 Alexandra Marinucci
Alexandra Marinucci Christine Grové
Christine Grové Goldie Rozendorn
Goldie Rozendorn
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 09 March 2022
Sec. Educational Psychology
Volume 7 - 2022 | https://doi.org/10.3389/feduc.2022.829578
This article is part of the Research TopicMental Health Literacy: How to Obtain and Maintain Positive Mental HealthView all 19 articles
Young people expressed concern about their mental health before COVID-19, and these concerns have escalated in response to the pandemic. A lack of knowledge, stigma and unfamiliarity with how to seek help contribute to low self-efficacy in mental health care. There is a need for school settings to include mental health education, or mental health literacy (MHL), to address youth mental health needs. Evaluation of school-based MHL programs often occur without the consultation of key stakeholders, such as young people. This study aimed to understand young people’s experience of mental health education in their school and their perspectives of how future mental health education can be tailored to suit their needs. Four online group discussions were conducted with 13 participants aged 11 to 18 years old. Eight main themes were generated from these discussions: (1) limited mental health education and understanding in school, (2) struggle to help seek, (3) negative mental health attitudes, (4) desired content about mental health education, (5) understanding of mental health, (6) school as a place for support, (7) suggestions for mental health education, and (8) ways for schools to be responsive to youth needs. All the young people in this study expressed concerns around the lack of mental health education in their schools and indicated that this must change for the wellbeing of all youth.
Engaging youth as partners in research can play a crucial role in aligning preventative mental health approaches with their needs (Ozer, 2016; Sprague Martinez et al., 2018). Involving youth voice in development of school-based programs can lead to increased motivation, self-confidence and knowledge related to the program outcomes (Stewart-Brown, 2006; Nordin et al., 2010). A systematic review of youth participation in all stages of school-based health promotion programs identified this approach contributes to positive outcomes including effectiveness of the program and likelihood of acceptance among the targeted community (Griebler et al., 2017). Young people need their voices included to feel a sense of belonging and respect as active contributors who are also beneficiaries of these programs (Lind, 2007).
Mental illness accounts for 16% of the global burden of disease and injury in youth aged 10 to 19 years (World Health Organization [WHO], 2020). This is higher compared to previous generations (Collishaw et al., 2004; Allen and McKenzie, 2015) and has been exacerbated by COVID-19 (Nearchou et al., 2020). Young people report most concern about coping with stress and mental health, with the impact of COVID-19 on education, mental health and social isolation also raised as areas of concern (Tiller et al., 2020).
Given the rising rates of mental health concerns among youth, there is a need to develop innovative approaches that support youth mental health. Targeting mental health education and support within school environments has the potential to produce long term positive effects on mental, social, and behavioral development (Graham et al., 2011; Ekornes, 2020; Grové and Laletas, 2020; Kostenius et al., 2020). Yet youth have inadequate information about mental health, especially within their learning environment (Rickwood et al., 2005; Teng et al., 2017; Tharaldsen et al., 2017; Radez et al., 2021). Barriers for youth seeking help for mental health problems include negative attitudes toward mental illness, a lack of knowledge and help available (Radez et al., 2020). Negative stereotypes associated with mental illness may be internalized by individuals suffering mental health problems, termed self-stigma (Corrigan and Rao, 2012). Self-stigma can lead to negative emotional reactions such as low self-esteem and poor self-efficacy (Watson et al., 2007). Stigma, including self-stigma, is a large barrier to help seeking for mental illness among youth (Clement et al., 2015). These barriers could be addressed through educating youth on mental health, or mental health literacy (MHL; Wei et al., 2013). MHL has been defined as the ability to recognize mental health problems, knowledge of mental health, resilience building strategies and appropriate help-seeking behaviors (Jorm, 2012; Riebschleger et al., 2017; Morgan et al., 2018; Bale et al., 2020). Increasing young people’s MHL through a preventative approach in a school-based program could reduce prevalence of and stigma toward mental illness (Clement et al., 2015; Kutcher et al., 2016; Riebschleger et al., 2019). Linking education with actions to take care of one’s mental health through MHL programs is needed (Jorm, 2020). Research based in the United States, Canada and Norway have demonstrated positive effects on MHL from school-based programs, however, little research exists in Australia (Dix et al., 2020; Seedaket et al., 2020; Marinucci et al., 2021). A school provides an optimal context for mental health education as a large population of youth can be reached, the learning environment is already established and schools have an existing role in health and wellbeing development of youth (Conley and Durlak, 2017). This type of setting allows for promotion of mental health, resilience and early intervention (Allen and McKenzie, 2015).
Studies have examined youth perspectives of mental health care services (Coates and Howe, 2014; Loughhead et al., 2018), though little research has been conducted on their perspective of mental health education in a school setting. Kostenius et al. (2020) found Scottish and Swedish youth aged 15 to 21 years reported teaching mental health should be given the same time as teaching physical health, and youth demonstrated a desire to increase their knowledge of mental health to reduce stigma. Similarly, Tharaldsen et al. (2017) and Ekornes (2020) found Norwegian youth want to learn about mental health at school as part of regular curriculum. An Australian study found that youth have difficulty assisting peers who may suffer mental health problems, with fear of rejection stated as a barrier to discussing mental illness (Teng et al., 2017). Teng et al. (2017) suggest that youth need to be educated at school with practical information about mental health, though this study did not directly ask youth what mental health knowledge they want to learn about and whether this would be accepted in a school environment.
Mental health literacy skills should be taught before the need for them arises (Rickwood et al., 2005), and neglecting youth voice in research risks misinterpretation of their needs and misguided intervention approaches (Dennehy et al., 2020). A whole school approach combines health and wellbeing with learning in the school environment and includes the perspectives of both young people and school staff in development and implementation of such interventions (Rowling, 2009; Kostenius et al., 2020). Young people represent approximately 20% of the Australian population (Australian Bureau of Statistics, 2021), and inclusion of their voice in research provides a nuanced understanding of their unique knowledge, experience and perspectives (Grové et al., 2020). Scarce research exists on Australian youth perspectives and experience of school-based mental health education and this information is crucial to ensure future initiatives are guided by the needs of the community (Ennis and Wykes, 2013; Hellström and Beckman, 2021).
This study aims to understand the perspectives of youth on mental health education and MHL in school settings and is guided by the research question:
What are young people’s perspectives and experiences of mental health literacy and mental health education programs within a secondary school setting?
It is anticipated this study will contribute to evidence supporting inclusion of youth and their voice in mental health research and collaboration in development of MHL programs in future.
This study used a youth participatory action approach with qualitative data analyzed using Braun and Clarke’s (2021) method for thematic analysis. The study was approved by the University Human Research Ethics Committee (Project ID: 27638). Informed consent and assent were gained prior to the online group discussions by parents of participants and the participants themselves.
Participants were recruited for the study using snowballing and social media. Advertisements were placed on Facebook and Instagram to recruit participants. The researchers emailed professional and personal contacts and youth-based organizations, such as community centers and youth hubs, to distribute a flyer outlining the study to recruit young people. The flyer was also posted on the personal and professional Twitter, Instagram, Facebook and LinkedIn accounts of the researchers. Recruitment took place between April to June 2021. The flow of recruitment was as follows:
1. Prospective participant completed an expression of interest form via Qualtrics.
2. Participant and their parent/guardian were invited to participate, provided with an explanatory statement about the study and a consent form via email.
3. Consent form completed by parent/guardian and returned via email.
4. At the beginning of the online group discussion, participant completed an assent form via Qualtrics.
A total of 27 young people completed the expression of interest form during the recruitment process. Thirteen responded to the email invitation, completed the consent form, and participated in the online group discussions. In total, four online group discussions took place. Participants were grouped by age and availability to participate in the online discussions. Participants’ demographic characteristics are presented in Table 1.
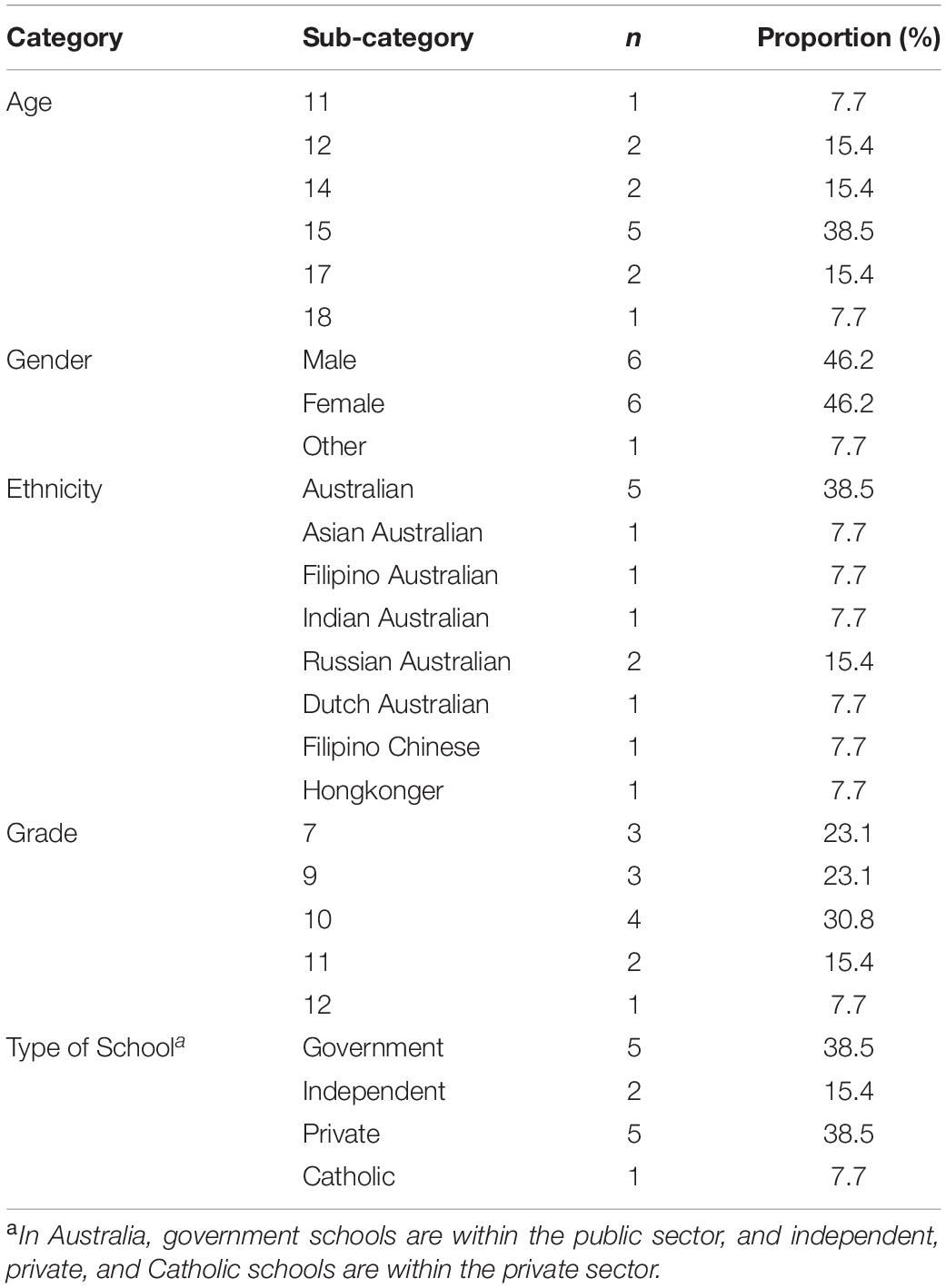
Table 1. Demographic characteristics of participants (N = 13).
Online group discussions were used to facilitate a collaborative partnership with the participants, reinforce that their perspective is valued and that they are the experts in their experience by providing a safe environment to voice their views, and identify their concerns (Grové et al., 2020). This was informed by the youth participatory action research methodology (DeJonckheere et al., 2017) and a research protocol was developed to carry out the online group discussions. The protocol was created based on previous research examining youth perspectives of mental health and youth involvement in research (Woolfson et al., 2009; Ekornes, 2020; Grové et al., 2020). The procedure for the online group discussions aimed to support participants to feel comfortable and share their perspectives. An explanatory statement was distributed to participants with helplines and resources if they felt distressed during or after the online group discussion. At the beginning of sessions, consent to audio and video recording was obtained for analysis purposes, group values were established, such as there were no right or wrong answers, and participants were able to pass on a question or withdraw from the online group discussion at any time. Participants were given a rationale for the research and invited to openly discuss their views on mental health education.
The online group discussions followed a semi-structured group interview style. Participants were split into groups of three to four based on their availability for the online group discussions led by two researchers. The online group discussions were carried out in June and July 2021 using online teleconferencing platform, Zoom Video Communications (2021). Each online group discussion took a minimum of 40 min to complete and were recorded and transcribed using Zoom.
To build rapport participants played a welcome game as a group which involved agreeing or disagreeing with fun “get to know you” statements, for example Snapchat over Instagram, camps are more fun than sports days. Questions were framed so youth responded based on their personal experience. Participants verbally answered questions or typed answers into the chat box function. Predetermined probing questions were asked such as “Does your school discuss mental health?”, “What is mental health?”, “What do you want to learn about in terms of mental health?”, “Are there barriers to talking about mental health?”, “Do you think school would be a good place to learn about mental health problems and where you can go for help if you develop symptoms?”. Participants were asked if they wanted to include more information that was missed before the online group discussion concluded. In one online group discussion, reluctance to help others due to fear of crossing personal boundaries was added at the end of the session.
Descriptive statistics were analyzed using Statistical Package for the Social Sciences Statistics, version 27.0.1.0 (IBM, 2021). Qualitative data from the online group discussions were extracted and analyzed according to Braun and Clarke’s (2021) method for thematic analysis with an inductive approach. This six-phase approach is used to identify, analyze and report patterns within data with the aim to organize and describe our verbatim records (Braun and Clarke, 2012). Transcriptions of the recordings were read several times by all authors to code patterns and themes of the data, to establish a coding scheme (Campbell et al., 2013). Two authors coded the data independently using Excel spreadsheets and named potential themes with data collated to each theme. Following this, the two authors met to discuss, review and refine the final themes. A third author reviewed the coding scheme and generated themes. Finally, using a negotiated coding approach for inter-rater reliability (Garrison et al., 2006), all authors collaborated to determine consistent or inconsistent themes across the data. No major discrepancies were identified during this process. Initially, 18 themes were identified from the transcriptions. After consultation and collaboration among the authors, eight themes were agreed upon with several themes of the 18 condensing into two or three main themes due to repetition of content.
Eight main themes and six subthemes were identified describing young people’s perspectives and experiences of mental health literacy and mental health education programs in schools. The main themes are: (1) limited mental health education and understanding in school, (2) struggle to help seek, (3) negative mental health attitudes, (4) desired content about mental health education, (5) youth understanding of mental health, (6) school as a place for support, (7) suggestions for the structure of mental health education, and (8) ways for schools to be responsive to youth needs. See Table 2 for main themes, subthemes, and their descriptions.
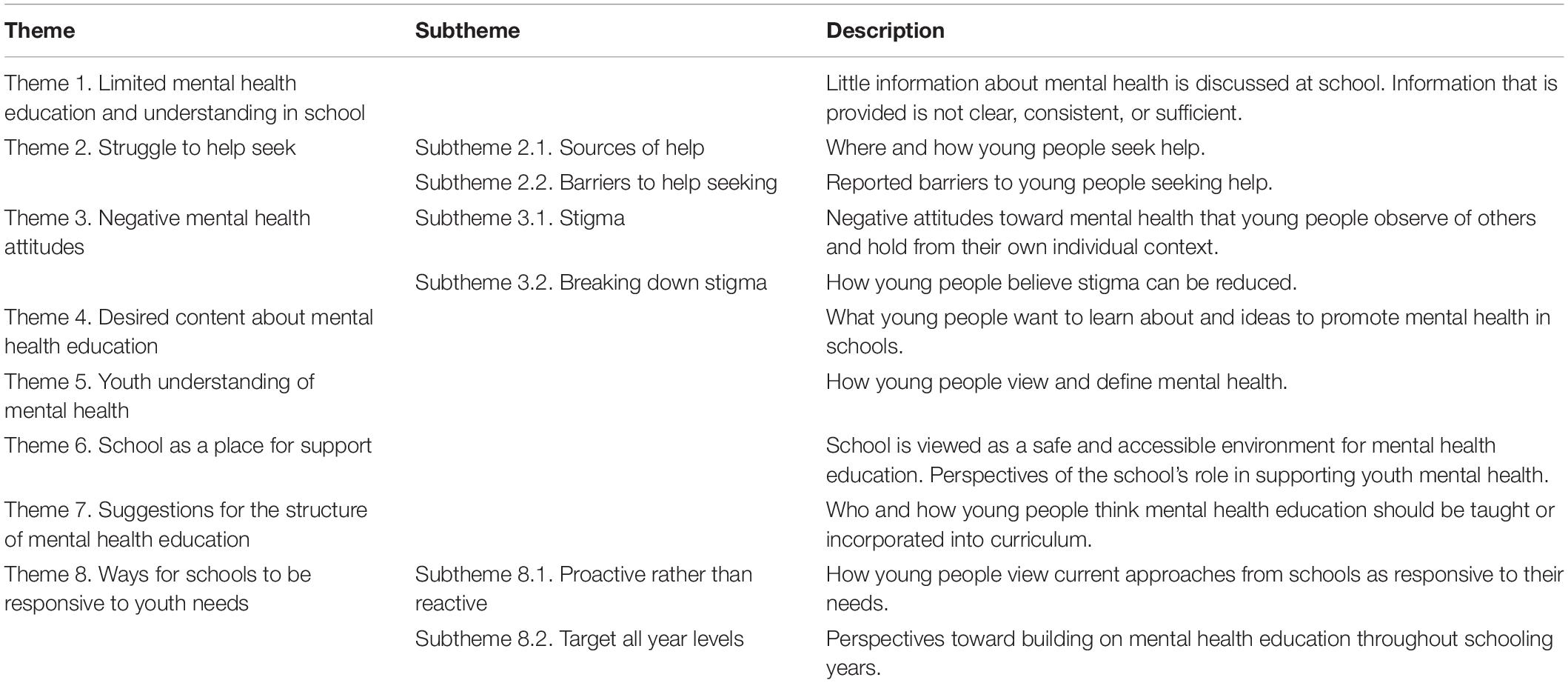
Table 2. Themes and subthemes with descriptions.
Young people stated that they do not receive enough information about mental health at school: “you have to go and figure it out yourself” (female, 14 years). Mental health is “vaguely” covered in health classes and the education that is provided is not clear or sufficient: “(teachers) don’t really explain it well enough so you don’t really understand” (female, 15 years).
Mental health topics that are discussed are general and youth expressed dissatisfaction that mental health is given little attention in their school environment: “I haven’t been happy with how little they talk about mental health” (male, 18 years). The content that is covered in school varied and included stress, anxiety, supporting others who may experience mental illness, and to speak out if experiencing mental health difficulties. Specific programs, such as bullying prevention programs and self-awareness interventions had been implemented, however, some were not viewed as useful: “we did this horrible thing called the (specific program name removed which targeted self-confidence, self-awareness and communication) it’s sort of irrelevant” (male, 18 years).
Mental health in relation to transitioning to secondary school and scheduling an appointment with the school counselor was discussed in Year 7, though it has not been discussed again, with the young person now in Year 10. A sense of incompetence and self-reliance was a shared experience: “The application of that (mental health information) into helping others (is) up to you, for you to figure out how to use that information to help others or to deal with mental health as an issue” (male, 17 years). Reflection on the self in wellbeing class was a common activity.
Mental health was discussed in homeroom classes, assemblies, and health classes, though often a brief discussion: “overall it’s just general it doesn’t go really in depth, it’s just kind of a reminder for people” (female, 15 years). Youth perceived lack of mental health education as having negative ramifications on helping others: “they don’t really talk about how you can help other people deal with it (mental health), so, like, then it is harder to help your friends” (female, 15 years). Group discussions that allow for open conversations and building on previous knowledge, but not as part of the syllabus, was found to be helpful. How to help a friend experiencing suicidal ideation was perceived as extremely important:
“If you have friends who are suicidal or whatever, you don’t know what to do, but it’s a bold thing to do for a school, but it’s also very important, because a lot of people don’t know how to respond to someone if they say they want to, you know” (male, 17 years).
A wellbeing team, school counselor, psychologist, or teachers were available for support for most but not all young people: “there’s nothing that’s like, a constant teacher, which you can go to” (female, 15 years). Barriers to providing support and mental health education were mentioned:
“The only problem they could face is time and if the teachers didn’t have time. I know a lot of schools probably wouldn’t have the budget or money it can be a lot to hire someone and get the whole presentation ready it’s up to the amount of money you’d have to pay” (male, 11 years).
“Some schools don’t know what could be triggering and not and they don’t want to make anything too hard on the kids, but also, like, it makes (it) a big barrier there just needs to be the right way to go around it, which is probably what the school struggle(s) with” (female, 15 years).
As the online group discussions took place during COVID-19, the impacts of “lockdowns” were mentioned. In Australia, lockdowns were imposed by state governments and entailed restricted movement and travel, schools closed, and only essential businesses operating. Communication was difficult during lockdowns and mental health was discussed less:
“When we’re online it’s a lot harder to get information out, so there are just topics that they just don’t touch on anymore, because already it’s hard to keep kids, like, at a screen all day, so yeah I feel like it’s talk(ed) about definitely less” (female, 15 years).
Help seeking behavior and experiences were identified as the second theme from the online group discussions. Overall, youth identified family, friends, and the internet as sources of help, however, this was dependent on the difficulties: “if it’s a bigger mental health issue that my friends wouldn’t be able to cope with, then I would go to my parents” (female, 14 years). Seeking help for themselves and others was difficult at times due to perceived stigma of talking about mental health, exposing vulnerability, and uncertainty of how to support a friend who may be experiencing mental health problems: “sometimes you have to get to the nitty gritty but not everyone’s comfortable with those details” (female, 15 years). This was separated into two subthemes: sources of help, and barriers to help seeking.
This subtheme pertains to where and how youth seek help if they experienced a mental health problem. A family member was a common help source: “I would most of the time go to family because I would feel a tiny bit weird approaching a teacher about problems” (non-specified, 14 years). Others specified that they would go to their friends unless they thought it was a larger issue that their friends would not be able to cope with. The internet, scholarly articles and specific websites such as Headspace, ReachOut.com, Google and Reddit were a source of initial information and support. Counselors, teachers and trusted adults were identified as sources of help, however, informal sources such as family and friends were preferred: “I would talk to friends about it cos that’s just easier for me” (female, 14 years) and “I would go to a family member before I went to the teacher because it just feels better going to a family member first” (male, 12 years).
Barriers to seeking help included feeling disconnected from others and so unwilling to share mental health difficulties: “sometimes you’re in a group of people that you just don’t want to talk about these issues with” (female, 15 years). There is a reluctance to discuss mental illness in fear of offending someone or pushing boundaries if a peer is suspected to be experiencing mental health difficulties:
“I think through my conversations of mental health that sometimes you want to go deeper. To really know the person more and to really take care of them you want to make everyone feel comfortable in your conversations, you don’t want to take that risk of them feeling like it’s an invasion of privacy” (male, 17 years).
Young people want to be genuine in their approach to support a friend if they were struggling with mental health concerns, however, felt unsure how to convey this: “it’s a very unclear, gray area about what is considered to be correct to talk about with someone, and I think because of that we just generally go for the safest option which seems a bit ungenuine” (male, 17 years).
Negative mental health attitudes in young people’s environment and individual context exist, with mental health described as a “hush hush topic,” “taboo,” and associated with “negative relationships.” However, young people are aware of how attitudes could be changed, such as through normalizing mental health problems, understanding mental health and openly talking about it at school. Two subthemes were generated: stigma and breaking down stigma.
From young people’s perspectives, there is stigma surrounding mental illness including self-stigma, an internalized stigma response from one’s own individual context, and observed stigma, stigma responses in one’s community from others. Mental health and mental illness is often framed negatively: “you could get into a panic state, like oh my God I’m the only one who has this and it’s going to affect me really badly” (male, 11 years) and “no one really wants to openly talk about if they’re struggling with something, because then they don’t really know how other people will react” (female, 15 years).
Language surrounding mental illness also appeared problematic, for example: “I had a friend, he made a comment that, “oh I have a depressed friend now,” when another friend said that they have depression, like not really talked about in a very positive way” (female, 15 years). Mental health and mental illness still seems to be a “taboo” topic and some people hold negative views of those who experience a mental illness: “I do think there is some groups that don’t take it seriously and do enforce some kind of harmful attitudes toward other people” (female, 15 years). Youth perceive that mental illness in young people goes unrecognized: “I don’t think that people realize that kids can experience bad mental health days” (female, 15 years). A lack of understanding of mental health was proposed as a contributing factor to stigma of mental illness: “When people don’t understand something they become afraid of it” (male, 17 years) and “it’s a bit alien to some people I think it’s always uncomfortable when they don’t really understand” (male, 18 years).
Suggestions of how to break down stigma included discussing mental health in school, sharing individual experiences, advertisements and normalizing mental health problems. Discussing mental health and sharing personal experiences of mental illness was identified as a helpful way to reduce stigma: “talking about mental health in class and in school regularly would make people feel a lot more comfortable with these things and they’d be able to openly express their feelings and ideas” (female, 15 years) and “other people sharing their story what they’re going through (so) other people don’t feel like they’re alone” (non-specified, 14 years).
Mental health should be discussed across settings and contexts: “those discussions can start (a) from an early age and, (b) they need to be discussed in more than one place, it shouldn’t just be (discussed) at school” (female, 15 years). By increasing the discussion of mental health and normalizing mental health problems, people would be more likely to show empathy toward those who experience mental illness. Mental health was a topic that young people believe to be important to understand: “it’s a sensitive topic it’s something that we all need to know about and just by learning about it from a young age, means that kids can grow up and be more comfortable talking about it” (female, 15 years).
The main content that youth wanted to learn about was how to recognize mental health symptoms in themselves and in others:
“I’d like to learn about how to spot these things if someone chooses not to be open and talk about what they’re going though I think definitely how to be able to see very clearly what is going on and take action, because I know it can be very, very difficult if you don’t understand or you can’t see the signs of what’s going on, and then something bad happens and you’re like oh man I should have seen the signs” (male, 17 years).
Young people want to know how to manage mental health symptoms in a practical way: “how to manage it, but not in a condescending, oh you know just organize yourself and chill out, have some “you” time in a way that is sort of out of touch” (male, 18 years) and “even learn about normal everyday things that can help you. Like things that might prevent people from having low self-esteem” (female, 15 years). Self-care behaviors, coping strategies, knowledge of mental illnesses and impact of mental illness were areas of interest:
“I think coping strategies could be good, because if you, like, originally don’t know any good coping strategies, you can turn to more negative things they could teach, like, basic counseling skills that can be very beneficial for students with anxiety in a classroom and you don’t exactly need a counselor to teach you that” (female, 15 years).
Certain topics should not be avoided in mental health education, such as suicide or self-harm as “if they exist, people are going to know about them” (male, 17 years):
“I think that there should be no limits school should prioritize educating their students on the most, kind of, relevant mental health issues and how to tackle those but I don’t think they should completely close off things (a) because we don’t know we only know things based on our previous experience, but what if there is a student who’s sitting right next to us who’s going through something that we could never even think possible (b) because you could experience that in the future, and if you’re equipped with everything you need to know prior to that experience you could better tackle that and you could better bounce back from that difficult time in the future if you’re equipped with the knowledge of how to overcome that issue” (female, 15 years).
Trigger and content warnings were recommended for sensitive mental health topics. Ways to incorporate mental health education in schools was through a special week (e.g., mental health awareness week), a program that runs every year or month and advertisements. A point of contact within schools as well as places outside of school and a list of resources to refer to were preferred as resources provided by schools:
“I just think plenty of options different options will suit everyone differently if the school can give you ways to find people outside of school and still have access to people inside of school, then I think that’s probably the best way to go about it” (male, 17 years).
Young people defined mental health as someone’s state of mind:
“Basically similar to physical and social health but it just revolves around, like, the mind, and I suppose how you deal with your emotions and, kind of, thoughts about yourself and others similar to physical health, you can have, you know, different health conditions and issues” (male, 17 years).
Mental health was described as serious, sensitive, and how someone copes, with some understanding mental health based on knowledge of depression, suicide, and mental health problems. The difference between physical and mental health underlined difficulties in recognizing mental illness, “I think sometimes that can be a lot harder to deal with because it’s quite a lot more underlying than, say, a broken toe” (male, 17 years). Young people acknowledged that mental health constitutes more than feeling happy:
“It’s not necessarily being happy, but it’s more being, like, in touch with yourself understanding that life has a meaning and wanting to wake up every day. I think there’s a common misconception that mental health is just being happy 100% of the time which isn’t true, and we all know that you’re not going to be happy 100% of the time” (female, 15 years).
Overall, mental health was not discussed solely in relation to mental illness and most participants held a holistic view of mental health, that mental health is more than the absence of mental illness.
Schools are a place of support and resources for mental health. Youth described school as a safe, easily accessible place to learn about mental health: “I think school is a place where they feel, you know, comfortable with their friends and their teachers and I think that makes for (a) good environment to talk about things like mental health” (male, 17 years) and “schools should be a place where people can speak about it, but it’s obviously going to be different for everyone” (female, 15 years). Young people spend most of their time in the school environment during their schooling years and so it is logical to have mental health education in school: “it’s almost like a second home, and within that second home, mental health needs to be the safe discussion topic” (female, 15 years). Schools should have “a really warm and friendly atmosphere where people are comfortable with talking to teachers” (male, 15 years). Schools, including teachers and wellbeing teams, have a critical role in supporting youth mental health:
“Schools really should have an obligation it should be their job to at least provide the service at least basic services and obviously they will have counselors, I think that if you went to school without counselors, that’s a whole other issue…(but) just because there are counselors doesn’t mean there aren’t other things that schools can do” (male, 18 years).
A trained professional who is knowledgeable in mental health, such as a teacher, counselor, psychologist or wellbeing leader, should deliver mental health education. Sport and health teachers were identified as ideal candidates for teaching mental health in classes: “sport teachers should take a bit of like, a responsibility to tell kids exactly what is happening” (female, 14 years) and “health teachers should be the ones teaching it, but I think every teacher has a responsibility and have a role in it” (female, 15 years). Whilst school counselors were recognized as important, regular classroom teachers were suggested to teach mental health as a connection to the person was perceived as important: “(it) needs to be someone who knows it really well and has, like, a good connection with the students. If you don’t feel comfortable talking to someone about it, then it’s not really going to be a good conversation” (male, 17 years). Young people want to know the services available to them and how to use online services, such as online counseling through Headspace, as providing a number to call is not sufficient. Guiding young people through websites and creating an account were perceived as helpful steps to explaining online services available.
There were various perspectives on whether mental health education should be formally taught or be informal discussions only: “if it was more formal, it would have more meaning to it. Because a lot of the time, when you only have one session a term or a few a year, people don’t really pay attention” (female, 15 years) and “with informal, those individualized check ins could be really helpful for the support for people who need that” (male, 17 years). For information not addressed in class, a mental health professional could lead a Q&A session with youth to address any concerns not covered in mental health educational classes. A curriculum adjustment was seen to be necessary: “I definitely think that more classes need to be done in it, I think the curriculum should be changed that makes it pretty much compulsory to talk about because I think it’s really important” (female, 15 years). This should be during regular classes, rather than after school due to obligations outside of school hours and homework: “outside of schools means kids definitely would not want to go I feel like (it) would be hard to justify making kids stay longer” (male, 18 years) and “if it was after school, they would feel like they’re being forced to go” (non-specified, 14 years). Weekly or fortnightly sessions with group discussions incorporated appeared to be preferred by young people. Some youth may not feel comfortable talking about mental health in school, however, if everyone received mental health education, rather than opt in, this could mitigate potential stigmatized views:
“I think that if you’re doing it at school, then, if kids, like, don’t really want to talk about their mental health or don’t want to make it known that, you know, they’re going to these mental health classes, then I think it’s a lot better to (do) it in an environment where everyone has to do it because, not only will it help people, like, who don’t want anyone to know, it will also help everyone else understand” (female, 15 years).
The ability to reach a wide range of young people is a benefit of incorporating mental health education in schools.
Schools need to be responsive to youth mental health needs. Instead of responding to crises or during times of stress, such as during exam periods, young people want mental health to be consistently discussed throughout their school years. Inclusion of their perspectives and needs in decision making of mental health education and support is a way schools could be responsive to youth needs. This resulted in two subthemes: proactive rather than reactive and target all year levels.
Schools often approach mental health in a reactive way and respond in times of crises or observed difficulty: “it feels more, kind of, spontaneously if something pops up they’ll do a talk about it and it feels kind of rushed” (female, 15 years) and “the conversation is more done one on one if you bring something first” (female, 15 years). Discussions surrounding mental health appeared to be more prominent during exam periods and the upper year levels (e.g., Year 12). The overall experience appeared that schools would not ask young people what they wanted to learn about:
“It should be more about stuff that students actually have, like, worries over, I guess, rather than on a general level, what they think everyone is dealing with because not everyone is dealing with the same thing, and I think the school just does what they think and it’s like, but we don’t apply to that or we think that we should focus on this” (female, 14 years).
However, if the school notices students talking about a specific topic, they will address this directly: “if it was a bit of a problem then they would spend quite a bit of time talking about it, whereas if it’s not really an issue, then they wouldn’t talk about it” (male, 12 years).
There is a clear need to target all year levels and begin in younger schooling years for mental health education: “Younger kids should be learning about it as well” (non-specified, 14 years) and “I definitely think that it needs to be discussed from a much younger age, from the primary school age” (female, 15 years). Young people are frustrated that they had not learnt skills to manage their mental health when younger:
“If we would have learnt it when we were younger, we would have already had the skills before. They just had to, like, suddenly teach it because we were going into exams talking about it as a kid would make it definitely more comfortable for us to talk about it as adults, instead of ignoring it as a child, and then when you become an adult, suddenly you have to deal with it all” (female, 14 years).
Young people would feel it easier to manage stress and mental health difficulties if they were explicitly taught about mental health and coping strategies before secondary school.
This study aimed to address the research question: What are young people’s perspectives and experiences of mental health literacy and mental health education programs within a secondary school setting?
Overall, young people in this study did not find that the current mental health education in their school addressed their needs nor did it cover what they wanted to understand. In their perspective, this has contributed to difficulties in seeking help for mental health problems and helping friends who may experience mental health problems. Youth viewed school as a good place to learn about mental health and support and wanted schools to be more proactive in their response to their wellbeing. There is an understanding of mental health being more than the absence of illness, demonstrating a move away from the traditionally medicalized view of mental health. The young people in this study wanted to learn about how to recognize declining mental health, self-care practices and strategies to obtain and maintain positive mental health. This content was viewed to be best taught within a school environment during regular classes as part of the curriculum to increase accessibility to youth. Programs targeting MHL within school settings that are delivered consistently and across different year levels may address the concerns raised by the young people who participated in this study.
The findings in this study are similar to those of Tharaldsen et al. (2017), O’Reilly et al. (2018), Ekornes (2020), and Kostenius et al. (2020). Youth consider schools to be a critical environment to increasing MHL by providing resources and support services, encouraging positive mental health behaviors, such as coping strategies and resilience, and promoting discussion of mental health to reduce stigmatized attitudes (Woolfson et al., 2009; Ekornes, 2020). There is a desire from youth to learn about mental health, and a shared view that teaching of health should include physical and mental health (Kostenius et al., 2020). This study and previous research identifies that youth should be engaged as key stakeholders in decisions of wellbeing curriculum within schools, as this was raised as a contributing factor to limited mental health education and schools not responding to youth needs (O’Reilly et al., 2018; Kostenius et al., 2020). Young people feel reluctant to reach out to others who they suspect may be experiencing mental health difficulties, as there is a fear of acting inappropriately or crossing a boundary (Teng et al., 2017). Existing literature highlights that youth tend to approach those with a mental illness cautiously (Secker et al., 1999; Teng et al., 2017). Teng et al. (2017) describes contradictions and confusion amongst young people regarding facets of mental health. Additionally, barriers to youth seeking help include perceived stigma, embarrassment and public stigma (Radez et al., 2020). Without adequate education of risk and protective factors for mental health, one’s ability to obtain and maintain good mental health is impaired and both negative views of mental illness and poor help-seeking behaviors may develop (Radez et al., 2021). There is a need for guidance and education of mental health and help seeking actions, such as through a MHL program, to empower youth to care for their own mental health and increase confidence in supporting others (Tharaldsen et al., 2017). A school setting is an optimal place for this to occur, with provision of accurate mental health information and strategies that could be incorporated into the health and wellbeing curriculum (Teng et al., 2017; Kostenius et al., 2020).
The findings from this study reveal that young people want schools to provide mental health education that is comprehensive and responsive to their needs. Directing youth to helpline phone numbers is not enough and there is a need to explicitly teach youth about the sources of help available to them and the steps to attain that help. There are still stigmatized attitudes toward mental health in the school environment. Educating young people on mental health throughout their schooling years and normalizing a discussion around mental health may reduce this stigma. Schools are viewed as a place for support, and young people want to learn how to recognize signs of mental illness, how to help others, and how to use practical coping strategies in this environment. The findings of this study suggest that more needs to be done in the school environment to support youth mental health. According to participants, ineffective mental health education at school contributed to in their lack of MHL. A lack of MHL was identified as an obstacle to seek help for mental health related concerns, assist friends and peers experiencing mental illness as well as contributing to negative attitudes and stigma associated with mental illness. Young people want classes focused on MHL with a deliberate effort from schools to include their voice in determining their needs.
The majority of MHL research investigates youth perspectives of mental illness with existing symptomatology of mental illness (Radez et al., 2021) or those with family members with a mental illness (Reupert et al., 2013; Bee et al., 2014; Grové et al., 2016; Riebschleger et al., 2019), however, this study contributes to a developing body of literature investigating youth perspectives of their mental health education in the general population. This study has a few limitations. Young people opted into the study, therefore the results may be subject to selection bias and participants may have had a pre-existing interest in mental health. The method of recruitment was through social media advertisements which were posted online, and therefore those without access to the social media sites would not have been reached. Future research could look at a larger sample of participants recruited through various means to determine whether these perspectives are held by a wide range of young people such as youth in rural or regional areas. Finally, the results may be limited by reliability of the data coding process. Although the authors independently coded the data and used a negotiated coding approach (Garrison et al., 2006), the themes generated may be biased by the authors’ judgments based on their knowledge and experience in research and the field of youth mental health. Future research could use standard reliability measures for coding data to determine a Krippendorff’s alpha (Hayes and Krippendorff, 2007).
This study highlights that from the perspectives of 13 young Australians, the current education system is not meeting their MHL needs. Youth shared a desire to learn about mental health, however, felt that the current mental health content is vague and ineffective. The lack of adequate mental health education and MHL content was perceived as a contributing factor to stigma of mental illness, and difficulties in help seeking behaviors and use of self-care strategies. Schools were considered a key environment for mental health education and support, with advocacy for a proactive and preventative approach. It is evident there is a need to address the lack of mental health education in the school curriculum. Mental illness among youth has been linked to an increased risk of academic failure, withdrawal from school, poor physical health outcomes, difficulty maintaining healthy relationships, and substance use (Chen et al., 2006; McGorry et al., 2013; McGorry et al., 2007; World Health Organization [WHO], 2020). Youth are vulnerable to mental illness (Woodward and Fergusson, 2001; Lee et al., 2014; Gee et al., 2018), though are inadequately informed about mental health (Rickwood et al., 2005; Teng et al., 2017; Radez et al., 2020, 2021). School-based MHL programs have demonstrated favorable outcomes (Seedaket et al., 2020), and increasing MHL of youth may prevent future development of mental illness. Young people want to learn about mental health, how to help others and how to care for their own mental health (Rosvall, 2020). Schools need to move from a reactive to a proactive approach to youth mental health. By highlighting that the school environment is considered a key avenue for mental health education and support, the importance of developing school-based interventions to increase youths’ inadequate knowledge of mental health is emphasized (Rickwood et al., 2005; Teng et al., 2017; Radez et al., 2021). Promoting mental health at school is particularly salient as school based MHL programs have demonstrated favorable outcomes (Grové and Laletas, 2020; Seedaket et al., 2020), and increasing MHL of youth may decrease the likelihood of future development of mental illness. A proactive and preventative school-based approach includes:
• Accessible MHL programs with input from young people as key stakeholders;
• Youth voice included in future development and research of MHL programs to ensure their relevant needs are addressed appropriately;
• Various mental health resources for youth to access and clear instruction on how to access these resources;
• Open discussions of mental health in the school environment;
• Increased awareness of where and how to seek help in the school environment, including what to do if immediate professional support is not available.
Young people want to be equipped with comprehensive MHL linked with actions to support their own and other’s mental health. Future research is needed to determine how MHL can be incorporated into the current education curriculum to address the needs of youth.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Monash University Human Research Ethics Committee. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
AM contributed to the literature review, research design, data collection, and data analysis. CG contributed to the research design, supervised analysis, and the development of the manuscript. GR contributed to the data collection and data analysis. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This study was based on the course requirements for the AM’s Ph.D.
Allen, K. A., and McKenzie, V. L. (2015). Adolescent mental health in an Australian context and future interventions. Int. J. Ment. Health 44, 80–93. doi: 10.1080/00207411.2015.1009780
Australian Bureau of Statistics (2021). Regional Population by Age and Sex. Canberra: Australian Bureau of Statistics.
Bale, J., Grové, C., and Costello, S. (2020). Building a mental health literacy model and verbal scale for children: results of a Delphi study. Child. Youth Serv. Rev. 109, 104–667. doi: 10.1016/j.childyouth.2019.104667
Bee, P., Bower, P., Byford, S., Churchill, R., Calam, R., Stallard, P., et al. (2014). The clinical effectiveness, cost-effectiveness and acceptability of community-based interventions aimed at improving or maintaining quality of life in children of parents with serious mental illness: a systematic review. Health Technol. Assess. 18, 1–250. doi: 10.3310/hta18080
Braun, V., and Clarke, V. (2012). “Thematic analysis” in APA Handbook of Research Methods in Psychology, Vol 2: research Designs: quantitative, Qualitative, Neuropsychological, and Biological. eds H. Cooper, P. M. Camic, D. L. Long, A. T. Panter, D. Rindskopf, and K. J. Sher (United States: American Psychological Association). 57–71. doi: 10.1037/13620-004
Braun, V., and Clarke, V. (2021). Thematic Analysis: a Practical Guide. United States: SAGE Publications.
Campbell, J. L., Quincy, C., Osserman, J., and Pedersen, O. K. (2013). Coding In-depth Semistructured Interviews: problems of Unitization and Intercoder Reliability and Agreement. Sociol. Methods Res. 42, 294–320. doi: 10.1177/0049124113500475
Chen, H., Cohen, P., Kasen, S., Johnson, J. G., Berenson, K., and Gordon, K. (2006). Impact of adolescent mental disorders and physical illnesses on quality of life 17 years later. Arch. Pediatr. Adolesc. Med. 160, 93–99. doi: 10.1001/archpedi.160.1.93
Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., et al. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 45, 11–27. doi: 10.1017/S0033291714000129
Coates, D., and Howe, D. (2014). The importance and benefits of youth participation in mental health settings from the perspective of the headspace Gosford Youth Alliance in Australia. Child. Youth Serv. Rev. 46, 294–299. doi: 10.1016/j.childyouth.2014.09.012
Collishaw, S., Maughan, B., Goodman, R., and Pickles, A. (2004). Time trends in adolescent mental health. J. Child Psychol. Psychiatry 45, 1350–1362. doi: 10.1111/j.1469-7610.2004.00842.x
Conley, C. S., and Durlak, J. A. (2017). “Universal mental health promotion and prevention programs for students” in Global Mental Health: prevention and Promotion. eds S. Bährer-Kohler and F. J. Carod-Artal (Germany: Springer). 127–139. doi: 10.1007/978-3-319-59123-0
Corrigan, P. W., and Rao, D. (2012). On the self-stigma of mental illness: stages, disclosure, and strategies for change. Can. J. Psychiatry 57, 464–469. doi: 10.1177/070674371205700804
DeJonckheere, M., Vaughn, L. M., and Bruck, D. (2017). Youth-led Participatory Action Research: a Collaborative Methodology for Health, Education, and Social Change. United States: SAGE Publications. doi: 10.4135/9781473956032
Dennehy, R., Meaney, S., Cronin, M., and Arensman, E. (2020). The psychosocial impacts of cybervictimisation and barriers to seeking social support: young people’s perspectives. Child. Youth Serv. Rev. 111:104872. doi: 10.1016/j.childyouth.2020.104872
Dix, K., Kashfee, S. A., Carslake, T., Sneidze-Gregory, S., O’Grady, E., and Trevitt, J. (2020). A Systematic Review of Intervention Research Examining Effective Student Wellbeing in Schools and their Academic Outcomes. Australia: Evidence for Learning, Social Ventures.
Ekornes, S. (2020). Upper secondary students’ perceptions of the effects of expanded student services on their mental health literacy. Pastor. Care Educ. 38, 355–372. doi: 10.1080/02643944.2020.1751686
Ennis, L., and Wykes, T. (2013). Impact of patient involvement in mental health research: longitudinal study. Br. J. Psychiatry 203, 381–386. doi: 10.1192/bjp.bp.112.119818
Garrison, D. R., Cleveland-Innes, M., Koole, M., and Kappelman, J. (2006). Revisiting methodological issues in transcript analysis: negotiated coding and reliability. Intern. High. Educ. 9, 1–8. doi: 10.1016/j.iheduc.2005.11.001
Gee, D. G., Bath, K. G., Johnson, C. M., Meyer, H. C., Murty, V. P., van den Bos, W., et al. (2018). Neurocognitive development of motivated behavior: dynamic changes across childhood and adolescence. J. Neurosci. 38, 9433–9445. doi: 10.1523/jneurosci.1674-18.2018
Graham, A., Phelps, R., Maddison, C., and Fitzgerald, R. (2011). Supporting children’s mental health in schools: teacher views. Teach. Teach. Theory Pract. 17, 479–496. doi: 10.1080/13540602.2011.580525
Griebler, U., Rojatz, D., Simovska, V., and Forster, R. (2017). Effects of student participation in school health promotion: a systematic review. Health Promotion Int. 32, 195–206. doi: 10.1093/heapro/dat090
Grové, C., and Laletas, S. (2020). Promoting Student Wellbeing and Mental Health Through Social and Emotional. Australia: Allen & Unwin. 317–335.
Grové, C., Reupert, A., and Maybery, D. (2016). The perspectives of young people of parents with a mental illness regarding preferred interventions and supports. J. Child Fam. Stud. 25, 3056–3065. doi: 10.1007/s10826-016-0468-8
Grové, C., Trainer, L., and Rangarajan, R. (2020). Youth Centred Research Brief Report 1: co-Collaborating with Youth as Active Stakeholders in Research. Australia: Monash University. doi: 10.26180/13158170.v1
Hayes, A. F., and Krippendorff, K. (2007). Answering the call for a standard reliability measure for coding data. Commun. Methods Measures 1, 77–89. doi: 10.1080/19312450709336664
Hellström, L., and Beckman, L. (2021). Life challenges and barriers to help seeking: adolescents and young adults voices of mental health. Int. J. Environ. Res. Public Health 18:13101. doi: 10.3390/ijerph182413101
IBM (2021). SPSS Statistics [Computer software]. Available online at: IBM. https://www.ibm.com/au-en/products/spss-statistics (accessed September 29, 2021).
Jorm, A. F. (2012). Mental health literacy: empowering the community to take action for better mental health. Am. Psychol. 67, 231–243. doi: 10.1037/a0025957
Jorm, A. F. (2020). We need to move from ‘mental health literacy’ to ‘mental health action’. Ment. Health Prevent. 18:200179. doi: 10.1016/j.mhp.2020.200179
Kostenius, C., Gabrielsson, S., and Lindgren, E. (2020). Promoting mental health in school—Young people from Scotland and Sweden sharing their perspectives. Int. J. Ment. Health Addict. 18, 1521–1535. doi: 10.1007/s11469-019-00202-1
Kutcher, S., Wei, Y., Costa, S., GusmΓJo, R., Skokauskas, N., and Sourander, A. (2016). Enhancing mental health literacy in young people. Euro. Child Adolesc. Psychiatry 25:567. doi: 10.1007/s00787-016-0867-9
Lee, F. S., Heimer, H., Giedd, J. N., Lein, E. S., Šestan, N., Weinberger, D. R., et al. (2014). Adolescent mental health—Opportunity and obligation. Science 346, 547–549. doi: 10.1126/science.1260497
Lind, C. (2007). The power of adolescent voices: co-researchers in mental health promotion. Educ. Action Res. 15, 371–383. doi: 10.1080/09650790701514309
Loughhead, M., Guy, S., Furber, G., and Segal, L. (2018). Consumer views on youth-friendly mental health services in South Australia. Adv. Ment. Health 16, 33–47. doi: 10.1080/18387357.2017.1360748
Marinucci, A., Grové, C., Allen, K.-A., and Riebschleger, J. (2021). Evaluation of a youth mental health literacy and action program: protocol for a cluster controlled trial. Ment. Health Prevent. 24:200216. doi: 10.1016/j.mhp.2021.200216
McGorry, P., Bates, T., and Birchwood, M. (2013). Designing youth mental health services for the 21st century: examples from Australia, Ireland and the UK. Br. J. Psychiatry 202, s30–s35. doi: 10.1192/bjp.bp.112.119214
McGorry, P. D., Purcell, R., Hickie, I. B., and Jorm, A. F. (2007). Investing in youth mental health is a best buy. Med. J. Austr. 187, S5–S7. doi: 10.5694/j.1326-5377.2007.tb01326.x
Morgan, A. J., Ross, A., and Reavley, N. J. (2018). Systematic review and meta-analysis of Mental Health First Aid training: effects on knowledge, stigma, and helping behaviour.(Research Article). PLoS One 13:e0197102. doi: 10.1371/journal.pone.0197102
Nearchou, F., Flinn, C., Niland, R., Subramaniam, S. S., and Hennessy, E. (2020). Exploring the impact of COVID-19 on mental health outcomes in children and adolescents: a systematic review. Int. J. Environ. Res. Public Health 17:8479. doi: 10.3390/ijerph17228479
Nordin, L., Jensen, J., and Simovska, V. (2010). Unges deltagelse i sundhedsfremme: hvad siger litteraturen [Young people’s participation in health promotion: what does the literature say]. Cursiv 5, 77–101.
O’Reilly, M., Adams, S., Whiteman, N., Hughes, J., Reilly, P., and Dogra, N. (2018). Whose responsibility is adolescent’s mental health in the UK? Perspectives of key stakeholders. Sch. Ment. Health 10, 450–461. doi: 10.1007/s12310-018-9263-6
Ozer, E. J. (2016). Youth-led participatory action research: developmental and equity perspectives. Adv. Child. Dev. Behav. 50, 189–207. doi: 10.1016/bs.acdb.2015.11.006
Radez, J., Reardon, T., Creswell, C., Lawrence, P. J., Evdoka-Burton, G., and Waite, P. (2020). Why do children and adolescents (not) seek and access professional help for their mental health problems? A systematic review of quantitative and qualitative studies. Euro. Child Adolesc. Psychiatry 30, 183–211. doi: 10.1007/s00787-019-01469-4
Radez, J., Reardon, T., Creswell, C., Orchard, F., and Waite, P. (2021). Adolescents’ perceived barriers and facilitators to seeking and accessing professional help for anxiety and depressive disorders: a qualitative interview study. Euro. Child Adolesc. Psychiatry Epub online ahead of print. doi: 10.1007/s00787-020-01707-0
Reupert, A. E., Cuff, R., Drost, L., Foster, K., Van Doesum, K. T. M., and Van Santvoort, F. (2013). Intervention programs for children whose parents have a mental illness: a review. Med. J. Austr. 199, S18–S22. doi: 10.5694/mja11.11145
Rickwood, D., Deane, F. P., Wilson, C. J., and Ciarrochi, J. (2005). Young people’s help-seeking for mental health problems. Austr. E-J. Adv. Ment. Health 4, 218–251. doi: 10.5172/jamh.4.3.218
Riebschleger, J., Costello, S., Cavanaugh, D. L., and Grové, C. (2019). Mental health literacy of youth that have a family member with a mental illness: outcomes from a new program and scale. Front. Psychiatry 10:2. doi: 10.3389/fpsyt.2019.00002
Riebschleger, J., Grové, C., Cavanaugh, D., and Costello, S. (2017). Mental health literacy content for children of parents with a mental illness: thematic analysis of a literature review. Brain Sci. 7:141. doi: 10.3390/brainsci7110141
Rosvall, P. -Å (2020). Perspectives of students with mental health problems on improving the school environment and practice. Educ. Inquiry 11, 159–174. doi: 10.1080/20004508.2019.1687394
Rowling, L. (2009). Strengthening “school” in school mental health promotion. Health Educ. 109, 357–368. doi: 10.1108/09654280910970929
Secker, J., Armstrong, C., and Hill, M. (1999). Young people’s understanding of mental illness. Health Educ. Res. 14, 729–739. doi: 10.1093/her/14.6.729
Seedaket, S., Turnbull, N., Phajan, T., and Wanchai, A. (2020). Improving mental health literacy in adolescents: systematic review of supporting intervention studies. Trop. Med. Int. Health 25, 1055–1064. doi: 10.1111/tmi.13449
Sprague Martinez, L., Richards-Schuster, K., Teixeira, S., and Augsberger, A. (2018). The power of prevention and youth voice: a strategy for social work to ensure youths’ healthy development. Soc. Work 63, 135–143. doi: 10.1093/sw/swx059
Stewart-Brown, S. (2006). What is the Evidence on School Health Promotion in Improving Health or Preventing Disease and, Specifically, what is the Effectiveness of the health Promoting Schools Approach?. Geneva: World Health Organization.
Teng, E., Crabb, S., Winefield, H., and Venning, A. (2017). Crying wolf? Australian adolescents’ perceptions of the ambiguity of visible indicators of mental health and authenticity of mental illness. Q. Res. Psychol. 14, 171–199. doi: 10.1080/14780887.2017.1282566
Tharaldsen, K. B., Stallard, P., Cuijpers, P., Bru, E., and Bjaastad, J. F. (2017). ‘It’s a bit taboo’: a qualitative study of Norwegian adolescents’ perceptions of mental healthcare services. Emot. Behav. Diff. 22, 111–126. doi: 10.1080/13632752.2016.1248692
Tiller, E., Fildes, J., Hall, S., Hicking, V., Greenland, N., Liayanarachchi, D., et al. (2020). Youth Survey Report 2020. Australia: Mission Australia.
Watson, A. C., Corrigan, P., Larson, J. E., and Sells, M. (2007). Self-stigma in people with mental illness. Schizoph. Bull. 33, 1312–1318. doi: 10.1093/schbul/sbl076
Wei, Y., Hayden, J. A., Kutcher, S., Zygmunt, A., and McGrath, P. (2013). The effectiveness of school mental health literacy programs to address knowledge, attitudes and help seeking among youth. Early Intervent. Psychiatry 7, 109–121. doi: 10.1111/eip.12010
Woodward, L. J., and Fergusson, D. M. (2001). Life course outcomes of young people with anxiety disorders in adolescence. J. Am. Acad. Child Adolesc. Psychiatry 40, 1086–1093. doi: 10.1097/00004583-200109000-00018
Woolfson, R., Woolfson, L., Mooney, L., and Bryce, D. (2009). Young people’s views of mental health education in secondary schools: a Scottish study. Child Care Health Dev. 35, 790–798. doi: 10.1111/j.1365-2214.2008.00901.x
Zoom Video Communications (2021). Zoom (Version 5.5.5). Available online at: https://zoom.us/ (accessed October 2, 2021).
Keywords: mental health literacy, young people, perspectives, experiences, education, school-based
Citation: Marinucci A, Grové C and Rozendorn G (2022) “It’s Something That We All Need to Know”: Australian Youth Perspectives of Mental Health Literacy and Action in Schools. Front. Educ. 7:829578. doi: 10.3389/feduc.2022.829578
Received: 06 December 2021; Accepted: 16 February 2022;
Published: 09 March 2022.
Edited by:
Lara Guedes De Pinho, University of Evora, PortugalReviewed by:
Lucília Nunes, Polytechnic Institute of Setubal, PortugalCopyright © 2022 Marinucci, Grové and Rozendorn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandra Marinucci, YWxleGFuZHJhLm1hcmludWNjaUBtb25hc2guZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.