
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 09 June 2021
Sec. Cardio-Oncology
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.590016
This article is part of the Research Topic Management of Arterial and Venous Thrombosis in Cancer Patients View all 4 articles
 Isabela Bispo Santos da Silva Costa1
Isabela Bispo Santos da Silva Costa1 Fernanda Thereza de Almeida Andrade1
Fernanda Thereza de Almeida Andrade1 Diego Carter2Vinicius B. Seleme2Maycon Santos Costa3Carlos M. Campos2*Ludhmila Abrahão Hajjar1,2
Diego Carter2Vinicius B. Seleme2Maycon Santos Costa3Carlos M. Campos2*Ludhmila Abrahão Hajjar1,2Cancer and cardiovascular disease are the leading causes of mortality in the world. The prevalence of cardiovascular risk factors and coronary artery disease in cancer patients is elevated, and it is associated with high mortality. Several mechanisms, such as the proinflammatory and procoagulant states present in cancer patients, may contribute to these scenarios. Oncological therapy can predispose patients to acute thrombosis, accelerated atherosclerosis and coronary spasm. Treatment decisions must be individualized and based on the cancer history and balancing bleeding and thrombosis risks.
Cancer and its treatment are highly associated with coronary artery disease (CAD), which is an important cause of mortality in cancer survivors (1–4). The state of chronic inflammation present in cancer patients, which is associated with their predisposition to present arterial and venous thromboembolic events, may favour adverse events in the cardiovascular system (5, 6). In addition, several oncological therapies may cause severe coronary lesions due to the predisposition to accelerated atherosclerosis, endothelial dysfunction, acute coronary thrombosis and coronary spasm (7).
Notably, cancer and CAD share several risk factors, such as hypertension, diabetes, obesity, sedentarism, and smoking. Moreover, some factors commonly present in cancer patients, such as anaemia, hypoxaemia and hyperviscosity, are factors that trigger acute coronary syndrome (ACS) due to the imbalance in oxygen supply and consumption (3).
In the largest registry published on acute myocardial infarction (AMI) in cancer patients, the most common types of cancer associated with ACS were as follows: lung, prostate and breast cancer. Lung cancer was associated with the highest rates of in-hospital mortality and major adverse cardiovascular and cerebrovascular complications (MACCEs). In addition to this higher ischaemic risk, cancer patients also have a higher bleeding risk; colon cancer presented the highest risk of major bleeding (8).
Thus, the interaction between cancer and ACS is frequent and extremely complex, which is reflected in the higher mortality of cancer patients in this scenario (9, 10). Alterations in oxidative metabolism play important roles in the pathophysiological mechanisms underlying cancer and heart disease, especially in elderly patients. The concentrations of antioxidant enzymes are reduced in elderly subjects and may explain the reduced cardiac tolerance to oxidative stress, thus favouring the development of cardiovascular alterations. Additionally, elderly patients are more susceptible to developing cancer, and high oxidative stress during their lifespan may be an explanation for this (11).
Therapeutic decisions for these patients must involve a multidisciplinary approach, in which the clinician, oncologist, interventional cardiologist and surgeon must consider the cancer prognosis, risk of bleeding (tumour bleeding or coagulopathies), planned cancer therapy (post-chemotherapy thrombocytopaenia or oncological surgical procedures) and risk of thrombotic events. These definitions are essential for the proper prescription of anticoagulation or dual antiplatelet therapy and for deciding which treatment strategy (clinical, percutaneous, or surgical) is appropriate for each patient. This review aims to summarise the main aspects of patients with cancer and acute coronary syndrome to assist in the management, which is sometimes challenging, of these patients.
Cancer patients present high arterial and venous thrombotic risk (12, 13). It has been shown that at 6 months, cancer patients have more than twice the risk of arterial thromboembolism than non-cancer patients (4.7 vs. 2.2%). Most of these patients had myocardial infarction (2.0% in cancer patients vs. 0.7% in those without cancer) (14). In this same study, the types of cancers that presented the highest rates of arterial thromboembolism were lung, gastric, and pancreatic cancers (8.3, 6.5, and 5.9%, respectively). The mortality in 30 days was high in cancer patients (17.6%) when compared with that in patients without cancer (11.6%) (14).
A procoagulant state was even more prominent in the study by Brenner et al. Despite a course of anticoagulation, 8.7% patients developed a recurrence of venous thromboembolism (VTE), and 1.1% developed arterial events. Arterial thrombosis occurs earlier than the recurrence of venous thromboembolism in the follow-up after the first VTE event (36 vs. 97 days, p < 0.01). At 30 days of follow-up, 59% of patients with arterial events died, and the mortality associated with acute myocardial infarction (AMI) was also considerably high (40%) (15).
The procoagulant state in cancer patients is secondary to multiple mechanisms. Cancer cells present some procoagulant properties [such as procoagulant proteins (tissue factor), microparticles (MPs), coagulation factors and fibrinolysis proteins], and there is a strong interaction of platelets and endothelial cells (16). Cancer cells have two possible ways of predisposing to platelet activation: (1) direct adhesion of the cancer cell to platelets and (2) the production of molecules that lead to platelet activation by tumour cells (i.e., interleukin-6, ADP, thrombin, matrix metalloproteinases). Another potential mechanism that can explain the higher thrombosis risk is that cancer cells can activate the endothelium through adherence to endothelial cells or by the production of proinflammatory cytokines, such as thrombomodulin I, tissue factor, von Willebrand factor, selectins, and fibrinolysis proteins (PAI-1) (16).
The challenge of treating a procoagulant state (with either antiplatelet or anticoagulation therapy) is that the risk of bleeding cannot be neglected in cancer patients. For years, there was an important concern of the risk of bleeding due to thrombocytopaenia in cancer patients. Initial studies showed that cancer patients had worse prognosis than the general population, with a 1-year survival rate of only 26% (4). In this study, thrombocytopaenia (platelet count <100,000) was present in 73% of the patients. In a recently published meta-analysis, Long et al. observed that the use of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) in thrombocytopaenic patients was associated with any major bleeding [odds ratio (OR) 1.67, 95% CI: 1.42–1.97; p = 0.00001], including gastro-intestinal bleeding and haemorrhagic stroke (17). In patients with cancer and VTE on anticoagulant therapy, bleeding was the main cause of mortality (15).
In addition, the most frequent cause of gastrointestinal bleeding in patients receiving antithrombotic therapy is related to cancer (18). Gastrointestinal, urological and gynaecological tumours often present with active bleeding as initial symptoms. Patients with glioma have an increased risk of spontaneous intracranial haemorrhage (19). Rarely, some patients can present with ACS due to vascular compression or invasion by metastatic cardiac tumours (20). The central illustration summarises the main aspects of ACS in cancer patients.
Myocardial ischaemia among cancer patients can manifest in several ways, such as AMI, until sudden cardiac death (SCD) (21). Many chemotherapeutic drugs can induce ischaemia, and the mechanism of action is variable. Usually, these mechanisms have direct action on the vessels, such as a vasospastic effect causing endothelial injury or acute arterial thrombosis (22). Long-term cancer treatment may predispose to metabolic changes such as dyslipidaemia, and previous mediastinal radiotherapy (RT) accelerates the atherosclerotic process (22). Table 1 summarises common chemotherapeutics that may induce AMI and are correlated with its main mechanisms of action.
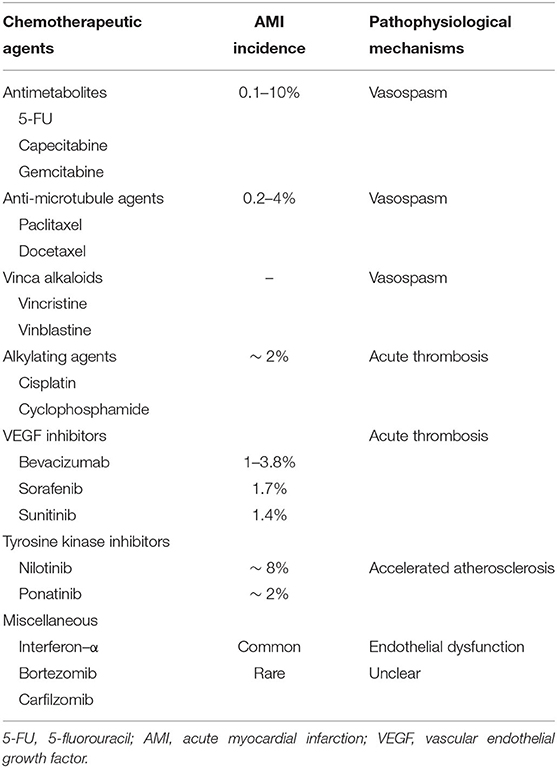
Table 1. Correlations among chemotherapy, AMI incidence, and pathophysiology.
Coronary vasoreactivity and consequently ACS presentations depend on the intensity and duration of vasoconstriction, and clinical manifestations vary from AMI to malignant ventricular arrhythmias (21). Among chemotherapeutic drugs, several have been listed as potential causes of coronary vasospasm, such as 5-fluorouracil (5-FU), capecitabine, paclitaxel, gemcitabine, rituximab and sorafenib (21).
Chemotherapy can precipitate type I AMI. Some drugs, such as cisplatin and vinca alkaloids, have a direct toxic effect on endothelial cells that predisposes them to the erosion and rupture of atherosclerotic plaques (21). Among cancer patients, several factors, such as infection and anaemia, induce tachycardia, which increases myocardial demand or the hypotension and hypoxaemia that reduce myocardial reserve (22). These imbalances between oxygen supply and consumption are substrates that cause type II AMI.
Fluoropyrimidines (5-FU and capecitabine) and anti-microtubule agents (taxanes and vinca alkaloids) are the classes of chemotherapies most related associated with acute vasospasm (23). Considering only documented myocardial ischaemia, the incidence in patients receiving 5-FU may be as high as 10% and is influenced by dose and the time of administration (21). Taxanes can cause myocardial ischaemia, with an incidence ranging from 0.2 to 4%, and preexisting CAD might be a risk factor (24, 25).
The regulation of coronary vascular tone depends on the vasodilators released by the endothelium (26). However, the change in endothelial function does not seem to be the main cause of vasospasm mediated by 5-FU. The activation of intracellular signaling pathways that control vascular smooth muscle cell tone via protein kinase C mediated by 5-FU causes hyperreactivity and coronary spasm (21).
Myocardial ischaemia can manifest from asymptomatic ST segment changes on electrocardiography (ECG) through to angina or MI (23). Vasospasm tends to occur at sites of thrombus and plaque formation; thus, preexisting CAD remains a risk factor for 5-FU-related vasospastic angina. Other chemotherapies, such as bevacizumab, have a synergistic effect on vascular complications (23).
Cisplatin agents, vascular endothelial growth factor (VEGF) signaling pathway inhibitors and cyclophosphamide predispose patients to AMI due to acute thrombosis (21). Cisplatin and cyclophosphamide are alkylating agents used in several types of solid and haematological tumours (22).
Cisplatin treatment is associated with thromboembolic events. Among arterial events, the incidence of AMI was 1.18%. These events occur mainly in the first 100 days after starting treatment (27). In the 20-year follow-up of testicular cancer survivors, the risk of developing CAD among patients treated with RT and chemotherapy was 5.3 times greater than that in the surgical group. Among survivors, the incidence of all atherosclerotic events was 8.0%. Coronary events, including AMI and unstable angina, occurred in 5.6%, with the highest incidence in the chemotherapy and RT group (28). Gietema et al. demonstrated that cisplatin can be detected in the blood even after 10 years of treatment, which explains the greater risk of developing CAD (29).
A coronary thrombosis secondary to cisplatin is mediated by platelet aggregation. Cisplatin treatment stimulates von Willebrand factor production by the endothelium stimulating platelet aggregation. Other mechanisms influenced by cisplatin, such as increased tumour necrosis factors, the formation of free radicals and decreased prostacyclin synthesis, cause intravascular platelet aggregation and predispose patients to thrombosis (30). Other potential mechanisms of ACS in patients during cisplatin treatment are related to hypomagnesaemia, which increases intracellular calcium, causing vasoconstriction and myocardial ischaemia due to the precipitation of the coronary vasospasm (30).
VEGF is a ligand present in the cell membrane that regulates signaling pathways useful for endothelial function, such as proliferation, muscle relaxation by nitric oxide and resistance to stress-induced apoptosis (31). It is estimated that the incidence and risk of ischaemic heart disease among patients treated with bevacizumab was 1 and 2.49%, respectively (32). In metastatic cancer, bevacizumab increased incidence of arterial thromboembolic events from 1.7 to 3.8% (33). Ranpura et al. showed that bevacizumab increased the risk of cardiac ischaemic events by 2.14 times (34).
A recent meta-analysis including 10,255 patients demonstrated that the risk of arterial thrombotic events in patients treated with sunitinib and sorafenib was 3.03 times greater than that in the control group (35). The inhibition of VEGF signaling pathways induces cardiotoxicity through mechanisms such as endothelial dysfunction, procoagulant status and arterial thrombosis (22). A reduction in nitric oxide production results in vasoconstriction and platelet aggregation, contributing to arterial thrombotic events (34).
In chronic myeloid leukaemia, the translocation of the Bcr-Abl gene is responsible for the formation of the Philadelphia chromosome, and multitargeted TKIs act to inhibit this translocation. Nilotinib and ponatinib are second- and third- generation TKIs, respectively, and both are associated with accelerated atherosclerosis. The most common cardiovascular events during treatment include rapidly progressive peripheral arterial occlusive disease and acute ischaemic events. The accelerated atherosclerotic process generates plaques that may be responsible for coronary obliteration and cause AMI (21).
In one larger retrospective study involving 81 patients receiving nilotinib, the incidence of AMI was 7.5% (23). In the analysis of 82 patients treated with nilotinib, the cumulative incidence of atherosclerotic events at 48 months was 8.5%, which was higher among patients with elevated cardiovascular risk (36). In a study that evaluated the effectiveness of ponatinib in the treatment of CML, treatment-related adverse cardiovascular events were observed in 2% (37).
Bortezomib is one of the key components of therapy for patients with multiple myeloma, and the association of ischaemic heart disease with bortezomib is unclear. The inhibition of proteasome activity by bortezomib should contribute to myocardial ischaemia by reducing the proliferation of endothelial progenitor cells useful in angiogenesis and decreasing the production of NO. Bortezomib also causes atherosclerotic plaque instability due to increased apoptosis (38).
Interferon-α is used to treat leukaemia, lymphomas, and melanoma. The main cardiotoxicities include fluctuations in blood pressure, arrhythmias and ischaemia. Some authors have suggested that the incidence of myocardial ischaemia induced by interferon-α is similar to that of 5-FU (39, 40).
Radiotherapy, especially supradiaphragmatic radiotherapy, may be associated with a higher incidence of myocardial ischaemia. Pathophysiological mechanisms include endothelial injury, thrombosis and plaque rupture (22). In a 5-year assessment Hodgkin lymphoma (HL) survivors, the cumulative incidence of coronary heart disease was directly proportional to the dose of radiotherapy that the heart was exposed to (41). Another trial showed that a cumulative incidence of CVD up to 50% in long-term follow-up of HL survivors (42). A retrospective cohort study showed that patients with breast cancer and CAD undergoing radiotherapy had a 1.49-fold higher incidence of ACS (43).
Patients with active hematologic malignancies usually present several conditions that difficult the management of ACS, such as: thrombocytosis, thrombocytopenia, anaemia, infection, renal and hepatic dysfunction, bleeding and thrombosis. The incidence ACS in hospitalized patients with active lymphoma or leukaemia range from 1.4 to 11.2% (44, 45).
In a retrospective analysis, Park et al. observed that cardiovascular risk factors were common in patients who developed ACS with active hematologic malignancies (45). In this cohort, most patients present complex coronary artery disease with coronary angiography showed intracoronary thrombus (33%), severe coronary artery disease (50%), and mild or moderate coronary artery disease (16.7%)(45). Despite the diagnosis of ACS, only half of patients received antiplatelet, anticoagulant and/or statin therapy. The use was extremely low in those not referred to the catheterization. When we applied the criteria of platelet count of 10,000 for aspirin and 30,000 for DAPT, only 58 and 27% of eligible patients received these therapies (45, 46). A multidisciplinary approach is often necessary to reinforce the importance of following the recommendations of the guidelines and to avoid unnecessary/prolonged chemotherapy interruptions.
Cancer patients present several challenges when they are admitted with acute coronary syndrome. They are generally older and have more comorbidities and a greater extent of coronary disease. In addition, as mentioned above, haematological, and blood coagulation changes require good planning of clinical and interventional treatment when indicated (8). It is important to have a multidisciplinary approach balancing the risks of ischaemic and haemorrhagic events with cancer risk.
Malignancy is considered an independent predictor of increased risk of repeated revascularization and intrastent thrombosis in patients with prior percutaneous coronary intervention (PCI)(8). Moreover, it has been shown that there is a higher atherosclerotic burden (as assessed by a higher SYNTAX score) with a high prevalence of complex lesions frequently located in the proximal segments of the coronary tree (47, 48). Figure 1 summarizes the risk factors, pathophysiology and therapeutic management of ACS in cancer patients.
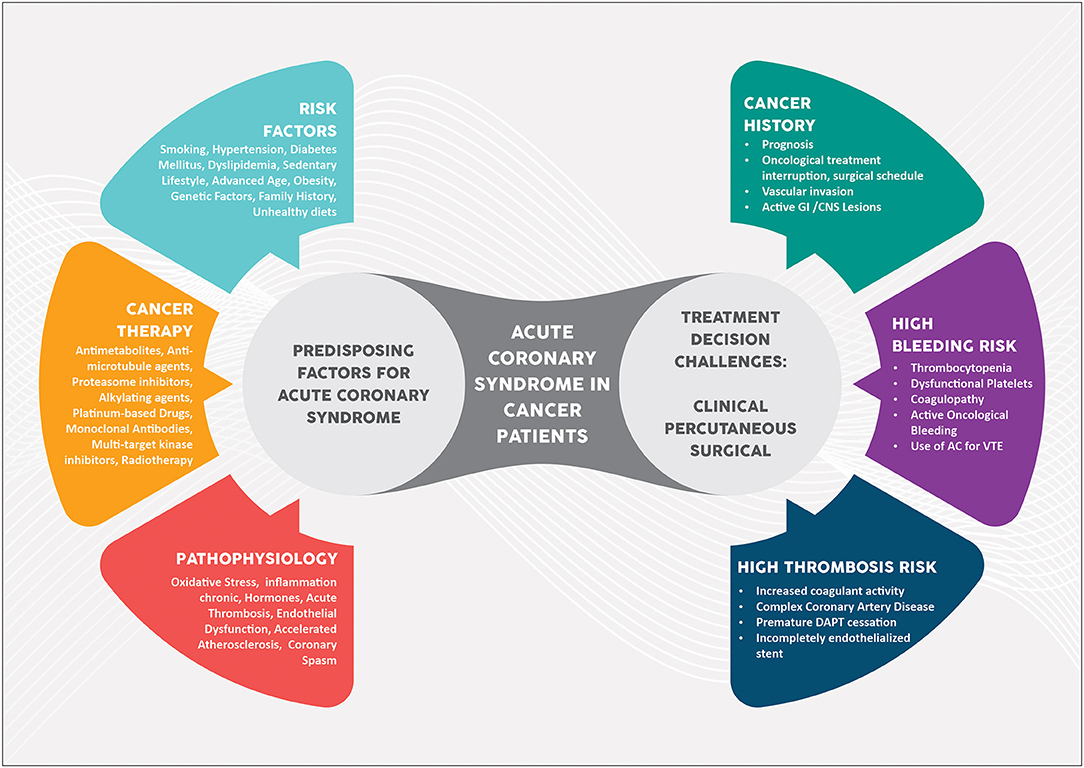
Figure 1. Central illustration. Acute coronary syndrome in cancer patients. AC, anticoagulation; CNS, central nervous system; DAPT, dual antiplatelet therapy, GI, gastrointestinal; VTE, venous thromboembolism.
There is considerable debate with regard to optimal medical therapy limitations in cancer patients suffering from ACS. Current medical guidelines favour a case-based approach (22). Balancing between bleeding and thrombotic risk is key to achieving the best clinical outcomes. A landmark study from the US National Inpatient Sample (NIS) database has made clear that cancer patients with ACS were frequently treated non-invasively despite worse outcomes than when an invasive strategy was used (8).
The coexistence of a thrombotic milieu and thrombocytopaenia offers a good practical view of the dilemma posed in this high-risk group of patients. A well-designed retrospective study on haematologic patients made the case for a reviewed contraindication for the use of aspirin. Patients with severe thrombocytopaenia (defined < 50.000) who received aspirin for ACS had improved survival compared with those who did not (92 vs. 70% at 7 days, 72 vs. 33% at 30 days, and 32 vs. 13% at 1 year; log rank p = 0.008). The mean platelet count was 31.000 ± 12.000. It is important to mention that these individuals did not have active bleeding (49).
Current guidelines are not unanimous in terms of the timing of DAPT and DAPT schemes for cancer patients (46, 50–53). A multidisciplinary approach (cardiologist, cardiac surgeon, interventional cardiologist, oncologist and haematologist) should be considered for the choice of an individualized treatment. The main problem in deciding the antiplatelet regimen is the lack of data to guide decisions on the type and duration of DAPT given the omission of cancer patients from most randomised trials. Furthermore, cancer is not a variable considered in DAPT prediction models (PRECISE-DAPT and DAPT scores)(50). Most recommendations consider cancer patients to be at a high risk of bleeding but do not consider their higher risk of ischaemic events. More recently, trials on antiplatelet monotherapy have shown favourable clinical outcomes in PCI patients (54–56). This may be an appealing approach for CAD in oncologic patients but requires proper validation in this population.
Importantly, compared with patients with stable CAD, patients with ACS are at increased thrombotic risk, warranting treatment with more potent, longer-duration antiplatelet therapy (51). The prescription of more potent platelet inhibitors, in addition to aspirin, in cancer patients suffering from myocardial infarction, was addressed in the Bern PCI Registry; in addition to them being less frequently prescribed (Cancer 30.6%vs No Cancer 41.6%; p < 0.001), there was not an association with increase in bleeding outcomes (57). Figure 2 provides a summary of the recommendations on DAPT schemes and duration according to the bleeding risk in ACS patients.
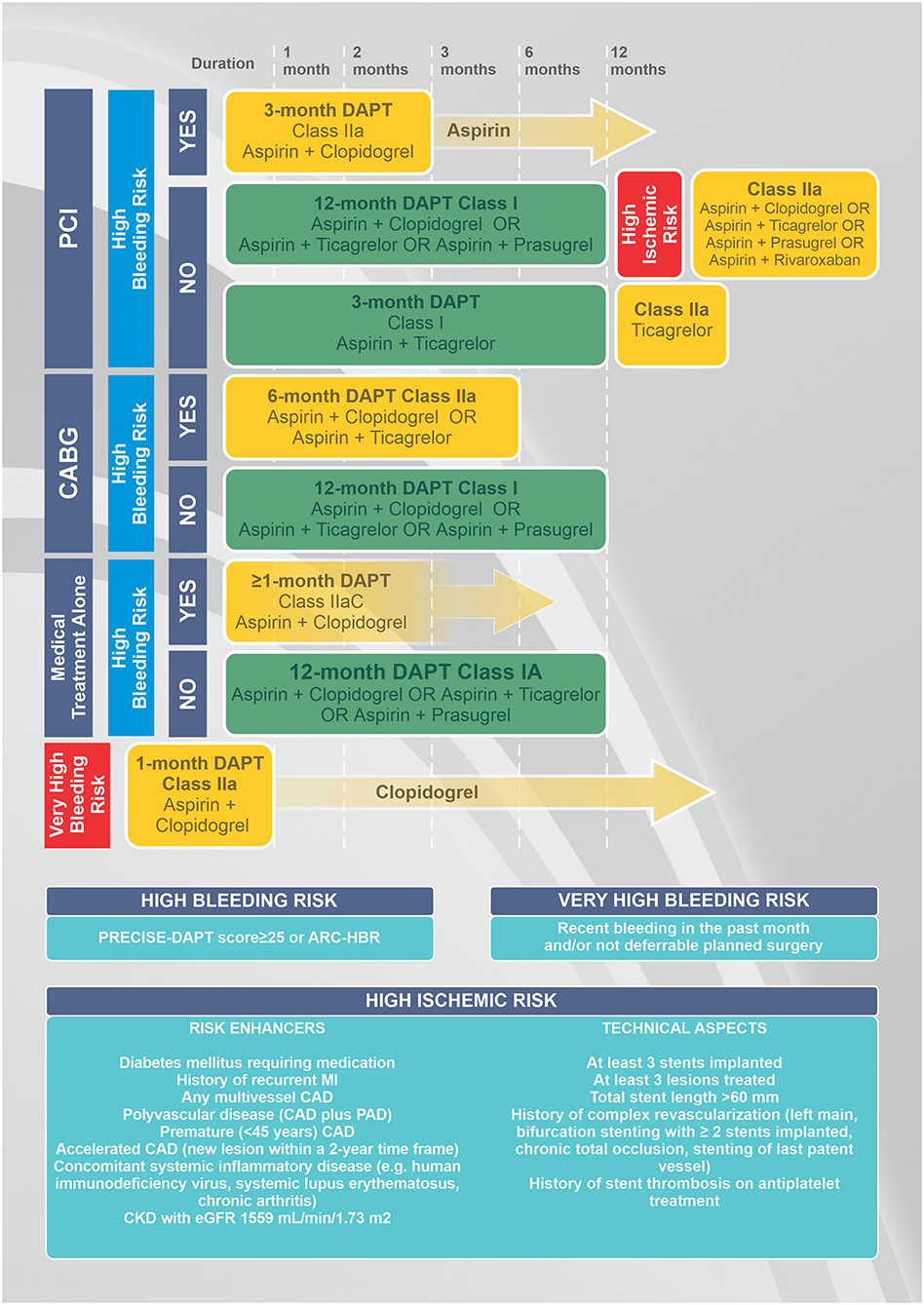
Figure 2. Algorithm for a dual antiplatlet therapy (DAPT) scheme and timing in patients with acute coronary syndrome according to the treatment and bleeding risk. PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting surgery; ARC-HBR, Academic Research Consortium High Bleeding Risk; PRECISE-DAPT, PREdicting bleeding Complications In patients undergoing Stent implantation and subsEquent Dual Anti Platelet Therapy; CAD, coronary artery disease; PAD, peripheral artery disease. Modified from Valgimigli et al. (50), Costa et al. (60), Collet et al. (65).
Currently, there are no randomised clinical studies that have evaluated the risks and benefits of clinical and interventional treatments in patients with cancer presenting with acute coronary syndromes. These patients are frequently excluded from clinical trials.
It has been shown that patients diagnosed with active cancer have lower rates of invasive management in ACS (coronary angiography, PCI and coronary artery bypass surgery) than patients without active cancer (8). The decision between CABG and PCI should take into account the coronary anatomical complexity, ability to provide complete coronary revascularization, need for an oncological surgery, and bleeding risk (including DAPT).
PCI is currently considered the most common type of coronary revascularization, especially in the context of ACS (8). It is the gold standard treatment for ST segment elevation acute myocardial infarction and is recommended over fibrinolysis within proper timeframes (58). For patients with refractory ischaemia, malignant arrythmias and favourable anatomy, PCI is also the therapy of choice most of the time because of the ability to reestablish coronary flow (58). For patients with more stable ACS, PCI still is a less invasive strategy and may be attractive for patients with ACS and systemic manifestations of cancer. Some anatomical factors may increase the odds of ischaemic events in patients undergoing PCI, such as three vessel disease, bifurcation with 2 stents, total stent length >60 mm, left main bifurcation PCI, saphenous graft PCI, and inability to provide complete revascularization (46, 50, 51, 53, 59–61). Another factor that must be taken into account is that the use of DAPT after PCI may postpone invasive procedures to treat cancer.
Traditionally, most of cancer patients were treated with bare-metal stents (BMS) due to concern for increased bleeding risk and expectant need for cancer-directed surgery. However, cancer patients usually present several risk factors for restenosis and stent thrombosis, such as diabetes, smoking and chronic inflammatory state. The drug-eluting stents (DES) have proven to reduce the risk of restenosis and stent thrombosis as compared with BMS. And, the newer-generation stent technology demonstrates the efficacy and safe of shorter duration of DAPT treatment. Thus, the current recommendation is that the DES is the stent of choice for cancer patients (62).
In cases of thrombocytopaenia secondary to cancer, careful vascular access and haemostasis (post-procedure) ensures greater safety and a lower incidence of adverse outcomes. There is no absolute platelet count that is a contraindication for cardiac catheterisation. Some well-established protocols recommend that this number should be at least 40,000 (so most interventional procedures are performed safely and without blood clotting abnormalities). When this count is below 50,000, a lower dose of unfractionated heparin (between 30 and 50 U/kg) may be considered, with the use of additional heparin if the ACT is below 250 s. The usual dose is 50–70 U/kg (46).
In the ACS setting, the use of the radial artery should be prioritized as the access site for PCI (Class I) (58). It has been demonstrated that, compared with transfemoral PCI, transradial PCI produces a clear reduction in adverse clinical outcomes, mainly driven by bleeding-related events. As cancer patients are considered to be at a high bleeding risk, radial access has the potential to be even more beneficial.
Intravascular imaging (intravascular ultrasound and optical coherence tomography) should be used to optimize stent implantation, assuring adequate stent expansion, apposition and a lack of edge dissection (46).
Overall, CABG should be the preferred strategy for coronary revascularization for patients with complex multivessel coronary artery disease (63). In a recent study, Guha et al. evaluated CABG in cancer patients, and they observed that although the number of surgical procedures has decreased in recent years, the proportion of cancer patients who have undergone these procedures has increased (7 vs. 12.6%) (64). Surgical results are similar in cancer patients and patients without cancer, with similar mortality rates (0.9 vs. 1%), despite increased major bleeding (4.5 vs. 15.3%), and stroke (0.9 vs. 1.5%)(64).
For patients with cancer, it is important to discuss hybrid surgical procedures, staged or simultaneous coronary artery bypass grafting (CABG) and tumour resection. The best timing, strategy and possibility to use cardiopulmonary bypass are still under scientific discussion.
Acute coronary syndrome in cancer patients is a frequent complication during the course of the disease and remains an important cause of mortality in these patients. Understanding the oncology history and therapy and estimating the embolic and bleeding risks are essential for proper management. The individualisation of treatment and a multidisciplinary approach are essential for a successful outcome.
LH, IC, and CC conducted the study conceptualisation, writing and review of the manuscript. FA, DC, VS, and MC participated in the writing and reviewing of the manuscript. All authors have read and approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ryan TD, Nagarajan R, Godown J. Cardiovascular toxicities in pediatric cancer survivors. Cardiol Clin. (2019) 37:533–44. doi: 10.1016/j.ccl.2019.07.002
2. Bradshaw PT, Stevens J, Khankari N, Teitelbaum SL, Neugut AI, Gammon MD. Cardiovascular disease mortality among breast cancer survivors. Epidemiology. (2016) 27:6–13. doi: 10.1097/EDE.0000000000000394
3. Lenneman CG, Sawyer DB. Cardio-oncology: an update on cardiotoxicity of cancer-related treatment. Circ Res. (2016) 118:1008–20. doi: 10.1161/CIRCRESAHA.115.303633
4. Yusuf SW, Daraban N, Abbasi N, Lei X, Durand JB, Daher IN. Treatment and outcomes of acute coronary syndrome in the cancer population. Clin Cardiol. (2012) 35:443–50. doi: 10.1002/clc.22007
5. Canale ML, Bisceglia I, Lestuzzi C, Parrini I, Force AC-OT. Arterial thrombosis in cancer: spotlight on the neglected vessels. Anticancer Res. (2019) 39:4619–25. doi: 10.21873/anticanres.13642
6. Young A, Chapman O, Connor C, Poole C, Rose P, Kakkar AK. Thrombosis and cancer. Nat Rev Clin Oncol. (2012) 9:437–49. doi: 10.1038/nrclinonc.2012.106
7. Narayan V, Ky B. Common cardiovascular complications of cancer therapy: epidemiology, risk prediction, and prevention. Annual Review Med. (2018) 69:97–111. doi: 10.1146/annurev-med-041316-090622
8. Bharadwaj A, Potts J, Mohamed MO, Parwani P, Swamy P, Lopez-Mattei JC, et al. Acute myocardial infarction treatments and outcomes in 6.5 million patients with a current or historical diagnosis of cancer in the USA. Eur Heart J. (2020) 41:2183–93. doi: 10.1093/eurheartj/ehz851
9. Landes U, Kornowski R, Bental T, Assali A, Vaknin-Assa H, Lev E, et al. Long-term outcomes after percutaneous coronary interventions in cancer survivors. Coronary Artery Dis. (2017) 28:5–10. doi: 10.1097/MCA.0000000000000429
10. Nakatsuma K, Shiomi H, Morimoto T, Watanabe H, Nakagawa Y, Furukawa Y, et al. Influence of a history of cancer on long-term cardiovascular outcomes after coronary stent implantation (an Observation from Coronary Revascularization Demonstrating Outcome Study-Kyoto Registry Cohort-2). Eur Heart J Quality Care Clin Outcomes. (2018) 4:200–7. doi: 10.1093/ehjqcco/qcy014
11. Mercurio V, Cuomo A, Cadeddu Dessalvi C, Deidda M, Di Lisi D, Novo G, et al. Redox imbalances in ageing and metabolic alterations: implications in cancer and cardiac diseases. An Overview from the Working Group of Cardiotoxicity and Cardioprotection of the Italian Society of Cardiology (SIC). Antioxidants. (2020) 9:641. doi: 10.3390/antiox9070641
12. Tuzovic M, Herrmann J, Iliescu C, Marmagkiolis K, Ziaeian B, Yang EH. Arterial thrombosis in patients with cancer. Curr Treat Options Cardiovasc Med. (2018) 20:40. doi: 10.1007/s11936-018-0635-x
13. Lee AY, Levine MN. Venous thromboembolism and cancer: risks and outcomes. Circulation. (2003) 107(23 Suppl. 1):I17–21. doi: 10.1161/01.CIR.0000078466.72504.AC
14. Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM, Elkind MSV, et al. Risk of arterial thromboembolism in patients with cancer. J Am Coll Cardiol. (2017) 70:926–38. doi: 10.1016/j.jacc.2017.06.047
15. Brenner B, Bikdeli B, Tzoran I, Madridano O, Lopez-Reyes R, Surinach JM, et al. Arterial ischemic events are a major complication in cancer patients with venous thromboembolism. Am J Med. (2018) 131:1095–103. doi: 10.1016/j.amjmed.2018.04.037
16. Falanga A, Schieppati F, Russo L. Pathophysiology 1. Mechanisms of thrombosis in cancer patients. Cancer Treatment Res. (2019) 179:11–36. doi: 10.1007/978-3-030-20315-3_2
17. Long M, Ye Z, Zheng J, Chen W, Li L. Dual anti-platelet therapy following percutaneous coronary intervention in a population of patients with thrombocytopenia at baseline: a meta-analysis. BMC Pharmacol Toxicol. (2020) 21:31. doi: 10.1186/s40360-020-00409-2
18. Flack KF, Desai J, Kolb JM, Chatterjee P, Wallentin LC, Ezekowitz M, et al. Major gastrointestinal bleeding often is caused by occult malignancy in patients receiving warfarin or dabigatran to prevent stroke and systemic embolism from atrial fibrillation. Clin Gastroenterol Hepatol. (2017) 15:682–90. doi: 10.1016/j.cgh.2016.10.011
19. Zwicker JI, Karp Leaf R, Carrier M. A meta-analysis of intracranial hemorrhage in patients with brain tumors receiving therapeutic anticoagulation. J Thromb Haemost. (2016) 14:1736–40. doi: 10.1111/jth.13387
20. Ozaki T, Chiba S, Annen K, Kawamukai Y, Kohno N, Horimoto M. Acute coronary syndrome due to coronary artery compression by a metastatic cardiac tumor. J Cardiol Cases. (2010) 1:e52–5. doi: 10.1016/j.jccase.2009.07.005
21. Herrmann J, Yang EH, Iliescu CA, Cilingiroglu M, Charitakis K, Hakeem A, et al. Vascular toxicities of cancer therapies: the old and the new–an evolving avenue. Circulation. (2016) 133:1272–89. doi: 10.1161/CIRCULATIONAHA.115.018347
22. Zamorano JL, Lancellotti P, Rodriguez Munoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: the Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. (2016) 37:2768–801. doi: 10.1093/eurheartj/ehw211
23. Yetis Sayin B, Oto MA. Acute coronary syndrome in cancer patients. Am J Cardiovasc Drugs. (2018) 18:361–72. doi: 10.1007/s40256-018-0286-z
24. Rowinsky EK, McGuire WP, Guarnieri T, Fisherman JS, Christian MC, Donehower RC. Cardiac disturbances during the administration of taxol. J Clin Oncol. (1991) 9:1704–12. doi: 10.1200/JCO.1991.9.9.1704
25. Shah K, Gupta S, Ghosh J, Bajpai J, Maheshwari A. Acute non-ST elevation myocardial infarction following paclitaxel administration for ovarian carcinoma: a case report and review of literature. J Cancer Res Ther. (2012) 8:442–4. doi: 10.4103/0973-1482.103530
26. Lanza GA, Careri G, Crea F. Mechanisms of coronary artery spasm. Circulation. (2011) 124:1774–82. doi: 10.1161/CIRCULATIONAHA.111.037283
27. Moore RA, Adel N, Riedel E, Bhutani M, Feldman DR, Tabbara NE, et al. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: a large retrospective analysis. J Clin Oncol. (2011) 29:3466–73. doi: 10.1200/JCO.2011.35.5669
28. Haugnes HS, Wethal T, Aass N, Dahl O, Klepp O, Langberg CW, et al. Cardiovascular risk factors and morbidity in long-term survivors of testicular cancer: a 20-year follow-up study. J Clin Oncol. (2010) 28:4649–57. doi: 10.1200/JCO.2010.29.9362
29. Gietema JA, Meinardi MT, Messerschmidt J, Gelevert T, Alt F, Uges DR, et al. Circulating plasma platinum more than 10 years after cisplatin treatment for testicular cancer. Lancet. (2000) 355:1075–6. doi: 10.1016/S0140-6736(00)02044-4
30. Jafri M, Protheroe A. Cisplatin-associated thrombosis. Anticancer Drugs. (2008) 19:927–9. doi: 10.1097/CAD.0b013e3283100e9c
31. Snider KL, Maitland ML. Cardiovascular toxicities: clues to optimal administration of vascular endothelial growth factor signaling pathway inhibitors. Target Oncol. (2009) 4:67–76. doi: 10.1007/s11523-009-0106-0
32. Chen XL, Lei YH, Liu CF, Yang QF, Zuo PY, Liu CY, et al. Angiogenesis inhibitor bevacizumab increases the risk of ischemic heart disease associated with chemotherapy: a meta-analysis. PLoS ONE. (2013) 8:e66721. doi: 10.1371/journal.pone.0066721
33. Scappaticci FA, Skillings JR, Holden SN, Gerber HP, Miller K, Kabbinavar F, et al. Arterial thromboembolic events in patients with metastatic carcinoma treated with chemotherapy and bevacizumab. J Natl Cancer Inst. (2007) 99:1232–9. doi: 10.1093/jnci/djm086
34. Ranpura V, Hapani S, Chuang J, Wu S. Risk of cardiac ischemia and arterial thromboembolic events with the angiogenesis inhibitor bevacizumab in cancer patients: a meta-analysis of randomized controlled trials. Acta Oncol. (2010) 49:287–97. doi: 10.3109/02841860903524396
35. Choueiri TK, Schutz FA, Je Y, Rosenberg JE, Bellmunt J. Risk of arterial thromboembolic events with sunitinib and sorafenib: a systematic review and meta-analysis of clinical trials. J Clin Oncol. (2010) 28:2280–5. doi: 10.1200/JCO.2009.27.2757
36. Breccia M, Colafigli G, Molica M, Alimena G. Cardiovascular risk assessments in chronic myeloid leukemia allow identification of patients at high risk of cardiovascular events during treatment with nilotinib. Am J Hematol. (2015) 90:E100–1. doi: 10.1002/ajh.23976
37. Cortes JE, Kim DW, Pinilla-Ibarz J, le Coutre P, Paquette R, Chuah C, et al. A phase 2 trial of ponatinib in Philadelphia chromosome-positive leukemias. N Engl J Med. (2013) 369:1783–96. doi: 10.1056/NEJMoa1306494
38. Takamatsu H, Yamashita T, Kotani T, Sawazaki A, Okumura H, Nakao S. Ischemic heart disease associated with bortezomib treatment combined with dexamethasone in a patient with multiple myeloma. Int J Hematol. (2010) 91:903–6. doi: 10.1007/s12185-010-0586-9
39. Teragawa H, Hondo T, Amano H, Hino F, Ohbayashi M. Adverse effects of interferon on the cardiovascular system in patients with chronic hepatitis C. Jpn Heart J. (1996) 37:905–15. doi: 10.1536/ihj.37.905
40. Senkus E, Jassem J. Cardiovascular effects of systemic cancer treatment. Cancer Treat Rev. (2011) 37:300–11. doi: 10.1016/j.ctrv.2010.11.001
41. van Nimwegen FA, Schaapveld M, Cutter DJ, Janus CP, Krol AD, Hauptmann M, et al. Radiation dose-response relationship for risk of coronary heart disease in survivors of hodgkin lymphoma. J Clin Oncol. (2016) 34:235–43. doi: 10.1200/JCO.2015.63.4444
42. van Nimwegen FA, Schaapveld M, Janus CP, Krol AD, Petersen EJ, Raemaekers JM, et al. Cardiovascular disease after Hodgkin lymphoma treatment: 40-year disease risk. JAMA Intern Med. (2015) 175:1007–17. doi: 10.1001/jamainternmed.2015.1180
43. Lee YC, Chuang JP, Hsieh PC, Chiou MJ, Li CY. A higher incidence rate of acute coronary syndrome following radiation therapy in patients with breast cancer and a history of coronary artery diseases. Breast Cancer Res Treat. (2015) 152:429–35. doi: 10.1007/s10549-015-3481-5
44. Maynard C, Lowy E, Rumsfeld J, Sales AE, Sun H, Kopjar B, et al. The prevalence and outcomes of in-hospital acute myocardial infarction in the department of veterans affairs health system. Arch Intern Med. (2006) 166:1410–6. doi: 10.1001/archinte.166.13.1410
45. Park JY, Guo W, Al-Hijji M, El Sabbagh A, Begna KH, Habermann TM, et al. Acute coronary syndromes in patients with active hematologic malignancies - Incidence, management, and outcomes. Int J Cardiol. (2019) 275:6–12. doi: 10.1016/j.ijcard.2018.10.008
46. Iliescu CA, Grines CL, Herrmann J, Yang EH, Cilingiroglu M, Charitakis K, et al. SCAI Expert consensus statement: evaluation, management, and special considerations of cardio-oncology patients in the cardiac catheterization laboratory (endorsed by the cardiological society of india, and sociedad Latino Americana de Cardiologia intervencionista). Catheter Cardiovasc Interv. (2016) 87:E202–23. doi: 10.1002/ccd.26379
47. Seleme VB CC, Bispo I, Borges DC, Bittar CS, Carolina C, Fonseca S, et al. Oncologic patients presenting acute coronary syndromes have high atherosclerotic burden, complex anatomical plaques and particular plaque rupture distribution. Circulation. (2019) 2019:A11931.
48. Yang Q, Chen Y, Gao H, Zhang J, Zhang J, Zhang M, et al. Chemotherapy-related anatomical coronary-artery disease in lung cancer patients evaluated by coronary-angiography SYNTAX score. Arq Bras Cardiol. (2020). 114:1004–12. doi: 10.36660/abc.20190201
49. Feher A, Kampaktsis PN, Parameswaran R, Stein EM, Steingart R, Gupta D. Aspirin is associated with improved survival in severely thrombocytopenic cancer patients with acute myocardial infarction. Oncologist. (2017) 22:213–21. doi: 10.1634/theoncologist.2016-0110
50. Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2018) 39:213–60. doi: 10.1093/eurheartj/ehx419
51. Urban P, Mehran R, Colleran R, Angiolillo DJ, Byrne RA, Capodanno D, et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention. Circulation. (2019) 140:240–61. doi: 10.1161/CIRCULATIONAHA.119.040167
52. Capodanno D, Alfonso F, Levine GN, Valgimigli M, Angiolillo DJ. ACC/AHA versus esc guidelines on dual antiplatelet therapy: JACC guideline comparison. J Am Coll Cardiol. (2018) 72(23 Pt A):2915–31. doi: 10.1016/j.jacc.2018.09.057
53. Levine GN, Bates ER, Bittl JA, Brindis RG, Fihn SD, Fleisher LA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention, 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery, 2012 ACC/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease, 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction, 2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes, and 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery. Circulation. (2016) 134:e123–55. doi: 10.1161/CIR.0000000000000452
54. Vranckx P, Valgimigli M, Juni P, Hamm C, Steg PG, Heg D, et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: a multicentre, open-label, randomised superiority trial. Lancet. (2018) 392:940–9.
55. Mehran R, Baber U, Sharma SK, Cohen DJ, Angiolillo DJ, Briguori C, et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N Engl J Med. (2019) 381:2032–42. doi: 10.1056/NEJMoa1908419
56. Kogame N, Modolo R, Tomaniak M, Cavalcante R, de Martino F, Tinoco J, et al. Prasugrel monotherapy after PCI with the SYNERGY stent in patients with chronic stable angina or stabilised acute coronary syndromes: rationale and design of the ASET pilot study. EuroIntervention. (2019) 15:e547–e50. doi: 10.4244/EIJ-D-19-00131
57. Ueki Y, Vogeli B, Karagiannis A, Zanchin T, Zanchin C, Rhyner D, et al. Ischemia and bleeding in cancer patients undergoing percutaneous coronary intervention. JACC. (2019) 1:145–55. doi: 10.1016/j.jaccao.2019.11.001
58. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. (2017). ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018). 39:119-77.
59. Rhee TM, Park KW, Kim CH, Kang J, Han JK, Yang HM, et al. Dual antiplatelet therapy duration determines outcome after 2- but not 1-stent strategy in left main bifurcation percutaneous coronary intervention. JACC Cardiovasc Interv. (2018) 11:2453–63. doi: 10.1016/j.jcin.2018.09.020
60. Costa F, Van Klaveren D, Feres F, James S, Raber L, Pilgrim T, et al. Dual antiplatelet therapy duration based on ischemic and bleeding risks after coronary stenting. J Am Coll Cardiol. (2019) 73:741–54. doi: 10.1016/j.jacc.2018.11.048
61. Genereux P, Campos CM, Yadav M, Palmerini T, Caixeta A, Xu K, et al. Reasonable incomplete revascularisation after percutaneous coronary intervention: the SYNTAX revascularisation index. EuroIntervention. (2015) 11:634–42. doi: 10.4244/EIJY14M10_05
62. Ganatra S, Sharma A, Levy MS. Re-Evaluating the safety of drug-eluting stents in cancer patients. JACC Cardiovasc Interv. (2017) 10:2334–7. doi: 10.1016/j.jcin.2017.06.068
63. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention. (2019) 14:1435–534. doi: 10.4244/EIJY19M01_01
64. Guha A, Dey AK, Kalra A, Gumina R, Lustberg M, Lavie CJ, et al. Coronary artery bypass grafting in cancer patients: prevalence and outcomes in the United States. Mayo Clin Proc. (2020) 95:1865–76. doi: 10.1016/j.mayocp.2020.05.044
Keywords: acute coronary syndrome, cancer, cardiotoxicity, coronary disease, cardio oncology
Citation: Costa IBSdS, Andrade FTdA, Carter D, Seleme VB, Costa MS, Campos CM and Hajjar LA (2021) Challenges and Management of Acute Coronary Syndrome in Cancer Patients. Front. Cardiovasc. Med. 8:590016. doi: 10.3389/fcvm.2021.590016
Received: 31 July 2020; Accepted: 20 April 2021;
Published: 09 June 2021.
Edited by:
Reto Asmis, Wake Forest School of Medicine, United StatesReviewed by:
Sherry-Ann Brown, Mayo Clinic, United StatesCopyright © 2021 Costa, Andrade, Carter, Seleme, Costa, Campos and Hajjar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos M. Campos, Y2FybG9zYWNhbXBvczFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.