 Elizabeth Downes
Elizabeth Downes Judith Wold
Judith Wold Mesrak Belatchew2
Mesrak Belatchew2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CURRICULUM, INSTRUCTION, AND PEDAGOGY article
Front. Educ. , 31 July 2017
Sec. Public Health Education and Promotion
Volume 2 - 2017 | https://doi.org/10.3389/feduc.2017.00029
This article is part of the Research Topic International Partnerships for Strengthening Health Care Workforce Capacity: Models of Collaborative Education View all 33 articles
There is an acute shortage of health-care workers in Sudan. The Academy of Health Sciences was created to prepare health-care professionals in order to restore and ultimately maintain the requisite skills-mix. This necessitates transformative education using a context-relevant curricula. A context-relevant curriculum is one that is feasible, consistent with the mission of the educational institution, and responsive to the communities of interest. This article describes a partnership to strengthen the local capacity of health workforce educators. The article describes one of a series of faculty development workshops, with this first aimed at the skills to develop and evaluate context-relevant curricula using community midwifery curriculum as exemplar.
There is an acute shortage of health-care workers in Sudan. According to the Sudan Academy of Health Sciences (AHS), an estimated 180,000 health professionals are needed (Elhuda, 2015). A transformative scaling up of health professional preparation is imperative to the improvement of population health outcomes in Sudan, similar to other low- and middle-income countries. Critical elements of transformative education include a clear strategy or framework, and effective and relatable health sciences education to increase—not just the quantity—but also the quality and relevance of health-care professionals (Celletti et al., 2011; World Health Organization, 2013). This necessitates context-relevant curricula developed and revised by local faculty. Iwasiw and Goldenberg (2015) define context-relevant curricula as feasible, responsive to the communities of interest, and consistent with the mission of the educational institution.
Aiming at such a transformative scaling up, the Federal Ministry of Health (FMH) in Sudan created the AHS. The AHS has 17 campuses throughout the country and is dedicated to sustained “improvement of the health of the people of Sudan through innovation, equity, excellence in health professions education, service, and research” (Elhuda, 2015). Envisioned as a unique institute for educating and developing nurses, midwives, and other health-care professionals including; community health workers, anesthesia assistants, theater room attendants, sanitary overseers, and medical assistants, with a mission “to restore and maintain the skill-mix of the health team” (Elhuda, 2015). This article describes a partnership to strengthen the local capacity of educators to develop and evaluate context-relevant curriculum to support such a transformative education of the health workforce. While the focus of the article is on the process of curriculum review and revision, findings from the review will be shared.
The SPHTI is a collaborative effort between The Carter Center (TCC) and the AHS to build capacity for the education of community midwives and community health workers, among others. The SPHTI creates an enabling environment to leverage local expertise and skills contributing to the development of a health work force that is able to respond to the primary health-care needs of both urban and rural communities. As in many countries, there is a need for faculty development (Kiguli-Malwadde et al., 2014; Olopade et al., 2016) and SPHTI works with health science faculty at AHS to strengthen curriculum and teaching skills, develop health learning materials based on the local context, and build capacity of local health science educational institutions. The Carter Center–Emory University partnership creates a platform for north–south collaboration among higher education institutions with faculty from Emory’s Nell Hodgson Woodruff School of Nursing (NHWSN) serving as educational consultants to the program.
The goal of the (SPHTI) is to strengthen the health professions education system to develop a well-performing, stable, and equitably distributed workforce with an appropriate mix of skills to meet maternal and child health needs in Sudan. Objectives include:
• Develop skills of health science faculty members;
• Develop/adapt health learning materials; and
• Monitor and evaluate SPHTI contributions to United Nations’ Sustainable Development Goals 3 and 4 focusing on health and quality of education, respectively.
A core structure for the project is the SPHTI Technical Working Group (TWG). Based in Sudan, the TWG is composed of technical advisors from the FMH with expertise in health workforce development, management, planning, and monitoring of public health training. The TWG works with TCC on a daily basis and provides technical input to the project. In an effort to address the first two objectives, the TWG identified a need for faculty development and the NHWSN was asked to design a series of workshops. This article describes the first of these workshops.
Rather than importing curricula, health sciences education should be aligned with the health needs of the country (Miller et al., 2011) and context relevant. Using the “CIPP Model” can help determine the feasibility, responsiveness, and relevance of curriculum. The CIPP model, developed by Daniel Stufflebeam, is a unique, inclusive method of evaluation (Stufflebeam and Shinkfield, 2007). Each of the four components of the model; CIPP, is important, and when viewed together allow evaluators to access a rich, full picture in terms of not just the content and implementation of a project, but also it’s setting. This is imperative when analyzing curricula and programs in places as diverse as Taiwanese universities (Chien et al., 2007), agricultural schools in Nigeria (Osokoya and Adekunle, 2007), service-learning programs in North Carolina (Zhang et al., 2011), and allied health education in Sudan. The underlying theme of the CIPP model is “that evaluation’s most important purpose is not to prove but to improve” (Stufflebeam, 2003, p. 31).
Two, 2-day workshops were held in Khartoum, the capital of Sudan in a conference room of a centrally located hotel. The two workshops were attended by 42 faculty and administrators of the AHS (chosen by the FMH and AHS) who were involved in the various programs of the AHS. The NHWSN team consisted of two faculty members from NHWSN with expertise in education to serve as workshop facilitators, two staff from TCC, including local national staff and two Ethiopian midwives, staff of NHWSN’s Maternal and Newborn Health Program (MaNHEP) in Ethiopia. Facilitators from NHWSN were educational experts with many years of global health experience. In addition to the workshop, the team was requested to produce a standard operating procedure (SOP) for the evaluation of AHS curriculum. The CIPP model was chosen for the SOP.
The NHWSN team facilitated the workshop in English as the AHS faculty went through a curriculum review process, using the CIPP framework and the midwifery curriculum as a template. Ideally, having completed the process once, it can be repeated for the curricula for the other health cadres. Participants were divided into groups, sitting at tables of 5–7 in order to potentiate participation. Each group had a copy of the AHS mission and vision statement, the AHS midwifery curriculum and supporting documents, the International Confederation of Midwives (ICM) Global Standards for Midwifery Education [International Confederation of Midwives (ICM) (2011)] and Essential Competencies [International Confederation of Midwives (ICM) (2013)], the World Health Organization Global Standards for the Initial Education of Professional Nurses and Midwives (World Health Organization, 2009), and other relevant documents. These documents were used to assess the alignment of the curriculum with the AHS mission and values as well as the alignment with international standards.
Additionally, in-depth interviews and focus group discussions were conducted with faculty, students, and alumna of the program outside the capital in Wad Madani in Al Gezira state. This was an important part of the CIPP process to assure input from the communities of interest as discussed below. A full analysis of these focus groups is beyond the scope of this paper and is forthcoming. Interviews and focus groups were conducted by Arabic-speakers, recorded, transcribed, and translated into English.
Workshop objectives were met. By the end of each training session, participants demonstrated competency in the use of the CIPP model for curriculum review. Findings of the review are discussed below.
Further, the curriculum documents were reviewed separately by the two team members from Ethiopia using the CIPP Model. These Ethiopian team members have created curriculum and taught community midwifery skills in the Emory MaNHEP program (Spangler et al., 2014) and are familiar with Ethiopia’s community health worker program. Ethiopia borders Sudan and faces similar challenges in maternal/child and reproductive health. Suggestions for improvement were given. Ethics approval for the project was given by both Emory and AHA Institutional Review Boards Teaching.
Curriculum must be considered in the context, or “big picture,” of where the program “lives.” Curriculum to prepare midwives at an institution in Ireland (Phelan et al., 2014), Jordan (Shaban and Leap, 2012), and Sudan may have shared competencies, but should also reflect the local context. A context evaluation looks at the fit of a program within a larger framework, be that university, college, or community. It can determine opportunities and threats/strengths and weaknesses that can influence the program (Mertens and Wilson, 2012). Context includes the program’s written and published vision, mission, and goals and should be compatible and aligned with the mission of the institution in which the program is offered. These serve as the basis for development of the curriculum.
This component identifies assets and needs in order to determine current system capabilities. Both material and human resources for the program should be included. Material resources such as teaching facilities, textbooks, computers, skills lab items, and student living facilities are included. Existing and proposed student-related policies are considered. Human resources include faculty, staff, students, and other communities of interest. When identified at the onset of a program, inputs describe the starting point and help to define a program’s needs, propose budgets, and identify appropriate curriculum design (Zhang et al., 2011; Frye and Hemmer, 2012).
Process evaluation monitors, assesses, and documents the implementation of a program. Process evaluation provides feedback on the program by assessing and documenting the level of success in meeting the needs of the communities of interest. The evaluators regard the original plan, explore its implementation and, through multiple methods, determine the alignment and accuracy of the proposed and implemented plans. These methods can include document review, interviews with students and alumni, and observations of classes and practical experiences. The goal of process evaluation is: “to forecast the mistake of designs; to provide information for decisions; and to assure the procedure of plans” (Tseng et al., 2010, p. 257). Keeping in mind the underlying theme for using the CIPP model, process evaluation is better seen as identifying areas for improvement, rather than simply proving the planned activities were completed as designed.
This component seeks to determine if the product of the program meets the needs of the targeted beneficiaries and communities of interest. In order to consider short- and long-term outcomes for a community midwifery educational program, evaluators would look not just at a graduating class, but ideally, the performance of those graduates 3–5 years after graduation. Additionally, faculty outcomes must also be considered as they are also of the community of interest. Product evaluation necessitates a variety of resources and techniques. Document review, including student logs, papers, and exams and summative evaluations, is important. As well, focus groups and interviews with students, alumni, faculty, employers, and other members of the community of interest can be informative. Finally, determining the program’s own systematic plan for evaluation is informative. When compared to the standards identified for the context of the program, product evaluation may inform “decisions to continue, stop, or improve the effort” (Stufflebeam, 2003, p. 32).
Workshop participants reviewed the mission and vision statements for the FMH, the AHS, the midwifery curricula, and the competencies and standards for midwifery education per the ICM [International Confederation of Midwives (ICM, orld Health Organization, 2011, 2013)] and World Health Organization (World Health Organization, 2009). The mission, vision, and goals of the FMH, AHS, and the midwifery curriculum are well aligned (see Table 1). The mission of the midwifery program, however, is limited to reducing maternal mortality. Participant faculty indicates that this should be expanded to include health promotion of women and infants.
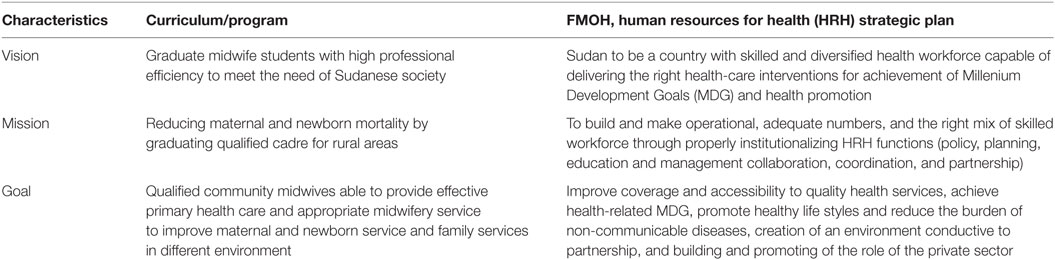
Table 1. Comparison of vision, mission, and values.
A strength of the CIPP model for evaluation of this program is the inclusion of context. During the curriculum review, the AHS faculty found the midwifery curriculum to be consistent with the mission statements of both of the FMH and AHS, which seek to address the critical shortage. In the situation of Sudan, the context includes a lack of midwives and other health professions, high maternal and infant mortality, and limited capacity for educating health professionals. The innovation of a 15-month community midwifery program is designed specifically for Sudan to fill the gap. However, even with the 1-year apprenticeship program required for the students to sit the qualifying exams, this does not meet the minimum length of education as published in the Global Standards for Midwifery Education (ICM, 2013). A footnote to these standards recognizes that “the actual time needed may vary depending on many factors within countries” [International Confederation of Midwives (ICM), 2013, p. 6]. This is an important consideration. Further analysis is needed to determine if quality of care is compromised by AHS’ variance from the recommended time frame.
As stated above, inputs include both material and human resources for the program. For many low resource settings, this can present a challenge. There are limited materials published in Arabic for midwifery education. Furthermore, sanctions on Sudan make the importation of learning materials and equipment problematic. However, there are some teaching and learning materials published locally in Arabic including lecture notes. In terms of human resources, an additional consideration is the admission criteria presently being unmarried females under the age of 25. Officially, the entry criteria include high school completion (consistent with the ICN standards), but students are accepted in rural areas with completion of primary school. In more remote areas, recruiting candidates interested in midwifery who meet all the entry requirements can be challenging. It was felt that having communities select and recommend candidates might improve the recruitment of young women into the profession.
The third component of the CIPP is process evaluation. Following a review of the curriculum, workshop participants determined that the World Health Organization’s International Guidelines for Midwifery Education (World Health Organization, 2009) were adapted appropriately for the context in Sudan. The curriculum is well developed both vertically and horizontally, allowing students to build on previous knowledge. The core competencies were all addressed but individual curricular objectives could be revised for clarity. For instance, ethics content, which was felt to be essential for this cadre, was lacking in the first semester. Faculty teaching in the program was able to describe the student log books used for continual assessment but the process of evaluation of this component was limited in that the workshop format did not allow for participants to view actual student documents, visit classrooms, or interview students.
The last aspect of the CIPP is product evaluation. While lacking a published systematic plan for evaluation, the AHS does have standard assessment tools and requirements for passing. Faculty and students complete end of course questionnaires and some are interviewed. A year-long mentorship after graduation assists with competency evaluation after which graduates take a national qualifying examination.
The CIPP model for curriculum design and evaluation served as a useful tool to determine the context-relevance of one of the AHS program curricula. It allows for a rich, full picture in terms of not just the content and implementation but considers the context for the program. Overall, the review of the community midwifery curriculum by the AHS was seen by participants of the workshop as providing sustainable skill for the expansion of health professional education. It was seen as important efforts to increase the quantity and relevance of the health-care work force in Sudan. To determine if the program will truly strengthen the country’s health system and improve outcomes, it is imperative to evaluate the quality of care provided by the new class of midwives 3–5 years after completion of the program. Faculty attending the workshop will train other AHS education personnel in the use of the CIPP model in evaluating other health professions programs taught by AHS.
ED, JW, MB, AM, and SB were all substantial contributors to the conception or design of the work; the drafting and revisions of it; responsible for important intellectual content; for final approval of the version to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Celletti, F., Reynolds, T. A., Wright, A., Stoertz, A., and Dayrit, M. (2011). Educating a new generation of doctors to improve the health of populations in low- and middle-income countries. PLoS Med. 8:e1001108. doi: 10.1371/journal.pmed.1001108
Chien, M., Lee, C., and Cheng, Y. (2007). The construction of Taiwan’s educational indicator systems: experiences and implications. Educ. Res. Policy Pract. 6, 249–259. doi:10.1007/s10671-007-9026-x
Elhuda, D. (2015). “Academy of health sciences (AHS),” in Paper Presented at: PHTI Program Review, Atlanta, GA.
Frye, A. W., and Hemmer, P. A. (2012). Program evaluation models and related theories: AMEE guide no. 67. Med. Teach. 34, e288–e299. doi:10.3109/0142159X.2012.668637
International Confederation of Midwives (ICM). (2011). Global Standards for Midwifery Education: Companion Guidelines 2010. The Hague: ICM, 9.
International Confederation of Midwives (ICM). (2013). The Essential Competencies for Basic Midwifery Practice 2010. The Hague: ICM, 6.
Iwasiw, C. L., and Goldenberg, D. (2015). Curriculum Development in Nursing Education, 3rd Edn. New York, NY: Jones & Bartlett Learning, 454.
Kiguli-Malwadde, E., Olapade-Olaopa, E. O., Kiguli, S., Chen, C., Sewankambo, N. K., Ogunniyi, A. O., et al. (2014). Competency-based medical education in two Sub-Saharan African medical schools. Adv. Med. Educ. Pract. 9, 483–489. doi:10.2147/AMEP.S68480
Mertens, D. M., and Wilson, A. T. (2012). Program Evaluation Theory and Practice: A Comprehensive Guide. New York: The Guilford Press.
Miller, B. M., Eichbaum, Q., Brady, D. W., and Moore, D. E. (2011). Aligning health sciences education with health needs in developing countries. Acad. Med. 86, e10. doi:10.1097/ACM.0b013e318232cc89
Olopade, F., Adaramoue, O., Raji, Y., Faola, A., and Olapade-Olaopa, E. (2016). Developing a competency-based medical curriculum for the core basic medical sciences in an African medical school. Adv. Med. Educ. Pract. 18, 389–398. doi:10.2147/AMEP.S100660
Osokoya, M., and Adekunle, A. (2007). Evaluating the trainability of enrollees of the Leventis foundation (Nigeria) agricultural schools’ programs. Aust. J. Adult Learn. 47(1):111–135.
Phelan, A., O’Connell, R., Murphy, M., McLoughlin, G., and Long, O. (2014). A contextual clinical assessment for student midwives in Ireland. Nurse Educ. Today 34, 292–294. doi:10.1016/j.nedt.2013.10.016
Shaban, I., and Leap, N. (2012). A review of midwifery education curriculum documents in Jordan. Women Birth 25, e47–e55. doi:10.1016/j.wombi.2011.09.001
Spangler, S., Barry, D., and Sibley, L. M. (2014). An evaluation of equitable access to a community-based maternal and newborn health program in rural Ethiopia. J. Midwifery Womens Health 59, S101–S109. doi:10.1111/jmwh.12133
Stufflebeam, D. (2003). “The CIPP model for evaluation,” in International Handbook of Educational Evaluation, eds T. Kellaghan and D. Stufflebeam (Boston, MA: Kluwer Academic Publishers), 31–62.
Stufflebeam, D. L., and Shinkfield, A. J. (2007). Evaluation Theory, Models, & Applications. San Francisco, CA: Jossey-Bass, 768.
Tseng, K. H., Diez, C. R., Lou, S. J., Tsai, H. L., and Tsai, T. S. (2010). Using the context, input, process and product model to assess an engineering curriculum. Trans. Eng. Tech. Ed. 8(3):256–261.
World Health Organization. (2009). Global Standards for the Initial Education of Professional Nurses and Midwives. Available at: http://www.who.int/hrh/nursing_midwifery/hrh_global_standards_education.pdf
World Health Organization. (2013). Transforming and Scaling Up Health Professionals’ Education and Training. Geneva: World Health Organization Guidelines. Available at: http://apps.who.int/iris/bitstream/10665/93635/1/9789241506502_eng.pdf
Zhang, G., Griffith, R., Metcalf, D., Williams, J., Shea, D., and Misulis, K. (2011). Using the Context, Input, Process, and Product Evaluation Model (CIPP) as a comprehensive framework to guide the planning, implementation, and assessment of service-learning programs. J. High Educ. Outreach Engage. 15(4):57–84.
Keywords: curriculum, CIPP, transformative education, evaluation, capacity, pre-service education
Citation: Downes E, Wold J, Belatchew M, Mustafa A and Blount S (2017) Strengthening Educational Capacity through Context-Relevant Curriculum Design and Evaluation. Front. Educ. 2:29. doi: 10.3389/feduc.2017.00029
Received: 29 December 2016; Accepted: 15 June 2017;
Published: 31 July 2017
Edited by:
Jennifer Gail Audette, University of Rhode Island, United StatesReviewed by:
Darcell P. Scharff, Saint Louis University, United StatesCopyright: © 2017 Downes, Wold, Belatchew, Mustafa and Blount. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elizabeth Downes, ZWRvd25lc0BlbW9yeS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.