 Catherine Malboeuf-Hurtubise
Catherine Malboeuf-Hurtubise Geneviève Taylor
Geneviève Taylor Linda Paquette
Linda Paquette Eric Lacourse5
Eric Lacourse5
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Educ. , 03 September 2018
Sec. Educational Psychology
Volume 3 - 2018 | https://doi.org/10.3389/feduc.2018.00066
This article is part of the Research Topic How Can Education Better Support the Mental Health & Wellbeing of Young People? Contributions from Developmental Psychopathology & Educational Effectiveness Research View all 13 articles
Background: Mindfulness-based interventions (MBIs) constitute a promising option to alleviate psychological symptoms in students with psychiatric disorders.
Objective: This study evaluated the impact of a MBI on psychological symptoms of elementary school students with psychiatric disorders in a special education curriculum.
Method: A series of n-of-1 trials with an experimental A-B-A design and 10 assessment time-points was used. Participants were two special education classrooms of elementary school students (Group A, n = 7; Group B, n = 6; ntotal = 13) and their teachers.
Results: Analyses showed that, at follow-up, students from Group A reported significant decreases in inattention and a trend (p = 0.051) was observed in anxiety symptoms, whereas their teacher reported only deteriorating anxiety scores. No significant results were found in students from Group B.
Conclusion: Results from this study show substantial variation between students, tested cohorts and raters of internalizing and externalizing symptoms and behaviors. Therefore, the conservative conclusion from such variation can only be that more research is needed, as no firm conclusion as to the utility of MBIs for such groups of children with special education needs can be established.
In Canada, 20% of students suffer from a mental health problem, causing significant educational and psychosocial adaptation difficulties (Canadian Teachers' Federation., 2012). These problems jeopardize academic achievement and lead to impaired functioning in school-based settings (Oberle et al., 2014). Students with psychiatric disorders show important deficits on several levels: cognitive (e.g., more or less severe and frequent loss of contact with reality, incoherent speech, academic delays), emotional (e.g., anxiety, irritability, and/or depression symptoms, aggressiveness), behavioral (e.g., bizarre or incoherent behavior, limited interests, opposition, and disorganized behavior) and social skills (e.g., withdrawal, rejection from peers). They also present significant levels of internalized and externalized symptoms (Lavoie et al., 2017). These difficulties can be linked to significant deficits in emotional regulation skills. Special education classrooms for students with severe psychiatric disorders typically regroup youth showing a vast array and heterogeneity in symptoms and diagnoses, namely because of administrative constraints and paucity of space and resources. Thus, these children are very often regrouped within the same classrooms. Faced with such an important proportion of psychological problems, it appears crucial to develop empirical and skill-based interventions adapted to the reality of these very heterogeneous classrooms. Mindfulness-based interventions (MBIs) are increasingly implemented in school-based settings to foster better emotional regulation skills and higher resilience to stress in students with special education needs such as severe learning disabilities and psychological disorder diagnoses (Malboeuf-Hurtubise et al., 2017c). This article presents a first, small-scale attempt to conduct research on a MBI with two small classes of special needs boys. Specifically, the goal of this n-of-1 trial design was to evaluate the impact of a MBI on internalized and externalized symptoms in two groups of elementary school students with psychiatric disorders in a special education curriculum.
Mindfulness can be defined as “…the process by which we pay attention in a particular way, on purpose, in the present moment, and non-judgmentally” (Kabat-Zinn, 1994). Mindfulness research in youth is still considered to be in its early phase, although there has been a significant amount of articles published in recent years documenting the impact of MBIs for children and adolescents (Taylor and Malboeuf-Hurtubise, 2016). Evidence from a recent meta-analysis suggests that MBIs hold promise in reducing internalized symptoms (d = 0.37) such as anxiety, depression, and inattention, while promoting better emotional and stress regulation skills in youth both in regular classrooms and with an identified psychological disorder (Zenner et al., 2014; Zoogman et al., 2014). For the purposes of this article, we present results from research evaluating the impact of MBIs that were adapted, developed and inspired from the Mindfulness-Based Stress Reduction (Kabat-Zinn, 2003) and/or Mindfulness-Based Cognitive Therapy (Segal et al., 2018) interventions, in which the major component of all cited interventions constitutes the practice of mindfulness meditation itself.
In school settings, the impact of MBIs has been studied with students in regular classrooms and students in a special education curriculum. In regular classrooms, from a universal prevention perspective, mindfulness has been shown to decrease inattention symptoms and overall internalized problems in elementary school students with no known psychological difficulties, when compared to students in an active emotion awareness intervention control group (Crescentini et al., 2016). Decreases in anxiety have also been reported in elementary school children from regular classrooms, in comparison to wait-list controls (Tarrasch et al., 2017). In a recent study, Sibinga et al. (2016) have reported similar decreases in depressive symptoms, rumination and negative affect in elementary school students from regular classrooms in underprivileged neighborhoods, when compared to an active health education control group, indicating that MBIs can be useful in alleviating the negative impact of stress in these students. Finally, using a similar study design, Schonert-Reichl et al. (2015) have reported that mindfulness had a positive impact on elementary school students' social and emotional regulation skills, while decreasing depressive and aggressiveness symptoms. Overall, the available evidence tends to indicate that MBIs are useful in promoting better mental health and coping strategies in school settings for children in regular classrooms with no identified psychological diagnoses, namely by acting preventively on stress and on the emotional burden that children experience daily.
In recent years, researchers have started to investigate and evaluate the impact of transdiagnostic treatments to alleviate symptoms of psychological disorders in youth and adults (Boswell et al., 2014). This line of research aims to evaluate and develop unified evidence-based treatment options that can be applied across different psychological conditions and diagnoses. As such, MBIs have been identified as potentially good transdiagnostic options for treating various psychological disorders in children (Malboeuf-Hurtubise et al., 2017b). However, to date, this research remains preliminary and results are still inconclusive.
Students with identified disabilities in special education curriculum classrooms rarely present homogeneous conditions and diagnoses, and, thus, would greatly benefit from the development of such transdiagnostic MBI treatments. However, the amount of research published on the impact of MBIs for elementary school students with special education needs (e.g., students in a special education curriculum or students with an identified mental health disorder) is far less voluminous. The available evidence shows contradictory results regarding the benefits of mindfulness practice in this population. For example, a recent article presenting results from a quasi-experimental, one group pre-test post-test design for elementary school students with severe learning disabilities showed that MBIs could be useful in decreasing anxiety, depression, inattention, and aggressiveness in these students, thereby alleviating the psychological distress and overall mental health burden associated with severe learning disabilities (Malboeuf-Hurtubise, Lacourse, et al., 2017). On the other hand, inconclusive results were found in three elementary school students suffering from major depressive and anxiety disorders, as two participants reported improvements on anxiety and depression, while their teachers reported deteriorating scores on these variables (Malboeuf-Hurtubise et al., 2017b). These preliminary, contradictory results suggested that caution should be exercised when considering the overall applicability of MBIs as a universal treatment option for children with special education needs in elementary schools. Furthermore, the small number of current studies highlights the need to document the impact of MBIs in greater detail for students who have underlying mental health issues, to determine in which contexts and with what populations (e.g., as a transdiagnostic clinical intervention for children with a variety of mental health disorders or a clinical intervention for children with a specific mental health disorder, such as an anxiety disorder, ADHD or major depressive disorder) this practice can be of use to decrease internalized and externalized symptoms.
Elementary school students struggling with severe mental health problems are particularly vulnerable to physical and psychological stress, along with psychological distress (Mental Health Commission of Canada, 2013). Given the high cost of these psychological difficulties on a personal, social and school level, it is paramount to pay attention to these issues, in order to foster better mental health and to avoid future psychosocial adaptation problems in these students (Smetanin et al., 2015). However, there is a paucity of available MBI research on this issue. Only two studies were found pertaining to the impact of a MBI for adolescents with psychiatric disorders in a psychiatric setting. Results from these studies indicated that the intervention had an overall positive impact on mood (decreasing, namely, anxiety and depression), self-regulation, self-esteem, and social skills in adolescents with severe mood and anxiety disorders, oppositional-defiant and conduct disorders, attention deficit and hyperactivity disorders and reactive attachment disorders (Biegel et al., 2009; Van Vliet et al., 2017). To our knowledge, no published quantitative study has ever evaluated the impact of a MBI for children with similar psychiatric disorders in a school-based setting.
N-of-1 trials are used to evaluate within-subject differences over time. Research projects using N-of-1 trials can be comprised of one person (i.e., case study) or multiple individuals (Wood and Brown, 1994; Molenaar and Campbell, 2009). This design has been suggested to be especially relevant and informative in intervention development and research, such as MBI research for youth in school-based settings. Through the use of repeated measures, N-of-1 trials provide large amounts of data that allow for a detailed study of change in targeted variables, longitudinally (Schork, 2015). Although the main concern with n-of-1 trials is not generalizability, with large enough sample sizes, results from multiple n-of-1 trials can be aggregated to provide an estimated global effect of a given treatment option for a specific population, such as students in a special education curriculum (Schork, 2015).
N-of-1 trials are considered to be a sound, experimental design alternative to studies incorporating larger sample sizes, allowing for a more detailed measure of the amplitude of change through means of regularly scheduled repeated assessment (Vohra et al., 2016). Furthermore, n-of-1 trials are considered to be especially appropriate when small pools of participants are available—e.g., in program evaluation studies targeting a specific population such as students with special education needs—and when a control group is not available (Spector, 1981; Harris et al., 2006; Gravetter and Forzano, 2011; Vohra et al., 2016). N-of-1 trials are considered to be a rigorous approach that allows an evaluation of the impact of interventions such as MBIs, while narrowing the gap between educational or psychological research and practice (Vohra et al., 2016). As an example, n-of-1 trials can be especially useful to evaluate the impact of alternative and complementary therapies such as MBIs for youth.
This article presents a first, small-scale attempt to conduct research on a MBI with two small classes of special needs boys. The goal of the present study was to evaluate the impact of a MBI on internalized (anxiety, depression, and inattention) and externalized (hyperactivity and aggressiveness) symptoms in elementary school students with psychiatric disorders in a special education curriculum. In order to do so, we implemented a n-of-1 trial design in which 10 assessment time-points were included (three pre-intervention, four during the intervention, three follow-ups), and documented the progression of symptoms in our participants over a 3-months during the follow-up period. Student and teacher-reported data was collected in this project.
Given the prevalence of both internalized and externalized symptoms in these students, we hypothesized that the MBI would have a significant and positive impact on all symptoms studied (i.e., anxiety, depression, inattention, hyperactivity, and aggressiveness), while increasing mindfulness skills in participants. Specifically, we hypothesized that:
1) We would observe clinically and statistically significant decreases in anxiety, depression, inattention, hyperactivity, and aggressiveness scores pre-to-post intervention;
2) These decreases would be maintained at follow-up.
3) Mindfulness scores would increase pre-to-post intervention;
4) This increase would be maintained at follow-up.
An experimental A-B-A n-of-1 trials series design with 10 assessment time-points and a 3-months follow-up was used in this project. This project was conducted in collaboration with a school board and elementary school from Chicoutimi, Canada. Ethics approval was obtained from all institutions involved. Informed consent was obtained from all individual participants, their parents, and the teachers taking part in this study.
Elementary school students with psychiatric disorders from two special education classrooms took part in this study, along with their teachers. Two different classrooms of elementary school students (Group A and Group B) took part in this study (ntotal = 13). Students received the intervention separately and at a different moments in time, and were consequently considered as two distinct cohorts. All students in both classrooms were boys. To be in a special education classroom for students with psychiatric disorders, all students had been previously assessed, and were still closely monitored, either by a child psychiatrist or a by child psychiatry unit at the regional hospital. They had all received a diagnosis of a severe form of psychological disorder (e.g., major depressive disorder, anxiety disorder, attention-deficit, and hyperactivity disorder, conduct disorder). The severity of their disorder prevented them from being schooled in a regular classroom. Specifically, 69% of them had a diagnosis of Attention Deficit and Hyperactivity Disorder (ADHD), 31% had a diagnosis of Tourette's disorder and 8% had a diagnosis of major depressive disorder. A significant proportion (92%) of students met the diagnostic criteria for more than one mental health disorder. In addition to their pervasive psychological disorders, a large majority of these students (69%) were in foster care at the time of this study, and had an additional diagnosis of reactive attachment disorder or disinhibited social engagement disorder (American Psychiatric Association, 2013). As such, these students were receiving additional psychological support in their respective classroom, namely through regular visits from the school psychologist. As part of the educational model of these two classrooms—called Kangaroo or nurture classrooms—students were not taught to or treated according to their age, but according to their level of emotional development (Bennathan and Boxall, 2013; Lavoie et al., 2017). For the purposes of this study, participants had to be willing to participate in an 8-week MBI and be available to answer questionnaires during all phases of the study. It was also necessary that their teachers were available to fill out questionnaires at the same time as their students for all assessment time-points. As this project was conducted in French, participants were required to speak and understand the language. No attrition was experienced in this study; all students and their respective teachers filled out pre- and post-intervention questionnaires. Participant characteristics can be found in Table 1.
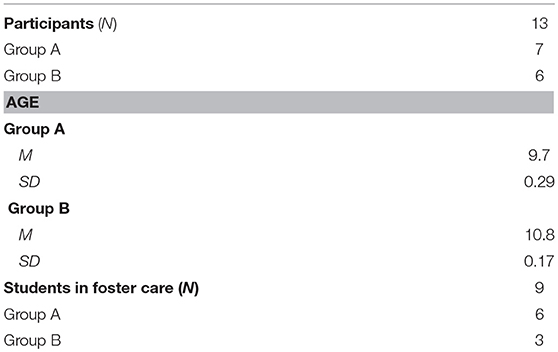
Table 1. Participant demographics.
An 8-weeks MBI, specifically adapted for elementary school children, and empirically validated with students having special education needs, was used in this project (Malboeuf-Hurtubise et al., 2017a,c). The group met once a week. This intervention, called Mission Meditation, was designed to be implemented specifically in school-based settings, namely by ensuring that each session fit into a daily classroom period (~45–60 min) and that mindfulness practices were developmentally appropriate to match elementary school students' shorter attention span (Malboeuf-Hurtubise and Lacourse, 2016). MBI sessions were led by a school psychologist with extensive knowledge and an ongoing personal practice of mindfulness meditation of many years. She also had extensive experience and skills in providing therapy in group-based settings. This psychologist was specifically trained to facilitate the Mission Meditation workshops and received individual supervision from the main researcher on this project throughout the course of the intervention. Weekly sessions included introduction to formal and informal mindfulness practices (e.g., mindful eating, mindfulness through the senses, body scan, sitting, and breathing meditations), with a specific emphasis on awareness of thoughts, emotions and physical sensations. On average, students spent 30–40 min on various mindfulness practices, and 15–20 min were allocated to psychoeducational components. Homework was assigned every week and in-class practice, led by the teacher, was required at least once a week. Teachers were trained in order to guide in-between session meditation practices, and individual supervision was offered both by the school psychologist and members of the research team, upon request. In-class practice was carefully tracked through a weekly log filled out by the teachers. As requested, homework was completed every week during class time and a minimum of one in-class practice took place between sessions. The intervention did not include a silent retreat. Although Mission Meditation was not originally intended for students with psychiatric disorders, previous work from the first author has evaluated its impact in elementary school students with special education needs, such as severe learning disabilities and various mental health disorders (e.g., major depressive disorder, ADHD, and anxiety disorders), and, in our experience, this technique appears to have been useful in alleviating internalized symptoms in these populations. Thus, the content of the intervention was not adapted specifically for this population. In terms of safety precautions, given the school psychologist was familiar with all students taking part in this project, she was able to ensure that all of them felt at ease while completing meditation exercises. She also reminded students on multiple occasions of their right to opt out of practice without having to provide a reason to do so. The aim of this intervention was to provide an in-school treatment option youth with severe psychiatric disorders in a special education curriculum, in order to alleviate symptoms and to foster better functioning in school and at home. The MBI was not intended to replace any treatment and guidance that was given by the hospital, doctors and psychiatrists in tertiary prevention. For a detailed description of the intervention, please refer to Table 2. The full intervention content has also been published as a book by the first and last authors of this paper (Malboeuf-Hurtubise and Lacourse, 2016).
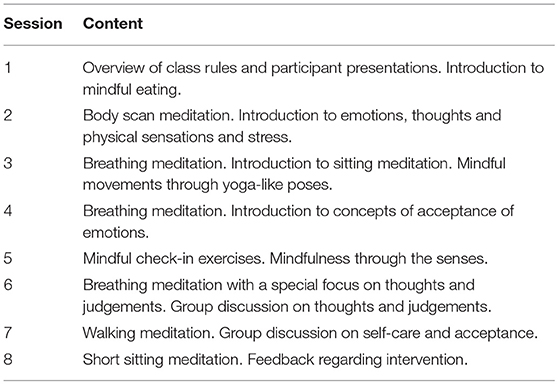
Table 2. Mindfulness-based intervention session content.
For the purposes of this study, a validated French version of each scale was selected. Given the amount of assessment time-points included in this project, specific items of the following scales were selected, to ensure that both students and teachers could fill out the questionnaires in a reasonable amount of time (~5–10 min). A total of 21 items were administered to students and 20 items were administered to teachers.
This measure was used to evaluate internalized and externalized symptoms in students. Items from the Teacher Report Form and the Self-Report Form were used for this project. This measure presents good inter-rater agreement (r = 0.53–0.74) and test-retest reliability (r = 0.7–0.8), along with high internal consistency (α = 0.8–0.9) and clinical validity (Reynolds and Kamphaus, 2004). The following subscales were used: anxiety (self-report; 3 items, e.g., “I worry about little things” and teacher report; 3 items, e.g., “Worries about things that cannot be changed”), depression (self-report; 5 items, e.g., “Nothing ever goes right for me” and teacher report; 5 items, e.g., “Seems lonely”), inattention (self-report; 4 items, e.g., “ I forget to do things” and teacher report; 3 items, e.g., “Has a short attention span”), hyperactivity (self-report; 3 items, e.g., “I have trouble standing still in lines” and teacher report; 4 items, e.g., “Is overly active”) and aggressiveness (teacher report; 5 items, e.g., “Defies teacher”). All subscales presented good to excellent internal consistency in this sample, except for the aggressiveness subscale: anxiety (self-report: α = 0.90; teacher-report: α = 0.90), depression (self-report: α = 0.94; teacher-report: α = 0.78), inattention (self-report: α = 0.93; teacher-report: α = 0.79), hyperactivity (self-report: α = 0.97; teacher-report: α = 0.84) and aggressiveness (teacher-report: α = 0.47).
This measure was used to evaluate mindfulness in students (Baer et al., 2008). It assesses the extent to which students become more mindful as they are exposed to the intervention. The measure presented excellent internal consistency in this sample (α = 0.96). A total of six items from this scale were used in this project, taken from the following subscales: Observe (e.g., “When I take a shower or bath, I stay alert to the sensations of water on my body”), Act with Awareness (e.g., “I do jobs or tasks automatically without being aware of what I am doing”) and Non-react (e.g., “I perceive my feelings and emotions without having to react to them”). Items were selected based on their relevance with regards to mindfulness concepts that were taught in this MBI.
Both students and teachers completed a total of 10 assessment time-points in this study. Teachers completed one questionnaire per student at each assessment time-point. No financial incentive was given to the teachers, although an agreement with the school board allowed them to fill out the questionnaires during working hours. Three baseline assessments were completed during phase A (one assessment per week), four assessments were completed during the active treatment phase B (one assessment every 2 weeks in order to allow participants to acquire and practice new skills) and three assessments were taken during the 3-months follow-up phase A (one assessment per month). All questionnaires were completed by students during class time, at the beginning of the MBI sessions.
Methods of assessment in n-of-1 trials have been the subject of ongoing debates in the past years, specifically with regards to the appropriateness and accuracy of suggested methods of analysis (Smith, 2012). Experts in quantitative research and statistical methods have recently suggested that statistical analyses be used in analyzing results of n-of-1 trials (Kratochwill et al., 2012; Shadish, 2014). Multilevel modeling strategies, when used in n-of-1 trials research, have been put forward as a method that can inform researchers with regards to the presence of treatment effects. Namely, these allow to test for differences in intercept and slopes of scores (i.e., symptoms) from the pre-intervention to the active intervention and post-intervention phases (Shadish et al., 2008; Van den Noortgate and Onghena, 2008; Smith et al., 2015). Furthermore, multilevel modeling is a valid approach with small sample sizes (e.g., N = 4–8) (Ferron et al., 2009; Shadish et al., 2013).
In this study, primary hypotheses were tested using a multiple, single case multilevel modeling strategy to compare and evaluate statistical significance in fluctuations of scores between A-B-A phases. These analyses are based on a modeling strategy suggested by Moeyaert and colleagues (Moeyaert et al., 2014). The parameter b0 is interpreted as the baseline intercept, b1 as the treatment-baseline difference in intercepts and b2 as the follow-up-baseline difference in intercepts (Moeyaert et al., 2014; Maric et al., 2015). Autocorrelation was considered through AR1. Fixed effect coefficients and their p-values are presented in Tables 2, 3. P-values were considered according to the p = 0.05 threshold. Visual analysis of the mean change in participants from both groups separately was also completed. As students received the intervention separately and at different moments in time, they were considered as two distinct cohorts in our statistical analyses. Group-based analyses allowed to control for cohort effects. Statistical analyses were conducted using SPSS 24 software.
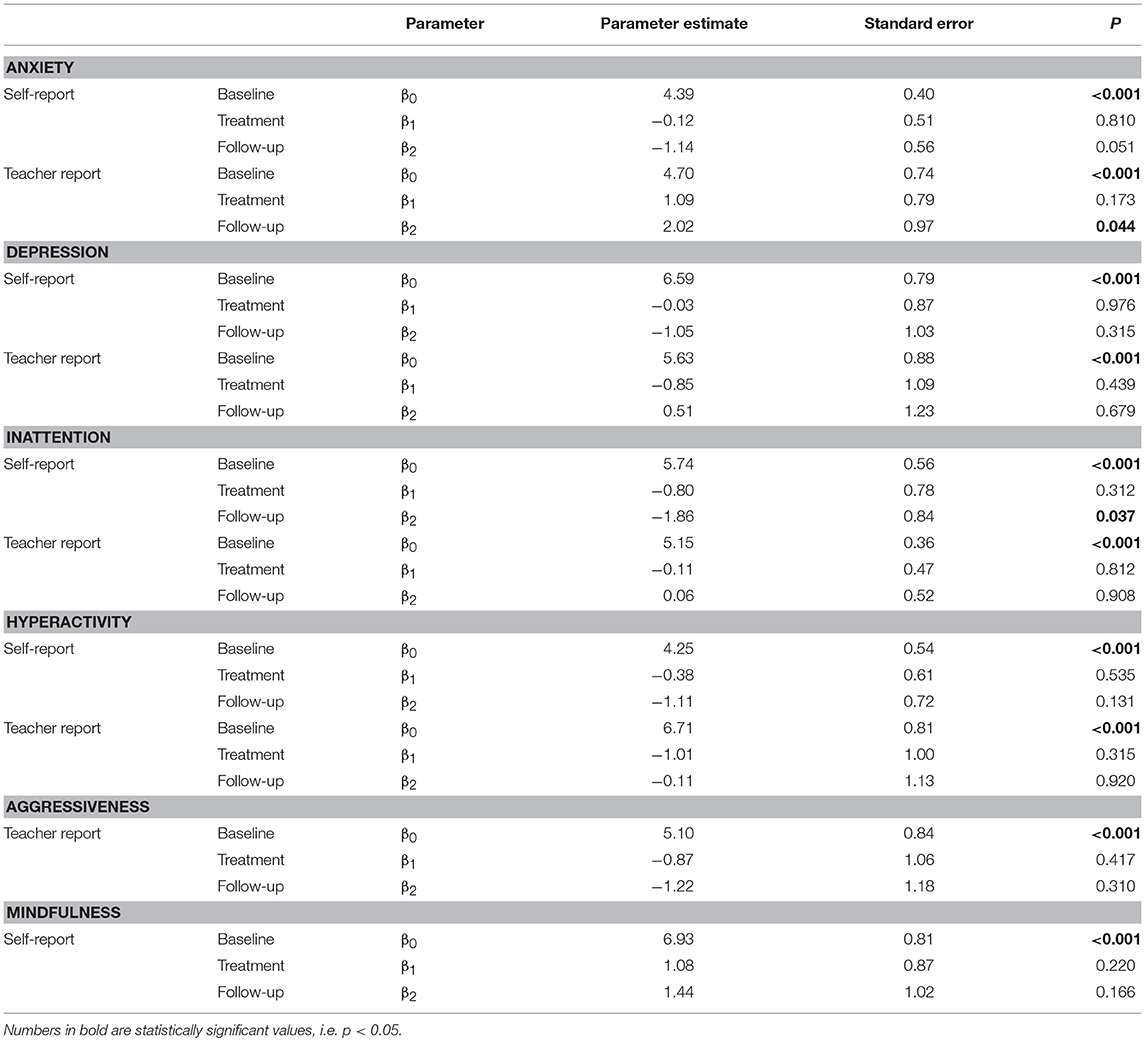
Table 3. Results of empirical estimations of the case-specific effects using the basic three levels model for all variables for Group A students.
Statistical analyses show a trend in phase differences between the treatment and follow-up phases for anxiety scores [β2 = −1.14, t(4.16) = −2.04, p = 0.051] of Group A students, indicating lower anxiety scores at the end of the follow-up period, when compared to the active treatment phase (see Table 3). Visual analysis of the group mean data shows moderately high levels of anxiety symptoms in the baseline and active treatment phases, followed by a steady decrease in scores during the follow-up period (see Figure 1). Specifically, out of the seven students comprising the Group A, two have overall stable scores, whereas two have decreasing anxiety scores, two have increasing scores and one shows no clear pattern in the data.
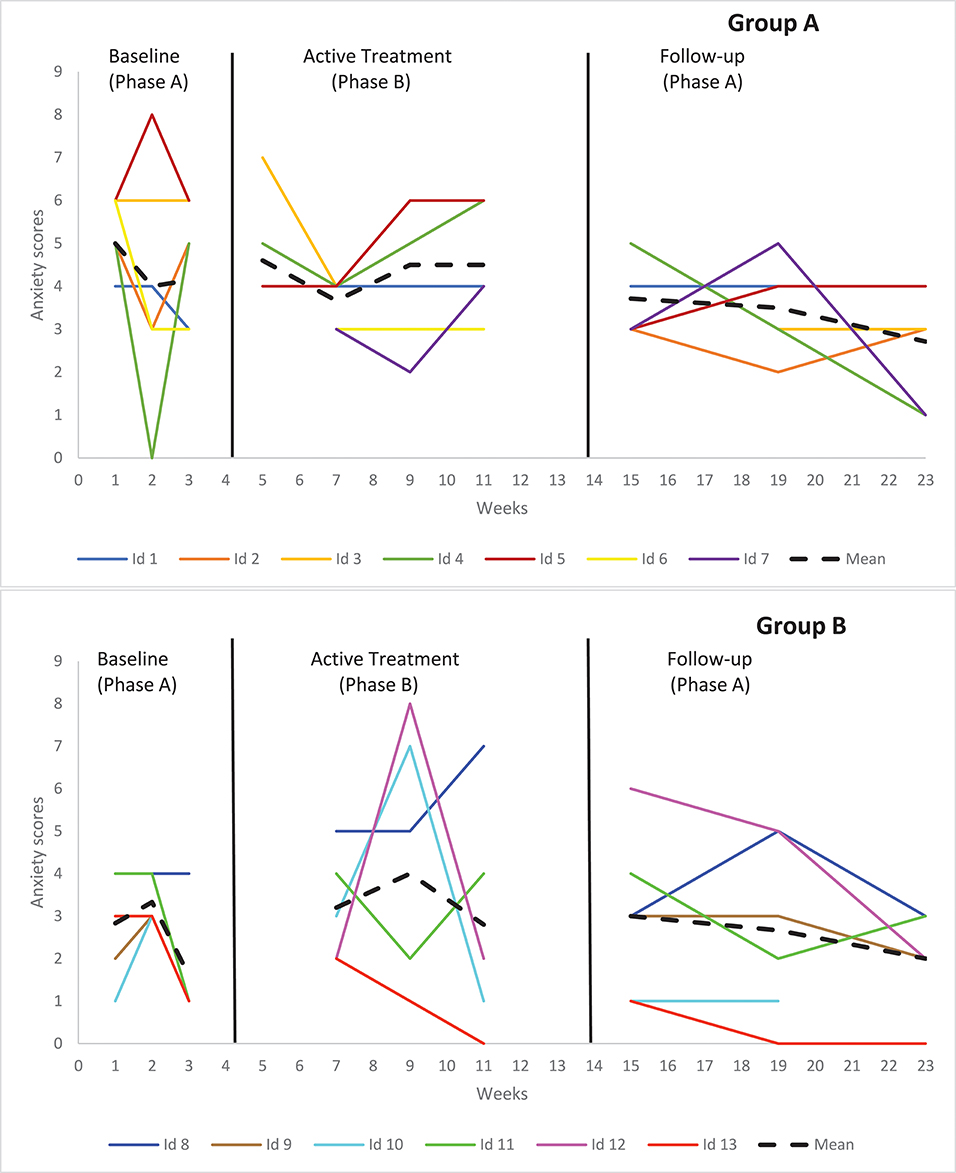
Figure 1. Graphical display of baseline level and changes in level between consecutive phases in anxiety for self-reported data.
Results further show significant phase differences between the treatment and follow-up phases for inattention scores [β2 = −0.19, t(4.88) = −2.21, p = 0.037] of Group A students, indicating lower inattention scores at the end of the follow-up period, when compared to the active treatment phase (see Table 4). Visual analysis of the group mean inattention data shows somewhat unstable scores during the baseline phase, followed by a subtle increase in scores during the active treatment phase. At follow-up, inattention scores decrease sharply (at the beginning of the phase) and steadily throughout the period (see Figure 2). Specifically, out of the seven students comprising the Group A, three have overall stable scores and three have decreasing scores, after showing an initial increase in inattention at the beginning of the active treatment phase.
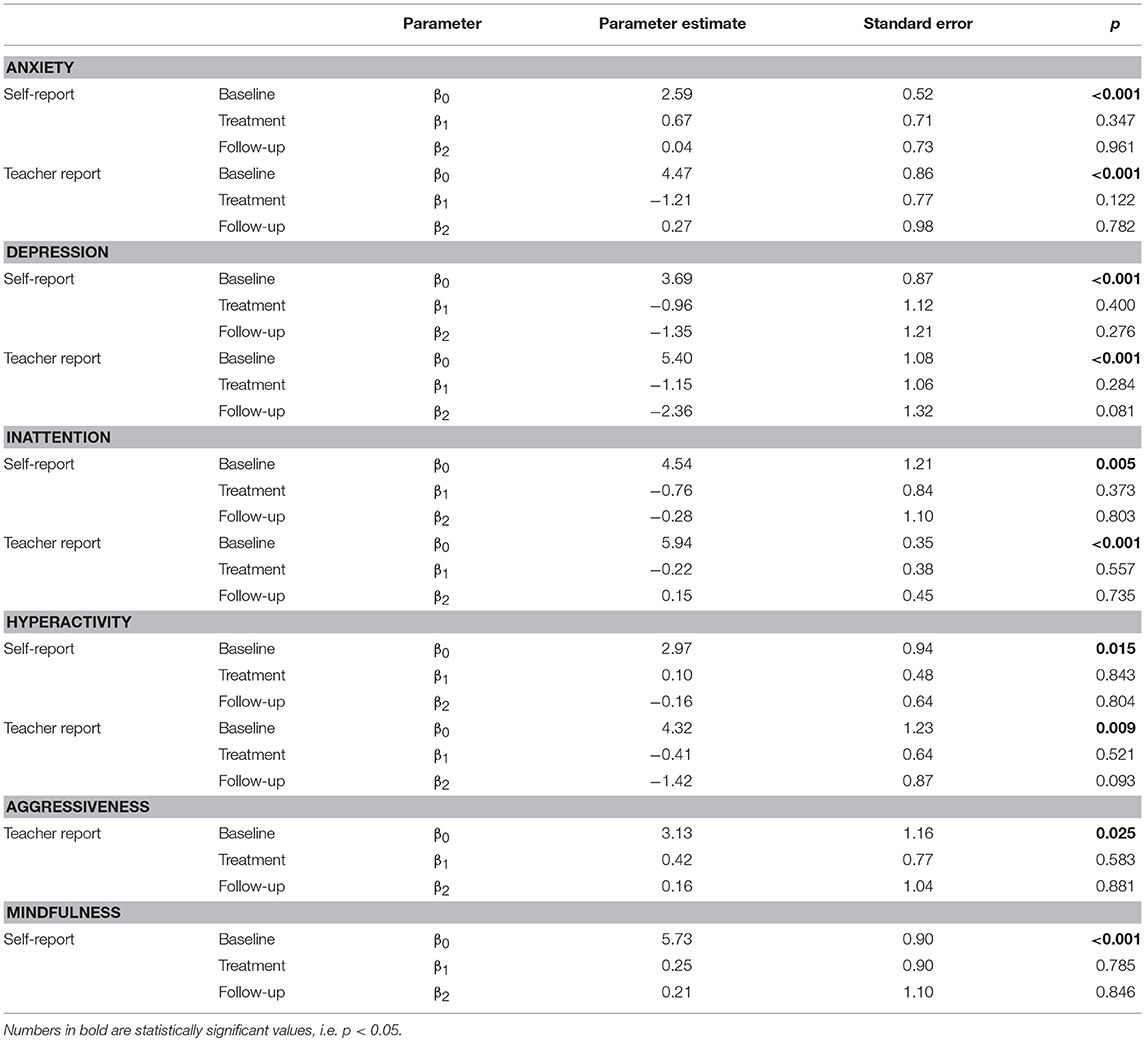
Table 4. Results of empirical estimations of the case-specific effects using the basic three level model for all variables for Group B students.
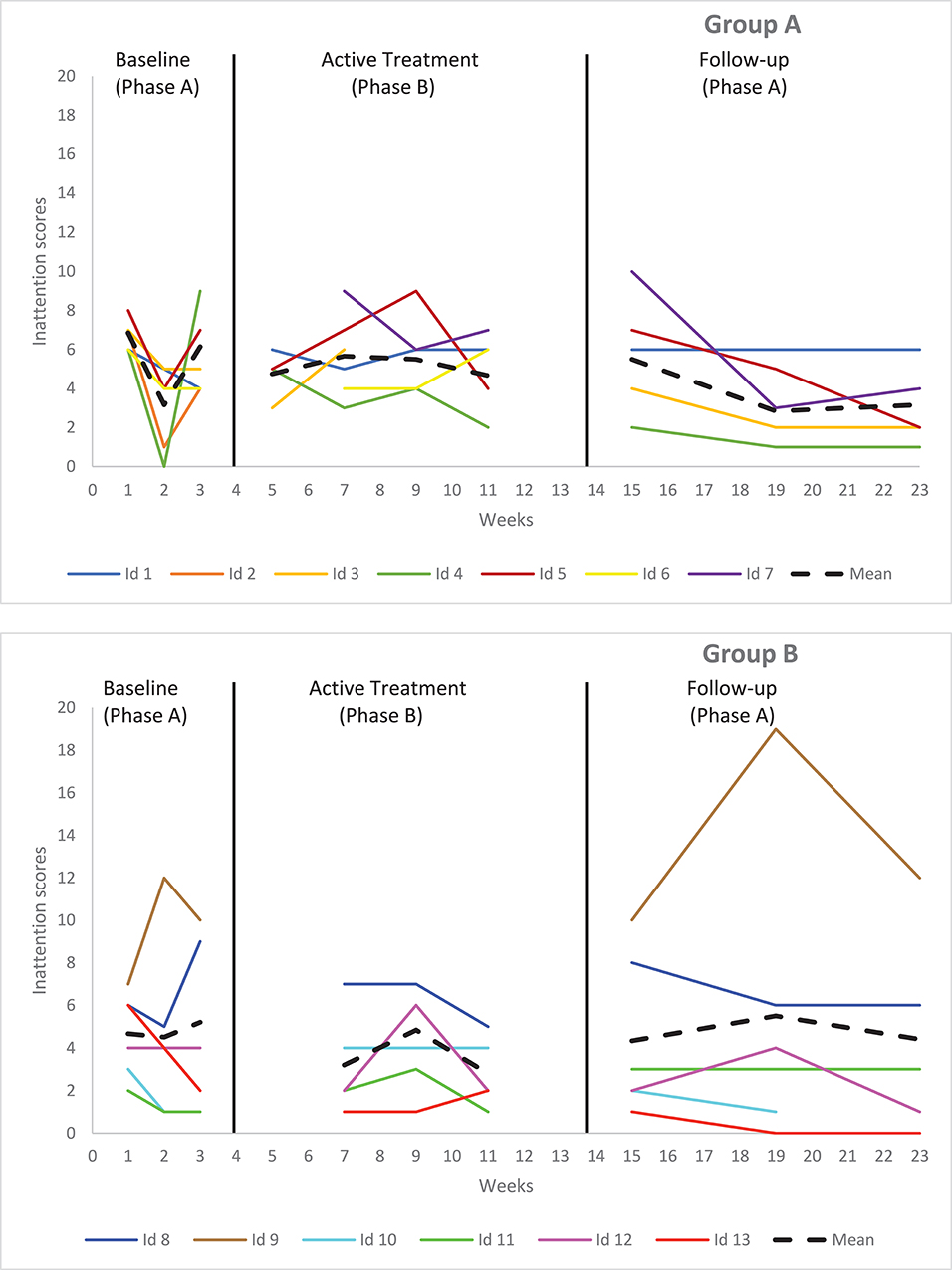
Figure 2. Graphical display of baseline level and changes in level between consecutive phases in inattention for self-reported data.
The results of the weekly assessments showed no significant phase differences in scores or rates of change between the baseline, the active treatment and the follow-up phases for depression and hyperactivity symptoms of Group A students (see Table 3 and Figures 3, 4). Visual analysis of depression scores shows that, out of the seven students comprising Group A, two had overall stable scores, two had constant decreasing scores, one had increasing scores, and two showed no clear pattern in their data. Visual analysis of hyperactivity scores shows that, for the same age group, all students had overall stable scores throughout the baseline, intervention and follow-up periods.
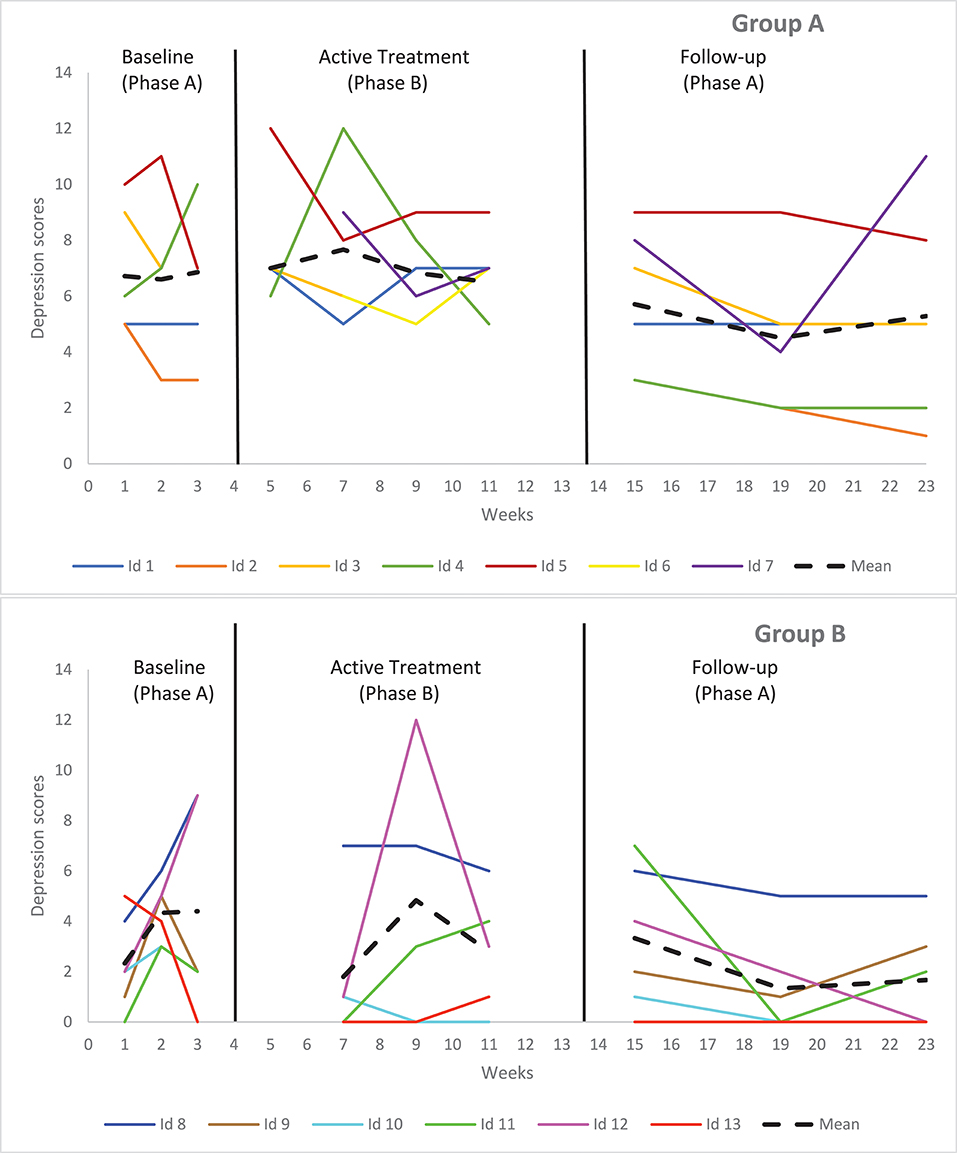
Figure 3. Graphical display of baseline level and changes in level between consecutive phases in depression for self-reported data.
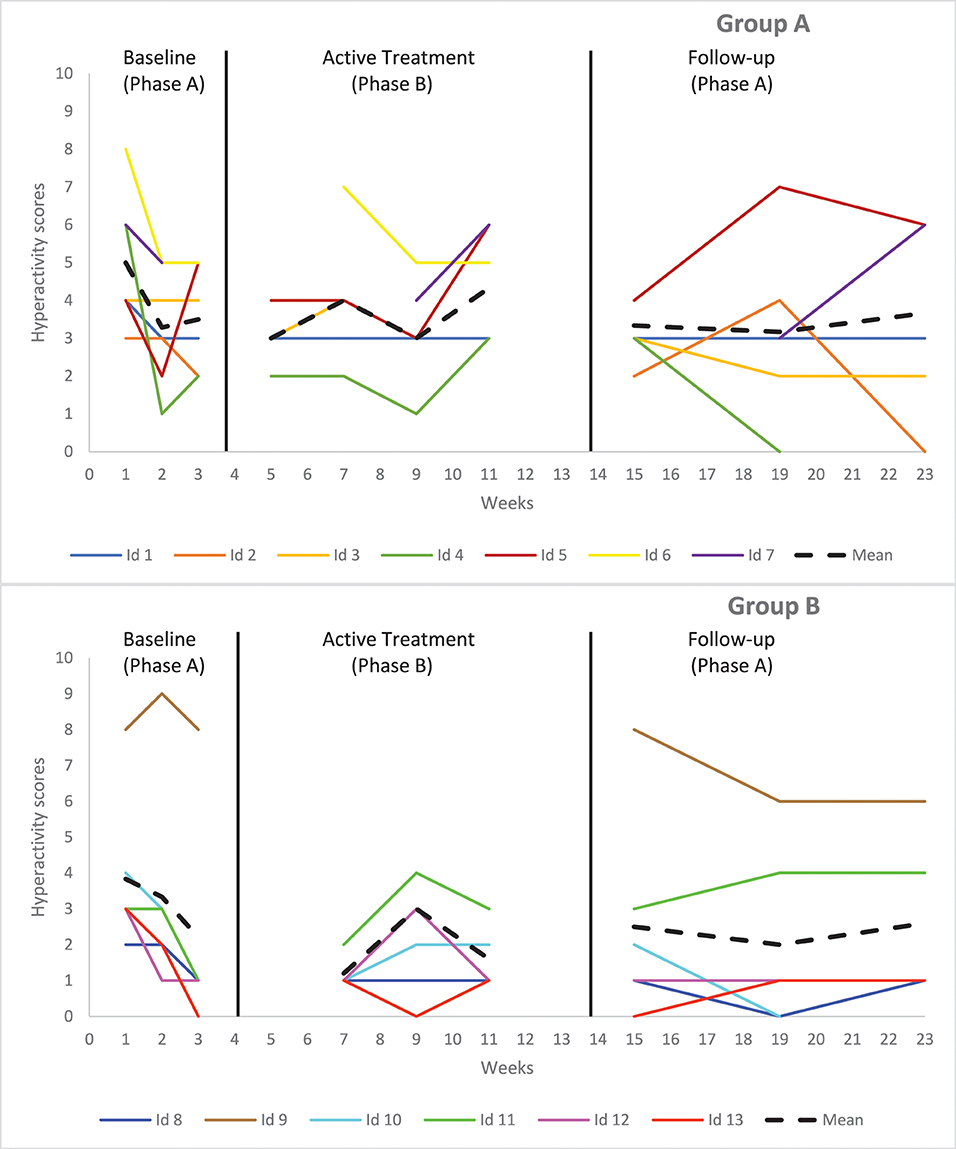
Figure 4. Graphical display of baseline level and changes in level between consecutive phases in hyperactivity for self-reported data.
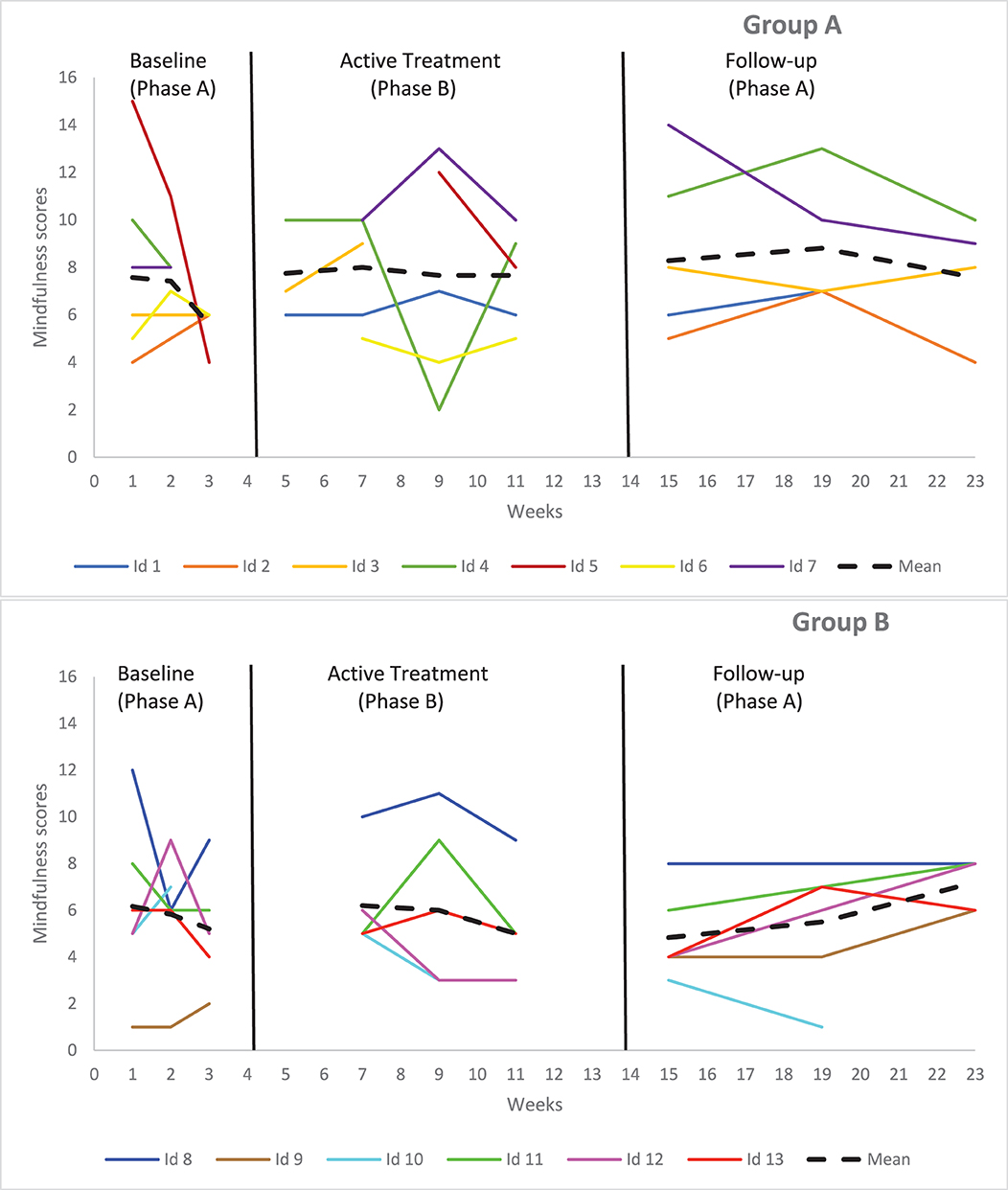
Figure 5. Graphical display of baseline level and changes in level between consecutive phases in mindfulness for self-reported data.
The results of the weekly assessments showed no significant phase differences in scores or rates of change between the baseline, the active treatment and the follow-up phases for anxiety, depression, inattention, and hyperactivity symptoms of Group B students (see Table 4 and Figures 1–4). Visual analysis of anxiety scores shows that, out of the six students comprising this group, two have overall stable scores, three have increasing anxiety scores, and one has decreasing scores. Visual analysis of inattention scores shows that two students have initial increase in scores, followed by a subsequent and constant decrease, two have noticeable increases in scores during the follow-up period, and two have overall stable scores. Visual analysis of depression scores shows that three students have overall low and stable scores, one has an initial increase in scores that subsequently stabilizes and two do not show any clear pattern in their data. Finally, visual analysis of hyperactivity scores shows that all students have overall low and stable scores, except for one student who has stable and high scores.
Statistical analyses show significant phase differences in scores between the treatment and follow-up phases for anxiety scores [β2 = 2.02, t(4.31) = 2.07, p = 0.044] from teacher-reported data of Group A students, indicating higher anxiety scores at the end of the follow-up period, when compared to the active treatment phase (see Table 4). Visual analysis of the group mean data shows declining scores in anxiety during the baseline phase, followed by a sharp increase in scores at the beginning of the active treatment phase. Scores then decrease up until the 7th week of the project, to finally re-increase steadily throughout the active treatment phase and the follow-up period (see Figure 6). Specifically, out of the seven students comprising Group A, four have an initial decrease in anxiety, followed by a constant increase in their scores, two have overall stable scores, and one does not show a clear pattern in the data.
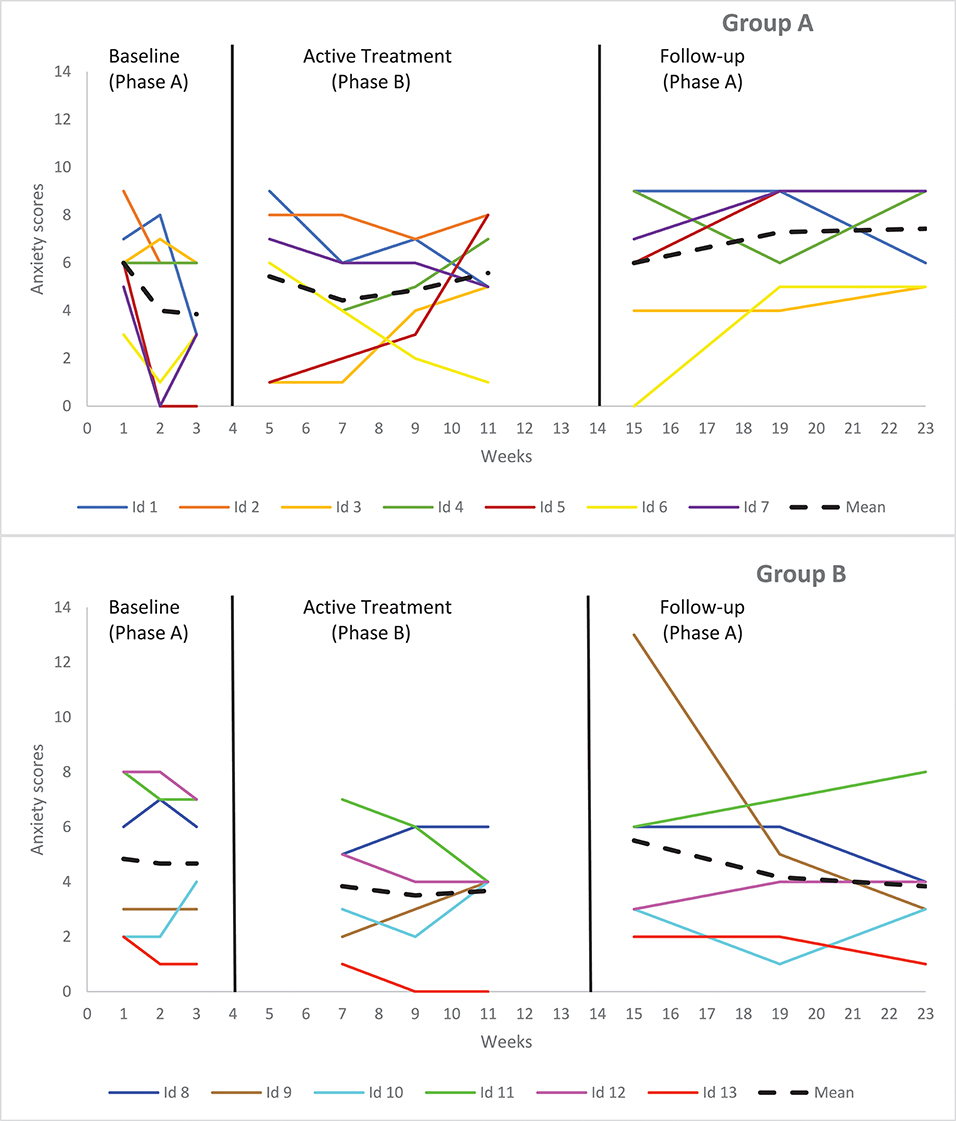
Figure 6. Graphical display of baseline level and changes in level between consecutive phases in anxiety for teacher-reported data.
Visual analysis of all teacher-reported group mean data for Group A indicates similar patterns of initial decreases in scores, followed by a steady increase throughout the active treatment phase and follow-up periods, starting at week 7 (see Figures 7–10). Specifically, visual analysis of inattention scores show that, out of the seven students comprising Group A, four have overall stable scores, whereas three have initial increases in scores, followed by a small decrease. Visual analysis of depression scores shows that all students have initial decreases in their depression scores. However, out of the seven students, five of them have a significant peak increase in scores at the beginning of the active treatment phase, followed by a subsequent and constant decrease in scores. Visual analysis of hyperactivity scores for the same group shows that two have initial decreases in scores, followed by an increase, whereas three students have a strong overall decrease in hyperactivity scores, and two do not show a clear pattern in their data. Finally, visual analysis of aggressiveness scores shows that four students have overall decreasing scores, whereas three do not show a clear pattern in their data.
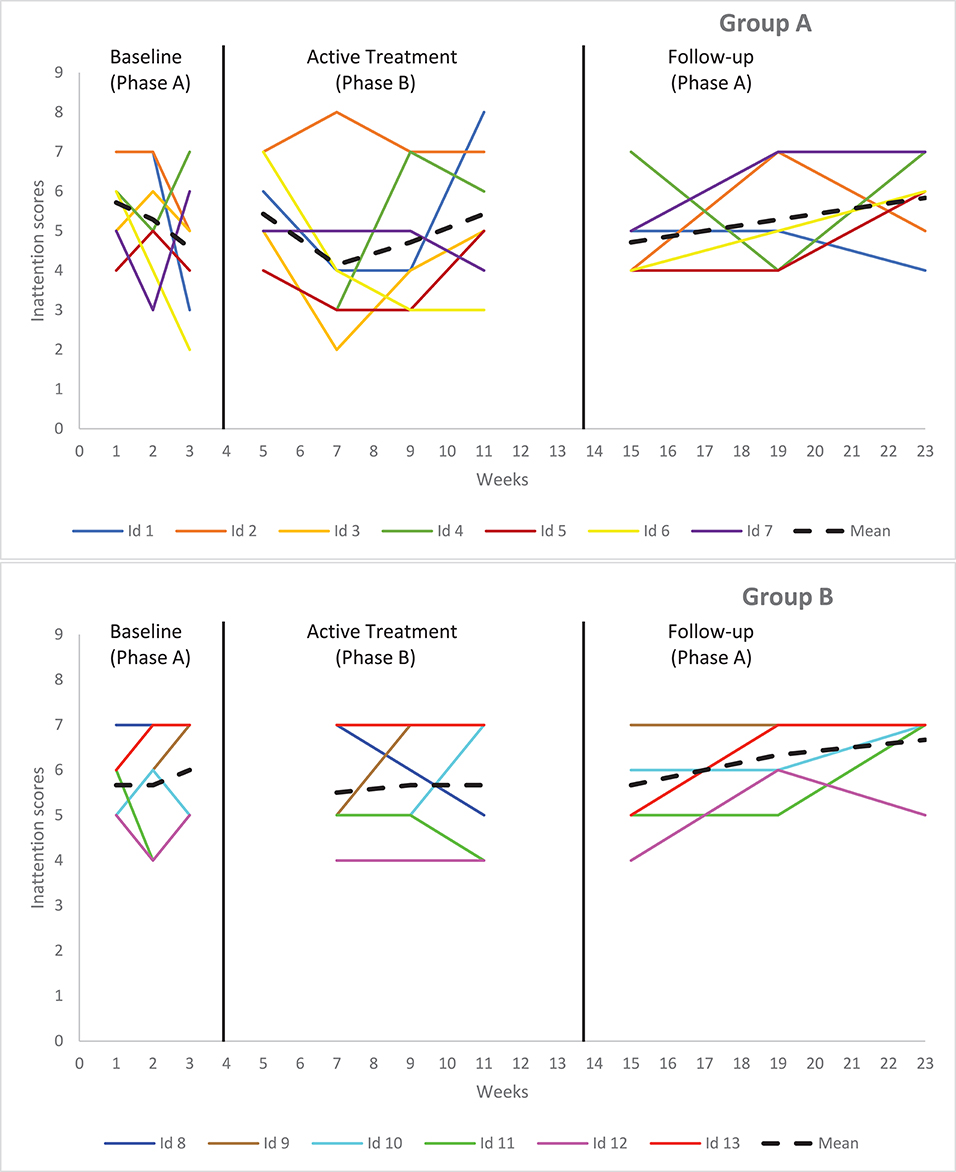
Figure 7. Graphical display of baseline level and changes in level between consecutive phases in inattention for teacher-reported data.

Figure 8. Graphical display of baseline level and changes in level between consecutive phases in depression for teacher-reported data.
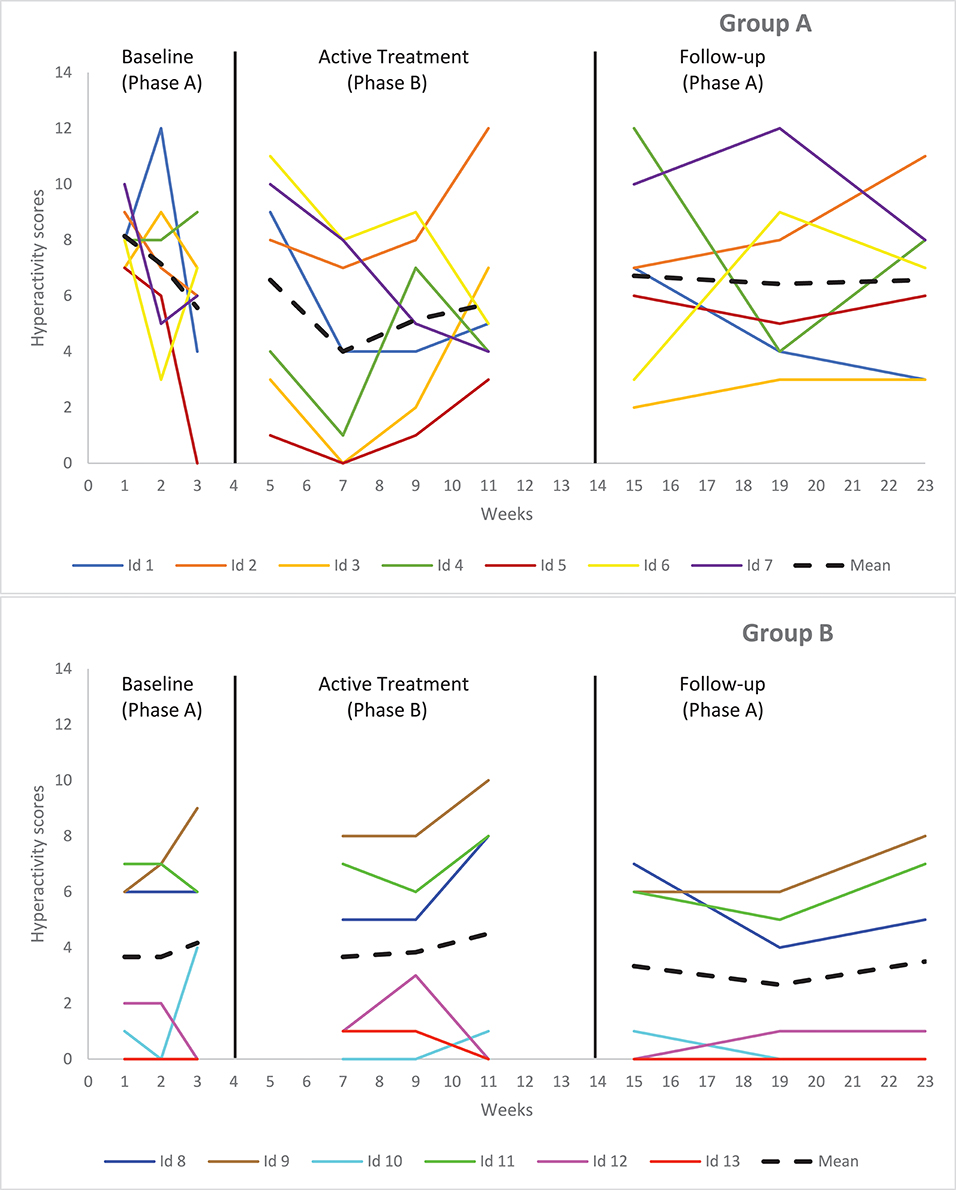
Figure 9. Graphical display of baseline level and changes in level between consecutive phases in hyperactivity for teacher-reported data.
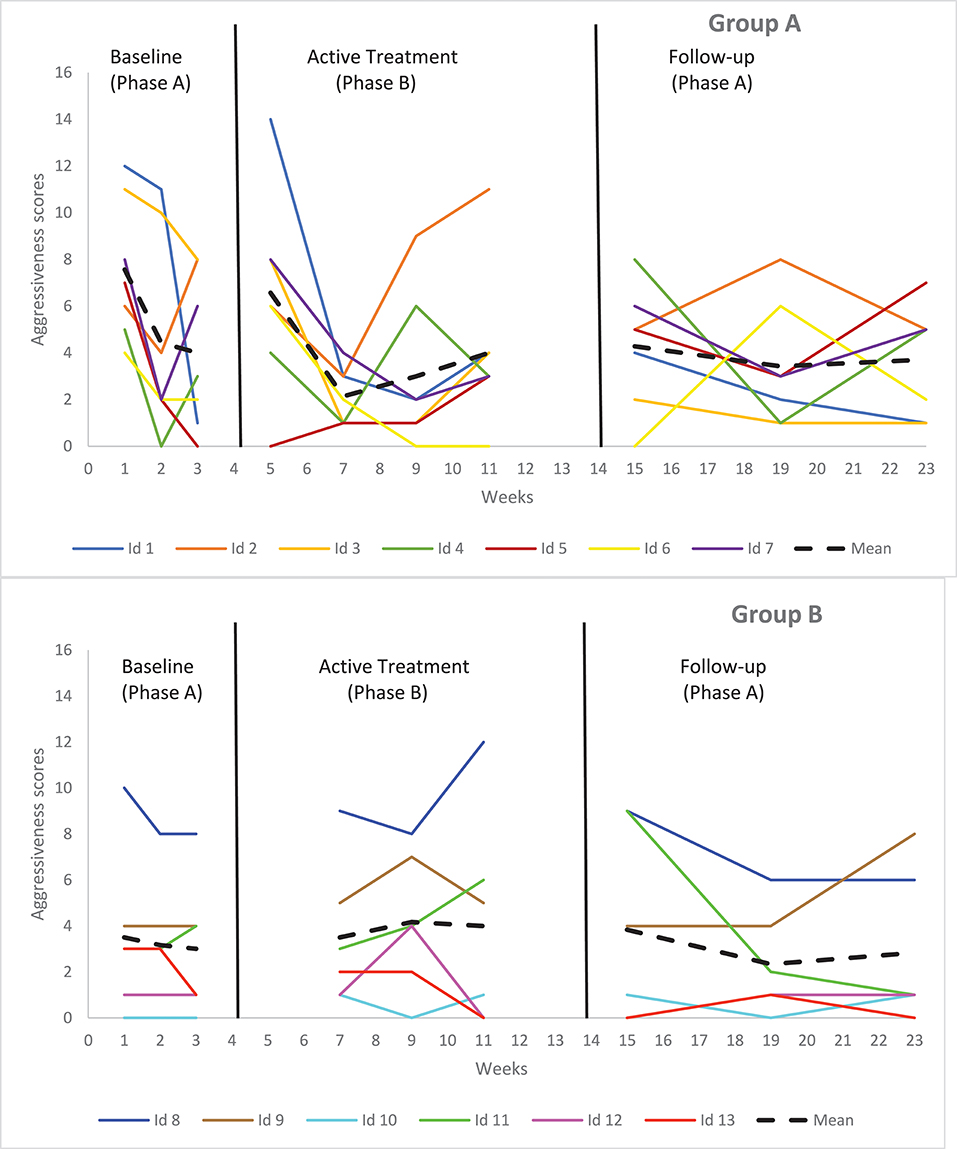
Figure 10. Graphical display of baseline level and changes in level between consecutive phases in aggressiveness for teacher-reported data.
The results of the weekly assessments showed no significant phase differences in scores or rates of change between the baseline, the active treatment phase and the follow-up phase for anxiety, depression, inattention, hyperactivity, and aggressiveness symptoms from teacher-reported data of Group B students (see Table 4 and Figures 6–10). Visual analysis of anxiety scores shows that, out of the six students comprising Group B, three have constant decreasing scores, whereas two have overall stable scores and one has an initial increase in scores, followed by a subsequent decrease. Visual analysis of inattention scores shows that all students have overall stable scores. Visual analysis of depression scores shows that four students have overall stable scores, whereas two have a marked increase in scores at the beginning of the active treatment phase, followed by a decrease. Finally, visual analysis of hyperactivity and aggressiveness scores shows that all students have overall stable scores throughout the baseline, intervention and follow-up periods.
The results of the weekly assessments showed no significant phase differences in scores or rates of change between the baseline, the active treatment and the follow-up phases for mindfulness scores from self-reported data in both Groups A and B (see Tables 3, 4). Visual analysis of the mean data shows somewhat flat and stable scores in mindfulness for students from both groups throughout all phases of this project, although a slight but non-significant increase in scores can be detected during the follow-up period for Group B students (see Figure 5). Specifically, out of the seven students comprising Group A, six have overall stable, but slightly increasing scores, whereas one has an initial drop in scores, followed by a stable increase. In Group B, out of the six students comprising this group, all have overall stable and slightly increasing scores.
The goal of this study was to evaluate the impact of a MBI on internalized and externalized symptoms in elementary school students with psychiatric disorders. In accordance with our initial hypothesis, the MBI was useful in decreasing inattention and indicative of a small effect on anxiety symptoms in Group A students, although there were no significant changes in symptoms from pre-to-post intervention in Group B students. Thus, our initial hypotheses have been somewhat supported in Group A students with regards to decreases in symptoms such as anxiety and inattention. However, our hypotheses were not supported for Group B students. Hypotheses regarding changes in mindfulness scores were not supported either. These results are similar to those that have been previously reported in the literature with regards to the impact of MBIs on mental health in clinical and school settings, among students in regular and special education classrooms (Zenner et al., 2014; Zoogman et al., 2014). However, it is imperative to note the high variability in individual trajectories from students in both groups, as highlighted by the detailed visual analysis. As such, although, as a whole, Group A students seem to have benefited more from the intervention than Group B students, high variability in scores showed that, in both groups, some students benefited from the intervention, whereas others reported a worsening of their symptoms. This is true of both Groups A and B students. Thus, results from this first, small-scale attempt to measure the impact of a MBI on students with severe psychological disorders need to be interpreted with caution. Furthermore, interestingly, results from the teacher-reported data showed a reversed pattern, i.e., a significant increase in anxiety scores during the follow-up phase for Group A students, and an absence of significant results for Group B students. This discrepancy between student and teacher reported data warrants careful attention.
Contrary to the self-reported data from Group A, the teacher-reported data show a significant increase in anxiety scores at follow-up. Furthermore, a visual analysis of all the teacher-reported data from Group A shows a similar pattern: an initial decrease in anxiety scores until week 7 (i.e., mid-intervention phase or 4th week of the MBI), followed by a steady increase in scores. At first glance, these results appear counterintuitive. Anecdotal evidence indicates that this teacher was especially fond of the MBI, convinced of its impact on her students and that she diligently completed in-between sessions assignments with her students. Specifically, she practiced a 3-min mindful stopping exercise once per day, every day, with her students. She also verbally reported that she saw important improvements in her students, specifically in terms of anxiety and inattention symptoms, and that she was impressed with their introspection skills and ability to share how they felt and reacted in regards to the mindfulness practice. However, the data seem to be telling a different story. Perhaps the process by which mindfulness develops can explain this discrepancy. As such, given that the teacher was taking part in the mindfulness sessions and that she extensively practiced with her students, it is quite possible that she, herself, developed heightened awareness skills throughout the intervention. This would have allowed her to identify and notice subtler manifestations of internalized and externalized symptoms in her students that she might not have noticed before. Thus, it is possible that, although she claimed that overall symptoms decreased in her students, she reported higher levels of these symptoms in the questionnaire, especially during the active treatment and follow-up phases, because of her sharpened and renewed awareness. Similar findings have been documented in children, where an initial increase in symptom scores was reported because of increased awareness skills, before an improvement could be observed (Malboeuf-Hurtubise et al., 2017b). This can impede the ability to use the multiple assessment design for MBIs. An avenue to disentangle this issue would be to assess the teachers' own mindfulness skills, before and after the intervention, as teachers' increasing self-awareness and self-regulation may indeed allow them to develop a higher degree of attachment with students, thus creating a shift in their ability to detect both internalized and externalized symptoms in their students. Direct assessment of awareness (e.g., breath counting tests) may also represent a good avenue to solve this issue in future work (Levinson et al., 2014). Another potential avenue to settle this issue and to control for this in future research would be to assess teacher expectations at pre-intervention. A teacher with high initial expectations could be potentially disappointed with a smaller decrease in symptoms than what would have been initially expected. This might bias the reporting of symptoms throughout time in students (G. Dupuis, personal communication, May 2017).
Discrepancies between self-reported and teacher-reported data from Group A also point to the importance of maintaining a regular meditation practice after the end of the intervention, in order to maintain and acquire lasting mindfulness skills. Specifically, these results shed light on the choice of the mindfulness instructor in school-based settings. In this study, the school psychologist led the intervention sessions. Thus, after the eighth and final session, she stopped visiting the classrooms once per week to meditate with students. Perhaps providing extensive mindfulness training to teachers, allowing them to lead sessions with their students, would ensure that regular practice and acquired skills are maintained over time throughout the follow-up period and once the 8-weeks intervention is completed, and that both teachers and students continue to observe improvements in internalized and externalized symptoms. This important consideration could be addressed in future MBI work in school settings, both in regular and special education classrooms, being as teachers, at least in the Quebec/French Canadian school system, have more consistent presence with students than school psychologists, namely for financial and budgetary reasons.
Furthermore, as previously stated, self-reported data from Group A indicates improvements in internalized symptoms (anxiety and inattention) that were not observed by their teacher. This might speak to the fact that improvements that were noted in internalized symptoms did not translate into overall improvements in classroom and school functioning, thus making it difficult for the teacher to notice. One tentative explanation for this would be that teachers would be less able to discern changes in internalized symptoms, namely because these are less noticeable by a third-party observer, and because manifestations of this type of symptoms do not tend to disrupt classroom dynamics as much as manifestations of externalized symptoms (e.g., hyperactivity, aggressiveness). However, there is a paucity of research on teachers' ability to discern changes in internalized symptoms (namely anxiety) in their students, so this potential explanation needs to be interpreted with caution (Stanger and Lewis, 1993; Layne et al., 2006). This being said, similar results showing this type of discrepancy have been reported in previous work with elementary school students in regular and special education classrooms (Malboeuf-Hurtubise et al., 2017b,c).
Finally, it is worth noting that only Group A students reported significant decreases in anxiety and inattention at follow-up. Group B students did not report significant changes on any variable. It is possible that Group A students were more impressionable and wanted to impress adults (whether this be the psychologists, researchers, or teachers), thusly impacting their self-report. However, anecdotal evidence provided by Group B's teacher and the school psychologist who led the sessions seems to indicate that these students were globally less motivated to participate in MBI sessions and to fill out the questionnaires. They also seemed to display more limits in terms of cognitive reasoning and introspection skills, which made sharing periods more strenuous. It seems that Group B students were also much more prone to social desirability and aware of others' reactions during sharing time, verbalizing that they did not want to “look stupid in front of others,” or “give the wrong answer.” Thus, given students from Group B were very sensitive to feedback from their peers, the judgment and perception of classmates might have a significant impact on their desire to engage in mindfulness meditation, especially in a classroom setting (Harter, 1990; Brown, 2004; Sebastian et al., 2008). In our opinion, this could have potentially biased the data collection for this group. Future work could evaluate if these feelings of self-consciousness and embarrassment around practicing with peers is a legitimate concern that could be generalized to a greater population. If so, designing a means to attenuate this effect would be desirable. Toward that end, having interventions delivered by trained individuals who are closer in age to students who are like peer-mentors might alleviate some of these concerns for students, as they look up to people of this age bracket in different manner than they do with older adults (Malboeuf-Hurtubise et al., 2016). Finally, including a validated scale of treatment adherence in future studies of this sort could be useful, as treatment adherence could be used as a covariate in statistical analyses.
Perhaps the presence of significant results in Group A and the absence of significant results in Group B could also be explained by the age difference that was observed between students from each group. Indeed, typically, younger students seem to be naturally more mindful than their older counterparts (Snel, 2012). From a developmental perspective, younger children, who have not yet reached the stage of abstract reasoning, are more naturally inclined to be aware of the present moment and are less prone to ruminations, anxious and depressive thoughts (Piaget, 1962; Semple et al., 2010). Consequently, it is possible that these children may be more receptive to mindfulness meditation, and thus could benefit more from this type of intervention. Furthermore, given their history and background of psychiatric disorders and potential trauma (especially in the case of students who were in foster care at the time of conducting this study), it is possible that the MBI was more useful in alleviating symptoms in younger students, as maladaptive behaviors and reactive patterns were less crystallized and thus more malleable, leaving more room for improvements in terms of decreasing internalized and externalized symptoms (Broidy et al., 2003). Further work on the impact of MBIs for students with psychiatric and attachment disorders could thus look into trauma-sensitive mindfulness practices (Thompson et al., 2011; Boughner et al., 2016; Hanley et al., 2017) in order to take into account recommendations for the treatment of students living with the intense emotional trauma that is often associated with living in foster care, in order to increase the potential impact of this type of intervention. Furthermore, for students with severe trauma, there is the possibility that mindfulness meditation could bring up sublimated or repressed memories that might actually lead to an increase in anxiety and symptoms of depression. Therefore, additional literature that engages with this as a possibility is needed, so as to not fall into the trap of typifying mindfulness as a “silver-bullet” intervention. This being said, it is also a possibility that students from Group B might have grown over time in biological or psychological markers of emotional resilience, thus contributing to the fact that they did not report significant differences in scores over time. However, anecdotal evidence based on the feedback obtained from professionals and teachers participating in this project suggests that this was not the case for these students. This being said, given the fact that group differences were not statistically tested as part of this project, and especially because the age difference between groups remains quite small, these explanations remain, at best, very tentative at the moment. These potential explanations are thus presented here as food for thought. Future work evaluating group differences would help in either confirming or infirming these age-related hypotheses.
This study counts notable strengths. It is the only one known to the authors that provides specific information regarding the impact of a MBI for students with psychiatric disorders (and, for the most part, a comorbid attachment disorder) in a special education curriculum. The n-of-1 trial design that was chosen for this study allowed for a detailed study of intra-individual changes in mindfulness as well as internalizing and externalizing symptoms over time in these students. This approach allowed us to evaluate statistically the process of change in both groups, which in turn provides valuable information to researchers interested in developing and testing MBIs for elementary school students with special education needs. Finally, no attrition was experienced in this study, solidifying our results.
The A-B-A design that was chosen for this study presents minor risks in regards to internal validity, such as time-related factors or history (Barlow et al., 2009). As the intervention was conducted during the winter, it is possible that the weather and time of year influenced participants' mood. Furthermore, as the follow-up period took place in the spring, it is possible that the end of the school year induced more positive feelings in our participants. If the design of a study looks at the unfolding of processes upon a certain time window, it is crucial that these issues are sensitively recorded and taken into account. It is thus possible that the lack of significant changes may reflect a positive result, given that children would have gotten worse on some of the scales, within the time frame of the study. A multiple baseline approach could help in solving these issues. It is also possible that self-reported data overstated pre-to-post changes, as they were potentially expecting a positive impact of the MBI. In this study, the participating personnel were fully aware of the study design and hypotheses, and so by definition were biased. Measuring expectations at pre-intervention, as stated above, could help control for this issue, as well as including blind observers in future work.
Furthermore, given the repeated-measures component of this study and, consequently, the need to shorten the questionnaire completion time, only a few selected items from each scale were administered to participants. Additionally, these scales were not used as a diagnostic tool, but rather as an indicator of within-subject fluctuations in chosen symptoms. However, a more methodologically sound alternative could be to aggregate all scores together and study positive and negative changes in symptoms, instead of fluctuations of individual categories of symptoms. Also noteworthy is the fact that these scales had not been previously used in N-of-1 trials, and that data regarding within-subject variability inherent to multiple administrations is not available. It is thus possible that this variability has created noise that is larger than the observed effect of the MBI.
The addition of an active control group and randomization of participants in future n-of-1 trials of this sort would provide additional methodological rigor, allowing to draw more robust conclusions in regards to the impact of MBIs for students with psychiatric disorders. The advantage of a control group, even a passive wait-list control group, is that it allows to track fluctuations that may be due to periods of possible increased stress (e.g., winter versus spring, examination periods, changes in school personnel, end of the year stress). Acknowledging caregivers and parental perspectives would also help to improve on this design, providing a more complete portrait of the situation. Caregivers can attest to pre-to-post changes in internalized and externalized symptoms in their children, which tend to manifest at home. Furthermore, it is possible that the degree of emotional support and engagement that students have in the home would have an impact on the degree to which they are able to emotionally engage in the MBI, as they are more likely to experience an environment in which they can have self and emotion regulation modeled for them in the home. Furthermore, combining MBI training programs for students and caregivers, in order to support students' practice at home, might be another viable option to bring about further positive results. However, given the fact that a majority of participants were in foster care at the time of conducting this study, it is a possibility that the involvement of parents would be difficult to obtain. Additional assessment time-points would also improve on the overall design of future studies of this sort. Although previous work on this issue has stated that a minimum of three assessment time-points per phase is necessary to observe change in participants, a targeted number of five per phase has been recommended, and would thus solidify future MBI n-of-1 trial designs (Smith, 2012).
Finally, results from this study evaluated the mean change in participants. However, individual differences in trajectories tend to reveal a more complex picture in regards to the impact of the MBI on participants' internalized and externalized symptoms. As such, individual variability of internalized and externalized symptoms scores suggests that the MBI worked differently for different students. However, individual trajectory analysis is beyond the scope of this paper. Future work could focus extensively on individual trajectories of elementary school students with psychiatric disorders receiving special education services, which would provide clues onto the differential impact of MBIs for this population. Another option could also be to include individual meetings in addition to the group-based intervention, in order to better track and understand why some youth benefit from the intervention and why some do not. This would allow researchers to have a more complete picture of the process of change in this heterogeneous sample of youth, especially given that the heterogeneity of the sample would be difficult to change in future work, because of the reality of school-based settings in which students with different severe psychiatric disorders are assigned to the same classroom. Individual meetings would also allow to identify further which factors can explain why some students report benefits from the intervention while others do not. It is quite possible that some of these factors were simply not identified in the present study, as we did not measure and control for individual characteristics attributable to group heterogeneity. Future work could also control for the differential impact of baseline meta-cognitive and self-awareness abilities in students, as one would expect that this would drive change more so than age.
Results from this study show substantial variation between students, tested cohorts and raters of internalizing and externalizing symptoms and behaviors. Therefore, the conservative conclusion from such variation can only be that more research is needed, as no firm conclusion as to the utility of MBIs for such groups of children with special education needs can be established: there was simply too much variation in the results. Nonetheless, the results do indicate directions for future research to explore this variation, namely in terms of who the respondents are, the homogeneity of the group within which the intervention is implemented, time of the year during which the intervention is implemented and by whom. Thus, these results warrant caution regarding the overall impact and efficacy of MBIs as a universal treatment option for youth with psychiatric disorders in a special education curriculum.
This study was carried out in accordance with requirements of the Research and Ethics Committee of the Sainte-Justine Mother and Child Hospital Center, in Montreal, Canada. The protocol and study were reviewed and approved by the Research and Ethics Committee of the Sainte-Justine Mother and Child Hospital Center, responsible for granting ethics approvals. All subjects and their parents gave written informed consent in accordance with the Declaration of Helsinki.
CM-H conceptualized and coordinated the study, adapted the mindfulness-based intervention and trained the school psychologist involved in this study, performed data analysis, and drafted the manuscript. GT contributed extensively to data interpretation and revision of the manuscript. LP helped in data collection and coordination of the study, while contributing to data interpretation and revision of the manuscript. EL contributed to the design of the study and revision of the manuscript.
CM-H and EL have released a manual on the mindfulness-based intervention described and used in this study (Midi Trente Publishers).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Arlington, TX: American Psychiatric Pub.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct validity of the five facet mindfulness questionnaire in meditating and nonmeditating samples. Assessment 15, 329–342. doi: 10.1177/1073191107313003
Barlow, M., Nock, M., and Hersen, M. (2009). Single Case Experimental Designs: Strategies for Studying Behavior for Change. Boston, MA: Pearson; Allyn Bacon.
Bennathan, M., and Boxall, M. (2013). Effective Intervention in Primary Schools: Nurture Groups. London: Routledge.
Biegel, G. M., Brown, K. W., Shapiro, S. L., and Schubert, C. M. (2009). Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: a randomized clinical trial. J. Consult. Clin. Psychol. 77, 855–866. doi: 10.1037/a0016241
Boswell, J. F., Anderson, L. M., and Barlow, D. H. (2014). An idiographic analysis of change processes in the unified transdiagnostic treatment of depression. J. Consult. Clin. Psychol. 82, 1060–1071. doi: 10.1037/a0037403
Boughner, E., Thornley, E., Kharlas, D., and Frewen, P. (2016). Mindfulness-related traits partially mediate the association between lifetime and childhood trauma exposure and PTSD and dissociative symptoms in a community sample assessed online. Mindfulness 7, 672–679. doi: 10.1007/s12671-016-0502-3
Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., et al. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: a six-site, cross-national study. Dev. Psychol. 39, 222–245. doi: 10.1037/0012-1649.39.2.222
Brown, B. B. (2004). “Adolescents' relationships with peers,” in Handbook of Adolescent Psychology, eds R. M. Lerner and L. Steinberg (New York, NY: Wiley), 363–394.
Canadian Teachers' Federation. (2012). Understanding Teachers' Perspectives on Student Mental Health: Findings From a National Survey. Ottawa, ON.
Crescentini, C., Capurso, V., Furlan, S., and Fabbro, F. (2016). Mindfulness-oriented meditation for primary school children: effects on attention and psychological well-being. Front. Psychol. 7:805. doi: 10.3389/fpsyg.2016.00805
Ferron, J. M., Bell, B. A., Hess, M. R., Rendina-Gobioff, G., and Hibbard, S. T. (2009). Making treatment effect inferences from multiple-baseline data: the utility of multilevel modeling approaches. Behav. Res. Methods 41, 372–384. doi: 10.3758/BRM.41.2.372
Gravetter, F. J., and Forzano, L.-A. B. (2011). Research Methods for the Behavioral Sciences: PSY 200 (300) Quantitative Methods in Psychology Series. Stamford, CT: Western Cengage Learning, 151–152.
Hanley, A. W., Garland, E. L., and Tedeschi, R. G. (2017). Relating dispositional mindfulness, contemplative practice, and positive reappraisal with posttraumatic cognitive coping, stress, and growth. Psychol. Trauma 9, 526–536. doi: 10.1037/tra0000208
Harris, A. D., McGregor, J. C., Perencevich, E. N., Furuno, J. P., Zhu, J., Peterson, D. E., et al. (2006). The use and interpretation of quasi-experimental studies in medical informatics. J. Am. Med. Inform. Assoc. 13, 16–23. doi: 10.1197/jamia.M1749
Harter, S. (1990). Developmental differences in the nature of self-representations: implications for the understanding, assessment, and treatment of maladaptive behavior. Cognit. Ther. Res. 14, 113–142. doi: 10.1007/BF01176205
Kabat-Zinn, J. (1994). Wherever You Go There You Are: Minfulness Meditation in Everyday Life. New York, NY: Hyperion.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context–past, present, and future. Clin. Psychol. Sci. Pract. 10, 144–156. doi: 10.1093/clipsy.bpg016
Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., et al. (2012). Single-case intervention research design standards. Remedial Spec. Educ. 34, 26–38. doi: 10.1177/0741932512452794
Lavoie, C., Couture, C., Bégin, J.-Y., and Massé, L. (2017). The differentiated impact of Kangaroo Class programmes in Quebec primary schools: examining behavioural improvements in relation to student characteristics. Emotional Behav. Difficulties. 22, 1–15. doi: 10.1080/13632752.2017.1335118
Layne, A. E., Bernstein, G. A., and March, J. S. (2006). Teacher awareness of anxiety symptoms in children. Child Psychiatry Hum. Dev. 36, 383–392. doi: 10.1007/s10578-006-0009-6
Levinson, D. B., Stoll, E. L., Kindy, S. D., Merry, H. L., and Davidson, R. J. (2014). A mind you can count on: validating breath counting as a behavioral measure of mindfulness. Front. Psychol. 5:1202. doi: 10.3389/fpsyg.2014.01202
Malboeuf-Hurtubise, C., Achille, M., Muise, L., Beauregard-Lacroix, R., Vadnais, M., and Lacourse, É. (2016). A mindfulness-based meditation pilot study: lessons learned on acceptability and feasibility in adolescents with cancer. J. Child Family Stud. 25, 1168–1177. doi: 10.1007/s10826-015-0299-z
Malboeuf-Hurtubise, C., Joussemet, M., Taylor, G., and Lacourse, E. (2017a). Effects of a mindfulness-based intervention on the perception of basic psychological need satisfaction among special education students. Int. J. Disabi. Dev. Educ. 65, 33–44. doi: 10.1080/1034912X.2017.1346236
Malboeuf-Hurtubise, C., and Lacourse, É. (2016). Mission Méditation: Pour des Élèves Épanouis, Calmes et Concentrés. Québec: Éditions Midi Trente.
Malboeuf-Hurtubise, C., Lacourse, E., Herba, C., Taylor, G., and Amor, L. B. (2017b). Mindfulness-based intervention in elementary school students with anxiety and depression: a series of n-of-1 trials on effects and feasibility. J. Evid. Based Complement. Altern. Med. 22, 856–869. doi: 10.1177/2156587217726682
Malboeuf-Hurtubise, C., Lacourse, E., Taylor, G., Joussemet, M., and Amor, L. B. (2017c). A mindfulness-based intervention pilot feasibility study for elementary school students with severe learning difficulties: effects on internalized and externalized symptoms from an emotional regulation perspective. J. Evid. Based Complement. Altern. Med. 22, 473–481. doi: 10.1177/2156587216683886
Maric, M., de Haan, E., Hogendoorn, S. M., Wolters, L. H., and Huizenga, H. M. (2015). Evaluating statistical and clinical significance of intervention effects in single-case experimental designs: an SPSS method to analyze univariate data. Behav. Ther. 46, 230–241. doi: 10.1016/j.beth.2014.09.005
Mental Health Commission of Canada (2013). School-Based Mental Health in Canada: A Final Report. Available online at: https://www.mentalhealthcommission.ca/Francais/system/files/private/document/ChildYouth_School_Based_Mental_Health_Canada_Final_Report_ENG.pdf
Moeyaert, M., Ferron, J. M., Beretvas, S. N., and Van den Noortgate, W. (2014). From a single-level analysis to a multilevel analysis of single-case experimental designs. J. Sch. Psychol. 52, 191–211. doi: 10.1016/j.jsp.2013.11.003
Molenaar, P. C., and Campbell, C. G. (2009). The new person-specific paradigm in psychology. Curr. Dir. Psychol. Sci. 18, 112–117. doi: 10.1111/j.1467-8721.2009.01619.x
Oberle, E., Schonert-Reichl, K. A., Hertzman, C., and Zumbo, B. D. (2014). Social-emotional competencies make the grade: predicting academic success in early adolescence. J. Appl. Dev. Psychol. 35, 138–147. doi: 10.1016/j.appdev.2014.02.004
Piaget, J. (1962). The stages of the intellectual development of the child. Bull. Menninger Clin. 26, 120–128.
Reynolds, C. C., and Kamphaus, R. W. (2004). The Behavior Assessment System for Children. 2nd Edn. Bloomington, IN: AGS Publishing.
Schonert-Reichl, K. A., Oberle, E., Lawlor, M. S., Abbott, D., Thomson, K., Oberlander, T. F., et al. (2015). Enhancing cognitive and social–emotional development through a simple-to-administer mindfulness-based school program for elementary school children: a randomized controlled trial. Dev. Psychol. 51, 52–66. doi: 10.1037/a0038454
Schork, N. J. (2015). Personalized medicine: time for one-person trials. Nature 520, 609–611. doi: 10.1038/520609a
Sebastian, C., Burnett, S., and Blakemore, S.-J. (2008). Development of the self-concept during adolescence. Trends Cogn. Sci. 12, 441–446. doi: 10.1016/j.tics.2008.07.008
Segal, Z. V., Williams, J. M. G., and Teasdale, J. D. (2018). Mindfulness-Based Cognitive Therapy for Depression. New York, NY: Guilford Publications.
Semple, R. J., Lee, J., Rosa, D., and Miller, L. F. (2010). A randomized trial of mindfulness-based cognitive therapy for children: promoting mindful attention to enhance social-emotional resiliency in children. J. Child Fam. Stud. 19, 218–229. doi: 10.1007/s10826-009-9301-y
Shadish, W. R. (2014). Analysis and meta-analysis of single-case designs: an introduction. J. Sch. Psychol. 52, 109–122. doi: 10.1016/j.jsp.2013.11.009
Shadish, W. R., Kyse, E. N., and Rindskopf, D. M. (2013). Analyzing data from single-case designs using multilevel models: new applications and some agenda items for future research. Psychol. Methods 18, 385–405. doi: 10.1037/a0032964
Shadish, W. R., Rindskopf, D. M., and Hedges, L. V. (2008). The state of the science in the meta-analysis of single-case experimental designs. Evid. Based Commun. Assess. Interv. 2, 188–196. doi: 10.1080/17489530802581603
Sibinga, E. M., Webb, L., Ghazarian, S. R., and Ellen, J. M. (2016). School-based mindfulness instruction: an RCT. Pediatrics 137:e20152532. doi: 10.1542/peds.2015-2532
Smetanin, P., Briante, C., Stiff, D., Ahmad, S., and Khan, M. (2015). The Life and Economic Impact of Major Mental Illnesses in Canada. Ottawa, ON: Mental Health Commission of Canada.
Smith, J. D. (2012). Single-case experimental designs: a systematic review of published research and current standards. Psychol. Methods 17, 510–550. doi: 10.1037/a0029312
Smith, J. D., Eichler, W. C., Norman, K. R., and Smith, S. R. (2015). The effectiveness of collaborative/therapeutic assessment for psychotherapy consultation: a pragmatic replicated single-case study. J. Pers. Assess. 97, 261–270. doi: 10.1080/00223891.2014.955917
Stanger, C., and Lewis, M. (1993). Agreement among parents, teachers, and children on internalizing and externalizing behavior problems. J. Clin. Child Psychol. 22, 107–116. doi: 10.1207/s15374424jccp2201_11
Tarrasch, R., Margalit-Shalom, L., and Berger, R. (2017). Enhancing visual perception and motor accuracy among school children through a mindfulness and compassion program. Front. Psychol. 8:281. doi: 10.3389/fpsyg.2017.00281
Taylor, G., and Malboeuf-Hurtubise, C. (2016). “La présence attentive en milieu scolaire: État des connaissances et pistes de recherche pour l'avenir,” in La Présence Attentive (Mindfulness): État des Connaissances Théoriques, Empiriques et Pratiques, eds S. Grégoire, L. Lachance, and L. Richer (Québec: Presses de l'Université du Québec), 161–180.
Thompson, R. W., Arnkoff, D. B., and Glass, C. R. (2011). Conceptualizing mindfulness and acceptance as components of psychological resilience to trauma. Trauma Violence Abuse 12, 220–235. doi: 10.1177/1524838011416375
Van den Noortgate, W., and Onghena, P. (2008). A multilevel meta-analysis of single-subject experimental design studies. Evid. Based Commun. Assess. Interv. 2, 142–151. doi: 10.1080/17489530802505362
Van Vliet, K. J., Foskett, A. J., Williams, J. L., Singhal, A., Dolcos, F., and Vohra, S. (2017). Impact of a mindfulness-based stress reduction program from the perspective of adolescents with serious mental health concerns. Child Adolesc. Ment. Health 22, 16–22. doi: 10.1111/camh.12170
Vohra, S., Shamseer, L., Sampson, M., Bukutu, C., Schmid, C. H., Tate, R., et al. (2016). CONSORT extension for reporting N-of-1 trials (CENT) 2015 Statement. J. Clin. Epidemiol. 76, 9–17. doi: 10.1016/j.jclinepi.2015.05.004
Wood, P., and Brown, D. (1994). The study of intraindividual differences by means of dynamic factor models: rationale, implementation, and interpretation. Psychol. Bull. 116, 166–186. doi: 10.1037/0033-2909.116.1.166
Zenner, C., Herrnleben-Kurz, S., and Walach, H. (2014). Mindfulness-based interventions in schools—a systematic review and meta-analysis. Front. Psychol. 5:603. doi: 10.3389/fpsyg.2014.00603
Keywords: school psychology, mindfulness-based interventions, psychiatric disorders, internalized symptoms, externalized symptoms, mental health
Citation: Malboeuf-Hurtubise C, Taylor G, Paquette L and Lacourse E (2018) A Mindfulness-Based Intervention for Students With Psychiatric Disorders in a Special Education Curriculum: A Series of n-of-1 Trials on Internalized and Externalized Symptoms. Front. Educ. 3:66. doi: 10.3389/feduc.2018.00066
Received: 12 April 2018; Accepted: 31 July 2018;
Published: 03 September 2018.
Edited by:
Claudio Longobardi, Università degli Studi di Torino, ItalyReviewed by:
Sharinaz Hassan, Curtin University, AustraliaCopyright © 2018 Malboeuf-Hurtubise, Taylor, Paquette and Lacourse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Malboeuf-Hurtubise, Y2F0aGVyaW5lLm1hbGJvZXVmLWh1cnR1YmlzZUB1YmlzaG9wcy5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.