 Jorunn Bjerkan
Jorunn Bjerkan Victor Valderaune3,4
Victor Valderaune3,4 Rose Mari Olsen
Rose Mari Olsen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Comput. Sci., 01 June 2021
Sec. Digital Public Health
Volume 3 - 2021 | https://doi.org/10.3389/fcomp.2021.624555
This article is part of the Research TopicPersonalized Digital Health and Patient-Centric ServicesView all 21 articles
Background: Although access to accurate patient documentation is recognized as a prerequisite for delivering of safe and continuous municipal elderly care, healthcare professionals often fail to provide comprehensive clinical information in an accurate and timely manner. The aim of this study was to understand the perceptions of healthcare professionals and healthcare students regarding existing barriers to patient safety through the performance of documentation practices.
Methods: Using a qualitative, exploratory design, this study conducted six focus group interviews with nurses and social educators (n = 12) involved in primary care practice and nursing and social educator bachelor’s degree students from a University College (n = 11). Data were analyzed using qualitative content analysis.
Results: Four themes emerged from the analysis, which described barriers to patient safety and quality in documentation practices: “Individual factors,” “Social factors,” “Organizational factors,” and “Technological factors.” Each theme also included several sub-themes.
Conclusion: According to the findings, several barriers negatively influenced documentation practices and information exchange, which may place primary care patients in a vulnerable and exposed situation. To achieve successful documentation, increased awareness and efforts by the individual professional are necessary. However, primary care services must facilitate the achievement of these goals by providing adequate resources, clear mission statements, and understandable policies.
High-quality patient documentation in primary care is crucial for ensuring the quality of care, continuity of care, and patient safety. For many years, the quality of nursing documentation has been reported as inadequate (Hellesø and Ruland, 2001; Blair and Smith, 2012; Akhu-Zaheya et al., 2018). Thus, knowledge about primary care staff perceptions of barriers to documenting in electronic health records is necessary to ensure patient safety in the services.
The elderly population is expected to grow in both European and American countries in the near future, which will be accompanied by increased demand for elderly healthcare services. This growing patient population will require both complex medical treatment and nursing care (Ministry of Health and Care Services, 2012; Kulik et al., 2014). To ensure the effective use of healthcare resources and improve patient outcomes, many Western countries are attempting to transfer responsibilities from specialist care to primary care. This change has resulted in patients who are treated in municipalities being frailer and presenting with more advanced, complex, and treatment-demanding issues (Gautun and Syse, 2017; Næss et al., 2017). In Norway, we have enacted “the Coordination reform” (Ministry of Health and Care Services, 2009), a collaborative model for the provision of care services between hospital care and primary care, which is similar to the international concept of “integrated care” (Ahgren, 2014; Ferrer and Goodwin, 2014). The implementation of such increased and formalized coordination strategies represents a political focus as a potential tool for ensuring the efficacy and safety of elderly care.
This increased complexity in primary care nursing requires awareness and a focus on providing appropriate nursing-supportive tools, such as high-quality electronic patient records (EPRs) as a main tool for nursing documentation practices. The provision of sufficient documentation of healthcare associated with the patients’ physical and mental health issues is particularly important among elderly patients because even minor changes in health status could be symptoms of severe or acute illnesses (Gray et al., 2002; Chong and Street, 2008; Cerejeira and Mukaetova-Ladinska, 2011). Any lapse in mental or physical health requires specific medical, nursing, and caring actions to be taken (Marengoni et al., 2011).
The implementation of EPR as a tool for documenting healthcare has resulted in major changes and increased requirements for nursing documentation (Ammenwerth et al., 2003). EPR implementation was intended to replace handwritten documentation practice and improve documentation structures to promote increased standardization (Hellesø and Ruland, 2001). In Norway, nursing homes and community care document care electronically use one of only three EPR systems (The Norwegian Directorate of eHealth, 2018). The EPR documentation practice consists typically of income notes, patient mapping, nursing actions, daily notes and -evaluation as well as discharge notes. E-messaging modules, medication, and collaboration with other professionals such as doctors and physiotherapists are included and used as well. In any case, to complete the documentation requirements, there seems to be a need for paper-based supportive systems, which tend to involve checklists, calendars, books, and post-it notes (Keenan et al., 2013). Nursing procedures and other supportive systems, such as tools for reporting adverse events, are either included in the chosen EPR system or solved in external systems. This study addresses this broad documentation practice.
Both legislation and practice for nursing documentation in healthcare services vary among countries; however, primary care nurses occupy a unique position within healthcare structures worldwide. Primary care nurses often work with few other nurses in primary care wards, or they meet patients alone at the patients’ homes. Therefore, they are often required to assess and evaluate patients, acting independently of other colleagues. Home-health nurses might not have access to online EPRs, which would allow for them to consult previous nursing interventions and evaluations, and they must perform their own documentation, which they may be unable to do until they return to the home care center office (Olsen et al., 2013).
Even though EPR was implemented over a decade ago and is widely used in primary care in Norwegian municipalities, healthcare services continue to face documentation challenges that result in adverse events. Studies have shown that primary care employees often struggle to coordinate patient information in the EPRs (Gehring et al., 2012; Melby et al., 2018), and primary healthcare documentation continues to be both incomplete and inaccurate (Tuinman et al., 2017; Moldskred et al., 2020).
Patient safety and EPR documentation tasks are closely connected. Documentation in EPR is important to ensure continuity, quality, and safety of patient care. EPRs represent a communicative and collaborative tool, in addition to serving as the written record for which actions have been implemented.
Various definitions of patient safety have emerged over time (Mitchell, 2008), including:
Patient safety is a discipline in the health care sector that applies safety science methods toward the goal of achieving a trustworthy system of health care delivery. Patient safety is also an attribute of health care systems; it minimizes the incidence and impact of, and maximizes recovery from, adverse events (Emanuel et al., 2008, p. 16).
The World Health Organization (WHO) vision for patient safety is “A world where every patient receives safe healthcare, without risks and harm, every time, everywhere” (WHO, 2017, p. 4). In this vision, it is stated that, until recently, patient safety research has primarily focused on the hospital setting rather than primary care. The WHO strategy “Safer primary care” focuses on nine improvement areas: patient engagement, education and training, human factors, administrative errors, diagnostic errors, medication errors, multimorbidity, transitions of care, and electronic tools (WHO, 2012). These focus areas are all relevant to the context of patient safety and documentation.
Elderly patients often suffer from comorbidities, which require complex and tight regimes of treatment and care (Marengoni et al., 2011). Meeting this demand requires high-quality nursing homes and ambulant healthcare services capable of working among elderly patients outside of hospital settings. The coordination of treatment and care, documentation, and patient information exchange represent particular challenges, and these areas have been characterized as being of particular risk for adverse events (Olsen et al., 2012; Blais et al., 2013; Olsen et al., 2013; Gjevjon 2014; Wekre, 2014).
Patient safety can be evaluated by mapping adverse events that occur in healthcare units. Studies have shown that 1–24 adverse incidents occur during every 100 consultations in the primary care context (Panesar et al., 2015). A link between patient safety and inadequate documentation has previously been reported by studies examining documentation and adverse events in primary care. For example, Andersson et al. (2018) examined serious adverse events reports submitted by nurses in Swedish nursing homes to the Health and Social Care Inspectorate and found that a “lack of competence” and “incomplete or lack of documentation” were the two most common factors that contributed to adverse events.
This study has identified few articles focusing on the connection between patient safety and nursing documentation practices at home health nursing services or nursing homes. Additionally, there is a need observed for additional research projects that focus on students’ experiences regarding the practice of patient documentation and the use of EPRs.
Social educators are employed in municipal care: in nursing homes and home healthcare units in Norway. They take part in a variety of nursing and caring tasks and activities, but their profession has more substantial knowledge in caring for people with various forms of disability than Registered Nurses. They have a deeper focus on rehabilitation and habilitation for disabled patients. On the other hand, Registered Nurses have a deeper awareness of the medical issues of nursing, as understanding of all kind of illness and its consequences, as well as medical treatment and medication (Grung, 2016). Nevertheless, when social educators are employed within the healthcare domain in Norway they are obligated to act under the same legislation guidelines regarding documentation as Registered Nurses. Understanding the experiences and perceptions of these staff members can also influence their contributions to collaboration in healthcare services. Therefore, the aim of this study was to better understand the perceptions of healthcare professionals and healthcare students regarding existing barriers to patient safety through the performance of documentation practices.
A descriptive, exploratory design (Polit and Beck, 2012) with a focus group methodology was applied to provide insights into the perceptions of nurses, social educators, and students and to understand their experiences in terms of patient safety and their documentation practices. To secure accurate and complete reporting of the study, the COREQ checklist (Tong et al., 2007) was used as a guideline.
The study was conducted between March 2015 and June 2015 at three3 primary care agencies and one University College located in central Norway. In the chosen region, all municipalities use the same EPR system—one of three main systems used in primary care in Norway—and similar to all other systems being used this one responds to the legislation requirements for digital documentation of healthcare information in Norway as well as GDPR regulations which Norway joined in 2018 (Ministry of Health and Care Services, 2012; The Norweigian Directorate of eHealth, 2019). This particular EPR solution, as is the case for the other two EPR systems, offers an enlarged EPR solution where the EPR module is connected to other relevant modules; for example, basic personal information, billing, and medication order modules.
Purposive sampling was used to recruit participants. The inclusion criteria for the nurses and social educators included that they were employed in primary healthcare (nursing homes or home nursing care) and that they were involved in direct patient care. The inclusion criteria for students included regular enrollment as a nursing or social educator student (at the bachelor-degree level) and previous practice in nursing homes and/or in-home healthcare settings as part of their education. Whereas the professionals were recruited by their ward managers, the students were recruited by contact persons at the University College. Both professionals and students were forwarded written information about the study, and all signed a consent form prior to participating in the study.
In total, 12 nurses and social educators and 11 students (22 women and one man) volunteered for this study. The mean working experience among the nurses and social educators was 13°years (ranging from 1 to 25 years), and their mean age was 40.5°years (ranging from 23 to 51°years). The students’ mean age was 23°years (ranging from 22 to 28°years). six of the students were in their final semester of a 3 years degree program, and five were in their penultimate year. The participants were interviewed in six focus groups; three groups of nurses and social educators (“staff informants”) and three groups of students. The sizes of the groups ranged from 3–5 participants, which is considered an optimal size for focus groups (Kitzinger 1995).
Focus group interviews were used to study perceptions among the group participants (Polit and Beck, 2012). In the focus groups, the participants were invited to reflect upon and compare each other’s views and experiences to contribute to a broader understanding of patient safety and documentation practices (Kitzinger, 1995).
The study applied an interview guide, which was developed based on performing a literature search and including previous clinical experiences and knowledge among the researchers. The interview guide included these areas:
Descriptions of patient information exchanges, collaborative procedures, and documentation practices applied during patient transfer.
Descriptions of daily nursing and care planning, communications, and documentation processes.
Uncovering whether EPR solutions meet professional needs with regard to patient information.
Descriptions of communications or EPR documentations that have caused or could cause adverse events.
As described by Krueger and Casey (2009), the focus group interviews were performed by two researchers: a moderator and an assistant. The moderator guided the discussion while the assistant kept track of the tape recording, made notes, and summarized the discussion. The focus group interviews lasted from 90 to 120 min, and all audio was recorded and transcribed verbatim.
Data were analyzed using qualitative content analysis (Krippendorff, 2018). The authors listened to each recorded interview and simultaneously read the transcribed text to obtain an overall view of the data. The texts were re-read several times to allow reflection on barriers to patient safety through the documentation practices for healthcare professionals and healthcare students. Then, the text was broken down into meaning units (i.e., words, phrases and sentences that relate to the same central meaning), which were condensed and labeled with a code. Based on similarities and differences, the codes were compared and sorted into nine sub-themes and four main themes. All authors participated in the data analysis and jointly discussed possible approaches to each theme until a consensus was reached (Patton, 2012).
By following Lincoln and Guba (1985) criteria, several strategies were used to enhance the trustworthiness of the study. Credibility was supported by including an adequate number of professional and student informants, encouraging dialogue in the focus group sessions, and by discussing the interpretation of data until a consensus on themes and sub-themes was reached. Providing descriptions of informants, data collection, analysis, and quotes from the focus group interviews enabled each individual reader to assess the transferability of the study findings to other contexts. Dependability and confirmability were achieved by using audio-recording during the interviews and transcribing all interviews verbatim and by having all authors discussing the data interpretations together.
The study was implemented in accordance with the Declaration of Helsinki (World Medical Association, 2001). Formal permission to perform data collection was obtained from the authorities at all municipalities and the University College. All nurses, social educators, and students were written-informed of the study and provided informed consent to participate. They were made aware of their rights to withdraw from the study at any time without consequence. The project was conferred with the Norwegian Center for Research Data (NSD), which concluded it not being notifiable.
The focus group analysis resulted in the identification of four main themes to describe the perceptions held by healthcare professionals and healthcare students regarding existing barriers to patient safety through the performance of documentation practices in primary care: 1) Technological barriers, 2) Organizational barriers, 3) Social barriers, and 4) Individual barriers. As shown in Table 1, each of these themes included several sub-themes. All participants responded based on experiences using the same EPR system to perform documentation tasks. In the presentation of results, the municipal nurses and social educators are described as a single group, referred to as “staff” or “nurse”. Quotes from the focus group sessions are used to elucidate the themes and sub-themes.
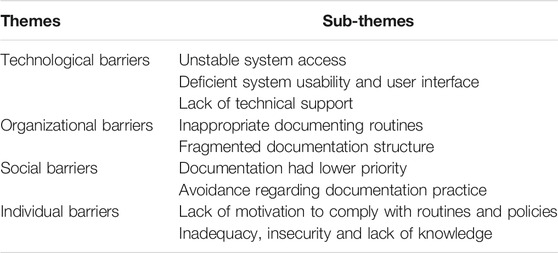
TABLE 1. Themes and sub-themes describing barriers for patient documentation.
This theme included three sub-themes and refers to the technological obstacles that the nursing staff and students were required to overcome when documenting patient care. The informants of this study described unstable system access as one of the main technological challenges. All participants described experiencing time-consuming log-in procedures, lasting more than 5 min each time, and not particularly connected to the EPR system itself but to the municipal server setup system requiring several levels of log-on procedures. Encountering this barrier would result in participants leaving the computer without logging off as expected, or they would ask a colleague to perform documentation on their behalf to avoid using their time for waiting for system access. They admitted that both practices were against security rules. Another example was unannounced system downtime caused by random and unforeseen internet issues, which could occur in the middle of documentation or while using the EPR system for shift reports or doctor’s visits. These experiences prevented the informants from using the system completely. Nursing staff and students had described experiencing the loss of system access due to planned, unannounced technical maintenance. These episodes resulted in a lack of trust in the EPR system, and respondents reported the regular use of paper-based backups for the most important patient information, such as patient personalia, patient contacts, and medication lists.
Further, the respondents presented the EPR system as incomplete, with deficient system usability and user interface that did not support their needs and requirements for daily nursing documentation routines, resulting in the use of a paper-based documentation system as a supplement to secure documentation, information exchange, and patient safety. One example was a staff informant group who still used the previous manual documentation system as a back-up:
When we need to find information about a patient, we must first go to the EPR system to see if we can find it there. If it is not there, we must look in the ‘Kardex’. It can take some time, then, if you are unsure where to find it.
Deficient system usability and user interface were found to be risk factors for adverse events. Multiple areas could be used to document the same information within the EPR system, which made documentation fragmented and difficult to rediscover when the nursing staff required the information. The EPR system did not follow the logical nursing planning structure that the informants expected and were trained for, which also increased the potential for adverse events. One staff informant stated:
…and it is a bit scary in everyday life because we are actually responsible for what we do, and when the system is designed so that you are tricked into making mistakes, as we do our job.
Usability and interface problems also included small fonts and compressed text that made information difficult to read and was another possible risk for adverse events.
The final technological barrier was the lack of technical support. When informants experienced problems, such as the system being down or log-on problems, these issues could only be addressed during a normal working day between 08:00–16:00, with no support offered during night shifts, weekends, or holidays. This lack of support was another reason many of the staff informants relied on paper-based backups and handwritten notes that would later be added to the EPR system. Paper-based backup routines were viewed as a necessary workaround; however, all participants admitted that paper backups were a safety risk because documentation became fragmented and paper notes could be lost.
This theme includes two sub-themes and refers to barriers within the organizational system, which made informants struggle when documenting patient information. Even though the informants of this study had experience using the same EPR system, each municipality was able to some extent to technically adjust the system setup according to their existing or desired organizational routines. This ability resulted in some variety in documentation routines. Thus, informants reported both shared and unique organizational documentation challenges and barriers between the focus groups.
Many of the organizational barriers were ascribed to inappropriate documentation routines in the unit. The EPR system was implemented many years ago, and it included areas suitable for registrations. However, some units maintained old routines, using notes, lists, and notebooks to document care. Some focus groups reported the reduced use of paper-based documentation, even though some paper-based routines were maintained due to technical issues, as described above. Other routines were maintained despite an awareness of the possibility of causing adverse events. The complete and expected reorganization of documentation routines was simply never initiated after implementing the EPR. In one of the student groups having experiences from a variety of municipalities, this frustration was shared:
A big source of error is that you always have to remember where to look for things; where to check the patch, the medications, where to find time appointments, and there, and there, and there and in addition you have to take care of the patients and keep them in mind, and then you have to keep in mind if there is any wound procedure, and then you have to keep in mind inhalation and the eye drop form in the closet, and. -You have to constantly go and keep in mind!
This inappropriate routine was confirmed by the student informant groups, who faced even more substantial challenges when attempting to retrieve information from multiple sources.
Furthermore, this theme also addressed a severe barrier to patient safety: inappropriate routines that included a lack of patient information. A lack of patient information either caused adverse events, or these adverse events were avoided by the clinical skills of the nursing staff or, as described by study informants, pure luck. Nursing staff had experienced rigid organizational EPR routines, in which only a few persons were permitted to add or change basic patient information. One example provided was an acute situation in which no family information could be found. The nurse involved traced the phone number of the patient’s daughter on the internet because she knew her name, but this informant said, ‘It was a bit hectic to find the daughters phone number, and simultaneously trying to save the patient`s life while waiting for the ambulance to come’. Lack of such information could lead to phone calls to the wrong individuals and a breach of confidentiality.
Staff informants had experienced not being allowed to add medical diagnoses to the EPR system because this task was reserved for the patient’s doctor. However, if the doctor did not perform this task diligently, the nurses had to guess which underlying illness the patient suffered to complete their nursing observations and actions. Lacking blood sample results was a recurring problem that was reported by multiple groups of informants. These results did exist, but sample information was not found. Partly, the results were not sent as e-messages and thereby not found within the EPR system as expected, or results were not inserted into the EPR system when received through a letter or phone call. Much time and effort were spent tracking answers to determine the correct administration of medications, potentially causing harm to the patients. In a staff focus group, one informant told:
Yes, we can wait for several days for answers for blood samples (…), and quite a few nurses get frustrated. We take a test on Monday and do not receive a response from the doctor before Thursday. So, then you should be happy that the nurse knows the users and give them what they think is right. It’s a big problem in the rural areas. It takes time.
One result of the different documentation practices in the various units was a fragmented documentation structure, which led to confusing patient information. This barrier was viewed as an organizational reinforcement of the technological barrier due to the organization allowing so much confusion in the structure of the EPR system. In the focus group sessions, the informants discussed the lack of overview of patient information in their documentation practice. In all of the focus group meetings, the informants discussed the time spent searching for patient information within the fragmented patient information structure. “There is a lot of paper lying all around.”
Both within the EPR system and between the EPR system and the paper-based supplementation systems, time was spent searching for, checking, and double-checking information. Both students and nursing staff experienced the documentation structure as a risk for patient safety. Furthermore, variations were found in the structure of care planning within the EPR system. Our informants reported the availability of both firm templates for documenting nursing actions and evaluations in addition to day-to-day reporting practices. Day-to-day reporting did not provide a broad overview and represented a risk of losing important follow-up areas for each patient. In contrast, a care-planning template with too much detail could overly fragment patient information and increase the risk of adverse events.
Another identified risk area was patient transfer reports. Our groups discussed the lack of a transfer documenting template and the various shapes of the reports. The following quote from one staff informant was representative for concerns expressed among all groups interviewed:
It is not specified what to write in the transfer report, so it is left to each person to decide and what she emphasizes of observations.
Poor reports increased the risks for adverse events, which could often only be prevented by making phone calls to verify the necessary information required for medical treatments and nursing follow-up.
This theme included two sub-themes associated with barriers to patient documentation that were not recognized as being caused by the organizational structures of the units. The main social barrier associated with an increased risk of adverse events was that documentation had lower priority compared with other tasks in the caring unit. Practical, daily tasks and patient-oriented work had higher priority and were more accepted among the nursing staff than spending time on the computer. During hectic shifts, our informants would rather relieve their colleagues than update the EPR. Thus, documentation tasks were postponed. This finding was confirmed by some student informants, who had received negative feedback if they spent too much time reading or updating the EPR instead of participating in direct patient-related activities. Our informants provided multiple examples in which they did not spend time learning how to use the EPR system or did not know where to document their nursing actions, and they described the dilemma. One staff informant said:
It is the issue of closeness to the patient. It is central in our caring to spend time with the patient. Documentation becomes a secondary issue, which I feel have to get into the heads of nurses: they must understand the importance of documentation! Why should you read? To stay updated.
A reoccurring issue that appeared in the focus group discussions was obvious avoidance regarding documentation practices in some units. The study found unequal attitudes towards the documentation of adverse events, even if the informants all agreed that the public strategy in their working units was to welcome such registration. However, the social attitude was that documenting an adverse event could be viewed as a form of self-punishment rather than as an opportunity for common learning and improvement. One of the focus groups consisting of staff participants discussed their proactive system developed to report and address adverse events, which was accepted and followed by staff members. The unit maintained a quality system known to everyone, and deviations from procedures were marked and reported as an adverse event and was followed up by leaders, as the procedure required. But even here:
We have had many plenary discussions now about the positivity of documenting deviations (…), but we think there is a lot below the surface that is not registered and reported.
This response revealed a developing culture for the handling of adverse events, which continued to face cultural challenges. The staff informants discussed their experiences with social change, moving towards a more pro-active attitude regarding the documentation and learning from the mistakes that led to adverse event registrations.
This theme includes two sub-themes and refers to the barriers associated with personal characteristics that may influence a staff member’s documentation practices. The barrier lack of motivation to comply with routines and policies was neither a result of the organizational regime nor a social structure within the units. When documenting nursing actions, the units had routines and procedures designating where in the EPR system nursing assessments and measures should be documented, but these guidelines were not always followed. Some staff informants admitted that they did not want to use the available tablet personal computer (PC) to document the EPR.
We act so different. Some of us document and take it very seriously. Document everything (…) everything done in a day, while others are better at documenting what is relevant for the patient care (…) And some do not write at all.
The staff informants stated that they and their colleagues did not always read the EPR when they began their shifts or did not thoroughly examine the documentation, such as when administering medications. Important information could be missed, leading to adverse events of varying degrees of severity. Time shortage or not sharing the same sense of responsibility for documentation were the explanations given for not accomplishing documentation tasks, either in a standardized way or at all. However, not having complete and sufficient patient information is a risk factor for adverse events and was also a stress factor for our informants in their daily work.
Our focus group informants discussed their common experiences of inadequacy, insecurity, and lack of knowledge regarding the ability to document patient information properly. In particular, staff informants experienced a lack of confidence, skills, and knowledge necessary for documentation tasks, even if they had have received both an education and formal training on the topic.
It’s easier not to do it, when you are insecure, than to do it. It is about they don’t exactly know how to do it … and then they do not; not document at all, leaving it to someone who can. And then there are a few who are very good at it, and the days they are not here, then it will not be done.
Basic information and communications technology (ICT) skills varied among the participants and strengthened the sense of insecurity described above. Our student groups did not address such insecurity in the same manner as our staff informants did. The challenge included where to search for or document patient care.
It feels safer to document it all under “general information” because you have not analyzed so much yourself then, on your own.
They reported low confidence in their own and their colleagues’ ability to place documentation elements correctly in the EPR system, resulting in a fundamental concern regarding the quality of patient documentation and a constant fear that adverse events will occur. To overcome these barriers, they searched for, checked, and double-checked available patient information sources within and outside the EPR system to secure the quality of care. They had to rely on oral handover for adequate patient information.
You must ask the nurses you work with; maybe they know, but it is not certain you get the right answer.
Individual use of phrases in documentation practice was also discussed in the focus groups. The student groups, in particular, felt unsafe when nurses used phrases and words not familiar to them; however, staff informants also expressed problems with individual approaches toward documenting language, subsequently making it difficult to contextualize follow-up activities.
Our informants worried about their ability to remember all messages and tasks and their ability to accomplish their documenting duties correctly, particularly during busy periods. The documentation of drug administration was a major challenge reported for individual documentation practices among our informants. Most adverse event reports were associated with the area of medication. One student representative had the following experience:
One of our patients had anti-constipation treatment without being constipated: His elimination status was just not recorded anywhere.
Another example was not being aware of a missing blood sampling that was necessary to perform medication adjustments, resulting in incorrect medication; this error was recognized as a potential patient safety risk.
Uncertainty among the nursing staff was observed by the student groups, making them insecure during their practical study periods. Students also experienced expectations among the nurse staff, who expected them to know without being taught:
It is not documented anywhere! (…) and then they just said that I will learn this as I am working here more permanently.
This expectation of tacit knowledge frustrated them and made them anxious about potentially harming the patients due to a lack of patient information.
This study aimed to better understand the perceptions of healthcare professionals and healthcare students regarding the barriers to patient safety through the performance of documentation practices. The results demonstrated that technological, organizational, social, and individual barriers to nursing documentation pose potential risks to patient safety. Our results could be associated with seven of the nine areas outlined in the WHO strategy “Safer primary care” (2012). Follow-up thematic reports (WHO, 2016) underpin the study’s results by many converging elements that involve safety risks.
Technological barriers were a basic challenge reported by our participants. Unstable system access, deficient EPR usability, and poor user interfaces, together with scarce technical support, did not support their nursing practice needs. The respondents struggled to document and access sufficient information to perform daily care. Similar findings were reported in Priestman et al. (2018) and in a review by Stevenson et al. (2010) and followed up by a study in 2012 where nurses reported that the EPR does not support their nursing practice (Stevenson and Nilsson, 2012). WHO (2016) also emphasized the increased use of technical devices in primary care to improve patient safety. The report admitted that poorly designed EPR systems might create more work and frustration among staff, similar to our findings. A literature review by Gesulga et al. (2017) also recognized barriers, such as user resistance arising from data security concerns. Technological tools, such as EPRs aim for but do not necessarily achieve the prevention of human errors and the improvement of information exchange. Such tools can also create additional human work or new ways of working. Thus, the nursing staff became dependent on technological usability and stability to provide nursing and care and secure patient safety (Dekker, 2016).
One of this study’s four main themes was organizational barriers, also identified as a main patient safety area by WHO (2012); WHO (2016). Barriers were identified in this study, such as incomplete or inaccurate documentation routines and fragmented documentation structures. Kutney-Lee et al. (2019) also found correlations between organizational issues, such as work environment, patient safety and EPR system usability. Many documentation errors by use of the EPR systems can be caused by deficiencies in the organizational structure in a care unit, such as patient transfers, something many participants also described in the study, including “poorly written or illegible discharge summaries” (WHO, 2016). “Transitions of care” is also emphasized as a focus area by WHO (2016) as well as in other studies (Graabæk et al., 2019; Patel and Landrigan, 2019). This topic identifies several risk areas related to patient safety that were also discussed by our informants: increased adverse events, delays in receiving appropriate treatment, and lost tests or blood sample results. Studies suggest interventions to prevent safety risks such as standardization of documentation and discharge information (Törnvall and Jansson, 2017; De Groot et al., 2019), all of which were supported by our informants: for both transition situations and to improve the documentation structure in general.
Two sub-themes were regarded as social barriers to documentation in the EPR. The study found that spending time documenting had a lower priority than other tasks and that in some units, the staff groups showed avoidance behavior toward documenting practices. Similar negative attitudes toward documentation have been reported previously, such as in Bøgeskov and Grimshaw-Aagaard (2018) research, in which nurses in hospitals perceived documentation as being a meaningless burden that hindered them from focusing on the patient. When the safety culture within staff groups undermines documentation tasks, identifying whether the underlying reasons for these attitudes and behaviors are associated with the priority of direct patient care or whether other causalities exist is imperative (Barkhordari-Sharifabad et al., 2017).
Individual barriers to documentation practices included both a lack of motivation for documenting practices and the informant’s sense of inadequacy, insecurity, and lack of knowledge regarding correct documentation procedures. Designing systems that better support the nursing staff can contribute to their motivation to comply with the established routines and policies for documenting tasks (Stevenson et al., 2010). Improved system usability may reduce the occurrence of potential adverse events and increase patient safety (Williams, 2019). One area associated with severe patient risk that was reported in our work was nursing staff not correctly updating or carefully reading the EPR when handling medication. WHO (2016) confirmed, in line with our results, “workload and time pressure” and “lack of accuracy in the patient record” as factors that increased the risk of patient safety harm. This is also found by other studies (Al-Jumaili and Doucette 2018; Dunn Lopez et al., 2021). There appears to be a need for a more systematic approach to handling medication information, such as computerized decision support systems (Marasinghe, 2015).
Reasons for not using the tablet PC for documentation were not provided in our result. However, tablets may reduce the time spent on documentation, as reported in the reviews by Dall’ora et al. (2020) and Blair and Smith (2012). Lack of time was discussed by the healthcare staff as a reason for not documenting or postponing documentation tasks during their shift, as also noted by Söderberg et al. (2009): therefore, it is necessary to cross this barrier to patient safety by providing an understanding of the use of the EPR as an efficient way of documentation time in contrast to time spent walking around, collecting necessary information among colleagues in the unit.
Lack of training, which was also emphasized by our informants, in our view, was regarded as an individual issue rather than an organizational problem. Our participants indicated inadequacy, insecurity, and lack of knowledge among their individual challenges but did not necessarily describe these issues as part of the organizational strategy because they had all received training sessions within their units. Bing-Jonsson et al. (2016) investigated the sufficiency of nursing staff competence in Norwegian community elderly care and found that documentation is one of the areas where nurses, auxiliary nurses, and assistants may have insufficient competence. The authors concluded that education and training alone appeared to have a limited impact on competence, potentially due to health professionals having unclear roles and inadequate standards for judging their own competence; they perform many of the same tasks, regardless of formal competence based on education (Bing-Jonsson et al., 2016).
The student informants in our study described nursing staff who sometimes omitted the documentation of patient information and expected the students to know without being taught (i.e., tacit knowledge). Staff members in long-term elderly care often know their patients quite well and, therefore, may find documentation redundant because they maintain a lot of information “in their heads” (Østensen et al., 2019).
One strength of this study is that the sample included a combination of healthcare professionals with considerable experience and bachelor-degree students with an outside view of the workplace. The students had experience from health services in several municipalities during their practical studies and contributed with useful reflections on similarities and differences between these areas in the focus group interviews. Only one man attended the study, which could be considered a limitation. However, this skewed gender distribution is reflective of the large proportion of women employed in elderly care.
The student informants were recruited from the University College where all authors were employed, but none of the authors were involved in assessing these participants’ academic elements of their studies. All students were made aware that participating in the research would have no impact on their progression through their bachelor’s program.
The use of a topic-based interview guide, instead of narrow questions, contributed to data-rich discussions in the focus groups. The authors experienced an open and trusting atmosphere during the sessions, where all informants shared honest reflections and described real challenges from practice. Lively discussions, both in the staff focus groups and the student focus groups, contributed to rich qualitative data. The years between data collection and publication may be seen as a limitation in the study, but we have also learned that changes due to digitalization in healthcare take many years to implement and adopt, as described by Morris et al. (2011). Thus, we suggest that the experiences will still be relevant for healthcare organizations preparing for the implementation of ICT tools. The fact that the study involved one EPR solution may be regarded as a limitation. On the other hand, one may also consider this as a strength, because all informants reported on their experiences from a common starting point when describing their challenges. Involving municipalities with other EPR solutions could have expanded the picture of challenge. On the other hand it could have given responses based on more unequal prerequisites referring to various EPR systems. This could further have drawn attention away from challenges described in the result of this study, and more toward variations between EPR systems as such.
The fact that all 3 authors were involved in the analysis process was also an advantage. Due to the qualitative design, the results cannot be generalized. However, because the documentation of patient information is an important part of any healthcare professional’s practice, the study results could be transformed and applied to several other contexts in healthcare.
In this study, our results identified several barriers that negatively influenced patient documentation practices, exposing patients in primary care to increased safety risks and potentially harmful situations. To enhance and secure patient safety, increased individual, social, organizational, and technological support is necessary to overcome these barriers to ensure that optimal patient information is available when required for nursing care. To achieve this aim, primary care services must facilitate the necessary improvements by prioritizing technical, economic, and human resources for system development, training, and the definition of clear mission statements and policies.
The study results may inform various stakeholders in designing, implementing, using, and teaching EPR systems:
• System vendors may gain more knowledge of the complexity in nursing staff’s everyday lives, and to what extent implemented EPR systems still fail to meet the needs for documentation and information exchange continuing to risks of adverse events.
• Health service leaders and ICT leaders should pay close attention to system implementation and adoption phases paving the path for their staff members, not underestimating the complexity in documentation and information exchange in their caring units, all in order to secure and improve patient safety.
• Staff members and healthcare students may learn how colleagues and co-students experience their EPR documentation practice, reflecting upon their own situation regarding patient safety and EPR use.
• Teaching organizations at high school and university level may become more effectively supported in their focus on teaching their students documentation in both theory and practice as well as the connectivity between structured EPR use for documentation and an improved level of patient safety.
• System vendors may gain more knowledge of the complexity of nursing staff practices and the fact that implemented EPR systems still do not meet the needs for documentation and information exchange but continue to pose risks of adverse events.
• Health service leaders and ICT leaders should pay close attention to system implementation and adoption phases: This study shows the need for these leaders to pave the path for their staff members and not to underestimate the complexity in documentation and information exchange in their caring units: all in order to secure and improve patient safety.
• Staff members and healthcare students may learn how colleagues and co-students experience their EPR documentation practice, engaging in reflection about their own situation regarding patient safety and EPR use.
• Teaching organizations at high school and university level may be better supported in their focus on teaching their students documentation in both theory and practice: This study could also deepen the understanding of the connectivity between structured EPR use for documentation and the necessary level of patient safety.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and the approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank our participants, students and nursing staff participants as well as their leaders for time spent in the focus group discussions: for sharing experiences and thoughts with the research team in order to achieve the results of the study.
Ahgren, B. (2014). The Path to Integrated Healthcare: Various Scandinavian Strategies. Int. J. Care Coord. 17, 52–58. doi:10.1177/2053435414540606
Akhu-Zaheya, L., Al-Maaitah, R., and Bany Hani, S. (2018). Quality of Nursing Documentation: Paper-Based Health Records versus Electronic-Based Health Records. J. Clin. Nurs. 27 (3–4), e578–e589. doi:10.1111/jocn.14097
Al-Jumaili, A. A., and Doucette, W. R. (2018). A Systems Approach to Identify Factors Influencing Adverse Drug Events in Nursing Homes. J. Am. Geriatr. Soc. 66 (7), 1420–1427. doi:10.1111/jgs.15389
Ammenwerth, E., Mansmann, U., Iller, C., and Eichstädter, R. (2003). Factors Affecting and Affected by User Acceptance of Computer-Based Nursing Documentation: Results of a Two-Year Study. J. Am. Med. Inform. Assoc. 10, 69–84. doi:10.1197/Fjamia.M111810.1197/jamia.m1118
Andersson, Å., Frank, C., Willman, A. M., Sandman, P.-O., and Hansebo, G. (2018). Factors Contributing to Serious Adverse Events in Nursing Homes. J. Clin. Nurs. 27 (1−2), e354–e362. doi:10.1111/jocn.13914
Barkhordari-Sharifabad, M., Ashktorab, T., and Atashzadeh-Shoorideh, F. (2017). Obstacles and Problems of Ethical Leadership from the Perspective of Nursing Leaders: A Qualitative Content Analysis. J. Med. Ethics Hist. Med. 10, 1.
Bing-Jonsson, P. C., Hofoss, D., Kirkevold, M., Bjørk, I. T., and Foss, C. (2016). Sufficient Competence in Community Elderly Care? Results from a Competence Measurement of Nursing Staff. BMC Nurs. 15, 5. doi:10.1186/s12912-016-0124-z
Blair, W., and Smith, B. (2012). Nursing Documentation: Frameworks and Barriers. Contemp. Nurse 41, 160–168. doi:10.5172/conu.2012.41.2.160
Blais, R., Sears, N. A., Doran, D., Baker, G. R., Macdonald, M., Mitchell, L., et al. (2013). Assessing Adverse Events Among home Care Clients in Three Canadian Provinces Using Chart Review. BMJ Qual. Saf. 22 (12), 989–997. doi:10.1136/bmjqs-2013-002039
Bøgeskov, B. O., and Grimshaw-Aagaard, S. L. S. (2018). Essential Task or Meaningless burden? Nurses’ Perceptions of the Value of Documentation. NJNR 39, 9–19. doi:10.1177/2057158518773906
Cerejeira, J., and Mukaetova-Ladinska, E. B. (2011). A Clinical Update on Delirium: from Early Recognition to Effective Management. Nurs. Res. Pract. 2011, 1–12. doi:10.1155/2011/875196
Chong, C. P., and Street, P. R. (2008). Pneumonia in the Elderly: a Review of the Epidemiology, Pathogenesis, Microbiology, and Clinical Features. South. Med. J. 101, 1141–1145. doi:10.1097/smj.0b013e318181d5b5
Dall’ora, C., Griffiths, P., Hope, J., Barker, H., and Smith, G. B. (2020). What Is the Nursing Time and Workload Involved in Taking and Recording Patients’ Vital Signs? A Systematic Review. J. Clin. Nurs. 29, 2053. doi:10.1111/jocn.15202
De Groot, K., Triemstra, M., Paans, W., and Francke, A. L. (2019). Quality Criteria, Instruments, and Requirements for Nursing Documentation: A Systematic Review of Systematic Reviews. J. Adv. Nurs. 75 (7), 1379–1393. doi:10.1111/jan.13919
Dekker, S. (2016). Patient Safety: A Human Factors Approach. Boca Raton: CRC Press. doi:10.1201/b10942
Dunn Lopez, K., Chin, C.-L., Leitão Azevedo, R. F., Kaushik, V., Roy, B., Schuh, W., et al. (2021). Electronic Health Record Usability and Workload Changes over Time for Provider and Nursing Staff Following Transition to New EHR. Appl. Ergon. 93, 103359. doi:10.1016/j.apergo.2021.103359
Emanuel, L., Berwick, D., Conway, J., Combes, J., Hatlie, M., Leape, L., et al. (2009). “What Exactly Is Patient Safety?,” in Advances in Patient Safety: New Directions and Alternative Approaches. Editors H. Kerm, B., J., B, M., A. Keyes, M., and L. Grady (Rockville (MD): Agency for Healthcare Research and Quality)), 95, 13–24. doi:10.30770/2572-1852-95.1.13
Ferrer, L., and Goodwin, N. (2014). What Are the Principles that Underpin Integrated Care?. Int. J. Integr. Care 14, e037. doi:10.5334/ijic.1884
Gautun, H., and Syse, A. (2017). Earlier Hospital Discharge: a challenge for Norwegian Municipalities. Nord J. Soc. Res. 8, 1–17. doi:10.7577/njsr.2204
Gehring, K., Schwappach, D. L., Battaglia, M., Buff, R., Huber, F., Sauter, P., et al. (2012). Frequency of and Harm Associated with Primary Care Safety Incidents. Am. J. Manag. Care 18, e323–37. doi:10.7892/BORIS.14040
Gesulga, J. M., Berjame, A., Moquiala, K. S., and Galido, A. (2017). Barriers to Electronic Health Record System Implementation and Information Systems Resources: A Structured Review. Proced. Comput. Sci. 124, 544–551. doi:10.1016/j.procs.2017.12.188
Gjevjon, E. L. R. (2014). Continuity in Long-Term home Health Care. Perspectives of Managers, Patients and Their Next of Kin. [dissertation]. Oslo: Faculty of Medicine, University of OsloAvailable at: http://urn.nb.no/URN:NBN:no-44164 (Accessed October 15, 2020).
Graabæk, T., Terkildsen, B. G., Lauritsen, K. E., and Almarsdóttir, A. B. (2019). Frequency of Undocumented Medication Discrepancies in Discharge Letters after Hospitalization of Older Patients: a Clinical Record Review Study. Ther. Adv. Drug Saf. 10, 2042098619858049. doi:10.1177/2042098619858049
Gray, L. K., Smyth, K. A., Palmer, R. M., Zhu, X., and Callahan, J. M. (2002). Heterogeneity in Older People: Examining Physiologic Failure, Age, and Comorbidity. J. Am. Geriatr. Soc. 50, 1955–1961. doi:10.1046/j.1532-5415.2002.50606.x
Grung, R. M. (2016). The Role of the Norwegian Social Educator. Learn. Disabil. Pract. 19 (10), 24–26. doi:10.7748/ldp.2016.e1810
Helleso, R., and Ruland, C. M. (2001). Developing a Module for Nursing Documentation Integrated in the Electronic Patient Record. J. Clin. Nurs. 10, 799–805. doi:10.1046/j.1365-2702.2001.00557.x
Keenan, G., Yakel, E., Dunn Lopez, K., Tschannen, D., and Ford, Y. B. (2013). Challenges to Nurses' Efforts of Retrieving, Documenting, and Communicating Patient Care Information. J. Am. Med. Inform. Assoc. 20 (2), 245–251. doi:10.1136/amiajnl-2012-000894
Kitzinger, J. (1995). Qualitative Research: Introducing Focus Groups. BMJ 311, 299–302. doi:10.1136/bmj.311.7000.299
Krippendorff, K. (2018). Content Analysis: An Introduction to its Methodology. California, USA: SAGE Publications.
Krueger, R. A., and Casey, M. A. (2009). Focus Groups: A Practical Guide for Applied Research. California, USA: SAGE Publications.
Kulik, C. T., Ryan, S., Harper, S., and George, G. (2014). Aging Populations and Management. Amj 57, 929–935. doi:10.5465/amj.2014.4004
Kutney-Lee, A., Sloane, D., Bowles, K., Burns, L., and Aiken, L. (2019). Electronic Health Record Adoption and Nurse Reports of Usability and Quality of Care: The Role of Work Environment. Appl. Clin. Inform. 10, 129–139. doi:10.1055/s-0039-1678551
Marasinghe, K. M. (2015). Computerised Clinical Decision Support Systems to Improve Medication Safety in Long-Term Care Homes: a Systematic Review. BMJ Open 5 (5), e006539. doi:10.1136/bmjopen-2014-006539
Marengoni, A., Angleman, S., Melis, R., Mangialasche, F., Karp, A., Garmen, A., et al. (2011). Aging with Multimorbidity: a Systematic Review of the Literature. Ageing Res. Rev. 10, 430–439. doi:10.1016/j.arr.2011.03.003
Melby, L., Obstfelder, A., and Hellesø, R. (2018). “We Tie Up the Loose Ends”: Homecare Nursing in a Changing Health Care Landscape. Glob. Qual. Nurs. Res. 5, 233339361881678–2333393618816780. doi:10.1177/2333393618816780
Ministry of Health and Care Services (2012). Morgendagens Omsorg”. Available at: https://www.regjeringen.no/contentassets/34c8183cc5cd43e2bd341e34e326dbd8/no/pdfs/stm201220130029000dddpdfs.pdf (Accessed October 15, 2020), [Governmental white paper. St. 29 (2012–2013), Tomorrow's care]
Ministry of Health and Care Services (2009). Samhandlingsreformen. Available at: https://www.regjeringen.no/contentassets/d4f0e16ad32e4bbd8d8ab5c21445a5dc/no/pdfs/stm200820090047000dddpdfs.pdf (Accessed October 15, 2020), [Governmental white paper. St. 29 (2012–2013, The coordination Reform]
Mitchell, P. H. (2008). “Defining Patient Safety and Quality Care,” in Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Editor R. G. Hughes (Rockville (MD): Agency for Healthcare Research and Quality (US). doi:10.1016/j.aorn.2009.09.014
Moldskred, P. S., Snibsøer, A. K., and Espehaug, B. (2020). Improving the Quality of Nursing Documentation at A Residential Care Home: A Clinical Audit. BMC Nurs. 23, 577–585. doi:10.21203/rs.3.rs-80580/v1
Morris, Z. S., Wooding, S., and Grant, J. (2011). The Answer Is 17 years, what Is the Question: Understanding Time Lags in Translational Research. J. R. Soc. Med. 104 (12), 510–520. doi:10.1258/jrsm.2011.110180
Næss, G., Kirkevold, M., Hammer, W., Straand, J., and Wyller, T. B. (2017). Nursing Care Needs and Services Utilised by home-dwelling Elderly with Complex Health Problems: Observational Study. BMC Health Serv. Res. 17, 645. doi:10.1186/s12913-017-2600-x
Olsen, R. M., Hellzén, O., Skotnes, L. H., and Enmarker, I. (2012). Content of Nursing Discharge Notes: Associations with Patient and Transfer Characteristics. Ojn 02 (3), 277–287. doi:10.4236/ojn.2012.23042
Olsen, R. M., Østnor, B. H., Enmarker, I., and Hellzén, O. (2013). Barriers to Information Exchange during Older Patients' Transfer: Nurses' Experiences. J. Clin. Nurs. 22 (19–20), 2964–2973. doi:10.1111/jocn.12246
Østensen, E., Bragstad, L. K., Hardiker, N. R., and Hellesø, R. (2019). Nurses' Information Practice in Municipal Health Care-A Web‐like Landscape. J. Clin. Nurs. 28, 2706–2716. doi:10.1111/jocn.14873
Panesar, S. S., deSilva, D., Carson-Stevens, A., Cresswell, K. M., Salvilla, S. A., Slight, S. P., et al. (2015). How Safe Is Primary Care? A Systematic Review. BMJ Qual. Saf. 25, 544–553. bmjqs-2015-004178. doi:10.1136/bmjqs-2015-004178
Patel, S. J., and Landrigan, C. P. (2019). Communication at Transitions of Care. Pediatr. Clin. North America 66 (4), 751–773. doi:10.1016/j.pcl.2019.03.004
Patton, M. Q. (2012). Qualitative Research and Evaluation Methods. California, USA: SAGE Publications.
Polit, D., and Beck, C. (2012). Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th eds. NY: Lippincott Williams & Wilkins.
Priestman, W., Sridharan, S., Vigne, H., Collins, R., Seamer, L., and Sebire, N. J. (2018). What to Expect from Electronic Patient Record System Implementation: Lessons Learned from Published Evidence. BMJ Health Care Inform. 25 (2), 92–104. doi:10.14236/jhi.v25i2.1007
Söderberg, J., Grankvist, K., Brulin, C., and Wallin, O. (2009). Incident Reporting Practices in the Preanalytical Phase: Low Reported Frequencies in the Primary Health Care Setting. Scand. J. Clin. Lab. Invest. 69, 731–735. doi:10.3109/00365510903007018
Stevenson, J. E., Nilsson, G. C., Petersson, G. I., and Johansson, P. E. (2010). Nurses' Experience of Using Electronic Patient Records in Everyday Practice in Acute/inpatient ward Settings: A Literature Review. Health Inform. J 16, 63–72. doi:10.1111/j.1365-2648.2011.05786.x10.1177/1460458209345901
Stevenson, J. E., and Nilsson, G. (2012). Nurses' Perceptions of an Electronic Patient Record from a Patient Safety Perspective: a Qualitative Study. J. Adv. Nurs. 68 (3), 667–676. doi:10.1111/j.1365-2648.2011.05786.x
The Norwegian Directorate of eHealth (2018). A Brief Overview of Health IT Collaboration and Interoperability in Five Countries in 2018. Available at: https://ehelse.no/publikasjoner/a-brief-overview-of-health-it-collaboration-and-interoperability-in-five-countries-in-2018 (Accessed October 15, 2020).
The Norwegian Directorate of eHealth (2019). Implementation of GDPR in Health Care Sector in Norway. Available at: https://ehelse.no/personvern-og-informasjonssikkerhet/implementation-of-gdpr-in-health-care-sector-in-norway (Accessed October 15, 2020).
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated Criteria for Reporting Qualitative Research (COREQ): a 32-item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 19 (6), 349–357. doi:10.1093/intqhc/mzm042
Törnvall, E., and Jansson, I. (2017). Preliminary Evidence for the Usefulness of Standardized Nursing Terminologies in Different fields of Application: A Literature Review. Int. J. Nurs. Terminol Knowledge 28 (2), 109–119. doi:10.1111/2047-3095.12123
Tuinman, A., de Greef, M. H. G., Krijnen, W. P., Paans, W., and Roodbol, P. F. (2017). Accuracy of Documentation in the Nursing Care Plan in Long-Term Institutional Care. Geriatr. Nurs. 38 (6), 578–583. doi:10.1016/j.gerinurse.2017.04.007
Wekre, L. J. (2014). Implementation of Multidose Drug Dispensing in a Home Care Setting: Changes in Safety of Medicines Management. Trondheim: Norwegian University of Technology and Science. [dissertation], Available at: http://hdl.handle.net/11250/264576.
WHO (2017). Patient Safety: Making Health Care Safer. Geneva: World Health OrganizationAvailable at: https://www.who.int/patientsafety/publications/patient-safety-making-health-care-safer/en/ (Accessed October 15, 2020).
WHO (2012). “Safer Primary Care,” in A Global challenge. The Safer Primary Care Expert Working Group. Geneva: Word Health OrganizationAvailable at: https://www.who.int/patientsafety/summary_report_of_primary_care_consultation.pdf (Accessed October 15, 2020).
WHO (2016). Safer Primary Care: Technical Series. Geneva: Word Health OrganizationAvailable at: https://www.who.int/patientsafety/topics/primary-care/technical_series/en/ (Accessed October 15, 2020).
Williams, A. (2019). Nursing Informaticians Address Patient Safety to Improve Usability of Health Information Technologies. Stud. Health Technol. Inform. 257, 501–507. doi:10.3233/978-1-61499-951-5-501
World Medical Association (2001). World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. Bull. World Health Organ. 79 (4), 373–374. Available at: http://search.ebscohost.com/login.aspx?direct=true&db=c8h&AN=106094131&site=ehost-live (Accessed October 15, 2020).
Keywords: electronic patient record, nursing, patient safety, primary health care, documentation, focus group
Citation: Bjerkan J, Valderaune V and Olsen RM (2021) Patient Safety Through Nursing Documentation: Barriers Identified by Healthcare Professionals and Students. Front. Comput. Sci. 3:624555. doi: 10.3389/fcomp.2021.624555
Received: 31 October 2020; Accepted: 17 May 2021;
Published: 01 June 2021.
Edited by:
Åsa Cajander, Uppsala University, SwedenReviewed by:
Lex Van Velsen, Roessingh Research and Development, NetherlandsCopyright © 2021 Bjerkan, Valderaune and Olsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorunn Bjerkan, am9ydW5uLmJqZXJrYW5Abm9yZC5ubw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.