
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 23 December 2022
Sec. Cardiovascular Imaging
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1074956
This article is part of the Research TopicNovel Approaches In Cardiac ImagingView all 20 articles
 Christophe Beyls1,2*
Christophe Beyls1,2* Pierre Huette1,2Paul Vangreveninge1Florent Leviel1Camille Daumin1BenAmmar Ammar1Gilles Touati3
Pierre Huette1,2Paul Vangreveninge1Florent Leviel1Camille Daumin1BenAmmar Ammar1Gilles Touati3 Bouzerar Roger4
Bouzerar Roger4 Thierry Caus3
Thierry Caus3 Hervé Dupont1,2Osama Abou-Arab1
Hervé Dupont1,2Osama Abou-Arab1 Diouf Momar5
Diouf Momar5 Yazine Mahjoub1,2
Yazine Mahjoub1,2Background: Conventional transthoracic (TTE) and transoesophageal echocardiography (TEE) parameters assessing right ventricle (RV) systolic function are daily used assuming their clinical interchangeability. RV longitudinal shortening fraction (RV-LSF) is a two-dimensional speckle tracking parameter used to assess RV systolic function. RV-LSF is based on tricuspid annular displacement analysis and could be measured with TTE or TEE.
Objective: The aim of the study was to determine if RV-LSFTTE and RV-LSFTEE measurements were interchangeable in the perioperative setting.
Methods: Prospective perioperative TTE and TEE echocardiography were performed under general anesthesia during scheduled cardiac surgery in 90 patients. RV-LSF was measured by semi-automatic software. Comparisons were performed using Pearson correlation and Bland-Altman plots. RV-LSF clinical agreement was determined as a range of −5 to 5%.
Results: Of the 114 patients who met the inclusion criteria, 90 were included. The mean preoperative RV-LSFTTE was 20.4 ± 4.3 and 21.1 ± 4.1% for RV-LSFTEE. The agreement between RV-LSF measurements was excellent, with a bias at −0.61 and limits of agreement of −4.18 to 2.97 %. All measurements fell within the determined clinical agreement interval in the Bland-Altman plot. Linear regression analysis showed a high correlation between RV-LSFTTE and RV-LSFTEE measurement (r = 0.9; confidence interval [CI] 95%: [0.87–0.94], p < 0.001).
Conclusion: RV-LSFTTE and RV-LSFTEE measurements are interchangeable, allowing RV-LSF to be a helpful parameter for assessing perioperative changes in RV systolic function.
NCT: NCT05404737. https://www.clinicaltrials.gov/ct2/show/NCT05404737.
Echocardiography is a non-invasive, simple, and helpful technique in patients undergoing interventional cardiology procedures, cardiac surgery, high-risk non-cardiac surgery, and for diagnosing intra- or post-operative complications (1). Two-dimensional transthoracic echocardiography (TTE) and transoesophageal echocardiography (TEE) are routinely used to qualitatively and quantitatively evaluate the structure and function of the heart (2). TTE and TEE echocardiographic assessment of the right ventricular (RV) systolic function is challenging and requires a multiparametric approach that combines conventional parameters, such as tricuspid annular plane displacement (TAPSE), RV fractional area change (RV-FAC), and advanced speckle tracking parameters (3).
In interventional cardiology procedures, TEE is used to guide device placement and assess the periprocedural changes of RV systolic function (4). During cardiac surgery, intraoperative TEE is crucial in assisting surgical decision-making. It is also a helpful monitoring tool for providing an immediate point-of-care assessment of RV systolic function, especially with TAPSE and RV-FAC parameters (1, 3, 5). In the intensive care unit, RV systolic function is routinely assessed using conventional parameters measured by transthoracic echocardiography. This evaluation is crucial for RV failure diagnosis, global hemodynamic management, and ventilator parameters setting (5). In daily practice, RV systolic parameters measured by TTE and by TTE are often used interchangeably and assumed clinically equivalent, even if their measurement must be done with caution (6). Actually, the values of conventional RV-systolic function parameters obtained in TTE and TEE were not comparable due to a large variability, a poor correlation (8), and an underestimation with TEE (7). For some authors, RV strain parameters and 3D RV ejection fraction (3D-RVEF) should be used to avoid the variability and angle dependency of the conventional RV systolic parameters (6). However, the measurement of RV strain parameters and 3D-RVEF required high image quality and specific probes, thus limiting their use in clinical routine.
The right ventricle longitudinal shortening fraction (RV-LSF) is a two-dimensional speckle tracking echocardiography (2D-STE) parameter based on the longitudinal tricuspid annular displacement (TAD) that assesses the global RV systolic function (9). RV-LSF is a semi-automatic, angle-independent, and accurate 2D-STE parameter for assessing RV systolic dysfunction in several clinical settings (10, 11). Besides, RV-LSF is a fast and reproducible post-processing 2D-STE parameter less dependent on image quality (12) and loading conditions (13) than RV strain parameters. RV-LSF combines the longitudinal displacement of the lateral (TADlat) and septal (TADsep) portion of the tricuspid ring toward the RV apex. RV-LSF can be measured by TTE or TEE (14). In TTE, RV-LSF is more correlated to the RV ejection fraction, evaluated in magnetic resonance imaging (9) or three-dimensional echocardiography (12), than conventional and strain parameters. Besides, RV-LSF is more accurate for identifying patients with RV dysfunction (10).
However, to our knowledge, RV-LSF values measured by TTE and TEE have not been compared. Mainly, there are no data assessing the interchangeability of RV-LSFTTE and RV-LSFTEE. In TEE, several factors could affect RV-LSF measurement and, therefore, its interchangeability: TEE view is foreshortened and does not fully display the apical portion of the RV, which is crucial for ROI placement. Besides, the dynamic and non-planarity of the tricuspid annulus could also affect the measurement of TADlat and TADsep.
The first aim of the study was to determine whether RV-LSFTTE and RV-LSFTEE measurements could be considered interchangeable in the perioperative setting. The second aim was to study the interchangeability of the two components of RV-LSF (TADlat and TADsep).
This prospective interventional study was conducted at Amiens university hospital (Amiens, France) between August 2021 and April 2022. We prospectively included all adult patients (>18 years old) hospitalized for a scheduled cardiac surgery under cardiopulmonary bypass that required intraoperative TEE. Exclusion criteria were patients with a contraindication to TEE performance (gastric or esophageal pathology), a poor echogenicity on TEE, a TTE not allowing evaluation of RV-LSF, and patients with a rapid supraventricular rhythm disorder at the time of TEE and TTE.
This is a single-center, prospective and interventional study of patients hospitalized at Amiens University Hospital for scheduled cardiac surgery under cardiopulmonary bypass (CPB). The study was approved by the Amiens University Hospital IRB (CHU–Place V. Pauchet, 80054 AMIENS Cedex) and by an institutional ethics committee (Comité de Protection des Personnes Ile de France VIII, ID-RCB 2021_A000908-33). Oral and written information was provided to the patients.
Echocardiography images were obtained using high-quality commercially available probes (S5-1 for TTE, X7-2T for TEE, Philips Healthcare) and ultrasound systems (CX 50, Philips Healthcare). To assess the interchangeability of RV-LSF, TTE and TEE exams, respectively, were performed in patients under general anesthesia immediately after induction of anesthesia, oral intubation, and muscle blockade. The procedures for general anesthesia and mechanical ventilation were standardized for all patients. The TEE and TTE echocardiography protocols followed the American Society of Echocardiography and the European Society of Cardiology recommendations for assessing RV systolic function (3, 15).
RV-LSF was measured using dedicated software (Automated Cardiac Motion Quantification, QLAB version 15.0, Philips Medical Systems, Andover, MA, USA). For RV-LSF analysis, three regions of interest (ROI) were used to initialize the first diastolic frame in a mild-esophageal four-chamber (ME-4CH) view (Figure 1A, Supplementary Video 1) for the TEE procedure and in an RV-focused apical four-chamber view for the TTE procedure (Figure 1B, Supplementary Video 2). These ROI were placed 1) on the tricuspid annulus at the insertion of the anterior tricuspid valve leaflet (RV free wall), 2) on the tricuspid annulus at the insertion of the septal leaflet, and 3) on the RV apex. The software automatically tracked and calculated three parameters: (1) the displacement between the RV free wall and the RV apex (TADlat), (2) the displacement between the interventricular septum and the RV apex (TADsep), and (3) the RV-LSF. RV-LSF was calculated as the maximum end-systolic displacement (LES) of the mid-annular point from the measured annular motion and is expressed as a percentage of the end-diastolic RV longitudinal dimension (LED): 100 × (LED–LES)/LED. The software automatically selected the mid-annular point.
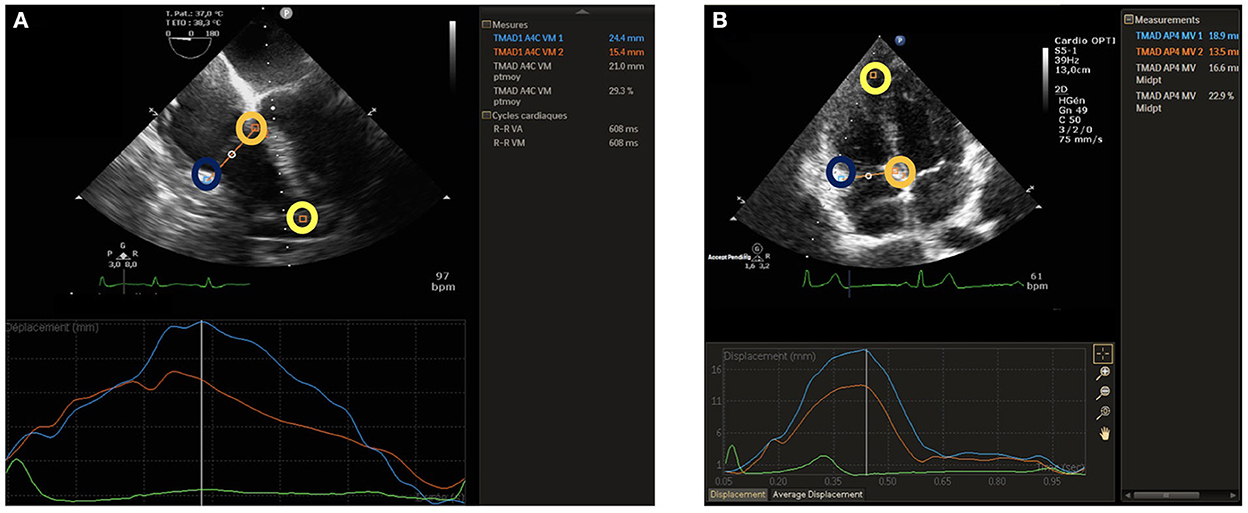
Figure 1. TEE RV-LSF measurement (A) and TTE RV-LSF measurement (B). A lateral point (blue circle) and a septal point (orange circle) were placed at the bottom of the RV free wall and the bottom of the interventricular septum. A third point was placed at the apex (yellow circle). TAD lateral, septal, and RV longitudinal shortening fraction (RV-LSF) values were automatically displayed in percentage. The mid-annular point is automated and selected by the software.
RV-LSF was analyzed in a single beat, and the reported value was the average of 3 measurements. All TTE and TEE RV-LSF measurements were analyzed offline (separately and randomly) by an expert sonographer 2 weeks after the inclusion period.
In TTE, conventional RV systolic parameters were measured according to international guidelines: tricuspid annular plane systolic excursion (TAPSE) was measured using M-mode with a cursor placed at the junction of the lateral tricuspid leaflet and the RV free wall. RV-S' wave was measured in the apical four-chamber view using Doppler tissue imaging mode. RV systolic and diastolic areas were measured in the apical four-chamber view in 2D mode. RV-fractional area change was calculated by subtracting the end-systolic area from the end-diastolic area and dividing this value by the end-diastolic area. The following variables were recorded: age, gender, body weight, personal medical history, logistic EuroSCORE II, type of cardiac surgery, preoperative plasmatic creatinine, and hemoglobin.
Continuous variables were expressed as mean and 95% confidence interval or standard deviation. Categorical variables are presented as absolute numbers and percentages. The correlation between TTERV − LSF and TEERV − LSF measurements was quantified using Pearson's coefficient. Bland-Altman (BA) analysis was performed to assess the level of agreement between RV-LSFTTE and RV-LSFTEE.
Assuming a common standard deviation equal to 5 points for each of the RV-LSF values (TTE and TEE), the standard deviation of the difference between the two measures is estimated to be 3.87 if a correlation coefficient (ρ) of 0.7 is assumed between the two RV-LSF measures. Thus, according to Bland and Altman (16), at least 90 evaluable patients would be required to estimate the limits of agreement (LOA) with an accuracy equal to 1 point in RV-LSF. We also performed Bland and Altman analysis to evaluate the levels of agreement between TADlat − TTE, TADlat − TEE, TADsep − TTE, and TADsep − TEE.
Limits of clinical relevance for RV-LSF: given that the mean RV-LSFTTE from healthy volunteers was 25.6 ± 4.8% (13), we expect a clinically insignificant difference between RV-LSFTTE and RV-LSFTEE to be 5 % (clinical LOA was −5 to 5%). The threshold for statistical significance was set to p < 0.05. To analyze the discrepancy between the different measures, we performed a Spearman correlation and a calculation of the intra-class coefficient (ICC). All statistical analyses were performed with R software (version 4.0.4).
From August 2021 to February 2022, 201 consecutive patients were hospitalized for scheduled cardiac surgery under cardiopulmonary bypass. Among the 114 patients who met the inclusion criteria, 90 patients were included, and 24 patients were finally excluded: 18 patients for poor TTE image quality, five patients due to a failed ROI placement, and one for rapid rhythm disorder (see Figure 2, Flow chart). Demographic and preoperative data were summarized in Table 1. Among the 90 patients, 82% (n = 74/90) were men with an average age of 63 ± 11 years. The average logistic EuroSCORE II was 4.3 ± 4, and valve repair/replacement was the main cardiac surgical procedure (n = 33/90, 37%).
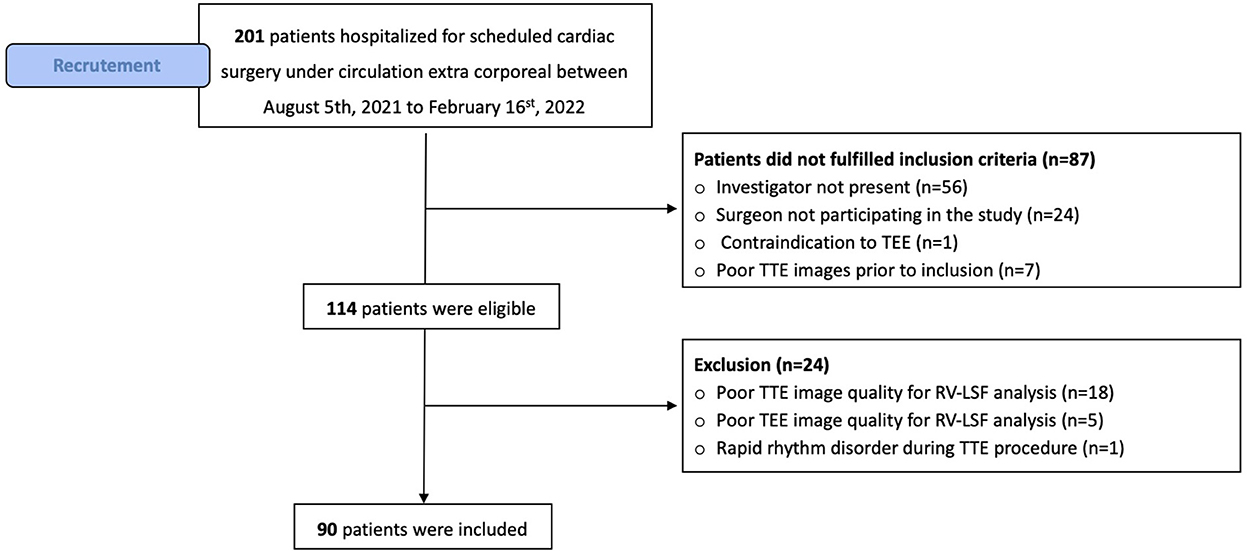
Figure 2. Flow chart of the study.
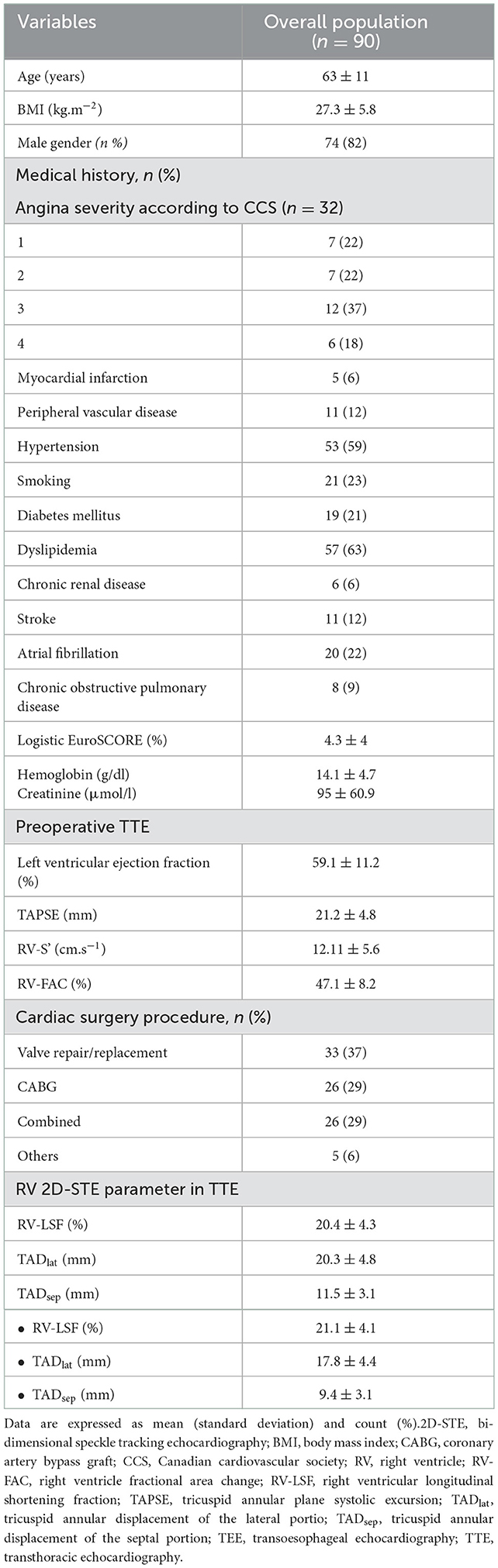
Table 1. Demographics and echocardiographic data of the population.
The mean preoperative RV-LSFTTE was 20.4 ± 4.3% and 21.1 ± 4.1% for RV-LSFTEE measurements. Bland-Altman analysis showed an excellent agreement between RV-LSFTTE and RV-LSFTEE measurements. The bias between the two methods was −0.61%, with LOA ranging from −4.18 to 2.97% (Table 2). Figure 3A showed that 95% of RV-LSF measurements fell within the LOA (−4.18 to 2.97 %) and, therefore, within the clinical relevance limits (−5 to 5%) that we had initially determined. Linear regression analysis showed that there was a strong positive correlation between RV-LSFTTE and RV-LSFTEE with a Pearson linear correlation coefficient of 0.91 (CI95% = [0.87–0.94]; P < 0.001) and with an excellent model fit (y = 0.36 + 0.95x, r = 0.82, Figure 4A).
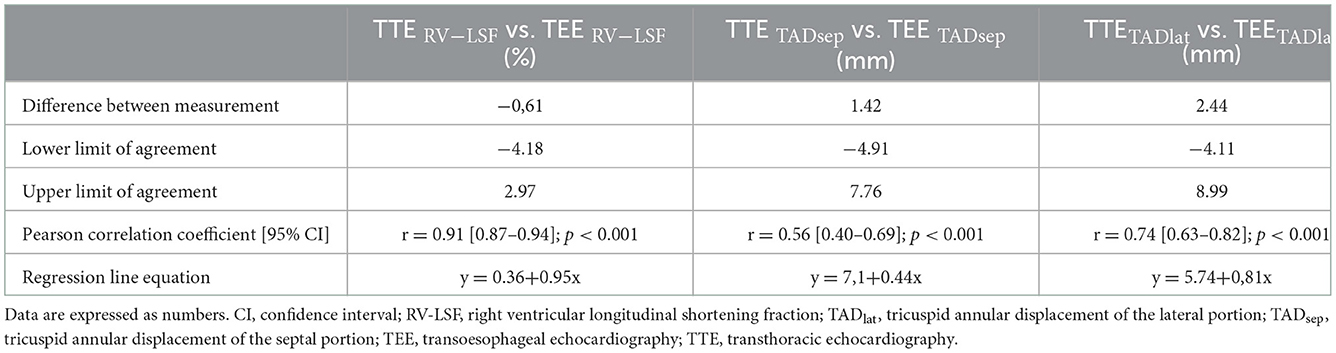
Table 2. Correlation coefficient and difference between RV-LSF, TADsep, and TADlat measurement in TTE and TTE.
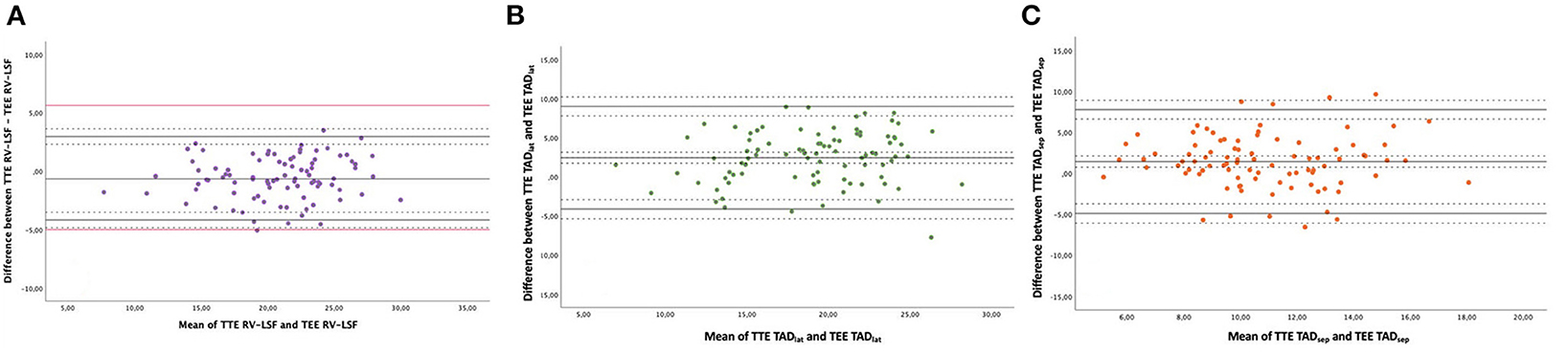
Figure 3. Bland-Altman plots between TTE and TEE measurements with (A) TTE RV-LSF vs. TEE RV-LSF. (B) TTE TADlat vs. TEE TADlat. (C) TTE TADsep vs. TEE TADsep. This plot displays a scatter diagram of the difference between the two techniques' measurements plotted against the average of the two technique's measurements. The black plain line represents the mean of the difference (= bias) between the two ultrasound methods. The other plain lines represent the upper and lower limits of agreement. Dotted black horizontal lines represent the 95% CI interval for the bias and the limits of agreement. The red line represents the determined pertinent clinical agreement (−5; +5%) of the RV-LSF measurement.
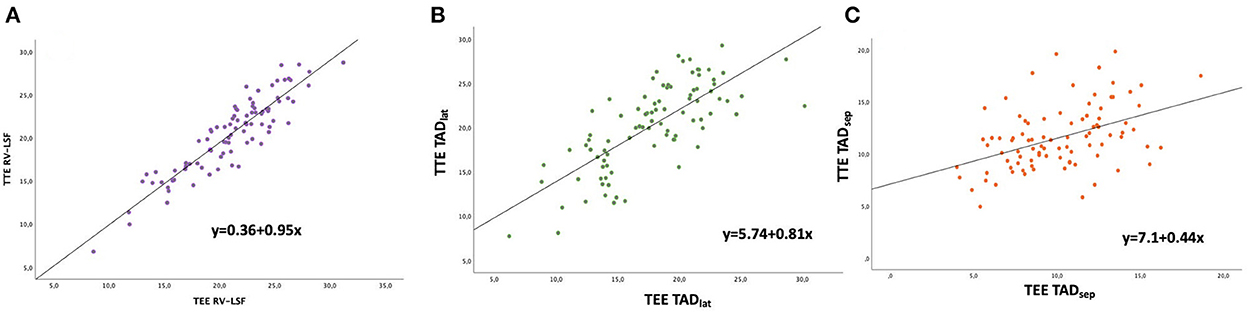
Figure 4. Scatter plots of TTE as a function of TEE measurements of (A) RV-LSF (B) TAD lateral, and (C) TAD septal.
The mean preoperative TADlat − TTE was 20.3 ± 4.8 mm and 17.8±4.4 mm for TADlat − TEE measurement. Figure 3B showed a reasonable agreement between the two echocardiographic methods for TADlat measurement with a bias of 2.44 mm and LOA ranging from −4.11 to 8.99 mm (outside the range for clinical agreement). The 2.44 mm bias corresponded to 12.8% relative bias compared to the overall TADlat measurements with LOA from −21.6 to 47.3%. A good correlation was found between TADlat − TTE and TADlat − TEE (r = 0.74, CI95% = [0.63–0.82], P < 0.001, Figure 4B). For the TTE and TEE TADsep measurements, Figure 3C showed that TEE underestimated the TADsep measurement compared to the TADsep − TTE measurement with a bias of 1.42 mm and LOA ranging from −4.9 to 7.7 mm. The corresponding relative bias of TADsep was 13.1% with LOA from −45.2 to 71.0% and moderate correlation between two TADsep measurements (r = 0.56, CI95% = [0.40–0.69], P < 0.001, Figure 4C). We found similar results after calculating the Spearman correlation and intra-class coefficients (Appendix Table 1).
The main findings of the present study can be summarized as follows: (1) RV-LSF measurements using TTE and TEE techniques were interchangeable, (2) TADlat exhibited a limited bias and good agreement between the two techniques but outside acceptable clinical agreement, and (3) TEE underestimated TADsep measurement.
Clinicians need interchangeable RV parameters between TTE and TEE because an accurate assessment of RV systolic function is of utmost importance for perioperative RV monitoring and precise diagnosis of RV dysfunction during postoperative follow-up. The most used TTE RV systolic parameters were RV-FAC and TAPSE, which are assumed to apply to TEE. In TEE, TAPSE measurement is challenging due to a problematic M-mode alignment. Hence, modified methods were proposed for assessing tricuspid systolic excursion with controversial results (7). RV-FAC measurement is limited by the endocardial border definition and its poor reproducibility (8). Despite significant disagreement between TTE and TEE measures (7, 8), RV systolic parameters are often used interchangeably in daily practice.
In this study, we demonstrated that RV-LSF measurements were interchangeable between TTE and TEE. The graphical Bland-Altman analysis showed a limited bias and LOA between the two ultrasound techniques. This is the first study to report an excellent agreement between TTE and TEE techniques using a clinical significance agreement (−5 to 5%) for a 2D-RV global systolic function parameter (8). Several factors explain this result: first, RV-LSF is a highly reproducible, repeatable, and accurate 2D-STE parameter (10). Indeed, RV-LSF is measured semi-automatically by the software (10). Second, unlike RV-strain assessment, RV-LSF measurement does not require high-resolution images. Moreover, during the TEE procedure, tricuspid annulus tracking is less affected by acoustic shadowing than RV-free wall myocardium (needed for strain analysis) (7). Hence, RV-LSF might be helpful in clinical follow-up from admission to the post-operative setting.
This is the first study that reported data about TADlat and TADsep measurement interchangeability. We found that TTE and TEE TADsep measurements were poorly correlated (r = 0.5) and not interchangeable. We observed a good correlation (r = 0.7) between TTE and TEE TADlat measurements. However, the graphical Bland-Altman analysis showed that both TADlat measurement were underestimated, and the LOA between the two methods were too broad for reasonable clinical interchangeability. The underestimation of the TEE measurement was probably because the TEE ME-4CH view may not represent the true long axis of the interventricular septum and causes a “foreshortening” view. Foreshortening view is a frequent problem in 2D echocardiography examinations. It occurs when the ultrasound beam does not cut through the true apex, leading to geometric distortion of the image. Therefore, the long axis of the ventricle appears shorter. Previous studies on LV function identified similar findings about underestimation of volumes due to foreshortening of the transesophageal imaging plane (17). The impact of the foreshortening view on RV-LSF measurement was probably limited because RV-LSF is a length ratio and because the underestimation of TADsep and TADlateral values, on which RV-LSF value depends, is relatively homogeneous (close to 12% for both).
Besides, as in our study, these results are probably related to using the RV apex as the reference point. Selection of RV apex can be challenging because TEE only partially reveals the apical portion of the RV, which is truncated or shortened; this leads to underestimating the measured parameters. The use of 3D echocardiography for assessing the RV systolic function is the best approach to avoid a foreshortening view and an underestimation of ventricle size or volumes (18).
Our results were close to that of other studies which assess the interchangeability between the longitudinal displacement analysis of the lateral portion of the tricuspid annular and TAPSE. Markin et al. compared TTE TAPSE by M-mode and TEE TAPSE by speckle tracking in 84 patients. They found that TAPSE by M-mode was correlated with TAPSE by speckle tracking in the ME-4CH view (Pearson r = 0.62), but they did not analyze the agreement between the two methods. In the study by Mauermann et al., TAD lateral (named speckle tracking TAPSE) was assessed in TEE and compared to TTE TAPSE. The authors found a significant correlation (r = 0.59) but with large LOA (−9.4 to 8.4 mm) (7).
This study had several strengths. First, this study prospectively acquired TTE and TEE images under identical clinical situations in mechanically ventilated patients under general anesthesia. Secondly, we performed a sample size calculation to assess clinical agreement between the two techniques to avoid underpowered analysis. Nevertheless, this study admits some limitations. First, RV-LSFTEE and RV-LSFTTE were calculated from loops recorded in a supine position, possibly resulting in a foreshortened apical view in TTE. To limit the impact of a foreshortening apical view on RV long-axis measurement due to supine position, we measured RV-LSF in an RV-focused apical four-chamber view as recommended (3). Second, we did not evaluate the inter-observer reproducibility for TTE and TEE for RV-LSF measurement. Indeed, because both ultrasound procedures were performed just before the surgical draping of the patient, we chose to shorten the duration of image acquisition to avoid any extensive delay before starting the surgical procedure. Third, TEE and TTE measurements were acquired by an echocardiography expert (level III competence according to the EACVI definition) (19) because the main issue is related to the imaging window. The ROI positioning on the lateral part of the tricuspid annular or the RV-apex may be limited because the sector window is too narrow and requires an optimal view. We believe that RV-LSF measurement should be performed by a physician with advanced training in TTE. Fourth, we failed to measure RV-LSFTEE in four patients with large aortic root. Hence, the use of RV-LSF appears to be limited for monitoring RV systolic function in aortic root surgery. Finally, as with many 2D-STE parameters, the software version is a potential limitation. It is possible that RV-LSF values measured by the Philips QLAB version 15.0 may not reflect results from another version of the same software (20, 21).
In this study, we showed that RV-LSFTTE and RV-LSFTEE measured in the operating room for patients undergoing cardiac surgery exhibited excellent clinical agreement, and thus were interchangeable. RV-LSF could be helpful in assessing RV systolic function during and after high-risk surgery.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Protection des Personnes Ile de France VIII, ID-RCB 2021_A000908-33. The patients/participants provided their written informed consent to participate in this study.
Study conception and manuscript drafting: CB, OA-A, DM, and YM. Clinical data collection: PV, FL, CD, PH, BA, GT, and TC. Statistical analysis: BR and DM. Manuscript revision: CB, HD, and YM. All authors approved the final version of the manuscript.
We want to thank Mrs. Annabelle Boussault for his precious help in this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.1074956/full#supplementary-material
2D-STE, two-dimensional speckle tracking echocardiography; LOA, limits of agreements; RV, right ventricle; RV-LSF, right ventricle longitudinal shortening fraction; TAD, tricuspid annular displacement; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
1. An Updated Report by the American Society of Anesthesiologists and the Society of Cardiovascular Anesthesiologists Task Force on Transesophageal Echocardiography. Practice Guidelines for Perioperative Transesophageal Echocardiography. Anesthesiology. (2010) 112:1084–96. doi: 10.1097/ALN.0b013e3181c51e90
2. Mahmood F, Shernan SK. Perioperative transoesophageal echocardiography: current status and future directions. Heart. (2016) 102:1159–67. doi: 10.1136/heartjnl-2015-307962
3. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the european association of cardiovascular imaging. J Am Soc Echocardiogr. (2015) 28:1–39.e14. doi: 10.1016/j.echo.2014.10.003
4. Labus J, Uhlig C. Role of echocardiography for the perioperative assessment of the right ventricle. Curr Anesthesiol Rep. (2021) 11:306–17. doi: 10.1007/s40140-021-00474-1
5. Vieillard-Baron A, Naeije R, Haddad F, Bogaard HJ, Bull TM, Fletcher N, et al. Diagnostic workup, etiologies and management of acute right ventricle failure: a state-of-the-art paper. Intensive Care Med. (2018) 44:774–90. doi: 10.1007/s00134-018-5172-2
6. Gebhardt BR, Asher S, Maslow A. the limitations of using transthoracic echocardiographic–derived normative values for grading intraoperative transesophageal echocardiography examinations of the right ventricle: are they really interchangeable? J Cardiothorac Vasc Anesth. (2020) 34:1260–2. doi: 10.1053/j.jvca.2020.02.024
7. Mauermann E, Vandenheuvel M, François K, Bouchez S, Wouters P. Right ventricular systolic assessment by transesophageal versus transthoracic echocardiography: displacement, velocity, and myocardial deformation. J Cardiothorac Vasc Anesth. (2020) 34:2152–61. doi: 10.1053/j.jvca.2020.03.009
8. Roberts SM, Klick J, Fischl A, King TS, Cios TJ. A comparison of transesophageal to transthoracic echocardiographic measures of right ventricular function. J Cardiothorac Vasc Anesth. (2020) 34:1252–9. doi: 10.1053/j.jvca.2019.11.039
9. Ahmad H, Mor-Avi V, Lang RM, Nesser H-J, Weinert L, Tsang W, et al. Assessment of right ventricular function using echocardiographic speckle tracking of the tricuspid annular motion: comparison with cardiac magnetic resonance: tricuspid annular displacement by speckle tracking. Echocardiography. (2012) 29:19–24. doi: 10.1111/j.1540-8175.2011.01519.x
10. Beyls C, Bohbot Y, Huette P, Booz T, Daumin C, Abou-Arab O, et al. Usefulness of right ventricular longitudinal shortening fraction to detect right ventricular dysfunction in acute cor pulmonale related to COVID-19. J Cardiothorac Vasc Anesth. (2021) 35:3594–03. doi: 10.1053/j.jvca.2021.01.025
11. Beyls C, Bohbot Y, Huette P, Abou-Arab O, Mahjoub Y. Tricuspid longitudinal annular displacement for the assessment of right ventricular systolic dysfunction during prone positioning in COVID-19 patients. J Am Soc Echocardiogr. (2020) 33:1055 doi: 10.1016/j.echo.2020.05.016
12. Maniwa N, Hozumi T, Takemoto K, Wada T, Kashiwagi M, Shimamura K, et al. Value of tissue-tracking tricuspid annular plane by speckle-tracking echocardiography for the assessment of right ventricular systolic dysfunction. Echocardiography. (2019) 36:110–8. doi: 10.1111/echo.14206
13. Beyls C, Bohbot Y, Caboche M, Huette P, Haye G, Dupont H, et al. Preload dependency of 2D right ventricle speckle tracking echocardiography parameters in healthy volunteers: a prospective pilot study. JCM. (2021) 11:19. doi: 10.3390/jcm11010019
14. Shen T, Picard MH, Hua L, Burns SM. Andrawes MN. Assessment of tricuspid annular motion by speckle tracking in anesthetized patients using transesophageal echocardiography. Anesth Analg. (2018) 126:62–7. doi: 10.1213/ANE.0000000000002614
15. Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, Lang RM, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr. (2013) 26:921–64. doi: 10.1016/j.echo.2013.07.009
16. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. (1986) 1:307–10. doi: 10.1016/S0140-6736(86)90837-8
17. Chengode S. Left ventricular global systolic function assessment by echocardiography. Ann Card Anaesth. (2016) 19:26. doi: 10.4103/0971-9784.192617
18. Medvedofsky D, Mor-Avi V, Amzulescu M, Fernández-Golfín C, Hinojar R, Monaghan MJ, et al. Three-dimensional echocardiographic quantification of the left-heart chambers using an automated adaptive analytics algorithm: multicentre validation study. Eur Heart J Cardiovasc Imaging. (2018) 19:47–58. doi: 10.1093/ehjci/jew328
19. Popescu BA, Andrade MJ, Badano LP, Fox KF, Flachskampf FA, Lancellotti P, et al. European Association of Echocardiography recommendations for training, competence, and quality improvement in echocardiography. Eur J Echocardiogr. (2009) 10:893–905. doi: 10.1093/ejechocard/jep151
20. Il'Giovine ZJ, Mulder H, Chiswell K, Arges K, Tomfohr J, Hashmi A, et al. Right Ventricular Longitudinal Strain Reproducibility Using Vendor-Dependent and Vendor-Independent Software. J Am Soc Echocardiogr. (2018) 31:721–32.e5. doi: 10.1016/j.echo.2018.01.008
21. Silverton NA, Lee JP, Morrissey CK, Tanner C, Zimmerman J, A. Comparison of left- and right-sided strain software for the assessment of intraoperative right ventricular function. J Cardiothorac Vasc Anesth. (2019) 33:1507–15. doi: 10.1053/j.jvca.2018.10.038
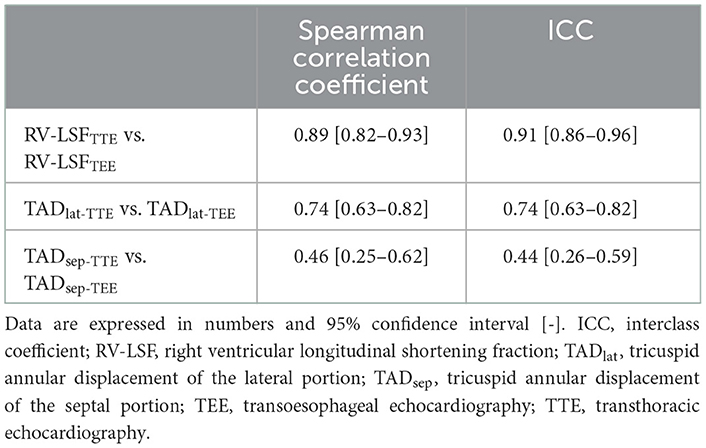
Table A1. Spearman correlation coefficient and ICC between RV-LSF, TADsep, and TADlat measurement in TTE and TTE.
Keywords: right ventricular shortening fraction, speckle tracking, interchangeability, right ventricle, tricuspid
Citation: Beyls C, Huette P, Vangreveninge P, Leviel F, Daumin C, Ammar B, Touati G, Roger B, Caus T, Dupont H, Abou-Arab O, Momar D and Mahjoub Y (2022) Interchangeability of right ventricular longitudinal shortening fraction assessed by transthoracic and transoesophageal echocardiography in the perioperative setting: A prospective study. Front. Cardiovasc. Med. 9:1074956. doi: 10.3389/fcvm.2022.1074956
Received: 20 October 2022; Accepted: 05 December 2022;
Published: 23 December 2022.
Edited by:
Francesco Pelliccia, Sapienza University of Rome, ItalyReviewed by:
Jian Wu, Fudan University, ChinaCopyright © 2022 Beyls, Huette, Vangreveninge, Leviel, Daumin, Ammar, Touati, Roger, Caus, Dupont, Abou-Arab, Momar and Mahjoub. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christophe Beyls,  YmV5bHMuY2hyaXN0b3BoZTU5QGdtYWlsLmNvbQ==
YmV5bHMuY2hyaXN0b3BoZTU5QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.