 Julie Castagna1,†François Chasset1,2,†Jean-Eric Autegarden1Claire Le Thai1Emmanuelle Amsler1,†
Julie Castagna1,†François Chasset1,2,†Jean-Eric Autegarden1Claire Le Thai1Emmanuelle Amsler1,† Annick Barbaud1,3,†
Annick Barbaud1,3,† Angèle Soria1,2*†
Angèle Soria1,2*†
- 1Médecine Sorbonne Université, Service de dermatologie et d’allergologie, Hôpital Tenon, Assistance Publique des Hôpitaux de Paris (AP-HP), Paris, France
- 2Centre d’Immunologie et de Maladies Infectieuses, Cimi-Paris, INSERM, Paris, France
- 3INSERM, Institut Pierre Louis d’Epidémiologie et de Sante Publique, Paris, France
Introduction: Approximately 10% of individuals report a suspected allergy to penicillin, but according to allergy work-ups, only 10%–15% of them are truly allergic. A clinical decision score, the PEN-FAST, was developed and validated to identify adults with low-risk penicillin allergy.
Objectives: The objective of this study was to improve the performance of the PEN-FAST score, particularly for those with delayed hypersensitivity (HS), by improving the negative predictive value.
Methods: STEP 1: Retrospective evaluation of the PEN-FAST score in patients with proven immediate and delayed penicillin allergy. STEP 2: Identification of additional criteria among Step 1 patients misclassified by PEN-FAST score. Development of the PEN-FAST+ score using multivariable logistic regression in a prospective cohort of patients with a suspicion of HS to penicillin. STEP 3: Comparison of diagnostic performances of PEN-FAST and PEN-FAST+ scores.
Results: The PEN-FAST score showed limitations in predicting the relapse of immediate skin HS or delayed maculopapular exanthema, with 28.6% and 38.4% of patients misclassified, respectively. We identified two potential additional criteria: skin rash lasting more than 7 days and immediate reaction occurring in less than 1 h (generalized or localized on palmoplantar area or scalp itching/heat feeling). A total of 32/252 (12.7%) patients were confirmed to be allergic to penicillin. With PEN-FAST, 37% of patients (n = 10) with delayed allergic penicillin HS were misclassified. With PEN-FAST+, 3 patients with delayed HS confirmed by a ST (11.1%) were misclassified. The AUC was significantly higher for PEN-FAST+ than PEN-FAST (85% vs. 72%, p = 0.03).
Introduction
Approximately 10% of individuals report a suspected allergy to penicillin, but according to allergy work-ups, only 10% to 15% of them are truly allergic (1). Skin tests (STs) followed by a drug provocation test (DPT) with penicillin are the gold standard detection methods but are time-consuming (1). Trubiano et al. developed and validated a clinical decision score, the PEN-FAST, with 3 criteria (Five years or less since reaction [yes +2], Anaphylaxis or angioedema OR Severe cutaneous adverse reaction [yes +2], Treatment required for reaction (including unknown) [yes +1]), to identify adults with low-risk penicillin allergy (2).
A PEN-FAST score below 3 points is in favor of a low risk of allergy to penicillin. A score of less than 3 includes both patients with a PEN-FAST score of 0 and those with a PEN-FAST score of 1 or 2 with a very low (<1%) and low (5%), respectively, risk of having a positive penicillin allergy test. This score was validated in European and North American cohorts of adults with predominantly immediate hypersensitivity (HS). However, delayed HS, and more specifically maculopapular exanthema (MPE), represents the most common form of penicillin allergy (3, 4), whereas the percentage of patients with delayed HS represented 33.1% of the initial cohort (2).
Our first objective was to evaluate the decision score of penicillin allergy PEN-FAST in a retrospective cohort of patients with a proven allergy (immediate and delayed allergy to penicillin, especially in those with MPE). In these patients, the allergy to penicillin was shown after immediate or delayed reading of positive skin tests (STs).
The secondary objective was to improve the performance of the PEN-FAST score, particularly the negative predictive value (NPV). Challenging a patient with a penicillin allergy using the same or another penicillin is considered unjustifiable without STs for some authors, due to the potential risk of severity (5, 6). PEN-FAST has been validated in a prospective cohort, demonstrating non-inferiority compared to STs when direct drug provocation tests (DPT) were performed without STs if PEN-FAST scores were less than 3 before DPT. However, it is important to note that this analysis was limited to patients with immediate HS after DPT (7). It appears crucial to increase the probability of correctly classifying nonallergic patients, including those with delayed HS.
Methods
This study was performed in three successive steps. In the first step, we applied the PEN-FAST score retrospectively in the latest 27 adult patients diagnosed in our department with a proven immediate or delayed allergy to penicillin through penicillin STs or positive drug provocation test (DPT). Fourteen and 13 patients had allergic HS proven by prick tests or intradermal tests positive for penicillin during immediate or delayed readings, respectively or positive DPT (Figure 1(A) and Supplementary Materials). No hypersensitivity phenotype that can be explored through the allergological explorations is excluded.
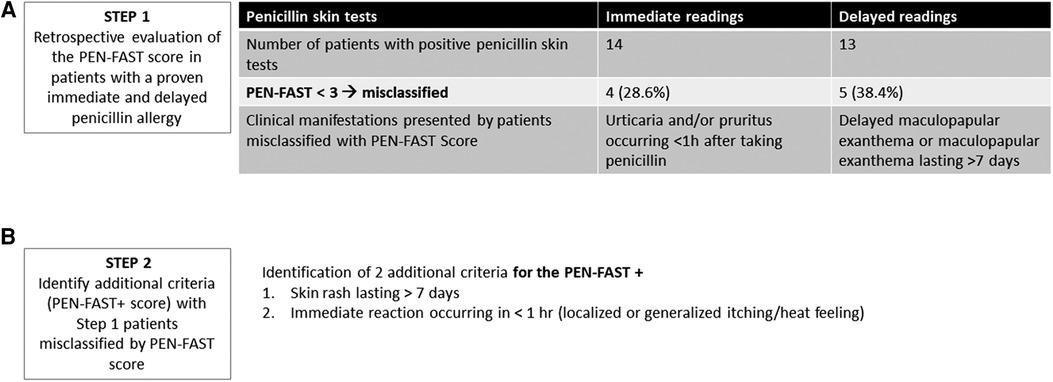
Figure 1. STEP 1 and 2 of the study. (A) Results of the analysis of PEN-FAST in 27 adults with true penicillin-allergy immediate and delayed. STs, skin. (B) Two additional criteria of PEN-FAST+ score.
In the second step, among these 27 patients, we assessed the clinical features of patients with a proven penicillin allergy misclassified by the PEN-FAST score (i.e., having a positive ST or a positive DPT result while having a PEN-FAST score of <3) and we reviewed existing literature to identify potential additional criteria to better classify these allergic patients (Figure 1(B)).
A multivariable logistic regression was performed to identify factors associated with true allergy by using the 3 PEN-FAST criteria with these additional criteria to develop a new score (PEN-FAST+) in a monocentric prospective cohort of 252 successive patients (over a period of six consecutive months, excluding the 27 patients from step 1) with a suspicion of HS (immediate or delayed) to penicillin with STs and DPT.
The third step was the comparison of PEN-FAST and PEN-FAST+ scores in our prospective cohort of 252 patients. The PEN-FAST and PEN-FAST+ scores were used in this cohort, and a posteriori and diagnostic performance were calculated. The diagnostic performance of the 2 scores was assessed by comparing the area under the receiver operating characteristic curve (AUC) with the Delong Test (8). The calculation of the cutoff scores for the clinical decision rules PEN-FAST and PEN-FAST+ allowed for determining the statistical performance of the 2 tests using the Youden index. Statistical analysis are detailed in Supplementary Materials.
For all patients, the penicillin STs were conducted and interpreted according to the ENDA recommendations (for more details see Supplementary Materials).
This was an observational study, and patients' informed consent was obtained in accordance with local ethics committee requirements.
Results
The PEN-FAST score showed limitations in predicting the relapse of immediate skin HS or delayed MPE, with 28.6 (n = 4) and 38.4% (n = 5) of patients misclassified, respectively (Figure 1(A)). None of the patients met the criteria for the two points related to anaphylaxis or angioedema or severe cutaneous adverse reactions. Their inclusion was based only on either a history of “Five years or less since reaction” or “Treatment required for reaction (including unknown)”.
After reviewing the medical records of the misclassified patients with PEN-FAST, we identified two potential additional criteria, occurring in all penicillin-allergic patients who were misclassified for each other (Figure 1(B) and Supplementary Table S1): skin rash lasting more than 7 days and immediate reaction occurring in less than 1 h (generalized or localized on the palmoplantar area or scalp itching/heat sensation occurring in the four patients misclassified by PEN-FAST). To improve the PEN-FAST NPV using these two additional criteria, we aimed to develop a new score, PEN-FAST+, and compare its diagnostic performance with that of PEN-FAST in a prospective validation cohort of 252 consecutive adult patients referred in our center for suspected penicillin HS. The multivariable model is presented in Table 1.
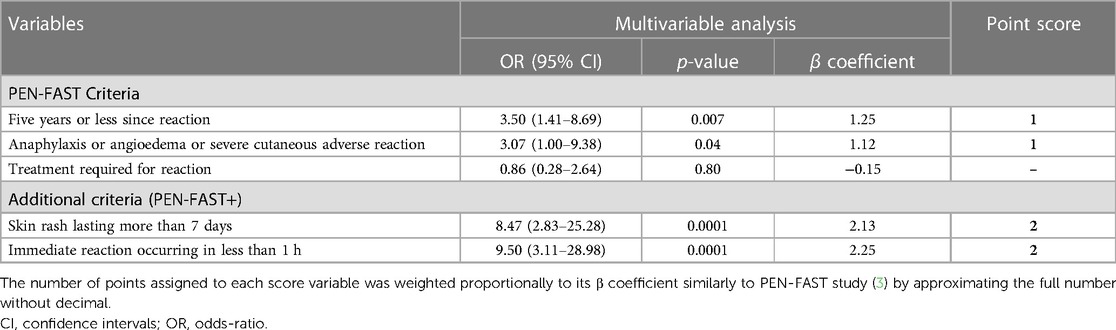
Table 1. Multivariable model with variables from PEN-FAST and two additional criteria for the PEN-FAST + clinical decision rule.
In our model, the third criterion of PEN-FAST was no longer relevant (Treatment required for reaction, p = 0.80).
Patient characteristics, allergy work-up, PEN-FAST, and PEN-FAST+ score results are shown in Figure 2. Briefly, STs were positive in 27/252 (10.7%) patients, 13 with immediate and 14 with delayed readings, who were confirmed to be allergic to penicillin. For 12 patients, the PEN-FAST score was <3 (44.4%): 2 and 10 with immediate and delayed HS, respectively. With PEN-FAST, 37% of patients (n = 10) with delayed allergic penicillin HS were misclassified. With PEN-FAST+, 3 patients with delayed HS confirmed by a ST (11.1%) were misclassified (Figure 2). Among them, 2 were correctly classified by PEN-FAST (less than 5 years since reaction and treatment received): one with benign MPE lasting less than 7 days and one with history of grade I HS but delayed positivity of STs controlled twice. None of them met the diagnostic criteria for DRESS syndrome. PEN-FAST+ correctly classified all penicillin allergic patients with immediate HS.
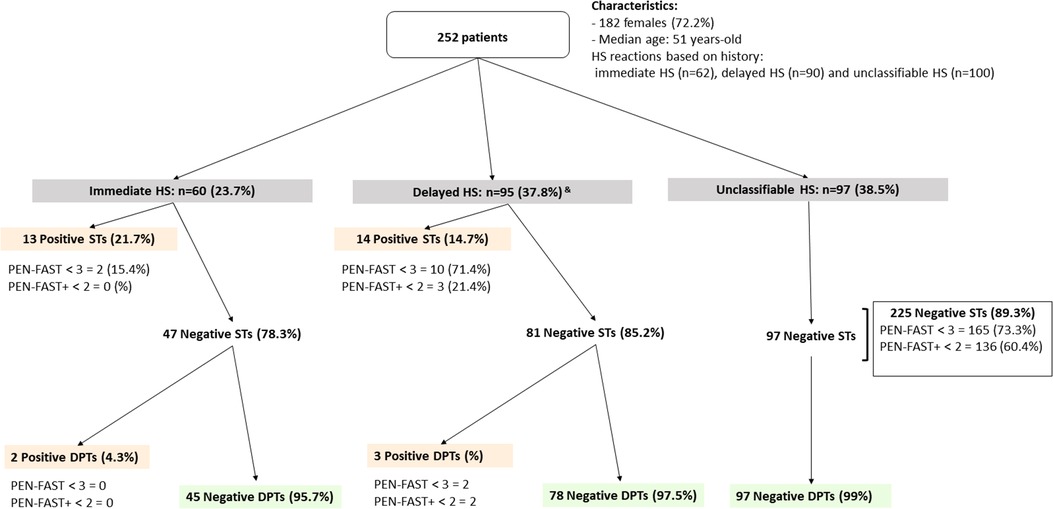
Figure 2. PEN-FAST and PEN-FAST+ score applied in a prospective cohort of 252 patients suspected to penicillin-allergy. HS, hypersensitivity; STs, skin tests, DTPs, drug provocation tests with penicillin. Orange: Penicillin-allergic patients, Green: non allergic patients. &Four patients, two with an unclassifiable history of HS and two with an immediate history, had positive skin tests with delayed readings and were subsequently classified as having delayed HS. One patient with an unclassifiable history of hypersensitivity had a positive delayed drug provocation test and was also classified as having delayed HS.
Discussion
A total of 88.9% of patients with positive STs and 84.4% of truly allergic patients (shown by positive STs or DPT) were correctly identified by PEN-FAST+ compared with 55.6% and 56.2%, respectively, by PEN-FAST. Although we increased the sensitivity, we did not decrease the specificity. Indeed, compared with PEN-FAST, PEN-FAST+ proposed STs for 5 less non-allergic patients. The AUC was significantly higher for PEN-FAST+ than PEN-FAST (85% vs. 72%, p = 0.03) (Figure 3(A)). The threshold to identify patients with low-risk penicillin allergy who may not require an ST is defined here by the Youden index, with a PEN-FAST+ score <2 (Figure 3(B)).
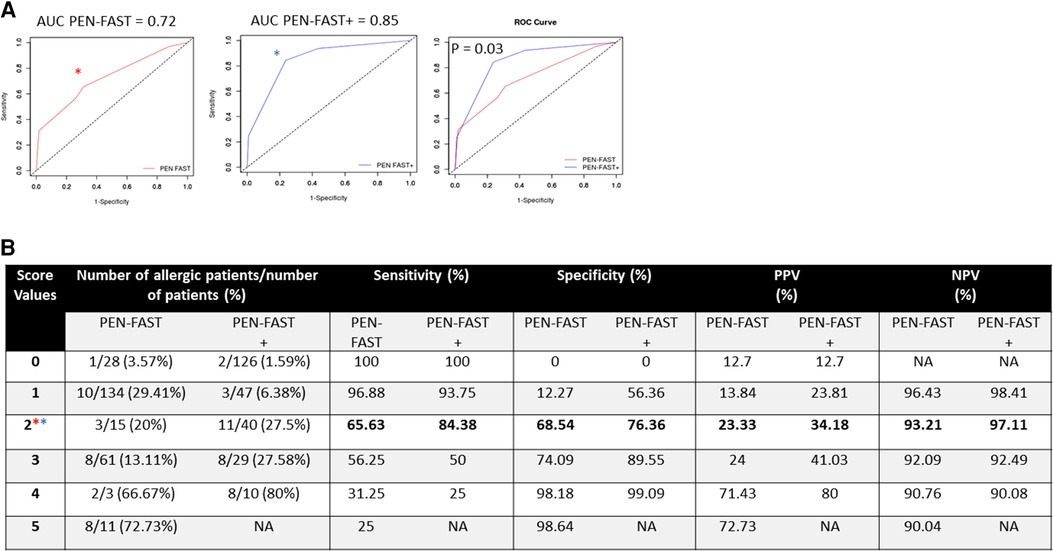
Figure 3. Diagnostic performances for PEN-FAST and PEN-FAST+. (A) Comparison of the AUC for PEN-FAST and PEN-FAST+. (B) Derivation of cutoff scores for clinical decision rules for PEN-FAST and PEN-FAST+, determining the statistical performance of the 2 tests using the Youden index: *Youden index PEN-FAST, *Youden index PEN-FAST+. AUC, area under the receiver operating characteristic curve; DPT, drug provocation test; HS, hypersensitivity; NA, not applicable; NPV, negative predictive value; PPV, positive predictive value; ST, skin test.
Different penicillin-allergy decision clinical rules have been proposed, with a risk of misclassifying truly sensitized patients from 3.7% to 10% (2, 9–11).Unfortunately, regardless of the score, the objective of 100% NPV is difficult to reach because of memory bias. The effectiveness of the PEN FAST score was recently validated in a multicenter randomized clinical trial involving 351 participants with a low-risk immediate penicillin allergy (PEN-FAST score <3) (7). The results demonstrated that direct oral penicillin DPT was non-inferior to the current standard of STs followed by 1-step oral DPT if the ST results were negative. However, this study exclusively analyzed patients with immediate HS occurring up to one hour after penicillin DPT. Moreover, MPE, the most common form of penicillin allergy, was not clearly distinguished in previous studies evaluating penicillin-allergy decision rules (2, 7, 9–11).
Although it is a mild form of delayed HS in the majority of cases, some studies have demonstrated that prolonged MPE (lasting more than 5–7 days), sometimes with systemic symptoms, may be an early form of drug reaction with eosinophilia and systemic symptoms (DRESS), a severe cutaneous adverse drug reaction, with an overlap between these two forms (12–14). The definition of severe MPE (1) has been proposed by Romano et al, but identifying these cases can be challenging for non-drug allergist specialists. In such cases, there is a risk of developing DRESS on subsequent re-exposure to penicillin. Therefore, it is clinically highly relevant to use a score with the highest NPV to ensure the confidence of physicians and their adherence to the guidelines.
PEN-FAST has been validated in large cohorts of patients with history of penicillin allergy worldwide (2, 7, 9). The 3 criteria selected for its calculation are easy for patients to remember and can be easily retrieved by non-allergist doctors.
Furthermore, there is a risk of false positives with immediate reading of STs. Among the two patients with a positive ST and a PEN-FAST score of less than 3, the possibility of a false positive result for the ST cannot be ruled out.
Conclusion
Our results suggest that the PEN-FAST+ score is a better tool for identifying penicillin-allergic patients, especially those with delayed HS with MPE lasting more than 7 days, which can be serious. A large prospective and multicentric study using PEN-FAST+ would be beneficial to better select patients at low risk of reaction, particularly those with delayed HS who could have a direct DPT without previous STs, for delabeling penicillin allergies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Sorbonne Universités Ethics Committee (Number 2021030514423). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JC: Data curation, Investigation, Writing – original draft. FC: Validation, Writing – review & editing. J-EA: Data curation, Writing – original draft. CT: Data curation, Validation, Writing – original draft. EA: Investigation, Writing – review & editing. AB: Validation, Writing – review & editing. AS: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2023.1302567/full#supplementary-material
References
1. Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet JC, et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams - an EAACI position paper. Allergy Juin. (2020) 75(6):1300–15. doi: 10.1111/all.14122
2. Trubiano JA, Vogrin S, Chua KYL, Bourke J, Yun J, Douglas A, et al. Development and validation of a penicillin allergy clinical decision rule. JAMA Intern Med. (2020) 180(5):745–52. doi: 10.1001/jamainternmed.2020.0403
3. Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and management of penicillin allergy: a review. JAMA. (2019) 321(2):188–99. doi: 10.1001/jama.2018.19283
4. Borch JE, Andersen KE, Bindslev-Jensen C. The prevalence of suspected and challenge-verified penicillin allergy in a university hospital population. Basic Clin Pharmacol Toxicol. (2006) 98(4):357–62. doi: 10.1111/j.1742-7843.2006.pto_230.x
5. Romano A, Valluzzi RL, Caruso C, Maggioletti M, Gaeta F. Non-immediate cutaneous reactions to beta-lactams: approach to aiagnosis. Curr Allergy Asthma Rep. (2017) 17(4):23. doi: 10.1007/s11882-017-0691-4
6. Salkind AR, Cuddy PG, Foxworth JW. The rational clinical examination. Is this patient allergic to penicillin? An evidence-based analysis of the likelihood of penicillin allergy. JAMA. (2001) 285(19):2498–505. doi: 10.1001/jama.285.19.2498
7. Copaescu AM, Vogrin S, James F, Chua KYL, Rose MT, De Luca J, et al. Efficacy of a clinical decision rule to enable direct oral challenge in patients with low-risk penicillin allergy: the PALACE randomized clinical trial. JAMA Intern Med. (2023) 183(9):944–52. doi: 10.1001/jamainternmed.2023.2986
8. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. (1988) 44(3):837–45. doi: 10.2307/2531595
9. Piotin A, Godet J, Trubiano JA, Grandbastien M, Guénard-Bilbault L, de Blay F, et al. Predictive factors of amoxicillin immediate hypersensitivity and validation of PEN-FAST clinical decision rule. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. (2022) 128(1):27–32. doi: 10.1016/j.anai.2021.07.005
10. Soria A, Masson N, Vial-Dupuy A, Gaouar H, Amsler E, Chollet-Martin S, et al. Allergological workup with half-dose challenge in iodinated contrast media hypersensitivity. Allergy. (2019) 74(2):414–7. doi: 10.1111/all.13638
11. Fransson S, Boel JB, Mosbech HF, Poulsen LK, Ruff S, Garvey LH. Safe De-labeling of patients at low risk of penicillin allergy in Denmark. Int Arch Allergy Immunol. (2022) 183(6):640–50. doi: 10.1159/000521708
12. Pinto Gouveia M, Gameiro A, Coutinho I, Pereira N, Cardoso JC, Gonçalo M. Overlap between maculopapular exanthema and drug reaction with eosinophilia and systemic symptoms among cutaneous adverse drug reactions in a dermatology ward. Br J Dermatol. (2016) 175(6):1274–83. doi: 10.1111/bjd.14704
13. Ortonne N, Valeyrie-Allanore L, Bastuji-Garin S, Wechsler J, de Feraudy S, Duong TA, et al. Histopathology of drug rash with eosinophilia and systemic symptoms syndrome: a morphological and phenotypical study. Br J Dermatol. (2015) 173(1):50–8. doi: 10.1111/bjd.13683
Keywords: penicillin allergy, diagnostic score, drug hypersensitivity, delayed hypersensitivity, PEN-FAST clinical decision rule, delabelling
Citation: Castagna J, Chasset F, Autegarden J-E, Le Thai C, Amsler E, Barbaud A and Soria A (2023) Assessing delayed penicillin hypersensitivity using the PENFAST+ score. Front. Allergy 4:1302567. doi: 10.3389/falgy.2023.1302567
Received: 27 September 2023; Accepted: 30 October 2023;
Published: 13 November 2023.
Edited by:
Igor Kaidashev, Poltava State Medical University, UkraineReviewed by:
Tetiana Umanets, National Academy of Sciences of Ukraine, UkraineSemanur Kuyucu, Mersin University, Türkiye
© 2023 Castagna, Chasset, Autegarden, Le Thai, Amsler, Barbaud and Soria. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Angèle Soria YW5nZWxlLnNvcmlhQGFwaHAuZnI=
†ORCID Julie Castagna orcid.org/0000-0002-9983-9521 François Chasset orcid.org/0000-0003-2580-8607 Emmanuelle Amsler orcid.org/0000-0001-5011-8056 Annick Barbaud orcid.org/0000-0001-8889-1589 Angèle Soria orcid.org/0000-0002-8726-6658