 Aylin Baysan
Aylin Baysan Usman Naeem
Usman Naeem
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 22 September 2023
Sec. Higher Education
Volume 8 - 2023 | https://doi.org/10.3389/feduc.2023.1148344
This article is part of the Research TopicFlipped classroom or flipped learning in health professionals' educationView all 5 articles
In today’s educational landscape, active learning is often overlooked during lectures, seminars, and tutorials. The aim of this study was to investigate perceptions of online and face-to-face lecture formats and their impact on the learning experiences of undergraduate dental students in Years 3–5. This qualitative study was conducted to investigate the effectiveness of different lecture formats at the Institute of Dentistry for undergraduate dental students in Years 3–5. There were two specific questions asked to dental undergraduate students with additional free-text questions. In total, 120 of 221 undergraduate students participated in this study between October 2019 and February 2020, and only 42 participants included the free-text comments. Three core themes related to the blended learning approach were identified: (1) scheduled versus recorded lectures, (2) duration of academic lectures, and (3) neurodiversity and learning experiences. The results showed that the learners perceived the traditional didactic lectures as the least effective format. There is not a “one fits all” lecture format that would accommodate a neurodiversity-based approach that focuses on the strengths, abilities, and interests of students. Hybrid lecture formats in combination with online teaching coupled with small group tutorials could be suggested. There is a unique challenge in the post-COVID-19 era for both educators and learners due to the lack of clinical practice and heavy reliance on online methods of teaching in Dentistry. Therefore, the implication of these results on the planning and financing of programmes could be discussed in Higher Education.
Pedagogy in Higher Education (HE) is a complex concept that supports a critical and reflective understanding of teaching and learning by both students and educators in a holistic way. The pedagogical approach covers not only teaching techniques and educator–student partnership but also embraces and informs inclusive educational theories, personal learning styles, assessments, and continuous partnership inside and outside the classrooms.
Inclusive education is a pertinent and necessary concept in HE. This pedagogical strategy would create an environment in which the learning needs of all students with different types of neurodiversity are considered so that learners can engage, participate, and become active recipients. Furthermore, diversity is valued in inclusive educational contexts, which foresees accessible resources, taking account of different learning styles and anticipating the possible needs of learners (Moriña, 2017).
In HE, promoting learning through active engagement has been shown to improve learner performance (Hake, 1998; Knight and Wood, 2005; Michael, 2006; Chaplin, 2009). The traditional learning experiences in lecture theaters are reported to be ineffective when the goals involve the application of knowledge. Consequently, learners become passive recipients of large amounts of information, which leaves them with limited mental capacity to actively engage in their learning experiences (Brown and Manogue, 2001). In this respect, Moore et al. (2008) reported the reasons for lecture non-attendance of 230 undergraduate business students in an Irish university and discovered that the students: “….. do not articulate a sense of obligation to attend lectures, despite the messages, assumptions, and convictions that faculty members may share about the importance of such attendance. Among this sample of students, at the very least, occasional lecture absenteeism is the norm and, for many, absenteeism is a relatively regular occurrence.”
Tormey and Henchy (2008) also noted that traditional lectures failed to motivate contemporary thinking. Therefore, the conventional ways of education delivery could be redefined by the combination of online learning technologies, which might become mainstream since the inception of Education 4.0 (Hussin, 2018). This way of learning could be effective, especially when linked to face-to-face teaching in a blended learning format. This strategy would then impact on:
• traditional pedagogical approaches for large classes,
• dental undergraduate learners being expected to review topic material at a later time,
• the intense assessment strategies that evaluate the applied knowledge in clinical dentistry.
In dental schools, online education failed to be accepted widely due to essential practical skills in the clinical skills laboratory and patient treatment in conjunction with theoretical knowledge. Recently, many dental schools in the world have moved to the “didactic” teaching temporarily/permanently online due to the COVID-19 pandemic and are currently planning to adapt their curriculum to the post-pandemic “new normal.” In this respect, different educational modalities could be considered, that is, PowerPoint presentations, live/recorded lectures, video-based or case-based learning, interactive learning, online whiteboard teaching, and virtual models (Singh et al., 2021). However, these methods have limitations in clinical dentistry due to the practical and skill-based nature of the education (Chavarría-Bolaños et al., 2020). Planning these mixed modalities in dental education is essential. In this respect, the process of learning aims to move away from a time-based paradigm to focus on the acquisition of skills and abilities without traditional time constraints (Camacho and Legare, 2021). It should also be noted that learning objectives need to be aligned for virtual environments by considering how available technologies can facilitate the delivery of programmes. In addition, Wiggins and McTighe (2005) previously encouraged educators to design courses by identifying learning objectives and required evidence through constructive alignment as suggested in Biggs (2002). In this respect, learners are able to understand the educators’ expectations to demonstrate the desired level of proficiency.
Interestingly, captured (recorded) lectures provide learners with the flexibility to review module content at their own pace. Using such strategies, learners in online lecture groups demonstrated their ability to learn at the same level with less time than in face-to-face lecture groups (Spickard et al., 2002). With this respect, the captured lectures were also found to be helpful for non-native language learners as this lecture format allows them to slow down or repeat the unfamiliar or fast-moving content that would otherwise have been lost (Simpson, 2006; Scutter et al., 2010).
Grainger (2013) reported that up to 20% of all learners attend online courses at Canadian Universities. Many Universities have already implemented a blended learning approach, which combines traditional didactic teaching with alternative learning technologies such as teleconferencing and requires personal research outside of class time to maximize the in-class discussions. Online learning has become a new way of continued education, which is largely due to being easily accessible and time flexible. Given this, the essential question is “What impact do different learning technologies have on learner experience?”
Despite encouraging evidence, online platforms still possess challenging outcomes due to the lack of student engagement. Amir et al. (2020) previously reported that students indicated suboptimal learning satisfaction and challenging communication with either educators or peers during online learning. This means that internal factors of student readiness, time management, and challenges in focusing online for a long time were indicated. Therefore, the percentage of online courses and/or blended learning courses requires further research.
Lecture recordings aim to provide a way of different interaction; however, student learning experiences could not be tailored actively. Therefore, virtual learning needs to be in the form of online theory with flipped teaching in practical sessions, small group tutorials/seminars, and structured assessments on applied knowledge. Overall, inclusive approaches are novel ways of promoting student engagement, motivation, and performance (Schonwetter et al., 2016). With this respect, the rationale for conducting this current study was to understand the students’ perceptions in the view of inclusive education. The primary objective was to plan the curriculum delivery by considering the ratio of online, in-person, and hybrid education modalities in dental schools.
In summary, dental education faces challenges with respect to delivering an intense dental curriculum with applied knowledge in consideration of patient care. Remote communication and learning activities in each aspect are utilized creatively to enhance the activities for inclusive education. Therefore, the effectiveness of different modes of learning would need to be evaluated in order to decide where and how to use the best elements of both in-person and remote teaching and know how to implement quality improvements. The ultimate aim was to establish high-quality and effective educational interventions; therefore, it is important to understand dental students’ attitudes toward their preparedness for different modes of teaching, as well as their perceptions about the value and effectiveness of these learning experiences (Hew and Lo, 2018; Hussin, 2018).
Whilst existing literature demonstrates the importance of active learning, much is still unknown about the format of lectures and their impact on learners’ experiences. This study aimed to investigate the perceptions of dental undergraduates in Years 3–5 on different lecture formats and the impact of these lecture formats on students’ experiences.
The study protocol was approved by the ethics committee of the local university. The online secure software which was developed by the University of Bristol was disseminated to dental students in Years 3, 4, and 5 (n = 221). The period for the survey was between October 2019 and February 2020. All undergraduate dental students in Years 3–5 were invited to participate and received official emails notifying them of the aim of the survey. Participation in the study was voluntary. All participants were reassured that responses will be anonymous and will be dealt with confidentially. In addition, due to the anonymity of the survey and to provide a safe space for students’ perspectives on the lecture delivery modes, demographic data were not recorded. The ultimate aim was also to investigate the best practice for inclusive education and to provide a mechanism for student voice and culture-building in dental school despite gender, age, and background differences.
The study design used a qualitative approach to explore the data in order to provide an in-depth understanding of the research question. The questionnaire aimed to identify the effectiveness of various online tools and technologies, students’ preferences in relation to learning methods, and factors that might influence the learning experience. The parameters were based on different types of learners, advantages, and challenges of different modalities of teaching (Davis et al., 2019).
The participants were required to answer two specific questions with additional free texts (Table 1). Question 1 was used to comprehend the learning style of a student whilst the free text was added since the potential of free-text responses has increasingly been invaluable for personalized and narrative potentials. Interestingly, free-text comments would suggest that qualitative data sets provide intrinsic value and can be analyzed further with respect to survey evaluation purposes (Rich et al., 2013).

Table 1. Study questionnaire.
Thematic analysis was conducted by the authors to analyze the survey responses as this highly flexible approach provides a rich and detailed account of data (Braun and Clarke, 2006; Clarke and Braun, 2013; Nowell et al., 2017). Any disagreements have been resolved through an open discussion. A discussion of the existing literature and how this present research contributes to the area has also been included.
In addition, both authors repeatedly read the free-text comments and independently coded the data. Subsequently, the coded data were re-analyzed until the researchers believed the codes accurately represented the participants’ comments. Three themes were chosen following an open discussion. The data were then collated under the proposed themes and reviewed repeatedly to ensure the themes reflected the data. Following this, data extracts were chosen to illustrate the chosen themes and enhance the transparency of the analysis (Sandelowski, 1986).
Researchers who are relatively unfamiliar with qualitative methods might find this analysis to be a useful method for examining the perspectives of different research participants, highlighting similarities and differences, and generating unanticipated insights. The thematic analysis could also summarize the key features of a large data set, as a well-structured approach would enable to produce a clear and organized final report (Nowell et al., 2017).
A total of 120 undergraduate dental students participated in this study, and only 42 participants included free-text comments. The results showed that the majority of students preferred the hybrid approach combining scheduled lectures with Q-review content or short seminars. Q-review is the video portal that provides learners with recorded content related to their modules. This is available via the learning management system (LMS), called Moodle. However, the learners perceived the traditional didactic lectures alone as the least effective format (Figure 1).
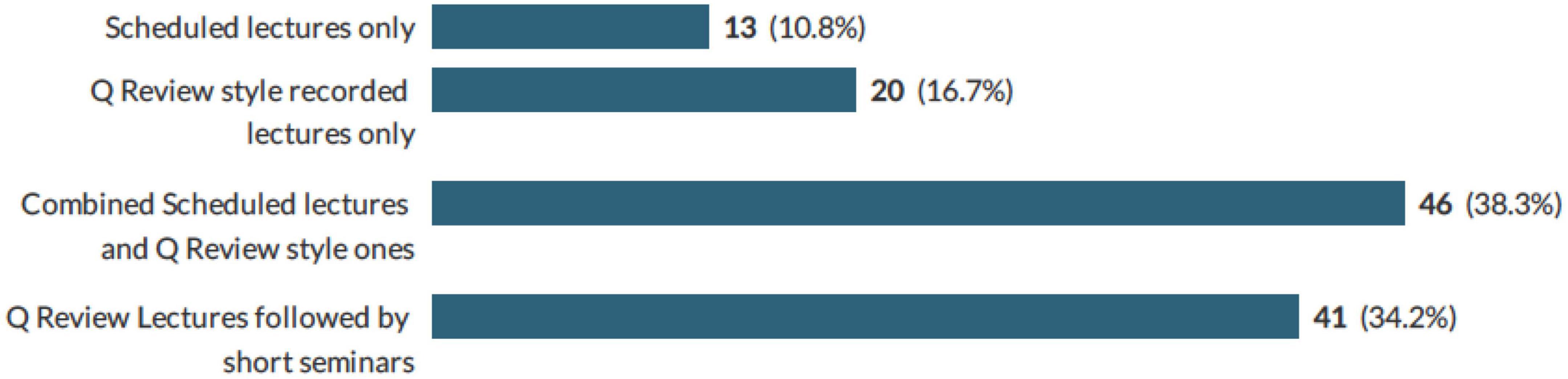
Figure 1. Percentage of the learners’ choice of the different lecture formats.
Other factors that influence the learners’ preference toward online recorded lectures were as follows:
• the time to travel to the campus,
• delivery speed during the face-face lectures (accepted speech rate is approximately 150 words per minute),
• duration of the lectures, that is, up to 120 min,
• lack of engagement during the lectures due to different learning styles,
• challenges in understanding the lecture content.
The three identified core themes (Figure 2) related to the blended learning approach were as follows: (1) scheduled versus recorded lectures, (2) duration of academic lectures, and (3) neurodiversity and learning experiences.
Figure 2. Themes identified from qualitative analysis.
In total, 5 of the 42 students’ comments preferred to have the scheduled face-to-face lectures and stated:
“I find that having a given lectures [SIC]forces me to go over them and learn them, whereas it is much easier to forget about and ignore online ones.”
“I personally enjoy having the lectures delivered as they give me the opportunity to ask questions then and there.”
“Scheduled lectures are valuable as they allow easy opportunity to ask questions.”
“I think it’s good to have scheduled lectures but they should be supplemented by recorded lectures and resources we can access in free time.”
“I find that having a given lectures [SIC]forces me to go over them and learn them, whereas it is much easier to forget about and ignore online ones.”
A learner stated, “Scheduled lectures but with no attendance so that we can see it at home, which saves time.” This was an interesting observation, as it is important to consider learners’ accommodation and the effect of in-campus or at-home living on their learning experiences. It should be noted that studying dentistry is known to be technically and academically extremely demanding (Institute of Medicine (US) Committee on the Future of Dental Education, 1995).
A Year 5 student stated, “I think it’s good to have scheduled lectures but they should be supplemented by recorded lectures and resources we can access in free time.” It can be speculated that students who are used to face-to-face education would prefer supplementing their learning with asynchronous lectures.
Another suggestion was to deliver challenging topics face to face and the others online. In this respect, a Year 4 dental student suggested that “Some larger/more difficult topics delivered in person. Others recorded and put on QMPlus as going through in own time can be easier and more beneficial.”
In this respect, Horvath et al. (2013) reported that the lecture recording enabled less class time for active learning activities such as the application of knowledge or problem-solving. The changes following the recorded lectures included providing supplementary material, focusing on case and problem integration, incorporating more videos, and avoiding statements in lectures that cannot be supported. However, more evidence is required to understand the best approach to combine both modes of delivery in dental education.
There were specific comments on the concentration span of the learners during the didactic teaching, such as “After 2 h sat on lectures I can no longer concentrate.” [SIC] Interestingly, the year of dental school was not disclosed by the participant despite the additional request for this information stating that this would enable us to tailor students’ needs according to the expectations.
A Year 4 dental student’s comment also reflected this:
“I think it is quite unfortunate that the university expects students and young adults to be wide awake and able to retain 3–4 h worth of lecture content back to back. The concentration span of the average student is around 30 mins which is why short interactive seminars would be ideal. This combined with seminars will undoubtedly be an optimal way to improve the UG teaching. Also, everyone studies differently, a lot of students feel forced to attend lectures just because of the rule of “compulsory attendance.” I can tell you with 100% certainty that 80% of students attending the lecture are only there to “sign in” yet continue doing whatever they want to do or even funnily enough, Q-reviewing ANOTHER lecture as the lecture is going on.”
Another student suggested that attendance should be recorded “I hope attendance to lectures is not compulsory as not everyone finds listening to live lectures on spot more useful than watching recording.”
There were a couple of additional comments from different participants without disclosing the year of dental school which revealed the importance of lecture delivery speed and the long duration of lectures. Both feedback suggested ineffective learning experiences when the lectures were delivered at scheduled times with long duration. “Sometimes difficult to follow the speed of scheduled lecture, easier to follow Q-review lecture as you can pause to make notes, look up additional information, etc.”
“I do not gain much value from sitting in a lecture theater for several hours. Time would be much better used by giving lectures via an online service followed by small seminars where understanding can be cemented and questions answered where understanding can be cemented and questions answered.”
In addition, three learners noted that pre-recorded lectures have been beneficial in addition to the face-to face ones in case of any possible IT issues with schedules lectures.
“The pre-recorded lectures with slides and commentary are very useful as they can be looked at any time and there is no need to worry about any issues with the Q-review recording that happens in scheduled lectures.”
In this respect, Bruner (1967) reported the assimilation of knowledge by utilizing four sensory modalities: visual (images, pictures, symbols, or diagrams), auditory (listening and discussing), visual/iconic (reading and writing), and kinesthetic (by smell or touch). There are many tools that have been proposed such as Vermunt’s inventory, Kolb’s learning style indicator, Myers–Briggs type indicator, and Fleming’s Visual, Aural, Read/Write, and Kinesthetic (VARK) questionnaires, and it was noted that there should not be any restriction to use one particular style only. Educators are encouraged to explore learners’ experiences and styles (Fleming and Mills, 1992; Cassidy, 2004; Coffield et al., 2004).
In HE, lectures generally last nearly 45–50 min; however, there is evidence suggesting that students’ attention span is 10–15 min, and Bradbury (2016) indicated that the lecture time should be limited to this duration. However, the undergraduate dental curriculum presents complexities, uncertainties, and challenges due to the nature of clinical practice and the required applied knowledge to achieve the learning outcomes, which were set by the General Dental Council (GDC) in the UK (The General Dental Council [GDC], 2015). These learning outcomes reflect the knowledge, skills, attitudes, and behaviors of a clinician who must practice safely, effectively, and professionally. This provides eligibility to apply to join the GDC registers. Therefore, dental education should produce an individual who can demonstrate that they have met the required learning outcomes and are safe and fit to practice independently within their knowledge and ability. Due to the high demands of complex dental education, innovative and creative way of curriculum delivery is required by considering the short attention span of dental students. However, more research in this area is required.
Diversity in learning styles is a major part of the learner learning experiences. In this context, a Year 5 student pointed out the importance of learning styles.
“Lectures don’t take into account different learning styles which is important.”
Garrison and Kanuka (2004) reported the benefits of blended learning by utilizing online and face-to-face teaching to enhance learner-centered learning and facilitate interactive discussions among learners and educators.
Interestingly, a total of eight participants suggested blended learning due to the following reasons:
“I find questioning based on clinical scenarios seems most effective with the students in our year.” A Year 5 student.
“I don’t mind scheduled lectures. It can be a mix of all scheduled, q review and short seminars depending on topic.” A Year 5 student.
From three different participants whose year of studies was unspecified.
“Although lectures are useful, sometimes I find that seminars are better at developing a better understanding of lectures.”
“I think most lectures should be previously recorded q review format followed by a more case-based discussion lectures.”
“I think pre-recorded lectures posted on QMPlus along with the lecture handout would be a very good idea.”
“I like that you cover all the content again in the morning of the session, and videos and diagrams as always useful to help grasp certain concepts.” A Year 3 student.
“I find it hard to engage with lecture content. However, through having seminars, this knowledge is more likely to be reinforced as it is with a smaller group of people.”
“Online lectures aren’t often recorded and they aren’t updated; having seminars may be more useful as smaller group teaching is often more effective.”
Cognitive psychologists divide “knowledge” into three areas: (1) declarative knowledge, (2) procedural knowledge, and (3) an ill-defined gray zone between declarative and procedural knowledge that includes the reasoning skills described as critical thinking and problem-solving. In dental education, critical thinking and problem-solving are often loosely defined as clinical reasoning, diagnostic thinking, or clinical judgment. In this respect, declarative knowledge formulates subconsciously retrieved memory, known as implicit memory, so that the guiding action happens automatically without any thought such as “an automatic pilot.” Therefore, implicit memory consists of past experiences that influence our current behavior, i.e., the memory of a challenging restoration, which was successfully managed on a previous patient.
Implicit memories are subconsciously blended into our thought formation and are usually instantly available. In this respect, one student suggested that “I believe that teaching is much better learnt in a scenario based.”[SIC].
This could be a student-centered community-based learning method for handling real-life situations. However, this education strategy would require students to develop in-depth basic knowledge and skills in different topics within Clinical Dentistry. In addition, logical thinking processes and a clear understanding of how to evaluate the dental literature need to be carefully considered by educators prior to scenario-based coherent discussions.
This is the first dental survey to understand the learning experiences of students with respect to different lecture formats in order to provide inclusive education. It would be absurd to propose “all means all” such as all pilots would be expected to fly all airplanes for all purposes, by disregarding the number or type of engine(s)/size/purpose (Kauffman, 2021). In this respect, the results from this study clearly reported that there is no “one format” of a lecture that would fit the neurodiverse student population. The integration of technology into pedagogy has the potential to facilitate flexible, learner-centered diverse teaching and encourage interaction among students and educators, which would enable them to collaborate and communicate asynchronously (Ellaway and Masters, 2008).
Therefore, blended learning would be beneficial by utilizing the available IT resources; however, this approach still needs to consider the learners’ diversity related to a topic and then determine how technology might enhance education (Laurillard, 2002). It should also be noted that the virtual learning strategy possesses limitations such as loss of collegiality and networking. In addition, challenging interactions between educators and students in an “artificial” encounter could result in inefficient personal-level communication, potential technical problems due to suboptimal infrastructure, and the inability to cover all disciplines in the dental curriculum (Elledge et al., 2020). In this survey, there were specific comments suggesting the decision-making process for the format of teaching could be related to the subject base due to the complexity of the implementation of knowledge into clinical practice in dental education. With this respect, it is also important to note, however, that blended learning is highly context-dependent and that the generalization of concepts across disciplines is challenging (Harris et al., 2009).
With living expenses increasing, university life becomes challenging for many dental students in the UK. Therefore, the majority of students’ preference to provide online scheduled lectures was evident in this study. In addition, dental curriculum might have an impact on the emotions, psychology, and ultimately the well-being of students, as the students consistently deal with the demands of time and scheduling pressures in relation to academic lectures, tutorials, laboratory sessions with clinics, management of patients, examination anxiety, and financial commitments (Divaris et al., 2008). Schmitter et al. (2008) reported that some dental students need to work to cover living expenses and this might also influence their stress levels. Therefore, a holistic and inclusive approach to dental education considering different platforms to deliver the curriculum plays a key role in student learning experiences.
Previously, a systematic review on blended learning in clinical education stated that there might be practical benefits to further explore the use of blended learning in clinical education among healthcare learners despite having a limited pool of evidence. Therefore, broad claims of improvement are challenging, and further research in this area is required before any assumptions with regard to the benefits of blended learning in dental education (Rowe et al., 2012).
In addition, the success of online education (Huss and Eastep, 2015) depends on the attitudes, interactive, and diverse teaching styles of education. The effectiveness of education needs to be measured from a pedagogical, organizational, teaching, and learning perspective. Learners’ proactivity and willingness to engage with educators are ongoing concerns in online education. In this respect, neurodiversity which focuses on differences in individual brain function and behavioral traits, regarded as part of normal variation in the population, would need to be considered. The trustable environment to be resilient to differences without labeling would allow all learners to flourish. Therefore, an inclusive curriculum and delivery would enable these potential barriers to be eliminated for learners’ academic achievement.
It should also be noted that the majority of students who are currently studying/completing dental school belong to the so-called “Generation Z” born between 1996 and 2012 (Eckleberry-Hunt et al., 2018). This generation was described as “hyperconnected to computers and Internet,” and has “expectations of global learning opportunities.” Therefore, it is crucial to acknowledge that the current generation may have different learning expectations in comparison with previous generations. In addition, the use of technologies such as artificial intelligence during online educational platforms may allow the identification of clinical and professional behaviors of students and this can then be modeled for future learners (Davey, 2020; Marshall and Wolanskyj-Spinner, 2020). However, there is a lack of evidence with respect to the “Generation Z” dental students and their learning experiences.
Post-COVID-19 era, there is also a unique challenge for educators and learners due to the lack of clinical practice and heavily relying on online methods of teaching. Despite continuous efforts, the inclusion of neurodiverse learners has not yet resulted in significant universal outcomes. However, the introduction and implementation of innovative and holistic approaches in the dental curriculum would enable and improve inclusive dental education. Therefore, the implication of the results from this study on planning and financing of programmes can be discussed in Higher Education.
There are limitations to this study related to data collection. The study consisted of an online survey alone. The face-to-face interviews and/or focus groups would have provided detailed information about the research question. However, this study was carried out pre-COVID-19 pandemic and was initially aimed to provide evidence with hybrid learning. Therefore, an online survey with a large sample size was the appropriate form of data collection to address the aim of this study. Another limitation was that the current study also represented a cross-sectional view of undergraduate dental students’ perceptions in Years 3–5 about lecture formats in one dental school during the pre-COVID-19 period.
A collection of demographic data would also enable researchers to correlate learning preferences according to age, gender, and socio-demographic background. Further research with focus groups and/or structured interviews is required to understand the learning experiences in relation to different lecture formats using different types of technologies such as virtual reality and artificial intelligence. The inclusion of different dental schools and years would also be invaluable.
This study provides valuable information on inclusive education to understand the learning experiences of Years 3–5 undergraduate dental students. The importance of two-way communication and understanding the needs of students should not be underestimated. Educators are required to be receptive to constructive feedback and adaptive to the neurodiversity of students to ensure robust and engaging learning experiences. Strategies for inclusive education in Higher Education could start with the consideration of different delivery formats and providing a safe environment to start the conversation for open, encouraging, and constructive student feedback.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Queen Mary University Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
AB carried out the data collection, analysis, and writing. UN performed the review and further editing process. Both authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Amir, L. R., Tanti, I., and Maharani, D. A. (2020). Student perspective of classroom and distance learning during COVID-19 pandemic in the undergraduate dental study program Universitas Indonesia. BMC Med. Educ. 20:392. doi: 10.1186/s12909-020-02312-0
Biggs, J. (2002). Constructive alignment: A guide for busy academics. New York, NY: LTSN Generic Centre.
Bradbury, N. (2016). Attention span during lectures: 8 seconds, 10 minutes, or more? Adv. Physiol. Educ. 40, 509–513. doi: 10.1152/advan.00109.2016
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Brown, G., and Manogue, M. (2001). AMEE medical education guide no. 22: Refreshing lecturing: A guide for lecturers. Med. Teach. 23, 231–244. doi: 10.1080/01421590120043000
Camacho, D., and Legare, J. (2021). Pivoting to online learning-the future of learning and work. J. Competency Based Edu. 6:e1239. doi: 10.1002/cbe2.1239
Cassidy, S. (2004). Learning styles: An overview of theories, models, and measures. Educ Psychol. 24, 419–444.
Chaplin, S. (2009). Assessment of the impact of case studies on student learning gains in an introductory biology course. J. Coll. Sci. Teach. 39, 72–79.
Chavarría-Bolaños, D., Gómez-Fernández, A., Dittel-Jiménez, C., and Montero-Aguilar, M. (2020). E-learning in dental schools in the times of COVID-19: A review and analysis of an educational resource in times of the COVID-19 pandemic. Odovtos 22, 69–86.
Clarke, V., and Braun, V. (2013). Successful qualitative research: A practical guide for beginners. Successful qualitative research. London: SAGE Publication, 1–400.
Coffield, F., Moseley, D., Hall, E., and Ecclestone, K. (2004). Should we be using learning styles?: What research has to say to practice. London: Learning & Skills Research Centre.
Davey, L. (2020). Exploring the subjectivities of people with alopecia areata - a critical qualitative study to inform applied psychology practice. (Thesis). Bristol: University of the West of England.
Davis, N. L., Gough, M., and Taylor, L. L. (2019). Online teaching: Advantages, obstacles, and tools for getting it right. J. Teach. Travel Tour. 19, 256–263.
Divaris, K., Barlow, P. J., Chendea, S. A., Cheong, W. S., Dounis, A., Dragan, I. F., et al. (2008). The academic environment: The students’ perspective. Eur. J. Dent. Educ. 12, 120–130.
Eckleberry-Hunt, J., Lick, D., and Hunt, R. (2018). Is medical education ready for generation Z? J. Grad. Med. Educ. 10, 378–381.
Ellaway, R., and Masters, K. (2008). AMEE guide 32: E-Learning in medical education Part 1: Learning, teaching and assessment. Med. Teach. 20, 455–473. doi: 10.1080/01421590802108331
Elledge, R., Williams, R., Fowell, C., and Green, J. (2020). Maxillofacial education in the time of COVID-19: The West Midlands experience. Br. J. Oral Maxillofac. Surg. 60:52–57. doi: 10.1016/j.bjoms.2020.07.030
Fleming, N. D., and Mills, C. (1992). Not another inventory, rather a catalyst for reflection. Improve Acad. 1992, 137–155.
Garrison, D. R., and Kanuka, H. (2004). Blended learning: Uncovering its transformative potential in higher education. Internet Higher Educ. 7, 95–105.
Grainger, B. (2013). University of London International Programmes: MOOC Report. London: University of London.
Hake, R. R. (1998). Interactive-engagement versus traditional methods: A six-thousand-student survey of mechanics test data for introductory physics courses. Am. J. Phys. 66, 64–74.
Harris, P., Connolly, J. F., and Feeney, L. (2009). Blended learning: Overview and recommendations for successful implementation. Ind. Commer. Train. 41, 155–163. doi: 10.1016/j.nepr.2017.09.011
Hew, K. F., and Lo, C. K. (2018). Flipped classroom improves student learning in health professions education: A meta-analysis. BMC Med. Educ. 18:38. doi: 10.1186/s12909-018-1144-z
Horvath, Z., O’Donnell, J. A., Johnson, L. A., Karimbux, N. Y., Shuler, C. F., and Spallek, H. (2013). Use of lecture recordings in dental education: Assessment of status quo and recommendations. J. Dent. Educ. 77, 1431–1442. doi: 10.1002/j.0022-0337.2013.77.11.tb05619.x
Huss, J. A., and Eastep, S. (2015). Faculty expectations toward their online courses: Are they on the same screen with their students? J. Inq. Action Educ. 6, 15–41.
Hussin, A. A. (2018). Education 4.0 made simple: Ideas for teaching. Int. J. Educ. Literacy Stud. 6, 92–98. doi: 10.1039/d1nr05090g
Institute of Medicine (US) Committee on the Future of Dental Education (1995). Dental education at the crossroads: Challenges and change, ed. M. Field (Washington, DC: National Academies Press).
Kauffman, J. M. (2021). The promises and limitations of educational tiers for special and inclusive education. Educ. Sci 11:323. doi: 10.3390/educsci11070323
Knight, J. K., and Wood, W. B. (2005). Teaching more by lecturing less. Cell Biol. Educ. 4, 298–310. doi: 10.1187/05-06-0082
Laurillard, D. (2002). Rethinking university teaching: A conversational framework for the effective use of learning technologies, 2nd Edn. London: Routledge. doi: 10.4324/9781315012940
Marshall, A. L., and Wolanskyj-Spinner, A. (2020). COVID-19: Challenges and opportunities for educators and generation Z learners. Mayo Clin. Proc. 95, 1135–1137. doi: 10.1016/j.mayocp.2020.04.015
Michael, J. (2006). Where’s the evidence that active learning works? Adv. Physiol. Educ. 30, 159–167. doi: 10.1152/advan.00053.2006
Moore, S., Armstrong, C., and Pearson, J. (2008). Lecture absenteeism among students in higher education: A valuable route to understanding student motivation. J. High. Educ. Policy Manag. 30, 15–24. doi: 10.1080/13600800701457848
Moriña, A. (2017). Inclusive education in higher education: Challenges and opportunities. Eur. J. Spec. Needs Educ. 32, 3–17. doi: 10.1080/08856257.2016.1254964
Nowell, L. S., Norris, J. M., White, D. E., and Moules, N. J. (2017). Thematic analysis: Striving to meet the trustworthiness criteria. Int. J. Qual. Meth. 16, 1–13. doi: 10.1177/1609406917733847
Rich, J. L., Chojenta, C., and Loxton, D. (2013). Quality, rigour and usefulness of free-text comments collected by a large population based longitudinal study - ALSWH. PLoS One 8:e68832. doi: 10.1371/journal.pone.0068832
Rowe, M., Frantz, J., and Bozalek, V. (2012). The role of blended learning in the clinical education of health care students: A systematic review. Med. Teach. 34, e216–e221. doi: 10.3109/0142159X.2012.642831
Sandelowski, M. (1986). The problem of rigor in qualitative research. Adv. Nurs. Sci. 8, 27–37. doi: 10.1097/00012272-198604000-00005
Schmitter, M., Liedl, M., Beck, J., and Rammelsberg, P. (2008). Chronic stress in medical and dental education. Med. Teach. 30, 97–99. doi: 10.1080/01421590701769571
Schonwetter, D. J., Gareau-Wilson, N., Cunha, R. S., and Mello, I. (2016). Assessing the impact of voice-over screen-captured presentations delivered online on dental students’ learning. J. Dent. Educ. 80, 141–148.
Scutter, S., Stupans, L., Sawyer, T., and King, S. (2010). How do students use podcasts to support learning? Aust. J. Educ. Technol. 26, 180–191.
Simpson, N. (2006). Asynchronous access to conventional course delivery: A pilot project. Br. J. Educ. Technol. 37, 527–537.
Singh, H. K., Joshi, A., Malepati, R. N., Najeeb, S., Balakrishna, P., and Pannerselvam, N. K. (2021). A survey of E-learning methods in nursing and medical education during COVID-19 pandemic in India. Nurse Educ. Today 99:104796. doi: 10.1016/j.nedt.2021.104796
Spickard, A. III, Alrajeh, N., Cordray, D., and Gigante, J. (2002). Learning about screening using an online or live lecture: does it matter? J. Gen. Int. Med. 17, 540–545. doi: 10.1046/j.1525-1497.2002.10731
The General Dental Council [GDC] (2015). Preparing for practice. Dental team learning outcomes for registration. London: GDC.
Tormey, R., and Henchy, D. (2008). Re-imagining the traditional lecture: An action research approach to teaching student teachers to ‘do’ philosophy. Teach. High. 13, 303–314. doi: 10.1080/13562510802045337
Keywords: inclusive education, academic lectures, online education, face-to-face teaching, blended learning
Citation: Baysan A and Naeem U (2023) Inclusive education: pedagogical approach to online versus face-to-face teaching. Front. Educ. 8:1148344. doi: 10.3389/feduc.2023.1148344
Received: 20 January 2023; Accepted: 21 July 2023;
Published: 22 September 2023.
Edited by:
Netilia Silva Dos Anjos Seixas, Federal University of Pará, BrazilReviewed by:
Angélica Monteiro, University of Porto, PortugalCopyright © 2023 Baysan and Naeem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aylin Baysan, YS5iYXlzYW5AcW11bC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.