
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 06 February 2023
Sec. Special Educational Needs
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.951970
This article is part of the Research TopicThe Impact of COVID-19 Pandemic on Children and Adolescents with Disabilities: Education, Development, and Well-being of Culturally and Linguistically Diverse FamiliesView all 5 articles
 Giona Di Poi1,2,3
Giona Di Poi1,2,3 Daniel Dukes2,3
Daniel Dukes2,3 Ben Meuleman3
Ben Meuleman3 Pamela Banta Lavenex1
Pamela Banta Lavenex1 Pierre Lavenex4
Pierre Lavenex4 Anouk Papon1
Anouk Papon1 Michel Tran1
Michel Tran1 Lina Stallmann2,3Noémie Treichel2,3
Lina Stallmann2,3Noémie Treichel2,3 Andrea C. Samson1,2,3*
Andrea C. Samson1,2,3*In the spring of 2020, the COVID-19 pandemic generated a health, social, political, and economic crisis that dramatically reduced the institutional support for families of individuals with neurodevelopmental conditions (NDCs). To understand how these families may have experienced and coped with the pandemic, we created an online questionnaire that reached more than 10,000 families in 78 countries. The current manuscript - framed within the International Classification of Functioning, Disability and Health (ICF-10) model - investigates the impact of specific health conditions and personal or environmental factors on the anxiety of families living in Switzerland during the early months of the pandemic. To assess how differences in anxiety over time were predicted by specific health conditions or personal and environmental factors, two separate multilevel analyses were conducted for parents and their children with NDCs (N = 256). First, results showed that only parents reported an increase in anxiety when the pandemic started. Second, concerns related to loss of institutional support and financial and economic problems were the most anxiety-provoking factors for parents, whereas parents reported that the most anxiety-provoking factor for children was their concern about becoming bored. Many parents may have struggled with economic problems and managed multiple extra roles and tasks in their daily lives because institutional support was no longer available. As reported by their parents, although individuals with NDCs did not show an increase in anxiety, they may have struggled with boredom. This result may represent the inability to engage in satisfactory activities in daily life associated with a partial unawareness of the pandemic and the respective protective measures. Further research should more thoroughly investigate the potential effects of the individual’s primary condition, presence and severity of intellectual disability and awareness of the pandemic on the anxiety of individuals with NDCs. Ultimately, we present a series of reflections and practical suggestions that could help guide policymakers in potential future periods of crisis, social estrangement, and distance learning.
In the spring of 2020, the COVID-19 pandemic generated a health, social, political, and economic crisis that dramatically reduced the institutional support for all members of society. This reduction of support was the result of a series of protective measures that principally consisted of the closure of all non-essential services such as non-food stores, schools, and therapy centers. These events had an important psychological impact on society. Several studies conducted in the general population have documented a wide range of associated negative symptoms such as acute panic, anxiety, obsessive behaviours, hoarding, paranoia, depression, and post-traumatic stress disorder (Brooks et al., 2020; Dubey et al., 2020; Liu et al., 2020; Miranda et al., 2020).
Families of individuals with neurodevelopmental conditions (NDCs), a particularly vulnerable segment of the population, may have been especially impacted by these protective measures. Studies conducted during the pandemic have shown a higher prevalence of burden, depression, anxiety, and stress in parents and caregivers of individuals with NDCs compared to parents or caregivers of typically developing (TD) individuals (Chafouleas and Iovino, 2020; Willner et al., 2020), and an increase in challenging behaviours in individuals with NDCs, for example, in individuals with an autism spectrum condition (ASC; Colizzi et al., 2020; Panjwani et al., 2021). These findings may be linked to the specific vulnerabilities reported for individuals with NDCs. For instance, a higher prevalence of physical health problems, such as somatic disorders (Tye et al., 2019; Samson et al., 2020), obesity or cardiovascular disease (Perera et al., 2020), and the presence of mental health comorbidities like anxiety and depression (Patel et al., 2018; Röhr et al., 2020) are reported for this population. In addition, restrictions on participation in habitual activities could be a source of increased anxiety, particularly for individuals with ASC (Courtenay and Perera, 2020). Finally, it is also possible to interpret these results in terms of the need for additional daily life support in these families. For example, distance learning for children with NDCs may require not only physical support such as books, computers, or internet access but also access to specific and individualized curricula and pedagogical methods that meet the child’s specific abilities and special needs (United Nations International Children’s Emergency Fund, 2020).
The concept of special needs can be conceptualized within the International Classification of Functioning, Disability and Health (ICF-10; World Health Organization, 2001), which identifies a series of interrelated factors that influence how a health condition – seen as an impairment in bodily function, including psychological function (e.g., an individual’s primary condition/diagnosis, presence of intellectual disability (ID), or specific learning disabilities (LD) such as impairments in reading, written expression or mathematics) can limit an individual’s activity (e.g., communication, interpersonal interactions and relationships, education) and participation in daily life contexts. In the present study, we refer to the International Classification of Diseases and Related Health Problems (ICD-10; World Health Organization, 2015) to classify all specific health conditions reported for individuals with NDCs. In parallel, we use the ICF-10 framework to understand how these specific health conditions, in concert with environmental and personal factors, may have limited activity and participation during the COVID-19 pandemic.
Environmental factors include the “physical, social and attitudinal environment in which individuals live and conduct their lives” (p. 16; e.g., products and technology, support and relationships, services, systems, and policies). Personal factors include the “particular background of an individual’s life and living and comprise features of the individual that are not part of a health condition or health states” (p. 17; e.g., age, gender, habits, preferences). Amongst the environmental factors, barriers and facilitators can be identified, which “through their absence or presence, improve [or limit] functioning and reduce [or produce] disability” (p. 222; e.g., assistive technology, attitudes of individuals towards disability, inclusive services, systems, and policies). The concept of special needs can therefore be viewed as the need for a variety of environmental facilitators, such as institutional support and public services, that can help individuals overcome impairments, activity limitations, and participation restrictions in daily life.
Public services and easy access to them may then be considered strong facilitators and vehicles for functioning and participation for all members of society, but particularly for families of individuals with NDCs. In this regard, conducting a study on the psychological impact of the first months of the pandemic in Switzerland is of importance for two reasons. First, Switzerland is one of the top-ranked countries in the Public Services Index, which is an international indicator of basic state functions (including essential services such as health, electricity, or connectivity services) and the state’s ability to protect its citizens through perceived effective policing (i.e., The Global Economy, n.d.). Second, the Swiss government imposed comparably less restrictive protective measures compared to its neighboring countries, such as France, Italy, Germany, or Austria (Our World in Data, 2022).
For the current study, it is crucial to describe the protective measures and restrictions implemented by the government in Switzerland and to explain how these measures may have generated environmental barriers for families of individuals with NDCs. The Federal Council announced on March 13, 2020, that schools would be closed until at least April 4 (Federal Council, 2020a) and that students would be in distance learning mode as of March 16. On the same date, the Federal Council declared a state of health emergency, leading to measures that included the temporary closure of all non-essential services until April 19 (Federal Council, 2020c). This measure thus meant the abrupt interruption of certain support services for individuals with NDCs and their families, and an interruption or adaptation of other therapies and services to a remote format (e.g., online speech therapy or psychotherapy). Perhaps in recognition of these difficulties, on March 20, the federal government (Federal Council, 2020d) published a prescription offering a loss-of-earnings allowance for parents of children with NDCs up to the age of 12 who had to stop working to care for children at home. As of April 16, the Federal Council extended this offer to parents of individuals with NDCs up to the age of 18 who qualified for an intensive care supplement, and to parents of individuals up to the age of 20 who were attending a special school or institution that had been closed (Federal Council, 2020b). On May 25, the idea of specific aid aimed at explaining the COVID-19 situation to individuals with NDCs emerged with a set of recommendations on how to publish information in easy-to-read language and sign language (Federal Office for Disability Equality, 2020).
However, despite the Swiss government’s efforts to provide environmental facilitators to these families, a lack of daily support and an increased risk of social isolation and burnout among parents has been observed (Rosenstein, 2020). While these families may have already exhibited increased vulnerability before the pandemic, changes in daily life due to protective measures may have produced additional environmental barriers, activity limitations, and participation restrictions. The COVID-19 pandemic generated a decrease in the availability and accessibility of support services for these families, and the lack of this usual support required many parents to adapt to meet the specific educational, emotional, physical, and therapeutic needs of their child on a daily basis, all while trying to manage distress and anxiety in their own lives and in the lives of other family members (Toseeb et al., 2020). For instance, in a study conducted in Switzerland, parents reported difficulties such as lack of time, computer equipment and practical skills to cope with the accumulation of tasks in their daily lives due to working at home, home schooling and distance learning (Widmer et al., 2020). Some international studies have already reported increased stress and anxiety among individuals with NDCs and their families in relation to the pandemic (Iovino et al., 2021; Pettinicchio et al., 2021; Siracusano et al., 2021; Navas et al., 2022). Nevertheless, published reports have highlighted the gaps in our knowledge and the limited amount of robust and good quality research concerning COVID-19 and people with NDCs (Croft and Fraser, 2021; Doody and Keenan, 2021). The present study aims to document more of the concerns of families of children with NDCs by including a large and representative sample of the entire population of individuals with NDCs, by conducting inferential analysis to allow for predictions, by investigating the impact of family conflicts and financial concerns, and by assessing the influence of specific inclusive and protective policy measures implemented in Switzerland during the COVID-19 pandemic.
Given the findings from previous studies, we hypothesized that the presence of physical and mental health issues, interruption of support services, and restrictions on habitual activities and routines may also have led to increased stress and anxiety in these families in Switzerland. First, it was important to understand the situation experienced by these families before and during the first months of the pandemic. To this end, we relied on descriptive statistics and qualitative data collected from an online questionnaire completed by parents of individuals with NDCs in Switzerland between April 8 and June 27, 2020. These data present the health condition of individuals with NDCs, their daily occupation before and during the pandemic, their reactions to the closure of institutions, their awareness of the pandemic, their abilities to express fears and anxieties, and the wishes or specific needs of these families during the early months of the pandemic. We further assessed whether there was a general increase in anxiety during the early months of the pandemic. We hypothesized that the primary condition of the individual with NDCs (i.e., ASC, Williams syndrome (WS), Down syndrome (DS), attention deficit disorder with or without hyperactivity (ADHD), and intellectual disability (ID)) would have an influence on their anxiety due, at least in part, to condition-specific predispositions to develop anxiety. For example, individuals with ASC, WS or ID are reported to present higher levels of anxiety in daily life compared to the TD population (Emerson and Hatton, 2007; Dankner and Dykens, 2012; Rodgers et al., 2012; Reardon et al., 2015). It is important to mention that since some individuals with the above-mentioned conditions, such as ASC or WS, may also present with ID, we decided to create a specific category for ID as a primary condition. This category refers to a condition for which the etiology of the ID is not attributed to other syndromes or conditions. To test this hypothesis, we evaluated the anxiety levels of parents and the parent-reported anxiety of their children with NDCs for three different timepoints (Time 1: “before COVID-19”; Time 2: “when the pandemic started” – with reference to the closure of all non-essential services on March 13, 2020; Time 3: “at the time of completion of the questionnaire” – i.e., between April 8 and June 27, 2020) and correlated that with the individuals’ primary conditions. Anxiety levels for Time 1 and Time 2 were retrospectively collected at Time 3, based on the parents’ recollection of memories for these timepoints. Finally, we aimed to better understand the influence of personal factors (e.g., age, gender), potential environmental barriers (e.g., loss of institutional support, financial and economic problems, loss of routine, ability to meet peers and friends) and additional cognitive conditions (e.g., self-and parent-reported presence of a mild, moderate or severe ID, LD, or anxiety disorders) on anxiety in parents and individuals with NDCs. Based on initial reports of factors that may have affected the level of anxiety in these families during the pandemic (Greenway and Eaton-Thomas, 2020; Cacioppo et al., 2021; Cheng et al., 2021; Lebrasseur et al., 2021; Lee et al., 2021; Redquest et al., 2021; Navas et al., 2022), we expected different anxiety-provoking factors for parents and individuals with NDCs. We hypothesized that the most anxiety-provoking factors for parents would be primarily linked to environmental barriers such as the loss of institutional support (e.g., schools, therapy centers, workplace) whereas for individuals with NDCs we predicted they would be primarily related to environmental barriers such as the loss of daily life routine (e.g., school, therapy centers) and social relationships. Additionally, we investigated if and how these factors interacted with the primary condition of the individual with NDCs.
In an attempt to understand how individuals with NDCs and their families experienced and coped with the early months of the COVID-19 pandemic in different countries, we created an online questionnaire (Van Herwegen et al., 2020; Dukes et al., 2021). An international network of collaborators translated and disseminated the questionnaire in 16 languages, eventually reaching more than 10,000 families in 78 countries around the world. The questionnaire (original English version available in Supplementary Materials) and database have been used for other papers that have been published (Su et al., 2021; Furar et al., 2022; Sideropoulos et al., 2022a, 2022b). One parent of each family completed the anonymous survey which contained a total of 299 questions. The initial section concerning their child with NDCs took an average of 30 min to complete, while an additional section concerning a TD sibling, if completed, took on average an extra 15 min. Open-ended questions were included in the questionnaire to allow participants to describe in their own words how their family handled some specific concerns and situations, with the goal of avoiding overlooking any relevant information about participant’s subjective experiences.
The questionnaire was divided into four main sections. The first section was devoted to collecting general sociodemographic information about the parent, the child with NDCs and the family (e.g., child’s primary condition, child’s health conditions, child’s daily occupation before and during confinement, percent of employment of the parent).
The second section comprised general questions designed to establish a timeline of region-specific events (e.g., access to or eventual closure of schools and institutions, changes in government guidelines, whether the child or any family member had been tested or infected) and the extent of concern about specific events (e.g., when they heard about COVID-19, when they heard about social distancing measures or when the government suggested to self-isolate).
The third section focused on the anxiety levels and specific anxiety-related concerns of people with NDCs and their parents for three distinct time points: (1) before COVID-19; (2) when the pandemic started; and (3) at the time of completion of the questionnaire. Parents were asked to answer the following questions for each timepoint: “How anxious were/are you?” and “How anxious was/is your child?.” Parents rated the level of anxiety on a Likert scale ranging from 1 (not anxious) to 5 (very anxious). The 13 questions about concerns were informed by the eight well-being categories for individuals with developmental and intellectual disabilities as defined by Schalock and Verdugo (2002), and included worries related to social inclusion (e.g., not being able to meet others), physical well-being (e.g., worries about catching COVID-19 and own health), interpersonal relations (e.g., worries about family conflict and others becoming ill), material well-being (e.g., financial worries), emotional well-being (e.g., worries about boredom), self-determination (e.g., loss of routine), and personal development (e.g., loss of institutional support). These were grouped into the following categories: health-related worries, social-related worries, school closure-related worries, and family-related worries (for the entire list of concerns see Tables 1 and 2). Parents indicated the level of each concern on a Likert scale ranging from 1 (not at all) to 5 (extremely). In addition, the responding parent was asked to qualitatively report in the questionnaire (in a series of open-ended questions) their child’s reaction to the closure of institutions, additional relevant information about specific concerns with respect to COVID-19, or thoughts about specific needs or wishes for their families.
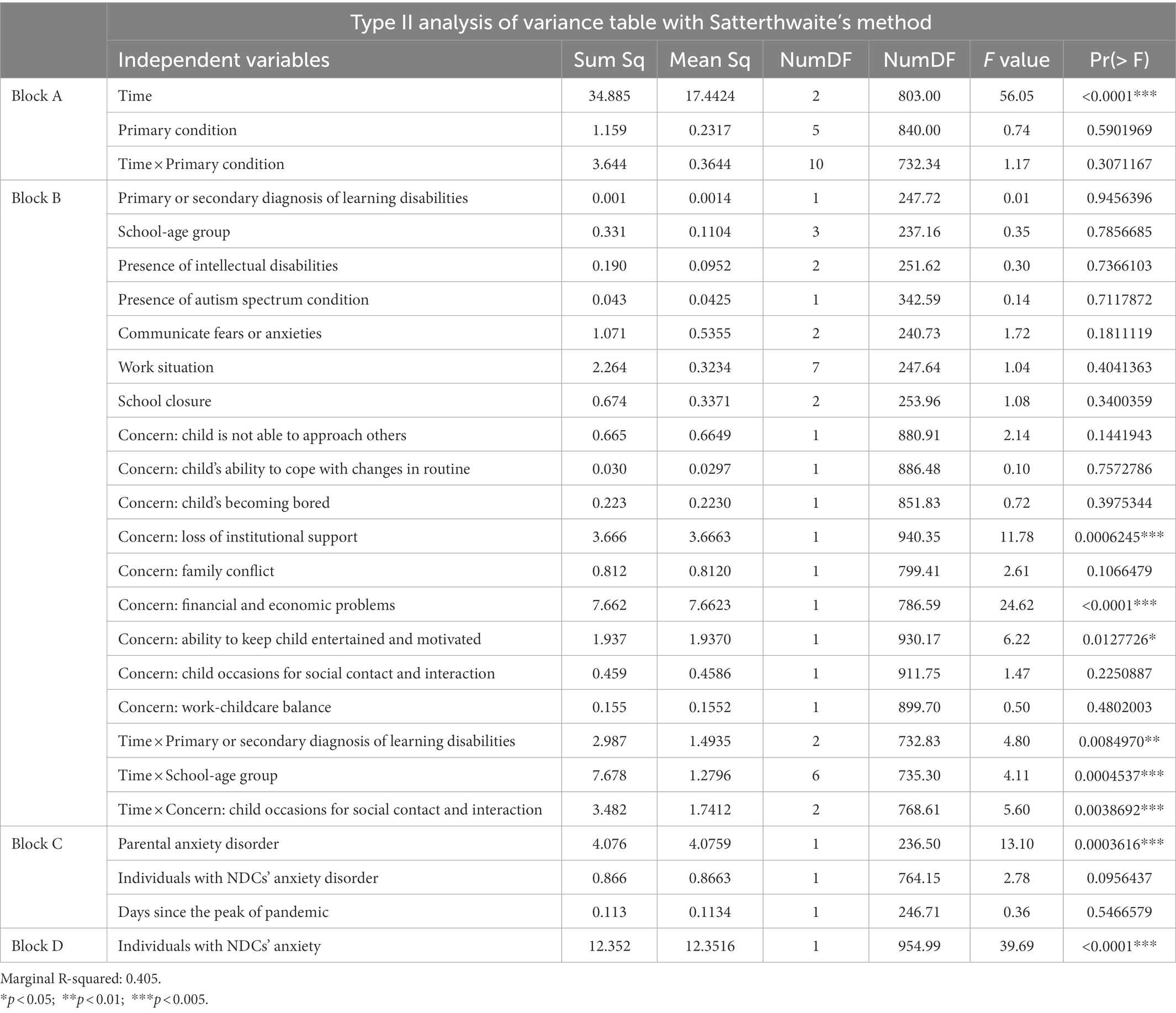
Table 1. Conditional multilevel analysis on parental anxiety.
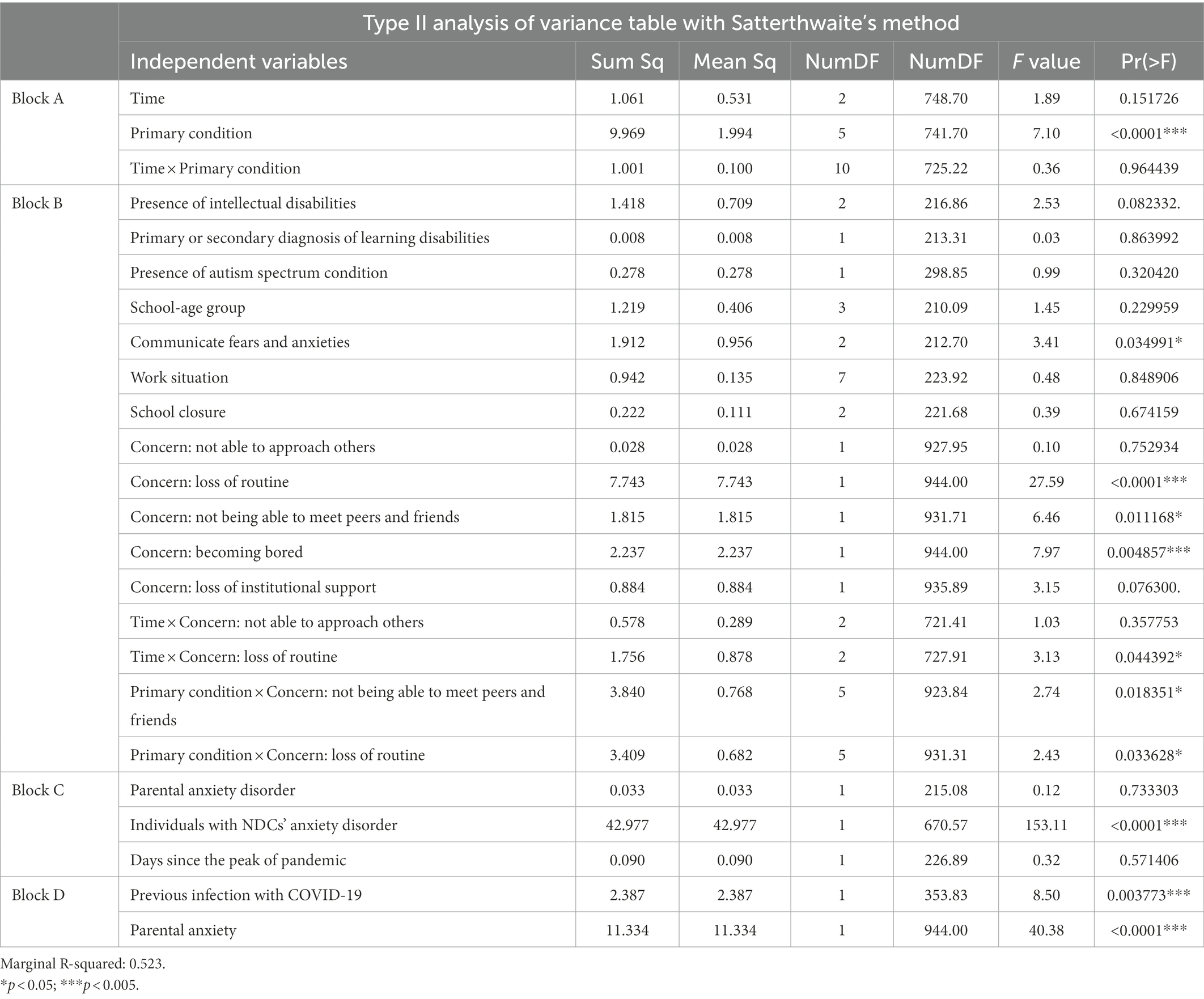
Table 2. Conditional multilevel analysis on Individuals with NDCs’ anxiety.
The fourth section investigated the emotion regulation strategies implemented by individuals with NDCs and TD siblings to cope with stress during the pandemic. For parents that responded for their TD sibling as well, they were asked to answer some socio-demographic questions (e.g., age of the TD child), in the third and in the fourth sections of the questionnaire. The data regarding emotion regulation strategies implemented by individuals with NDCs and TD siblings are not presented in the present study.
Participants were recruited through flyers distributed via social networks, social media, and e-mails to special education institutions, associations, and individuals throughout Switzerland (original flyer available in Supplementary Materials). Several research partner groups were involved in the recruitment process. Participants were able to access the questionnaire in the language of their choosing through a QR code or a website link displayed on the flyers.
The anonymous study was approved by the Ethics Commission of UniDistance Suisse. Participation was voluntary and not compensated.
Prior to analysis of the Swiss dataset, we removed participants that contained over 70% missing values from the data. This procedure reduced the sample from 601 to 392 families for Switzerland. For the remaining variables, we chose not to impute missing values in order to avoid the complexities associated with the multiple imputation of hierarchically structured data. Instead, we relied on a combination of complete-case-analysis (i.e., only fully observed variables are considered for analysis) and the implicit imputation properties of multilevel regression models. Such models perform an implicit imputation on repeated observations that are missing based on the pool estimate of repeated measures covariance. The complete-case-analysis approach assumes that the messiness mechanism for those variables is Missing Completely At Random (MCAR), while the implicit multilevel imputation assumes that the messiness mechanism for those variables is Missing At Random (MAR). MAR implies that unobserved data can be recovered from observed data (Fitzmaurice et al., 2012).
First, a series of descriptive statistics and chi-squared tests were performed to describe the demographics of the sample and to report the situation of the families during the early months of the pandemic. Second, a simple qualitative analysis was performed to properly code and sort into categories the open-ended questions with respect to the individual with NDCs’ reaction to the closure of institutions. A preliminary analysis of the responses resulted in the creation of five categories: positive reaction; negative reaction; understood the situation; did not understand the situation; the child had the impression (or was told by the parents) that they were on vacation. To assess the reliability of the categories, an intercoder reliability analysis was performed. The agreement was 100% on a randomly selected 20% of the data units. The results of this analysis, some of the parents’ testimonials and the specific wishes reported by parents will be included in the discussion section to anecdotally present personal experiences with the pandemic. Third, two separate multilevel analyses were conducted for parents and their children with NDCs to analyze how differences in anxiety over time were predicted by specific concerns, health conditions, personal factors or potential environmental barriers.
Multilevel models are regression models that can deal with more than one source of random sampling error simultaneously (e.g., error due to measurement, error due to subjects), including hierarchical nesting of random error. The structure of the current analysis consists of 3 levels: (1) timepoints, which were nested in (2) family members, which were nested in (3) families. In this model, timepoints are treated as “repeated” observations within the group of parents and children, and up to two children (NDC and/or TD) as “repeated” observations within families. For the multilevel analyses, random effects in the model consisted of (1) a random intercept for families, and (2) pure residual error. This simple structure assumed that repeated measures within families were correlated. Fixed effects in the model reflected the effects of the chosen independent variables (IVs), as sources of fixed variance in the dependent variable (e.g., time, demographics, concerns).
A selection from the entire list of concerns was made both to test our hypotheses as well as to investigate other potential operable, as opposed to abstract, environmental barriers encountered by these families over time. Therefore, all health-related concerns (e.g., about illness in general, about COVID-19, about the child’s health) were excluded from these analyses because they were not operable environmental barriers that could reveal environmental facilitators capable of improving activity and participation in daily life (for an overview of health-related concerns in the UK, see Sideropoulos et al., 2022a). In addition, the concern about “financial and economic problems” was removed from the model for individuals with NDCs because their average age was only 12. We divided our chosen set of IVs into four main blocks, to explore their association with the level of anxiety experienced by parents and individuals with NDCs. Block A represented basic “design” variables, consisting of the main effects and interaction between time and individual’s primary condition on anxiety. Block B represented confirmatory moderator variables, which investigated our hypotheses and included variables such as concern about the loss of institutional support or concern about loss of routines (for complete lists, see the second blocks of variables in Tables 1; 2). Main effects of Block B were never removed from the final model, due to their confirmatory nature. However, significant main effects in Block B were further tested for moderation effects with the design variables in Block A, with only significant moderators kept in the final model. Block C represented confirmatory confounder variables that may have confounded other effects on anxiety (e.g., presence of an anxiety disorder, days since the peak of pandemic). Main effects in Block C were never removed from the final model, and interactions with block A (or B) were not allowed (i.e., they were included as pure controlling variables). Block D represented additional exploratory variables regarding anxiety (e.g., parental or individual with NDCs’ anxiety, infection by COVID-19, gender). Main effects in Block D were removed from the final model if they were non-significant, and interactions were not allowed.
Once a model was fitted, all non-significant confirmatory interactions and exploratory variables were removed, followed by a Type II ANOVA breakdown of the remaining effects with F-tests. Follow-up tests to significant F-tests – if needed – were conducted with pairwise t-tests between group levels (for factors), or by simple t-tests for continuous regression slopes. For the latter, we also report the standardized regression coefficients (denoted βz) as a measure of effect size. Goodness-of-fit for the entire model was quantified by marginal R2, which is a measure of proportion-of-variance-explained for multilevel models that collapses across random effects (Rights and Sterba, 2019). A reduced significance level of α = 0.005 for all inferential tests was employed in order to reduce errors in statistical hypothesis testing (Benjamin et al., 2018). Furthermore, the degrees of freedom of F-tests and t-tests in the multilevel analysis were adjusted for the presence of random effects using Satterthwaite’s correction (Fitzmaurice et al., 2012). For scientific interest, the results section also reports findings that do not meet the strict threshold of p < 0.005. These findings are indicated by an asterisk (p < 0.05*) and should be interpreted with caution, providing only suggestions for future research. Finally, it is important to note that unlike traditional approaches such as repeated measures (M) ANOVA, multilevel models allow for the inclusion of missing levels in the data hierarchy. Therefore, missing data and valid sample percentage will be reported in the sociodemographic results.
R statistical software (version 4.0.3; R Core Team, 2020) was used, with packages “mice” for analysis of missing data patterns (Van Buuren and Groothuis-Oudshoorn, 2011); and with packages “lme4” (Bates et al., 2015) and “lmerTest” (Kuznetsova et al., 2017) for multilevel analyses. For all other analyses, JASP (version 0.16) was used.
From a total of 601 families that completed the questionnaire at least partially between April 8 and June 27, 2020, a first missing data analysis reduced the sample to 392 families. To further eliminate incomplete and inconsistent data from our database, and to focus on individuals who lived with the family before and during the pandemic, four additional inclusion criteria were used: (1) available information about sociodemographic questions and family situation during the pandemic; (2) families of individuals with NDCs presenting with ASC, WS, DS, ADHD or ID primary condition, or families who completed information for an additional TD sibling; (3) correct response to control questions provided by an automated bot (to determine whether the user is a human and not a computer); and (4) parents who lived with their child with NDCs before and during the pandemic. Note that some families did not meet more than one of the four inclusion criteria (e.g., unavailable information about sociodemographic questions and family situation during the pandemic AND parents did not live with their child with NDCs before and during the pandemic).
The final sample resulted in 256 families of individuals with NDCs (who also responded for 95 additional TD siblings), and 37 additional families who responded for a TD sibling (but whose child with NDCs did not meet at least one of the conditions reported in the inclusion criteria), for a total of 293 families. The 256 families who matched the primary condition criteria were included in all analyses, while the additional 37 families were only included as a TD comparison group (primary condition variable) in the multilevel analyses, amounting to a total of 132 TD siblings. Thus, the comparison TD sibling group in this study is composed of individuals who are siblings of the other participants whose results are analyzed as well as siblings of participants who are not included in the analysis but who do have NDCs.
Table 3 presents the sociodemographic characteristics of the sample. To investigate differences in anxiety among different school-age groups of individuals with NDCs, we created four categories based on the average age of children in preschool and primary, secondary or tertiary school (and beyond) in Switzerland. Among individuals with NDCs, 67.6% (n = 173) were male and ranged in age from 1 to 50 years (M = 12.61, SD = 6.98), while 43.9% (n = 58) of the TD siblings were male and ranged from 1 to 43 years (M = 12.64, SD = 7.05).
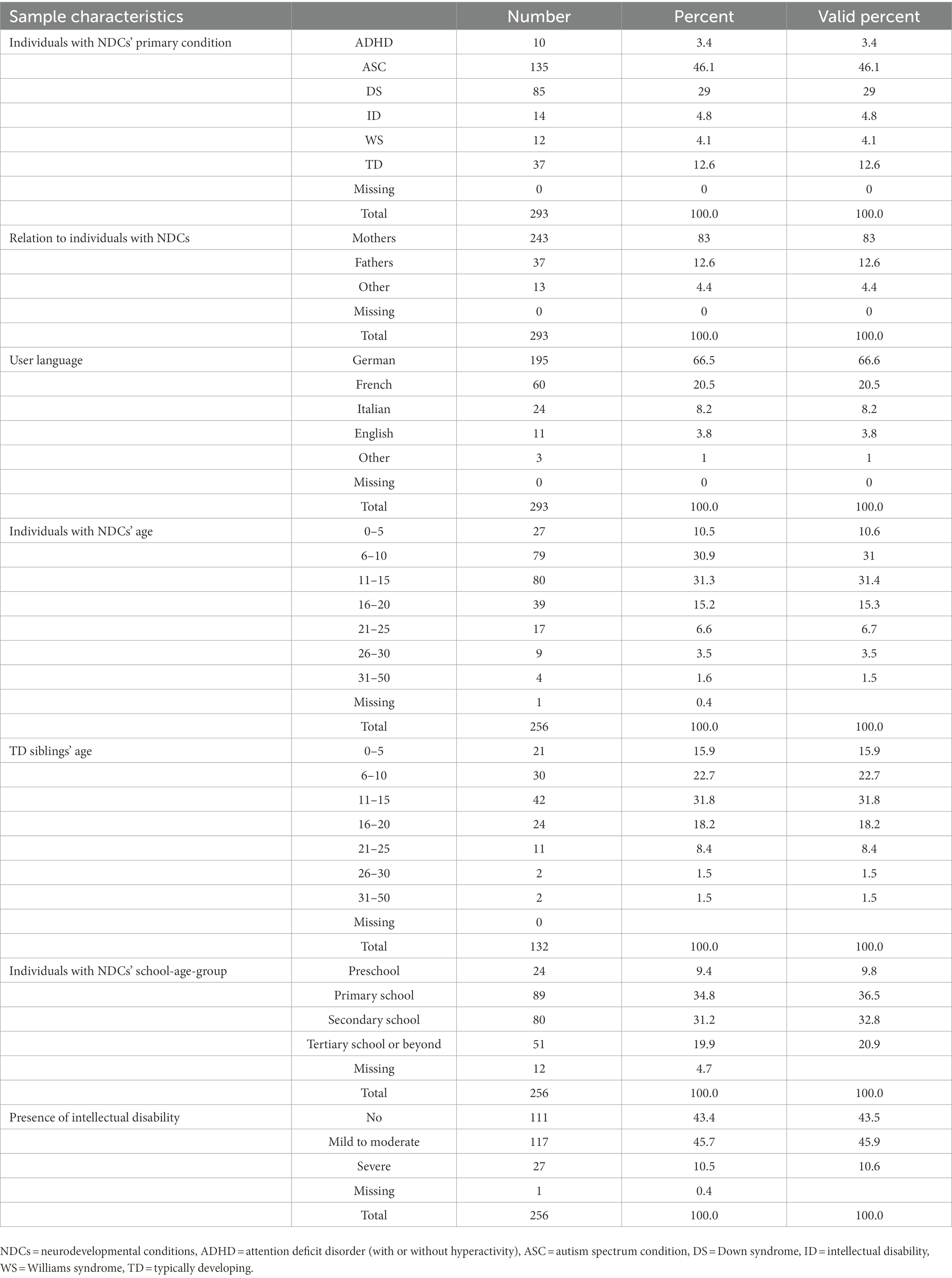
Table 3. Sociodemographic characteristics of the sample.
At Time 1 individuals with NDCs were attending a regular school (n = 86; 33.6%), a special school (n = 83; 32.4%), working in a protected environment (n = 24; 9.4%), in preschool (n = 19; 7.4%), living at home without daily occupation (n = 19; 7.4%), with paid full or part-time work (n = 5; 2%) or in other situations (n = 20; 7.8%). At Time 3, 90.2% (n = 220) of parents mentioned the closure of the institution or school attended by their child. In cases where the institutions remained open (n = 24, 9.8%), a third of the parents decided to withdraw their children and keep them home (n = 8). Further investigation revealed that 16.7% of individuals with NDCs (n = 38) were reported by their parents as not being aware of the COVID-19. An analysis revealed a main effect of the individual’s primary condition on unawareness of COVID-19, X2(4, N = 227) = 26.4, p < 0.001. Individuals reported as unaware of COVID-19 presented with the following primary conditions: 0 (of 9) with ADHD, 10 (of 115) with ASC, 20 (of 80) with DS, 7 (of 12) with ID, and 1 (of 11) with WS. Another analysis revealed a main effect of the presence and severity of ID on reported unawareness of COVID-19, X2(2, N = 227) = 50.3, p < 0.001: 2% (2 of 96) of individuals with no form of ID, 19% (20 of 104) of individuals with a mild to moderate ID and 59% (16 of 27) of individuals with a severe ID were reported as unaware of COVID-19. A mild to severe ID was more widely reported for individuals with DS (82 of 85), ASC (36 of 134), or ID (14 of 14) as a primary condition than for individuals with ADHD (0 of 10) or WS (1 of 11). A last analysis revealed a main effect of the school-age group on reported unawareness of COVID-19, X2(3, N = 220) = 43.7, p < 0.001: among individuals with NDCs, 15 (of 23) in the 0–5 age group, 10 (of 77) in the 6–11 age group, 6 (of 73) in the 12–15 age group, and 6 (of 47) in the over-15 age group were reported as unaware of COVID-19. In addition, 66.4% (n = 170) of individuals with NDCs could express their fears or anxieties verbally, 18.4% (n = 47) could express them only non-verbally and 15.2% (n = 39) could not express fears or anxieties in any form. Finally, to have a clearer idea about specific facilitators to implement in future times of crisis, we asked parents about wishes and specific needs they may have had during the early months of the pandemic. Parents who responded to this question primarily reported: in-home respite care, in-home or online therapy, telephone or online support, family coaching (e.g., support to manage challenging behaviours or improve transitions), more support and detailed planning from teachers and institutions, help with grocery shopping and housework, and more medical information about the risk that COVID-19 posed with respect to their child’s specific primary condition (e.g., Down syndrome or multiple disabilities).
Table 1 shows a moderate marginal R2 (40.5%) for the final multilevel analysis of anxiety in parents. The ANOVA output of effects showed no significant interaction for time, their children’s primary condition and anxiety. However, an interaction for time and anxiety was found, F(2, 803.00) = 56.05, p < 0.001. Contrasts revealed that parents experienced an increase in anxiety from Time 1 to Time 2, t(779.6) = 4.101, p < 0.005, with no significant difference between Time 2 and Time 3. Parental anxiety means are reported in Figure 1.

Figure 1. Anxiety for individuals with NDCs and their parents at the three timepoints. Time 1: “before COVID-19”; Time 2: “when the pandemic started”; Time 3: “at the time of completion of the questionnaire” – time frame between April 8 and June 27, 2020. Anxiety is measured with a 5-point Likert scale from 1 (not anxious) to 5 (very anxious). The anxiety level of individuals with NDCs was reported by their parents or caregivers. NDCs = neurodevelopmental conditions.
Figure 2 shows three continuous main positive effects on parental anxiety. Slopes revealed small effects for concern about loss of institutional support, βz = 0.14 [95%CI: 0.06–0.21], for concern about financial and economic problems, βz = 0.18 [95%CI: 0.11–0.25], and for their children with NDCs’ anxiety, βz = 0.20 [95%CI, 0.14–0.26].
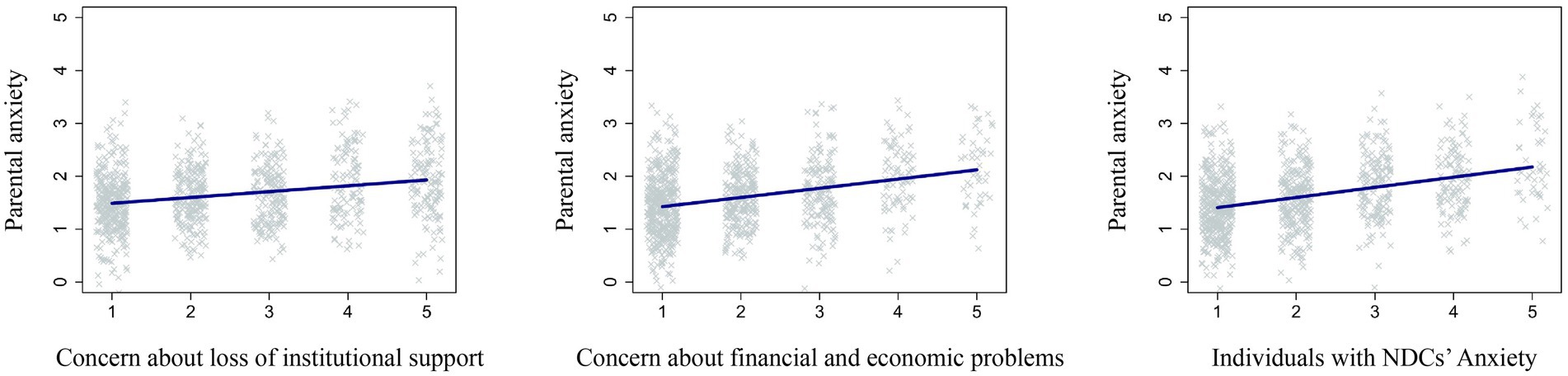
Figure 2. Continuous main positive effects of concern about loss of institutional support, concern about financial and economic problems and children with NDCs’ anxiety on parental anxiety. Anxiety and concerns are measured with a 5-point Likert scale from 1 (not anxious/not concerned at all) to 5 (very anxious/extremely concerned). NDCs = neurodevelopmental conditions.
An important descriptive finding at Time 3 revealed that approximately one third of the parents were highly (45 parents, 16.7%) or extremely (43 parents, 16%) concerned about the loss of institutional support during the early months of the pandemic. In comparison, one in six parents were highly (27 parents, 10.1%) or extremely (19 parents, 7.1%) concerned about financial and economic problems. Interestingly, two contrast analyses revealed no differences in concerns at Time 3 for financial and economic problems between parents that were eligible or ineligible for a loss-of-earnings allowance: with children under or above the age of 18, t(228) = 1.333, p < 0.184; and with children under or above the age of 20, t(228) = 1.166, p < 0.245). A three-way interaction for time, concern for their child’s occasions for social contact and interaction, and anxiety was also found, F(2, 768.61) = 5.60, p < 0.005. Slopes revealed a small effect of concern for their child’s occasions for social contact and interaction on anxiety at Time 1, βz = 0.10 [95%CI: 0.00–0.20] and Time 2, βz = 0.09 [95%CI, 0.00–0.19], whereas no effect was found for Time 3. A three-way interaction for time, child’s age group, and parental anxiety was found, F(6, 735.30) = 4.11, p < 0.001. Contrasts analyses revealed that at Time 3, parents of children aged between 12 and 15 years old experienced higher anxiety than parents of children aged from 0 to 5 years old, t(417.3) = 2.233, p < 0.05, and parents of children older than 15 years, t(413.6) = 2.112, p < 0.05. A three-way interaction was also found for time, the presence of a primary or secondary diagnosis of LD, and parental anxiety, F(2, 732.83) = 4.80, p < 0.01*. Contrasts analyses revealed no differences between parents of individuals with or without a diagnosis of LD for the same timepoints. However, descriptive results show a decrease in anxiety in parents of individuals without a primary or secondary diagnosis of LD from Time 2 (M = 2.80) to Time 3 (M = 2.57), while parents of individuals with a primary or secondary diagnosis of LD reported an increase in anxiety from Time 2 (M = 2.71) to Time 3 (M = 2.85), showing a peak of anxiety at the last timepoint. Finally, the self-reported presence of an anxiety disorder in parents was correlated with higher anxiety, t(236.5) = 3.619, p < 0.001. This effect revealed the importance of using the presence of an anxiety disorder as a confirmatory confounder variable for adjusting the model.
Table 2 shows a moderate marginal R2 (52.2%) for the final multilevel analysis of anxiety in individuals with NDCs. The ANOVA output of effects showed no significant interaction for time, primary condition and anxiety, and no significant interaction for time and anxiety, but an interaction for individual’s primary condition and anxiety was found, F(5, 741.70) = 7.10, p < 0.001. Average reported anxiety levels for individuals with NDCs are shown in Figure 1. Contrasts analyses revealed that overall anxiety was reported to be lower for individuals with a primary condition of ID compared to individuals with WS, t(858.1) = -4.413, p < 0.001, ASC, t(923.6) = -3.961, p < 0.001, ADHD, t(565.1) = -2.456, p < 0.05, or TD individuals t(900.8) = -3.226, p < 0.01; lower for individuals with DS compared to individuals with WS, t(799.7) = -3.952, p < 0.005, ASC, t(934.5) = -3.768, p < 0.005, or TD individuals, t(927.8) = -2.732, p < 0.01; and lower for TD individuals than for individuals with WS, t(863.4) = -2.881, p < 0.01 or individuals with ASC, t(932.3) = -2.249, p < 0.05 (see Figure 3).
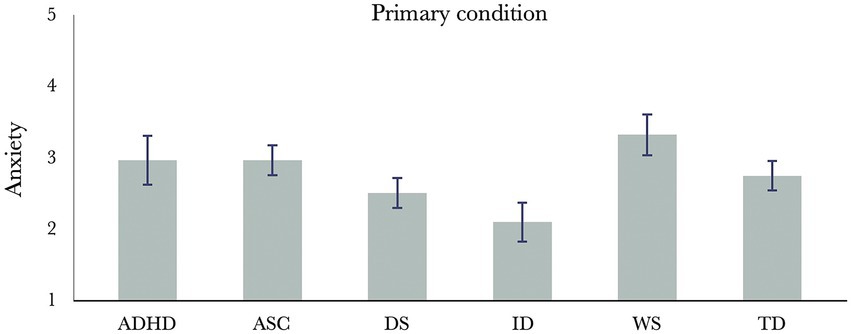
Figure 3. Anxiety levels in individuals with different primary conditions and TD siblings. Anxiety is measured with a 5-point Likert scale from 1 (not anxious) to 5 (very anxious). The anxiety level of individuals with NDCs and TD siblings was reported by their parents or caregivers. NDCs = neurodevelopmental conditions, ADHD = attention deficit disorder (with or without hyperactivity), ASC = autism spectrum condition, DS = Down syndrome, ID = intellectual disability, WS = Williams syndrome, TD = typically developing.
Figure 4 shows two continuous main positive effects on individuals with NDCs’ anxiety. Slopes revealed a small effect of concern about becoming bored, βz = 0.09 [95%CI: 0.03–0.15] and parental anxiety, βz = 0.18 [95%CI: 0.12–0.23].
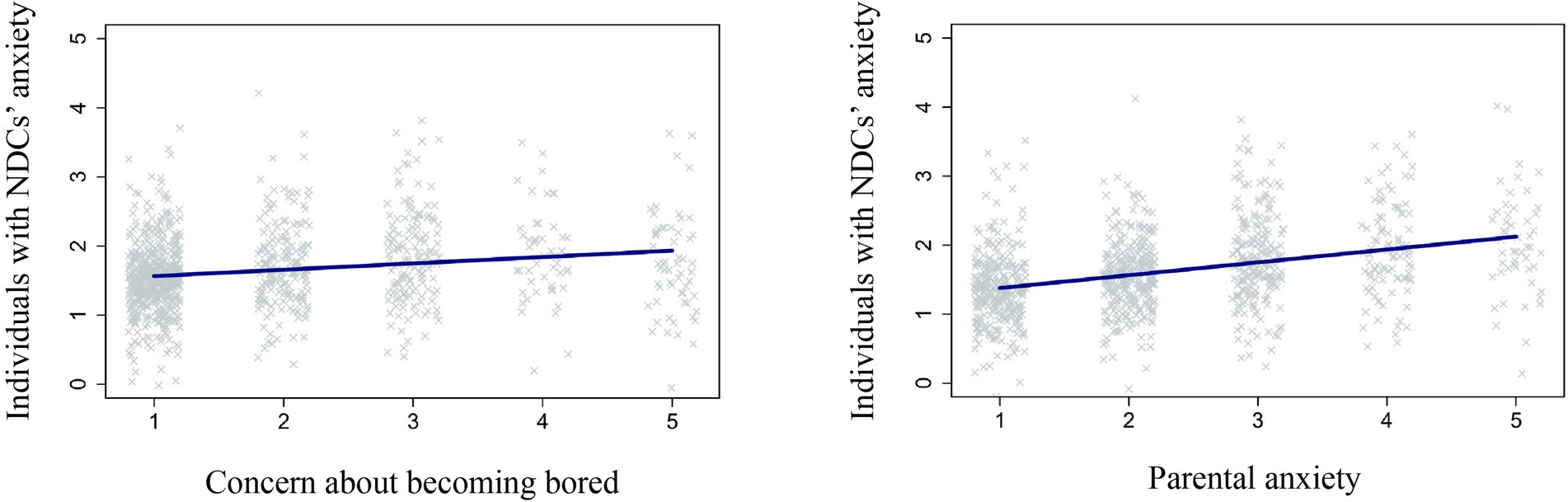
Figure 4. Continuous main positive effects of concern about becoming bored and parental anxiety on individuals with NDCs’ anxiety. Anxiety and concerns are measured with a 5-point Likert scale from 1 (not anxious/not concerned at all) to 5 (very anxious/extremely concerned). The level of anxiety and concern of individuals with NDCs was reported by their parents or caregivers. NDCs = neurodevelopmental conditions.
A previous infection with COVID-19 was correlated with higher anxiety, F(1, 353.83) = 8.50, p < 0.005. A contrast analysis revealed that individuals who were infected with COVID-19 were reported to experience higher anxiety compared to individuals who were not, t(353.8) = 2.916, p < 0.005. An interaction between concern for loss of routine and anxiety, F(1, 944.00) = 27.59, p < 0.005, and a three-way interaction for time, concern for loss of routine, and anxiety were also found, F(2, 727.91) = 3.13, p < 0.05*. Slopes revealed a small effect of concern for loss of routine on anxiety at Time 2, βz = 0.25 [95%CI: 0.16–0.33] and Time 3, βz = 0.19 [95%CI: 0.10–0.27], whereas no effect was found for Time 1. Figure 5 shows another three-way interaction for individual’s primary condition, concern for loss of routine and anxiety, F(5, 931.31) = 2.43, p < 0.05*. Slopes revealed a medium effect of concern for loss of routines on anxiety in individuals with WS, βz = 0.45 [95%CI: 0.19–0.70], and a small effect in individuals with ASC, βz = 0.24 [95%CI: 0.15–0.33] and TD individuals, βz = 0.19 [95%CI: 0.09–0.29]. A small inverse effect was found for individuals with a primary condition of ID, βz = -0.20 [95%CI: -0.41 – 0.00].
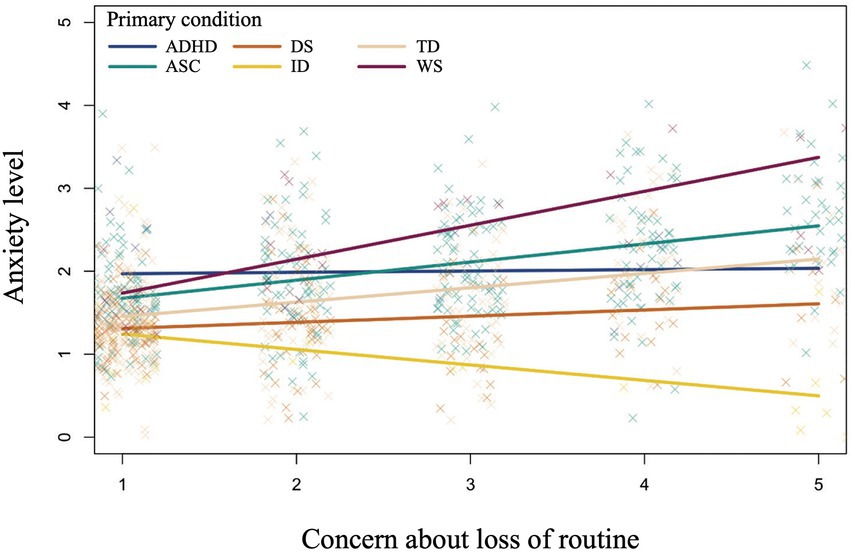
Figure 5. Three-way interaction for individual’s primary condition, concern for loss of routine and anxiety. Anxiety and concerns are measured with a 5-point Likert scale from 1 (not anxious/not concerned at all) to 5 (very anxious/extremely concerned). The level of anxiety and concern of individuals with NDCs and TD siblings was reported by their parents or caregivers. NDCs = neurodevelopmental conditions, ADHD = attention deficit disorder (with or without hyperactivity), ASC = autism spectrum condition, DS = Down syndrome, ID = intellectual disability, WS = Williams syndrome, TD = typically developing.
Another interaction was found for the ability to communicate fears or anxieties and anxiety, F(2, 212.70) = 3.41, p < 0.05*. A contrast analysis revealed that individuals able to verbally express fears and anxieties were reported to experience lower anxiety than individuals only able to express fears and anxieties nonverbally, t(207.2) = -2.043, p < 0.05, and individuals who were not able to express fears and anxieties at all, t(220.6) = -2.239, p < 0.05. An interaction was also found for the concern about not being able to meet peers and friends and anxiety, F(1, 931.71) = 6.46, p < 0.05*. Figure 6 shows a three-way interaction for individual’s primary condition, concern about not being able to meet peers and friends, and anxiety, F(5, 923.84) = 2.74, p < 0.05*. Slopes revealed a medium to large effect of concern for the ability to meet peers and friends on anxiety in individuals with WS, βz = 0.62 [95%CI: 0.31–0.93], and a small effect in TD individuals, βz = 0.11 [95%CI: 0.03–0.20]. A small to medium inverse effect was found for individuals with a primary condition of ID, βz = -0.38 [95%CI: -0.64 – -0.12].

Figure 6. Three-way interaction for individual’s primary condition, concern about not being able to meet peers and friends, and anxiety. Anxiety and concerns are measured with a 5-point Likert scale from 1 (not anxious/not concerned at all) to 5 (very anxious/extremely concerned). The level of anxiety and concern of individuals with NDCs and TD siblings was reported by their parents or caregivers. NDCs = neurodevelopmental conditions, ADHD = attention deficit disorder (with or without hyperactivity), ASC = autism spectrum condition, DS = Down syndrome, ID = intellectual disability, WS = Williams syndrome, TD = typically developing.
Finally, the reported presence of an anxiety disorder in individuals with NDCs was correlated with higher reported anxiety in these individuals, t(670.6) = 12.373, p < 0.005. This effect again revealed the importance of using the presence of an anxiety disorder as a confirmatory confounder variable for adjusting the model.
Previous research has already documented a dramatic change in the daily lives of individuals with NDCs and their families during the early months of the pandemic (Iovino et al., 2021; Lebrasseur et al., 2021; Siracusano et al., 2021; Navas et al., 2022). These studies specifically focused on vulnerabilities linked to particular health conditions, environmental barriers, and limitations in performing activities compared to the TD population.
The present study was performed in Switzerland, which ranks highly in the Public Services Index and imposed comparably less restrictive protective measures compared to its neighboring countries. Most of the individuals with NDCs in this study were attending a regular school, a special school or working in a protected environment before the pandemic, and in more than nine out of 10 cases these institutions closed. These closures resulted in a dramatic change in the daily life of these families because the support generally provided by the institution was no longer available. In the context of the ICF-10 model (World Health Organization, 2001), this change may be interpreted as an immediate and drastic environmental barrier to accessing general social support and educational services. However, the simple qualitative analysis of the individuals with NDCs’ reaction to the closure of institutions showed that 37% of the parents reported neutral or positive sentiments (e.g., happy, relieved, satisfied, good, without problems) on the part of their child, while 7% of the parents reported that their child understood or accepted the situation. Conversely, 40% parents reported negative sentiments (e.g., sad, frustrated, scared, anxious, confused, aggressive), and 15% of the parents wrote that their child did not understand the situation. Finally, 7% of the parents reported that their child had the impression (or were told by their parents) that they were on vacation (note that parents may have reported reactions that fall into multiple categories such as with “negative sentiments” and “did not understand the situation”). It is interesting to note that more than one third of the parents reported a positive reaction of their child to the closure of institutions. Further research should examine in more detail the factors that may have led to a positive reaction, with particular attention to the individual’s primary condition and potential environmental barriers experienced in their daily life before the pandemic (e.g., overwhelming social or sensorial environment, social isolation, lack of structure at school or at work, bullying). However, despite these figures, it would be wrong to recommend that these individuals should stay at home permanently as any short-term benefit is likely to be outweighed by longer-term negative impact. Indeed, some studies already reported long-term effects on the physical and mental health of individuals with NDCs in relation to aspects such as prolonged screen time, decreased physical activity, prolonged sedentary time (Theis et al., 2021), increased social isolation and loneliness (Heinze et al., 2021; Holm et al., 2021), reduced sleep quality, poorer diet and increased medication dosage (Masi et al., 2021).
It is also relevant to note that nearly one in six individuals with NDCs were reported to be unaware of the COVID-19 pandemic. Although half of these individuals were below 6 years old, the majority of the individuals reported as unaware of the pandemic older than 5 years of age presented with mild to severe ID and/or a primary condition of ASC, DS, or ID. It is important to understand potential transdiagnostic differences in receptive communication and how to more effectively explain complex life situations such as pandemics to these individuals for future times of crisis.
An important limitation of the present study is the collection of data regarding individuals with NDCs’ concerns and anxieties through parental report. Caution must therefore be exercised when interpreting our analyses and results. Indeed, previous studies (e.g., Lester et al., 2009) showed that parents with high levels of anxiety may exhibit more negative interpretative biases than less anxious parents. In this view, parents with high levels of anxiety may have reported a higher level of anxiety and concern for their child than the child actually experienced. While parental reports were employed here due to the importance of launching the survey quickly, future research should also include responses directly from individuals with NDCs. Another limitation is that anxiety levels “before COVID-19″ and “when the pandemic started” were retrospectively reported by parents at the time of completion of the questionnaire, posing a potential risk of memory bias. In addition, the questionnaire did not present specific dates of reference for these two timepoints, so parents may have presented a marginal error in the exact placement of the timepoints in the timeline of events. Finally, it is also important to note that anxiety was assessed with a Likert scale based on anxiety levels from 1 “not anxious” to 5 “very anxious” rather than with a specific and validated psychometric tool.
Nevertheless, in line with previous research (Chafouleas and Iovino, 2020; Willner et al., 2020), our results show that parents reported to experience an increase in anxiety when the pandemic started. The multilevel model revealed no differences in parental anxiety in relation to the primary condition of their child, suggesting that all parents experienced a comparable increase in anxiety. Interestingly, the multilevel analysis for individuals with NDCs revealed a different pattern. First and foremost, no effect of time on reported anxiety was found. This result suggests that parents did not perceive increased anxiety in their children when the pandemic started. These results are in line with our other findings and those of others, reporting that individuals with NDCs may have experienced positive effects from staying at home, such as reduced stress, more and improved sleep, reduced social pressure, more time for relaxation, play or hobbies, improved affect (Bruining et al., 2021), or better employment opportunities with home-based work (Schur et al., 2020). Nevertheless, studies are beginning to report evidence of increased mental health concerns in children and adolescents with NDCs as the pandemic has endured (for a review, see Samji et al., 2022). It is thus possible that the present study failed to show an increase in anxiety because it focused only on the early months of the pandemic. Another possible explanation for this lack of effect is that individuals with NDCs may find their normal daily lives to be relatively stressful and were relieved to be spending time at home with the family and without external pressures or environmental barriers, particularly if they were unaware of the root cause of the changes to their daily lives. Second, some primary conditions such as ASC and WS were strongly correlated with higher reported overall anxiety. This effect is consistent with previous research, indicating that individuals presenting with these primary conditions experience higher overall anxiety compared to the TD population (Dankner and Dykens, 2012; Rodgers et al., 2012). However, it is important to note that in contrast to previous studies reporting higher anxiety in individuals with ID in comparison to the TD population (Emerson and Hatton, 2007; Reardon et al., 2015), we found that individuals with a primary condition of ID were reported to be the least anxious group. Finally, it is also relevant to mention that the TD individuals were reported to experience higher anxiety than individuals with DS or a primary condition of ID. These effects may be due to the relative lack of awareness regarding COVID-19 that has been reported by parents for individuals with DS or ID as a primary condition. Altogether these results suggest that the primary condition of individuals with NDCs may prove to be a strong predictive factor of everyday anxiety. Further research should investigate the potential effects of the individual’s primary condition, presence and severity of ID and awareness of the COVID-19 pandemic on anxiety.
In line with our initial assumption, one of the most anxiety-provoking factors for parents concerned the loss of institutional support, and our analyses revealed that about one-third of parents were highly to extremely concerned about this environmental barrier. Many parents may have found themselves in the situation of having to manage multiple extra roles and tasks in their daily lives because institutional support was no longer available during the first months of the pandemic. In addition to caring for their child with NDCs, parents may have potentially had to work (at their workplace or from home), find an appropriate method to explain the situation to their child, take care of their child’s special educational needs, disabilities, or health conditions, support and motivate their child with distance learning, learn how to use new technology tools for work and distance learning, and teach them to their child. Some of the parents’ testimonies may provide some information about this type of environmental barrier. One parent reported: “Suddenly we lost all the support we had. Teaching the three kids at home and knowing you cannot breathe for a minute is very intense. We as parents reached our limits. We felt really alone.” Another parent wrote: “We would need extra care sometimes. Right now, I am a teacher, mom-wife, crisis manager and sometimes 24 h a day. Sometimes the days are too long! Taking a break from the daily grind is very difficult right now.”
The second most anxiety-provoking environmental barrier for parents was related to financial and economic problems incurred due to the pandemic, since approximately one in six parents experienced high to extreme concern about this environmental barrier. The loss-of-earnings allowance for families of children with NDCs up to 12 years of age and its extension to a wider population 1 month later was a facilitator intended to support these families on a daily basis in Switzerland. However, parents of children eligible for a loss-of-earnings allowance did not report less concern about financial and economic problems as compared to ineligible parents. Some parents may also have found specific and singular barriers in relation to financial and economic problems. For instance, one mother reported: “I work as a nurse and would be directly involved with COVID-19 patients. For fear of infection, which I could transfer to my child, I am not working at the moment. So, we have less money. It is financially problematic!.” Further investigation is needed to understand possible environmental barriers with respect to both the communication of information about the availability of loss-of-earnings allowances to eligible families and the procedures that must be followed to obtain them.
Another important result that appeared in both models is the bidirectional relation between parental anxiety and reported individuals with NDCs’ anxiety. While not knowing the causality of this relation, it may prove interesting to explore this phenomenon through the Interpersonal Emotion Transfer theory. The theory suggests that anxiety can serve both a comfort-seeking function that leads to empathic worry, and an alerting function to activate a defensive reaction to potential threats (Parkinson and Simons, 2012). This mechanism can be partially explained by the process of emotional contagion, which can be defined as an automatic synchronization of expressions, vocalizations, postures, and movements between individuals with the end consequence of emotional convergence (Hatfield and Cacioppo, 1992). In this view, parents and children may have converged emotionally in cycles of mutual influence to seek comfort through empathic worry and alert on COVID-19-related dangers. However, since the anxiety levels of the individuals with NDCs are reported by parents, another possible mechanism that could explain this relationship is the potential influence of parents’ negative interpretation biases (Lester et al., 2009). According to this view, parents experiencing increased anxiety during the pandemic may have tended to interpret their children’s anxiety from a more pessimistic viewpoint.
Parents also reported experiencing anxiety due to concern for the child’s occasions for social contact and interaction for retrospective Times 1 and 2, but this effect was not present at Time 3. The lack of effect at Time 3 may be due to several factors, such as the increase of parental concerns for other environmental barriers (e.g., loss of institutional support or financial and economic problems), the fact that individuals with NDCs may have been able to adapt and maintain social contact and interaction at a distance, or that the reduced social contact and interaction did not upset individuals with NDCs during the pandemic as much as the parents had initially feared. Interestingly, results show that parents of children aged 12 to 15 were the group most affected by anxiety. This result may be explained by the fact that adolescents are much more sensitive to peer acceptance and approval than are children or adults (Somerville, 2013; Foulkes and Blakemore, 2016). From this perspective, parents may have been confronted with the child’s specific need for social connections, with potential consequences such as a quest for greater autonomy, more time spent out of home and more social contacts (with related higher risk of infection). In addition, alongside the burdens of childcare and distance learning, parents of individuals in this age-range may have been confronted with specific additional health risks, barriers, and special needs for their child. For example, in comparison to younger children, older children showed more probability to develop symptoms such as respiratory tract infection in relation to the COVID-19 pandemic (for a review see Ludvigsson, 2020). Furthermore, the presence of a primary or secondary diagnosis of LD may have additionally impacted parental anxiety. A study conducted by Bol (2020) concerning TD students reported that only between 50 and 70% of parents (depending on their level of education) felt able to help their child with primary school homework during the pandemic, and that this percentage varied between 40 and 75% for parents whose children were in secondary school. As such, if many parents with TD children already felt unable to help with distance learning in mainstream education, for parents of children diagnosed with LD this task may have been even more challenging. In support of this hypothesis, our descriptive analysis reveals that, unlike all other parents who reported a decrease in anxiety after Time 2, parents of children with a specific primary or secondary diagnosis of LD reported a peak of anxiety at Time 3. This effect could be partially explained by the need of individualized and specific teaching strategies, materials, and instructions for these students to follow the curriculum (Gersten et al., 2001; Jitendra and Star, 2011; Mason and Hedin, 2011).
Interestingly, anxiety and anxiety-provoking concerns reported by parents showed that the most anxiety-provoking factor for children was their concern about becoming bored. Eastwood et al. (2012, 482) defined boredom as “the aversive experience of wanting, but being unable to engage in satisfying activity.” In the early months of the pandemic, it is possible that individuals with NDCs wanted but were unable to engage in satisfactory activities such as school, work, recreational activities, or social interactions. From this perspective, parents may have interpreted the inability to engage in satisfactory activities as the major source of concern and anxiety for their children. In addition, Boylan et al. (2021, para. 3) suggested that “the likelihood of people experiencing boredom during the COVID-19 pandemic should reflect, in part, high perceived costs of adhering to public-health rules in comparison to the perceived benefits of protecting the community from COVID-19.” In this regard, more than half of individuals with NDCs were reported to have mild to severe ID and one in six individuals with NDCs was reported to be unaware of COVID-19. These results suggest that a substantial subset of individuals with NDCs may not have understood the full rationale behind the measures implemented to address the pandemic, perceiving only the costs of adhering to public-health rules (e.g., respect physical distance, wear a mask, stay at home without normal daily life occupations and recreational activities), but not the benefits. It is relevant to note that individuals presenting with mild to severe ID may need specific environmental facilitators (e.g., augmentative and alternative communication) to express and understand complex life situations such as the COVID-19 pandemic (for a review of augmentative and alternative communication in individuals with ID, see Wilkinson and Hennig, 2007). Therefore, the inability to engage in satisfying activities for an undetermined time and difficulties in understanding the reasons for this inability may partially explain the anxiety reported in this population. The following testimonials reveal some of the difficulties that parents may have encountered in this domain: “My son does not understand the severity of the disease, the few times he has been hospitalized he was untreatable and unmanageable”; “It is very difficult to ensure that our child respects social distancing. He does not understand why you are not allowed to hold hands with anyone anymore.” In addition to difficulties in understanding the situation, limitations in verbally expressing fears and anxieties may have additionally affected the ability of individuals with NDCs to socially regulate emotions, preventing proper adherence to rules and their benefit with respect to the pandemic. In this regard, the link between language, emotional understanding, and emotional regulation has been widely reported in literature (Kopp, 1989, 1992; Eisenberg et al., 2005; Harris et al., 2005; Cole et al., 2010). One parent reported his own experience about this specific limitation: “Our child is non-verbal, so he cannot express his feelings well, but we feel that he is more irritated, and his mood is less stable.” Finally, previous COVID-19 infection also seems to have had an influence on anxiety of individuals with NDCs, but further investigation is needed to understand how variables such as the family’s reaction, degree of illness, or hospitalization may have further affected anxiety in these individuals.
While not meeting the strict threshold set for the multilevel analysis, two additional anxiety-provoking factors with a strong transdiagnostic difference were found. These results must be considered with caution but may prove noteworthy for future research on the psychological effects and specific strengths and needs of individuals with NDCs in times of crisis and social estrangement. Concerns about loss of routine for individuals with ASC in times of pandemic have been previously investigated (Ameis et al., 2020; Courtenay and Perera, 2020; White et al., 2021). However, results show that the impact of this concern on anxiety does not appear to be limited to individuals with ASC, but it is also present in individuals with WS and TD individuals. Interestingly, individuals with a primary condition of ID may have experienced the opposite effect: counter-intuitively, the more these individuals were reported to be concerned about the loss of routine, the less they were reported to be anxious. To better understand these effects, future research should investigate what changes in daily routine activities (e.g., school, therapies, sports, entertainment) may have impacted concerns and anxiety levels over time and what type of needs these activities provided to the individual (e.g., physical well-being, recreation, socialization, prediction of the environment). Finally, we also found higher anxiety in individuals with WS and TD in relation to the concern about not being able to meet peers and friends. As before, individuals with a primary condition of ID showed a somewhat counter-intuitive opposite effect, in that the more they were concerned about meeting peers and friends, the less anxious they were. Again, to better understand the effect for this type of concern it would be interesting to investigate potential transdiagnostic differences concerning the need for socialization, the meaning of friendship, or the need of support from friends and peers during difficult times. About the inverse effect found for both types of concerns in individuals with a primary condition of ID, it may prove interesting to investigate whether there is a potential difference in the behavioral effect of anxiety in this population (e.g., propensity to react with internalizing symptoms such as depression instead of physical tension or hyperactivity). From this perspective, if individuals with a primary condition of ID were to show a tendency to react to anxiety with internalizing symptoms, they may have verbalized their concerns or asked questions about these types of concerns to their parents, but parents may have perceived depression or sadness instead of anxiety.
It is important to consider the implications for policy and practice with the goal of better meeting the educational needs and enhancing overall well-being in families of individuals with NDCs. First, it is important to highlight that the availability and accessibility of support services for parents of people with NDCs are fundamental factors contributing to their well-being. The abrupt disruption of these support services may be seen as a strong source of anxiety for parents, and future policymaking should focus on how to provide continuity of support – remotely or on-site – to these families in challenging times. In the present study, parents specifically highlighted needs such as in-home respite care, help with grocery shopping and housework, in-home or online therapy, telephone or online support, family coaching, more support and detailed planning from teachers and institutions. With this in mind, a strong synergy and sharing of practices and information between schools, therapy centers and families may be seen as an important protective measure empowering all the relevant actors around and including the individual with NDCs (for a review on the relationship between families and schools during the COVID-19 pandemic, see Carrión-Martínez et al., 2021).
Second, it is important to understand how to best adapt specific tools and software to improve distance learning, social sharing, or homework supervision for some of the individuals with NDCs that may find it difficult to use anything commercially available. To this end, it may be useful to closely examine the specific needs of each individual with NDCs within the ICF-10 model. Rather than a general list of needs, supports, and goals, this model may allow for precise contextual support for the individual, such as the specific adaptations needed to make distance learning accessible at home. Some studies already started to review the advantages, disadvantages, and ways to improve distance learning for specific sub-groups and developmental ages of students with NDCs (e.g., Buchnat and Wojciechowska, 2020; Petretto et al., 2021; Supratiwi et al., 2021). Several guidelines have also been created to help schools and families improve the quality of distance learning practices for special education (e.g., Fajardo Bravo et al., 2020; Hanover Research, 2020). Policymakers should consult these studies and guidelines to improve the quality of public education services.
Third, given that more than one third of the parents indicated their child responded positively to the closure of institutions, future research should examine the extent to which the daily living environments (e.g., schools, workplaces) are appropriately adapted to the needs of the individual and the extent to which these individuals enjoy their daily activities. Trying to better evaluate life satisfaction and quality of life in the context of school or work in individuals with NDCs, for example through questionnaires or interviews, could help to determine whether these individuals find their daily life too stressful to be pleasant.
Fourth, the present study showed how particular health conditions (e.g., primary condition) or personal factors (e.g., ability to express fears and anxieties, age) may have differential impacts on anxiety and specific concerns. For instance, parents of children aged between 12 and 15 years old reported higher overall anxiety, individuals with WS were reported to experience higher anxiety in relation to concerns for the ability to meet peers and friends, and individuals not able to express fears and anxieties were reported to experience higher overall anxiety. In the future, policymakers and institutions may consider these kinds of potential differences among individuals with NDCs in order to provide proper support for specific needs in particular sub-groups and their families.
Fifth, it may be worthwhile to develop a national questionnaire targeted at individuals with NDCs to self-report well-being, quality of life and particular needs for both ordinary times and in anticipation of future times of crisis. This type of approach may allow for a more self-determined life and may help to avoid parental biases in data collection. Several validated psychometric tools and current research in these topics may provide the basis for such questionnaires (e.g., Schalock et al., 2002; Cummins et al., 2011; Verdugo et al., 2020).
Sixth, an important point for future investigation is the long-term effect of the pandemic on individuals with NDCs, and particularly the effect of physical distancing on their social development and social skills. Focused research would help in future times of crisis to achieve the delicate balance between applying measures to protect the health of individuals and possible long-term risks to freedom and liberty linked to too many restrictions (e.g., loss of social skills, agoraphobia, social anxiety). Policymakers could certainly benefit from research establishing ethical positions concerning distance learning and physical distancing.
Finally, it is crucial to highlight the importance of associations and umbrella organizations that defend the rights of individuals with NDCs and help families with specific needs to be heard. In this perspective, a strong synergy with these kinds of services may prove to be a virtuous circle in both ordinary and future challenging times. In Switzerland’s case, these umbrella organizations include “Agile.ch” and “Inclusion Handicap.” Creating a strong synergy between government, families, and individuals with NDCs may help everyone to be better prepared in future challenging times.
Switzerland is well known for the quality of its public services; however, the governmental measures taken to combat the spread of the COVID-19 pandemic drastically reduced institutional support for these families, leaving a substantial number of them “highly” to “extremely” concerned. The present study, framed within the ICF-10 model, revealed the extent to which measures implemented to address the pandemic may have created environmental barriers, limited activity, and restricted participation of individuals with NDCs and their families in Switzerland. In this light, and despite government efforts to provide specific facilitators, additional measures appear to have been needed to reduce anxiety and environmental barriers in the daily lives of families with children with NDCs during the pandemic. Importantly, however, whereas an increase in anxiety was reported for parents during the first months of the pandemic, individuals with NDCs were not perceived as more anxious than before COVID-19. Indeed, more than one third of them reacted positively to the closure of institutions. Importantly, our results suggest that in addition to personal factors and environmental barriers, health conditions such as the individual’s primary condition may have contributed to different patterns of anxiety and anxiety-related concerns in individuals with NDCs during the pandemic. To conclude, we presented a series of reflections and practical suggestions that could help guide policy makers in potential future periods of crisis, social estrangement, and distance learning.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://psyarxiv.com/rtswa/.
The studies involving human participants were reviewed and approved by Ethics Commission of UniDistance Suisse. The patients/participants provided their written informed consent to participate in this study.
AS and DD designed and directed the project. AP coordinated all practical aspects of survey creation and data collection. NT, LS, GP, and AS contributed to the translation of the survey and data collection. MT created the website and contributed to data collection and data pre-processing. BM performed the multilevel analyses and contributed to the interpretation and writing of the results. GP performed the other statistical analyses and wrote the first draft of the manuscript. PB and PL contributed to the creation and translation of the survey and manuscript preparation. All authors actively contributed to recruitment, manuscript revision, read, and approved the submitted version.
This work was supported by the Research Funds of Unidistance Suisse, the European Federation of Williams Syndrome association, and the Swiss National Science Foundation (PP00P1_176722 for AS).
We would like to thank all the families who donated their time to participate in this study. Special thanks go to all the associations and institutions that shared the study with their members.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2023.951970/full#supplementary-material
Ameis, S. H., Lai, M.-C., Mulsant, B. H., and Szatmari, P. (2020). Coping, fostering resilience, and driving care innovation for autistic people and their families during the COVID-19 pandemic and beyond. Mol. Autism. 11:61. doi: 10.1186/s13229-020-00365-y
Bates, D., Mächler, M., Bolker, B., and Walker, S. (2015). Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48. doi: 10.3929/ethz-b-000105397
Benjamin, D. J., Berger, J. O., Johannesson, M., Nosek, B. A., Wagenmakers, E.-J., Berk, R., et al. (2018). Redefine statistical significance. Nat. Hum. Behav. 2, 6–10. doi: 10.1038/s41562-017-0189-z
Bol, T. (2020). Inequality in homeschooling during the Corona crisis in the Netherlands. First results from the LISS Panel. SocArXiv. doi: 10.31235/osf.io/hf32q
Boylan, J., Seli, P., Scholer, A. A., and Danckert, J. (2021). Boredom in the COVID-19 pandemic: trait boredom proneness, the desire to act, and rule-breaking. Pers. Individ. Differ. 171:110387. doi: 10.1016/j.paid.2020.110387
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Bruining, H., Bartels, M., Polderman, T. J. C., and Popma, A. (2021). COVID-19 and child and adolescent psychiatry: an unexpected blessing for part of our population? Eur. Child Adolesc. Psychiatry 30, 1139–1140. doi: 10.1007/s00787-020-01578-5
Buchnat, M., and Wojciechowska, A. (2020). Online education of students with mild intellectual disability and autism spectrum disorder during the COVID-19 pandemic. Int. Cont. Spec. Pedagog. 29, 149–171. doi: 10.14746/ikps.2020.29.07
Cacioppo, M., Bouvier, S., Bailly, R., Houx, L., Lempereur, M., Mensah-Gourmel, J., et al. (2021). Emerging health challenges for children with physical disabilities and their parents during the COVID-19 pandemic: the ECHO French survey. An. Phys. Rehabil. Med. 64:101429. doi: 10.1016/j.rehab.2020.08.001
Carrión-Martínez, J. J., Pinel-Martínez, C., Pérez-Esteban, M. D., and Román-Sánchez, I. M. (2021). Family and school relationship during COVID-19 pandemic: a systematic review. Int. J. Environ. Res. Public Health 18:11710. doi: 10.3390/ijerph182111710
Chafouleas, S. M., and Iovino, E. A. (2020). Initial impact of covid-19 on the well-being of caregivers of children with and without disabilities. University of Connecticut’s Institute for Collaboration on Health. Available at: https://csch.uconn.edu/wp-content/uploads/sites/2206/2020/07/CSCH-Brief-COVID-19-Impact-on-Caregivers-July-2020.pdf (Accessed May 06, 2021).
Cheng, S., Yang, Y., and Deng, M. (2021). Psychological stress and perceived school success among parents of children with developmental disabilities during the COVID-19 pandemic. J. Autism Dev. Disord. 52, 3194–3201. doi: 10.1007/s10803-021-05209-z
Cole, P. M., Armstrong, L. M., and Pemberton, C. K. (2010). “The role of language in the development of emotion regulation” in Child development at the intersection of emotion and cognition. Human brain development (Washington, DC, US: American Psychological Association), 59–77. doi: 10.1037/12059-004
Colizzi, M., Sironi, E., Antonini, F., Ciceri, M. L., Bovo, C., and Zoccante, L. (2020). Psychosocial and behavioral impact of COVID-19 in autism spectrum disorder: an online parent survey. Brain Sci. 10:341. doi: 10.3390/brainsci10060341
Courtenay, K., and Perera, B. (2020). COVID-19 and people with intellectual disability: impacts of a pandemic. Ir. J. Psychol. Med. 37, 231–236. doi: 10.1017/ipm.2020.45
Croft, S., and Fraser, S. (2021). A scoping review of barriers and facilitators affecting the lives of people with disabilities during COVID-19. Front. Rehabil. Sci. 2:784450. doi: 10.3389/fresc.2021.784450
Cummins, R. A., Lau, A. L. D., Davey, G., and McGillivray, J. (2011). “Measuring subjective wellbeing: the personal wellbeing index–intellectual disability” in Enhancing the quality of life of people with intellectual disabilities: From theory to practice. ed. R. Kober (Dordrecht: Springer Netherlands), 33–46.
Dankner, N., and Dykens, E. M. (2012). “Chapter three – anxiety in intellectual disabilities: challenges and next steps” in International review of research in developmental disabilities. ed. R. M. Hodapp (Cambridge, Massachusetts, USA: Academic Press), 57–83.
Doody, O., and Keenan, P. M. (2021). The reported effects of the COVID-19 pandemic on people with intellectual disability and their carers: a scoping review. Ann. Med. 53, 786–804. doi: 10.1080/07853890.2021.1922743
Dubey, S., Biswas, P., Ghosh, R., Chatterjee, S., Dubey, M. J., Chatterjee, S., et al. (2020). Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 14, 779–788. doi: 10.1016/j.dsx.2020.05.035
Dukes, D., Van Herwegen, J., Alessandi, M., Alnemary, F., Amani Rad, J., Banta Lavenex, P., et al. (2021). Introducing the COVID-19 crisis special education needs coping survey. PsyArXiv. doi: 10.31234/osf.io/rtswa
Eastwood, J. D., Frischen, A., Fenske, M. J., and Smilek, D. (2012). The unengaged mind: defining boredom in terms of attention. Perspect. Psychol. Sci. 7, 482–495. doi: 10.1177/1745691612456044
Eisenberg, N., Sadovsky, A., and Spinrad, T. L. (2005). Associations of emotion-related regulation with language skills, emotion knowledge, and academic outcomes. New Dir. Child Adolesc. Dev. 2005, 109–118. doi: 10.1002/cd.143
Emerson, E., and Hatton, C. (2007). Mental health of children and adolescents with intellectual disabilities in Britain. Br. J. Psychiatry 191, 493–499. doi: 10.1192/bjp.bp.107.038729
Fajardo Bravo, I., Gomez-Merino, N., Jury, M., Klang, N., Lüke, T., Mannik, S., et al. (2020). Guidance for the inclusion of students with special educational needs for online learning. European Association for Research on Learning and Instruction. Available at: https://earli.org/sites/default/files/2020-11/EARLI%20guidelines_COVID%20online%20inclusion.pdf [Accessed August 29, 2022].
Federal Council (2020a). Coronavirus: extension du droit à l’allocation pour perte de gain aux cas de rigueur. Swiss Confederation. Available at: https://www.admin.ch/gov/fr/accueil/documentation/communiques.msg-id-78813.html#:~:text=Allocation%20pour%20perte%20de%20gain%20en%20faveur%20des%20parents,enfants%20en%20situation%20de%20handicap&text=Le%20droit%20des%20parents%20qui,parents%20d'enfants%20sans%20handicap (Accessed May 06, 2021).
Federal Council (2020b). Coronavirus: le Conseil fédéral qualifie la situation de « situation extraordinaire » et renforce les mesures. Swiss Confederation. Available at: https://www.admin.ch/gov/fr/accueil/documentation/communiques.msg-id-78454.html (Accessed May 06, 2021).
Federal Council (2020c). Le Conseil fédéral renforce les mesures contre le coronavirus pour protéger la santé de la population et soutient les secteurs touchés. Swiss Confederation. Available at: https://www.admin.ch/gov/fr/accueil/documentation/communiques.msg-id-78437.html (Accessed May 06, 2021).
Federal Council (2020d). Ordonnance sur les mesures en cas de pertes de gain en lien avec le coronavirus (COVID-19). Swiss Confederation. Available at: https://www.admin.ch/opc/fr/classified-compilation/20200841/index.html (Accessed May 06, 2021).
Federal Office for Disability Equality (2020). Recommandations du BFEH relatives à la publication d’informations sur le nouveau coronavirus en langue facile à lire et en langue des signes. Swiss Confederation. Available at: https://www.edi.admin.ch/dam/edi/fr/dokumente/gleichstellung/E-Accessibility/empfehlungencoronalsgs.pdf.download.pdf/Recommandations%20du%20BFEH%20relatives%20%C3%A0%20la%20publication%20d%E2%80%99informations%20sur%20le%20nouveau%20coronavirus%20en%20langue%20facile%20%C3%A0%20lire%20et%20en%20langue%20des%20signes.pdf (Accessed May 25, 2021).
Fitzmaurice, G. M., Laird, N. M., and Ware, J. H. (2012). Applied longitudinal analysis. Hoboken N. J.: John Wiley & Sons.
Foulkes, L., and Blakemore, S.-J. (2016). Is there heightened sensitivity to social reward in adolescence? Curr. Opin. Neurobiol. 40, 81–85. doi: 10.1016/j.conb.2016.06.016
Furar, E., Wang, F., Durocher, J. S., Ahn, Y. A., Memis, I., Cavalcante, L., et al. (2022). The impact of COVID-19 on individuals with ASD in the US: parent perspectives on social and support concerns. PLoS One 17, e0270845–e0270819. doi: 10.1371/journal.pone.0270845
Gersten, R., Fuchs, L. S., Williams, J. P., and Baker, S. (2001). Teaching reading comprehension strategies to students with learning disabilities: a review of research. Rev. Educ. Res. 71, 279–320. doi: 10.3102/00346543071002279
Greenway, C. W., and Eaton-Thomas, K. (2020). Parent experiences of home-schooling children with special educational needs or disabilities during the coronavirus pandemic. Br. J. Spec. Educ. 47, 510–535. doi: 10.1111/1467-8578.12341
Hanover Research (2020). Best practices for addressing challenges in special education in distance learning. Available at: https://wasa-oly.org/WASA/images/WASA/6.0%20Resources/Hanover/Best%20Practices%20for%20Special%20Education%20in%20Distance%20Learning.pdf [Accessed August 29, 2022].
Harris, P. L., Rosnay, M. D., and Pons, F. (2005). Language and children’s understanding of mental states. Curr. Dir. Psychol. Sci. 14, 69–73. doi: 10.1111/j.0963-7214.2005.00337.x
Hatfield, E., and Cacioppo, J. T. (1992). “Primitive emotional contagion” in Emotion and social behavior thousand oaks, CA (US: SAGE Publications), 151–177.
Heinze, N., Hussain, S. F., Castle, C. L., Godier-McBard, L. R., Kempapidis, T., and Gomes, R. S. M. (2021). The long-term impact of the COVID-19 pandemic on loneliness in people living with disability and visual impairment. Front. Public Health 9:738304. doi: 10.3389/fpubh.2021.738304
Holm, M. E., Sainio, P., Parikka, S., and Koskinen, S. (2021). The effects of the COVID-19 pandemic on the psychosocial well-being of people with disabilities. Disabil. Health J. 15:101224. doi: 10.1016/j.dhjo.2021.101224
Iovino, E. A., Caemmerer, J., and Chafouleas, S. M. (2021). Psychological distress and burden among family caregivers of children with and without developmental disabilities six months into the COVID-19 pandemic. Res. Dev. Disabil. 114:103983. doi: 10.1016/j.ridd.2021.103983
Jitendra, A. K., and Star, J. R. (2011). Meeting the needs of students with learning disabilities in inclusive mathematics classrooms: the role of schema-based instruction on mathematical problem-solving. Theory Pract. 50, 12–19. doi: 10.1080/00405841.2011.534912
Kopp, C. B. (1989). Regulation of distress and negative emotions: a developmental view. Dev. Psychol. 25, 343–354. doi: 10.1037/0012-1649.25.3.343
Kopp, C. B. (1992). “Emotional distress and control in young children” in Emotion and its regulation in early development (San Francisco, CA, US: Jossey-Bass), 41–56.
Kuznetsova, A., Brockhoff, P. B., and Christensen, R. H. B. (2017). lmerTest package: tests in linear mixed effects models. J. Stat. Softw. 82, 1–26. doi: 10.18637/jss.v082.i13
Lebrasseur, A., Fortin-Bédard, N., Lettre, J., Bussières, E.-L., Best, K., Boucher, N., et al. (2021). Impact of COVID-19 on people with physical disabilities: a rapid review. Disabil. Health J. 14:101014. doi: 10.1016/j.dhjo.2020.101014
Lee, V., Albaum, C., Tablon Modica, P., Ahmad, F., Gorter, J. W., Khanlou, N., et al. (2021). The impact of COVID-19 on the mental health and wellbeing of caregivers of autistic children and youth: a scoping review. Autism Res. 14, 2477–2494. doi: 10.1002/aur.2616
Lester, K. J., Field, A. P., Oliver, S., and Cartwright-Hatton, S. (2009). Do anxious parents interpretive biases towards threat extend into their child’s environment? Behav. Res. Ther. 47, 170–174. doi: 10.1016/j.brat.2008.11.005
Liu, C. H., Zhang, E., Wong, G. T. F., Hyun, S., and Hahm, H. C. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for U.S. young adult mental health. Psychiatry Res. 290:113172. doi: 10.1016/j.psychres.2020.113172
Ludvigsson, J. F. (2020). Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 109, 1088–1095. doi: 10.1111/apa.15270
Masi, A., Mendoza Diaz, A., Tully, L., Azim, S. I., Woolfenden, S., Efron, D., et al. (2021). Impact of the COVID-19 pandemic on the well-being of children with neurodevelopmental disabilities and their parents. J. Paediatr. Child Health 57, 631–636. doi: 10.1111/jpc.15285
Mason, L. H., and Hedin, L. R. (2011). Reading science text: challenges for students with learning disabilities and considerations for teachers. Learn. Disabil. Res. Pract. 26, 214–222. doi: 10.1111/j.1540-5826.2011.00342.x
Miranda, D. M. D., Athanasio, B. D. S., Oliveira, A. C. S., and Simoes-e-Silva, A. C. (2020). How is COVID-19 pandemic impacting mental health of children and adolescents? Int. J. Disaster Risk Reduct. 51:101845. doi: 10.1016/j.ijdrr.2020.101845
Navas, P., Verdugo, M. Á., Martínez, S., Amor, A. M., Crespo, M., and Deliu, M. M. (2022). Impact of COVID-19 on the burden of care of families of people with intellectual and developmental disabilities. J. Appl. Res. Intellect. Disabil. 35, 577–586. doi: 10.1111/jar.12969
Our World in Data (2022). COVID-19 stringency index. Our World in Data. Available at: https://ourworldindata.org/grapher/covid-stringency-index?time=2022-01-09®ion=Europe&country=~CHE.
Panjwani, A. A., Bailey, R. L., and Kelleher, B. L. (2021). COVID-19 and behaviors in children with autism spectrum disorder: disparities by income and food security status. Res. Dev. Disabil. 115:104002. doi: 10.1016/j.ridd.2021.104002
Parkinson, B., and Simons, G. (2012). Worry spreads: interpersonal transfer of problem-related anxiety. Cognit. Emot. 26, 462–479. doi: 10.1080/02699931.2011.651101
Patel, V., Saxena, S., Lund, C., Thornicroft, G., Baingana, F., Bolton, P., et al. (2018). The lancet commission on global mental health and sustainable development. Lancet 392, 1553–1598. doi: 10.1016/S0140-6736(18)31612-X
Perera, B., Audi, S., Solomou, S., Courtenay, K., and Ramsay, H. (2020). Mental and physical health conditions in people with intellectual disabilities: comparing local and national data. Br. J. Learn. Disabil. 48, 19–27. doi: 10.1111/bld.12304
Petretto, D. R., Carta, S. M., Cataudella, S., Masala, I., Mascia, M. L., Penna, M. P., et al. (2021). The use of distance learning and E-learning in students with learning disabilities: a review on the effects and some hint of analysis on the use during COVID-19 outbreak. Clin. Pract. Epidemiol. Ment. Health 17, 92–102. doi: 10.2174/1745017902117010092
Pettinicchio, D., Maroto, M., Chai, L., and Lukk, M. (2021). Findings from an online survey on the mental health effects of COVID-19 on Canadians with disabilities and chronic health conditions. Disabil. Health J. 14:101085. doi: 10.1016/j.dhjo.2021.101085
R Core Team (2020). R: A language and environment for statistical computing. Available at: https://www.R-project.org/ (Accessed October 03, 2022).
Reardon, T. C., Gray, K. M., and Melvin, G. A. (2015). Anxiety disorders in children and adolescents with intellectual disability: prevalence and assessment. Res. Dev. Disabil. 36, 175–190. doi: 10.1016/j.ridd.2014.10.007
Redquest, B. K., Tint, A., Ries, H., and Lunsky, Y. (2021). Exploring the experiences of siblings of adults with intellectual/developmental disabilities during the COVID-19 pandemic. J. Intellect. Disabil. Res. 65, 1–10. doi: 10.1111/jir.12793
Rights, J. D., and Sterba, S. K. (2019). Quantifying explained variance in multilevel models: an integrative framework for defining R-squared measures. Psychol. Methods 24, 309–338. doi: 10.1037/met0000184
Rodgers, J., Riby, D. M., Janes, E., Connolly, B., and McConachie, H. (2012). Anxiety and repetitive behaviours in autism spectrum disorders and Williams syndrome: a cross-syndrome comparison. J. Autism Dev. Disord. 42, 175–180. doi: 10.1007/s10803-011-1225-x
Röhr, S., Müller, F., Jung, F., Apfelbacher, C., Seidler, A., and Riedel-Heller, S. G. (2020). Psychosoziale Folgen von Quarantänemaßnahmen bei schwerwiegenden Coronavirus-Ausbrüchen: ein Rapid Review. Psychiatr. Prax. 47, 179–189. doi: 10.1055/a-1159-5562
Rosenstein, E. (2020). “Handicap, confinement et l’expérience de la vulnérabilité.,” in COVID-19: Le regard des sciences sociales (Seismo), 215–225. Available at: https://seismoverlag.ch/de/daten/covid-19/ [Accessed May 6, 2021].
Samji, H., Wu, J., Ladak, A., Vossen, C., Stewart, E., Dove, N., et al. (2022). Review: Mental health impacts of the COVID-19 pandemic on children and youth – a systematic review. Child Adolesc. Mental Health 27, 173–189. doi: 10.1111/camh.12501
Samson, A. C., van den Bedem, N. P., Dukes, D., and Rieffe, C. (2020). Positive aspects of emotional competence in preventing internalizing symptoms in children with and without developmental language disorder: a longitudinal approach. J. Autism Dev. Disord. 50, 1159–1171. doi: 10.1007/s10803-019-04336-y
Schalock, R. L., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., et al. (2002). Conceptualization, measurement, and application of quality of life for persons with intellectual disabilities: report of an international panel of experts. Ment. Retard. 40, 457–470. doi: 10.1352/0047-6765(2002)040<0457:CMAAOQ>2.0.CO;2
Schalock, R. L., and Verdugo, M. A. (2002). Handbook on quality of life for human service practitioners. Washington, DC, US: American Association on Mental Retardation.
Schur, L. A., Ameri, M., and Kruse, D. (2020). Telework after COVID: a “silver lining” for workers with disabilities? J. Occup. Rehabil. 30, 521–536. doi: 10.1007/s10926-020-09936-5
Sideropoulos, V., Dukes, D., Hanley, M., Palikara, O., Rhodes, S., Riby, D., et al. (2022a). The impact of COVID-19 on anxiety and worries for families of individuals with special education needs and disabilities in the UK. J. Autism Dev. Disord. 52, 2656–2669. doi: 10.1007/s10803-021-05168-5
Sideropoulos, V., Kye, H., Dukes, D., Samson, A. C., Palikara, O., and Van Herwegen, J. (2022b). Anxiety and worries of individuals with down syndrome during the COVID-19 pandemic: a comparative study in the UK. J. Autism Dev. Disord. 52, 1–16. doi: 10.1007/s10803-022-05450-0
Siracusano, M., Riccioni, A., Gialloreti, L. E., Segatori, E., Arturi, L., Vasta, M., et al. (2021). Parental stress and disability in offspring: a snapshot during the COVID-19 pandemic. Brain Sci. 11:1040. doi: 10.3390/brainsci11081040
Somerville, L. H. (2013). The teenage brain: sensitivity to social evaluation. Curr. Dir. Psychol. Sci. 22, 121–127. doi: 10.1177/0963721413476512
Su, X., Cai, R. Y., Uljarević, M., Van Herwegen, J., Dukes, D., Yang, Y., et al. (2021). Brief report: a cross-sectional study of anxiety levels and concerns of Chinese families of children with special educational needs and disabilities post-first-wave of COVID-19. Front. Psychol. 12:708465. doi: 10.3389/fpsyt.2021.708465
Supratiwi, M., Yusuf, M., and Anggarani, F. K. (2021). Mapping the challenges in distance learning for students with disabilities during Covid-19 pandemic: survey of special education teachers. Int. J. Pedagog. Curric. 5:11. doi: 10.20961/ijpte.v5i1.45970
The Global Economy (n.d.). Public services index. Available at: https://www.theglobaleconomy.com/rankings/public_services_index/ (Accessed November 26, 2021).
Theis, N., Campbell, N., Leeuw, J. D., Owen, M., and Schenke, K. C. (2021). The effects of COVID-19 restrictions on physical activity and mental health of children and young adults with physical and/or intellectual disabilities. Disabil. Health J. 14:101064. doi: 10.1016/j.dhjo.2021.101064
Toseeb, U., Asbury, K., Code, A., Fox, L., and Deniz, E. (2020). Supporting families with children with special educational needs and disabilities during COVID-19. PsyArXiv. doi: 10.31234/osf.io/tm69k
Tye, C., Runicles, A. K., Whitehouse, A. J. O., and Alvares, G. A. (2019). Characterizing the interplay between autism spectrum disorder and comorbid medical conditions: an integrative review. Front. Psychol. 9:751. doi: 10.3389/fpsyt.2018.00751
United Nations International Children’s Emergency Fund (2020). Leaving no one behind during the pandemic: Children with disabilities and COVID-19. UNICEF. Available at: https://data.unicef.org/topic/child-disability/covid-19/ [Accessed October 20, 2020].
Van Buuren, S., and Groothuis-Oudshoorn, K. (2011). Mice: multivariate imputation by chained equations in R. J. Stat. Softw. 45, 1–67. doi: 10.18637/jss.v045.i03
Van Herwegen, J., Dukes, D., and Samson, A. (2020). COVID19 crisis response survey for families of individuals with special needs. Available at: https://doi.org/10.17605/OSF.IO/5NKQ9 [Accessed December 10, 2021].
Verdugo, M. A., Aguayo, V., Arias, V. B., and García-Domínguez, L. (2020). A systematic review of the assessment of support needs in people with intellectual and developmental disabilities. Int. J. Environ. Res. Public Health 17:9494. doi: 10.3390/ijerph17249494
White, L. C., Law, J. K., Daniels, A. M., Toroney, J., Vernoia, B., Xiao, S., et al. (2021). Brief report: impact of COVID-19 on individuals with ASD and their caregivers: a perspective from the SPARK cohort. J. Autism Dev. Disord. 51, 3766–3773. doi: 10.1007/s10803-020-04816-6
Widmer, E. D., De Bel, V., Ganjour, O., Girardin, M., and Zufferey, M.-E. (2020). “Dynamiques familiales et covid-19: réactions à la période de confinement.,” in COVID-19: Le regard des sciences sociales (Seismo), 159–177. Available at: https://seismoverlag.ch/de/daten/covid-19/ [Accessed May 6, 2021].
Wilkinson, K. M., and Hennig, S. (2007). The state of research and practice in augmentative and alternative communication for children with developmental/intellectual disabilities. Ment. Retard. Dev. Disabil. Res. Rev. 13, 58–69. doi: 10.1002/mrdd.20133
Willner, P., Rose, J., Stenfert Kroese, B., Murphy, G. H., Langdon, P. E., Clifford, C., et al. (2020). Effect of the COVID-19 pandemic on the mental health of carers of people with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 33, 1523–1533. doi: 10.1111/jar.12811
World Health Organization (2001). International classification of functioning, Disability and Health. World Health Organization.
World Health Organization (2015). International statistical classification of diseases and related health problems. Available at: https://apps.who.int/iris/handle/10665/246208 (Accessed January 09, 2023).
Keywords: survey, COVID-19 pandemic, neurodevelopmental conditions, families, environmental barriers, concern, anxiety
Citation: Di Poi G, Dukes D, Meuleman B, Banta Lavenex P, Lavenex P, Papon A, Tran M, Stallmann L, Treichel N and Samson AC (2023) Anxiety in families of individuals with neurodevelopmental conditions in the early months of the COVID-19 pandemic in Switzerland. Front. Educ. 8:951970. doi: 10.3389/feduc.2023.951970
Edited by:
Joseph Mintz, University College London, United KingdomReviewed by:
Wen Yang, The Chinese University of Hong Kong, ChinaCopyright © 2023 Di Poi, Dukes, Meuleman, Banta Lavenex, Lavenex, Papon, Tran, Stallmann, Treichel and Samson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea C. Samson,  YW5kcmVhLnNhbXNvbkB1bmlmci5jaA==
YW5kcmVhLnNhbXNvbkB1bmlmci5jaA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.