
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Educ., 10 November 2023
Sec. Higher Education
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.1252842
This article is part of the Research TopicResearch and Discussions in Critical Discourses and Remedies in Global Health EducationView all 20 articles
 Wagaki Gicheru1*
Wagaki Gicheru1* Nyawira Mwangi2
Nyawira Mwangi2Background: The use of digital tools and applications in health professions education is increasing exponentially, however this has the potential to increase the digital inequities with the resulting effect of vulnerable groups facing an increased risk of digital exclusion. It is therefore important to approach digitalization with contextual determinants of the intended and unintended impact in mind. We present a perspective paper on digital equity, informed by lessons learnt at the Kenya Medical Training College (KMTC).
Methods: Using a case description methodology, we examined routine educational data collected from faculty at KMTC in November 2022. This included quantitative and qualitative data on access, ownership, utilization, confidence and skills to create, share, and exchange knowledge on the institution’s learning management system. We used these factors as the conceptual framework for understanding how faculty adopt digitalization in health professions education.
Results: 306 faculty responded to the survey (response rate 27.8%) of whom 90.8 and 75.2% had personal laptops at home and at work and 75.9% had internet at work. 53.4% (n = 163) knew they had accounts created on the institution’s learning management system (LMS) majority of whom had basic skills and were able to perform skills such as logging in and accessing learning resources. However, a minority had advanced skills needed for teaching and learning in the LMS.
Conclusion: Medical education institutions in LMICs need to adopt programs to enhance digital literacy and monitoring of access, utilization and self-efficacy across all learner and faculty groups, to ensure that digital technologies reduce rather than exacerbate existing inequities.
Digital transformation is an important intervention in the path to universal health coverage, and it is changing the landscape of health professions education in the 21st century (Kickbusch et al., 2021). There is a growing need to embrace digital technologies, especially following the lessons learnt from the COVID-19 pandemic, as well as the growing demand for training (Lakshmi, 2021). Many benefits to adoption in technology in health profession education have been postulated. These include the potential to transcend geographical and financial barriers, and the ability to expand opportunities for flexible training. Digital technology has therefore become a priority area for investment in institutions that offer health professional education in Lower- and Middle-income countries (LMICs), especially in elearning (Barteit et al., 2020; Gachanja et al., 2021).
The adoption of technologies by medical training institutions unfortunately has not meant that the benefits are experienced by all; in fact, it has created unintended disparities that has resulted in many faculty and students being left behind. The gains made through digitalization risk being lost or minimized if the threats presented by digital inequity are not addressed in a timely and appropriate manner (James, 2008). The threat posed by the digital divide is worse in sub–Saharan Africa where insufficient capacity in digital infrastructure, skills, connectivity, and supportive logistics such as electricity present challenges to training institutions even in urban areas.
The digital divide among faculty can be seen as simply as the gap between those who have access to ICT and those that do not. This is easy to measure especially for training institutions. However, this gap only reflects the first level of inequity (van de Werfhorst et al., 2022) and even in this level there may be nuances reflecting various sub-levels such as type of technology, duration of access, and internet speed. Multiple levels of capacity are required to attain self-efficacy. For example, personal characteristics of faculty, particularly age, gender, education, teaching experience and discipline need to be evaluated to understand their influence on adoption of digital technology (Lakshmi, 2021). Further, the context, including baseline technology penetration levels, cultural attitudes and infrastructure around digital technology mediate the outcomes around health equity and are at least as important as individual factors. It is known that digital transformation of health professions education is dependent upon the level of e-readiness, the measure of the degree to which a society “may be ready, willing or prepared to obtain benefits which arise from information and communication technologies (ICTs; Dada, 2006). E-readiness has been researched using many models, with central measurements being internet penetration, the capacity of human capital, ICT infrastructure, supportive policies and regulations. Training institutions that are not e-ready are not able to benefit from the opportunities presented by digital infrastructure. In such situations, digitalization may widen digital inequity (Heeks, 2022). It has been reported that most countries in Africa are not e-ready, and that digital interventions that do not account for limitations such as scarcity of steady power supply, lack of basic ICT skills by users, and low network coverage are likely to fail. The rapid diffusion of digital technology in African countries is creating great opportunities for marginalized groups, but it has also resulted in unequal access to new technologies, leading to what is now known as the “digital divide.” Interventions to widen access to technology are important, but in addition, the movement towards digitization should include digital skills development. Access to technology is a necessary but not sufficient intervention for the digitization needs in health professions education. This can prevent widening inequalities, as well as mitigate against the effects of harmful digital marketing around health professions education such as the mushrooming of online courses of low quality. Kenya is unique in that the mobile phone penetration is very high, at 130% (Kenya National Bureau of Statistics, 2023). The Kenya Medical Training College is a state corporation under the Ministry of Health, whose mandate focuses on health professions education for different cadres. What can we learn from the experience of KMTC, in terms of identifying and addressing digital inequity? How can digital equity be institutionalized?
We analyzed routine data collected during a faculty needs assessment at KMTC in March 2023. The data was obtained through an online survey conducted by the elearning department at KMTC, whose aim was to assess learning needs and practices. The survey was conducted on Google form, whose link was shared to all faculty in the college (n = 1,100) through an email sent to the Principal of each campus with instructions to share with all academic staff. The Google form contained questions around devices, access to the Learning Management System and faculty skills on LMS. Faculty were requested to respond within 7 days. Data collected was both qualitative and quantitative. Our conceptual framework was that adoption of digitalization among faculty should proceed along the continuum of Ownership, Access, Skills, Confidence, and Self-efficacy.
306 faculty responded to the survey (response rate 27.8%). The faculty represented all Departments (18) and 84% of the 74 Campuses of the institution. Of the 306 faculty, 90.8% had personal laptops, 75.2 and 75.9% had access to personal computers and internet at work, respectively, and 53.4% knew they had accounts created on the institution’s learning management system (LMS). The 53.4% (163) were then asked further questions about their ability to use the LMS. Majority of the respondents had basic skills and were able to perform skills such as logging in, accessing learning resources, a large number however, were not able to update their profile (Figure 1). The advanced skills, associated with teaching and learning on the LMS, had the majority of faculty expressing “No” or “Slight” levels of confidence in the performance of the skills. These skills included uploading content (64%), enrolling and un-enrolling learners (76%), tracking progress of learners (70%) and generating reports from the LMS (78%). Quantitative data indicated that the challenges faculty faced were mostly on Infrastructure (54.9%), Skills (32%), and Training (9.2%). Some of the stated infrastructure challenges included power (frequent blackouts, access points, e.g., few sockets or extension cables), lack of or old computers and poor internet connectivity. Skills challenges included lack of confidence and minimal ICT competency. They felt there is a need for retraining and offer face-to face training vis-a-vis online. One faculty member’s comment “Am not well versed on how to use online platforms in teaching hence very reluctant to adopt what I am not sure about” gives a clear insight on their personal assessment.
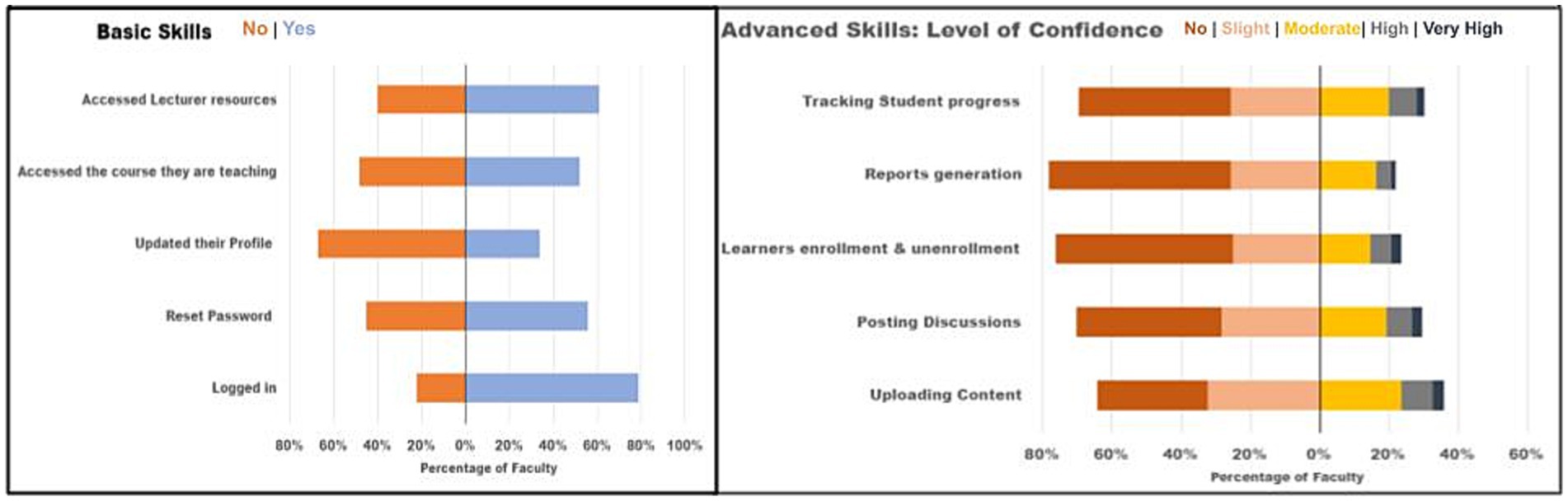
Figure 1. Faculty Skills for teaching and learning on the Learning Management system (n = 163) Only the 53.4% (163) who had accounts on the LMS responded to question on skills. The responses to the basic skill questions were Yes or No (left) and included those skills associated with access to and within LMS. The advanced skills were those directly associated to teaching and learning (right). A Likert scale was used to measure the individual faculty’s level of confidence to perform select advanced skills.
Figure 2 depicts the digital inequity among faculty (n = 306). The inequity can be seen as the “loss” of faculty along the pathway to self-efficacy. The first level of inequity is in infrastructure with 90% having personal computers (PCs) at home, 75% having no access to PCs or internet at work. The next level of inequity is on access to the institution’s LMS with 55% answering “Yes” to whether they had accounts.

Figure 2. Digital divide among faculty.
The following two levels of inequity are on digital literacy. 45% having basic skills on the LMS and only 15% having moderate to very high confidence on skills needed for teaching and learning (advanced skills).
This was a broad analysis that evaluated various aspects of adoption of technologies such as access, ownership, utilization, skills and self-efficacy. It provides evidence for the extent to which the needs at these levels have been addressed. The response rate of 27.8%, albeit low, is comparable to what has been reported in the literature on online surveys (Shiyab et al., 2023) but may perhaps be a reflection of the challenges on the use of technology.
Institutions of higher education are adopting digital technologies for teaching and learning. This has been necessitated by the potential gains and the emerging trends in use of digital technology in medical education. However digital inequities are present among faculty and can be seen in the various levels in the continuum of digitalization (Figure 2). In each level there are faculty who have been “left behind.”
The first level is personal ownership of laptops where 10% are left behind and do not own devices. This is interesting since the country has a very high (130%) mobile phone coverage, meaning that many Kenyans have more than one mobile phone device (Kenya National Bureau of Statistics, 2023). It is likely that the low ownership of laptops is related to their high cost, as compared to the cost of mobile phone devices. But importantly, it may point to the fact that the 130% overall coverage masks an unexplored digital divide. The divide increases progressively such that at the level of the skills needed for teaching and learning using the available technology, 85% of faculty are left behind. To our knowledge, we are the first group to demonstrate the progressive widening of this divide along the continuum.
It is important that training institutions identify and understand the divide among faculty (Soomro et al., 2020; Goh and Blake, 2021; Lakshmi, 2021) and actively work towards reducing the gap. One way to do this is to develop a checklist or questionnaire that identifies gaps at specific levels of the continuum of digitalization, such as the online tool used in this study. The second way is to collect and disaggregate data by key variables such sociodemographic factors, which are known to affect equity. PROGRESS plus factors (Place of residence, Race/ethnicity/culture/language, Occupation, Gender/sex, Religion, Education, Socioeconomic status, social capital) are often used to apply an equity lens to health interventions (Cochrane, 2023). It is expected that the same variables are relevant predictors for digital equity in medical education.
While the shift to digital learning modalities offers benefits in health professions education, it is dependent upon acquisition and maintenance of a certain standard of infrastructure, digital literacy and skills. These are the main determinants of digital equity. Heeks (2022) has described access, adoption and use of technology as key areas where inequity may be noticed. In this case study, we have shown that the access to infrastructure may be nuanced by location (at home and at work), given that faculty may facilitate online teaching and learning from remote locations. It is interesting that a higher proportion of faculty had access to infrastructure at home rather than at work. This points to the need for the institution to continue to invest in additional infrastructure, in addition to all the other levels of digitalization.
The digital divide is not expected to disappear without interventions. In fact, the digital inequities are likely to grow as technology increases, if there are no simultaneous interventions to address the divide. To ensure no faculty are left behind, inclusion should be complete not partial (Heeks, 2022). For example, faculty have different needs, competencies and attitudes which should be considered as interventions are developed. Secondly the value of digital equity must be acknowledged by all stakeholders, including faculty. Thirdly, individual and institutional context must be considered, such that innovative interventions are developed. Context may include institutional infrastructure, norms, sustainability, peer impact, geographical location of the campus, policies, standards, regulation and quality assurance. The multiple factors that should be considered shows that institutionalization of digital equity is likely to be a complex and multifaceted endeavor.
A key limitation of the study is that the socio-demographic data including gender, age and education level was not collected. There is a possibility that there are other levels of inequities that may have been masked. This evaluation was limited to the unique case of KMTC, however comparability with other institutions is feasible because the conceptual framework is applicable to diverse institutions. The use of an online survey may introduce bias in that only those with digital skills may take part, which adds to the richness of the reflections on the digital divide. An important strength of the paper is that we have examined how routine data can be used to identify digital inequity, which is lacking in the literature. Another strength is that the study fills an important gap, where there is paucity of evidence from low- and middle-income countries, which would benefit from digital education, and we provide evidence that is context specific.
Documenting the findings in this case report contributes to the knowledge base on understanding digital equity in health professions education. It contributes to the global debate on the digital divide in health and education, and may inform future implementation priorities at the KMTC. This includes programs to enhance digital literacy and monitoring of access, utilization and self-efficacy across all learner and faculty groups, to ensure that digital technologies reduce rather than exacerbate existing inequities and inequalities. Similar institutions should adopt policies that avert adverse effects of digital inequities, and analyze similar routine data to guide decisions and action on institutionalizing digital equity. Institutions in LMIC should explore enabling private-public and north–south partnerships that could provide infrastructure and digital skills solutions. Future research might explore the digital divide among other users such as learners, and the impact of various interventions towards institutionalization of digital equity.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request, and within the existing data protection laws.
WG: conception and analyzing data. NM and WG: interpretation of data, writing, revising, and approval of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ICT, Information, communication and technology; KMTC, Kenya Medical Training College; LMS, Learning management system; LMIC, Lower- and middle-income country; PC, Personal computer
Barteit, S., Guzek, D., Jahn, A., Bärnighausen, T., Jorge, M. M., and Neuhann, F. (2020). Evaluation of E-learning for medical education in low- and middle-income countries: a systematic review. Comput. Educ. 145:103726. doi: 10.1016/j.compedu.2019.103726
Cochrane (2023). Cochrane Methods Equity PROGRESS-Plus. Available at: https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus [Accessed June 2, 2023].
Dada, D. (2006). E-readiness for Developing countries: moving the focus from the environment to the users. Elect. J. Inform. Syst. Dev. Count. 27, 1–14. doi: 10.1002/j.1681-4835.2006.tb00183.x
Gachanja, F., Mwangi, N., and Gicheru, W. (2021). E-learning in medical education during COVID-19 pandemic: experiences of a research course at Kenya medical training college. BMC Med. Educ. 21:612. doi: 10.1186/s12909-021-03050-7
Goh, P. S., and Blake, D. (2021). E-readiness measurement tool: scale development and validation in a Malaysian higher educational context. Cogent Educ. 8, 1–24. doi: 10.1080/2331186X.2021.1883829
Heeks, R. (2022). Digital inequality beyond the digital divide: conceptualizing adverse digital incorporation in the global south. Inf. Technol. Dev. 28, 688–704. doi: 10.1080/02681102.2022.2068492
James, J. (2008). Digital Divide Complacency: Misconceptions and Dangers. Inf. Soc. 24, 54–61. doi: 10.1080/01972240701774790
Kickbusch, I., Piselli, D., Agrawal, A., Balicer, R., Banner, O., Adelhardt, M., et al. (2021). The lancet and financial times commission on governing health futures 2030: growing up in a digital world. Lancet 398, 1727–1776. doi: 10.1016/S0140-6736(21)01824-9
Lakshmi, Y. V. (2021). ELearning readiness of higher education faculty members. Indian J. Educ. Tech. 3.
Shiyab, W.'e., Ferguson, C., Rolls, K., and Halcomb, E. (2023). Solutions to address low response rates in online surveys. Eur. J. Cardiovasc. Nurs. 22, 441–444. doi: 10.1093/eurjcn/zvad030
Soomro, K. A., Kale, U., Curtis, R., Akcaoglu, M., and Bernstein, M. (2020). Digital divide among higher education faculty. Int. J. Educ. Technol. High. Educ. 17:21. doi: 10.1186/s41239-020-00191-5
Keywords: digital equity, digital divide, KMTC, digital learning, elearning, digitalization, digital skills
Citation: Gicheru W and Mwangi N (2023) Identifying the need to institutionalize digital equity among faculty: the experience of the Kenya Medical Training College. Front. Educ. 8:1252842. doi: 10.3389/feduc.2023.1252842
Edited by:
Jessica Evert, Child Family Health International, United StatesReviewed by:
Anna Kalbarczyk, Johns Hopkins University, United StatesCopyright © 2023 Gicheru and Mwangi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wagaki Gicheru, d2dpY2hlcnVAa210Yy5hYy5rZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.