 Graham Roberts1,2,3*
Graham Roberts1,2,3* Erkka Valovirta4
Erkka Valovirta4 Susanne Halken5Peter A. Eng6
Susanne Halken5Peter A. Eng6 Mika J. Mäkelä7Karin C. Lødrup Carlsen8,9Roland Knecht10L. Pekka Malmberg11
Mika J. Mäkelä7Karin C. Lødrup Carlsen8,9Roland Knecht10L. Pekka Malmberg11
- 1The David Hide Asthma and Allergy Research Centre, St Mary’s Hospital, Newport, Isle of Wight, United Kingdom
- 2NIHR Biomedical Research Centre, University Hospital Southampton NHS Foundation Trust, Southampton, United Kingdom
- 3Faculty of Medicine, University of Southampton, Southampton, United Kingdom
- 4Terveystalo Allergy Clinic, Department of Lung Diseases and Clinical Immunology, University of Turku, Turku, Finland
- 5Hans Christian Andersen Children’s Hospital, Odense University Hospital, Odense, Denmark
- 6Section of Paediatric Pulmonology and Allergy, Children’s Hospital, Aarau, Switzerland
- 7Skin and Allergy Hospital, Helsinki University Central Hospital and University of Helsinki, Helsinki, Finland
- 8Department of Paediatrics, Oslo University Hospital, Oslo, Norway
- 9Faculty of Medicine, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 10Doctors Surgery for Paediatrics, Bretten, Germany
- 11Unit of Clinical Physiology, Skin and Allergy Hospital, Helsinki University and Helsinki University Hospital, Helsinki, Finland
Asthma is a common chronic disease in children. It is a dynamic condition—symptoms change over time, and the outcome of diagnostic tests can vary. Consequently, evaluating the onset of asthma at a single point in time, perhaps when patients are asymptomatic with limited impairment of the lung function, may result in false diagnostic conclusions. The absence of consistent gold-standard diagnostic criteria in children challenges the ability of any study to ascertain an effect of treatment on asthma prevention. A comprehensive review of the diagnostic criteria used for new-onset asthma in school-age children was conducted based on existing recommendations from published clinical guidance, alongside evidence from paediatric asthma prevention trials. Findings from the review were used to propose suggestions for diagnosing new-onset asthma in future asthma prevention trials. Despite an overall lack of consensus in the published clinical guidance, there are similarities between the various recommendations for diagnosing asthma in children, which typically involve assessing the variable symptoms and supplementing the medical history with objective measures of lung function. For future paediatric asthma prevention trials, we suggest that paediatric clinical trials should use a new-onset asthma definition that incorporates the concepts of “possible”, “probable” and “confirmed” asthma. “Possible” asthma would capture self-reported features of chronic symptoms and symptom relief with β2-agonist bronchodilator (suggesting reversibility). “Probable” asthma would include symptom chronicity, self-reported symptom relief with β2-agonist bronchodilator, and objective features of asthma (reversibility or bronchial hyper-responsiveness). A “confirmed” diagnosis would be made only if there is a positive response to controller therapy. These suggestions aim to improve the diagnosis of new-onset childhood asthma in clinical trials, which will be useful in the design and conduct of future paediatric asthma prevention trials.
1 Introduction
Asthma is a major public health concern affecting more than 250 million people worldwide (2019 data) (1), and it is one of the most common chronic diseases in children (2). The underlying pathophysiology is heterogeneous, although the Th2-high phenotype predominates in the paediatric age group (3). Often, allergic and/or eosinophilic airway inflammation is present, and symptoms can be triggered by allergens, infections, or irritants such as pollution (3). The prevalence of asthma is higher in males than in females during childhood, but the situation reverses after adolescence and moving into adulthood when the predominance is female (4, 5).
Asthma is a disease of variable airflow obstruction, and no gold-standard diagnostic test for asthma exists (6). In clinical practice, asthma is diagnosed by a history of respiratory symptoms, such as wheeze, shortness of breath, chest tightness, and cough, that vary over time and in intensity, with variable expiratory airflow limitation [according to the Global Initiative for Asthma (GINA)] (7, 8). However, symptoms of wheeze, shortness of breath, and cough, in school-age children, may also be caused by conditions other than asthma—for example, bacterial or viral respiratory tract infections, congenital heart disease, or cystic fibrosis (8). Such conditions need to be excluded before a diagnosis of asthma is made (8). Wheeze, in particular, is common in preschool-age children (typically associated with upper respiratory tract infections) (8), making it a challenge to diagnose asthma in older, school-age children who have a history of wheezing.
In children, asthma is associated with comorbidities, impaired quality of life, limitations of physical activities/school performance, and psychological effects (9, 10). Asthma is also an important contributing factor for emergency department visits and hospitalisations in children (10, 11). The chronic, persistent nature of asthma (12) emphasises the need for preventive strategies. One such approach is to treat the underlying allergy that seems to be associated with much of childhood asthma (13, 14). Allergen immunotherapy (AIT) has been shown to have a preventive long-term effect on the development of asthma symptoms, the use of asthma medication, and on bronchial reactivity (15, 16). A window of opportunity for preventing asthma may exist during infancy in the early stages of immune development (17), or in young children during the early stages of disease where the level of allergic sensitisation is low (18). A meta-analysis of AIT trials suggested that AIT has a short-term benefit in preventing asthma in patients with allergic rhinitis (AR), particularly if AIT has been initiated in childhood (19). Other approaches, such as targeting microbial diversity, may also be important in primary asthma prevention (17). Despite the clinical evidence for AIT in asthma, the European Academy of Allergy and Clinical Immunology (EAACI) guidelines emphasise the need for further confirmatory studies (16). The EAACI guidelines also highlight the urgent need to define and standardise optimal clinical diagnostic criteria for asthma that should be used in future clinical trials (16).
With this in mind, we set out to review the criteria used to define new-onset asthma in the context of a paediatric clinical trial. This project developed from the authors' involvement in the Grazax Asthma Prevention (GAP) trial and their scientific discussions on the appropriateness of the definition for new-onset asthma used in the GAP trial (20). Here, we examine the recommendations for diagnosing paediatric asthma in clinical practice as outlined in various clinical guidelines and consider the challenges of defining diagnostic criteria for new-onset asthma in paediatric asthma prevention trials. We also provide suggestions for improving the definition of new-onset asthma in school-age children in the context of clinical trials, for use in future studies.
2 Methods
Figure 1 outlines the literature searching that was undertaken to identify clinical guidance reports containing recommendations for the diagnosis of asthma in children. Firstly, a PubMed search was conducted (on 29 June 2023) using the search string: {[children(Title)] OR [childhood(Title)] OR [paediatric(Title)] OR [pediatric(Title)]} AND [asthma(Title)] AND {[guidelines(Title)] OR [guideline(Title)]}. The returned abstracts were screened for relevance (i.e., guidance for diagnosing asthma in children, written in English) and were excluded if they did not meet the required criteria. For selected abstracts, the full publication was evaluated for inclusion/exclusion using the same criteria. In addition, targeted literature searching of relevant international organisations for consensus reports and other guidance documents not captured by the PubMed search, was conducted using the same relevance criteria. Sources were also excluded if they were, primarily, based on existing international guidance. A total of 17 guidance reports were selected for appraisal by the authors (Figure 1).
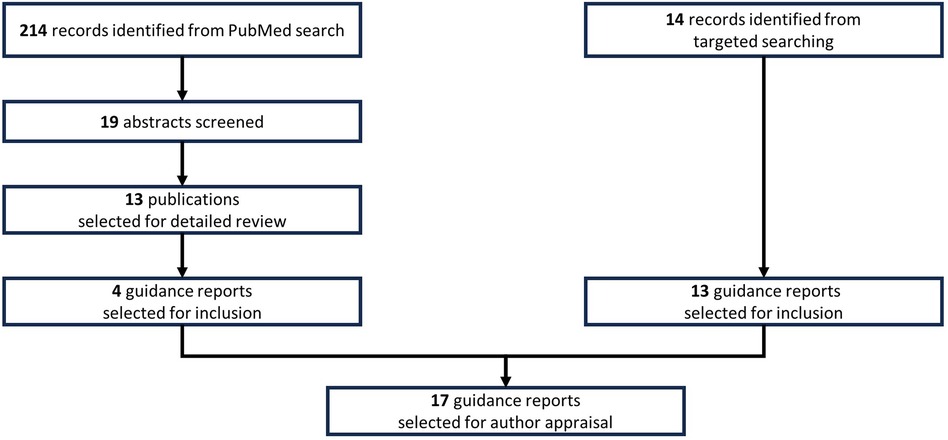
Figure 1 Literature searching conducted to identify clinical guidance reports containing recommendations on the diagnosis of asthma in school-age children.
A narrative approach was taken. The author group reviewed the clinical evidence for the use of objective tests to diagnose asthma in children across the identified guidance reports and concluded (by consensus through discussion, in person and virtually) on the clinical use of the following: (1) spirometry; (2) bronchodilator reversibility; (3) peak expiratory flow; (4) bronchial hyper-responsiveness tests; and (5) fractional exhaled nitric oxide. The clinical evidence was then compared with the diagnostic criteria for asthma used in previously conducted asthma prevention trials in children; these trials were identified through a separate targeted literature search, and a selection of examples were included in this review for illustrative purposes.
3 Review of clinical recommendations for the diagnosis of paediatric asthma from clinical guidelines
According to GINA, asthma is a heterogenous disease with symptoms that vary over time and in intensity (8). This heterogeneity is one of the major reasons why there are no uniform diagnostic criteria for asthma and, subsequently, why it is not possible to make unequivocal evidence-based recommendations for diagnosing asthma in clinical practice (21, 22). Various national and international initiatives, guidelines, and consensus reports provide recommendations for diagnosing asthma in children (summarised in Table 1). Whilst there are similarities between these sources, a substantial amount of variation exists, highlighting the need for standardised diagnostic criteria for paediatric asthma. This section reviews and evaluates these clinical recommendations.
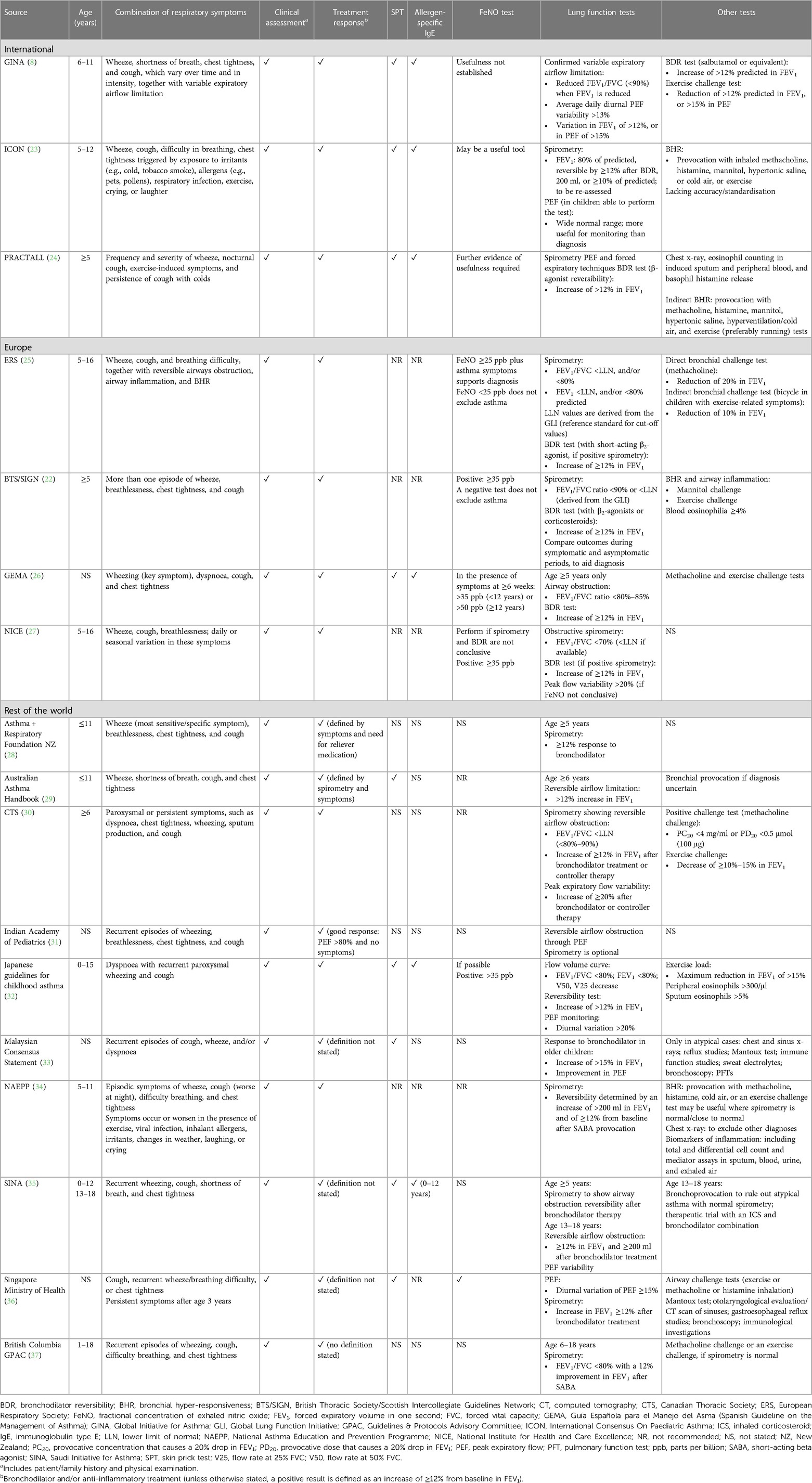
Table 1 Recommendations from international and national clinical guidance reports for the diagnosis of paediatric asthma.
3.1 Current approach to diagnosing asthma in children
Existing clinical guidance applies mostly to children aged ≥5 years old and recommends performing a clinical assessment (respiratory symptoms, patient/family history, physical examination) and pre- and post-bronchodilator spirometry [to evaluate bronchodilator reversibility (BDR)], as part of the diagnostic work-up for asthma (8, 22–37). Generally, the various guidelines recommend diagnosing asthma through combinations of respiratory symptoms (e.g., wheeze, cough, dyspnoea/shortness of breath, chest tightening) (8, 22–37). Characteristic symptom patterns include the presence of more than one respiratory symptom, symptoms that are often worse at night or early in the morning, and which vary over time and in intensity (8, 24, 26–37). In children, respiratory symptoms can be triggered by respiratory viral infections, exposure to cold, aeroallergens, pollution, and physical activity (among other factors) (8, 23, 24, 26, 28, 29, 34, 35). Objective tests to evaluate lung function or airway inflammation are used to support a diagnosis of asthma (Table 2); these tests include spirometry, peak flow variability, bronchial hyper-responsiveness (BHR; direct and indirect tests), and fractional concentration of exhaled nitric oxide (FeNO) (8, 22–37). The recommended objective test differs depending on the source of clinical guidance (8, 22–37). Ideally, objective testing would be performed before initiating inhaled corticosteroid (ICS) treatment to avoid influencing the results, but the clinical guidance is variable (8, 22–37).
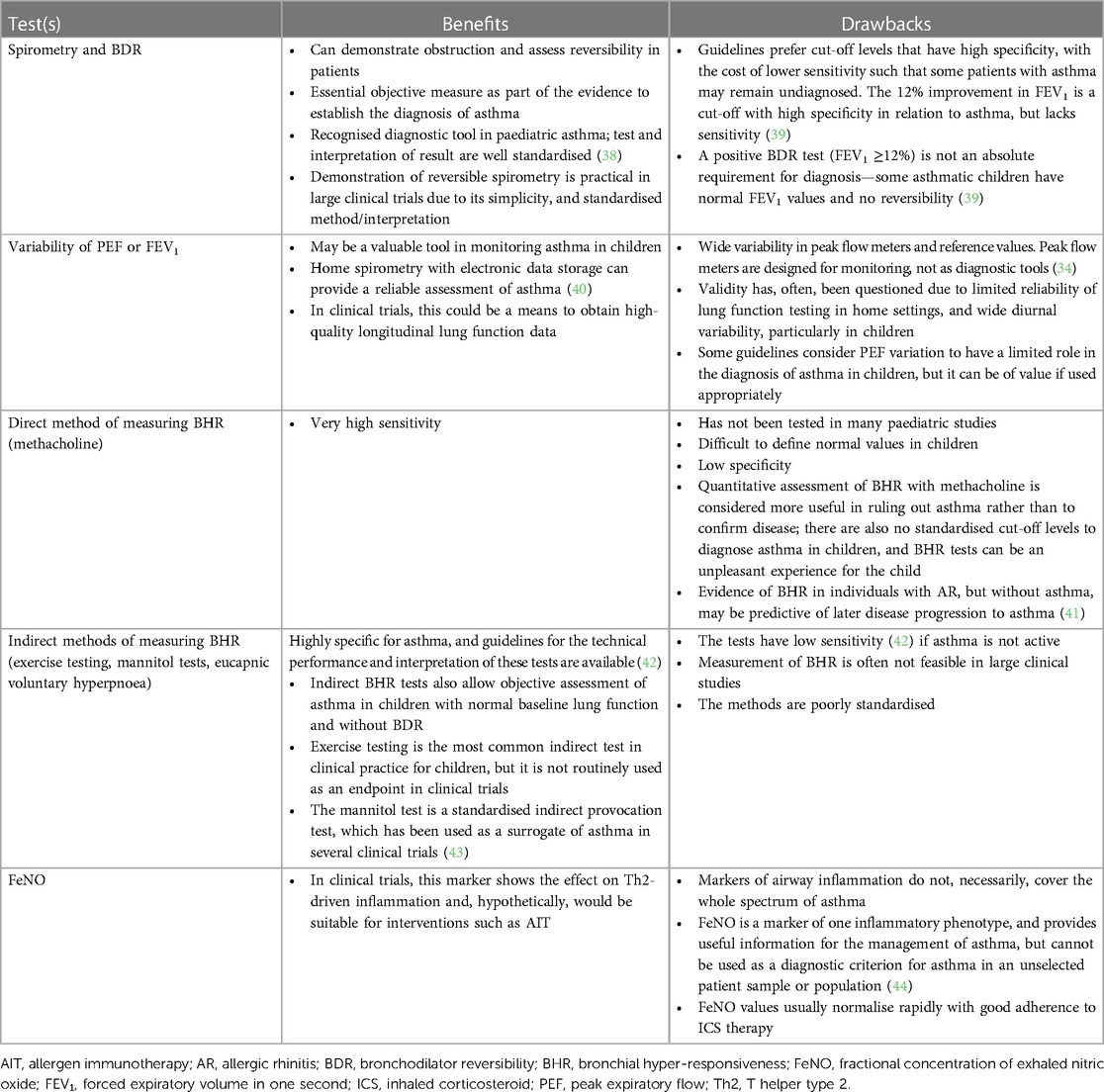
Table 2 Summary of objective tests for diagnosing asthma in school-age children as recommended in clinical guidelines.
3.1.1 Spirometry to detect airflow limitation
The most frequently used definition for airflow limitation in spirometry is the forced expiratory volume in one second to forced vital capacity (FEV1/FVC) ratio; the thresholds used to indicate airflow limitation can differ between clinical guidelines (see Table 1) (8, 22, 25–27, 30, 32, 37). For example, the UK National Institute for Health and Care Excellence (NICE) defines airflow obstruction as an FEV1/FVC ratio of <70% (27), whereas the GINA specifies <90% as the threshold (8). The British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) state that, in young children, the FEV1/FVC ratio can be as high as 90% and, therefore, the commonly used fixed value of 70% considerably underestimates airflow limitation (22). The European Respiratory Society (ERS) has championed a shift to using lower limits of normality (LLN) as the reference standard for spirometry to support a diagnosis of asthma; LLN values have been calculated for different age groups by the Global Lung Function Initiative (25, 44). The ERS guidance recommends using a threshold FEV1/FVC ratio, which is <LLN or <80% predicted (25). The use of LLN values is also recommended in the guidance from NICE, BTS/SIGN, and the Canadian Thoracic Society (CTS) (21, 27, 30). Although many children from the age of 5 years are able to perform reproducible spirometry if coached by an experienced technician and with visual incentives, according to GINA (8), it is important to note that some children are incapable of performing sufficient spirometry testing in clinical practice (25).
Our consensus is that, despite the challenges of performing spirometry in children, spirometric testing is fundamental to the assessment of asthma, and should use LLN values as the reference standard.
3.1.2 Bronchodilator reversibility
Some clinical guidelines recommend that, where spirometry is suggestive of asthma, a BDR test should be performed to confirm the diagnosis—generally, an increase in FEV1 of ≥12% is considered indicative of asthma (8, 25–29, 35, 37). However, there is considerable variation in normal FEV1 between different children meaning that a value in the normal range is not conclusive of normality for individual children. The latest ERS technical standard on interpreting spirometry states an increase of ≥10% of the predicted FEV1 as a threshold for a positive bronchodilator response (45). Spanish guidelines state that an 8% increase in FEV1 may better define the bronchodilator response in children (26). Guidelines from Malaysia recommend a 15% increase (older children) (33), whereas an increase of ≥12% is recommended in Singapore (36).
Our consensus is that a BDR test should be performed in children, regardless of FEV1 and the FEV1/FVC ratio. BDR tests should be repeated during symptomatic periods to establish a bronchodilator response (which may also be useful for differential diagnosis), since airway obstruction can be limited when the child is asymptomatic (22, 25).
3.1.3 Peak expiratory flow variability
Measuring peak expiratory flow (PEF) variability is recommended as a supportive objective test for children in some clinical guidelines (8, 23, 24, 27, 31–33, 35, 36) but not in others (22, 25, 26, 28, 29, 34, 35, 37), perhaps because it is less reliable than the alternative measure, FEV1 (which is measured in controlled settings) (8). The National Asthma Education and Prevention Program (NAEPP) Expert Panel Report recommends that peak flow meters function better as tools for asthma monitoring, rather than for diagnosis (34). In contrast, the NICE guidelines recommend measuring PEF variability for 2–4 weeks in children, where there is diagnostic uncertainty following an initial assessment (27). The recommended threshold for PEF variability differs between clinical guidelines (see Table 1).
Our consensus is that, for diagnostic purposes, only a PEF variability of ≥20% should be considered suggestive of asthma, in children who are able to perform repeatable tests.
3.1.4 Bronchial hyper-responsiveness tests
Many clinical guidelines recommend BHR tests as a supportive objective diagnostic test for asthma in children (8, 22–27, 29, 30, 32, 34–37). Direct BHR tests involve challenging with methacholine (or histamine), which interacts directly with muscarinic receptors on airway smooth muscle, resulting in contraction and airway narrowing. Indirect BHR tests, such as an exercise or mannitol challenge, elicit bronchoconstriction indirectly through pathways that trigger the narrowing of airways (42, 46). Although such measures can provide valuable supportive evidence (e.g., to establish asthma severity), there is a lack of clarity on the clinical definition of BHR in children. BHR is a hallmark of asthma, but it is a dynamic property—the presence and severity of BHR varies over time, influenced by disease activity, certain triggers, and treatment (47, 48). Furthermore, the quantitative assessment of methacholine responsiveness may be affected by technical factors in the administration of the test substance (46), and by dose–response characteristics that depend on the patient's body size (49). In adults, the association between BHR and asthma is quite strong, but the situation is less clear for children (50). Not all children with recurrent episodes of wheezing have increased BHR, and some children who do not have respiratory symptoms show signs of BHR (50, 51). Furthermore, recent data suggest that, in children with allergic sensitisation, BHR often appears after the onset of respiratory symptoms (52). Most clinical recommendations/guidelines endorse exercise challenge tests as an indirect method of assessing BHR (8, 22–26, 30, 34, 36, 37). Such physiological tests reflect the real-life clinical impact of asthma on children, confirming the relevance of these tests in the clinical evaluation of asthma. However, given that exercise-induced bronchospasm responds rapidly to ICS treatment, exercise challenge tests may be less helpful in patients who are currently receiving ICS treatment.
Our consensus is that exercise tests (running test or standardised exercise challenge test) can be valuable diagnostic tools in paediatric asthma.
3.1.5 Fractional exhaled nitric oxide
FeNO is a marker of type 2 inflammation (22). Perhaps the greatest discord between different clinical guidelines is in the use of the FeNO test as part of the diagnostic work-up for asthma. Some guidelines recommend the use of FeNO (22, 25–27, 32), others highlight that it may be a useful tool (23, 36), while some are of the opinion that the usefulness of FeNO is not yet established (8, 24). The ERS guidelines state that FeNO testing is relatively simple, non-invasive, and accepted by children and their caregivers (25). In contrast, FeNO is not recommended in the guidance from the CTS or the National Asthma Council of Australia (29, 30). Where recommended, the threshold value for a positive FeNO test differs between ≥20 parts per billion (ppb) and 35 ppb depending on the guideline (22, 25–27, 32). The values used to define a positive FeNO test can also be dependent on other factors, such as steroid use (22), and the presence of allergies (atopy is significantly associated with higher levels of FeNO (53) or an airway infection (54). Additionally, in healthy children, FeNO is significantly dependent on the individual's body size (55).
Our consensus is that the FeNO test is regarded as providing supportive, but not diagnostic, evidence for asthma in children, particularly those who are sensitised to allergens.
3.1.6 Navigating the challenges of diagnosing paediatric asthma
Existing clinical guidance highlights the challenges associated with diagnosing asthma in children:
1. Symptoms suggestive of asthma can result from several different conditions, which underlines the importance of considering differential diagnoses (8). Other illnesses, such as viral respiratory tract infections, can cause children to wheeze (8), manifesting as transient obstructive lung function that is reversible with a bronchodilator.
2. Significant BDR is often not observed when children are well (regardless of treatment with ICSs) and may be evident in children without asthma (e.g., following lower respiratory tract infections).
3. BHR is observed in children with AR, but without asthma (56), complicating its use as a diagnostic test for asthma in atopic children.
4. Elevated FeNO levels can be observed in children with AR (57), or in asymptomatic children with allergic sensitisations (58).
In clinical practice, algorithms combining a history, or presence of, respiratory signs and symptoms with supportive objective tests, are important in the diagnosis of asthma. No single diagnostic test can appropriately diagnose new-onset paediatric asthma and, therefore, the combination of different tests and patient clinical history must be considered. However, the Swiss Paediatric Airway Cohort study showed that the NICE and GINA algorithms for the diagnosis of paediatric asthma in children aged 5–17 years are challenging to apply in an outpatient setting and did not agree well with the diagnosis made by pulmonologists (59).
3.1.7 Summary of recommendations from clinical guidance
Despite an overall lack of consensus in the published clinical guidance, there are similarities between the various recommendations for diagnosing asthma in children, which typically involve supplementing medical history with objective measures of lung function. Most guidelines agree that no single symptom, sign, or test can be used alone to diagnose paediatric asthma, and that the predictive value of diagnostic tests is influenced by the context. A broader approach to diagnosis, involving a period of observation of the variable symptoms/signs of asthma to confirm or exclude asthma, may be preferable.
4 Review of new-onset asthma definitions in paediatric asthma prevention trials
The published European Medicines Agency (EMA) guidance for the development of medications for asthma is focused on the symptomatic treatment of asthma. It does not include standard criteria for diagnosing asthma, or recommendations for primary endpoints to assess the prevention of new-onset asthma in clinical trials (60, 61). Therefore, the guidance may not be directly relevant to clinical trials of treatments designed to prevent new-onset asthma (61). Instead, the guidance states that the diagnostic criteria for asthma in children aged ≥6 years should be based on the recommendations outlined in existing clinical guidelines (61). Consequently, the criteria for diagnosing asthma vary between the numerous clinical trials that have been conducted to evaluate the potential of different treatments in preventing the onset of asthma in children (Table 3) (62–70).
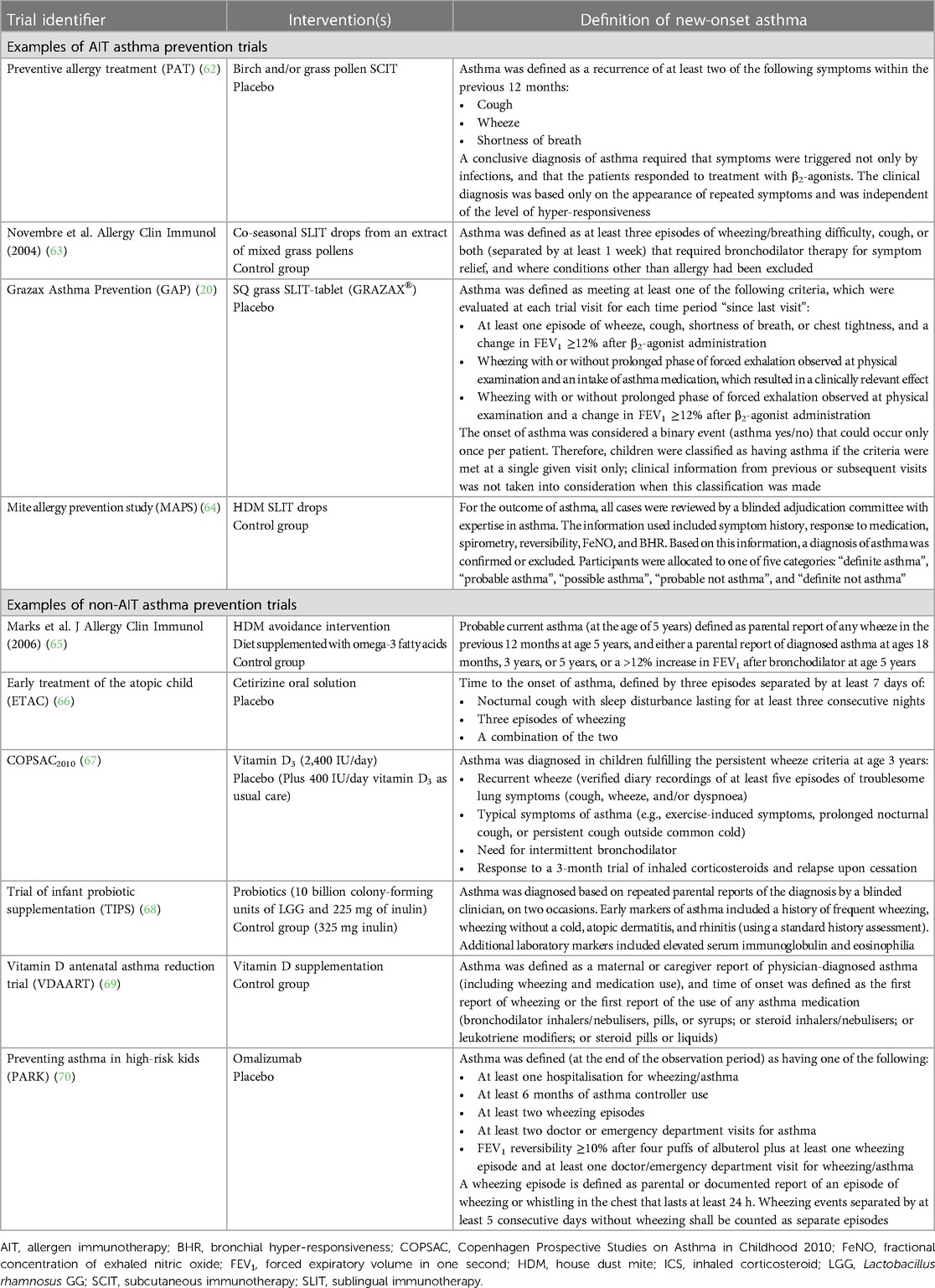
Table 3 Definitions of new-onset asthma used in paediatric clinical trials assessing asthma prevention.
Although many of these asthma prevention trials defined new-onset asthma primarily by asthma symptoms and medication use, the variation in criteria highlights the lack of a standard definition for new-onset asthma in paediatric clinical research. This section focuses on selected trials that have investigated AIT in preventing the development of asthma, alongside some examples of non-AIT asthma prevention trials.
4.1 Asthma prevention trials with allergen immunotherapy (AIT)
To illustrate how different definitions of asthma onset may impact the results in asthma prevention trials, we describe two large, randomised trials that have assessed the preventive effect of AIT on asthma development.
The Preventive Allergy Treatment (PAT) trial was a randomised open-label trial investigating the preventive effect of AIT on the risk of developing asthma (62). The trial randomised 205 children (aged 6–14 years) with grass or birch pollen AR to either symptom-relieving medication alone or symptom-relieving medication plus SQ subcutaneous immunotherapy (SCIT) (grass and/or birch) (62). Children with asthma requiring daily asthma treatment were excluded (62). Asthma was defined by trial investigators, based on the recurrence of at least two asthma symptoms (cough, wheeze, and/or shortness of breath) and responsiveness to β2-agonist treatment (confirmation of the asthma diagnosis by an objective test was not required) (Table 3) (62). Three years of SQ SCIT treatment increased the likelihood that children did not develop asthma vs. children who were not treated with SQ SCIT {odds ratio [OR] = 2.52; [95% confidence intervals (CI): 1.3, 5.1]; p < 0.05} (62). This clinical benefit for the prevention of new-onset asthma was observed long term, for up to 7 years after SCIT treatment completion [OR at Year 10 = 2.5 (95% CI: 1.1, 5.9)] (41).
The later GAP trial was conducted to investigate asthma prevention with SQ grass sublingual immunotherapy (SLIT) tablet vs. placebo in children with grass pollen AR, using a blinded randomised controlled trial design (20). The 5-year GAP trial enrolled 812 children (aged 5–12 years) and included a 3-year treatment course followed by a 2-year follow-up period (20). Children with any history of asthma and/or wheezing, or signs of asthma, were excluded (20). The protocol-specific asthma diagnostic criteria were devised during consultation with the EMA. This approach required an objective measure (BDR) in addition to an evaluation of asthma symptoms and medication use, resulting in a more stringent definition of asthma compared to that used in other trials with a similar objective (i.e., to evaluate asthma prevention) (Table 3) (20). No effect of SQ grass SLIT-tablet was observed on the primary endpoint of time to onset of protocol-defined asthma vs. placebo (20). Concerningly, some of the children who met the diagnostic criteria for asthma in the first part of the 3-year treatment period did not show signs of asthma later in the trial, whereas many other children who did not meet the diagnostic criteria during the trial did show signs suggestive of asthma (20). This finding indicated, to the investigators, that the definition of new-onset asthma used in the trial had not performed well—a probable reason being that, in children, a diagnosis of asthma is difficult to make on the basis of a single point-in-time evaluation that relies on demonstrating reversible lung function impairment. Rather, the diagnosis of asthma, in the context of clinical trials, needs to be based on a combined clinical assessment with objective testing conducted over a longer observation period, as is usually performed in routine clinical practice (20, 22, 25, 71, 72). Although a post hoc analysis conducted at the end of the 5-year trial period showed a significant effect for the SQ grass SLIT-tablet on reduction of asthma symptoms and asthma medication use (20), this is insufficient to confirm a diagnosis of asthma.
4.2 Non-AIT asthma prevention trials
We also examined a few asthma prevention trials that investigated interventions other than AIT. For these trials, the diagnostic criteria were based mainly around clinical symptoms (and also asthma medication use in some trials) and are, therefore, less stringent than the criteria used in the AIT trials (Table 3). Of the non-AIT trials listed in Table 3, none of the interventions showed a beneficial effect on asthma prevention, despite the different asthma diagnostic criteria applied across the trials (65–69). The “Preventing Asthma in High Risk Kids (PARK)” trial is ongoing (70).
4.3 Summary of asthma prevention trials
In summary, for clinical trials in asthma (including paediatric AIT and non-AIT trials), the regulatory recommendation is to diagnose asthma according to the clinical guidelines, which are clearly variable; however, the dynamic nature of the disease must also be considered. The paediatric asthma prevention trials conducted highlight the challenges of defining diagnostic criteria for asthma and, consequently, there is a need for standardised criteria to define new-onset asthma in a paediatric clinical trial setting.
5 Suggestions for the diagnosis of new-onset asthma in future paediatric clinical trials
In this section, we consider how new-onset asthma could be diagnosed in future clinical trials. The recurring and dynamic nature of asthma creates challenges when diagnosing new-onset asthma, and emphasises the need for regular evaluation over time with standardised objective measurements, as is done in routine clinical practice.
5.1 Self-reported symptoms
Chronicity and recurrence of symptoms (self-reports using patient-reported outcomes) need to be captured with a follow-up lasting 6–12 months. Patients should have experienced at least two episodes of at least two different characteristic asthma symptoms (including wheeze, shortness of breath, chest tightness, cough, exercise-induced symptoms). When chronic symptoms are documented, patient-reported symptom relief with β2-agonist bronchodilator treatment should be evaluated (indicating reversibility). Documented symptom relief in the presence of chronic symptoms is suggestive of “possible” asthma (Figure 2).
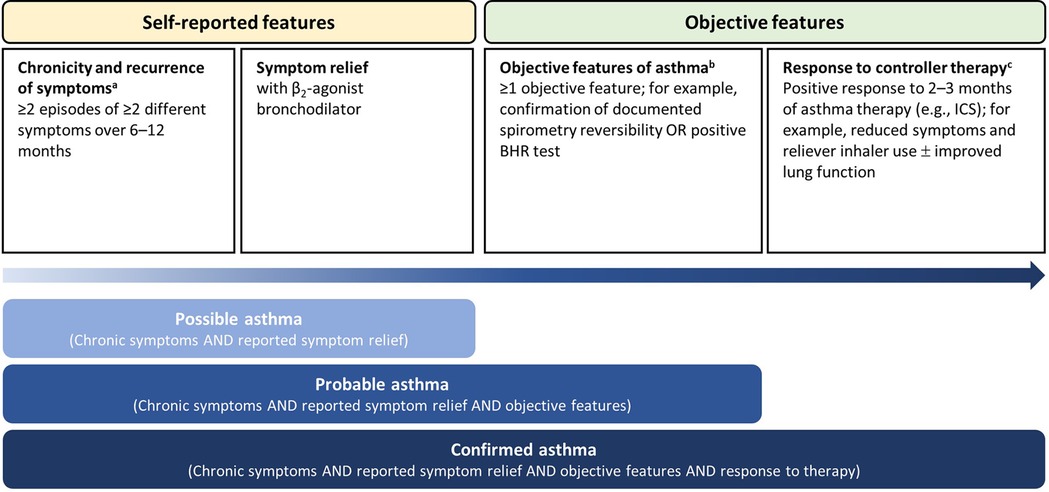
Figure 2 A suggested approach to diagnose new-onset asthma in a paediatric clinical trial (school-age children). aIncluding wheeze, shortness of breath, chest tightness, cough, exercise-induced symptoms, persistence of cough with colds, and daily or seasonal variation in symptoms. Symptoms may also be triggered by exposure to irritants (cold, tobacco smoke), allergens (pets, pollen, house dust mite, etc.), respiratory infection, exercise, crying, or laughter. Exclude symptoms of alternative diagnosis. bPreferably, objective diagnostic tests should not be performed during treatment with controller medication. cIn the case of poor response to controller therapy, a diagnosis of asthma is unlikely if ICS has been administered at an adequate dose with optimal inhalation technique and adherence. BHR, bronchial hyper-responsiveness; ICS, inhaled corticosteroid.
5.2 Objective features
The Lancet Asthma Commission Report emphasises the importance of performing objective measurements (73). We suggest that objective evidence should be obtained either as spirometry reversibility with an inhaled β2-agonist or a positive BHR test (methacholine or exercise test). Measuring BDR is an important clinical tool to monitor the effect of bronchodilators, but also to document reversible airway obstruction. Given that objective tests differ in sensitivity and specificity (Table 2), the diagnostic rate of asthma would vary dependent on the specific criteria used for the objective test. Since the full range of tests may not be available in all centres, the appropriate objective test should be tailored to each trial. Our preference would be for spirometry reversibility in children ≥6 years of age conducted before initiation of ICS therapy. Data from objective testing undertaken by other healthcare professionals should also be assessed as part of the trial protocol to minimise the chance that ICS treatment has already been initiated before the trial assessment and reversibility was missed. A BHR test may be a helpful supplementary objective marker to define asthma (42), even during periods of normal baseline lung function.
5.3 A suggested approach in school-age children
In a clinical trial setting, it is important to allow for unscheduled visits and to recall children when they are symptomatic to maximise the chance of capturing data when they have objective features and chronic symptoms. In cases where chronic symptoms are documented, patient-reported symptom relief with a β2-agonist bronchodilator has been reported (indicating reversibility), and there is evidence of positive objective tests (e.g., documented spirometry reversibility), we suggest that a diagnosis of “probable” asthma can be made (Figure 2). We also suggest 2–3 months of controller medication treatment with an ICS (Figure 2), and to reassess the treatment response through clinical assessment and objective measures, such as lung function, to confirm an asthma diagnosis. A positive response may include a reduction in reported symptoms and in the use of reliever inhaler, as well as improved lung function (on objective measures, such as spirometry and reversibility); this would deliver a conclusion of “confirmed” asthma (Figure 2). If the response to asthma therapy is poor, correct inhaler technique and adherence to the medication should be checked; further testing should be arranged, and alternative diagnoses considered.
6 Discussion
Review of the published clinical guidelines emphasises the importance of a broader approach to the diagnosis of asthma in children, including observation of the variable symptoms/signs of asthma over time supplemented with objective measures of lung function. Although a full consensus across clinical guidelines on the use and thresholds of different lung function tests is lacking, most guidelines agree that the predictive value of diagnostic tests is influenced by the context, and that no single test is sufficient to diagnose paediatric asthma alone.
The BTS/SIGN guidance acknowledges that asthma status and the outcome of diagnostic tests can vary over time, meaning that objective tests performed when patients are asymptomatic or during an “inactive period” (i.e., not having received a prescription for a year) may produce false negative results (22). Likewise, the PRACTALL consensus report highlights that, often, a diagnosis of asthma in children is possible only by understanding the symptom patterns over an extended period of time, observing a child's response to bronchodilator and/or anti-inflammatory treatment at different times (24).
It is important to ensure that the objective test of choice to confirm a diagnosis of asthma is appropriate for the age of the child. Objective tests are useful only when they are consistently performed properly and, therefore, should not be used for diagnosing asthma without evaluation of a patient's technique. Furthermore, it is important to remember that a normal result on any given objective test does not exclude asthma (22). Airway obstruction can be limited when the patient is asymptomatic or in the early onset of asthma symptoms (22, 25). Therefore, it is important to consider the optimal timing and frequency of objective tests in diagnosing new-onset asthma. Given that different centres employ different tests and that some tests are not appropriate for all age groups, an element of heterogeneity will be introduced into the definition due to the differences in sensitivity and specificity between the tests (Table 2). However, the inclusion of an objective component at the correct time in the trial pathway should improve diagnostic accuracy compared with the current situation.
Recent evidence-based guidance on defining new-onset asthma from clinical guidelines has not been implemented into clinical trial protocols, which has been to their detriment. Review of published paediatric asthma prevention trials showed that many different diagnostic criteria for new-onset asthma have been applied, and that many trials were focussed, primarily, on asthma symptoms and medication use. The variation in asthma diagnostic criteria highlights the lack of a standard definition for new-onset asthma in paediatric clinical research.
From asthma prevention trials using AIT and other interventions, we have learned that evaluation of chronic symptoms is important to establish a diagnosis of new-onset asthma. An assessment of asthma onset at one single timepoint can lead to both under- and over-diagnosis (6). Asthma is a dynamic condition. When diagnosing asthma, it is important to evaluate the chronicity and persistence of more than one clinical symptom, perform one or more objective tests, and monitor the clinical response to asthma treatment. We have made suggestions for diagnosing new-onset asthma in paediatric clinical trials, which encompass these key considerations. The suggestions aim to improve the accuracy of diagnosing asthma in school-age children, and the design and results of future clinical trials. In the absence of agreed standardised worldwide diagnostic criteria for asthma in children, we hope that our suggestions bring the definition of new-onset asthma used in clinical trials in line with current evidence-based recommendations and, in doing so, we may help to diagnose new-onset asthma in future paediatric asthma prevention trials.
Author contributions
GR: Conceptualization, Data curation, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EV: Conceptualization, Methodology, Validation, Writing – review & editing. SH: Conceptualization, Methodology, Validation, Writing – review & editing. PAE: Conceptualization, Methodology, Validation, Writing – review & editing. MJM: Conceptualization, Methodology, Validation, Writing – review & editing. KCLC: Conceptualization, Methodology, Validation, Writing – review & editing. RK: Conceptualization, Methodology, Validation, Writing – review & editing. LPM: Conceptualization, Methodology, Validation, Writing – review & editing.
Funding
The authors declare that no funding was received for the work conducted to inform this article, specifically. However, most authors received support from ALK-Abello A/S for their role as investigators in the GAP trial, from which this work has evolved.
Acknowledgments
All authors have had access to the data and have reviewed and approved the final manuscript. Writing and editorial assistance was provided by Cambridge—a Prime Global Agency (Knutsford, UK), funded by ALK-Abelló.
Conflict of interest
GR was an investigator in the ALK-Abelló Grazax Asthma Prevention (GAP) trial, a consultant/speaker for ALK-Abelló, a consultant for AstraZeneca, an author of the British Thoracic Society/Scottish Intercollegiate Guidelines Network (SIGN) guideline, President of the British Society for Allergy & Clinical Immunology (BSACI), has received funding for asthma studies from the National Institute for Health and Care Research (NIHR), National Institutes of Health (NIH), the EU, and the Medical Research Council (MRC). EV and SH were investigators in the ALK-Abelló GAP trial. PAE was an investigator in the ALK-Abelló GAP trial, is a consultant/speaker for ALK-Abelló, and has participated in an Advisory Board for Allergopharma. RK was a member of the ALK-Abelló GAP trial Steering Committee and an investigator in the ALK-Abelló GAP trial. ALK-Abello A/S provided funding for the writing and editorial support of the article and, also, reviewed the manuscript for scientific integrity. ALK-Abello A/S was not involved in the design, collection, analysis, interpretation of data, or the decision to submit for publication.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AIT, allergen immunotherapy; AR, allergic rhinitis; BDR, bronchodilator reversibility; BHR, bronchial hyper-responsiveness; BTS/SIGN, British Thoracic Society/Scottish Intercollegiate Guidelines; CTS, Canadian Thoracic Society; EAACI, European Academy of Allergy and Clinical Immunology; EMA, European Medicines Agency; ERS, European Respiratory Society; FeNO, fractional concentration of exhaled nitric oxide; FEV1/FVC, forced expiratory volume in one second to forced vital capacity; GAP, Grazax Asthma Prevention; GINA, Global Initiative for Asthma; ICS, inhaled corticosteroid; LLN, lower limits of normality; NAEPP, National Asthma Education and Prevention Program; NICE, National Institute for Health and Care Excellence; PARK, preventing asthma in high risk kids; PAT, preventive allergy treatment; PEF, peak expiratory flow; ppb, parts per billion; SCIT, subcutaneous immunotherapy.
References
2. World Health Organization (WHO). Asthma. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/asthma (Accessed July 20, 2023).
3. Pijnenburg MW, Frey U, De Jongste JC, Saglani S. Childhood asthma: pathogenesis and phenotypes. Eur Respir J. (2022) 59(6):2100731. doi: 10.1183/13993003.00731-2021
4. Raghavan D, Jain R. Increasing awareness of sex differences in airway diseases. Respirology. (2016) 21(3):449–59. doi: 10.1111/resp.12702
5. Latour M, Lal D, Yim MT. Sex differences in airway diseases. Otolaryngol Clin North Am. (2023) 56(1):55–63. doi: 10.1016/j.otc.2022.09.004
6. Kavanagh J, Jackson DJ, Kent BD. Over- and under-diagnosis in asthma. Breathe (Sheff). (2019) 15(1):e20–7. doi: 10.1183/20734735.0362-2018
7. Global Asthma Network. The Global Asthma Report 2018. Auckland, New Zealand: Global Asthma Network (2018). Available online at: http://www.globalasthmareport.org (Accessed July 20, 2023).
8. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. Updated. (2022). Available online at: https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf (Accessed July 20, 2023).
9. Ferrante G, La Grutta S. The burden of pediatric asthma. Front Pediatr. (2018) 6:186. doi: 10.3389/fped.2018.00186
10. Mirabelli MC, Hsu J, Gower WA. Comorbidities of asthma in U.S. children. Respir Med. (2016) 116:34–40. doi: 10.1016/j.rmed.2016.05.008
11. Nunes C, Ladeira S. Asthma, from childhood to adulthood: a prospective 20-year longitudinal study of a cohort of asthmatics. J Investig Allergol Clin Immunol. (2002) 12(4):242–9.12926183
12. Phelan PD, Robertson CF, Olinsky A. The Melbourne asthma study: 1964–1999. J Allergy Clin Immunol. (2002) 109(2):189–94. doi: 10.1067/mai.2002.120951
13. Ziyab AH, Karmaus W, Zhang H, Holloway JW, Steck SE, Ewart S, et al. Allergic sensitization and filaggrin variants predispose to the comorbidity of eczema, asthma, and rhinitis: results from the Isle of Wight birth cohort. Clin Exp Allergy. (2014) 44(9):1170–8. doi: 10.1111/cea.12321
14. Pakkasela J, Ilmarinen P, Honkamäki J, Tuomisto LE, Andersén H, Piirilä P, et al. Age-specific incidence of allergic and non-allergic asthma. BMC Pulm Med. (2020) 20(1):9. doi: 10.1186/s12890-019-1040-2
15. Passalacqua G, Rogkakou A, Mincarini M, Canonica GW. Allergen immunotherapy in asthma; what is new? Asthma Res Pract. (2015) 1:6. doi: 10.1186/s40733-015-0006-2
16. Halken S, Larenas-Linnemann D, Roberts G, Calderón MA, Angier E, Pfaar O, et al. EAACI guidelines on allergen immunotherapy: prevention of allergy. Pediatr Allergy Immunol. (2017) 28(8):728–45. doi: 10.1111/pai.12807
17. von Mutius E, Smits HH. Primary prevention of asthma: from risk and protective factors to targeted strategies for prevention. Lancet. (2020) 396(10254):854–66. doi: 10.1016/S0140-6736(20)31861-4
18. Gradman J, Halken S. Preventive effect of allergen immunotherapy on asthma and new sensitizations. J Allergy Clin Immunol Pract. (2021) 9(5):1813–7. doi: 10.1016/j.jaip.2021.03.010
19. Kristiansen M, Dhami S, Netuveli G, Halken S, Muraro A, Roberts G, et al. Allergen immunotherapy for the prevention of allergy: a systematic review and meta-analysis. Pediatr Allergy Immunol. (2017) 28(1):18–29. doi: 10.1111/pai.12661
20. Valovirta E, Petersen TH, Piotrowska T, Laursen MK, Andersen JS, Sørensen HF, et al. Results from the 5-year SQ grass sublingual immunotherapy tablet asthma prevention (GAP) trial in children with grass pollen allergy. J Allergy Clin Immunol. (2018) 141(2):529–38.e13. doi: 10.1016/j.jaci.2017.06.014
21. Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet. (2018) 391(10122):783–800. doi: 10.1016/S0140-6736(17)33311-1
22. British Thoracic Society and Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: a National Clinical Guideline. First published (2003). Revised edition published July 2019. Available online at: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/ (Accessed July 20, 2023).
23. Papadopoulos NG, Arakawa H, Carlsen KH, Custovic A, Gern J, Lemanske R, et al. International consensus on (ICON) pediatric asthma. Allergy. (2012) 67(8):976–97. doi: 10.1111/j.1398-9995.2012.02865.x
24. Bacharier LB, Boner A, Carlsen KH, Eigenmann PA, Frischer T, Götz M, et al. Diagnosis and treatment of asthma in childhood: a PRACTALL consensus report. Allergy. (2008) 63(1):5–34. doi: 10.1111/j.1398-9995.2007.01586.x
25. Gaillard EA, Kuehni CE, Turner S, Goutaki M, Holden KA, de Jong CCM, et al. European respiratory society clinical practice guidelines for the diagnosis of asthma in children aged 5–16 years. Eur Respir J. (2021) 58(5):2004173. doi: 10.1183/13993003.04173-2020
26. Plaza Moral V, Mostaza SA, Rodríguez CA, Gomez-Outes A, Gómez Ruiz F, López Vina A, et al. GEMA4.0. Spanish guideline on the management of asthma. J Investig Allergol Clin Immunol. (2016) 26(Suppl. 1):1–92. doi: 10.18176/jiaci.0065
27. National Institute for Health and Care Excellence (NICE). Asthma: Diagnosis, Monitoring and Chronic Asthma Management. NICE guideline. Published: 29 November 2017. Last updated March 2021. Available online at: https://www.nice.org.uk/guidance/ng80 (Accessed July 20, 2023).
28. Asthma Respiratory Foundation NZ. New Zealand Child Asthma Guidelines. (2020). Available online at: https://www.asthmafoundation.org.nz/assets/documents/ARF-NZ-Child-asthma-guidelines-update-30.6.20.pdf (Accessed July 20, 2023).
29. National Asthma Council. Australian Asthma Handbook v2.2. (2022). Available online at: https://www.asthmahandbook.org.au/ (Accessed July 20, 2023).
30. Yang CL, Hicks EA, Mitchell P, Reisman J, Podgers D, Hayward KM, et al. Canadian Thoracic society 2021 guideline update: diagnosis and management of asthma in preschoolers, children and adults. Can J Respir Crit Care Sleep Med. (2021) 5(6):348–61. doi: 10.1080/24745332.2021.1945887
31. Kumar L. Consensus guidelines on management of childhood asthma in India. Indian Pediatr. (1999) 36(2):157–65.10713809
32. Arakawa H, Adachi Y, Ebisawa M, Fujisawa T, Committee for Japanese Pediatric Guideline for Childhood Asthma, The Japanese Society of Pediatric Allergy and Clinical Immunology, The Japanese Society of Allergology. Japanese guidelines for childhood asthma 2020. Allergol Int. (2020) 69(3):314–30. doi: 10.1016/j.alit.2020.02.005
33. Academy of Medicine of Malaysia. Guidelines for the management of childhood asthma—a consensus statement. Med J Malaysia. (1997) 52(4):416–28.10968121
34. National Asthma Education and Prevention Program. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma—summary report 2007. J Allergy Clin Immunol. (2007) 120(Suppl 5):S94–138. doi: 10.1016/j.jaci.2007.09.043
35. Al-Moamary MS, Alhaider SA, Alangari AA, Idrees MM, Zeitouni MO, Al Ghobain MO, et al. The Saudi initiative for asthma—2021 update: guidelines for the diagnosis and management of asthma in adults and children. Ann Thorac Med. (2021) 16(1):4–56. doi: 10.4103/atm.ATM_697_20
36. Ministry of Health Singapore. Management of Asthma. (2008). Available online at: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/cpg_asthma.pdf (Accessed July 20, 2023).
37. BC Guidelines. Asthma in Children—Diagnosis and Management. (2015). Available online at: https://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc-guidelines/asthma-children-full-guideline-.pdf (Accessed July 20, 2023).
38. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. (2005) 26(2):319–38. doi: 10.1183/09031936.05.00034805
39. Murray C, Foden P, Lowe L, Durrington H, Custovic A, Simpson A. Diagnosis of asthma in symptomatic children based on measures of lung function: an analysis of data from a population-based birth cohort study. Lancet Child Adolesc Health. (2017) 1(2):114–23. doi: 10.1016/S2352-4642(17)30008-1
40. Brouwer AFJ, Roorda RJ, Duiverman EJ, Brand PLP. Reference values for peak flow and FEV1 variation in healthy schoolchildren using home spirometry. Eur Respir J. (2008) 32(5):1262–8. doi: 10.1183/09031936.00148107
41. Jacobsen L, Niggemann B, Dreborg S, Ferdousi HA, Halken S, Høst A. Specific immunotherapy has long-term preventive effect of seasonal and perennial asthma: 10-year follow-up on the PAT study. Allergy. (2007) 62(8):943–8. doi: 10.1111/j.1398-9995.2007.01451.x
42. Hallstrand TS, Leuppi JD, Joos G, Hall GL, Carlsen KH, Kaminsky DA, et al. ERS technical standard on bronchial challenge testing: pathophysiology and methodology of indirect airway challenge testing. Eur Respir J. (2018) 52(5):1801033. doi: 10.1183/13993003.01033-2018
43. Anderson SD. “Indirect” challenges from science to clinical practice. Eur Clin Respir J. (2016) 3:31096. doi: 10.3402/ecrj.v3.31096
44. Quanjer PH, Stanjevic S, Cole TJ, Baur X, Hall GL, Culver BH, et al. Multi-ethnic reference values for spirometry for the 3–95-year age range: the global lung function 2012 equations. Eur Respir J. (2012) 40(6):1324–43. doi: 10.1183/09031936.00080312
45. Stanojevic S, Kaminsky DA, Miller MR, Thompson B, Aliverti A, Barjaktarevic I, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. (2022) 60(1):2101499. doi: 10.1183/13993003.01499-2021
46. Coates AL, Wanger J, Cockcroft DW, Culver BH, Bronchoprovocation Testing Task Force: Carlsen K, Diamant Z, Gauvreau G, Hall GL, Hallstrand TS, Horvath I, de Jongh FHC, Joos G, Kaminsky DA, Laube BL, Leuppi JD, Sterk PJ. ERS Technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests. Eur Respir J. (2017) 49(5):1601526. doi: 10.1183/13993003.01526-2016
47. Comberiati P, Katial RK, Covar RA. Bronchoprovocation testing in asthma: an update. Immunol Allergy Clin North Am. (2018) 38(4):545–71. doi: 10.1016/j.iac.2018.06.010
48. Chapman DG, Irvin CG. Mechanisms of airway hyper-responsiveness in asthma: the past, present and yet to come. Clin Exp Allergy. (2015) 45(4):706–19. doi: 10.1111/cea.12506
49. Le Souëf PN, Sears MR, Sherrill D. The effect of size and age of subject on airway responsiveness in children. Am J Respir Crit Care Med. (1995) 152(2):576–9. doi: 10.1164/ajrccm.152.2.7633710
50. Law KW, Ng KK, Yuen KN, Ho CS. Detecting asthma and bronchial hyperresponsiveness in children. Hong Kong Med J. (2000) 6(1):99–104.10793409
51. Hopp RJ, Townley RG, Biven RE, Bewtra AK, Nair NM. The presence of airway reactivity before the development of asthma. Am Rev Respir Dis. (1990) 141(1):2–8. doi: 10.1164/ajrccm/141.1.2
52. Burman JI, Remes ST, Mäkelä MJ. Allergic sensitisation did not affect bronchial hyper-responsiveness in children without respiratory tract symptoms. Acta Paediatr. (2022) 111(2):424–31. doi: 10.1111/apa.16129
53. Scott M, Raza A, Karmaus W, Mitchell F, Grundy J, Kurukulaaratchy RJ, et al. Influence of atopy and asthma on exhaled nitric oxide in an unselected birth cohort study. Thorax. (2010) 65(3):258–62. doi: 10.1136/thx.2009.125443
54. de Gouw HWFM, Grünberg K, Schot R, Kroes AC, Dick EC, Sterk PJ. Relationship between exhaled nitric oxide and airway hyperresponsiveness following experimental rhinovirus infection in asthmatic subjects. Eur Respir J. (1998) 11(1):126–32. doi: 10.1183/09031936.98.11010126
55. Malmberg LP, Petäys T, Haahtela T, Laatikainen T, Jousilahti P, Vartiainen E, et al. Exhaled nitric oxide in healthy nonatopic school-age children: determinants and height-adjusted reference values. Pediatr Pulmonol. (2006) 41(7):635–42. doi: 10.1002/ppul.20417
56. Cibella F, Cuttitta G, La Grutta S, Hopps MR, Passalacqua G, Pajno GB, et al. Bronchial hyperresponsiveness in children with atopic rhinitis: a 7-year follow-up. Allergy. (2004) 59(10):1074–9. doi: 10.1111/j.1398-9995.2004.00559.x
57. Di Cara G, Bizzarri I, Fabiano C, Faina F, Di Cicco M, Rinaldi VE, et al. Prevalence of allergic rhinitis with lower airways inflammation: a new endotype with high risk of asthma development? J Paediatr Child Health. (2021) 57(12):1955–9. doi: 10.1111/jpc.15626
58. Yao TC, Ou LS, Lee WI, Yeh KW, Chen LC, Huang JL, et al. Exhaled nitric oxide discriminates children with and without allergic sensitization in a population-based study. Clin Exp Allergy. (2011) 41(4):556–64. doi: 10.1111/j.1365-2222.2010.03687.x
59. de Jong CCM, Pedersen ESL, Mozun R, Müller-Suter D, Jochmann A, Singer F, et al. Diagnosis of asthma in children: findings from the Swiss paediatric airway cohort. Eur Respir J. (2020) 56(5):2000132. doi: 10.1183/13993003.00132-2020
60. European Medicines Agency (EMA). Guideline on the Clinical Development of Products for Specific Immunotherapy for the Treatment of Allergic Diseases. CHMP/EWP/18504/2006. (2008). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-development-products-specific-immunotherapy-treatment-allergic-diseases_en.pdf (Accessed July 20, 2023).
61. European Medicines Agency (EMA). Guideline on the Clinical Investigation of Medicinal Products for the Treatment of Asthma. CHMP/EWP/2922/01 Rev.1. (2015). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-clinical-investigation-medicinal-products-treatment-asthma_en.pdf (Accessed July 20, 2023).
62. Möller C, Dreborg S, Ferdousi HA, Halken S, Høst A, Jacobsen L, et al. Pollen immunotherapy reduces the development of asthma in children with seasonal rhinoconjunctivitis (the PAT-study). J Allergy Clin Immunol. (2002) 109(2):251–6. doi: 10.1067/mai.2002.121317
63. Novembre E, Galli E, Landi F, Caffarelli C, Pifferi M, De Marco E, et al. Coseasonal sublingual immunotherapy reduces the development of asthma in children with allergic rhinoconjunctivitis. J Allergy Clin Immunol. (2004) 114(4):851–7. doi: 10.1016/j.jaci.2004.07.012
64. Alviani C, Roberts G, Mitchell F, Martin J, Zolkipli Z, Michaelis LJ, et al. Primary prevention of asthma in high-risk children using HDM SLIT: assessment at age 6 years. J Allergy Clin Immunol. (2020) 145(6):1711–3. doi: 10.1016/j.jaci.2020.01.048
65. Marks GB, Mihrshahi S, Kemp AS, Tovey ER, Webb K, Almqvist C, et al. Prevention of asthma during the first 5 years of life: a randomised controlled trial. J Allergy Clin Immunol. (2006) 118(1):53–61. doi: 10.1016/j.jaci.2006.04.004
66. Warner JO, ETAC Study Group. A double-blinded, randomized, placebo-controlled trial of cetirizine in preventing the onset of asthma in children with atopic dermatitis: 18 months’ treatment and 18 months’ post treatment follow-up. J Allergy Clin Immunol. (2001) 108(6):929–37. doi: 10.1067/mai.2001.120015
67. Chawes BL, Bønnelykke K, Stokholm J, Vissing NH, Bjarnadóttir E, Schoos AM, et al. Effect of vitamin D3 supplementation during pregnancy on risk of persistent wheeze in the offspring: a randomized clinical trial. JAMA. (2016) 315(4):353–61. doi: 10.1001/jama.2015.18318
68. Cabana MD, McKean M, Caughey AB, Fong L, Lynch S, Wong A, et al. Early probiotic supplementation for eczema and asthma prevention: a randomised controlled trial. Pediatrics. (2017) 140(3):e20163000. doi: 10.1542/peds.2016-3000
69. Litonjua AA, Carey VJ, Laranjo N, Stubbs BJ, Mirzakhani H, O'Connor GT, et al. Six-year follow-up of a trial of antenatal vitamin D for asthma reduction. N Engl J Med. (2020) 382(6):525–33. doi: 10.1056/NEJMoa1906137
70. Phipatanakul W, Mauger DT, Guilbert TW, Bacharier LB, Durrani S, Jackson DJ, et al. Preventing asthma in high risk kids (PARK) with omalizumab: design, rationale, methods, lessons learned and adaptation. Contemp Clin Trials. (2021) 100:106228. doi: 10.1016/j.cct.2020.106228
71. Saglani S, Menzie-Gow AN. Approaches to asthma diagnosis in children and adults. Front Pediatr. (2019) 7:148. doi: 10.3389/fped.2019.00148
72. Pavord ID, Beasley R, Agusti A, Anderson GP, Bel E, Brusselle G, et al. After asthma: redefining airways diseases. Lancet. (2018) 391(10118):350–400. doi: 10.1016/S0140-6736(17)30879-6
Keywords: allergen immunotherapy, children, clinical trials, diagnosis, new-onset asthma
Citation: Roberts G, Valovirta E, Halken S, Eng PA, Mäkelä MJ, Lødrup Carlsen KC, Knecht R and Malmberg LP (2024) Diagnosing new-onset asthma in a paediatric clinical trial setting in school-age children. Front. Allergy 5: 1418922. doi: 10.3389/falgy.2024.1418922
Received: 17 April 2024; Accepted: 21 May 2024;
Published: 15 July 2024.
Edited by:
Yuichi Adachi, Toyama Red Cross Hospital, JapanReviewed by:
Hector Badellino, University of Business and Social Sciences, ArgentinaIvana Filipovic, University Hospital Center Dr Dragiša Mišović, Serbia
© 2024 Roberts, Valovirta, Halken, Eng, Mäkelä, Lødrup Carlsen, Knecht and Malmberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Graham Roberts, Zy5jLnJvYmVydHNAc290b24uYWMudWs=