 César Daniel Alonso Bello1*
César Daniel Alonso Bello1* Otto Pavel González Guzmán2Carol Vivian Moncayo Coello1María Isabel Rojo Gutiérrez3María Isabel Castrejón Vázquez4
Otto Pavel González Guzmán2Carol Vivian Moncayo Coello1María Isabel Rojo Gutiérrez3María Isabel Castrejón Vázquez4
- 1Allergy and Immunology Service, Hospital Juárez de México, Secretaría de Salud, Mexico City, Mexico
- 2Spine Rehabilitation Service and Osteoporosis Clinic, Instituto Nacional de Rehabilitación, Mexico City, Mexico
- 3Allergy and Immunology Service, Medical Director, Unidad Médica Zurich Satélite, Naucalpan, Mexico
- 4Clinical Immunology and Allergy Service, Centro Médico Nacional 20 de Noviembre, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, Mexico City, Mexico
Progesterone is an endogenous hormone, produced by the adrenal cortex, the gonads and in women, its source is the corpus luteum. Progesterone is produced in the late phase of the menstrual cycle, when implantation of the zygote does not occur, the corpus luteum involutes and the release of progesterone is suppressed, thus initiating menstruation. Progestogen Hypersensitivity were initially identified as hormone allergy and were related to endogenous reactions to hormones and alteration of ovarian function. Skin manifestations such as dermatitis or urticaria were initially reported and described as progesterone autoimmune dermatitis, although the immune-mediated mechanism was not clear. Currently there is no standardization for in vivo or in vitro tests for Progestogen Hypersensitivity diagnosis. In this review, we will address the different diagnostic methods of this disease.
1 Introduction
Progestogen Hypersensitivity (PH) were initially identified as hormone allergy and were related to endogenous reactions to hormones and alteration of ovarian function (1). In 1947, Zondek and Bromnberg described hypersensitivity mechanisms related to endogenous hormones; These reactions were demonstrated by intradermal application tests of insulin and gonadotropin (2).
William Finch, in his article “The etiology of nausea and vomiting of pregnancy”, published in 1938, postulated that nausea during pregnancy was related to the functionality of the corpus luteum. The skin test performed to demonstrate sensitization and the desensitization scheme proposed in the case series of 30 patients were not standardized; the patients did not present skin symptoms or clinical manifestations additional to nausea; however, they presented erythema reactions at the site of intradermal application of progestin (3). This case series served as a background to recognize hypersensitivity reactions to endogenous progesterone.
The concept of allergy has evolved; today it is defined as an abnormal, unexpected, or exaggerated reaction to an external stimulus that involves the immune system. However, although the definition may be ambiguous, the current and recently published classification of the allergy European Academy of Allergy and Clinical Immunology (EAACI) helps us understand the mechanisms of how allergic pathologies are mediated by different immunological mechanisms; Thus, the classification of allergic mechanisms is classified into four main groups: antibody-mediated reactions, cell-mediated reactions, Tissue-driven mechanism and direct response to chemicals. In this way, the panorama opens up more, and the immunological mechanisms that can be considered allergy are recognized (4).
For this reason, we will call the reactions presented to endogenous or exogenous progesterone that we will study below, Progestogen Hypersensitivity, in this way we include any immunological mechanism that is currently classified as an allergy.
2 Progesterone in immunoendrocrinology
Progesterone (P4) was one of the first hormones identified, it is known for its role as a sex steroid (5). P4 is an endogenous 21-carbon steroid hormone synthesized from cholesterol in the corpus luteum of the ovaries and also by the placenta during pregnancy. To a lesser extent, P4 is also produced in the adrenal cortex, Leydig cells, adipose tissue, and the nervous system, being synthesized in both neurons and glia (6, 7).
Progesterone concentrations vary throughout the life course, presenting their greatest fluctuations during puberty and dynamic changes during the menstrual cycle in response to the pulsatile secretion of FSH and LH by the pituitary gland. Its levels are considerably higher in women than in men. During pregnancy, P4 increases its levels constantly and remains elevated throughout pregnancy, being essential for pregnancy retention; after childbirth, there is a rapid decrease in its serum concentration (8).
The immunomodulatory properties of progesterone have been described for several years in experimental models (9). Its role in tolerance towards paternal antigens during pregnancy is the best-known model. The presence of P4 nuclear receptors (PR) in the cells of the immune system has been strongly associated with pregnancy; most studies have shown the absence of PR in leukocytes in peripheral blood in non-pregnant women (10), However, the immunomodulatory actions of progesterone can also be mediated by pathways independent of its nuclear receptor, pathways that seem to be relevant in the regulation of immunity in people outside of pregnancy (11). A high percentage of RP-positive lymphocytes has been detected. in the peripheral blood of patients with liver transplants or transfusions (12), suggesting that the activation of lymphocytes resulting from permanent alloantigenic stimulation could induce the expression of RP in lymphocytes, in the setting of pregnancy the continuous exposure of the mother to fetal antigens could be a mechanism of induction of these receptors.
P4 has nuclear and non-nuclear pathways, the complex formed by progesterone and its nuclear receptor (RPn) regulates cellular functions through direct nuclear genomic pathways that affect gene expression and transcription, indirect genomic pathways are mediated by linked receptors to the membrane and cell surface that activate and modulate second messengers and ion channels to exert their genomic effects (13).
The RPn have two main isoforms PR-A and PR-B, these bind to P4 and translocate to the nucleus to join with the response elements. Although both isoforms are transcribed by the same gene, these are functionally different receptors and the relationship PR-A:PR-B determines the impact of P4 on cellular transcriptional activity (14). In PRs found in various non-reproductive tissues, including lymphoid, intestine and brain, progesterone may promote a primarily inhibitory effect on immune cell function, murine models highlight the importance of suppression of activation of NF-kB, which reduces the enzymatic activity of COX-2 (15) and the synthesis of proinflammatory cytokines, mainly TNF, L-1b and IL-12 in innate immune cells (16, 17). These immunological effects of P4 are mediated by progesterone-induced blocking factor (PFIP) (18). PIBF is mainly produced by PR-positive lymphocytes during pregnancy and some malignant tumors (19). Full-length PIBF (90 kDa) participates in the regulation of the cell cycle and the invasion of trophoblast and tumor cells (20). The smaller isoforms are located in the nucleus and act as cytokines (19). The most studied immunological effects of P4 and FBIP are those related to the activity of NK lymphocytes, the decrease in their degranulation and the balance of cytokines in favor of the Th2 response (21).
Inhibitory signaling of RP has been described from studies during pregnancy, however it is not the only nuclear signaling pathway that mediates the effects of P4. One of the most important cell populations during pregnancy are uterine NK cells. (uNK) these comprise up to 70% of the leukocytes in the decidual tissues, participate in the regulation of placental development and have a decreased cytotoxic capacity (8). Uterine NK cells do not express RP, however, P4 can mediate its actions on these cells through the glucocorticoid receptor (GR) (22).
The indirect progesterone genomic pathway is mediated by membrane-bound progesterone receptors (mPRs), which interact and activate mitogen-activated protein kinases (MAPKs) to modulate gene transcription, downregulating NF-kB, which inhibits transcription. of cyclooxygenase-2 (COX-2), blocking the synthesis of arachidonic acid derivatives and attenuating the inflammatory response (23), this pathway also increases the concentration of cAMP in the MAPK pathway.
P4 inhibits the inflammatory responses of macrophages and dendritic cells (DC) through the RP or indirectly through the pattern recognition receptor and cellular synthesis of cytokines (24). PR signaling in DCs also inhibits TLR3- and TLR4-mediated IL production and the expression of costimulatory molecules (25). The data indicate that P4 mediates these effects through RP and RG. In women's T cells, mRP expression varies throughout the menstrual cycle. mPR expression is 2–5 times higher in CD8+ T cells during the luteal phase compared to the follicular phase of the cycle menstrual (26). RP signaling generally suppresses the activity of both CD4+ and CD8+ T cells, decreasing their proliferation and activation, and can trigger apoptosis (27).
In the skin, both estrogens and progesterone have effects related to the menstrual cycle and therefore to the serum concentrations of these hormones. High levels of estrogen and progesterone in the periovulatory period inhibit delayed hypersensitivity reactions, while lower levels of both hormones (perimenstruation) are associated with greater skin test reactivity, explaining exacerbations in atopic patients. These data reaffirm the role of estrogen and progesterone as inhibitors of cellular immunity (28).
3 Progestogen hypersensitivity, clinical presentation
Progesterone sensitization may result from IgE-mediated sensitization to endogenous progestins or with exogenous exposure to contraceptive drugs; On, special cases are patients with a history of infertility therapy or assisted reproduction, where the administration of progestogens was necessary (29). Other mechanisms, such as cross-reaction with other types of steroids such as hydrocortisone, have been proposed (30, 31).
Skin manifestations such as dermatitis or urticaria were initially reported and described as progesterone autoimmune dermatitis, although the immune-mediated mechanism was not clear. The immunological mechanisms have been described according to the previous classification of hypersensitivity, such as immediate hypersensitivity (type I), or cellular or delayed hypersensitivity (type IV), with manifestations such as skin rash, up to presentations as serious as Stevens-Johnson syndrome or presence of IgG antibodies against progesterone with the subsequent formation of immune complexes (type III hypersensitivity); However, the common characteristic is the cyclical presentation depending on the period of the menstrual cycle (32).
The clinical data suggestive of this pathology are summarized in Table 1.
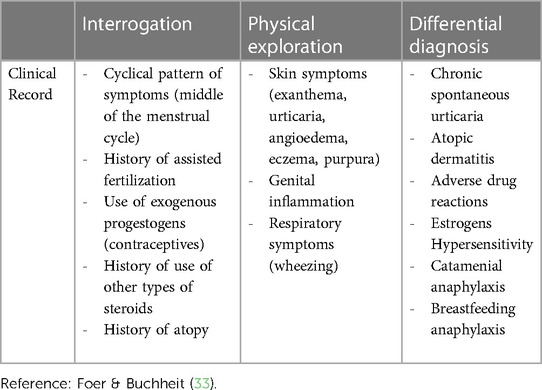
Table 1. Clinical approach to diagnosis of PH.
4 Diagnostic tests for progestogen hypersensitivity
4.1 Skin tests
Currently there is no standardization for in vivo or in vitro tests for PH diagnosis. Skin tests are performed by two techniques, prick tests and intradermal tests. Intradermal testing schemes are based on the initial concentration of the prick test, since concentrations for intradermal tests are usually ten to a thousand times lower.
The largest case series of skin testing for HP included 24 patients at Brigham and Women's Hospital; The diagnosis was made with clinical history and skin prick and intradermal tests (34). There are various clinical case reports and different proposals on how to perform this type of test in patients in whom PH is suspected, although sometimes the diagnosis is made only by consensus of experts, the skin test is performed as the initial study for evaluation (35). In our experience, skin tests can have late reactions, therefore it is necessary to maintain prolonged surveillance, and in a previous publication, the final reactivity was demonstrated by intramuscular challenge with progesterone (36).
Because PH is considered an autoimmune disease by some authors, testing such as autologous serum test, as performed in autoimmune urticaria and, has been implemented in certain cases (37); This is evidence that the immune-mediated mechanisms of the disease are not completely understood.
Recently Chamorro-Pareja et al. published a case of an 18-year-old woman who presented an adverse reaction to oral contraceptives. The reactivity occurred after 6 weeks of taking the hormones and, allergy skin tests were performed to corroborate the diagnosis. The tests were positive for progestin and estrogen. The test technique is included in Table 2 (42).
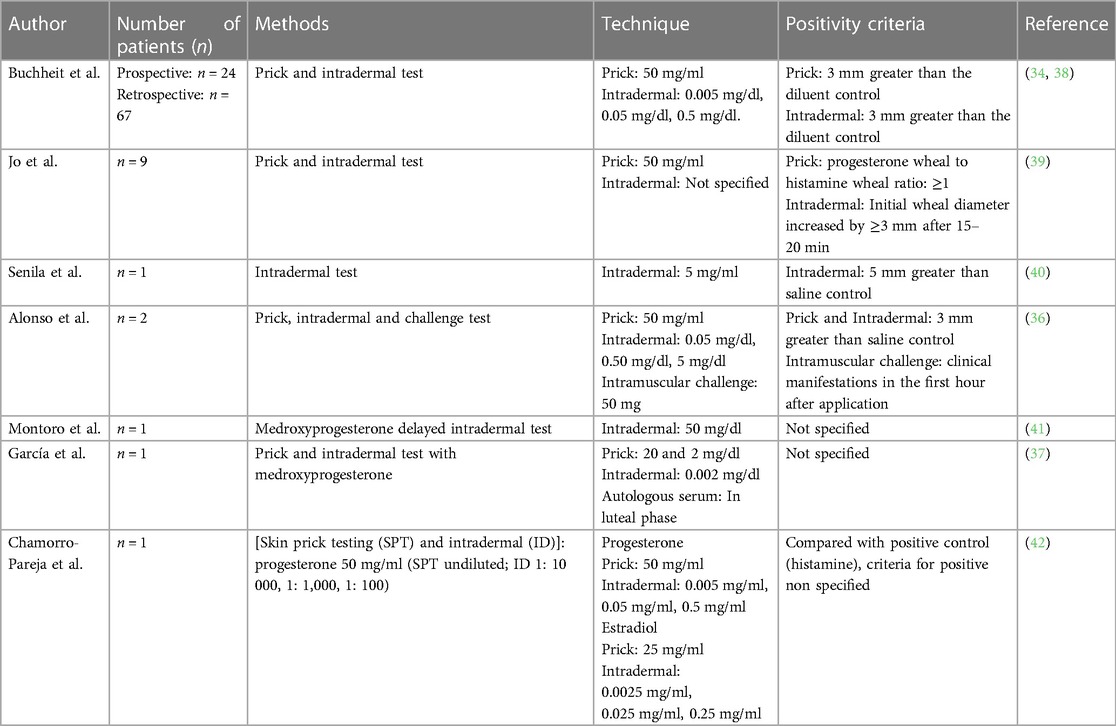
Table 2. Comparison of diagnostic methods with in vivo tests for progestogen hypersensitivity.
Only one case of cross-sensitization has been reported for one of the excipients that may contain progesterone, the product progesterone-in-oil, used for in vitro fertilization, was related to the presence of systemic symptoms in a 29-year-old woman, with pulmonary symptoms; In this case, no reactivity was verified by skin prick tests, intradermal or patch tests (43). This point is relevant to take into account since it is known that sesame oil may contain allergenic substances and, in this case, it would require considering testing progesterone products with different excipients (44, 45).
In Table 2 we compare different diagnostic methods using skin tests reported by different authors.
4.2 In vitro tests
Due to the clinical presentation, sometimes with immediate symptoms and other times with delayed symptoms, in vitro tests have been developed to determine Immunoglobulin E (IgE) and immunoglobulin G (IgG) against progesterone, given that the pathology is recognized in sometimes as allergic and other times as autoimmune.
There is no standardization to decide the positivity of the skin tests. Besides, the dilution of progesterone must be in an oily medium and, this can be irritating to the skin, thus creating false positive results. For these reasons, specific IgE direct enzyme-linked immunosorbent assay (ELISA) methods have been created to be applied in patients with suspected PH. The test was performed on patients who experienced symptoms 3–4 days before menstruation and had them resolve during or at the end of the menstrual cycle. Of the total number of individuals to whom the test was applied, 35% were atopic, presenting comorbidities such as allergic rhinitis, food allergy, drug allergy, atopic dermatitis, anaphylaxis and asthma; some of them with total IgE greater than 1,000 IU/ml. Five individuals (29.4%) had a negative result and the positive result was not related to skin testing (46).
An ELISA test was also used in the case report of a patient who was diagnosed by specific IgE for progesterone. The clinical data presented by the patient were cyclic urticaria with angioedema and, partial response to antihistamines, steroids and omalizumab. These symptoms can be classically related to IgE-mediated hypersensitivity (47). There are still no cutoff values for specific IgE for progesterone, this test cannot be considered standardized.
The identification of IgG antibodies has been a task carried out since the 1980s, first in 1982, Cheesman et al. identified 17-hydroxyprogesterone-binding immunoglobulin in the serum of a woman with cutaneous symptoms, suspected of sensitization to synthetic progestin (48).
In 1989, two cases of autoimmune dermatitis due to progesterone were reported, with pruritic erythema, edematous skin eruptions, and vesicles on the palms and soles. In addition to the skin tests performed and indirect basophil degranulation assay, an IgG-type serum factor was found; this serum factor bound to the rat corpus luteum (49). Additionally In a patient who presented erythema multiforme, immune complexes were detected after 48 h of the administration of medroxyprogesterone, reinforcing the evidence that IgG type antibodies exist for progestogens (50). These trials and results should be taken with caution since the presence of IgG, IgM, IgA and IgE antibodies has been demonstrated in allergic patients in whom the symptoms of asthma, joint pain and migraine changed in relation to the menstrual cycle or exogenous hormonal exposure (51).
As an innovative test, an ELISpot assay has been created for the detection of interferon-γ producing cells, in a report where the production of interferon-γ was demonstrated with the stimulation of PBMC in a patient with premenstrual vulvovaginal pruritus (52). To date, it is the only study that reports this innovative form of evaluation when symptoms are considered to be related to autoimmunity.
The use of tests such as basophil activation has not yet been explored and is a window of opportunity to contribute to the diagnosis of PH, in patients with symptoms that may be related to IgE-mediated hypersensitivity.
5 Decision to determinate the type of test to use
The decision of which test to perform should be based on the clinical symptoms and their presentation; And depending on the type of pathology, always take into account what time of the menstrual cycle the patient is at. Additionally, in the case of symptoms due to exogenous application of progestogens, the time of symptom presentation after exposure. Carrying out a challenge with the administration of endogenous progesterone requires specialized evaluation by trained personnel due to the high risk of anaphylaxis (53).
Next, we propose an algorithm to determine the type of test to use when PH is suspected (Figure 1).
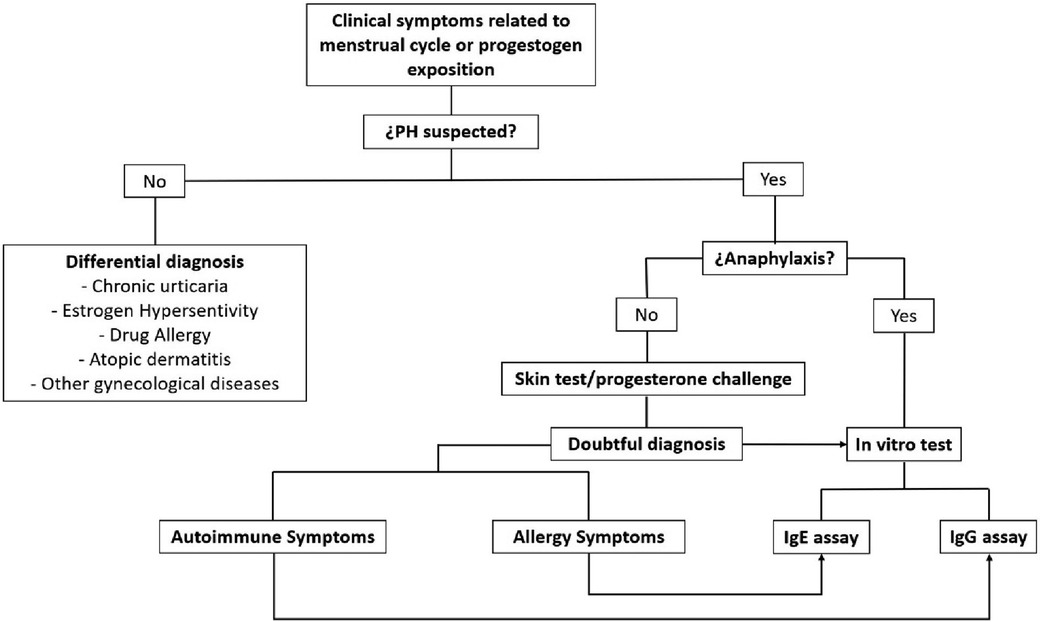
Figure 1. Algorithm for the use of tests to apply when PH is suspected.
6 Conclusions
The diagnosis of PH is a diagnostic challenge; The presence of clinical symptoms should guide us by the form and time of appearance. Exogenous exposure due to therapies that require the application of progestogens may be a risk factor for developing PH.
Skin tests can guide us if they are performed with the appropriate technique and concentrations so that they are not irritating. In patients who require complementary studies, in vitro tests can be performed, although these are not yet commercially available.
Although the immunological mechanisms of hypersensitivity to progesterone and other hormones have not been fully described, the in-depth study of each new case published helps us learn more about the etiology of this rare pathology.
Author contributions
CA: Conceptualization, Writing – original draft, Writing – review & editing. OG: Visualization, Writing – review & editing. CM: Methodology, Writing – review & editing. MR: Formal Analysis, Writing – review & editing. MC: Methodology, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Heckel GP. Endocrine allergy and the therapeutic use of pregnandiol. Am J Obstet Gynecol. (1953) 66(6):1297–312. doi: 10.1016/0002-9378(53)90171-9
2. Zondek B, Bromberg YM. Mechanism of endocrine allergy; interpretation of principal phenomena observed in hypersensitivity to the endogenous hormones. Acta Med Orient. (1947) 6(1):1–8.20294506
3. Finch JW. The etiology of nausea and vomiting of pregnancy: preliminary report. JAMA. (1938) 111(15):1368–70. doi: 10.1001/jama.1938.02790410024007
4. Jutel M, Agache I, Zemelka-Wiacek M, Akdis M, Chivato T, Del Giacco S, et al. Nomenclature of allergic diseases and hypersensitivity reactions: adapted to modern needs: an EAACI position paper. Allergy. (2023) 78(11):2851–74. doi: 10.1111/all.15889
5. Henderson VW. Progesterone and human cognition. Climacteric. (2018) 21(4):333–40. doi: 10.1080/13697137.2018.1476484
6. Rossato M, Nogara A, Merico M, Ferlin A, Foresta C. Identification of functional binding sites for progesterone in rat Leydig cell plasma membrane. Steroids. (1999) 64(1-2):168–75. doi: 10.1016/s0039-128x(98)00104-4
7. Stoffel-Wagner B. Neurosteroid metabolism in the human brain. Eur J Endocrinol. (2001) 145(6):669–79. doi: 10.1530/eje.0.1450669
8. Szekeres-Bartho J, Schindler AE. Progestogens and immunology. Best Pract Res Clin Obstet Gynaecol. (2019) 60:17–23. doi: 10.1016/j.bpobgyn.2019.07.001
9. Moriyama I, Sugawa T. Progesterone facilitates implantation of xenogenic cultured cells in hamster uterus. Nat New Biol. (1972) 236(66):150–2. doi: 10.1038/newbio236150a0
10. Szekeres-Bartho J, Reznikoff-Etievant MF, Varga P, Pichon MF, Varga Z, Chaouat G. Lymphocytic progesterone receptors in normal and pathological human pregnancy. J Reprod Immunol. (1989) 16(3):239–47. doi: 10.1016/0165-0378(89)90053-3
11. Ehring GR, Kerschbaum HH, Eder C, Neben AL, Fanger CM, Khoury RM, et al. A nongenomic mechanism for progesterone-mediated immunosuppression: inhibition of K+ channels, Ca2+ signaling, and gene expression in T lymphocytes. J Exp Med. (1998) 188(9):1593–602. doi: 10.1084/jem.188.9.1593
12. Szekeres-Bartho J, Weill BJ, Mike G, Houssin D, Chaouat G. Progesterone receptors in lymphocytes of liver-transplanted and transfused patients. Immunol Lett. (1989) 22(4):259–61. doi: 10.1016/0165-2478(89)90162-4
13. Kolatorova L, Vitku J, Suchopar J, Hill M, Parizek A. Progesterone: a steroid with wide range of effects in physiology as well as human medicine. Int J Mol Sci. (2022) 23(14):7989. doi: 10.3390/ijms23147989
14. Merlino AA, Welsh TN, Tan H, Yi LJ, Cannon V, Mercer BM, et al. Nuclear progesterone receptors in the human pregnancy myometrium: evidence that parturition involves functional progesterone withdrawal mediated by increased expression of progesterone receptor-A. J Clin Endocrinol Metab. (2007) 92(5):1927–33. doi: 10.1210/jc.2007-0077
15. Hardy DB, Janowski BA, Corey DR, Mendelson CR. Progesterone receptor plays a major antiinflammatory role in human myometrial cells by antagonism of nuclear factor-kappaB activation of cyclooxygenase 2 expression. Mol Endocrinol. (2006) 20(11):2724–33. doi: 10.1210/me.2006-0112
16. Butts CL, Bowers E, Horn JC, Shukair SA, Belyavskaya E, Tonelli L, et al. Inhibitory effects of progesterone differ in dendritic cells from female and male rodents. Gend Med. (2008) 5(4):434–47. doi: 10.1016/j.genm.2008.11.001
17. Jones LA, Anthony JP, Henriquez FL, Lyons RE, Nickdel MB, Carter KC, et al. Toll-like receptor-4-mediated macrophage activation is differentially regulated by progesterone via the glucocorticoid and progesterone receptors. Immunology. (2008) 125(1):59–69. doi: 10.1111/j.1365-2567.2008.02820.x
18. Szekeres-Bartho J, Kilaŕ F, Falkay G, Csernus V, Török A, Pacsa AS. The mechanism of the inhibitory effect of progesterone on lymphocyte cytotoxicity: I. Progesterone-treated lymphocytes release a substance inhibiting cytotoxicity and prostaglandin synthesis. Am J Reprod Immunol Microbiol. (1985) 9(1):15–8. doi: 10.1111/j.1600-0897.1985.tb00334.x
19. Lachmann M, Gelbmann D, Kálmán E, Polgár B, Buschle M, Von Gabain A, et al. PIBF (Progesterone induced blocking factor) is overexpressed in highly proliferating cells and associated with the centrosome. Int J Cancer. (2004) 112(1):51–60. doi: 10.1002/ijc.20326
20. Gutiérrez-Rodríguez A, Hansberg-Pastor V, Camacho-Arroyo I. Proliferative and invasive effects of progesterone-induced blocking factor in human glioblastoma cells. Biomed Res Int. (2017) 2017:1295087. doi: 10.1155/2017/1295087
21. Saito S. Cytokine network at the feto-maternal interface. J Reprod Immunol. (2000) 47(2):87–103. doi: 10.1016/s0165-0378(00)00060-7
22. Guo W, Li P, Zhao G, Fan H, Hu Y, Hou Y. Glucocorticoid receptor mediates the effect of progesterone on uterine natural killer cells. Am J Reprod Immunol. (2012) 67(6):463–73. doi: 10.1111/j.1600-0897.2012.01114.x
23. Lei K, Chen L, Georgiou EX, Sooranna SR, Khanjani S, Brosens JJ, et al. Progesterone acts via the nuclear glucocorticoid receptor to suppress IL-1β-induced COX-2 expression in human term myometrial cells. PLoS One. (2012) 7(11):e50167. doi: 10.1371/journal.pone.0050167
24. Azeez JM, Susmi TR, Remadevi V, Ravindran V, Sasikumar Sujatha A, Ayswarya RNS, et al. New insights into the functions of progesterone receptor (PR) isoforms and progesterone signaling. Am J Cancer Res. (2021) 11(11):5214–32.34873457
25. Jones LA, Kreem S, Shweash M, Paul A, Alexander J, Roberts CW. Differential modulation of TLR3- and TLR4-mediated dendritic cell maturation and function by progesterone. J Immunol. (2010) 185(8):4525–34. doi: 10.4049/jimmunol.0901155
26. Dosiou C, Hamilton AE, Pang Y, Overgaard MT, Tulac S, Dong J, et al. Expression of membrane progesterone receptors on human T lymphocytes and Jurkat cells and activation of G-proteins by progesterone. J Endocrinol. (2008) 196(1):67–77. doi: 10.1677/JOE-07-0317
27. Chien CH, Lai JN, Liao CF, Wang OY, Lu LM, Huang MI, et al. Mifepristone acts as progesterone antagonist of non-genomic responses but inhibits phytohemagglutinin-induced proliferation in human T cells. Hum Reprod. (2009) 24(8):1968–75. doi: 10.1093/humrep/dep099
28. Farage MA, Berardesca E, Maibach H. The possible relevance of sex hormones on irritant and allergic responses: their importance for skin testing. Contact Dermatitis. (2010) 62(2):67–74. doi: 10.1111/j.1600-0536.2009.01621.x
29. Ciampaglia W, Cognigni GE. Clinical use of progesterone in infertility and assisted reproduction. Acta Obstet Gynecol Scand. (2015) 94(161):17–27. doi: 10.1111/aogs.12770
30. Untersmayr E, Jensen AN, Walch K. Sex hormone allergy: clinical aspects, causes and therapeutic strategies—update and secondary publication. World Allergy Organ J. (2017) 10(1):45. doi: 10.1186/s40413-017-0176-x
31. Schoenmakers A, Vermorken A, Degreef H, Dooms-Goossens A. Corticosteroid or steroid allergy? Contact Dermatitis. (1992) 26(3):159–62. doi: 10.1111/j.1600-0536.1992.tb00286.x
32. Foer D, Buchheit KM. Presentation and natural history of progestogen hypersensitivity. Ann Allergy Asthma Immunol. (2019) 122(2):156–9. doi: 10.1016/j.anai.2018.10.023
33. Foer D, Buchheit KM. Progestogen hypersensitivity: an evidence-based approach to diagnosis and management in clinical practice. Immunol Allergy Clin North Am. (2017) 37(4):773–84. doi: 10.1016/j.iac.2017.07.006
34. Foer D, Buchheit KM, Gargiulo AR, Lynch DM, Castells M, Wickner PG. Progestogen hypersensitivity in 24 cases: diagnosis, management, and proposed renaming and classification. J Allergy Clin Immunol Pract. (2016) 4(4):723–9. doi: 10.1016/j.jaip.2016.03.003
35. Aghazadeh N, Chattha AJ, Hartz MF, Davis DMR. Autoimmune progesterone dermatitis in the adolescent population. Pediatr Dermatol. (2021) 38(2):380–4. doi: 10.1111/pde.14423
36. Alonso-Bello CD, Castañeda-Ávila VI, González-Rivera C. Autoimmune progesterone dermatitis diagnosed by skin-test [Article in Spanish]. Dermatol Rev Mex. (2023) 67(2):314–7. doi: 10.24245/drm/bmu.v67i2.8763
37. García-Ortega P, Scorza E. Progesterone autoimmune dermatitis with positive autologous serum skin test result. Obstet Gynecol. (2011) 117(2 Pt 2):495–498. doi: 10.1097/AOG.0b013e318206cb2c
38. Foer D, Tran LK, Wickner P, Castells M, Marquis KA, Buchheit KM. Challenges in skin testing for progestogen hypersensitivity. Ann Allergy Asthma Immunol. (2021) 126(1):100–2. doi: 10.1016/j.anai.2020.09.002
39. Jo EJ, Lee SE, Park HK. Clinical characteristics of exogenous progestogen hypersensitivity. Asian Pac J Allergy Immunol. (2019) 37(3):183–7. doi: 10.12932/AP-291217-0227
40. Senila SC, Ungureanu L, Candrea E, Danescu S, Vasilovici A, Cosgarea R, et al. Progesterone hypersensitivity: case report with favorable evolution. Exp Ther Med. (2019) 17(2):1125–7. doi: 10.3892/etm.2018.7055
41. Montoro J, Miquel FJ, Quecedo E, Martínez M, Orduña A, Gimeno E, et al. Autoimmune progesterone dermatitis: a Complex case. J Investig Allergol Clin Immunol. (2018) 28(5):348–50. doi: 10.18176/jiaci.0284
42. Chamorro-Pareja N, Carrillo-Martin I, Haehn DA, Gonzalez-Estrada A. Documented exogenous progesterone hypersensitivity related to the use of combined oral contraceptive. BMJ Case Rep. (2019) 12(9):e230416. doi: 10.1136/bcr-2019-230416
43. Phy JL, Weiss WT, Weiler CR, Damario MA. Hypersensitivity to progesterone-in-oil after in vitro fertilization and embryo transfer. Fertil Steril. (2003) 80(5):1272–5. doi: 10.1016/s0015-0282(03)01170-1
44. Asero R, Mistrello G, Roncarolo D, Antoniotti PL, Falagiani P. A case of sesame seed-induced anaphylaxis. Allergy. (1999) 54(5):526–7.10380788
45. Kanny G, De Hauteclocque C, Moneret-Vautrin DA. Sesame seed and sesame seed oil contain masked allergens of growing importance. Allergy. (1996) 51(12):952–7. doi: 10.1111/j.1398-9995.1996.tb02141.x
46. Ghosh D, Bernstein JA. Development of a progesterone-specific IgE assay for diagnosing patients with suspected progestogen hypersensitivity. Ann Allergy Asthma Immunol. (2019) 122(6):616–22. doi: 10.1016/j.anai.2019.03.032
47. Dhaliwal G, Batra J, Ankireddypalli AR, Gorle S, Kanugula AK, Kaur J. Progesterone hypersensitivity induced by exogenous progesterone exposure. Cureus. (2023) 15(9):e44776. doi: 10.7759/cureus.44776
48. Cheesman KL, Gaynor LV, Chatterton RT Jr, Radvany RM. Identification of a 17-hydroxyprogesterone-binding immunoglobulin in the serum of a woman with periodic rashes. J Clin Endocrinol Metab. (1982) 55(3):597–9. doi: 10.1210/jcem-55-3-597
49. Miura T, Matsuda M, Yanbe H, Sugiyama S. Two cases of autoimmune progesterone dermatitis. Immunohistochemical and serological studies. Acta Derm Venereol. (1989) 69(4):308–10.2568048
50. Wojnarowska F, Greaves MW, Peachey RD, Drury PL, Besser GM. Progesterone-induced erythema multiforme. J R Soc Med. (1985) 78(5):407–8. doi: 10.1177/014107688507800512
51. Roby RR, Richardson RH, Vojdani A. Hormone allergy. Am J Reprod Immunol. (2006) 55(4):307–13. doi: 10.1111/j.1600-0897.2006.00373.x
52. Cristaudo A, Bordignon V, Palamara F, De Rocco M, Pietravalle M, Picardo M. Progesterone sensitive interferon-gamma producing cells detected by ELISpot assay in autoimmune progesterone dermatitis. Clin Exp Dermatol. (2007) 32(4):439–41. doi: 10.1111/j.1365-2230.2007.02382.x
Keywords: progesterone, autoimmune diseases, menstrual cycle, urticaria, allergy
Citation: Alonso Bello César Daniel, González Guzmán OP, Moncayo Coello CV, Rojo Gutiérrez María Isabel and Castrejón Vázquez María Isabel (2024) Diagnostic tests for progestogen hypersensitivity. Front. Allergy 5:1384140. doi: 10.3389/falgy.2024.1384140
Received: 8 February 2024; Accepted: 27 March 2024;
Published: 24 April 2024.
Edited by:
Maria C. Jiménez Martínez, National Autonomous University of Mexico, MexicoReviewed by:
Gianfranco Calogiuri, Ospedale Vito Fazzi, Italy© 2024 Alonso Bello, González Guzmán, Moncayo Coello, Rojo Gutiérrez and Castrejón Vázquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: César Daniel Alonso Bello Y2VzYXJfYWxvbnNvODZAaG90bWFpbC5jb20=