 Jia Liu
Jia Liu Katherine Miles1,2
Katherine Miles1,2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 06 October 2022
Sec. Language, Culture and Diversity
Volume 7 - 2022 | https://doi.org/10.3389/feduc.2022.980633
This article is part of the Research TopicTeaching and Learning in a Global Cultural ContextView all 5 articles
The COVID-19 pandemic and the escalation of the Black Lives Matter Movement worldwide have foregrounded the long-standing inequality in society and healthcare. The provision of culturally competent care has become more necessary than at any other time. However, cultural competence (CC) education remains inconsistent across medical schools, and little is known about how students develop their CC through campus-based classroom teaching. We took an ethnographic approach to study students’ development of CC in campus-based formal classroom teaching. This study was conducted in a large London medical school in England. We triangulated data collected from 6-month participant observation, 25 individual interviews, and three focus groups to generate reliable accounts of students’ CC developmental experience. Thick descriptions were developed through iterative, inductive, interactive, and reflexive review and interpretation of data using NVivo 11. The results show that students undergo staged cultural learning throughout their undergraduate medical curriculum through bespoke CC lectures, workshops, clinical/research projects, and integrated clinical simulations that incorporate CC and other clinical subjects. The early learning mainly takes place in the pre-clinical year of the curriculum, among which a range of valued-based sessions is observed as conducive to students’ development of CC. As they progress, students develop their CC by attending clinical sessions with embedded cultural content. The curriculum in senior years presents reduced mandatory teaching, but more clinical exposure and opportunities to reach out to other subjects and disciplines. It means students start to have more diverse and dispersed learning experiences based on their individual choices, some of which may contribute to their development of CC. This study provides a rare insight into medical students’ CC development through participation in campus-based classroom teaching. Various learning opportunities contribute to different aspects of CC development and cater to different learning preferences of the diverse student population. To support students’ comprehensive development of CC, educators need to work collaboratively and use overt signposting to related disciplines and subjects. There needs to be recognition of students’ learning not only in the formal curriculum but also in the informal and hidden curricula.
The COVID-19 pandemic and the escalation of the Black Lives Matter (BLM) Movement worldwide have foregrounded the long-standing inequality in society and healthcare, making the provision of culturally competent care more necessary than at any other time. This requires medical and other health students to develop cultural competence (CC) in order to prepare for an increasingly diverse patient population, both culturally and linguistically. The wider drivers for cultural competence education in medicine and healthcare are important in the consideration of global healthcare, the movement of people, and the demand for healthcare professionals to care sensitively and compassionately for patients regardless of beliefs, values, and languages that may be different from their own.
The provision of culturally appropriate care is viewed as essential to creating a healthcare system and workforce that can deliver accessible and effective healthcare for people regardless of their backgrounds (Brach and Fraserirector, 2000; Betancourt, 2003; Betancourt et al., 2005). The Lancet paper on Culture and Health (Napier et al., 2014) acknowledges that health is inseparable from cultural perceptions of wellbeing, and cultural competence needs to be considered as a domain of medical and health training. Regulatory and accreditation bodies for medical training in many countries worldwide have established standards that require cross-cultural curricula as part of undergraduate medical education. These include stipulations such as the Tomorrow’s Doctors published by the General Medical Council in the UK1, the Standards for Assessment and Accreditation of Primary Medical Programs by the Australian Medical Council2, the Outcomes and Standards for Undergraduate Medical Education in Singapore by the Singapore Medical Council3 and the Functions and Structures of a Medical School by the Liaison Committee on Medical Education in the United States and Canada4. These stipulations and guidelines have given added impetus and emphasis to medical schools to introduce or enhance CC teaching in their medical curriculum.
Although the term Cultural Competence is widely used to underpin cross-cultural curricula and diversity education in medicine and healthcare (Green et al., 2002; Betancourt, 2003; Dogra et al., 2010), it remains conceptually contested. It was first used by Cross (1989), who defines it as “a set of congruent behaviors, attitudes, and policies that come together in a system, agency or among professionals and enables that system, agency or those professionals to work effectively in cross-cultural situations” (p. 2). Since then, scholars have attempted to define this term from different perspectives, coming up with a multitude of key cultural competence attributes (Srivastava, 2007). Burchum (2002) specified six essential attributes of CC, namely cultural awareness, cultural knowledge, cultural skill, cultural sensitivity, cultural interaction, and cultural understanding. Balcazar et al. (2009) listed four attributes of CC: cultural desire, cultural awareness/knowledge, cultural skill, and cultural support. Campinha-Bacote (2002) points out five constructs: cultural awareness, cultural knowledge, cultural skills, cultural encounters, and cultural desire. Alternative terms to cultural competence are also proposed, such as cultural sensibility, cultural humility, critical consciousness and cross-cultural efficacy (Tervalon and Murray-Garcia, 1998; Núñez, 2000; Dogra, 2003; Kumagai and Lypson, 2009).
In our earlier publication, we discussed the various terminologies around cultural competence (Liu et al., 2021). Although many terms have been used to underpin cultural education in healthcare, the ultimate goal is to train students to “communicate effectively and care for patients from diverse social and cultural backgrounds, and to recognize and appropriately address racial, cultural, gender and other sociocultural relevant biases in healthcare delivery” (Betancourt, 2003). In this paper, we use the term Cultural Competence or CC in an encompassing manner to incorporate relevant theories and concepts in this field. In our view, the identified components around cultural competence can be generally categorized into three interdependent domains – affective, cognitive and behavioral (Liu et al., 2021). The affective development of CC refers to the self-motivation and willingness to explore new cultural ideas and view differences positively and without judgment. The cognitive domain of CC requires individuals to consciously self-assess their perspectives such as ethnocentric, biased, and prejudiced beliefs toward others, as well as the gradual acquisition of cultural information and their implications on health provision and health behaviors. The behavioral domain of CC refers to effective communication and other behavioral capabilities/skills to resolve cultural conflicts and provide culturally appropriate healthcare to people from diverse cultural backgrounds.
Teaching around cultural competence remains inconsistent across medical schools (George, 2015; Dogra et al., 2016). There is a lack of consensus on what domains of cultural competence should be taught, and less is known about what is currently being taught. There are limited studies that have comprehensively looked at the current teaching around CC and diversity across medical schools, with the majority of existing studies originating from North America and Europe. A few existing studies (Dolhun et al., 2003; Betancourt et al., 2005) conclude that CC education in most medical schools aims to teach the general themes of culture, the doctor-patient relationship, clinical communication, equality and racism, and specific cultural information/knowledge pertaining to the ethnic communities they serve. However, sparse guidance is available for educators to design or implement a CC curriculum. A study titled Teaching cultural diversity: current status in U.K., U.S., and Canadian medical schools concludes that both British and North American medical schools are encountering a lack of conceptual clarity over the meanings of CC and diversity and how these concepts can be framed in teaching (Dogra et al., 2010). This conceptual ambiguity may lead to a gap in faculty training, prompting medical schools to devise their own pedagogical methods, formats and structure in addressing CC and diversity (Dogra et al., 2016).
The cross-disciplinary roots of cultural competence and diversity teaching means that contributed teaching is not being clearly identified (Dogra et al., 2016). CC teaching is closely linked with many value-based medical subjects, such as clinical communication, professionalism and interprofessional education. CC relevant content may also be embedded in a wide range of clinical and academic disciplines, such as primary care, psychiatry, palliative care, public health and social science subjects (Dogra et al., 2016). Multi-disciplinary input facilitates valuable comprehensive and interconnected teaching, as each discipline offers a different perspective for understanding culture and culturally appropriate care. For instance, social sciences subjects, such as sociology, language studies and political science, may contribute to students’ knowledge of cultural issues through the cross-disciplinary exploration of issues around diversity, equality, policy-making and patients’ lived experience (Dogra et al., 2016). However, whether the cross-disciplinary input may create challenges for educators and students to integrate the teaching resources remains under-discussed in existing literature.
In CC teaching, a variety of teaching methods can be used so that students can explore their attitudes, increase their knowledge, and develop relevant skills (Dogra et al., 2016). The study of Dolhun et al. (2003) shows most American medical schools utilize common pedagogic techniques by offering a didactic component and encouraging active student participation through case studies and group-based discussions. However, there are considerable variations in CC teaching across medical schools (Brown and Manogue, 2001; Dolhun et al., 2003). The delivery of teaching may be influenced by the interest of staff and the resources available (Dogra et al., 2016). There are also variations across teaching areas, with some medical schools focused extensively on certain areas which others neglect (Dogra et al., 2010).
Given the innate complexity of CC and diversity education, the development of a range of tools to effectively assess the various components of CC is demanded. Existing assessment methods include multiple-choice questions, short answer questions, essays, reports, reflective portfolios and questionnaires (Dogra et al., 2016). Multiple-choice questions, questionnaires and short answer questions can help to embed CC and diversity into a wider range of clinical subjects. However, using these as assessment tools may reinforce the view that CC and diversity education is merely about acquiring a body of relevant knowledge (Dogra et al., 2016). These questions also need to be carefully designed and validated so as not to reinforce pigeonholing or stereotyping (Dogra et al., 2016). The most common form of written assessments is through the production of essays and reflective portfolios, which allow students to self-reflect on their clinical learning in relation to CC. In addition, there is a greater demand to incorporate relevant cultural elements in objective structured clinical examination (OSCE) stations so that students will be prepared to face the cultural and linguistic differences encountered when interacting with diverse patient communities (Altshuler and Kachur, 2001).
To summarize, the importance of cultural competence education in medicine and healthcare has been largely recognized throughout medical schools globally, but training remains inconsistent across structure, content and process. Little is known about how students develop their CC. Given the underdeveloped understanding of training and support to prepare medical students for culturally competent practice, it becomes clear that further study is required. This research, as part of a larger research project, aims to provide a rich ethnographic description of students’ experiences of learning and developing cultural competence in the formal classroom setting. The results of this ethnographic work provide insights into the personal experiences and multi-faceted factors around CC development among medical students who themselves come from culturally diverse backgrounds. As a result of increased understanding in the context of medical education, evidence-based arguments are formed to inform curricula development.
Ethnography was adopted as it allows researchers to explore cultural phenomena and examine behaviors of participants in given social contexts by focusing on social interaction and participants’ interpretation of their own behaviors (Murchison, 2010). For this research, an ethnographic approach enabled us to bridge the distance between our interpretation and the meaning of students’ life experiences that may contribute to their development of CC. The investigation of CC development among medical students required a close and systematic exploration of their behaviors and views, for which ethnography offered a unique way for examination via deep immersion and first-hand data collection. As a “toolbox of methods,” ethnography involves understanding how to best combine different methods or complement one method with additional ones to develop a comprehensive understanding of the phenomenon (Murchison, 2010).
This ethnographic study utilized participant observation, in-depth interviews and focus groups with participating undergraduate medical students enrolled in a London medical school. Ethical approval was granted in November 2017 (LRS-17/18-5013). Gatekeeper approval was granted by the director of Educational Research and Innovation at the chosen medical school, so the authors were allowed to observe relevant campus-based teaching activities.
This research was conducted in a medical school in central London. The setting is ideal for this research because it has three distinctive characteristics. First, the medical school is located in an area with a socially, culturally and linguistically diverse population, which allowed the authors to better capture the innate complexity of students’ experience of cultural diversity and cultural competence development. Second, the medical school has a student body that represents the breath of different racial, ethnic, linguistic and other sociocultural backgrounds. The diverse student population was considered relevant as previous literature showed that students from culturally and linguistically diverse backgrounds demonstrate different learning features (Abu-Arab and Parry, 2015). Third, the medical school has clear institutional support for cultural competence. It has a longitudinal cultural competence curriculum threaded across a 5-year Bachelor of Medicine and Bachelor of Surgery (MBBS) program. The relatively comprehensive CC curriculum helped the authors to gain a more comprehensive understanding of students’ development of CC in the classroom setting within a limited single-site case study. The strong institutional support in the medical school was demonstrated by the presence of a nominated academic lead on cultural competence and the ready access to relevant curriculum information on its official website.
Accessing campus-based formal classroom teaching was facilitated through the authors’ communication with relevant academic staff after gaining the gatekeeper approval from within the chosen medical school. Access to the teaching sessions was obtained from the corresponding module leads and instructors to introduce our research purpose.
JL undertook the primary role in data collection, which involved collecting data through conducting participant observation, individual interviews and focus groups. First, JL conducted 6-month participant observation (Jan 2018-July 2018) to observe students’ experiences of cultural competence learning in relevant teaching activities, including lectures, workshops, and project-based seminars with both direct and indirect links to teaching cultural competence. All instructors (e.g., lecturers, facilitators, patient educators and guest speakers) in the observed sessions allowed JL to observe their teaching sessions as a participant-observer. Some instructors in small group teaching sessions (e.g., workshops, seminars, clinical simulations) introduced JL to the students and briefly introduced the background of the research at the beginning of their teaching sessions. To collect data, fieldnotes were produced to record JL’s observation of students’ learning in light of relevant learning materials (e.g., official learning outcomes, students’ assignments and online learning resources). Based on Spradley’s (1979) nine observational dimensions in ethnography, an observational template (see Supplementary material 1) was formulated, which included the aspects of module background, teaching topic, space, time, participants, learning outcomes, teaching format, teaching activities, CC-related teaching content, pedagogy, students’ feedback and JL’s refection as an ethnographer.
Furthermore, 25 semi-structured individual in-depth interviews (each lasted around 25–35 min) were conducted simultaneously along with JL’s participant observation. The interviews were audio-recorded by an encrypted audio recorder and were transcribed. The interviews allowed the authors opportunities to explore their views and lived experiences of CC development in great depth. The question guide (see Supplementary material 2) covered topics such as students’ understanding of CC recognition in their medical school and university, their experiences with CC curriculum and feedback, and their general cultural learning experiences beyond classroom-based teaching. Based on a framework of pre-determined questions and themes, the semi-structured interviews allowed flexibility for new ideas to be brought up. In addition, three 1.5–2 hour focus groups (4–8 participants for each group) were conducted to member-check the results generated from the observation and interviews. The question guide (see Supplementary material 3) of the focus groups was based on the preliminary findings of JL’s participant observation and from the interviews. The focus groups were audio-recorded and were transcribed. They aimed to triangulate and further supplement data generated from other research methods.
Participants for the three research activities were recruited via different means including face-to-face recruitment, public advertisement and snowballing. Table 1 summarizes the participant recruitment and data collection.
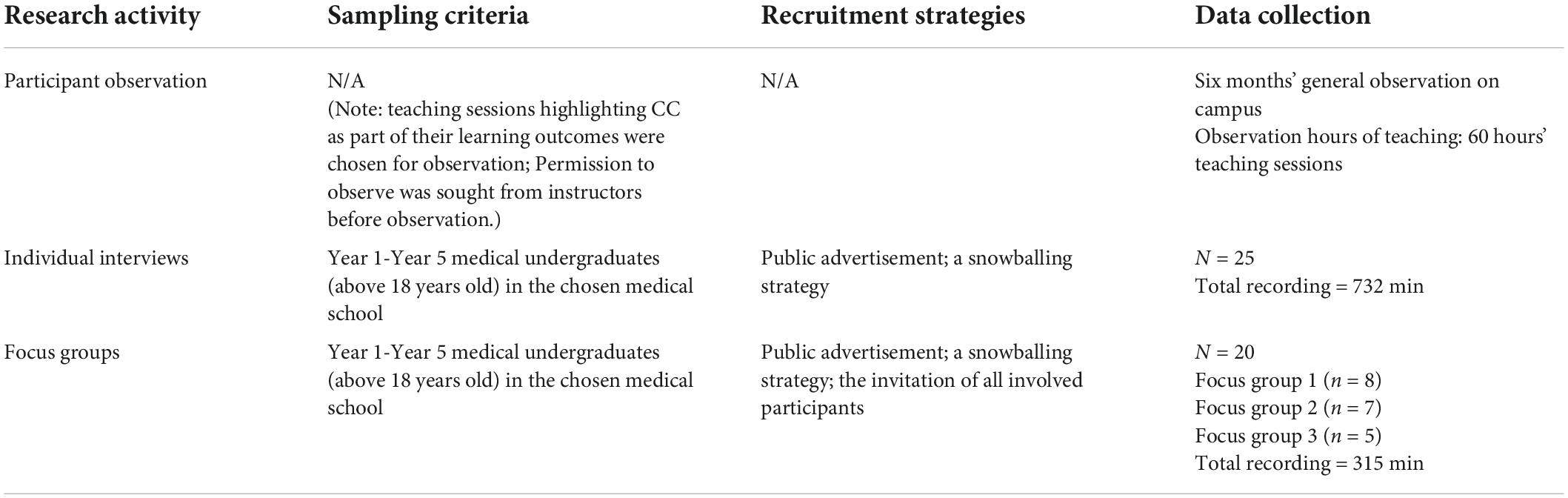
Table 1. Participant recruitment and data collection.
The authors reviewed the fieldnotes, interview transcripts and focus group transcripts using an iterative, inductive and reflexive approach to facilitate interpretation. The five steps of data synthesis were: (1) organizing the data; (2) reading and memoing the data; (3) describing the data; (4) analyzing the data; and (5) interpreting and presenting the data. Regular meetings were held among the authors to discuss interpretations and consider alternative explanations. Documentation throughout the data collection and analysis was randomly checked by SL to ensure consistency. Individual ethnographic accounts and narratives were formed by integrating the data. Combining fieldnotes with quotes from interview/focus group participants provided complementary details and explanations. Excerpts from interviews and focus groups were edited for improved readability and incomprehensible or irrelevant text was deleted and replaced with three dots in square brackets […]. All participants were anonymized. The demographic information of participants is provided in Tables 2, 3.
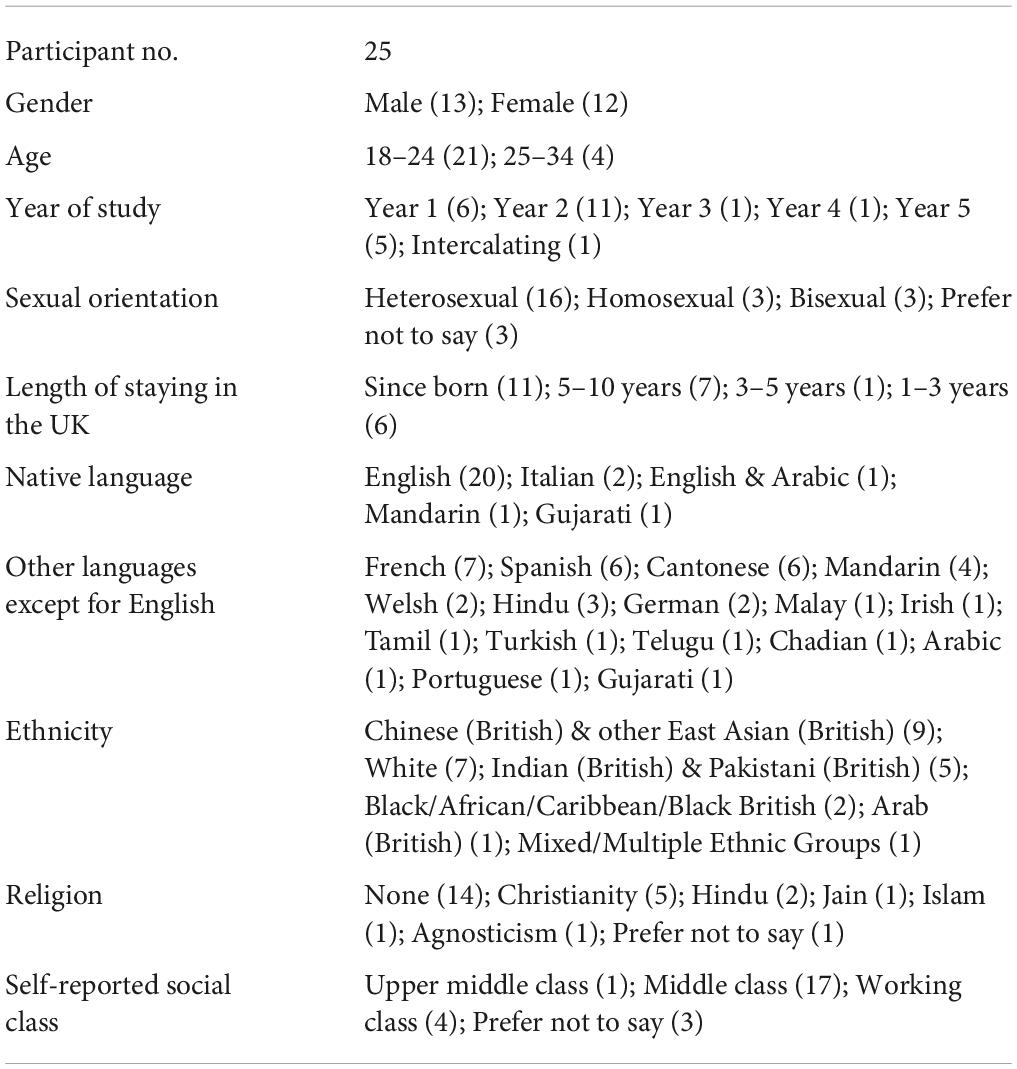
Table 2. Demographic information of interview participants (n = 25).
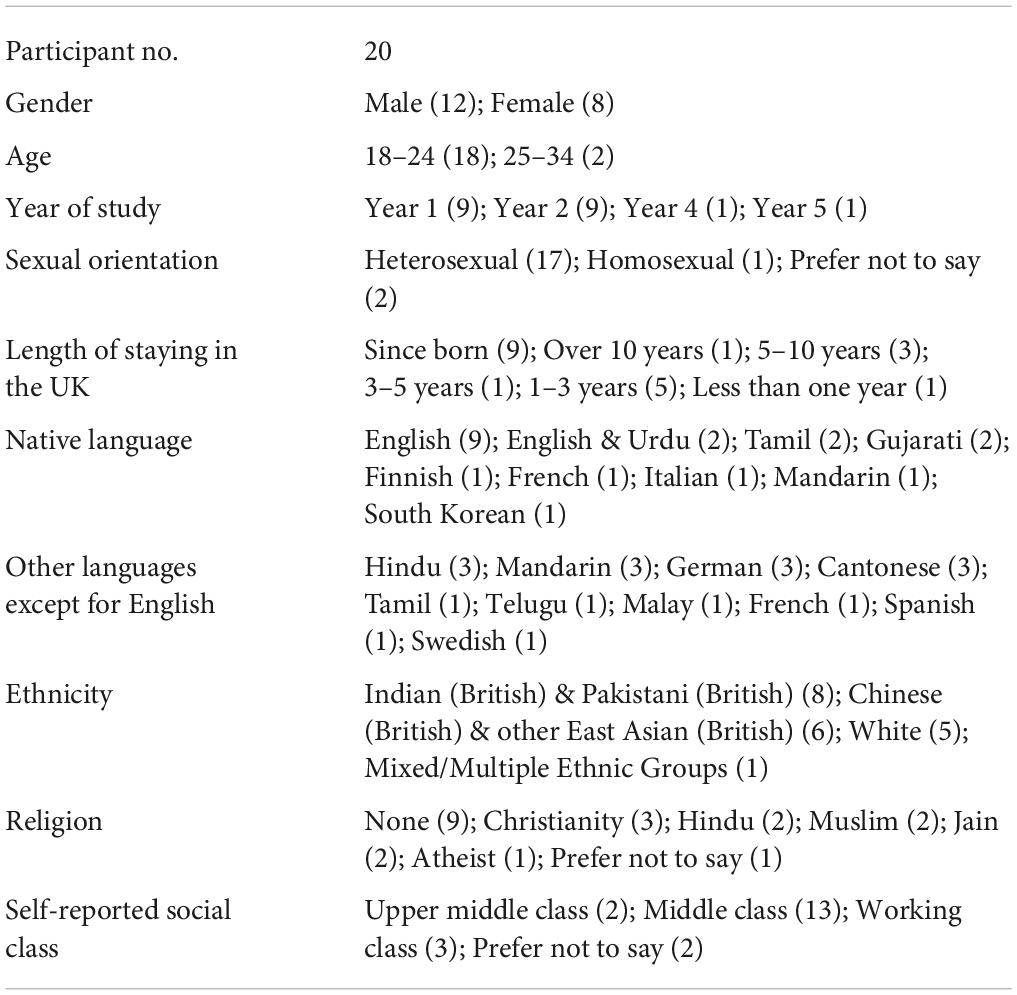
Table 3. Demographic information of focus group participants (n = 20).
The authors maintained a reflective stance, using an active approach to understand the representation or interpretation bias of this research. The awareness of keeping a reflexive mind encouraged us to reflect on our own biases that may be related to our roles, any past experiences, preconceptions, prejudice or cultural orientations. Throughout the research project, this reflexive process helped us evaluate our impact as ethnographers. It also contributed to the trustworthiness of this research.
In this research, JL independently carried out participant recruitment, data collection and analysis, supported by KM and SL. Reflecting on our participant recruitment helped us decide on a range of recruitment strategies as JL felt that her personal cultural background could have impacted these activities. When approaching potential participants, JL reflected she felt it easier to approach students with some shared cultural elements, such as students who are from similar ethnic, linguistic and cultural backgrounds. Acknowledging this potential bias in participant recruitment, the authors used diverse recruitment strategies (e.g., snowballing or recruiting participants through official university newsletters) to reach a group of participants with more diverse sociocultural backgrounds.
Being reflexive also required us to actively reflect on the dynamics between the researchers and participants during the process of data collection in different research environments, particularly during interviews and focus groups where face-to-face communication resided on trust. JL’s role as a doctoral student during the delivery of this research allowed her to quickly build rapport with participants. It proved to be a positive approach and a flat platform to encourage students to open communication. During the interviews, JL felt that positive relationships between the participants were evident because students were comfortable discussing topics and ideas frankly. For all three focus groups, student participants were highly active in discussions and yielded useful information, but different dynamics were noted with the presence of different facilitators. SL’s identity as an academic created an observable power asymmetry with his focus group students. Students in his group were inclined to express agreement and appraisal of their positive CC learning experiences. They were also likely to refer to the terminology they learned from their CC sessions. In contrast, for the other two focus groups that were facilitated by JL and another doctoral student, participants were more likely to voice critical opinions and the language tended to be less formal with constant reference to their inside stories as medical students. The participants in these focus groups also mentioned that they would not discuss some of the topics if the focus group was facilitated by a staff member who also teaches them for fear that some of the remarks might “upset the staff member.” In view of these points and potential conflict of interest, SL was not involved in the rest of data collection but only looked at anonymized data throughout the project to minimize any potential coercion. Moreover, he also dissociated from students’ assessment in any coursework that were related to the teaching of cultural competence.
During data analysis, JL acknowledges that she has used her feelings aroused from both the “etic” and “emic” stances to interpret the research findings (Murchison, 2010). This means sometimes JL’s understanding of a phenomenon as an observer may conflict with her feeling as a participant, therefore, it required her to make sense of the potential discrepancies in order to gain a more comprehensive view of students’ learning. For example, “putting on” the identity of a medical student, JL felt excited to learn all the relevant clinical knowledge and skills but neglected some occurred cultural learning that was taking place simultaneously (e.g., students’ in-class discussion of patients’ expectations from doctors in different cultural contexts). However, as a relatively objective observer, JL was able to note down these relevant learning opportunities. Phenomena as such required JL to constantly switch between the two stances and attempt to achieve a healthy balance between her participation and observation. By constantly thinking between a participant and an observer, JL managed to use her data analytical framework in a flexible manner, to remain open to alterations, to avoid overlaps, and to consider previously unavailable and unobservable categories. To deal with the potential bias in the process of data analysis, SL and KM randomly selected and checked content under certain coding categories to ensure consistency. Regular discussions among the authors were held on how to understand the codes and emerging themes.
SL as lead in cultural competence teaching in the medical school influences the design of the project. His insight into CC as a subject matter and into students’ learning benefited the research design, but at the same time, the authors were mindful of the potential imposition of pre-existing knowledge upon the interpretation of data. Therefore, JL had regular meetings with SL to discuss the different aspects of data interpretation using the anonymized data. This maximized the use of SL’s expertise without compromising the integrity and rigor of this research. Similarly, the authors recognized the limitations and potential biases that KM’s cultural experiences and knowledge could bring as a lecturer in clinical communication in an external medical school but also a doctoral student in this medical school. Working collaboratively and holding regular meetings among the authors helped to minimize hidden biases or misconceptions and maximize the authors’ insider and outsider knowledge and perspectives.
The results show that a strong institutional recognition on diversity, equality and inclusion is conducive to students’ development of CC. Students develop their CC following a longitudinal process through participating in the curriculum teaching in different formats. They also pick up cultural learning via sharing lived experiences.
Support and recognition of CC education at an institutional level benefits students’ development of cultural competence. As for the chosen medical school, its readiness of developing/enhancing the CC curriculum is noticed through academic leadership, curriculum development and faculty development. Our observation shows that the multi-level infrastructure of academic leadership at the medical school has facilitated the incorporation of CC as a subject. At the management level, the then Deputy Dean brought in an enhanced strategic approach to integrate CC as a subject with formal recognition in the curriculum. At the curriculum level, an academic lead is appointed to oversee CC curriculum design and delivery. At the research level, various educational/research projects were undertaken to explore the diversity issues both in the student and patient body, such as the decolonization of the medical curriculum in order to reflect a more diverse patient population, and the attainment gaps of the Black, Asian and Minority Ethnic (BAME) students.
The medical school was undergoing a curriculum review when this research was conducted. The new curriculum has a renewed focus on value-based medicine, among which Cultural Competence is included as a key learning outcome. A series of efforts were observed that may enhance the faculty development around teaching cultural competence. Designated staff in the medical school also actively participate in relevant academic groups that advocate CC and diversity education in healthcare, such as the Diversity in Medicine and Healthcare (DIMAH) group. In addition, the medical school runs a Master of Arts (MA) program on Clinical Education, within which there is a module on intercultural clinical education led by SL and delivered to clinical trainers from across the UK.
The school has a committee for Development, Diversity, and Inclusion (DDI), aiming to provide staff and students with a platform to identify equality and diversity challenges in order to create an inclusive, fair and equal community. Various institutional schemes were taking place, such as widening participation, tackling discrimination, and promoting gender equality. These schemes contribute to building a culturally inclusive environment, making the development of CC a more prominent subject. For instance, the medical school has a long-established widening participation medical program, which supports pupils from underrepresented backgrounds to get into studying medicine. This 6-year Extended Medical Degree Program (EMDP) “levels the educational playing field.” Students’ views on these schemes are generally positive as they consider these schemes as offering opportunities for them to enhance interaction with people from more diverse backgrounds. Interview Participant 13 said:
I definitely think the widening participation is really good, especially in medical school. […] Because that’s such a private school dominated course. They do outreach sessions, basically to poor and disadvantaged schools to talk about “Do you want to get to medical school? We are going to help you with it.” […] The more diverse a medical school, almost the fewer efforts you have to put into cultural competence [training] because people will learn from their peers. That automatically goes quite a long way.
However, there is also the possibility that the institutional labeling of students with certain backgrounds may reinforce unconscious cultural stereotypes and disadvantage the group of students. Whether the unconscious stereotypes of students with certain sociocultural features may act as hurdles to students’ personal and professional development remains under researched.
We found that students undergo staged cultural competence development throughout their curriculum: an early start, then deeper in the fields, and lastly, reaching out to respective fields. The early learning mainly takes place in the pre-clinical year of the curriculum, among which a range of value-based sessions are observed as conducive to students’ development of CC. As they progress into later years, students develop their CC by attending clinical sessions with embedded cultural content. The curriculum in senior years presents a reduced amount of mandatory teaching, but more clinical exposure and opportunities to reach out to other subjects/disciplines. It means students start to have more diverse and dispersed learning experiences based on their individual choices, some of which may contribute to their development of CC.
Results show that theme-specific teaching on CC in the early years of the medical curriculum introduces the concept of CC to students. Other value-based medical subjects, such as clinical communication, professionalism and interprofessionalism, further contribute to students’ development of CC. In the medical school, theme-specific teaching on CC takes place in the Year 1 Value-Based Clinical Practice Module, among which Human Values (HV) is an introduction teaching block. The HV block aims to integrate medical human values with healthcare practice and bridge the gap between techno-centric and caring-based learning. It serves as a strand to encompass subjects such as clinical communication, medical ethics and law, professionalism and well-being, cultural competence, interprofessional education, and medical humanities.
Theme-specific teaching on CC includes a lecture and workshop. When reflecting on their learning in these sessions, students mentioned in the focus groups that the relatively interactive CC lecture, using online polls and video resources, enhanced their motivation to learn compared to a traditionally didactic lecture. However, several students mentioned in the interviews that the focus on cultural theories in the lecture weakens students’ interest to learn as students are more motivated to explore how medical practitioners can translate cultural training into practice. Following the CC lecture, the subsequent CC workshop provided a safer environment for students to reflect on their deeply rooted unconscious bias, which further enhanced their cultural sensitivity and awareness. This sequence of delivery on subject-specific teaching was appreciated by students. According to focus group Participant 4:
They gave us […] a stepwise guide which I guess was good. I’m pretty sure we had a lecture on this where we explored the topic of cultural competence and […] introduced us to the topic and then at the workshop. So, I thought [the] sequence of events is very well laid out.
The integrated simulated patient scenarios, where learning takes place in a confined but simulated environment, are noticed as the most effective to support students’ CC learning. Almost all students participating in this research acknowledged that integrated patient scenarios have enhanced their CC. In the HV block, CC is integrated as a key learning outcome in simulated patient scenarios. Cultural elements are integrated into the design of these scenarios, covering topics such as cultural preferences in healthcare seeking, religious differences in death rituals, gender and sexuality, and communication with patients of limited English language ability. JL observed that as students participate in simulated patient scenarios, they start to demonstrate an enhanced level of cultural awareness, attitudes, knowledge and skills. According to Interview Participant 1:
I think having patient scenarios would really help because once again you’re experiencing it, you’re actively listening or asking questions. I guess that really helps because […] it can bring up a lot of topics you can discuss afterward or even with the patient there, and discuss with them their culture, their belief, and their views and thoughts.
Some students expressed that these patient scenarios have prepared them to deal with similar cultural challenges in clinical placements. Interview participant 7 shared how one patient scenario prepared her for interacting with similar patients in the clinical setting and demonstrating non-judgment through understanding:
I once met a patient. She was a sex worker who was an immigrant. […] I couldn’t really understand why she would choose to do this occupation here. But understanding her situation, like how […] desperate she was for a job, and how she wanted to meet more people from where she was, how she wanted that sense of community with the other sex workers as well. […] That’s interesting because that really reminds me of one of the scenarios we had, exactly the same scenario. Some of the patient’s words are so familiar as these are what we have discussed in that scenario.
Moving from the early contact of CC in the pre-clinical year, students develop their CC by attending clinical sessions with culturally embedded content. The campus events under the General Practice longitudinal placement, population science and students’ self-selected projects are used as cases to demonstrate how students can enhance their CC.
Observation of 2-day intensive training campus events under the General Practice longitudinal placement, with an introductory lecture and themed workshops, showed benefit for students’ development of CC by introducing them to a diverse range of cultural topics. The four themed workshops were case-based or discussion-led and topics included “homeless and inclusion health,” “LGBTQ+ issues,” “identifying and responding to domestic violence and abuse,” and “access to healthcare for patients with learning disabilities.” Taking the homeless session as an example, it was a collaborative session with teaching and experience sharing from five experts: a facilitator, a nurse, a sociologist, and two patients who were homeless. This collaborative session showed that from hearing guest speakers’ life experiences, together with the professionals’ explanation of homelessness, both as a sociocultural and health phenomenon, students enhanced their awareness and knowledge of how to work with homeless patients in a culturally appropriate manner.
Fieldnotes: This is a well-collaborated workshop on the topic of homelessness. […] Helen and Pete, who were homeless before, shared their experiences on how they became homeless […] When allowed to ask questions about Helen’s and Pete’s living experiences, many students remained quiet but extremely attentive. One student told JL after class that he felt he did not know what questions they should ask. Though “homelessness” is a familiar word, he has not realized the extent of the suffering of the group until this session, and how these can be related to a healthcare context, or they did not want to make Helen and Pete feel bad by asking inappropriate questions.
We found that teaching around public health, biostatics and epidemiology, continue to benefit students’ development of CC by exposing them to population-specific cultural knowledge. In a workshop on Population and Disease, the facilitator used a London borough as a case study to encourage students to explore the various dimensions of culture and the relationship between culture and health. Some categorical cultural facts were provided, such as the cultural knowledge that people of black Caribbean backgrounds have a higher risk of high blood pressure/strokes and Asians are more at risk of developing diabetes. Facilitated discussions around how these epidemiological patterns exist were addressed from the aspects of diet, health beliefs and other relevant cultural elements. More importantly, the facilitator emphasized that group-based cultural knowledge only applies at a populational level and does not immediately translate to individuals. In the group discussions, students exchanged their thoughts about acquiring cultural knowledge in a critical manner. According to Interview Participant 12:
Looking at this [demographic] figure and its implications on health, as medical students, we need to develop cultural competence. Having knowledge such as Asians might be more likely to develop diabetes, young people have higher risks of STI, which is only one component. It is also about the awareness that individuals are different. To be culturally competent, one needs to develop their cultural awareness, knowledge, and skills as a whole. Only by doing this can we become truly culturally competent.
Students can develop their CC through the involvement and management of projects, but this largely depends on students’ individual choices of projects. Our observation shows that students were involved in project-based learning on various occasions, including students’ self-selected components (SSCs), scholarly projects and clinical humanities projects. Taking the clinical humanities projects in Year 2 as an example, students are encouraged to think outside the box for health and healthcare using humanistic methods, such as photography, poetry, visual arts and embroidery.
Fieldnotes: In the session on clinical communication with visual methods, facilitator, who is a graphic designer, discussed the merits of using visual skills to communicate public health information to culturally diverse patients. The facilitator mentioned that it is necessary to use simple generic features so that these images can culturally relate to the general public. […] when drawing patients, a diversity of cultural elements needs to be represented, such as patients’ different ages, ethnicities, and religious backgrounds.
Students expressed that module-related online learning resources can benefit their development of CC. Examples included students mentioning they have acquired a better understanding of the cultural topics of “homelessness” “LGBTQ+ ” and “domestic violence” after accessing the online materials. However, despite the ready access to these materials, the use of these online resources varied among individual students. According to Interview Participant 21:
That [the online resources around LGBTQ+ issues] was very useful. Yeah, statistics do speak. […] But you know, as medical students, we are very busy, and there are so many resources out there. I’m not sure if other students have a chance to check the resources as well.
Our observation shows that the curriculum in senior years presents reduced mandatory teaching, but there is more clinical exposure and opportunities to reach out to subjects and disciplines. It means students start to have more diverse and dispersed learning experiences based on individual choices, some of which may contribute to their development of CC.
Some students expressed in the interviews that their intercalated degrees have enhanced their understanding of cultural diversity and expanded their relevant cultural knowledge and skills. Intercalating is often viewed as a way into academic medicine, as students may have the option to take a year off to study a different field or undertake research or education, such as through pursuing a bachelor’s degree. Those who had intercalated degrees in health-related subjects voiced that cross-disciplinary learning within the field of healthcare has enhanced their CC through enhancing their cultural awareness and gaining more cultural knowledge. For example, according to Interview Participant 25 who did an intercalated Bachelor of Science (BSc) in nutrition:
I did a year of intercalated BSc in nutrition, and then there was where it was talked about how different cultures have […] different cuisines, and some are more naturally nutritious than others, and you have to then speak to the patient quite respectfully about [it]. […] I did find it very helpful, and it was relevant to, you know, being a medical student and eventually being a doctor, but I only got that because I decided to do a nutrition degree.
Having an intercalated degree in non-health-related subjects, such as in arts and social science studies, benefits students’ CC development. For example, Interview Participant 23 mentioned that having an intercalated year in history has enhanced her critical thinking and critical awareness, which are key qualities to becoming culturally competent. Interview Participant 2, who did an intercalated degree in language studies, mentioned how learning a foreign language has helped him to understand a culture in great depth through the systematic learning of its language along with its shared values, beliefs and ways of behavior:
I suggest that everyone should try to learn a different language. It’s really not about speaking a foreign language with people from that culture. Instead, it is about understanding how the language came into being, what are the associated social and cultural elements. Also, in language studies, we have certainly been taught about the cultures of certain regions, which asked us to reflect on the cultural differences, […] and even our personal cultural bias. I guess through this I have developed my cultural competence in a way that I haven’t expected.
The Global Health Placements taking place in Year 5 of the curriculum offer great opportunities for cultural learning. Students expressed that through extended immersion during global health placements they have become more “modest” when facing diversity and started to understand that being sensitive to another culture requires being open to its dynamics, understanding its sociocultural structures, and recognizing other people’s beliefs about health and illness. According to Interview Participant 18, who completed his global placement in New Zealand:
I think in New Zealand they’re doing quite good in terms of cultural awareness, especially to the Maori population. […] The medical professionals, the nurses and the doctors, I think just from my brief observation, they seem quite well prepared in the way to talk with them, the Maori people. And also some of the leaflets, and because their cultural background is very different from the European one […]. In the medical setting […] like when the patient is ill and the way how they should convey the information to a Caucasian family, or a Maori, or a Chinese family is different. […] I think they, they’re quite considerate. There is quite a lot of information available and guidance about interaction. I think they pay quite a lot of attention.
Our observations show that drawing on the expertise of people with lived experiences benefits students’ development of CC as they bring cultural teaching to life. Students mentioned that having facilitators from certain cultural backgrounds or guest speakers with expertise/lived experiences can contribute to their understanding of certain cultural issues in great depth. For example, the Living with Disabilities Workshop in the Year 2 module Science to Clinical Practice was a collaborative session with teaching and experience sharing from one facilitator and four-panel members with different types of long-term disabilities. By hearing guest speakers’ life experiences, together with the facilitator’s explanation of disability’s impact on life, both as a sociocultural and health phenomenon, students enhanced their awareness and knowledge of how to work with patients with disabilities in a culturally appropriate manner. One student wrote her feedback via email to the module lead after attending the session:
I would like to say how fantastic, moving and completely worthwhile the workshop put on this afternoon was. I hope to take this feedback as a testament to how useful it is for the training of medics. It is amazing for us to hear different voices from different people. They did an excellent job, one that I feel all students should get a chance to experience.
We also found that students were more motivated to learn if they relate experts’ lived experiences to themselves. For instance, it was observed that a student from the LGBTQ+ community took active participation and challenged the existing research by asking profound questions in the workshop on LGBTQ+ issues. The facilitator was also a member of the LGBTQ+ community and expressed her feedback on the raised questions. This led to a discussion on how to develop structural competence to best support patients from LGBTQ+ backgrounds and further benefited students’ learning. Similar proactive engagements were observed when students encountered teaching regarding a cultural topic which they have a certain level of understanding. This reveals that students are more likely to pick up cultural learning if they relate to the lived experiences of others. Seemingly, diversifying instruction by involving teaching staff beyond the field of medicine and healthcare and showing an interest in students’ lives can potentially motivate students’ engagement. According to Focus Group Participant 9:
Getting an academic who’s either part of that community or who’s studied that culture to explain it to us and to explain why certain things the way they are, I feel that it’s a lot more beneficial than just a discussion. […] So I was put in the LGBTQ+ workshop and I thought that was really good, well it wasn’t really a lecture but the lecturer, I could say she was a member of LGBTQ+ community and she was also a healthcare professional, and she went through like so systematically, like what are the problems they face at every step of the way and it’s something that I hadn’t really considered […] It was a very well taught workshop because she got us to do little mind maps. […] She kind of explained the differences between how we would face the healthcare [professionals] and someone from the LGBTQ+ community would face it and I thought that comparison is really like eye-opening. It was insightful, and I thought that was miles better compared to just being taught like a didactic form of learning.
Over half of students in this research expressed that they unconsciously developed their cultural competence via immersion in a diverse student body. The medical school has a large student group of over 400 medical students with each student contributing distinctive cultures and perspectives. Students with black, Asian and minority ethnic (BAME) backgrounds make up approximately 60% of the whole population. The constant mixture of peers across years and programs enables students to interact with a range of cultural elements. According to Interview Participant 4:
I think one of the most important things to develop cultural competence is to meet people who are not the same as you, so one way of doing that is to get involved in societies which […] something maybe slightly outside your comfort zone, so you can meet different people and understand the way in which they look at the world. […] Just generally spending time with friends, discussing differences in culture and how we think differently and act differently in different situations is really important.
Medical schools in many western countries are traditionally dominated by students from relatively socioeconomically advantaged backgrounds (Garlick and Brown, 2008); however, this situation is gradually changing. The growing diversity within student groups enhances students’ understanding of socioeconomic differences and how they influence people’s participation in social interactions. Interview Participant 11, a Year-1 medical student who graduated from a well-known independent boarding school, expressed how studying in London exposed him to a more socioeconomically diverse population. He said that he faced challenges in adapting to the socioeconomic diversity when entering the medical school, which presents a much wider range of sociocultural diversity compared to the private boarding school he attended.
Fieldnotes: He told JL that after coming to uni[versity] he realized people can be “so different.” In his previous boarding school, students are similar in terms of socioeconomic backgrounds. However, after coming to London, he noticed that people can be different not only in terms of races and ethnicities but in aspects he has not considered before. He explained by using an example of how he became aware of people’s diversity in socioeconomic status by saying that “for example, I go to lunch in places like Wasabi [a fast-food restaurant chain] as a daily thing, but now I realized not everyone can afford Wasabi every day. Food was given to me before as it is, so I never thought about this.” […] he has been constantly challenging his attitudes and behaviors to adapt to this new environment. He also mentioned that he purposely avoided talking too much about his boarding school background as he does not intend to make himself appear more privileged than other students. He also said he is trying to achieve a balance between socializing with his “boys” from his boarding school and fitting in his new friend circle at university.
Taking part in student societies or attending student events can benefit students’ development of cultural competence because these activities improved students’ understanding of certain cultural groups. JL’s observation shows that the chosen medical school runs themed cultural events, such as the Curry Night, Celebrating Ramadan, Challenging Racism, or Black History Month. JL observed an Islamic-themed week where a group of medical student volunteers put up a stand to distribute free traditional Islamic food and introduce festivals such as Ramadan. A friendly and open environment was created for students to acquire more knowledge about the Islamic culture (e.g., the festive reasons for practices of fasting). Within the campus, JL also observed themed events discussing the issue of healthcare disparity and exploring the health concerns of marginalized cultural groups, covering topics such as female genital mutilation (FGM), LGBTQ+ health, deaf awareness, dementia and disability. Often with a healthcare focus, these events aim to improve students’ understanding of how individuals’ cultural background may influence their health. According to Interview Participant 23, the president of the Global Health Society at the medical school:
So, my society, Students for Global Health is very much involved in raising awareness of different marginalized groups and different experiences of healthcare, by different sorts of people, whether they live in the UK or globally. So, this past year we’ve had events on FGM, which is mostly in the UK experienced by people from East Africa who emigrate to the UK. And, I don’t know, if you go to that event and you don’t know anything about FGM, then obviously you’re going to get some cultural competence. You will learn that, actually, this is a cultural practice. We did a talk about racism in healthcare. The government released some figures that showed that the health of black and minority ethnic people in this country is slightly worse than the health of white people in this country. And they have worse experiences of going to the GP and going to the hospital. We had a discussion about why that might be the case and what we could do about it. […] And that’s, that’s the cultural competence exercise, isn’t it?
A few students expressed that they could enhance their CC if they actively participate in (research) projects that involve fieldwork, as these projects offer students opportunities to explore a different culture in more detail through fieldwork. Students named three such projects: two internal student projects run by the university and one external project that all focus on experiential learning. One example is the University Experience Award won by Interview Participant 6. This award is given for learning that students undertake outside the formal curriculum, which include undertaking an internship/employment, volunteering in local/global communities, or learning foreign languages outside their formal studies. Participant 6 said:
So [our university] has the Experience Awards. And I did the Global Award a couple of years ago, and I used a trip to the Philippines. and I wrote about cultural differences between my own culture and their culture. When I first started, I wasn’t expecting to get much out of it, but as I got further and further, I was surprised by the differences between cultures.
However, although these projects offer students opportunities to have experiential learning that may involve cultural diversity, it is unclear whether students are actually aware of these opportunities. The lack of signposting of potential learning opportunities is an issue, as expressed by Interview Participant 6:
So, opportunities like that exist, but they’re not sort of presented to us as learning opportunities. They’re things you have to go and do yourself. Likewise, I did the London Award looking at the different cultures of school children and their educational attainment, and whether they get to medical school. But that sort of thing isn’t formally taught in the curriculum. […] Not something that’s presented to us by the medical school. As this is an opportunity to develop your, cultural competence. […] So, there’s not a lot of signposting within the medical school for opportunities like this.
Students expressed that they value the incorporation of case studies in cultural competence teaching, but they also voiced that the occasional use of outdated cases can potentially lead to cultural stereotypes. It is further noticed that the teaching of stereotypical or outdated cultural information may make some students with certain cultural identities uncomfortable, jeopardizing the goal of providing a safe environment to initiate constructive discussion. This was mentioned by four interview participants. For example, interview Participant 13 said:
I remember […] feeling very angry in the first year, rolling my eyes a lot. Um, yeah, I think my sexual health lecture this year, [the] induction session was a bit […]. It was kind of like, here are diseases that gay people get. Very stereotypical. There was no mention of […] like ChemSex, LGBTQ+ mental health, which literally just could have been an extra slide on that, because in, in sexual health, clinics and stuff, they are trained to spot this. […] But that was not delivered to us at all in the teaching session. It was just very much like gay men get these diseases and gay men do these sexual practices.
To facilitate continuity, students suggested that stronger links need to be made across all teaching sessions with culturally embedded content. Taking the Human Values block as an example, it is observed that other sessions under the Human Values block, including professionalism, interprofessionalism, clinical communication, and medical ethics and law, all contribute to CC one way or another. Students gave positive feedback by saying that grouping these value-based subjects under one module enabled them to explore the interconnected links among these subjects. However, it is less obvious how CC is embedded and taught outside this module. While teaching was indeed happening, it was not signposted explicitly. This view is voiced by Interview Participant 5:
We’ve had a lot of cultural competence teaching. Like workshops or tutorials that are like, they are designed around […] or considering cultural competence, so I think they do recognize that it is important, but I think it could be integrated a little bit better. In terms of, when we talk about cultural competence, it’s often talked about, almost kind of like separately so like this is its own individual topic, without directly integrating into how this would be considered in real practice.
Observations showed that CC and diversity teaching not only exist in subject-specific teaching but are also embedded throughout the medical curriculum. Nevertheless, when asked where CC is addressed in the curriculum, most participants only recalled theme-specific teaching. With further elaboration, they could bring up other relevant sessions. As Interview Participant 16 said:
I have never realized that the different projects, such as the SSCs and clinical humanities projects, can also help with my cultural competence development. I never attempted to explore the link until been asked this question. But I would vote yes. Yes, for example, in my clinical humanities projects, I and my teammates co-conducted a project on how to enhance clinical communication with people of different religious backgrounds. We gathered information on how religious differences can influence patients’ health-seeking behaviors and choices, and how their diet can affect their health outcomes. Thinking back, this actually helped us get more cultural knowledge and improved our cultural competence. But I never realized this until been asked.
The limited understanding of students’ experienced learning indicates that stronger signposting on CC is needed. According to focus group Participant 2:
And I think all it would take is like a little bit of explicit signposting on behalf of the medical school or tutors […] just to make you aware of that sort of additional layer.
Our results show that students demonstrate different levels of engagement with CC. The differences in students’ desires to learn are partly attributed to how much they see CC as an essential medical competence and their self-perceived level of CC. On the one hand, a small number of students expressed that the sessions traditionally described as “soft skills” (Joubert et al., 2006), such as CC, are not medical students’ learning priorities. According to Interview Participant 20:
I mean speaking as medical students, having dedicated sessions on cultural competence is going to turn us off as we really have so much, so much work to do. […] I’d rather be in the library and studying.
The students’ lack of understanding of CC also led to them seeing CC as an intuition rather than a competence that can be enhanced through systematic training. A few students commented that existing teaching on CC tends to be a “heavy-handed,” “technical,” “magisterial” and a “less enjoyable” way to teach what is known as “common sense.” For example, focus group Participant 12’s comments represent the thoughts of some medical students:
[…] some of my friends, who grew up in London, would consider learning things like cultural competence as a joke. They say growing up in a culturally diverse place, they already know that different people have different cultural values, and this is not something new. […] some students do not understand the real significance of being culturally competent.
On the other hand, another group of students expressed that existing cultural teaching is not sufficient as the medical curriculum focused on teaching culturally respectful attitudes but not enough on cultural knowledge and skills. In particular, this need is expressed by international medical students who face a potentially culturally different patient population after moving to London to pursue a medical degree. According to French-born focus group Participant 8:
In cultural competence, […] if you want to be aware, if you want to be able to understand people “well,” you need to be aware of the kind of the basics of their cultures. For example, I was raised in a very like traditional Catholic area in France. […] I hadn’t seen many Muslims or even other religions. And then coming here and having so many patients. The cultural competence, sort of, in the module where I started it, I expected it to be sort of going over the basics that you need to know as a healthcare professional on different cultures, that you are going to encounter every day as a clinician here. Instead, I kind of had to ask friends and read around and everything, to become, to develop a bit more cultural[ly] competent because otherwise, completely, your job’s completely out of the blue. You’re told you need to be culturally competent, but you’re not given enough teaching to make you culturally competent.
This ethnographic study provides an in-depth exploration of how medical students can develop their CC through campus-based learning in a London-based medical school. We found that medical students develop their CC following longitudinal development. Throughout a 5-year MBBS curriculum in the chosen medical school, the early start of teaching mainly takes place in Year 1, when a range of sessions was observed as beneficial to students’ CC development. These sessions include theme-specific CC teaching and other allied medical subjects, such as clinical communication. When students move to more senior years, teaching is integrated among sessions in different clinical contexts. Project-based learning (e.g., student self-selected components) is also shown as relevant to students’ CC development, if students choose to lead or be involved in projects that have culturally relevant themes. In addition to the standard curriculum, students may enhance their CC by reaching out to other fields with more diverse and dispersed learning. Examples include students’ intercalated degrees or global placement programs.
We found that the chosen medical school adopts blended pedagogical approaches. This conforms with Dolhun et al.’s (2003) study summarizing that most medical schools combine didactic components with active student participation through case studies and group discussions. Teaching methods that were identified include lectures, workshops, simulated patient scenarios, project-based learning, as well as intercalated degrees and global health placements. Previous literature (Long, 2012; Dogra et al., 2016) shows there is little evidence to indicate which teaching methods are most effective in teaching CC and diversity. The results of this research show that most students perceived didactic lectures as a useful approach to introducing the concept of CC, due to lectures’ effectiveness in presenting information and providing explanation on complex terms (Brown and Manogue, 2001). Workshops were reported as helpful for students to reflect on their unconscious bias and enhance cultural awareness (Dogra et al., 2016). Some students considered workshops useful and a safe environment for discussion, others found it difficult to engage due to the potential difficulty in translating learning into clinical practice. Simulated patient scenarios were the most popular among students. This format allowed students to translate internalized cultural knowledge and attitudes into clinical interactions with simulated patients (Paroz et al., 2016). We found that students started to demonstrate an enhanced level of cultural sensitivity when participating in simulated clinical scenarios. However, due to the multiple learning outcomes to be achieved in simulation, learning about culturally sensitive communication and clinical care may take place unconsciously. Potential reinforcement of cultural stereotypes when using outdated teaching cases may also be a concern if case studies are not well developed or updated on a regular basis (Paroz et al., 2016).
Moreover, students develop their CC through engaging in research projects or reflective portfolios, which are usually part of their assessments. Project-based learning (Thomas, 2000) takes place when students engage with self-selected research projects that contain cultural elements. These allowed them opportunities to develop an in-depth understanding of cultural issues that interest them, but their learning varied depending on the nature of their chosen projects. This process may also lead to students’ reflective learning (Schon, 2010; Moon, 2013), as it allows students space for in-depth reflection, during which process unconscious learning may surface after being prompted. Self-reflection may enhance students’ motivation to learn. They may also trigger students’ self-driven reflective learning on CC, serving as the catalyst that moves surface learning into deep learning (Moon, 2013).
The results show that students develop CC in an informal manner by receiving cultural influences while immersed in the general institutional environment of the medical school. This is consistent with previous literature (Hafferty and Franks, 1994; Hafferty, 1998; Winter and Cotton, 2012) arguing that the informal and hidden curriculum has an impact on students’ learning through the daily environment and the language used within organizations. Students develop their awareness as part of CC when immersed in an environment with frequent communication and signposting to equality, diversity and inclusion. Strong institutional support is manifested in an institution’s motivation to deliver CC education, in its infrastructure and resources allocated for faculty development. All of this provides the organizational support to develop educational CC interventions. Various institutional schemes (e.g., widening participation, promoting gender equality, tackling discrimination) contribute to building a culturally inclusive environment (LeBlanc et al., 2020), which will increase students’ likelihood to engage in CC development more actively so students are even enabled to challenge inappropriate practices. In addition, the value-laden “institutional slangs or nomenclature” (Hafferty, 1998) also have an influence on students’ perception of the value of CC. An example in this research is that students frequently referred to the term “human values,” the name of a teaching block on values-based medicine in Year 1, to relate to their experiences in developing CC. This demonstrates how institutional nomenclature can influence students’ learning beyond the formal classroom setting.
Beyond the classroom, peer interaction and peer companionship interacting with peers can benefit students’ CC development. The innate diversity of the student body provides opportunities for students to learn and discuss cultural differences with their peers. Peer interaction also takes place when students join student societies or participate in cultural events on campus. Previous research (Loader et al., 2015) describes student societies as a significant dimension of the student experience of the campus life. Student societies represent the wide cultural interests of the student body. Their organized events provide a focal point for students to communicate and network with others with similar interests or affinities. Loader et al. (2015) argue that socializing with student peers can be regarded as an experiential learning process where students continually and mutually adjust their values, habits, and behaviors. However, the network established through these social interactions leads to “like-minded” students to form bonds and reinforce collective actions through multiplex networks (Crossley and Ibrahim, 2012). One concern is that students may become culturally exclusive by othering students who are outside their own networks.
Learning opportunities also exist outside the formal curriculum, such as the intercalated BScs, global health placements, or students’ extracurricular activities on campus. In these learning opportunities, students with stronger motivations to explore cultural issues may benefit more as they demonstrate a higher level of engagement with the CC subject, which allows them to experience both experiential and situated learning by interacting with people from different demographic backgrounds (e.g., global placements). A prolonged period of experiential/situated learning in a diverse environment may also contribute to students’ transformative learning (Mezirow, 1994), as students start to gather new cultural information and simultaneously evaluate their previous understanding or knowledge. This thinking and re-thinking process also leads to one’s critical reflection, through which means students may transform their worldviews and internalize CC as an essential clinical competence.
Drawing on students’ feedback we suggest that CC and diversity education be clinically relevant, case-based, expert-involved, and integrated with lived experience. Case studies need to be carefully selected to avoid the counterproductive effects of stereotypical or outdated teaching. On this basis, we suggest that training should allow educators to extensively discuss the following five blended learning strategies, and their pros and cons, when implementing preferably a longitudinal curricular design:
1) face-to-face/portfolio reflection
Reflection creates a safe and engaging learning environment for students to explore sensitive and challenging topics, such as identities, unconscious bias, and discrimination. Regular reflective activities can help students develop lifelong learning through thinking about their cultural encounters in clinical practices. This applies to face-to-face reflection that can be facilitated in a safe environment and portfolio reflection as part of students’ assessment.
2) interaction with patients/people with lived experience
Opportunities for students to talk with people with lived experiences (e.g., people with disabilities, members of the LGBTQ+ community, ethnic minorities) in a supportive and safeguarded environment are tantamount. This enables sensitive cross-cultural dialogs between students and patients.
3) clinical simulations
Clinical simulation allows students to practice communication and clinical skills under real-time constraints. Scenarios may include topics, such as working with interpreters, taking sexual histories from a transgender patient or sex worker, or discussing long-term condition management with a homeless patient. Simulating interprofessional care for acutely ill patients can also be used to develop team-level CC.
4) immersion/patient journey
Community-based immersion allows students to follow patients’ journey from family to community and learn about how culture impacts on every step of that journey. Students develop compassion and curiosity and learn how to communicate sensitively with members of the community.
5) research and quality improvement projects
Offering research opportunities to study culturally appropriate healthcare enables students to engage with cultural issues in depth. Research ties in with engaging students in quality improvement projects, through which students learn to conduct clinical audits and implement evidence-based interventions to improve the quality of care. These projects allow students to think strategically at the institutional level, preparing them with the methodology and leadership skills to manage change for improving culturally appropriate care.
Our experience suggests that strong institutional support is key to successful CC education. Medical schools need to pool resources and provide support to integrate cultural diversity in their institutional plans and address equality and diversity in areas such as admission, employment, and student support (Liu et al., 2021). This requires the institution’s recognition of CC as a core professional development. Clinical teachers who are responsible for course development need to be recognized by the senior managers. Resources should be given for them to develop teaching and research capacity so that CC can be integrated into the professional development framework and into the institution’s visions, missions, and values. A culturally diverse workforce among the faculty is also desirable because teachers’ personal and professional interests can drive CC development. In return the diverse faculty form natural role models for students.
The study has several limitations. One limitation is the participation of a relatively small number of medical students from the senior year groups (e.g., Year 4 or Year 5). This happened due to practical reasons as students in the senior years have started clinical placement and were seen as less motivated to participate in research projects that take place on campus. This was also partly due to the fact that most of the CC teaching takes place in the early years of the curriculum. Another limitation of this research is that it only focuses on exploring the CC development on a campus-based curriculum setting. In this study, we alluded to the connection between campus-based learning and learning in clinical placements and via extracurricular activities. The interconnected connection between students’ development of CC in the formal, informal and hidden curricula is beyond the scope of this research and needs further investigation. Lastly, this research focused on medical students’ development of cultural competence in one London Medical School with a strong commitment to creating a culturally inclusive environment. The diverse workforce in healthcare indicates that further research can be expanded beyond medicine to explore students’ experiences in nursing, midwifery, pharmacy, physiotherapy and other allied health professions. Added to this, the school’s teaching of CC in the formal curriculum and the geographic location, may have impacted students’ understanding and experiences of cultural diversity. Further research is required to fully understand students’ experiences in different types of health schools (e.g., schools in relatively more homogenous geographical locations) and their affiliated clinical learning sites.
This study provides a rare and novel insight into medical students’ CC development through participation in campus-based classroom teaching. Various learning opportunities contribute to different aspects of CC development and cater to different learning preferences of the diverse student population. To support students’ comprehensive development of CC, educators need to work collaboratively and use overt signposting to related disciplines and subjects. There needs to be a recognition of students’ learning not only in the formal curriculum but also in the informal and hidden curricula. Indeed, culturally competent care is not an endpoint, but a process, which consists of continuous re-evaluation and reform of current evidence, practice and policies. Challenges are increasingly raised to address the needs of mental and emotional health in individuals, aging populations, dietary preferences, global mobility, and acknowledgment of gender and sexuality as cultural issues. How cultural competence is addressed in these areas by medical education remains subject to pedagogic debate.
The original contributions presented in this study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the King’s College London Research Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
JL and SL were the main contributors in conceiving the project design. JL was the main contributor in gathering and analyzing the data. All authors contributed to writing and revising the manuscript, read and approved the final manuscript, and agreed to be accountable for the content of the work.
We acknowledge Elaine Gill, Emeritus Senior Lecturer at King’s College London, for her contribution to co-supervising the delivery of this research project. We are grateful to Deborah Bruce for supporting the delivery of this research and all students that participated in this research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2022.980633/full#supplementary-material
Abu-Arab, A., and Parry, A. (2015). Supervising culturally and linguistically diverse (CALD) nursing students: A challenge for clinical educators. Nurs. Educ. Pract. 15, e1–e9. doi: 10.1016/j.nepr.2015.02.006
Altshuler, L., and Kachur, E. (2001). A culture OSCE: teaching residents to bridge different worlds. Acad. Med. 76:514. doi: 10.1097/00001888-200105000-00045
Balcazar, F. E., Suarez-Balcazar, Y., and Taylor-Ritzler, T. (2009). Cultural competence: Development of a conceptual framework. Disabil. Rehabil. 31, 1153–1160. doi: 10.1080/09638280902773752
Betancourt, J. R. (2003). Cross-cultural medical education: conceptual approaches and frameworks for evaluation. Acad. Med. 78, 560–569. doi: 10.1097/00001888-200306000-00004
Betancourt, J. R., Green, A. R., Carrillo, J. E., and Park, E. R. (2005). Cultural competence and health care disparities: key perspectives and trends. Health Affairs 24, 499–505. doi: 10.1377/hlthaff.24.2.499
Brach, C., and Fraserirector, I. (2000). Can cultural competency reduce racial and ethnic health disparities? A review and conceptual model. Med. Care Res. Rev. 57, 181–217. doi: 10.1177/1077558700057001S09
Brown, G., and Manogue, M. (2001). AMEE Medical Education Guide No. 22: Refreshing lecturing: a guide for lecturers. Med. Teach. 23, 231–244. doi: 10.1080/01421590120043000
Burchum, J. L. R. (2002). “Cultural competence: An evolutionary perspective,” in Nursing Forum, Ed. P. S. Yoder-Wise (Hoboken, NJ: Blackwell Publishing Ltd), 5. doi: 10.1111/j.1744-6198.2002.tb01287.x
Campinha-Bacote, J. (2002). The process of cultural competence in the delivery of healthcare services: A model of care. J. Trans. Nurs. 13, 181–184. doi: 10.1177/10459602013003003
Cross, T. L. (1989). Towards a Culturally Competent System of Care: A Monograph on Effective Services for Minority Children Who Are Severely Emotionally Disturbed. [Online]. Available online at: https://files.eric.ed.gov/fulltext/ED330171.pdf (Accessed on March 30, 2020).
Crossley, N., and Ibrahim, J. (2012). Critical mass, social networks and collective action: Exploring student political worlds. Sociology 46, 596–612. doi: 10.1177/0038038511425560
Dogra, N. (2003). Cultural competence or cultural sensibility? A comparison of two ideal type models to teach cultural diversity to medical students. Int. J. Med. 5, 223–231.
Dogra, N., Bhatti, F., Ertubey, C., Kelly, M., Rowlands, A., Singh, D., et al. (2016). Teaching diversity to medical undergraduates: Curriculum development, delivery and assessment, AMEE GUIDE No. 103. Med. Teach. 38, 323–337. doi: 10.3109/0142159X.2015.1105944
Dogra, N., Reitmanova, S., and Carter-Pokras, O. (2010). Teaching cultural diversity: current status in UK, US, and Canadian medical schools. J. Gen. Int. Med. 25, 164–168. doi: 10.1007/s11606-009-1202-7
Dolhun, E. P., Muñoz, C., and Grumbach, K. (2003). Cross-cultural education in US medical schools: development of an assessment tool. Acad. Med. 78, 615–622. doi: 10.1097/00001888-200306000-00012
Garlick, P. B., and Brown, G. (2008). Widening participation in medicine. Bmj 336, 1111–1113. doi: 10.1136/bmj.39508.606157.BE
George, R. E. (2015). Exploration of cultural competency training in UK healthcare settings: A critical interpretive review of the literature. Divers. Equal. Health Care 12:100037. doi: 10.21767/2049-5471.100037
Green, A. R., Betancourt, J. R., and Carrillo, J. E. (2002). Integrating social factors into cross-cultural medical education. Acad. Med. 77, 193–197. doi: 10.1097/00001888-200203000-00003
Hafferty, F. W. (1998). Beyond curriculum reform: confronting medicine’s hidden curriculum. Acad. Med. 73, 403–407. doi: 10.1097/00001888-199804000-00013
Hafferty, F. W., and Franks, R. (1994). The hidden curriculum, ethics teaching, and the structure of medical education. Acad. Med. 69, 861–871. doi: 10.1097/00001888-199411000-00001
Joubert, P. M., Krüger, C., Bergh, A.-M., Pickworth, G. E., Van Staden, C., Roos, J. L., et al. (2006). Medical students on the value of role models for developing ‘soft skills’- “That’s the way you do it”. Afr. J. Psychiatry 9, 28–32. doi: 10.4314/ajpsy.v9i1.30204
Kumagai, A. K., and Lypson, M. L. (2009). Beyond cultural competence: critical consciousness, social justice, and multicultural education. Acad. Med. 84, 782–787. doi: 10.1097/ACM.0b013e3181a42398
LeBlanc, C., Sonnenberg, L. K., King, S., and Busari, J. (2020). Medical education leadership: from diversity to inclusivity. GMS J. Med. Educ. 37:Doc18.
Liu, J., Gill, E., and Li, S. (2021). Revisiting cultural competence. Clin. Teach. 18, 191–197. doi: 10.1111/tct.13269
Loader, B. D., Vromen, A., Xenos, M. A., Steel, H., and Burgum, S. (2015). Campus politics, student societies and social media. Sociol. Rev. 63, 820–839. doi: 10.1111/1467-954X.12220
Long, T. B. (2012). Overview of teaching strategies for cultural competence in nursing students. J. Cult. Divers. 19, 102–108.
Mezirow, J. (1994). Understanding transformation theory. Adult Educ. Q. 44, 222–232. doi: 10.1177/074171369404400403
Moon, J. A. (2013). Reflection in Learning and Professional Development: Theory and Practice. London and New York, NY: Routledge. doi: 10.4324/9780203822296
Murchison, J. (2010). Ethnography Essentials: Designing, Conducting, and Presenting Your Research. San Francisco, CA: Jossey-Bass.
Napier, A. D., Ancarno, C., Butler, B., Calabrese, J., Chater, A., Chatterjee, H., et al. (2014). Culture and health. Lancet 384, 1607–1639. doi: 10.1016/S0140-6736(14)61603-2
Núñez, A. E. (2000). Transforming cultural competence into cross-cultural efficacy in women’s health education. Acad. Med. 75, 1071–1080. doi: 10.1097/00001888-200011000-00011
Paroz, S., Daele, A., Viret, F., Vadot, S., Bonvin, R., and Bodenmann, P. (2016). Cultural competence and simulated patients. Clin. Teach. 13, 369–373. doi: 10.1111/tct.12466
Schon, D. A. (2010). Educating the reflective practitioner: Toward a new design for teaching and learning in the professions. Aus. J. Adult Learn. 50, 448–451.
Srivastava, R. (2007). The Healthcare Professional’s Guide to Clinical Cultural Competence. Amsterdam: Elsevier Health Sciences.
Tervalon, M., and Murray-Garcia, J. (1998). Cultural humility versus cultural competence: A critical distinction in defining physician training outcomes in multicultural education. J. Health Care Poor Underserv. 9, 117–125. doi: 10.1353/hpu.2010.0233
Thomas, J. W. (2000). A Review of Research on Project-Based Learning. Available online at: https://tecfa.unige.ch/proj/eteach-net/Thomas_researchreview_PBL.pdf (Accessed on March 31, 2020).
Keywords: cultural competence, medical education, medical students, undergraduate, ethnography
Citation: Liu J, Miles K and Li S (2022) Cultural competence education for undergraduate medical students: An ethnographic study. Front. Educ. 7:980633. doi: 10.3389/feduc.2022.980633
Received: 28 June 2022; Accepted: 20 September 2022;
Published: 06 October 2022.
Edited by:
Geoffroy Noel, University of California, San Diego, United StatesReviewed by:
Khoa Truong, Clemson University, United StatesCopyright © 2022 Liu, Miles and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuangyu Li, U2h1YW5neXUubGlAa2NsLmFjLnVr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.