 Yu Takizawa
Yu Takizawa Matthew Bambling2
Matthew Bambling2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 07 June 2024
Sec. Educational Psychology
Volume 9 - 2024 | https://doi.org/10.3389/feduc.2024.1396271
Introduction: While mental health problems are prevalent among children, Japanese schools face challenges in providing effective mental health support to children partly due to a lack of training in mental health intervention. This study aimed to address this problem by evaluating a co-designed online teacher training program to provide a neuroscience-informed mental health intervention (NIMHI) to Japanese children.
Method: The present study evaluated the effectiveness of an online teacher training program by conducting a single-arm trial involving a group of 20 teachers and 245 children aged 8–12 from a regional Japanese primary school. The researcher delivered online training to Japanese teachers, who subsequently administered NIMHI to Japanese children over a 4-week period. The evaluation involved the administration of pre- and post-intervention student questionnaires, pre- and post-training teacher questionnaires, and post-intervention teacher interviews.
Results: After the delivery of the training program, 80% of Japanese teachers expressed strong or moderate satisfaction with the training. There were significant improvements in teachers' knowledge, perceived skills, self-efficacy, and acceptability of using NIMHI. Teachers implemented intervention strategies at least twice a week over four weeks. Following the intervention, 70% of teachers reported qualitative changes in students' mental health, such as more stable emotions. However, there were no significant changes in students' emotional problems, school enjoyment, and psychological wellbeing.
Discussion: The findings offer a fresh perspective on the effectiveness of utilizing digital technology, as a modality for delivering training to Japanese teachers. However, the absence of quantitative changes in students' mental health could suggest that the effectiveness of the online teacher-training program may not have been sufficiently robust. Further improvements in the online teacher-training program would be useful, such as providing tablet applications to assist teachers in implementing suitable intervention strategies and teaching a more focused range of strategies.
There is an urgent need for early mental health interventions for Japanese children, as mental disorders among Japanese children have increased dramatically, with diagnoses of various mental disorders rising from 117,000 to 329,000 between 1999 and 2020 (Ministry of Health, Labour, and Welfare, 2021). Japanese schools play a pivotal role in early mental health intervention for children, yet they face challenges. However, due to the limited government budget allocated, school counselors work < 4 h a week in 73.5% of Japanese primary schools, 30.1% of Japanese junior high schools, and 56.9% of Japanese senior high schools (Ministry of Health, Labour, and Welfare, 2021). In these circumstances, Japanese teachers are required to play a primary role in providing mental health support to students. However, the lack of training in mental health intervention for teachers contributes to their challenges in providing adequate care to students. Japanese universities commonly provide limited mental health intervention training to pre-service teachers (Yamaguchi et al., 2021). In-service teachers also have difficulties in gaining training in mental health intervention due to the lack of paid leave for professional development, family commitment, and the heavy workloads averaging 55 h per week (Deguchi et al., 2018).
Online training offers geographical flexibility, granting teachers easier access compared to face-to-face sessions (Sheperis et al., 2020). No study listed in the major databases, such as Psych info and PubMed, has evaluated the effectiveness of online training for teaching mental health intervention to teachers. However, studies comparing online and face-to-face training for other professionals, such as psychologists and counselors, suggests that online training is comparable in enhancing learners' knowledge, skills, and self-efficacy (Dimeff et al., 2009; Snow et al., 2018). Hence, a potential solution to address a lack of teacher training in mental health intervention among Japanese teachers may be to provide online training program. However, the direct conversion of current face-to-face teacher programs designed for mental health intervention for Japanese teachers into an online format may not be advisable.
Currently, two major types of professional development training exist for Japanese teachers regarding mental health interventions for children: mental health literacy training and standardized group mental health intervention programs (Harada and Watanabe, 2021; Yamaguchi et al., 2021). However, the mental health literary program has a lack of evidence to support effectiveness in improving children's mental health (Yamaguchi et al., 2020). Furthermore, standardized group-mental health intervention programs, such as group SST and group CBT, only have a small effect on improving emotional problem (Hedges's g = 0.22) and conduct problem (Hedges's g = 0.20) (Takizawa et al., 2023a). There is a need for a new type of online teacher training program designed specifically to effectively enhance the mental health of Japanese children.
While it is a new type of teacher training program, teacher training program for providing neuroscience-informed mental health intervention (NIMHI) may contribute to the effective promotion of Japanese children's mental health. Serving as a biopsychosocial framework, NIMHI utilizes insights from neuroscientific research to comprehend mental health and formulate targeted interventions (Grawe, 2017). While neuroscientific knowledge is fundamental in understanding mental health and formulating intervention strategies, NIMHI combines intervention strategies from various psychotherapy schools, such as CBT and mindfulness-based therapy, to address individuals' mental health (Beeson and Field, 2017). Different NIMHI models exist in the literature, such as neuroscience-informed CBT (N-CBT) (Field et al., 2015), neuropsychotherapy (Grawe, 2017), and trauma adaptive recovery group education and therapy (TARGET) (Ford, 2015). These models synthesize techniques and therapeutic components from CBT and other psychotherapy approaches, aiming to foster both bottom-up and top-down regulation for improving individuals' mental health.
Bottom-up regulation involves the control of lower brain areas, such as the amygdala and hypothalamus, which oversee the autonomic nervous system responsible for emotional and physiological arousal (Field et al., 2019). This control enhances command over higher brain regions, particularly the prefrontal cortex, aiding in restoring cognitive functions such as learning, memory, and executive functioning. Conversely, top-down regulation manages higher brain regions, like the prefrontal cortex, governing cognitive abilities to regulate lower brain regions, controlling emotional and physiological reactions (Grawe, 2017). There are a variety of strategies for promoting bottom-up regulation, such as lifestyle interventions (e.g., diet, hydration, sleep, physical activity, sun exposure, social interactions), diaphragm breathing, muscle relaxation, posture maintenance, imagery, emotional expression, nature exposure, and environmental regulation (Lohaus et al., 2010; Wang et al., 2022). Studies also found that cognitive restructuring and mindfulness techniques are effective for improving top-down regulation (Clark, 2013; Seminowicz et al., 2013). For instance, N-CBT (Field et al., 2015) integrates CBT techniques like meditation, diaphragm breathing, and cognitive restructuring, facilitating both bottom-up and top-down brain regulation. Neuropsychotherapy (Grawe, 2017) applies CBT techniques and emphasizes the positive therapeutic relationship's impact on clients' mental health, fostering regulation across both bottom-up and top-down brain pathways. TARGET employs guided practices from CBT, mindfulness therapy, experiential therapy, psychodynamic therapy, and art therapy to address trauma, promoting regulation across both bottom-up and top-down brain pathways (Ford, 2015).
At this stage, there is limited empirical research into NIMHI in terms of outcome and compared with other treatments, such as CBT (Takizawa et al., 2022). However, qualitative support exists for N-CBT's credibility and positive outcome expectation among psychotherapists who underwent training (Field et al., 2017, 2019). Neuropsychotherapy is backed by a series of case studies highlighting qualitative benefits in treating depression and anxiety disorders (Rossouw, 2014). These studies consistently advocate that neuroscientific information assists therapists in comprehending adults' conditions effectively, enabling tailored interventions to suit individual client circumstances. Moreover, clinical trials have indicated that TARGET is more effective in reducing anxiety symptoms among children and adults compared to relational supportive therapy and person-centered therapy (Ford et al., 2012, 2018).
While no researchers have specifically designed and evaluated teacher training programs for delivering NIMHI to children, international studies also suggest that neuroscience education can empower teachers to offer more effective mental health support to children (Dubinsky et al., 2019; Brick et al., 2021). For instance, Dubinsky et al. (2019) examined the effectiveness of neuroscience education for 296 primary and high school teachers in the United States. This education encompassed neuroscience topics including learning and memory, emotions and mirror neurons, the autonomic nervous system, and stress. Teacher interviews and classroom observations indicated increased teaching confidence, heightened social and emotional support for students, and improved quality of teacher-student communication following the training. In addition, emerging studies indicate that personalized interventions that tailor specific strategies to address specific individual problems, may be more effective in promoting children's mental health compared to standardized interventions (Ghaderi, 2006; Weisz et al., 2012).
In summary, these findings suggest that online teacher training program for delivering NIMHI may be particularly effective in promoting mental health of Japanese children if it specifically includes four components: (1) neuroscience education, (2) the cultivation of skills in implementing diverse emotional, physiological, and cognitive strategies for both bottom-up and top-down regulation, (3) administration of personalized mental health interventions, and (4) a focus on initially applying emotional and physiological regulation strategies to initiate bottom-up brain regulation, preceding the introduction of cognitive regulation strategies for top-down regulation. However, to date, no studies have been published evaluating such training.
To fill the research gap, the present study aimed to develop and evaluate an online teacher training program for Japanese teachers to deliver NIMHI to Japanese children. This study focused on designing and evaluating an online teacher training program targeted at Japanese primary school teachers for providing early mental health interventions to children. Specifically, the study sought to evaluate the co-designed online teacher training program. Co-design represents a collaborative and inclusive approach to intervention and training design, harnessing the collective creativity of developers and users. By engaging users as “experts of their experiences” (Marín et al., 2018), co-design fosters a deeper understanding of user needs, emotions, and aspirations, ultimately leading to the development of more effective and user-centered services. Involving teachers in the co-design of training programs can enhance their adoption of new intervention strategies, as teachers are more likely to adopt learning materials that align with their pedagogical goals, teaching methods, and student learning expectations (Champion et al., 2020). Expert feedback also ensures that the program's format and content suit the intervention's target audience (Skivington et al., 2021).
There were four hypotheses tested in this study:
1. Japanese teachers have high satisfaction with learning from online training.
2. Japanese teachers have higher knowledge, skills, self-efficacy and acceptability of using NIMHI after attending online training.
3. Japanese teachers actively implement NIMHI after attending online training.
4. Japanese children have better mental health after receiving the teacher-delivered NIMHI.
The present study employed a single-arm experimental design with one intervention group comprising Japanese primary school teachers who underwent an online teacher training program and subsequently delivered the NIMHI to a group of primary school students (Figure 1). The study utilized a mixed-method research approach, incorporating both quantitative and qualitative measures (pre- and post-intervention student questionnaire, pre- and post-training teacher questionnaires, and post-intervention teacher interviews) for the evaluation of online teacher training. To comprehensively evaluate online teacher training, the study assessed all four levels outlined in Kirkpatrick and Kirkpatrick's evaluation model (2006), which include learning satisfaction, learning experience, behavior change, and outcomes.

Figure 1. Flow of study.
The first author, who is a Japanese native speaker with a profound understanding of Japanese culture, designed online teacher training in the Japanese language. The first author created an online teacher training program for delivering NIMHI, comprising four key components: neuroscience education, skill-building in emotional, physiological, and cognitive regulation strategies, personalized mental health interventions for classroom settings, and a phased approach focusing on bottom-up regulation (emotional and physiological) before introducing top-down cognitive regulation strategies. Detailed process for the development of online teacher training program for providing NIMHI is reported in author's prior study (Takizawa et al., 2022).
The first author co-designed this training program by integrating feedback from Japanese primary school teachers collected in the author's needs-analysis study, incorporating feedback from a panel of six experts, and conducting a focus group with Japanese primary school teachers and incorporating their feedback (Takizawa et al., 2023b). This co-design process was undertaken to ensure that the designed training program and intervention meet the expectations of the target group of teachers and provide more engaging, satisfying, and valuable services. Integrating feedback from teachers and experts, the training program was designed to involve the completion of hardcopy self-paced learning materials, along with reading and exercises in 6–10 modules (each module taking 15–20 min to complete), followed by attendance at a brief live interactive online session (1–2 h) with follow-up support.
The hardcopy self-paced learning booklet was 90 pages in length, comprised seven chapters, and included exercises with case studies for the development of knowledge and skills in delivering NIMHI (Table 1). The author developed PowerPoint slides to accompany a 90-min live interactive session. The slides were designed to provide a summary of the key points covered in the booklet and to facilitate discussion and sharing of the results from the exercises contained in the booklet. Online teacher training program was designed to provide a checklist that teachers can use to determine factors that influence individual students in each classroom and provide personalized intervention to address those factors that particularly impact on students in the classroom. The training program was also designed to provide guideline for individual intervention for addressing different factors that influence students' mental health and worksheet that teachers can use in the classroom for delivering intervention.
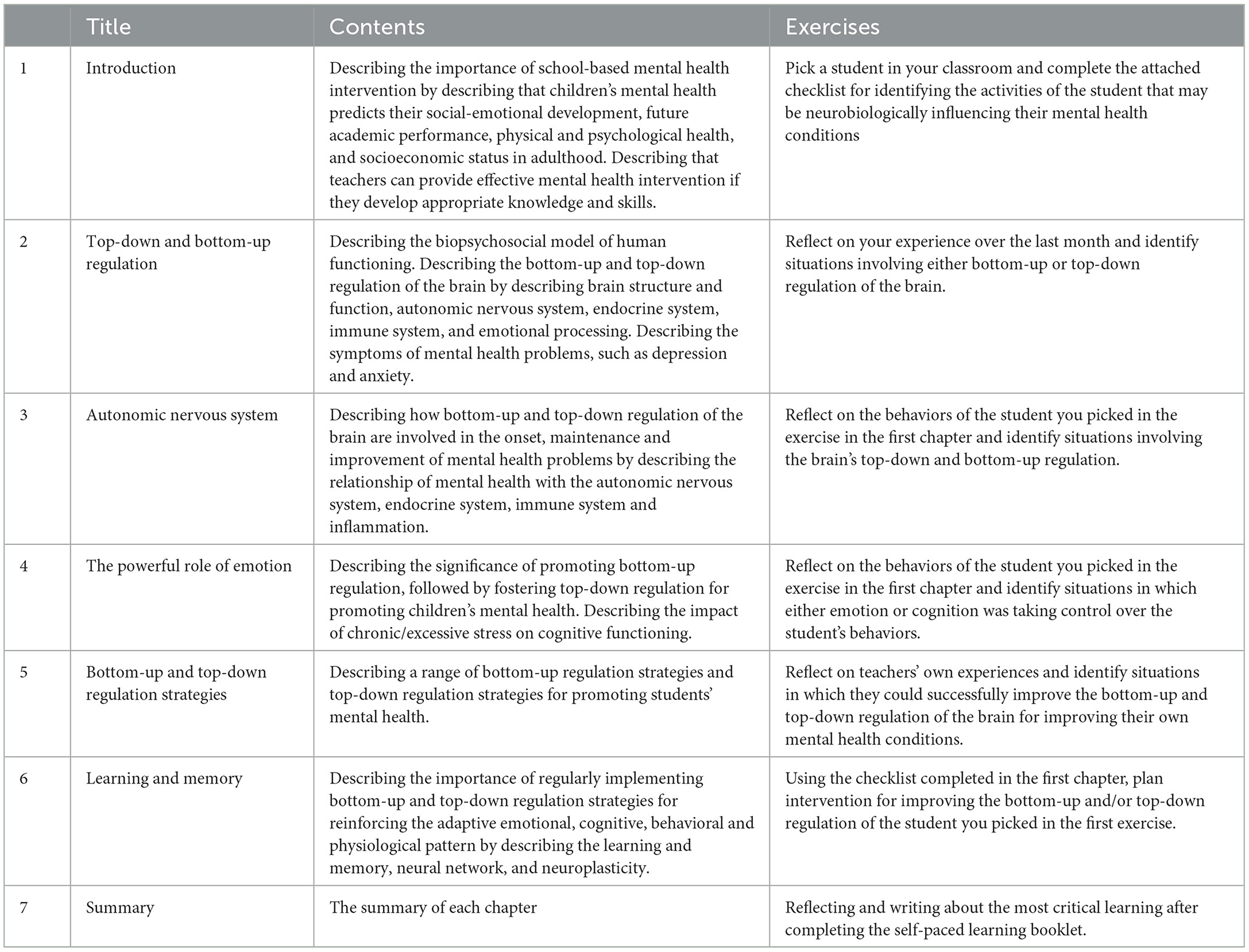
Table 1. Content of the self-paced learning booklet for online training.
The participants were 245 Japanese students (M = 133; F = 112) from Grade 3 to 6 aged 8–12 and 20 Japanese teachers (M = 11; F = 9) from a Japanese primary school in the Western Japanese region. Japanese students included 48 grade 3 students (M = 28; F = 30), 61 grade 4 students (M = 31; F = 30), 62 grade 5 students (M = 38; F = 24), and 67 grade 6 students (M = 38; F = 29). The teachers' age group ranged between their 20s and 50s, with 70% of them being in their 40s and 50s. Their teaching experience varied from 5 to 34 years (M = 18 years). Ten served as homeroom teachers for Grade 3–6, and the other 10 were assistant teachers for the same grade levels. The participants in this study represent typical primary school teachers and students in the regional areas of Japan.
After obtaining ethical approval from the University of Queensland Ethics Committees (Ethics Approval Number: 2022/HE000833), the researcher recruited students and teachers by contacting and describing the purposes of the study to the school principal of the primary school on the researcher's professional network. After obtaining approval from the school principal, the researcher described the purpose of the study to students, their parents and teachers with an information sheet and obtained informed consent from them for participation in the study. The students completed their questionnaires during regular classroom hours under the supervision of the homeroom teachers.
After developing the online teacher training, the researcher scheduled a date for the online teacher training for teachers in the primary school. Two weeks before the scheduled date of the online live interactive session, the researcher sent an online pre-training teacher questionnaire to teachers via email. The researcher also provided a hardcopy, self-paced learning booklet to Japanese teachers and requested that they complete it before attending the online live interactive session. The researcher conducted the online live interactive session with Japanese teachers on the scheduled date via Zoom. Immediately after the online live interactive session, the researcher requested that teachers complete the post-training questionnaires created on the Google form. The researcher also instructed teachers to implement the NIMHI they learned during the training. The researcher offered follow-up support to teachers through email and phone consultations, addressing questions and providing guidance on training content and intervention implementation.
After teachers delivered the NIMHI to students for 4 weeks, the researcher conducted post-intervention interviews with the school teachers who participated in the online training to evaluate the behavior change after the training. The interviews, which lasted between 20 and 25 min, were conducted via Zoom and were audio-recorded with the consent of the interviewees. The recordings were later transcribed for analysis. In addition to the online interviews, the researcher also emailed interview questions to teachers who were unable to attend the scheduled interviews, and obtained their responses via email.
After teachers delivered NIMHI to students for 4 weeks, the researcher instructed the teachers to administer the post-intervention student questionnaires during regular classroom hours. Same as the administration of pre-intervention student questionnaires, the homeroom teachers supervised the students while they completed the questionnaires. The completed post-intervention student questionnaires were collected by the researcher, who deidentified the data and entered it into a password-protected computer.
The post-training teacher questionnaire included a self-report measure of satisfaction with the online training program, consisting of three items measuring overall satisfaction with the training (I am satisfied with the overall learning experience from the training), the practical usefulness of the learning contents (The contents of the training were practical and valuable for providing mental health support to children), and the ease of understanding the learning contents (The contents of the training were easy to understand). A Likert-type scale ranging from 0 (strongly disagree) to 4 (strongly agree) was used for each item, and the total score for learning satisfaction was calculated. This measure was adopted from the teacher satisfaction questionnaire developed by Fisher et al. (2010). The total scores for knowledge, perceived skills, self-efficacy, and acceptability of NIMHI ranged from 0 to 10, 0 to 24, 0 to 20, and 0 to 16, respectively.
Pre-and post-training teacher questionnaires included 15-item multiple-choice questions (MCQs) to assess the knowledge gained from the training in NIMHI. For instance, one of the MCQs presented a statement: “Improving bottom-up regulation involves enhancing cognition to positively impact emotional, behavioral, and physiological states”. Participants were asked to select a response from options including “(A) the above explanation is correct,” “(B) the above explanation is incorrect,” “(C) it has not yet been clarified by neuroscience research,” and “(D) not sure”. The MCQs were developed for the present study, with reference to previous studies that used the MCQs to measure knowledge gained from training (Breckwoldt et al., 2014; Wei et al., 2016). To ensure the MCQs' suitability for Japanese teachers, the researcher checked and confirmed the ease of understanding and level of difficulty with five Japanese teachers in the researcher's professional network who did not participate in the study.
The pre-and post-training teacher questionnaires included self-report measures with a Likert-type scale (0 = strongly disagree; 4 = strongly agree) for evaluating teachers' perceived skills, self-efficacy, and acceptability in delivering NIMHI to children. The measure for perceived skills had six items (e.g., I have skills in using neuroscientific knowledge to plan interventions for children). The measures for self-efficacy (e.g., I feel confident in using neuroscientific knowledge to understand the mental health problems of children) and the acceptability of delivering NIMHI (e.g., I agree that using neuroscientific knowledge helps provide mental health intervention) had five items each. These measures were originally designed for the present study in reference to the measures employed in the previous studies that evaluated training programs (Bennett-Levy et al., 2012; Weiner et al., 2017).
The semi-structured teacher interviews inquired about (1) the details of how school teachers implemented NIMHI after the training, including the frequency and types of intervention implemented, (2) perceived changes in students' mental health after delivering NIMHI, and (3) perceived benefits of the components of neuroscience-informed menta health intervention (neuroscientific knowledge, bottom-up regulation strategies, top-down regulation strategies, and assessment checklist) for promoting students' mental health. Additionally, the interviews explored barriers to implementing NIMHI within the Japanese educational setting and gathered suggestions for further improving the online teacher training program.
The student questionnaire incorporated the Stirling Children's Wellbeing Scale (SCWBS) (Liddle and Carter, 2015), the school enjoyment scale (Furuichi and Tamaki, 1994), and emotional problem subscale of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997).
The SCWBS (Liddle and Carter, 2015) is a self-report measure of subjective wellbeing among children aged 8–12. This scale consists of 15 items that are divided into two dimensions: the first, Positive Emotional State, consists of six items measuring hedonic wellbeing (e.g., I've been feeling calm); the second, Positive Outlook, consists of six items measuring eudaimonic wellbeing (e.g., I think there are many things that I can be proud of); and the remaining three items indicate the existence of social desirability. Each item is rated on a 5-point Likert-type scale (1 = never; 5 = always). Nishida et al. (2021) translated and tested the SCWBS with a group of Japanese children aged 8–12 and found reasonable validity and reliability of the measure with Japanese children. The scores on SCWBS ranged between 12 and 60 and a higher score indicates higher subjective wellbeing. In this study, three items for measuring social desirability were not used because previous studies identified that a high score on social desirability does not mean that the scoring on hedonic and eudaimonic wellbeing is invalid (Nishida et al., 2021).
The School Enjoyment Scale (Furuichi and Tamaki, 1994) is a 10-item self-report measure of school enjoyment. School enjoyment is the cognitive appraisal of children's quality of life at school and is an important marker of children's wellbeing at school (Baker et al., 2003). Each item of the scale presents a statement that describes enjoyment or motivation for going to school (e.g., “I enjoy going to school”) and the likeability of school (e.g., “I like this school”). For each item, children were asked to answer on a five-point Likert scale (1 = “does not apply” to 5 = “applies”). Studies reported this scale's reasonable internal reliability and convergent validity for Japanese children (Furuichi and Tamaki, 1994). The total scores ranged between 10–50 and a higher score indicates higher school satisfaction.
The SDQ (Goodman, 1997) is a 25-item measure rated on a 3-point Likert scale that screens the emotions and behaviors of children. The SDQ consists of five subscales containing five items: emotional problems (e.g., I worry a lot), conduct problems (e.g., I get very angry), inattention/hyperactivity (e.g., I am restless), peer problems (e.g., I am usually on my own), and prosocial behaviors (e.g., I try to be nice to other people). The SDQ has three different versions rated by oneself, parents, and teachers. Japanese research (Noda et al., 2013) revealed that the Japanese self-report version of SDQ had reasonable validity and reliability with Japanese children and adolescents. This study specifically included the emotional problem subscale of the self-report SDQ that has five items with a three-point Likert scale (0 = “does not apply” to 2 = “applies”) designed to measure the level of anxiety and depression symptoms for evaluating the level of emotional problems among children. The emotional problem subscale score ranges between 0–10, with 0–3 representing a low score range, 4 a mid-score, and 5–10 representing a high score range. A score in the high range indicates that students are likely to have clinically significant emotional problems.
To assess hypothesis 1, the researcher calculated the proportion of teachers who had either strong or moderate satisfaction with the online teacher training program. To assess hypothesis 2, this study conducted a one-way repeated-measures multivariate analysis of variance (MANOVA) to statistically test the significance of changes in scores in knowledge, perceived skills, self-efficacy, and acceptability for delivering NIMHI. The independent variable was time with two levels: pre-training and post-training. Dependent variables were knowledge, perceived skills, self-efficacy, and acceptability of using NIMHI measured at pre-training and post-training. The final sample size of teachers was 20. The minimum sample size required for performing a one-way repeated measure MANOVA is greater than the number of dependent variables, which is four in the present study. Hence, it was possible to perform a one-way repeated measure MANOVA with this sample size. A power analysis using G-power software (Faul et al., 2007) indicated that the sample size of 20 teachers was sufficient to achieve the required power for conducting a one-way repeated measure MANOVA.
To assess hypothesis 3, the researcher analyzed the interview data from teachers, identifying the frequency, type, and number of bottom-up and top-down regulation intervention strategies delivered by teachers. To assess hypothesis 4, this study conducted a thematic analysis to analyse the qualitative data collected from the teacher interviews (Braun and Clarke, 2006). The thematic analysis involved a systematic process of data familiarization, data coding, and theme development and revision, which facilitated a rigorous data interrogation and engagement (Braun and Clarke, 2019). The researcher familiarized themselves with the entire interview data, coded the data, and identified a set of potential themes for each interview topic by sorting different codes and collating all relevant coded data extracts within the identified themes. Thematic maps were created for each topic and revised for sorting codes into themes. The researcher then read the collated extracts for each theme, analyzed a coherent pattern, and verified the validity of individual themes to reflect the meanings evident in the dataset. Finally, the researcher defined and named each set of candidate themes. The co-authors verified the appropriateness of the identified themes. Any disagreements in themes were discussed and revised until consensus was achieved.
To assess hypothesis 4, this study performed a one-way repeated measures MANOVA to test the significance of changes in scores for subjective wellbeing, school enjoyment, and emotional problems between pre- and post-intervention. The independent variable was time, with two levels: pre-intervention and post-intervention. The dependent variables were subjective wellbeing, school enjoyment, and emotional problems. A total of 224 participants responded to both pre- and post-intervention student questionnaires. A power analysis using G-power software (Faul et al., 2007) indicated that the sample size of 224 students was sufficient to achieve the required power for conducting a one-way repeated measure MANOVA.
All teachers (n = 20) completed both the pre- and post-training questionnaires and participated in post-training interviews. Five teachers completed the interviews online, while 15 teachers responded to interview questions via email. The percentage of missing responses for each measure was < 5% for the pre- and post-training questionnaires. Similarly, 224 students from grades 3–6 (91.4% of total participants) completed the pre-intervention student questionnaires, while 235 students from grades 3–6 (98.7% of full participants) completed the post-intervention questionnaires. The percentage of missing responses for each measure was also < 5%. Data screening revealed no systematic pattern for missing responses on the items of each measure. Hence, to minimize the loss of data, pairwise deletion was employed for handling missing data.
The results supported hypothesis 1 that Japanese teachers have high satisfaction with learning from online training. Ninety per cent of teachers strongly agreed or agreed that the overall learning experience of the online training was satisfying, 80% of teachers strongly agreed or agreed that the contents of the online training were practical, and 75% of teachers strongly agreed or agreed that the contents of the online training were easy to understand (Table 2).
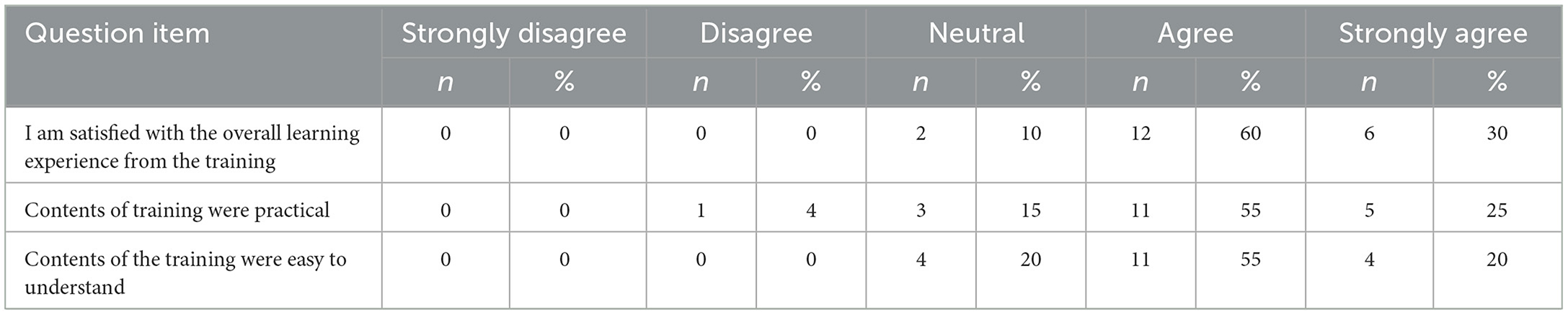
Table 2. Satisfaction and perception of practicality and ease of understanding of training.
The results supported hypothesis 2: Japanese teachers have higher knowledge, skills, self-efficacy, and acceptability of using NIMHI after online training. The dataset met assumptions for performing one-way repeated measure MANOVA (Table 3). The skewness and kurtosis for the distribution of each dependent variable were respectively between +1 and−1 and between +2 and −2 (George and Mallery, 2010). There were no extremely high correlations between each dependent variable (r < 0.90), which supported the assumption of no multicollinearity (Table 4). The results of Levene's test were not significant for all dependent variables, supporting the assumption of homogeneity of variances for each dependent variable. Internal reliability of measures at pre-and post-training was all acceptable (α = 0.61–0.84).
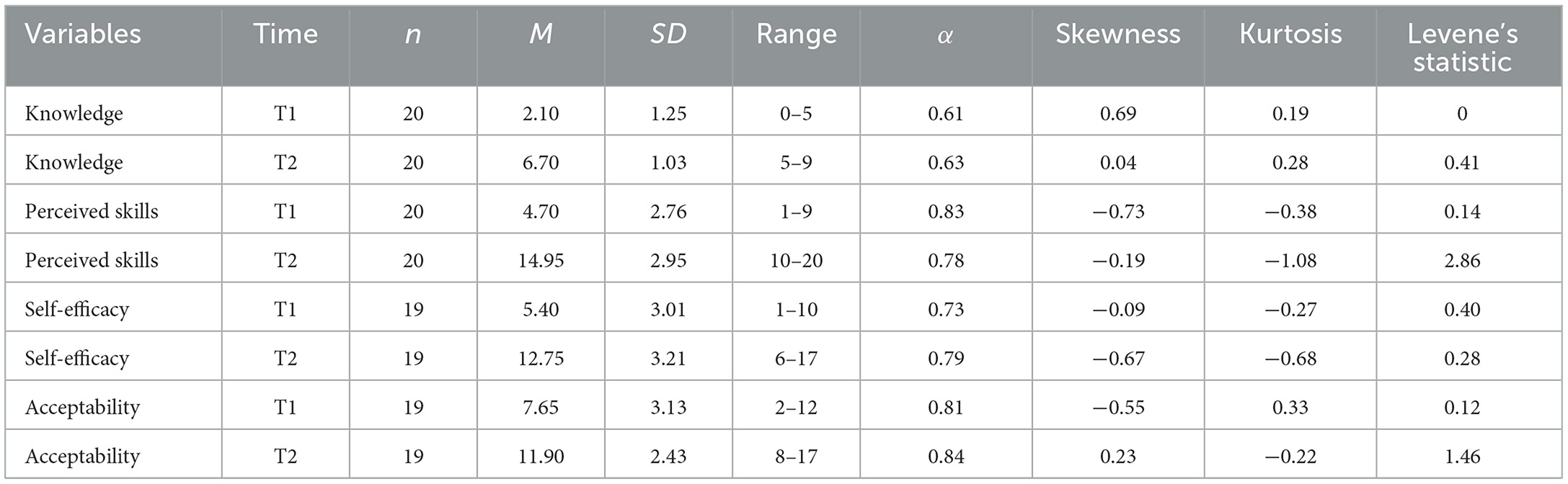
Table 3. Teachers' knowledge, perceived skills, self-efficacy and acceptability of using neuroscience-informed mental health intervention at pre-and post-training.
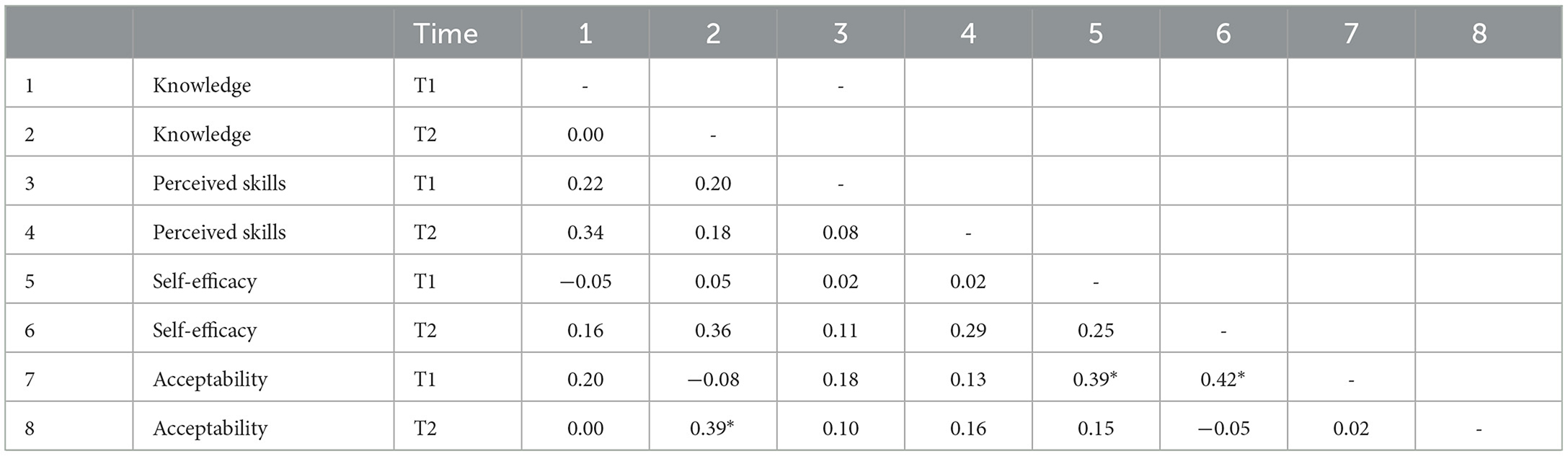
Table 4. Relationship between knowledge, perceived skills, self-efficacy and acceptability of using neuroscience-informed mental health intervention at pre-and post-training.
A repeated measure MANOVA revealed a large main effect of time, Wilk's Lambda = 0.016 [F(4, 14) =221.03, p < 0.01, η2 =0.95]. There was a large main effect of time for knowledge [F(1, 19) =147.91, p < 0.01, Cohen's F = 0.89], skills [F (1, 19) = 161.32, p < 0.01, η2 = 0.86], self-efficacy [F(1, 18) =118.84, p < 0.01, Cohen's F = 0.89] and acceptability of using NIMHI [F(1, 18) =24.97, p < 0.01, Cohen's F = 0.57]. These results indicated that there was a significant improvement in teachers' knowledge, perceived skills, self-efficacy, and acceptability of using NIMHI after attending the online training.
The results supported hypothesis 3: Japanese teachers actively implement NIMHI after attending online training. All teachers reported using the student checklist provided in the training program to assess students' bottom-up and top-down regulation activities and understand their needs in the first week following the online teacher training. The frequency of teachers' interventions is summarized in Table 5. All Japanese teachers implemented bottom-up and/or top-down regulation strategies for students in the classroom at least twice a week using the provided intervention sheets 4 weeks after attending the training (Table 6). In addition, 85% of Japanese teachers implemented one or more bottom-up and top-down regulation strategies at least three times a week. All teachers implemented at least five types of bottom-up and top-down regulation strategies 4 weeks after attending the training. Ninety percent (90%) of teachers implemented six or more types of bottom-up and top-down regulation strategies 4 weeks after attending the training. Tables 7, 8 presents the bottom-up and top-down regulation strategies implemented by teachers.
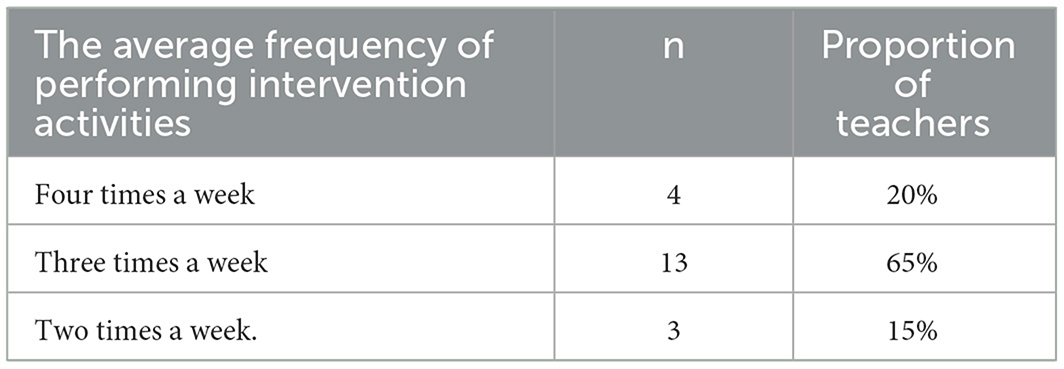
Table 5. Average frequency of teachers' intervention activities.
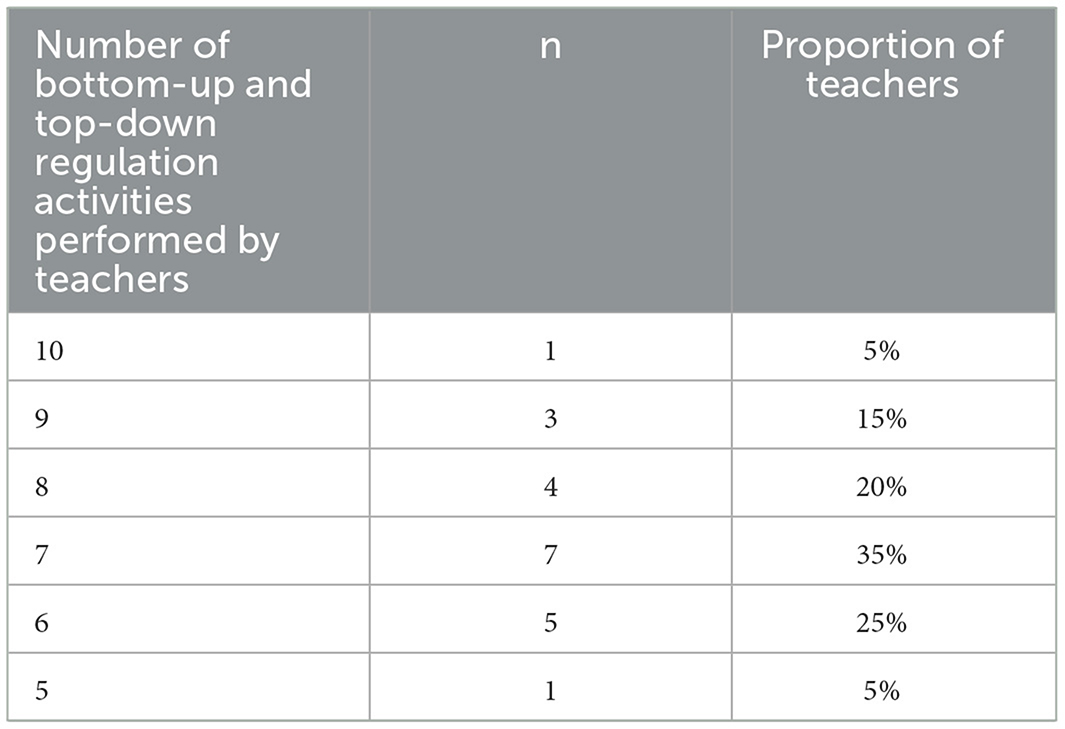
Table 6. Number of bottom-up and top-down regulation activities performed by teachers.
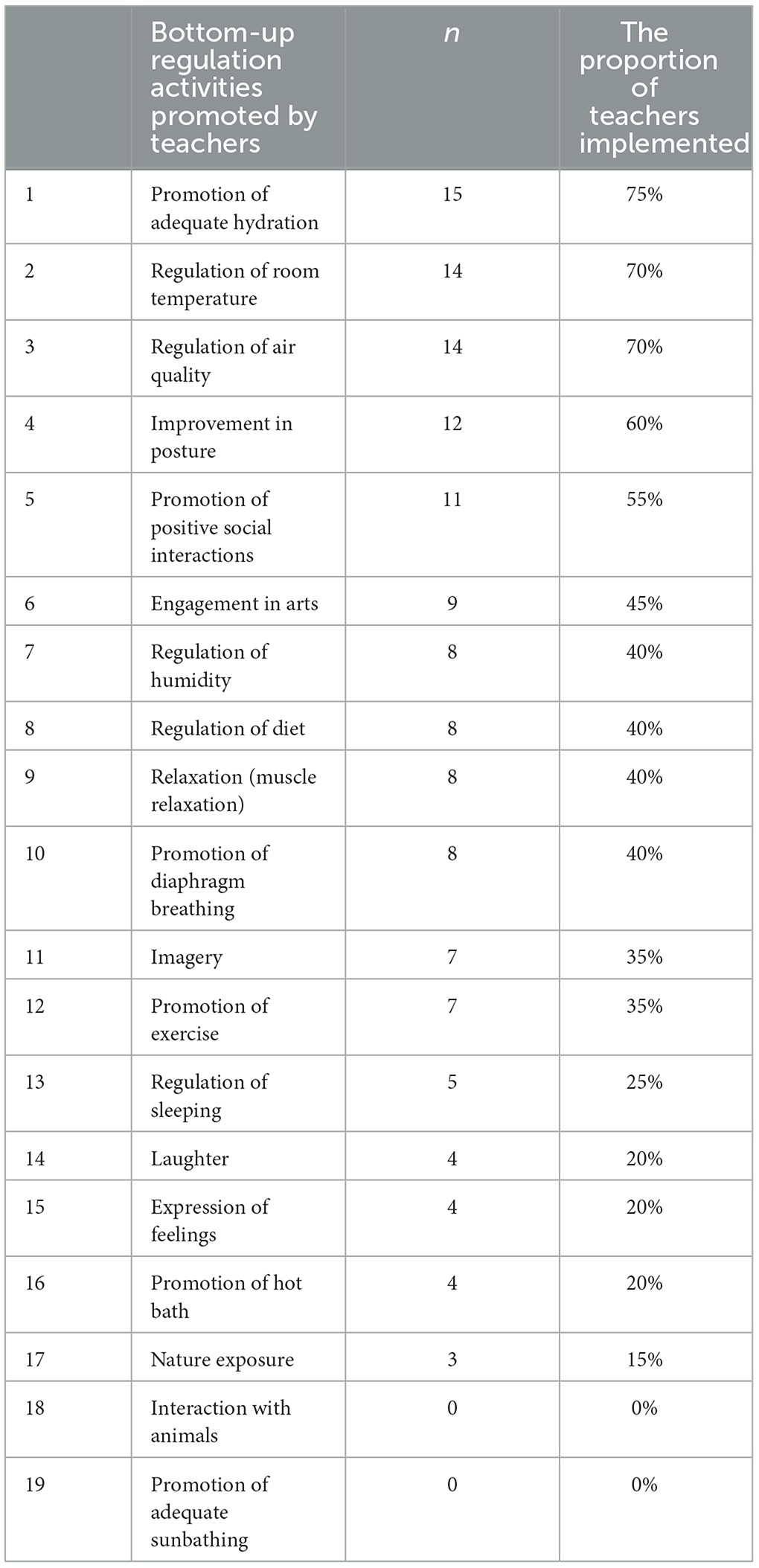
Table 7. Types of bottom-up regulation activities performed by teachers.
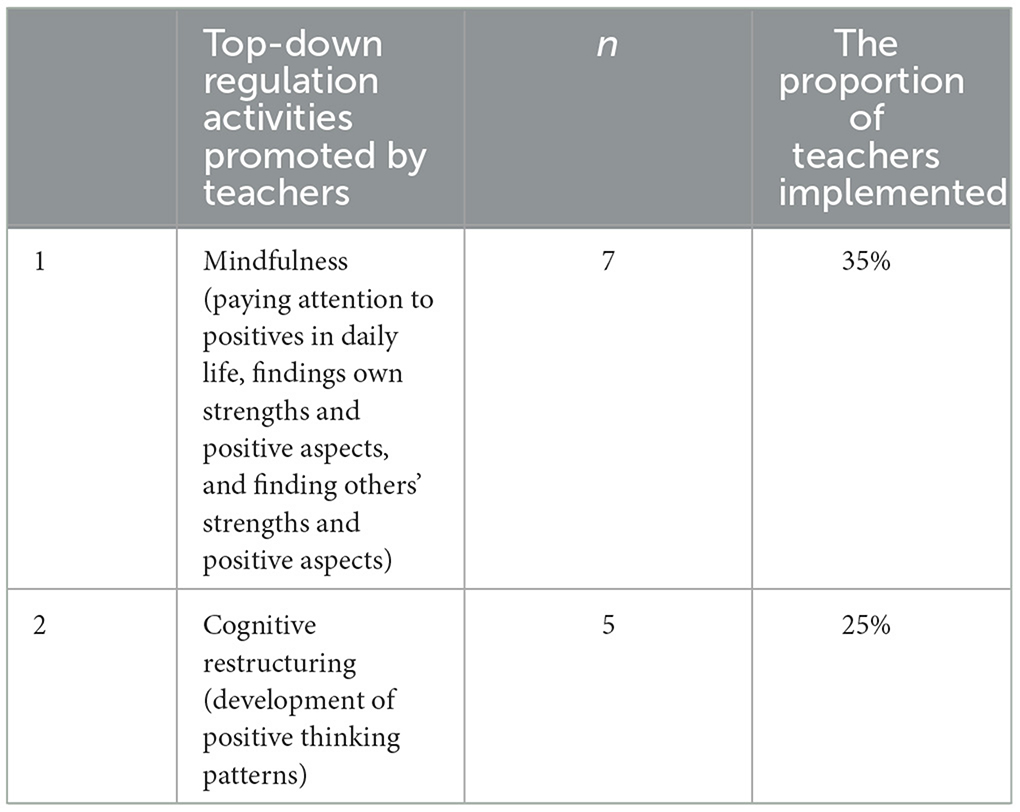
Table 8. Types of top-down regulation activities performed by teachers.
There were mixed findings regarding the hypothesis 4: Japanese children have better mental health after receiving the teacher-delivered neuroscience-informed mental intervention. The dataset met all assumptions for performing a one-way repeated measure MANOVA (Table 9). The skewness and kurtosis for the distribution of each dependent variable were respectively between +1 and −1 and between +2 and −2 (George and Mallery, 2010). There were moderate correlations between each dependent variable (r < 0.90) (Table 10), which supports the assumption of no multicollinearity. Levene's test was not significant for all dependent variables that support the assumption of homogeneity of variances for each dependent variable.
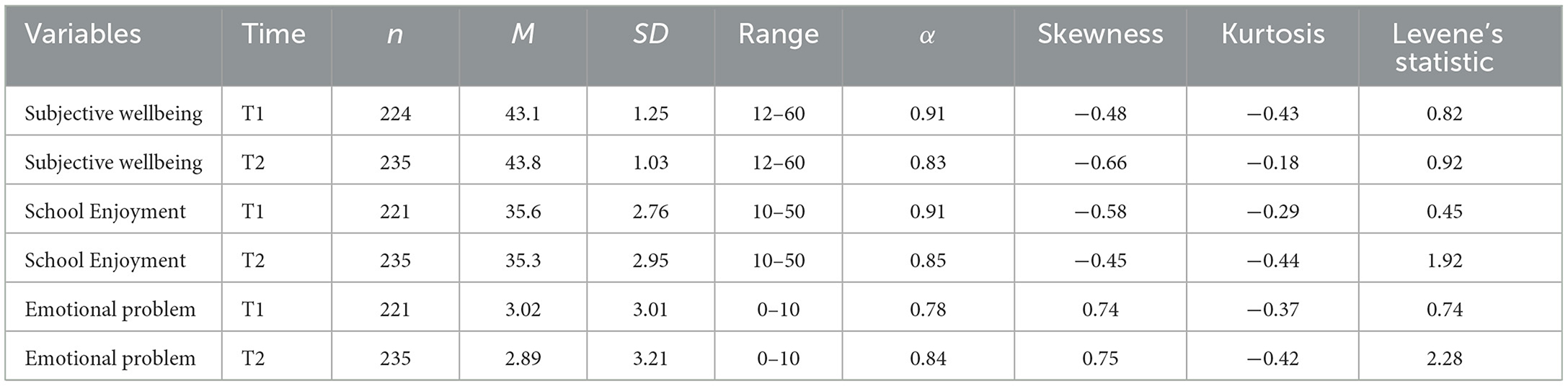
Table 9. A summary of subjective wellbeing, school enjoyment, and emotional problems among primary school students at T1 and T2.
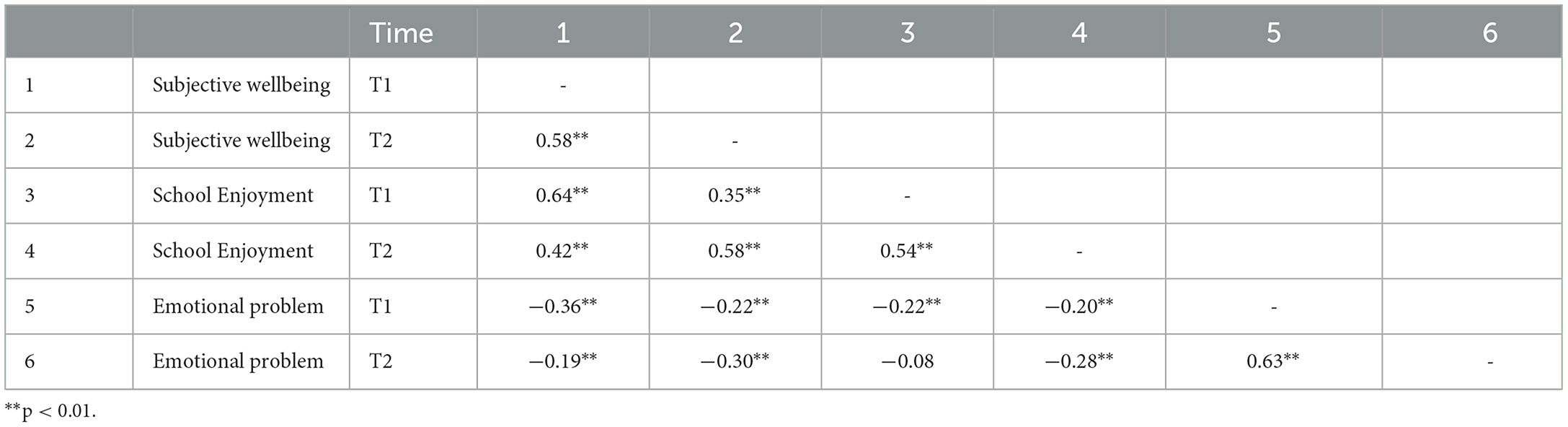
Table 10. The relationships between subjective wellbeing, emotional problem, and school enjoyment among Japanese primary school students.
The results of a repeated measure MANOVA revealed no significant effect of time (Wilk's Lambda=0.995, F (3,194) =0.35, ns, 01), indicating no difference in students' subjective wellbeing, emotional problems and school enjoyment between pre-and post-intervention. In addition, there was no interaction between time and gender [Wilk's Lambda = 0.988, F(3, 194) =0.81, ns], no interaction between time and grade level [Wilk's Lambda = 0.941, F(9, 472) =0.1.32, ns], and no interaction between time, gender and grade level [Wilk's Lambda = 0.926, F(9, 472) =0.1.68, ns]. These results indicated that, regardless of students' gender and grade level, there was no difference in students' subjective wellbeing, emotional problems, and school enjoyment between pre- and post-intervention.
Contrary to the quantitative analysis of student questionnaires, the qualitative analysis of post-intervention teacher interviews supported hypothesis 4: Japanese children have better mental health after receiving teacher-delivered neuroscience-informed mental intervention. Fourteen teachers (70% of teachers) reported that they found some improvement in students' mental health (Table 11). Nine teachers (45% of teachers) reported improvement in students' emotional problems, such as more stable emotions, being less anxious and depressed. Seven teachers (35%) reported positive changes in students' subjective wellbeing, such as presenting more positive moods and emotions after delivering the intervention. Five teachers (25%) reported noticing changes in students' behaviors, such as being less reactive, having better abilities to concentrate in the classroom, and less argument in the classroom.
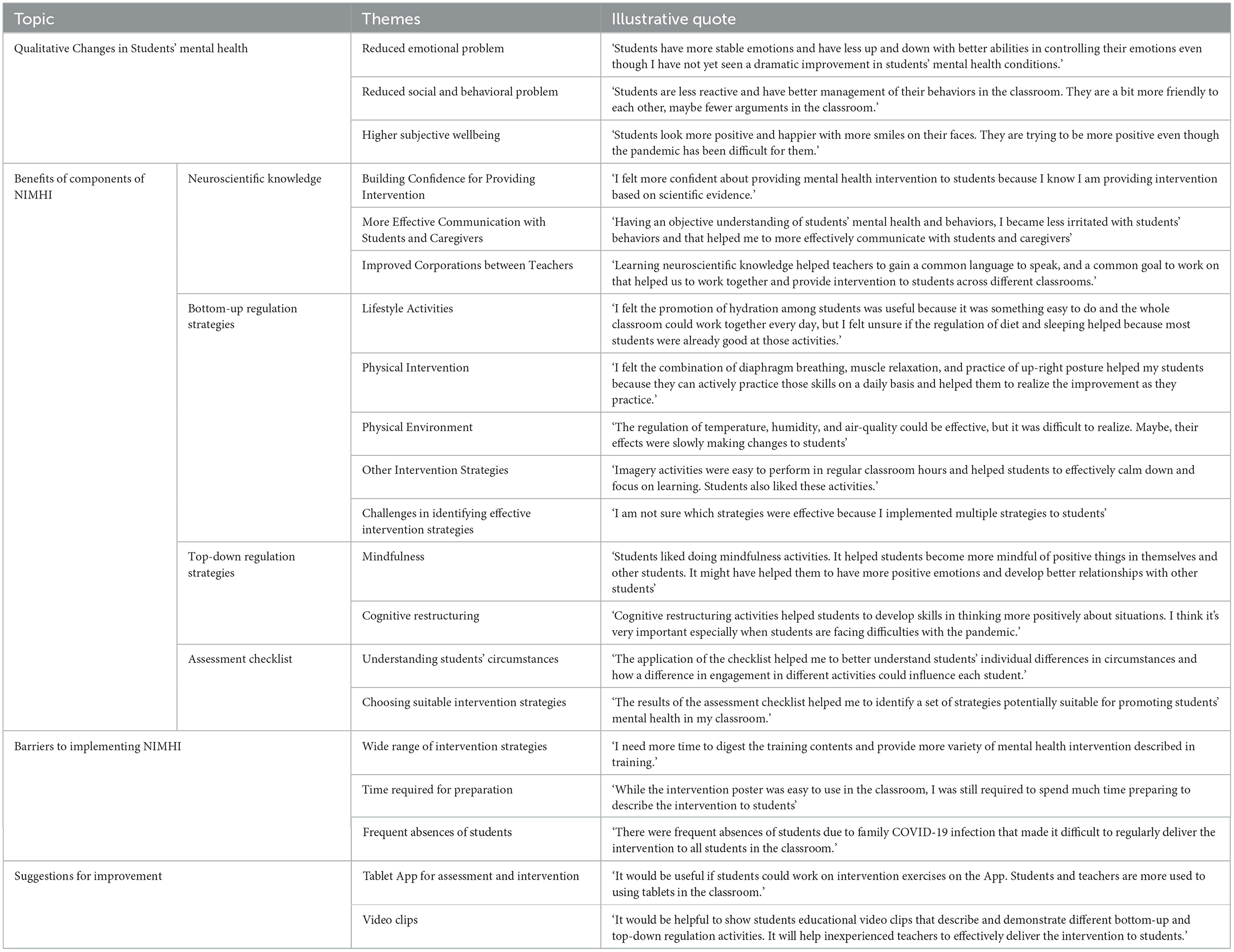
Table 11. Teachers' perceived benefits and challenges of using neuroscience-informed mental health intervention.
The analysis of post-intervention interviews found that 16 teachers (80%) reported the benefits of learning neuroscientific knowledge, including improvement in confidence for providing mental health support to students (n = 16; 80%), improvement in communication with students and caregivers regarding mental health problems (n = 10; 50%), and improvement in collaboration with other teachers for providing mental health support (n = 8; 40%).
Fourteen teachers (70%) reported the benefits of different bottom-up regulation strategies, including promotion of adequate hydration (n = 12; 60%), physical intervention, such as maintaining an upright posture, practicing muscle relaxation, and promoting diaphragmatic breathing (n = 10; 50%), and imagery (n = 5; 25%). Nevertheless, teachers reported that some bottom-up regulation strategies were not helpful, including lifestyle interventions besides promotion of hydration, such as diet, sleep, exercise, and hot baths (n = 10; 50%), and other bottom-up regulation strategies, such as laughter and nature exposure (n = 5; 25%).
Out of the 20 teachers, seven teachers (35%) incorporated either mindfulness and/or cognitive restructuring activities into their practice. Six teachers (30%) specifically reported that top-down regulation strategies were beneficial for promoting students' mental health. Three teachers (15%) highlighted the effectiveness of cognitive restructuring activities in promoting students' mental health.
All 20 teachers utilized an assessment checklist as part of their intervention process. The majority of teachers, 17 out of 20 (85%), reported that the learning and implementation of the assessment checklist proved to be beneficial for gaining a comprehensive understanding of their students' needs (n = 15; 75%) and selecting and implementing suitable bottom-up and top-down regulation interventions for their students (n = 14; 70%).
Six teachers (30%) reported needing more time and assistance to effectively deliver NIMHI because it involves a wide range of intervention strategies. In particular, teachers reported difficulties in delivering top-down regulation activities, such as cognitive restructuring, because they were not familiar with them and that they required more assistance and time for effectively delivering these interventions. Five teachers (25%) reported that they had limited time to provide the intervention to students. Five teachers (25%) reported difficulty delivering the regular intervention to all students in the classroom due to frequent absences of students under the COVID-19 pandemic.
Five teachers (25%) reported that it was more useful if they could use the application on students' tablet computers to identify students' mental health needs and deliver interventions to students. Teachers explained that, while many teachers initially experienced difficulties integrating ICT into teaching in the classroom, they gradually became used to using different types of ICT by using a computer, projector and student tablet computer.
Three teachers (15%) reported that to reduce teachers' time and energy required for providing intervention, it would be helpful if teachers could show a video clip that describes and demonstrates each intervention strategy to students via an App on the tablet computer.
The present study sought to evaluate a co-designed online teacher training program for Japanese teachers to deliver NIMHI to children. To achieve this objective, the present study addressed four hypotheses: (1) Japanese teachers have high satisfaction with learning from online training; (2) Japanese teachers have higher knowledge, skills, self-efficacy, and acceptability of using NIMHI after attending online training; (3) Japanese teachers actively implement NIMHI after attending online training; (4) Japanese children have better mental health after receiving the teacher-delivered NIMHI.
This study supports hypotheses 1, 2, and 3, demonstrating the success of a co-designed online teacher-training program in engaging and stimulating Japanese teachers. The program created an environment conducive to effective learning and implementation of NIMHI. Furthermore, it effectively promoted teachers' learning, enabling them to deliver interventions. Additionally, the program successfully promoted behavioral change among teachers, facilitating the adoption of NIMHI in the classroom. These findings offer a fresh perspective on the effectiveness of utilizing digital technology, specifically online interactive learning coupled with self-paced learning booklets, as an effective modality for delivering training to Japanese teachers. These insights align with international studies (Bragg et al., 2021) that emphasize the efficacy of online modalities in teacher-training programs. The present study's findings contribute a novel perspective, suggesting that co-design is a promising approach in developing online teacher-training programs that achieve satisfaction, foster learning, and produce behavioral changes among teachers. This aligns with international studies (Kelly et al., 2019; Ey and Spears, 2020) that demonstrate the effectiveness of co-design in designing engaging, satisfying, and valuable teacher-training programs. However, the study found mixed support for hypothesis 4, and therefore did not definitively support the effectiveness of online teacher training in promoting Japanese children's mental health due to mixed findings on its impact.
The findings suggest that the online teacher-training program aimed at delivering NIMHI to Japanese children may have had a limited impact on fostering positive changes in students' mental health. The discrepancy observed between the effectiveness of the online teacher-training program in promoting children's mental health, as indicated by statistical analysis, and the qualitative reports from teachers, can be partially attributed to expectation bias. This bias arises when individuals' preconceived notions about the effectiveness of an intervention shape their perceptions of the outcomes (De Boer et al., 2010). The majority of Japanese teachers displayed a moderate to strong interest in learning about NIMHI. Consequently, Japanese teachers may have been more inclined to report improvements in children's mental health resulting from the implementation of NIMHI, possibly more so than the objectively measured improvements. The absence of quantitative support for the effectiveness of online teacher training suggests that the program's effectiveness may be negligible.
The present study found that the effectiveness of NIMHI could be impeded by the barriers reported by teachers when implementing NIMHI. These barriers include a lack of time and support for effectively delivering a wide range of bottom-up and top-down regulation strategies, limited time for teachers to prepare for providing intervention, and frequent student absences due to COVID-19 infections. Some teachers reported difficulties in delivering top-down regulation strategies, such as cognitive restructuring, because they were not familiar and that they required more assistance and time to effectively provide these interventions. The duration of many school-based mental health intervention programs found effective in promoting mental health among children was 8 weeks or longer (Takizawa et al., 2023b). Therefore, the intervention duration in the present study may be insufficient to produce statistically significant changes in children's mental health. Furthermore, in the present study, follow-up support during the 4 weeks of interventions was only provided to teachers who actively contacted the researcher, and not all teachers received equal support. Providing regular catch-up sessions where all teachers can participate and supporting the implementation of interventions could be useful in improving the effectiveness of the interventions provided to students. Previous studies that have offered teacher training in implementing top-down regulation strategies, such as cognitive restructuring with children did not specifically report encountering such challenges (Matsumoto and Shimizu, 2016; Yamamoto et al., 2017). Therefore, it is possible that the quality of instruction and support provided to teachers for implementing top-down regulation strategies were insufficient in the present study.
Japanese teachers provided suggestions on how to overcome some of the barriers to the effective administration of intervention. They suggested that using a tablet application with video clips for delivering checklist assessments and intervention with different bottom-up and top-down regulation strategies could effectively remove these barriers, especially as Japanese teachers have become more familiar with such applications for academic teaching in the classroom since the start of the COVID-19 pandemic. Additionally, teachers recommended using an App on students' tablet computers to make it easier to deliver checklist assessments and interventions, saving time and energy for preparation. They also suggested that presenting video clips, for example, via a tablet App for delivering the intervention, could improve fidelity in implementing different types of bottom-up and top-down regulation strategies, as some intervention strategies, such as meditation and the development of a positive thinking pattern, are complex for teachers to deliver without adequate training. Although research on the effectiveness of using digital technology for promoting the mental health of Japanese children is still limited, there is a growing body of international evidence suggesting that integrating digital technology into mental health interventions can be effective in promoting mental health among children (Donker et al., 2013; Hollis et al., 2017). Hence, if the online teacher-training program provided a tablet App with video clips that they could use for delivering NIMHI, it could be more effective in improving the mental health of Japanese children.
The effectiveness of the online teacher-training program could also be impeded by the range of intervention strategies taught by the program. The majority of teachers who used top-down cognitive regulation strategies reported them to be effective in promoting students' mental health. However, only 35% of teachers implemented top-down cognitive regulation strategies. Additionally, certain bottom-up regulation strategies, such as physical interventions, promoting hydration, and utilizing imagery were found to be useful by the teachers. However, some physical intervention strategies, such as muscle relaxation and promotion of exercise, and imagery were used by 40% or less of teachers even though teachers reported these intervention strategies to be particularly effective. Furthermore, teachers did not report the benefits of regulating the physical environment, other lifestyle activities (diet, sleep, physical activity, sunlight exposure, and hot baths), and other bottom-up regulation strategies (nature exposure, engagement in arts, promotion of social interactions, and expression of feelings) in improving students' mental health. Therefore, the teacher-training program could be more effective in promoting students' mental health if it focused on a narrower range of bottom-up regulation strategies, limited to those reported by Japanese teachers to be useful, such as physical interventions, hydration regulation, and imagery activities. This, in addition to providing neuroscience education, teaching the assessment checklist, and offering top-down regulation strategies, could further support teachers in their efforts to promote students' mental health.
In summary, the findings of the current study suggest that the co-designed online teacher-training program for providing NIMHI to Japanese children may not have demonstrated sufficient effectiveness in enhancing the mental health of Japanese children. To enhance the efficacy of online teacher-training programs, several strategies can be considered. These include the provision of a tablet application for streamlined assessment and intervention delivery, enabling teachers to more effectively administer NIHMI to children. Additionally, emphasizing the teaching of focused intervention strategies, which teachers have reported as particularly valuable, could be considered for improvement.
The participants were teachers and students from a public primary school located in a regional city in western Japan. Thus, the generalisability of the results to the broader population in Japan may be limited. The scope of the assessment of students' mental health was restricted in this study. Furthermore, there exists a gap in studies supporting the validity of the Japanese version of the self-report SDQ for 8-year-olds, whereas previous research has substantiated the validity of the English self-report SDQ for children aged 8 to 17 and the Japanese self-report version for children aged 9 to 17 (Muris et al., 2004; Noda et al., 2013). Hence, the application of the Japanese self-report SDQ could have limited validity with 8-year-old Japanese children in the present study. There was a lack of control group that could reduce the accuracy of evaluation. Although the co-researchers evaluated the suitability of the identified themes, the primary author exclusively conducted the thematic analysis of the teacher focus group without independent parallel analysis by other researchers. Consequently, the qualitative basis supporting the effectiveness of the online teacher-training program in enhancing Japanese children's mental health could have limited reliability.
The present study provided novel insight regarding the effectiveness of a co-designed online teacher-training program for providing NIMHI to Japanese children. The findings contribute a novel perspective, suggesting that co-design holds promise as an effective approach in developing online teacher-training programs that not only achieve reasonable satisfaction but also effectively foster learning and bring about behavioral changes among teachers. The findings also offer a fresh perspective on the effectiveness of utilizing digital technology, specifically through online interactive learning coupled with self-paced learning booklets, as an effective modality for delivering training to Japanese teachers. However, the absence of quantitative support for the effectiveness of the online teacher-training program could suggest that the effectiveness of the online teacher-training program may not have been sufficiently robust to be detected by statistical testing. Further improvement in the online teacher-training program would be useful for effectively improving Japanese children's mental health, such as providing tablet applications to assist teachers in implementing suitable intervention strategies and teaching more focused range of strategies. Future studies could employ better study design for evaluation, such as randomized controlled trial and have multiple reviewers independently extracting themes for qualitative analysis. Once a future study establishes the robust effectiveness of such online teacher-training programs, there is potential to adapt and extend their implementation to a broader Japanese population and even other cultural contexts, with necessary cultural adjustments.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Institutional Review Board University of Queensland. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
YT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing—original draft, Writing—review & editing. MB: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing—review & editing, Resources. H-JT: Formal analysis, Methodology, Supervision, Writing—review & editing. SE: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing—review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Baker, J. A., Dilly, L. J., Aupperlee, J. L., and Patil, S. A. (2003). The developmental context of school satisfaction: schools as psychologically healthy environments. Sch. Psychol. Q. 18:206. doi: 10.1521/scpq.18.2.206.21861
Beeson, E. T., and Field, T. A. (2017). Neurocounseling: a new section of the journal of mental health counseling. J. Mental Health Counsel. 39, 71–83. doi: 10.17744/mehc.39.1.06
Bennett-Levy, J., Hawkins, R., Perry, H., Cromarty, P., and Mills, J. (2012). Online cognitive behavioural therapy training for therapists: outcomes, acceptability, and impact of support. Austral. Psychol. 47, 174–182. doi: 10.1111/j.1742-9544.2012.00089.x
Bragg, L. A., Walsh, C., and Heyeres, M. (2021). Successful design and delivery of online professional development for teachers: A systematic review of the literature. Comput. Educ. 166:104158. doi: 10.1016/j.compedu.2021.104158
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Braun, V., and Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 11, 589–597. doi: 10.1080/2159676X.2019.1628806
Breckwoldt, J., Svensson, J., Lingemann, C., and Gruber, H. (2014). Does clinical teacher training always improve teaching effectiveness as opposed to no teacher training? A randomized controlled study. BMC Med. Educ. 14:6. doi: 10.1186/1472-6920-14-6
Brick, K., Cooper, J. L., Mason, L., Faeflen, S., Monmia, J., Dubinsky, J. M., et al. (2021). Tiered neuroscience and mental health professional development in Liberia improves teacher self-efficacy, self-responsibility, and motivation. Front. Hum. Neurosci. 15:664730. doi: 10.3389/fnhum.2021.664730
Champion, K. E., Gardner, L. A., McGowan, C., Chapman, C., Thornton, L., Parmenter, B., et al. (2020). A web-based intervention to prevent multiple chronic disease risk factors among adolescents: co-design and user testing of the Health4Life school-based program. JMIR Form. Res. 4:e19485. doi: 10.2196/19485
Clark, D. A. (2013). “Cognitive restructuring,” in The Wiley Handbook of Cognitive Behavioral Therapy. New York, NY: John Wiley and Sons, Ltd.
De Boer, D., Bosker, H. R. J., and van der Werf, M. P. C. (2010). Sustainability of teacher expectation bias effects on long-term student performance. J. Educ. Psychol. 102, 168–179. doi: 10.1037/a0017289
Deguchi, Y., Iwasaki, S., Kanchika, M., Nitta, T., Mitake, T., Nogi, Y., et al. (2018). Gender differences in the relationships between perceived individual-level occupational stress and hazardous alcohol consumption among Japanese teachers: a cross-sectional study. PLoS ONE 13:e0204248. doi: 10.1371/journal.pone.0204248
Dimeff, L. A., Koerner, K., Woodcock, E. A., Beadnell, B., Brown, M. Z., Skutch, J. M., et al. (2009). Which training method works best? A randomized controlled trial comparing three methods of training clinicians in dialectical behavior therapy skills. Dissem. Impl. Cognit. Behav. Ther. 47, 921–930. doi: 10.1016/j.brat.2009.07.011
Donker, T., Petrie, K., Proudfoot, J., Clarke, J., Birch, M. R., Christensen, H., et al. (2013). Smartphones for smarter delivery of mental health programs: a systematic review. J. Med. Int. Res. 15:e2791. doi: 10.2196/jmir.2791
Dubinsky, J. M., Guzey, S. S., Schwartz, M. S., Roehrig, G., MacNabb, C., Schmied, A., et al. (2019). Contributions of neuroscience knowledge to teachers and their practice. The Neurosci. 25, 394–407. doi: 10.1177/1073858419835447
Ey, L-. A., and Spears, B. (2020). Engaging early childhood teachers in participatory co-design workshops to educate young children about bullying. Pastoral Care Educ. 38, 230–253. doi: 10.1080/02643944.2020.1788129
Faul, F., Erdfelder, E., Lang, A.-G., and Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39, 175–191. doi: 10.3758/BF03193146
Field, T. A., Beeson, E. T., and Jones, L. K. (2015). The new ABCs: a practitioner's guide to neuroscience-informed cognitive-behavior therapy. J. Mental Health Counsel. 37, 206–220. doi: 10.17744/1040-2861-37.3.206
Field, T. A., Beeson, E. T., Jones, L. K., and Miller, R. (2017). Counselor allegiance and client expectancy in neuroscience-informed cognitive-behavior therapy: a 12-month qualitative follow-up. J. Mental Health Counsel. 39, 351–365. doi: 10.17744/mehc.39.4.06
Field, T. A., Miller, R., Beeson, E. T., and Jones, L. K. (2019). Treatment fidelity in neuroscience-informed cognitive-behavior therapy: a feasibility study. J. Mental Health Counsel. 41, 359–376. doi: 10.17744/mehc.41.4.06
Fisher, J. B., Schumaker, J. B., Culbertson, J., and Deshler, D. D. (2010). Effects of a computerized professional development program on teacher and student outcomes. J. Teach. Educ. 61, 302–312. doi: 10.1177/0022487110369556
Ford, J. (2015). An affective cognitive neuroscience-based approach to PTSD psychotherapy: the TARGET model. J. Cognit. Psychother. 29, 68–91. doi: 10.1891/0889-8391.29.1.68
Ford, J. D., Grasso, D. J., Levine, J., and Tennen, H. (2018). Emotion regulation enhancement of cognitive behavior therapy for college student problem drinkers: a pilot randomized controlled trial. J. Child Adoles. Subs. Abuse 27, 47–58. doi: 10.1080/1067828X.2017.1400484
Ford, J. D., Steinberg, K. L., Hawke, J., Levine, J., and Zhang, W. (2012). Randomized trial comparison of emotion regulation and relational psychotherapies for PTSD with girls involved in delinquency. J. Clin. Child Adoles. Psychol. Off. J. Soc. Clin. Child Adoles. Psychol. Am. Psychol. Assoc. 41, 27–37. doi: 10.1080/15374416.2012.632343
Furuichi, Y., and Tamaki, H. (1994). 学校生活のしさとその定要因 [Enjoyment of School Life and Its Determinants]. Okayama: Bulletin of Faculty of Education, Okayama University, 105–113. doi: 10.20587/pamjaep.36.0_169
Ghaderi, A. (2006). Does individualization matter? A randomized trial of standardized (focused) versus individualized (broad) cognitive behavior therapy for bulimia nervosa. Behav. Res. Ther. 44, 273–288. doi: 10.1016/j.brat.2005.02.004
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatr. Allied Disciplines 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Grawe, K. (2017). Neuropsychotherapy: How the neurosciences inform effective psychotherapy. Routledge. doi: 10.4324/9781315090573
Harada, E., and Watanabe, Y. (2021). ソシャルエモショナルラニングによる 高校生のソシャルスキルとレジリエンスへの果 [Effects of social and emotional learning on the social skills and resilience of Japanese high school students]. The Studies on Educational Practices 24, 1–14. doi: 10.50841/kyoikujissen.24.0_1
Hollis, C., Falconer, C. J., Martin, J. L., Whittington, C., Stockton, S., Glazebrook, C., et al. (2017). Annual research review: Digital health interventions for children and young people with mental health problems – a systematic and meta-review. Journal of Child Psychology and Psychiatry 58, 474–503. doi: 10.1111/jcpp.12663
Kelly, N., Wright, N., Dawes, L., Kerr, J., and Robertson, A. (2019). Co-design for curriculum planning: A model for professional development for high school teachers. Australian Journal of Teacher Education (Online) 44, 84–107. doi: 10.14221/ajte.2019v44n7.6
Kirkpatrick, D. L., and Kirkpatrick, J. D. (2006). Evaluating Training Programs: The Four Levels. Berrett-Koehler Publishers.
Liddle, I., and Carter, G. F. A. (2015). Emotional and psychological well-being in children: The development and validation of the Stirling Children's Well-being Scale. Educational Psychology in Practice 31, 174–185. doi: 10.1080/02667363.2015.1008409
Lohaus, A., Klein-Heßling, J., Vögele, C., and Kuhn-Hennighausen, C. (2010). Psychophysiological effects of relaxation training in children. British Journal of Health Psychology 6, 197–206. doi: 10.1348/135910701169151
Marín, V. I., Asensio-Pérez, J. I., Villagrá-Sobrino, S., Hernández-Leo, D., and García-Sastre, S. (2018). Supporting online collaborative design for teacher professional development. Technol. Pedag. Educ. 27, 571–587. doi: 10.1080/1475939X.2018.1547787
Matsumoto, Y., and Shimizu, E. (2016). The FRIENDS cognitive behavioral program in Japanese schools: An examination of the treatment effects. School Psychology International 37, 397–409. doi: 10.1177/0143034316649639
Ministry of Health Labour, and Welfare. (2021). Statistics of suicide: Circumstances in each year. Available online at: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsu_year.html
Muris, P., Meesters, C., Eijkelenboom, A., and Vincken, M. (2004). The self-report version of the Strengths and Difficulties Questionnaire: Its psychometric properties in 8- to 13-year-old non-clinical children. The British Journal of Clinical Psychology, 43(Pt 4), 437–448. doi: 10.1348/0144665042388982
Nishida, C., Ishimoto, Y., Takizawa, Y., Katayama, T., and Matsumoto, Y. (2021). Preliminary evidence for the reliability and validity of the Stirling children's well-being scale (SCWBS) with Japanese children. Int. J. Educ. Res. Open 2:100034. doi: 10.1016/j.ijedro.2021.100034
Noda, W., Ito, H., Harada, S., Nakajima, S., Takayanagi, N., Someki, F., et al. (2013). Examination here liability and validity of the Japanese version of the strengths and difficulties questionnaires self-raing form using the entire cohort data in one suburban city in Japan. Rinsho Seisin Igaku 42, 119–127.
Rossouw, P. J. (2014). Neuropsychotherapy: Theoretical underpinnings and clinical applications. Mediros.
Seminowicz, D. A., Shpaner, M., Keaser, M. L., Krauthamer, G. M., Mantegna, J., Dumas, J. A., et al. (2013). Cognitive-behavioral therapy increases prefrontal cortex gray matter in patients with chronic pain. The Journal of Pain 14, 1573–1584. doi: 10.1016/j.jpain.2013.07.020
Sheperis, D. S., Coker, J. K., Haag, E., and Salem-Pease, F. (2020). Online counselor education: A student-faculty collaboration. Professional Counselor 10, 133–143. doi: 10.15241/dss.10.1.133
Skivington, K., Matthews, L., Simpson, S. A., Craig, P., Baird, J., Blazeby, J. M., et al. (2021). A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 374, n2061. doi: 10.1136/bmj.n2061
Snow, W. H., Lamar, M. R., Hinkle, J. S., and Speciale, M. (2018). Current practices in online counselor education. Professional Counselor 8, 131–145. doi: 10.15241/whs.8.2.131
Takizawa, Y., Bambling, M., Hsien-Jin, T., and Edirippulige, S. (2023a). The feasibility of developing an online teacher training program. Health Open Research.
Takizawa, Y., Bambling, M., Matsumoto, Y., Ishimoto, Y., and Edirippulige, S. (2023b). Effectiveness of universal school-based social-emotional learning programs for promoting social-emotional skills, attitudes towards self and others, positive social behaviors, and Improving emotional and conduct problems among Japanese Children: A meta-analytic systematic review. Frontiers in Education, 8. doi: 10.3389/feduc.2023.1228269
Takizawa, Y., Murray, J., Bambling, M., Matsumoto, Y., Ishimoto, Y., Yamane, T., et al. (2022). Integration of clinical neuroscience into psychotherapy: A narrative review of neuroscience-informed psychotherapy models for the treatment of depression and anxiety disorders. Psychotherapy and Counselling Journal of Australia 10, 71199. doi: 10.59158/001c.71199
Wang, P., Wang, S. C., Liu, X., Jia, S., Wang, X., Li, T., et al. (2022). Neural functions of hypothalamic oxytocin and its regulation. ASN NEURO 14, 17590914221100706. doi: 10.1177/17590914221100706
Wei, Y., McGrath, P. J., Hayden, J., and Kutcher, S. (2016). Measurement properties of tools measuring mental health knowledge: a systematic review. BMC Psychiatry 16:297. doi: 10.1186/s12888-016-1012-5
Weiner, B. J., Lewis, C. C., Stanick, C., Powell, B. J., Dorsey, C. N., Clary, A. S., et al. (2017). Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 12:108. doi: 10.1186/s13012-017-0635-3
Weisz, J. R., Chorpita, B. F., Palinkas, L. A., Schoenwald, S. K., Miranda, J., Bearman, S. K., et al. (2012). Testing standard and modular designs for psychotherapy treating depression, anxiety, and conduct problems in youth: a randomized effectiveness trial. Arch. Gen. Psychiatry 69, 274–282. doi: 10.1001/archgenpsychiatry.2011.147
Yamaguchi, S., Foo, J. C., Kitagawa, Y., Togo, F., and Sasaki, T. (2021). A survey of mental health literacy in Japanese high school teachers. BMC Psychiatry 21, 478. doi: 10.1186/s12888-021-03481-y
Yamaguchi, S., Foo, J. C., Nishida, A., Ogawa, S., Togo, F., Sasaki, T., et al. (2020). Mental health literacy programs for school teachers: A systematic review and narrative synthesis. Early Intervention in Psychiatry 14, 14–25. doi: 10.1111/eip.12793
Yamamoto, T., Matsumoto, Y., and Bernard, M. E. (2017). Effects of the cognitive-behavioral You Can Do It! Education program on the resilience of Japanese elementary school students: A preliminary investigation. International Journal of Educational Research 86, 50–58. doi: 10.1016/j.ijer.2017.08.006
Keywords: mental health intervention, teacher, training, Japanese, online, neuroscience, children, co-design
Citation: Takizawa Y, Bambling M, Teoh H-J and Edirippulige S (2024) Evaluation of co-designed online teacher training program for providing neuroscience-informed mental health intervention to Japanese children. Front. Educ. 9:1396271. doi: 10.3389/feduc.2024.1396271
Received: 05 March 2024; Accepted: 27 May 2024;
Published: 07 June 2024.
Edited by:
Benjamin Dreer-Goethe, University of Erfurt, GermanyReviewed by:
Nicole Jacqueline Albrecht, Flinders University, AustraliaCopyright © 2024 Takizawa, Bambling, Teoh and Edirippulige. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Takizawa, eXUudGFraXphd2FAdXFjb25uZWN0LmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.