 Daniel Prause
Daniel Prause Venke Sørlie
Venke Sørlie Lars Johan Danbolt2,4
Lars Johan Danbolt2,4 Kirsten Anne Tornøe
Kirsten Anne Tornøe
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ., 26 October 2020
Sec. Educational Psychology
Volume 5 - 2020 | https://doi.org/10.3389/feduc.2020.541498
This article is part of the Research TopicDevelopment, Wellbeing, and Lifelong Learning in Individuals with a Dual Sensory LossView all 21 articles
Introduction: Experiencing deafblindness is frequently accompanied by existential struggles. The number of older people with acquired deafblindness is fast increasing, and older persons’ health-related burdens are particularly associated with existential challenges. Hence, older persons with acquired deafblindness are explicitly exposed to existential struggles. Chaplains have a vital role in providing existential care. They do this both in congregational as well as health and social care contexts and are confronted with older persons’ religious, spiritual, and secular concerns.
Aim: The aim of this study is to explore chaplains’ lived experiences with providing existential care to older persons with acquired deafblindness.
Materials and Methods: Individual open narrative interviews were conducted with five chaplains. The interview texts were analyzed by using Lindseth and Norberg’s phenomenological hermeneutical method for researching lived experience based on Ricoeur’s interpretation theory.
Findings: The chaplains are direct and immediate during their encounters with older persons with acquired deafblindness. They can experience personal limitations when they try to alleviate the older persons’ burdens. Establishing trust and confidentiality appears to be a prerequisite for conversations about the older peoples’ existential struggles. The chaplains emphasize the importance of acknowledging the persons’ negative feelings and addressing new perspectives to a life with deafblindness. In this way, the older persons can experience reconciliation with their lives. The chaplains struggle with creating inclusive fellowships, but show high commitment trying to make that possible.
Conclusion and Implications for Health and Social Care: Chaplains can contribute to the existential well-being of older persons with acquired deafblindness through their presence in times of existential struggle. They provide existential care in a highly compassionate way, but can also experience the support they offer as insufficient. The implementation of a systematically organized service for existential care to older persons with acquired deafblindness could be worthwhile. Discourse about different ways of using (sign) language and other possibilities for the inclusion of older persons with acquired deafblindness in the Deaf Church and other communities is recommended.
Older persons are a fast increasing group within the population with acquired deafblindness due to the rising number of older people in general and, accordingly, an increasing number of persons with age-related dual sensory loss (World Federation of the Deafblind, 2018; Simcock and Wittich, 2019). The need for existential care appears explicitly in older age because of prevalent physical and mental decline and the awareness of the increasing likelihood to die (McFadden, 2013). A life with deafblindness is often accompanied by identity crises, implying an existential feeling of loneliness (Gullacksen et al., 2011), disconnection from others (Roets-Merken et al., 2017), and the world (Prause et al., in press), as well as questions about one’s value (Johansson, 2017). Therefore, access to existential care appears to be an essential concern for older persons with acquired deafblindness. Providing existential care to persons of this population is a vital function of chaplains working in the Norwegian Deaf Church. The Deaf Church serves persons with deafness and deafblindness and is an important agent within the Deaf community (Church of Norway, 2019). As with other chaplains within the Church of Norway, chaplains for the Deaf work both in congregational and institutional health and social care contexts (NOU, 2013; Church of Norway, 2015). They also serve persons with deafness or deafblindness who are not affiliated with the Deaf community and visit them in their familiar environments.
Research in existential care of persons with sensory loss is mainly confined to people with either deafness or blindness (Brennan and Bally, 2007). A literature overview of the Swedish National Resource Center for Deafblindness (2020) revealed a few studies emphasizing existential aspects regarding the support and well-being of persons with acquired deafblindness. We found no studies with an explicit focus on chaplains’ approaches toward this group. This suggests that there is a gap in the research literature about how the existential well-being of older persons with acquired deafblindness may best be supported. Since chaplains for the Deaf have a key role in providing existential care to individuals of this population, studying their experiences is a contribution to bridge this gap.
Thus, the aim of this study is to explore chaplains’ lived experiences with providing existential care to older persons with acquired deafblindness.
There exist several definitions and understandings of deafblindness in the research literature, and there has been an ongoing debate trying to conceptualize the term for suitable use in research contexts (Wittich et al., 2013; Larsen and Damen, 2014). In this study, deafblindness is understood as “a combined vision and hearing impairment of such severity that it is hard for the impaired senses to compensate for each other” (Nordic Welfare Centre, 2016). The acquired form of deafblindness is characterized by its onset after language acquisition (Larsen and Damen, 2014; World Federation of the Deafblind, 2018) and is caused by traumata, infections, genetic defects, diseases, or age-related physical degeneration (Brennan and Bally, 2007; Gullacksen et al., 2011; World Federation of the Deafblind, 2018). This definition implies varying degrees and combinations of dual sensory impairment, which makes the population of persons with acquired deafblindness a highly heterogeneous group. Persons with late-life acquired deafblindness are the largest and fastest-growing group within the population with acquired deafblindness (Brennan and Bally, 2007; World Federation of the Deafblind, 2018).
There seems to be no universal definition of the term existential care in the literature. In international research, the terms religious care and spiritual care are frequently used both as overlapping (MacKinlay, 2017) and separate concepts (Zucker et al., 2007). Due to an increasingly secularized and multicultural society in Scandinavia (DeMarinis, 2008; Stifoss-Hanssen et al., 2019), we consider the use of the term existential care as an umbrella term covering both the religious, spiritual, and also the secular dimension, as suitable in the context of this study. In addition, the challenges of older persons with acquired deafblindness elaborated in the Introduction resonate with the existential “givens” by Yalom (1980) isolation, meaninglessness, mortality, and freedom. This, we regard as a strength for using the term existential care as an overarching concept in our study.
This study is one of three parts of an article-based Ph.D. dissertation exploring existential care to older persons with acquired deafblindness. It has a qualitative design and was conducted using the phenomenological hermeneutical method for researching lived experience developed by Lindseth and Norberg (2004). This method is inspired by the interpretation theory of Ricoeur (1976) and verified to be suitable for exploring lived experience (Sørlie, 2001; Lindseth and Norberg, 2004).
Five chaplains were recruited through the Norwegian Deaf Church, which belongs to the Church of Norway, an evangelical Lutheran denomination of Protestant Christianity. It is the largest religious community in Norway (Statistics Norway, 2020). The first author contacted 12 chaplains after having received their contact information from the Deaf Church. Four of them did not wish to participate due to little or no work experience with older persons with acquired deafblindness. Three chaplains did not answer the request. The five participating chaplains were all men, between 51 and 64 years old, and their work experience with older persons with acquired deafblindness ranged from 6 to 25 years. The participants operated both in their own congregations for the Deaf and served residents with deafness and deafblindness at nursing homes. They represent all Norwegian regions (Northern, Eastern, Southern, and Western Norway). The chaplains were trained in and mastered different communication methods used by persons with acquired deafblindness. This could range from different oral to advanced and individualized tactile and haptic strategies, depending on the individual’s preferences and the nature of deafblindness (Hersh, 2013; World Federation of the Deafblind, 2018).
The first author conducted individual open narrative interviews (Mishler, 1986) with a duration of approximately 1 h. The interviews were held at the chaplains’ offices. Following the interview method described by Mishler (1986), the researcher asked one open-ended question: “What are your experiences with providing existential care to older persons with acquired deafblindness?”
Through asking clarifying questions, the researcher followed up on the chaplains’ narrations (Mishler, 1986; Lindseth and Norberg, 2004; van Manen, 2017). This interview strategy was chosen on the background of the supposition of Mishler (1986) and van Manen (2017) that the use of spontaneous language is best suitable to reveal the interviewees’ perspectives in their narrations. The data collection was provided in Norwegian oral language, and the first author transcribed the audiotaped interviews verbatim. The quotations were translated into English for the purpose of this article.
The interview texts were analyzed using the analysis method for researching lived experience by Lindseth and Norberg (2004). Following the interpretaion theory of Ricoeur (1976), the method is based on a dialectic movement between the text as a whole and parts of it. The interview transcripts were processed as one text in order to highlight general phenomena (Lindseth and Norberg, 2004). The analysis consists of the following three steps:
1. Naive reading: The researchers read the text several times. They intend to grasp the text’s meaning as a whole and make first conjectures about it.
2. Structural analysis: The text is divided into meaning units. A meaning unit can be a piece of any length containing one meaning. On the background of the naive reading, the meaning units are condensed into sub-themes, which afterward are combined into themes. The researchers discuss and reflect on the themes and sub-themes, aiming to validate the naive reading. In the case of invalidation, the whole text is reread. This process continues until the naive reading is validated by the structural analysis by all researchers. The outcome of this step corresponds to the chapter in this article under Findings.
3. Comprehensive understanding: Through rereading the text, the researchers reflect on the themes and sub-themes in reference to the interview question, the aim, and the context of the study. With the aid of relevant literature, theories, and the researchers’ preunderstandings, the text is discussed on the background of steps 1 and 2. The Discussion in this article represents this step of the analysis.
Four themes and six sub-themes emerged from the structural analysis. They are shown in Table 1. In the presentation of the findings, quotations from the interviews are used to illustrate the themes and sub-themes.
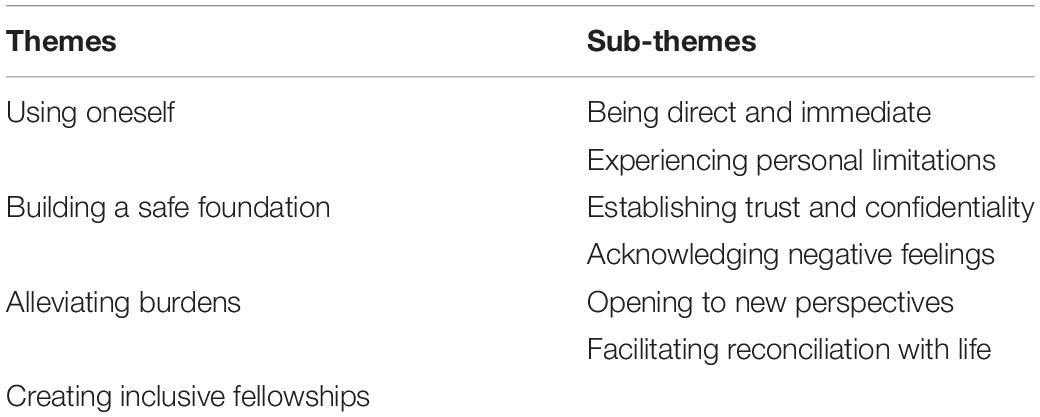
Table 1. Overview of the themes and sub-themes from the structural analysis.
The chaplains wished to give the older persons with acquired deafblindness the possibility to live out their faith equally to every other person. This appeared to be challenging because of the heterogeneity of the nature of their deafblindness, which required individual approaches to facilitate existential experiences. The chaplains were aware of finding alternative ways of providing existential care for the older persons. They sometimes found creative ways of facilitating church services and preaching the gospel for the persons. Through an individually adapted celebration with a person with deafblindness as the only participant, it was, for instance, possible to focus the entire attention on the one person, as one narration shows. The chaplain could communicate and respond directly to the older person’s current existential needs. The person with deafblindness did not follow the church service through an interpreter sitting among others, but could perceive it as a direct existential experience aligned with his individual needs:
I celebrated a complete church service individually with a deafblind man without interpreters. He experienced everything directly from me as every other church visitor usually does. This is pure and authentic. Nothing gets lost; this is church.
Sometimes, the older persons themselves asked the chaplains for direct facilitation:
An old deafblind woman wanted me to interpret her husband’s funeral ceremony for her. She knew that I mastered tactile sign language fluently and that I knew much about deafblindness. She probably wanted to have a direct experience of the ceremony through me as a chaplain. I am not an interpreter, but I could communicate without any obstacles and give her a good and direct experience.
The chaplains said that their immediacy was an essential ingredient in providing existential experiences to the older persons. They reflected that the more they knew about the distinct needs and how to communicate with the individual person, the nearer they came to creating a “real” existential experience.
According to the chaplains, such highly individual adaptations did not represent the norm, but were rare exceptions. They described that such individual adjusting could be both energy-draining and time-consuming. The chaplains felt that they usually could not prioritize the individual needs of persons with acquired deafblindness. One reason for that, mentioned during the interviews, was that chaplains for the Deaf had to cover broad areas of the country. Persons with acquired deafblindness were few, but spread throughout the regions. Due to their reduced mobility, the older persons mostly did not visit the chaplains but were reliant on being visited in their homes. This meant that the chaplains had to travel a lot to provide existential care to them.
The chaplains wished to have the possibility of focusing more detail on existential care for older persons with acquired deafblindness. They also narrated that their private engagement was the primary source of their work with this group. They said that they had several ideas to facilitate activities for persons with acquired deafblindness and put some of them into practice. They also mentioned that they would not promote these ideas due to fearing a high amount of inquiries, which they were not able to manage:
I don’t tell openly about this individually adapted church service I came up with. I don’t want to cause high expectations. You have, unfortunately, to be cynical and say ‘no’ to things you don’t have time to do.
The chaplains said that one reason for their high engagement was the feeling of experiencing something exceptional during encounters:
To be preacher and organizer for spiritual experiences for this deafblind man was at the other end of the scale of all things I have done. If I had to choose, I would rather celebrate an individual church service with him than having a great church service with the king. The deafblind man, in a way, is my king.
Contributing to the older persons’ existential well-being sometimes could go along with the chaplains feeling that the support they offered was insufficient. The following narration illustrates this: A chaplain tried to explain to an older man with severe dual sensory loss that they were about to have a church service. Establishing communication with the man was very difficult,
[…], but when I succeeded in making him understand that we were about to celebrate a church service, I felt that I really had contributed to something important. At the same time, I recognized that I actually did not do much at all. I felt desperate because I wasn’t able to do more for him.
The chaplains explained that although they succeeded in contributing to positive experiences, the consequences of deafblindness, nevertheless, invaded the older persons’ lives so much that it was highly challenging to make a difference at all.
The chaplains experienced that older persons with acquired deafblindness often met them with skepticism and caginess during their first encounters. This could be expressed through meetings where the older people showed interest in a conversation but wished to finish it and withdrew after a short time. The chaplains said that they repeatedly emphasized during these encounters that professional confidentiality was an inherent part of their profession. They also described a possible lack of confidentiality as a recurring topic, which the older persons often were concerned about. The chaplains elaborated that deafblindness could provoke a loss of control of where private information was spread, especially with a view to the small population of persons with deafblindness and its transparency. According to the chaplains, it usually took several meetings before the older persons felt confident enough to allow a conversation of a private character. The following quotation about encounters with a resident at a nursing home illustrates this:
We talked about very sensitive issues, which affected her life to a great extent, but it took many rounds before she introduced these private aspects to me. Among other things, she somehow checked if my colleague knew about our meetings. Not until she got confirmed that he didn’t know anything about them, she trusted in me and my confidentiality and opened up.
Achieving trust, especially in their confidentiality, the chaplains experienced as a long process requiring patience and sensibility. According to them, they had to sense during their conversations whether it was appropriate or not to go deeper into the older persons’ narrations. Sometimes, when the older people opened up and started to talk about existential matters, it could, nevertheless, feel right to give the older persons’ thoughts time to mature before continuing in that vein:
Some doors don’t open up at once, but there is a tiny crack. You must not misuse this crack, but you have to wait. Sometimes you even have to withdraw.
The chaplains also thought that the simple fact of being a chaplain could be sufficient to establish the older persons’ trust. The following quotation about a chaplain’s first workday at a nursing home describes how important the role of a chaplain could be for an older man with acquired deafblindness. The nursing home had no permanent chaplain service during a period before the chaplain started working there. This made the older man increasingly restless and anxious. He smoked much more than he used to. The man asked the nursing staff to send the new chaplain to him as soon as possible:
He sat agitatedly in his little “cave” filled with cigarette smoke. During our first conversation, I recognized that he calmed down. The following period with regular meetings helped to decrease smoking a lot. He was genuinely interested in religious questions and had a deep belief in God. He did also take Communion for the first time. The nursing staff was astonished. Nobody had recognized that this was such an urgent need for him.
The chaplains described their strategy approaching older people as carefully observant. They wanted to avoid them feeling pressure to talk about existential issues. When the persons opened up and talked about sensitive life experiences, the ability to listen and acknowledge the older persons’ feelings was an essential skill, according to the chaplains. The analysis revealed that the chaplains’ specific mission was to acknowledge the older persons’ negative feelings. Showing them that their feelings were normal reactions on negative experiences could help the older people cope with them:
I visited a deafblind woman at a nursing home. She said that she was very unhappy due to deafness, blindness, and not living at her house anymore. I replied: “Just be sad and tell me more about it if you want.” During our next meeting, she said: “Last time you visited me, I was so depressed, and you said: ‘Just be sad’. Simply that made me very happy.”
Reflecting on this narration, the chaplain interpreted that his conversations did not have to lead to anything. His ambition was not to make the woman think that her problems would disappear. Instead, she was provided the possibility to enunciate her feelings, which he acknowledged as normal human reactions.
During their visits to nursing homes, the chaplains sometimes observed that nursing staff did not focus on the older persons’ negative feelings. The nurses tried instead to distract them by cheering them up and focusing on abilities and resources, which the older people, despite their deafblindness, still had. According to the chaplains, negative feelings often were neglected when the staff was pressed for time. Nursing staff had to embed existential conversations between several other challenging tasks during their shifts. The chaplains also experienced time limitations, but they could plan their visits and, therefore, often avoid being stressed.
According to the chaplains, to acknowledge negative feelings meant more than just listening to and confirming the older persons. They also saw it as their duty to follow them all the way through grievous and challenging life episodes. They wanted to understand and endure the persons’ existential pain, as the following example illustrates: An older woman had experienced domestic violence, which caused deafblindness. Subsequently, she also lost contact with her children. Due to her needs, she lived at a nursing home and became unassertive and isolated. A chaplain became one of her persons of trust. He got to know her tale of woe and followed her through the coping process. He described the essence of providing existential care to the woman as follows: “It is my mission daring to go into her pain of losing both hearing and sight because of a meaningless trauma. I also have to dare to go into her pain of missing her children. I must have the strength to be with her in her unfathomable loss.”
The chaplains also talked about acknowledging the older persons’ philosophy of life, notwithstanding if it was of religious, spiritual, or secular nature. The conversations were seldom about God, but the chaplains had an overarching comprehension that challenges in life also were about the relation to God:
I don’t necessarily talk with them [the older persons with acquired deafblindness] about their belief in God, but often about resources and possibilities in life. For me, God actually is about that. When life is challenged, your relation to God also is challenged. So, you can provide good existential care in periods of crises without talking about God, but about life.
The chaplains did not directly confront the older people with their perspective that life automatically is about God. Still, they said that it helped them to understand the persons’ existential struggles.
During the encounters and conversations with older people with acquired deafblindness, the chaplains observed that the need for existential care was more urgent in the period where hearing and sight were about to disappear. This period they described as an experience of crisis for the persons concerned. Finally, becoming completely deafblind could go along with a feeling of relief. Instead of using their energy on the remaining hearing and sight abilities, they could focus entirely on the haptic sense, according to the chaplains.
A central subject emerging during the interviews was the chaplains’ experiences with the older persons’ loss of independence. They narrated about the grief of losing the ability to live an independent life. In this context, the chaplains emphasized that the older people had to carry multiple burdens. They had to adapt to all the “usual” changes related to becoming old, e.g., frailty, diseases, or moving to a nursing home. In addition, they had to cope with becoming both deaf and blind, which meant to arrange their lives in a fundamentally new way. The chaplains tried to help the older persons to see their life from a different perspective by supporting them to strengthen both their faith in God and possibilities to improve their life situation:
To protect yourself in such a period of change, you have to hold on to something. This ‘something’ can be the belief in God or the trust in finding a solution for living your life differently.
The chaplains saw it as their responsibility to support the persons’ adaptation to a new life. At the same time, it filled them with contentedness when the persons overcame a period of crisis and could accept life changes with their help:
We can’t remove all adversity from life, but we can have a role in helping to endure difficult life periods. To see persons developing themselves through my contribution gives me a feeling of satisfaction.
The chaplains experienced that some older persons did not overcome this period. Instead, the persons constantly uttered their experiences of injustice about their distinct needs as persons with deafblindness not being understood by others or society in general. The chaplains experienced that some persons could be so obsessed with fighting for their rights that they were stuck in the process of accepting their deafblindness. For the chaplains, it was challenging to encourage them to focus on new possibilities. Instead, some persons continued to look at their life from the perspective of a victim.
Sometimes, conversations about the past could reveal burdens, which the older persons had carried during a long life period, sometimes without telling anyone else. According to the chaplains, some persons could feel like a failure and still be ashamed because of something they did in their early life, which did not correspond to social conventions:
When she [an older woman with acquired deafblindness] was young, she left home with a man who was not liked by her family. They broke up, and she came back. She had been ashamed about that since then.
The chaplain tried to help the woman to view this life episode in light of a new perspective. While she focused on her weakness of failing, the chaplain suggested instead to look at her strength:
I said to her: ‘You left your family and home town for love. I think that was actually very courageous.’
Through this approach, she was able to look at her life in a different light and began to accept it:
She began to rethink. No one had ever proposed this perspective to her.
After that, the woman could cope better with her shame, according to the chaplain. Her deafblindness was not the cause of her shame and struggles, but the chaplains experienced that isolation through deafblindness could increase the feeling of being alone with one’s problems and worries. According to the chaplains, deafblindness seemed to be an intensifier of burdens.
The chaplains placed great emphasis on creating inclusive fellowships for the older persons with deafblindness. They tried to do this, for instance, through facilitating participation at church services. These were both held in the chaplains’ congregations for the Deaf and during their visits to health and social care institutions. The church services gathered both persons with deafness and deafblindness. The chaplains experienced the inclusion of the latter as a challenge. The findings show that their participation at activities required detailed practical preparation by the chaplains. The older persons had varying degrees of hearing and sight, as well as different ways of communicating. Therefore, the chaplains had to ponder on different strategies to place the persons considering their remaining senses and abilities to grasp acoustic and/or visual signals. They strove to give every single person an experience of wholeness and being included. To find one communication method suiting everyone, the chaplains experienced as practically impossible. They said that, during church services for the Deaf, they were required to use Norwegian sign language (which has a visual–manual modality without sound with its own grammar). Sometimes, the chaplains experienced that the use of signed speech (a word-by-word translation where the spoken words are signed simultaneously to their pronunciation) could be beneficial to include participants with acquired deafblindness:
I agree that it is important to have Norwegian sign language as our standard language. However, there is an increasing amount of people with sensory loss profiting from voice and sound. Without opening up for alternatives, we risk to exclude some people from our fellowship.
It appeared especially challenging to include older persons without any sign language skills in fellowships because of the restricted possibilities to communicate. The following narration exemplifies how a chaplain can succeed in creating an inclusive fellowship for such an individual: A chaplain welcomed a resident to a church service at a nursing home. He had no sight, extremely minimal hearing, and did not know sign language:
[…] so I just had to shout at him: ‘I am the chaplain!’ Usually, after three or four attempts, he asked: ‘Are you the chaplain?’ I answered: ‘Yes!’ Then he asked: ‘Are we having a church service now?’ I shouted: ‘Yes!’ He answered: ‘So nice!’ and sat down. He neither saw anything nor noticed any words or hymns. Nevertheless, I saw him smiling and enjoying being there. I think he understood what was going on, so he could feel being a part of our Christian fellowship. Just reaching him with a few shouts made him understand the context of the situation and feel included. A tiny effort can make a big difference.
The chaplains also reflected on the ability of persons with deafblindness to have existential experiences by sensing the atmosphere inside a church, as is expressed in this quotation:
I believe that people with deafblindness can sense a certain spirit when they are at church even without hearing and seeing anything. Something changes.
In this study, chaplains narrated about their experiences with providing existential care to older persons with acquired deafblindness. The analysis revealed that for the chaplains, using oneself, building a safe foundation, alleviating burdens, and creating inclusive fellowships were essential aspects of providing existential care. According to the third step of the analysis, comprehensive understanding, some of the findings are discussed with a focus on the chaplains’ challenges of being present and inclusive.
The chaplains were attentive to the older persons’ degree of openness to existential issues and adjusted the content of the conversations to their receptivity. They were aware of not giving the older persons an expectation of solving their problems or eliminating all adversity, as one chaplain described it. Instead, they focused on being present and guiding the persons through the process of accepting and embracing their challenges and, in this way, adapt to a new life condition, namely deafblindness. One chaplain, for instance, described it as his mission to share the deepest moments of pain and loss with the person. This corresponds with Cramer et al. (2013) and Adams (2019), who emphasize that chaplains’ presence is crucial for the person’s healing process. Adams (2019) describes presence as “establishing an environment of care based on empathy, curiosity, and respect in which the chaplain is attentive to the verbal and non-verbal two-way communication and assessing questions of the spiritual, the sacred, and of meaning […]” (p. 1255).
According to this definition, presence is an intimate active task that leads to a person’s recovery and well-being. Like Adams, Pargament (2013), and Schnell (2016) describe the vital role of the sacred dimension and the search for meaning. Through the following two paragraphs, we discuss existential challenges related to acquired deafblindness and our findings using the approaches of Pargament (2013) and Schnell (2016).
Pargament (2013) emphasizes that sacred experiences in a caring relationship can not only help patients to mobilize hope but also support providers to feel more empowered to do their work. He describes the sacred as being “touched by each other” and “moments of profound interconnectedness” (Pargament, 2013, p. 406) between the providers and patients. Research shows that nurses have expressed similar experiences in the care of patients with acquired deafblindness. They connected empathically with the patients and had “no words that can describe this feeling” (Prause et al., in press). Related to our current study, the description of the individually adapted celebration of a church service with the chaplains’ expressions “the deafblind man, in a way, is my king” and “nothing gets lost; this is church” can be a sign of such a sacred element. According to this understanding, the chaplain’s presence preaching the gospel in his direct, close, and immediate way created a sacred atmosphere. Through interconnecting, the older man with deafblindness became “his king,” and the chaplain had an experience of “living church.”
Schnell (2016) points out that experiencing meaning relies on how a person experiences life as coherent, significant, orientated, and belonging. According to Gullacksen et al. (2011), the experience of becoming deafblind interrupts the connection between the past and the present, which in turn makes it difficult to imagine one’s future. Caregivers can counteract this feeling of incoherence over time through a combination of emotional and practical support (Olesen and Jansbøl, 2005). Roets-Merken et al. (2017) describe a category of existential challenges when becoming deafblind, implying thoughts like being stupid, forgotten, and not being significant anymore. As well, to orientate oneself is one of the most affected abilities when becoming deafblind. It hinders independent participation in social life and makes everyday activities nearly unfeasible without personal and technical support (Nordic Welfare Centre, 2016). Many persons with acquired deafblindness also struggle with the feeling of belonging. Neither communities for the Deaf nor the Blind share their distinct needs (Kyle and Barnett, 2012; Hersh, 2013). Because of the complexity and the individual differences of their disability, it is challenging to form a group identity together with other persons with deafblindness (Gullacksen et al., 2011; Kyle and Barnett, 2012). Concluding, becoming deafblind restricts all the four elements Schnell (2016) describes as fundamental for experiencing meaning in life. This is exemplified through the narration about the woman who lost both hearing and sight due to domestic violence. Additionally, she missed contact with her children. Drawing on Schnell (2016), her life’s coherence, significance, orientation, and belonging were turned upside down by “a meaningless trauma.” Through being present and enduring with the woman through her pain “in her unfathomable loss,” the chaplain stayed by her side when she searched for meaning.
Our findings show that the chaplains provided existential care with a high amount of compassion. Being present during existential encounters with the older persons could be energy-draining for the chaplains. Although they apparently contributed to existential well-being, they questioned whether their support was sufficient to alleviate the older persons’ burdens and wished to do more for them. This corresponds with Cramer et al. (2015), who state that chaplains regularly are uncertain about whether their interventions had been successful or not. Furthermore, they write that the feeling of having succeeded often relies on the chaplains’ intuition. Hotchkiss and Lesher (2018) emphasize in this context chaplains’ experiences of compassion satisfaction, which they define as benefiting “from many intrinsic emotional rewards for caring for patients and other clients” (p. 87). The narration about the celebration of the individual church service can again be mentioned as an example illustrating this.
In contrast, Figley and Figley (2017) point out that care workers can also experience compassion fatigue. This is described as a condition of exhaustion where the carer experiences an uncontrolled increase of compassion due to the cumulative exposure to a client’s suffering (Figley and Figley, 2017). The chaplains in our study did not talk about exhaustion. However, although they experienced success, they felt that their effort had almost no significance. They could feel desperate because they were not able to do more for the older persons. Highlighting our findings from the perspective of Figley and Figley (2017) and Hotchkiss and Lesher (2018), it is appropriate to assume that the chaplains could be exposed to a constant tension between compassion satisfaction and compassion fatigue.
Even though the chaplains talked about being energy-drained, they were not exhausted, but rather highly motivated. In this context, Pargament (2013) describes that sacred moments between a care provider and a client can be a source of satisfaction for the carer. Drawing on Pargament (2013) in relation to Figley and Figley (2017) and Hotchkiss and Lesher (2018), it is reasonable to suggest that experiencing sacred moments could be a source of energy and satisfaction. This could help the chaplains to endure the older persons’ suffering and protect themselves from compassion fatigue.
The chaplains were touched by the existential challenges, which dual sensory loss inflicted on the older people, and pointed out that deafblindness could intensify a person’s burdens. We highlight this from the perspective of existential psychology by Yalom (1980). Following Yalom (1980), isolation, meaninglessness, mortality, and freedom are existential “givens” in everyone’s life. Older persons with acquired deafblindness are left behind (Simcock and Wittich, 2019) in isolation, disconnected from others (Roets-Merken et al., 2017) and the world (Prause et al., in press), and questioning their self-value (Johansson, 2017). Besides, older persons have to cope with approaching frailty and death (McFadden, 2013). This can indicate that the “givens” described by Yalom (1980) are challenged extraordinarily in older persons with acquired deafblindness. It seems reasonable to suggest that the accumulation of existential struggles makes it especially challenging for the chaplains to get through to the older persons. In this vein, acquired deafblindness could be experienced as an intensifier not only by the persons concerned but also by the chaplains when caring for them. Hence, experiencing a sacred moment when caring for an older person with acquired deafblindness could be perceived in an intensified and highly compassionate way.
However, in health and social care contexts, chaplaincy is one of several professions providing existential care, which makes the chaplains’ role diffuse and difficult to distinguish from others (Cramer et al., 2013). Nurses, for instance, have a significant role in taking care of patients’ existential needs (Clarke, 2017; MacKinlay, 2017; Giske and Cone, 2019). Tornøe (2017) found that nurses’ presence and relatedness to patients in palliative care could have a consoling effect in a period of suffering. A recent study shows that nurses can guide older patients with acquired deafblindness through existential crises in periods of loss and loneliness (Prause et al., in press). The field of spiritual and existential care in nursing practice is getting increasing attention (Puchalski, 2013; Clarke, 2017; Giske and Cone, 2019). Consequently, it seems appropriate to question the chaplains’ distinct function of providing existential care in health and social care contexts.
The chaplains in our study, for example, distinguished their role in existential care from the nursing profession. They talked about observations that nurses could neglect the patients’ negative feelings. The chaplains, in contrast, saw responding to these feelings as their specific responsibility. The narration about the older man who reduced smoking and began talking about his existential struggles exemplifies the chaplain’s significance. The man did not address his challenges to the nursing staff. His urgent religious–existential need to take Communion was revealed through the chaplain’s acknowledgment of the man’s negative feelings and enduring his existential suffering. This narration is an example of a chaplain’s distinct function, with immediate positive consequences for an older person’s well-being and recovery. The example also shows that the importance of religious aspects in geriatric care must not be underestimated, especially for the current cohort of older persons with a closer relation to religious beliefs and faith than do younger generations (MacKinlay, 2017).
However, chaplains are increasingly confronted with peoples’ secular challenges and struggles (DeMarinis, 2008; Swift, 2019). The understanding of chaplaincy has changed from a traditional focus on preaching the gospel to a holistic view on what is at stake in a person’s life and through this answer his/her need for existential care (Stifoss-Hanssen et al., 2019). The switch between a traditional and a holistic way of providing existential care can be challenging for chaplains. A narration in our study exemplifies how they can manage to bridge this: A chaplain talked about his understanding of life as given by God. He said that a challenged life automatically challenged the relation to God. In this vein, talking about life means talking about God, although God is not explicitly mentioned in his conversations with the older persons. The chaplain adapted his understanding of life as God-given to the persons’ understanding of life without adopting a preaching attitude. This broad way of providing existential care could give a forward-looking hint to a chaplain’s role in an increasingly secular society as well as the need for cooperation between professions in health and social care contexts. Opening up to religious and spiritual diversity could also mean engaging religious workers from other faiths and initializing cooperation with their congregations.
Another significant concern for the chaplains in our study was to include older persons with acquired deafblindness in fellowships, for instance through participation at church services. The chaplains strove to adapt the physical environment to the older persons’ individual needs, but felt that this was impossible and experienced the support they offered as insufficient. This resonates with several studies confirming that facilitating social participation for older persons with acquired deafblindness is highly challenging (Möller, 2008; Gullacksen et al., 2011; Johansson, 2017; Simcock and Wittich, 2019). These challenges can be a reason for the lack of participation in church attendance and other religious activities of older persons with dual sensory loss (Mick et al., 2018). The diversity of the older persons’ presuppositions, even within the population of persons with acquired deafblindness, makes it impossible to gather everyone under one umbrella (Gullacksen et al., 2011). The chaplains in our study described these challenges as the main reason for struggling with creating inclusive fellowships.
In addition, the chaplains were obliged to act in accordance with the mandated liturgy of the Deaf Church, and they missed a more flexible practice of using (sign) language in a way that also included persons who benefit from auditive stimuli. New technologies can help persons with deafness and deafblindness benefit from speech and sound (Gifford and Revit, 2010). Hence, the number of persons using several language modalities could increase in the future. Besides, the population of persons who become deafblind in older age will grow rapidly (World Federation of the Deafblind, 2018; Simcock and Wittich, 2019), which implies that the number of those without any relation to the Deaf community and sign language also increases. Furthermore, teaching older persons new communication methods, such as sign language, requires extensive prerequisites, which are challenging to achieve (Simcock and Wittich, 2019). This implicates that there is a growing number of older persons with acquired deafblindness without any sign language skills. Following this argumentation, taking care of an increasing number of non-sign language users within a community, whose identity is based on sign language, sounds contradictory. Thus, the chaplains inevitably ended up in a predicament: They were torn between a basic commitment to the Deaf Church and the commitment to the individual congregation members or participants of the church services. In this context, the differences between the needs of persons who are deaf and persons with deafblindness emerge. Kyle and Barnett (2012) found that both persons with deafblindness and persons who are (only) deaf frequently have an alienated picture of the respective other group. Vision impairment restricts possibilities for communication between them to a great extent. In addition, persons with acquired deafblindness often are not familiar with the feeling of being part of a community because group activities mostly are conducted with the aid of individual interpreters, while direct contact between the persons is rare (Kyle and Barnett, 2012).
However, the Church of Norway (2010) sees itself as a serving and caring church “expressed through the grace of charity, including fellowship, protection of the work of creation, and the battle for justice” (p. 9). In line with that, the Deaf Church has the ambition to include persons with deafblindness into its fellowship and place them on equal terms with persons who are (only) deaf (Church of Norway, 2019). As elaborated above, the diversity of persons with acquired deafblindness in consideration of their different needs can make it highly challenging to reach this aim. Hence, using either sign language or signed speech strictly during church services would, in any case, exclude individuals or groups.
As an alleviating factor, the Deaf Church supports the facilitation of interpreter and guide services for persons who want to stay in their home congregations (Church of Norway, 2019). This could help answer the older persons’ distinct communicational needs, and they could stay in their familiar arenas. Following this approach, a distinction within the population with deafblindness between persons related to the Deaf milieu and persons without that relatedness could be appropriate. Persons without a relation to the Deaf community could benefit from following church services for hearing and sighted people with the aid of adapted technical devices and/or voice interpreters. Persons knowing the Deaf milieu and sign language could join the Deaf Church. Due to the challenges of belonging, discussed above, a feeling of alienating nevertheless might be unavoidable for the persons concerned.
Although the chaplains often experienced the support they offered as insufficient, they showed much dedication to their work. They did not resign trying to give the older persons a sense of belonging and inclusion. This is especially illustrated in the narration about the older man without any possibilities to communicate orally or touch-based. In this case, the crucial thing for him was to understand the context of his attendance. Although he did not understand any words or hymns, he smiled and enjoyed the church service. Following the argumentation of Pargament (2013), the man might have felt fellowship through a sacred experience, which made him feel included. Using the meaning-making model of Schnell (2016), this experience, in turn, could help restore the man’s coherence, significance, orientation, and belonging as a person living isolated by deafblindness. In this vein, the chaplain’s effort in letting the man know what was going on can be seen as an act of care contributing to the man’s existential well-being.
Further, the chaplains reflected on how persons with deafblindness without any systematic communication strategies could perceive existential experiences. One narration was about a chaplain’s belief that persons with deafblindness were even able to experience an inwardly change when they were at church. In this context, Morris (2008) discusses whether the pure act of being in a church could provoke a mysterious experience and enable a person with deafblindness to “encounter something of God and respond to it” (p. 86). According to the chaplain’s narration and Morris (2008), these are conjectures based on single beliefs and observations. Still, in light of Pargament (2013) and Schnell (2016), these conjectures could be a reason to fathom this aspect further.
A text analysis can result in different interpretations. Hence, the interpretation presented in this study has to be seen as one possible way to understand the chaplains’ experiences. To ensure rigor, all authors undertook the naive reading individually. They discussed their outcomes together as a basis for the structural analysis, which was performed by the first author. Each co-author critically reviewed the first author’s structural analysis. Aiming to attain a comprehensive understanding, all authors discussed the first author’s structural analysis and concluded that it was consistent with the naive readings.
The first author’s background as a nurse caring for older persons with dual sensory loss may have influenced his data interpretation. However, the co-authors, coming from different backgrounds such as theology/psychology of religion and nursing education, supported the first author’s interpretation, which strengthened the confirmability of the structural analysis.
Due to its qualitative design with five participants, this study cannot draw upon generalization. However, highlighting a narrow aim and experiences, which are sparsely described in the research literature, as it is in our study, few participants can generate sufficient information power to give valid insights into individuals’ lives (Malterud et al., 2016).
This study explored the experiences of chaplains of an evangelical Lutheran denomination. Considering Norway as an increasingly multicultural and secularized society (DeMarinis, 2008; Stifoss-Hanssen et al., 2019), we take into account that existential care is also provided by agents of other belief systems, which could lead to different findings.
Providing existential care to older persons with acquired deafblindness is a demanding task for chaplains. The findings suggest that chaplains can contribute to existential well-being and a positive change of perspectives to life by being present and accompanying older persons through periods of existential struggle. The chaplains’ compassion can be a resource for providing existential care, but can also activate a feeling that the support they offer is insufficient. Existential care to older persons with acquired deafblindness is mainly based on the chaplains’ private engagement. Therefore, the implementation of a systematically organized service within the Deaf Church or other communities could be worthwhile. Challenges with including the older people in fellowships could be alleviated by enabling the chaplains to use (sign) language more flexibly. Both in general and concerning the ambition of the Deaf Church, reaching equal possibilities for participation for both persons with deafness and deafblindness, a discourse about how to achieve this aim can be recommended. Due to the limited body of literature about existential care to older persons with acquired deafblindness, we require a closer research focus on this topic.
The datasets generated for this study are available on request to the corresponding author.
The study followed the rules of the Declaration of Helsinki and was approved by the Norwegian Centre for Research Data (NSD) with project number 60098. The chaplains were informed that participation was voluntary and that they could withdraw from the study at any time. Confidential data were anonymized in the transcripts. The participants gave their written and informed consent prior to the interviews.
DP, VS, LD, and KT designed the study, performed the structural analysis, and contributed to the interpretation of the findings and the critical review of the manuscript. DP collected the data, transcribed the interviews, and drafted the manuscript. All authors approved and read the final manuscript.
This study received funding from Signo Conrad Svendsen Centre, Oslo, Norway (grant no. 253).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank the chaplains for participating.
Adams, K. (2019). Defining and Operationalizing Chaplain Presence: A Review. J. Rel. Health 58, 1246–1258. doi: 10.1007/s10943-018-00746-x
Brennan, M., and Bally, S. J. (2007). Psychosocial Adaptations to Dual Sensory Loss in Middle and Late Adulthood. Trends Amp. 11, 281–300. doi: 10.1177/1084713807308210
Church of Norway (2019). Årsmelding 2018, Døvekirken [Annual Report 2018, Deaf Church]. Oslo: Den norske kirke.
Clarke, J. (2017). Spiritual care in everyday nursing practice. A new approach, 2nd. Edn., London: Palgrave Macmillan.
Cramer, E. M., Tenzek, K. E., and Allen, M. (2013). Translating Spiritual Care in the Chaplain Profession. J. Past. Care Counsel. 67, 1–16. doi: 10.1177/154230501306700106
Cramer, E. M., Tenzek, K. E., and Allen, M. (2015). Recognizing Success in the Chaplain Profession: Connecting Perceptions With Practice. J. Health Care Chaplain. 21, 131–150. doi: 10.1080/08854726.2015.1071543
DeMarinis, V. (2008). The Impact of Postmodernization on Existential Health in Sweden: Psychology of Religion’s Function in Existential Public Health Analysis. Arch. Psychol. Rel. 30, 57–74. doi: 10.1163/157361208x316962
Figley, C. R., and Figley, K. R. (2017). “Compassion Fatigue Resilience,” in Oxford Handbooks Online, eds E. M. Seppälä, E. Simon-Thomas, S. L. Brown, M. C. Worline, C. D. Cameron, and J. R. Doty (Oxford: Oxford University Press), doi: 10.1093/oxfordhb/9780190464684.013.28
Gifford, R. H., and Revit, L. J. (2010). Speech Perception for Adult Cochlear Implant Recipients in a Realistic Background Noise: Effectiveness of Preprocessing Strategies and External Options for Improving Speech Recognition in Noise. J. Am. Acad. Audiol. 21, 441–451. doi: 10.3766/jaaa.21.7.3
Giske, T., and Cone, P. H. (2019). Å ta vare på heile mennesket. Handbok i åndeleg omsorg [Caring for the whole person. Handbook of spiritual care]. Oslo: Det Norske Samlaget.
Gullacksen, A.-C., Göransson, L., Rönnblom, G. H., Koppen, A., and Jørgensen, A. R. (2011). Life Adjustment and Combined Visual and Hearing Disability/Deafblindness: An Internal Process over Time. Stockholm: Nordic Centre for Welfare and Social Issues.
Hersh, M. (2013). Deafblind people, communication, independence, and isolation. J. Deaf Stud. Deaf Edu. 18, 446–463. doi: 10.1093/deafed/ent022
Hotchkiss, J. T., and Lesher, R. (2018). Factors Predicting Burnout Among Chaplains: Compassion Satisfaction, Organizational Factors, and the Mediators of Mindful Self-Care and Secondary Traumatic Stress. J. Past. Care Counsel. 72, 86–98. doi: 10.1177/1542305018780655
Johansson, A.-B. (2017). Se och hör mig: Personer med förvärvad dövblindhets erfarenheter av delaktighet, rehabilitering och medborgerligt liv [See and hear me: Experiences of persons with acquired deafblindness with participation, rehabilitation, and civic life]. Ph.D. Dissertation, University of Gothenburg, Gothenburg.
Larsen, F. A., and Damen, S. (2014). Definitions of deafblindness and congenital deafblindness. Res. Dev. Disabil. 35, 2568–2576. doi: 10.1016/j.ridd.2014.05.029
Lindseth, A., and Norberg, A. (2004). A phenomenological hermeneutical method for researching lived experience. Scand. J. Caring Sci. 18, 145–153. doi: 10.1111/j.1471-6712.2004.00258.x
MacKinlay, E. (2017). The spiritual dimension of ageing, 2nd. Edn., London: Jessica Kingsley Publishers.
Malterud, K., Siersma, V. D., and Guassora, A. D. (2016). Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 26, 1753–1760. doi: 10.1177/1049732315617444
McFadden, S. H. (2013). “Old Persons, Old Age, Aging, and Religion,” in Handbook of The Psychology of Religion and Spirituality, 2. Edn., eds R. F. Paloutzian and C. L. Park (London: The Guilford Press), 198–212.
Mick, P., Parfyonov, M., Wittich, W., Phillips, N., and Pichora-Fuller, M. K. (2018). Association between sensory loss and social networks, participation, support, and loneliness. Analysis of the Canadian Longitudinal Study on Aging. Can. Fam. Physician. 64, e33–e41.
Mishler, E. G. (1986). Research interviewing: Context and narrative. Cambridge: Harvard University Press.
Möller, K. (2008). Impact on Participation and Service for Persons With Deafblindness. Ph.D. Dissertation, Örebro University, Örebro.
Morris, W. (2008). Theology Without Words: Theology in the Deaf Community. Explorations in Practical, Pastoral and Empirical Theology. Hampshire: Ashgate Publishing Limited.
National Resource Center for Deafblindness (2020). Research overview. Lund: National Resource Center for Deafblindness.
NOU (2013). Det livsåpne samfunn. En helhetlig tros- og livssynspolitikk [The life open society. Holistic politics concerning faith and philosophy of life]. Oslo: Departementenes servicesenter.
Olesen, B. R., and Jansbøl, K. (2005). Experiences from people with deafblindness - A Nordic project. Herlev: Information Center for Acquired Deafblindness.
Pargament, K. I. (2013). Conversation with Eeyore: Spirituality and the generation of hope among mental health providers. Bull. Menninger. Clin. 77, 395–412. doi: 10.1521/bumc.2013.77.4.395
Prause, D., Sørlie, V., Danbolt, L. J., and Tornøe, K. A. (in press). Sensing loneliness - Nurses’ experiences with providing existential care to older patients with acquired deafblindness. Nordic Nursing Research.
Puchalski, C. M. (2013). Integrating spirituality into patient care: an essential element of person-centered care. Pol. Arch. Med. Wewn. 123, 491–497. doi: 10.20452/pamw.1893
Ricoeur, P. (1976). Interpretation theory: Discourse and the surplus of meaning. Fort Worth: Texas Christian University Press.
Roets-Merken, L., Zuidema, S., Vernooij-Dassen, M., Dees, M., Hermsen, P., Kempen, G., et al. (2017). Problems identified by dual sensory impaired older adults in long-term care when using a self-management program: A qualitative study. PloS One 12:e0173601. doi: 10.1371/journal.pone.0173601
Schnell, T. (2016). Psychologie des Lebenssinns [The psychology of meaning in life]. Berlin: Springer.
Simcock, P., and Wittich, W. (2019). Are older deafblind people being left behind? A narrative review of literature on deafblindness through the lens of the United Nations Principles for Older People. J. Soc. Welf. Fam. Law 41, 339–357. doi: 10.1080/09649069.2019.1627088
Sørlie, V. (2001). Being in ethically difficult care situations. Narrative interviews with registered nurses and physicians within internal medicine, oncology and paediatrics. Ph.D. Dissertation, Umeå University, Umeå.
Stifoss-Hanssen, H., Danbolt, L. J., and Frøkedal, H. (2019). Chaplaincy in Northern Europe. An overview from Norway. J. Pract. Theol. 36, 60–70.
Swift, C. (2019). “The Role of the Healthcare Chaplain: A Summary of the Contribution of Healthcare Chaplains to Modern Healthcare Practice,” in Spirituality in Healthccare: Perspectives for Innovative Practice, eds F. Timmins and S. Caldeira (Cham: Springer), 151–164. doi: 10.1007/978-3-030-04420-6_10
Tornøe, K. A. (2017). The Challenge of Consolation: A qualitative study of nurses’ experiences with practicing and teaching spiritual and existential care for the dying. Ph.D. Dissertation, Norwegian School of Theology, Oslo.
van Manen, M. (2017). Researching Lived Experience. Human Science for an Action Sensitive Pedagogy, 2nd. Edn., New York, NY: Routledge.
Wittich, W., Southall, K., Sikora, L., Watanabe, D. H., and Gagné, J.-P. (2013). What’s in a name: Dual sensory impairment or deafblindness? Br. J. Vis. Imp. 31, 198–207. doi: 10.1177/0264619613490519
World Federation of the Deafblind (2018). At risk of exclusion from CRPD and SDGs implementation: Inequality and Persons with deafblindness. Initial global report on situation and rights of persons with deafblindness. Oslo: World Federation of the Deafblind.
Keywords: existential care, deafblindness, dual sensory loss, chaplain, older persons, qualitative interview, phenomenological hermeneutics, Ricoeur
Citation: Prause D, Sørlie V, Danbolt LJ and Tornøe KA (2020) The Challenge of Being Present and Inclusive: Chaplains’ Experiences With Providing Existential Care to Older Persons With Acquired Deafblindness. Front. Educ. 5:541498. doi: 10.3389/feduc.2020.541498
Received: 09 March 2020; Accepted: 30 September 2020;
Published: 26 October 2020.
Edited by:
Walter Wittich, Université de Montréal, CanadaReviewed by:
Peter Simcock, Birmingham City University, United KingdomCopyright © 2020 Prause, Sørlie, Danbolt and Tornøe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Prause, ZGFuaWVsLnByYXVzZUBzaWduby5ubw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.