein: evidence for the cholinergic anti-inflammatory pathway in healthy human adults. J Intern Med (2009) 265:439–47. doi:10.1111/j.1365-2796.2008.02023.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
43. Blake GJ, Rifai N, Buring JE, Ridker PM. Blood pressure, C-reactive protein, and risk of future cardiovascular events. Circulation (2003) 108:2993–9. doi:10.1161/01.CIR.0000104566.10178.AF
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: type 1 diabetes, cardiovascular risk, cardiovascular autonomic neuropathy, heart rate variability, chronic complications
Citation: Tannus LRM, Drummond KRG, Clemente ELdS, da Matta MdFB and Gomes MB (2014) Predictors of cardiovascular autonomic neuropathy in patients with type 1 diabetes. Front. Endocrinol. 5:191. doi: 10.3389/fendo.2014.00191
Received: 29 July 2014; Accepted: 18 October 2014;
Published online: 25 November 2014.
Edited by:
Tomris Erbas, Hacettepe University Medical School, TurkeyCopyright: © 2014 Tannus, Drummond, Clemente, da Matta and Gomes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucianne Righeti Monteiro Tannus, Diabetes Unit, Department of Medicine, State University Hospital of Rio de Janeiro (UERJ), Avenida 28 de Setembro, 77, 3rd floor, Vila Isabel, Rio de Janeiro 20551-030, Brazil e-mail: luciannetannus@ig.com.br