 Albert C. Chong
Albert C. Chong Neema Izadi
Neema Izadi Won Jong Chwa
Won Jong Chwa Jonathan S. Tam
Jonathan S. Tam
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Allergy , 16 October 2023
Sec. Food Allergy
Volume 4 - 2023 | https://doi.org/10.3389/falgy.2023.1277631
This article is part of the Research Topic Biomarkers in Allergic Eczema View all 7 articles
Background: Suspected strawberry and tomato (S/T) food allergy (FA) can be evaluated using specific immunoglobulin E (sIgE) testing despite its low specificity and positive predictive value.
Objective: This study aims to understand ordering patterns for S/T sIgE testing and identify relevant factors to clinical decision-making.
Methods: We retrospectively reviewed 814 patients with sIgE testing available for strawberries (651), tomatoes (276), or both (113) from January 2012 to May 2022 at a tertiary pediatric hospital. Patient demographics, provider specialty, and reasons for testing were collected. Student’s t-test and multiple regression analyses were performed to test the association between the S/T sIgE level and clinically relevant outcome (CRO) status. Fisher’s exact test and general linear models were used to evaluate and compare potential predictive factors for CRO status.
Results: Allergy and immunology, gastroenterology, and general pediatrics ordered most S/T sIgE testing. Testing was ordered most frequently for non-IgE-mediated gastrointestinal symptoms, mild possible IgE-mediated reactions, and eczema. Testing was most often ordered for infants and school-age children. Mean sIgE levels were higher for S/T tests resulting in a CRO when controlling for other predictor variables (p = 0.015; p = 0.002 for S/T, respectively). Only 2.2% and 5.4% of tests resulted in a CRO for S/T, and severe allergy was rare. Testing for non-IgE-mediated GI symptoms or eczema, or in non-atopic patients, yielded no CROs. Exposure and reaction history of present illness (ERH) was associated with CROs (p < 0.001; p = 0.04) with a high negative predictive value (99.5%; 100%) and low positive predictive value (11.5%; 15.0%). ERH (p < 0.001, η2 = 0.073; p = 0.009, η2 = 0.123) was a more significant predictor than the sIgE level (p = 0.002, η2 = 0.037; p = 0.212, η2 = 0.030) for CRO status.
Conclusion: The diagnosis of S/T food allergy is made primarily based on clinical history. S/T sIgE testing for children and adolescents should be avoided for patients without an ERH and in the workup of non-IgE-mediated GI symptoms. Testing for eczema and non-atopic patients is likely low-yield.
According to self-reported measures, food allergy (FA) is a major public health concern, affecting one in 13 children and one in 10 adults in the United States (US) (1, 2). Strawberry and tomato (S/T) are frequent suspects for FA as they are commonly consumed worldwide; however, these fruits may cause many non-allergic or local irritant reactions because they are highly acidic and may even cause pseudoallergic histamine release (3, 4). While accurate prevalence data are essential for developing effective strategies to prevent and manage FA, obtaining these measures is a complex and challenging task. The prevalence of strawberry allergy has been reported as 0.5%–4% in childhood (5); meanwhile, tomato allergy may account for 1.5% of FA in Northern Europe (6, 7). Severe reactions to S/T have rarely been described (8–10), and S/T allergy presents more often as pollen FA syndrome (PFAS), which is usually mild (11). A major mechanism of S/T PFAS is thought to involve cross-reactivity of strawberry Fra a 1 or tomato Sola l 4 to Bet v 1 in birch-pollen sensitized individuals, which may represent 8%–16% of Europe’s population and more than 100 million persons globally (12–15).
Specific immunoglobulin E (sIgE) testing is often ordered in the FA workup but may not always be appropriately applied given its low specificity and positive predictive value (16, 17). While identifying FA is critical for preventing life-threatening reactions, overdiagnosis may result in physical, mental, and financial consequences for patients and their caregivers (18–22). For example, food avoidance can lead to nutritional problems or the development of FAs from a delayed introduction of allergenic foods (23–25). Meanwhile, patients and caregivers may suffer a worse quality of life due to the daily challenge of acquiring allergen-free foods, fear of accidental exposure, and bullying of food-allergic children (22, 26, 27). Further, unnecessary testing increases medical costs. Per food, sIgE testing costs $15–$35 in the US and £15–£100 in the United Kingdom (28). The need for special foods and epinephrine autoinjectors greatly magnifies the financial burden of FAs (21, 29, 30).
Given the significant consequences of FA misdiagnosis, highly predictive sIgE thresholds would be greatly beneficial. Some thresholds have been determined for the most common food allergens (i.e., milk, egg, and peanut), and component testing has further improved diagnostic accuracy, particularly for peanut allergy (20, 31, 32). However, sIgE testing for S/T remains poorly studied. Recently, a retrospective study conducted in Spain studied 43 children with a self-reported history of strawberry allergy. Among these children, 67% had positive strawberry allergy testing, but 94% tolerated the fruit, bringing into question the relevance of reported reactions and testing (33). A similar study for tomato allergy has not been reported. To improve quality and value in FA care, we aim to understand provider ordering patterns for S/T sIgE testing and identify clinically relevant factors to guide decision-making for these tests.
All sIgE testing at our institution was performed on a Phadia 250 instrument (Thermo Fisher, Article #12-3900-01) using three positive controls (pooled human samples containing sIgE antibodies to house dust mite, common silver birch, or cat dander, respectively, for the high, medium, and low controls, all in 0.05% sodium azide) and one negative control (pooled human samples in 0.05% sodium azide without antibodies). The lower bound of testing was <0.35 kU/L prior to 2020 and <0.10 kU/L thereafter per manufacturer update. The upper bound was 100 kU/L for all samples.
We retrospectively reviewed 814 patients who had sIgE testing performed for strawberry (651), tomato (276), or both (113) from January 2012 to May 2022 at Children’s Hospital Los Angeles (CHLA). For patients with multiple S/T sIgE tests, the most recent test was used for analysis. Age at testing was grouped into one of five categories: infant (0–2 years old), preschool (3–6 years old), school age (6–12 years old), adolescence (13–17 years old), and adult (18 years old and over). Reasons for sending to S/T sIgE testing were determined from the ordering encounter note when available or the electronic test order form. We identified one or more testing reasons for each case using 10 categories: eczema, mild possible IgE-mediated reaction (i.e., hives, non-specific rash, and eye itching), severe possible IgE-mediated reaction (i.e., anaphylaxis), non-IgE-mediated gastrointestinal symptoms (i.e., abdominal pain, constipation, and diarrhea), PFAS (i.e., lip swelling and throat itching), unspecified reaction to S/T, previous positive S/T testing without a history of reaction, history of other food allergies, parental request otherwise not indicated, and unknown.
Data were filtered systematically (Figure 1) for whether sIgE testing was for strawberry or tomato allergy, reliability of outcome data (i.e., a clear recommendation from any specialty regarding S/T following S/T sIgE testing), documentation of a final outcome (i.e., patient told to avoid the tested food or patient recommended/allowed to continue eating the food), availability of rationale, availability of the provider note from the ordering encounter, and availability of atopy data. For diagnostic yield analyses, we defined a clinically relevant outcome (CRO) as a definitive outcome where the patient was ultimately told to avoid S/T or consume cautiously due to PFAS. For analyses involving testing rationale, all reasons for sending a single test were considered to maximize fidelity; this was accomplished by treating each reason documented as a separate testing data point. To explore the relevance of an exposure and reaction history of present illness (ERH), patients were positive for ERH if the patient (themselves or via caregiver) reported an exposure to the specific food (ingestion or cutaneous contact) with a subsequent reaction during the ordering encounter (no specific time to reaction was required). Patients were considered atopic if they were diagnosed with eczema, asthma, and/or allergic rhinitis by an allergy and immunology (A/I) specialist at our hospital.
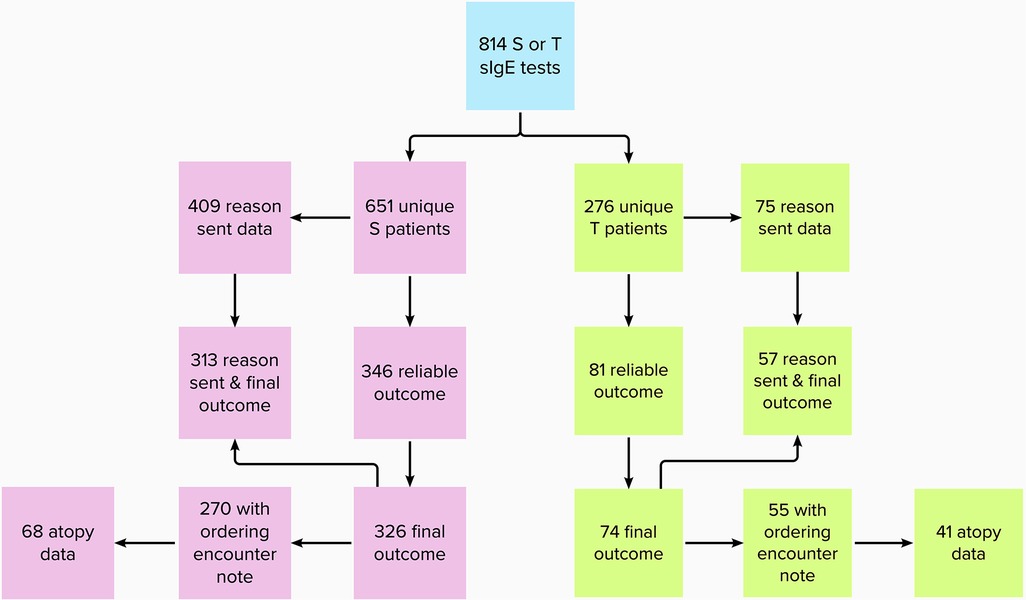
Figure 1. Flowchart of available data for each strawberry and tomato test.
Statistical analyses were conducted using SPSS (version 28, 2022) and Prism (version 9, 2022). Student’s t-test was used to compare the mean sIgE levels between CRO and non-CRO groups for each food. (“<0.10” and “<0.35” were converted to “0.35” for quantitative analysis, given different minimum thresholds before and after 2020.) Multiple regression was then performed to compare mean sIgE levels between CRO and non-CRO groups while controlling for age at testing, sex, ethnicity, and ordering specialty. Fisher’s exact test was used to evaluate associations between potential predictive factors (i.e., ERH and atopy) and having a CRO following S/T sIgE testing. A general linear model was employed to calculate partial eta-squared effect sizes for comparing the effect of ERH vs. S/T sIgE testing on CROs.
Our sample included 51.5% male participants for strawberry testing and 56.5% male participants for tomato testing. The mean age at testing was 7.7 ± 8.1 years for strawberry allergy and 8.8 ± 12.6 years for tomato allergy. Age distribution was bimodal, with the largest peak seen for infants (0–2 years old) (36.7%; 41.7%) and a second smaller peak observed for school-age children (6–12 years old) (27.0%; 23.6%) (Figure 2). Adults represented the smallest fraction for both S/T (4.1%; 9.4%) tests. Race/ethnicity for strawberry testing was 28.9% White, 4.3% Black, 7.1% Hispanic/Latino, 6.0% Asian/Pacific Islander, 1.2% multiple, 20.1% other, and 32.4% unknown; for tomato testing, race/ethnicity was 22.8% White, 5.4% Black, 7.2% Hispanic/Latino, 5.8% Asian/Pacific Islander, 0.4% multiple, 22.5% other, and 35.9% unknown. Inpatients represented only 0.8% (5/651) and 1.4% (4/271) of S/T sIgE tests, respectively. Atopy was present in 60.6% (86/142) of patients tested for strawberry allergy and 61.2% (52/85) of patients tested for tomato allergy seen and with testing ordered by A/I specialists at CHLA.
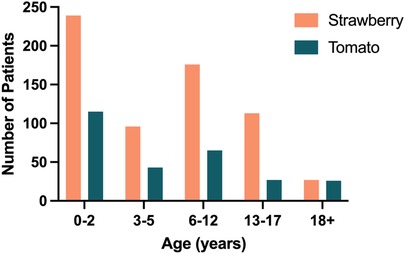
Figure 2. Number of patients in each age group with strawberry and tomato testing.
The specialty of the ordering provider was available for 651 strawberry and 274 tomato tests (Figure 3). A/I, GI, and general pediatrics (GP) were the top ordering specialties, accounting for 97.8% and 98.2% of S/T sIgE tests, respectively. For strawberry allergy, GI (43.0%) ordered the most tests, followed by A/I (38.2%) and GP (16.6%). For tomato allergy, A/I (68.7%) ordered the most tests, followed by GP (23.7%) and GI (5.8%).

Figure 3. Specialty ordering strawberry and tomato testing.
Reasons for sIgE testing were available for 409 strawberry and 75 tomato tests (Figure 4). Non-IgE-mediated gastrointestinal symptoms, mild possible IgE-mediated reactions, and eczema were the top reasons, accounting for 90.9% of strawberry and 66.7% of tomato tests. For strawberry allergy, non-IgE-mediated gastrointestinal symptoms (60.1%) were the most common reason for testing, followed by mild possible IgE-mediated reactions (24.7%) and eczema (6.1%). For tomato allergy, mild possible IgE-mediated reactions (32%) were the most common reason, followed by non-IgE-mediated gastrointestinal symptoms (20%) and eczema (14.7%). PFAS symptoms (4.2%; 9.3%) and a history of other food allergies (2.0%; 12%) were the next most common reasons for S/T testing, respectively.
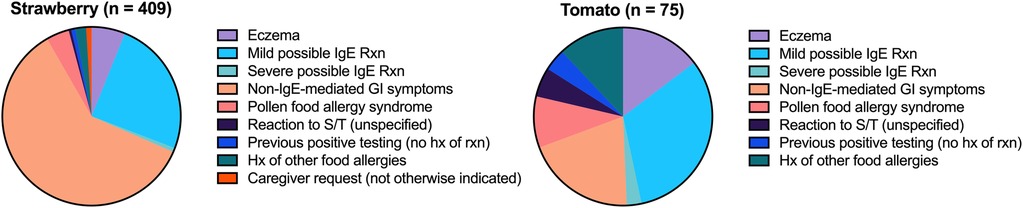
Figure 4. Reasons for strawberry and tomato testing.
Final outcome data were available for 326 strawberry and 74 tomato cases. Of these, 2.15% (7/326) and 5.41% (4/74) of S/T sIgE tests resulted in a CRO. PFAS represented 42.9% (3/7) and 50% (2/4) of these CROs for S/T, respectively. For the four non-PFAS cases where the patient was ultimately told to avoid strawberries, reasons for avoidance included anaphylaxis, rash, unspecified acute reaction, and concern for strawberry allergy due to unspecified blueberry allergy. For the two non-PFAS tomato cases, rash (specifically eczema and hives) and unspecified acute reaction were the reasons for avoidance. Only one patient required epinephrine administration for strawberry allergy (0.3%, 1/326), and epinephrine was never required for tomato allergy (0/74).
sIgE levels were available for all cases with final outcome data (7 and 4 with CROs and 319 and 70 without CROs for S/T, respectively). The mean sIgE levels for S/T tests resulting in CROs were 5.5 ± 5.8 kU/L and 12.5 ± 1.7 kU/L, respectively. For tests without CROs, the mean sIgE levels were 0.9 ± 4.0 kU/L and 1.8 ± 3.7 kU/L, respectively. For both foods, the mean sIgE level was significantly higher among S/T tests resulting in CROs vs. no CROs (p = 0.003; p < 0.001 for S/T, respectively). Multiple linear regression models, including CRO status and other covariates, significantly predicted sIgE levels for strawberry [F(5,320) = 3.730, p = 0.003] and tomato [F(5,68) = 2.633, p = 0.031] allergy (Supplementary Material A). For strawberry allergy, CRO status (p = 0.015) and ordering specialty (p = 0.015) predicted sIgE levels, while for tomato allergy, only CRO status (p = 0.002) predicted sIgE levels.
Age at testing was available for all cases with final outcome data. Following strawberry sIgE testing, CROs were observed for all age groups prior to adulthood: 2.3% (2/88) for infants, 4.3% (2/47) for preschool children, 1.0% (1/99) for school-age children, 2.4% (2/83) for adolescents, and 0% (0/9) for adults. One infant and two preschool children accounted for the three strawberry PFAS outcomes. Following tomato testing, CROs were observed for 7.1% (2/28) of school-age children and 18.2% (2/11) of adolescents but not for any other age group (0/17 for infants, 0/12 for preschool children, and 0/6 for adults). Adolescents accounted for the only two PFAS outcomes after tomato sIgE testing.
Filtering for cases with a documented reason to test and final outcome data resulted in 313 strawberry and 57 tomato cases (Table 1). S/T sIgE testing for non-IgE-mediated GI symptoms or eczema resulted in no CROs. Testing for PFAS symptoms yielded 21.4% and 40% CROs for S/T, respectively. Testing for mild and severe possible IgE-mediated reactions resulted in some CROs for strawberry allergy but none for tomato allergy.
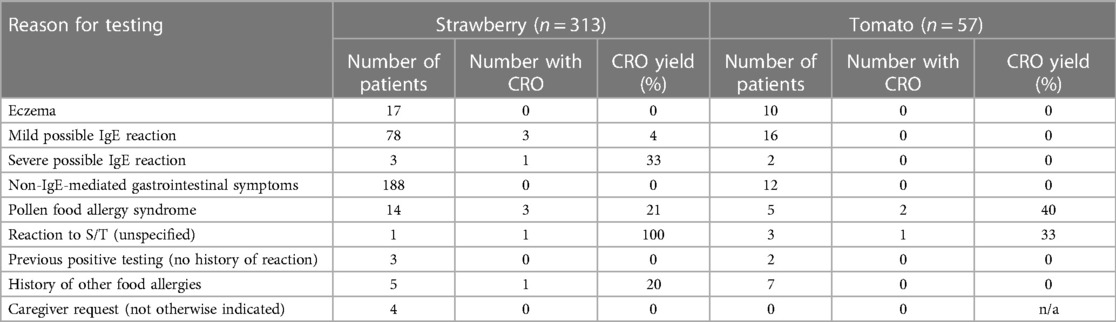
Table 1. CRO yield by reason for strawberry and tomato testing.
An ordering encounter note and final outcome data were available for 270 strawberry and 55 tomato tests. ERH was significantly associated with a CRO following sIgE testing for S/T (p < 0.001; p = 0.04) with a high negative predictive value (99.5%; 100%) and a low positive predictive value (11.5%; 15.0%) (Figure 5). For strawberry cases, ERH significantly predicted CROs (p < 0.001) with a medium effect size (η2 = 0.073), while sIgE levels also significantly predicted CROs (p = 0.002), albeit with a small effect size (η2 = 0.037). For tomato cases, ERH significantly predicted CROs (p = 0.009) with a large effect size (η2 = 0.123), while sIgE levels did not (p = 0.212, η2 = 0.030).

Figure 5. ERH was highly associated with CROs for strawberry and tomato testing.
An ordering encounter note and final outcome data from A/I providers at our hospital were available for 68 strawberry and 41 tomato cases. Among this subgroup of cases, atopy was present in 75.0% (51/68) of strawberry and 78.0% (32/41) of tomato patients. None of the non-atopic S/T patients had a CRO following S/T sIgE testing (0/17; 0/9 for S/T, respectively). Meanwhile, 11.8% (6/51) and 9.4% (3/32) of atopic patients had a CRO following S/T testing, respectively. The association between atopic status and CRO following S/T sIgE testing was not statistically significant even when both were considered together (p = 0.11).
Our study characterized the ordering patterns for more than 800 S/T sIgE tests at a tertiary pediatric hospital over 10 years and assessed factors that may influence diagnostic yield. S/T sIgE testing was most frequent for infants, reflecting caregiver and provider prioritization of establishing allergenic triggers with initial food introduction. Testing decreased for preschool children before increasing again for school-age children, which may reflect the increased risk of exposure to new foods with the start of school. At our hospital, S/T sIgE testing was almost exclusively used by A/I, GI, and general pediatrics and rarely by any other specialty. For both foods, mild possible IgE-mediated reactions, non-IgE-mediated gastrointestinal symptoms, and eczema were the most frequent reasons for testing.
Mean sIgE levels were significantly higher for S/T tests with a CRO, yet diagnostic yield was quite low, with only 2.2% (7/326) and 5.4% (4/74) of tests yielding a CRO. While the prevalence of S/T allergy was low in our sample, it is likely even lower in the general population. Patients in this study were suspected to have S/T allergy before testing and thus had an elevated pretest probability for a CRO. Further, atopy is associated with food allergy (34–37), and the presence of atopy in our sample was 2–8-fold higher than in the general population of developed countries (10%–30%) (38, 39). Perhaps expectedly, PFAS represented more than 40% of these CROs following S/T sIgE testing for both foods. Given the low CRO yields and rare S/T reactions in our cohort, more judicious testing for these foods should be considered.
Strikingly, non-IgE-mediated gastrointestinal symptoms accounted for more than 60% of strawberry tests despite no current evidence suggesting the benefit of sIgE testing for non-IgE-mediated gastrointestinal symptoms. Specialties other than A/I accounted for the majority of tests. Given that IgE testing for non-IgE-mediated gastrointestinal symptoms is contrary to known pathophysiology, it is unsurprising that none of the 188 strawberry sIgE tests sent for non-IgE-mediated gastrointestinal symptoms with final outcome data resulted in a CRO. This underscores the need for education on the situational value of IgE testing to specialties outside of A/I. Non-IgE-mediated gastrointestinal symptoms accounted for 20% of tomato tests. As with strawberry cases, this testing yielded no CROs. These findings highlight an opportunity to optimize ordering patterns by avoiding S/T sIgE testing for GI symptoms that are unlikely to be IgE-driven.
Atopic dermatitis (AD) is another condition for which S/T sIgE testing may not be helpful. Recent evidence suggests a limited role for sIgE testing (40) in AD management and mixed results from anti-IgE therapies (41). Of 17 strawberry and 10 tomato sIgE tests sent for “atopic dermatitis” or “eczema,” none resulted in a CRO. These results support the current understanding that food is not the primary cause of AD (42) and that dietary elimination for AD has little benefit and more potential for harm (40). Meanwhile, patients with AD tend to have higher sIgE levels to many allergens, many of which may have no clinical relevance, which reduces any utility of sIgE testing in AD (43). In this context, our data support that S/T sIgE testing is not indicated in the evaluation of most eczema.
S/T testing for PFAS symptoms and strawberry testing for possible IgE-mediated reactions had some CROs. CROs were expected when testing for PFAS symptoms for S/T, given that fruits are common triggers of PFAS, which is IgE-mediated (44, 45). However, PFAS may be diagnosed from clinical history and testing for pollen sensitization and generally does not require testing for specific foods. Meanwhile, testing for mild and severe possible IgE-mediated reactions resulted in only a small number of CROs for strawberry allergy and none for tomato allergy, suggesting that S/T infrequently cause IgE-mediated allergy beyond PFAS.
From an age standpoint, tomato sIgE testing resulted in no CROs for children under 11 years old (0/29), suggesting that tomato sIgE testing may not be of value for infants and preschool children. Furthermore, tomato sIgE resulted in PFAS only with the start of adolescence, consistent with previous observations that PFAS is less common in younger children (45). These trends were not observed for strawberry allergy, for which CROs were found for all age groups prior to adulthood and PFAS was found in patients under 6 years old and even in infants.
We also evaluated the potential relevance of an ERH or atopy in the decision to order S/T testing. Interestingly, the absence of an ERH made a CRO following S/T sIgE testing statistically unlikely, with high negative predictive values for both strawberry (99.5%) and tomato (100%) fruits. Alternatively, the presence of an ERH could not reliably predict a CRO with low positive predictive values for both strawberry (11.5%) and tomato (15.0%) fruits. Thus, a negative ERH may largely rule out S/T allergy. Furthermore, results showed that ERH rather than sIgE testing had a greater bearing on CRO status, revealing the importance of taking a good clinical history and that, in many cases, sIgE testing may not affect management. Regarding atopy, non-atopic patients were never found to have a CRO following testing (0/26). While this is consistent with increased atopy with FA, our study was underpowered to evaluate this association due to a lack of relevant data.
Our report had several limitations. Owing to the retrospective nature of this study and our relatively strict systematic approach to analysis, data were not always available. Racial/ethnic composition was also unclear in many instances. Regarding the reasons for testing analysis, since multiple reasons could be provided for a single sIgE test, we could not ascertain which of these reasons was linked to CROs in these cases. Finally, since our sample was largely pediatric, extrapolation of these findings to the adult population is limited.
At a large tertiary pediatric center, S/T sIgE testing was predominately ordered by A/I, GI, and GP, mostly for infants and school-age children. Clinical history rather than serological testing was the primary determinant of CRO status. ERH had a very high negative predictive value but a poor positive predictive value for CROs. Although mean sIgE levels were higher for S/T tests resulting in CROs, the overall yield was quite low. A large number of strawberry tests were sent for non-IgE-mediated gastrointestinal symptoms with no CROs. Further, S/T tests may have minimal yield for patients without atopy and in the workup of most eczema, although larger studies are needed to confirm these additional findings. Taken together, the threshold for ordering sIgE testing for S/T may need to be re-evaluated.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Children’s Hospital Los Angeles IRB. The studies were conducted in accordance with local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
AC: Methodology, Investigation, Data Curation, Formal Analysis, Writing – Original draft, Visualization. NI: Conceptualization, Methodology, Data Curation, Writing – Review & editing, Resources. WC: Methodology, Formal Analysis, Writing – Review & editing. JT: Conceptualization, Methodology, Writing – Review & editing, Resources, Supervision.
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors thank Dr. Richard M Watanabe for advising on statistical analysis methods and Ms. BeeChoo Liang for her technical assistance in the preparation of Table 1.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2023.1277631/full#supplementary-material
Supplementary Table S1
Specific immunoglobulin E level regression models.
S/T, strawberry and tomato; FA, food allergy; sIgE, specific immunoglobulin E; CRO, clinically relevant outcome; US, United States; PFAS, pollen food allergy syndrome; A/I, allergy and immunology; GI, gastroenterology; GP, general pediatrics; ERH, exposure and reaction history of present illness; AD, atopic dermatitis.
1. Gupta RS, Warren CM, Smith BM, Blumenstock JA, Jiang J, Davis MM, et al. The public health impact of parent-reported childhood food allergies in the United States. Pediatrics. (2018) 142(6):e20181235. doi: 10.1542/peds.2018-1235
2. Gupta RS, Warren CM, Smith BM, Jiang J, Blumenstock JA, Davis MM, et al. Prevalence and severity of food allergies among US adults. JAMA Netw Open. (2019) 2(1):e185630. doi: 10.1001/jamanetworkopen.2018.5630
3. Ballmer-Weber BK, Hoffmann-Sommergruber K. Molecular diagnosis of fruit and vegetable allergy. Curr Opin Allergy Clin Immunol. (2011) 11(3):229–35. doi: 10.1097/ACI.0b013e3283464c74
4. Aninowski M, Kazimierczak R, Hallmann E, Rachtan-Janicka J, Fijoł-Adach E, Feledyn-Szewczyk B, et al. Evaluation of the potential allergenicity of strawberries in response to different farming practices. Metabolites. (2020) 10(3):102. doi: 10.3390/metabo10030102
5. Bajraktarevic A, Trninic S, Penava S, Mahinic A, Begovic B, Selmovic A, et al. Prevalence of strawberry allergy in Bosnian children and management. Clin Transl Allergy. (2011) 1(1):45. doi: 10.1186/2045-7022-1-S1-P45
6. Petersen A, Vieths S, Aulepp H, Schlaak M, Becker WM. Ubiquitous structures responsible for IgE cross-reactivity between tomato fruit and grass pollen allergens. J Allergy Clin Immunol. (1996) 98(4):805–15. doi: 10.1016/s0091-6749(96)70130-6
8. Collins A, Derkenne B, Giebels K, Carvelli T. [Strawberry and raspberry anaphylaxis]. Rev Med Liege. (2020) 75(7–8):494–6.32779896
9. Larramendi CH, Ferrer A, Huertas AJ, García-Abujeta JL, Andreu C, Tella R, et al. Sensitization to tomato peel and pulp extracts in the Mediterranean coast of Spain: prevalence and co-sensitization with aeroallergens. Clin Exp Allergy J Br Soc Allergy Clin Immunol. (2008) 38(1):169–77. doi: 10.1111/j.1365-2222.2007.02865.x
10. Kim M, Ahn Y, Yoo Y, Kim DK, Yang HJ, Park HS, et al. Clinical manifestations and risk factors of anaphylaxis in pollen-food allergy syndrome. Yonsei Med J. (2019) 60(10):960–8. doi: 10.3349/ymj.2019.60.10.960
11. Carlson G, Coop C. Pollen food allergy syndrome (PFAS): a review of current available literature. Ann Allergy Asthma Immunol. (2019) 123(4):359–65. doi: 10.1016/j.anai.2019.07.022
12. Kurze E, Kock V, Lo Scalzo R, Olbricht K, Schwab W. Effect of the strawberry genotype, cultivation and processing on the Fra a 1 allergen content. Nutrients. (2018) 10(7):857. doi: 10.3390/nu10070857
13. Kurze E, Lo Scalzo R, Campanelli G, Schwab W. Effect of tomato variety, cultivation, climate and processing on Sola l 4, an allergen from Solanum lycopersicum. PLoS One. (2018) 13(6):e0197971. doi: 10.1371/journal.pone.0197971
14. Biedermann T, Winther L, Till SJ, Panzner P, Knulst A, Valovirta E. Birch pollen allergy in Europe. Allergy. (2019) 74(7):1237–48. doi: 10.1111/all.13758
15. Akinfenwa O, Huang HJ, Linhart B, Focke-Tejkl M, Vrtala S, Poroshina A, et al. Preventive administration of non-allergenic Bet v 1 peptides reduces allergic sensitization to major birch pollen allergen, Bet v 1. Front Immunol. (2021) 12:744544. doi: 10.3389/fimmu.2021.744544
16. Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. (2010) 126(6 Suppl):S1–58. doi: 10.1016/j.jaci.2010.10.007
17. Santos AF, Brough HA. Making the most of in vitro tests to diagnose food allergy. J Allergy Clin Immunol Pract. (2017) 5(2):237–48. doi: 10.1016/j.jaip.2016.12.003
18. Robbins KA, Guerrerio AL, Hauck SA, Henry BJ, Keet CA, Brereton NH, et al. Growth and nutrition in children with food allergy requiring amino acid-based nutritional formulas. J Allergy Clin Immunol. (2014) 134(6):1463–6.e5. doi: 10.1016/j.jaci.2014.08.053
19. Abrams EM, Greenhawt M, Alqurashi W, Singer AG, Shaker M. The revenge of unintended consequences of anaphylaxis-risk overdiagnosis: how far we have come and how far we have to go. J Allergy Clin Immunol Pract. (2021) 9(11):3911–7. doi: 10.1016/j.jaip.2021.05.038
20. Gupta M, Cox A, Nowak-Węgrzyn A, Wang J. Diagnosis of food allergy. Immunol Allergy Clin North Am. (2018) 38(1):39–52. doi: 10.1016/j.iac.2017.09.004
21. Shroba J, Das R, Bilaver L, Vincent E, Brown E, Polk B, et al. Food insecurity in the food allergic population: a work group report of the AAAAI adverse reactions to foods committee. J Allergy Clin Immunol Pract. (2022) 10(1):81–90. doi: 10.1016/j.jaip.2021.10.058
22. Khamsi R. Food allergies: the psychological toll. Nature. (2020) 588(7836):S4–6. doi: 10.1038/d41586-020-02778-4
23. Alvarez A, Gupta M, Poowuttikul P, Baptist AP. Are primary care physicians following National Institute of Allergy and Infectious Disease guidelines for the prevention of peanut allergy? A survey-based study. Allergy Asthma Proc. (2020) 41(3):167–71. doi: 10.2500/aap.2020.41.200019
24. Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med. (2015) 372(9):803–13. doi: 10.1056/NEJMoa1414850
25. Skjerven HO, Lie A, Vettukattil R, Rehbinder EM, LeBlanc M, Asarnoj A, et al. Early food intervention and skin emollients to prevent food allergy in young children (PreventADALL): a factorial, multicentre, cluster-randomised trial. Lancet. (2022) 399(10344):2398–411. doi: 10.1016/S0140-6736(22)00687-0
26. Teufel M, Biedermann T, Rapps N, Hausteiner C, Henningsen P, Enck P, et al. Psychological burden of food allergy. World J Gastroenterol. (2007) 13(25):3456–65. doi: 10.3748/wjg.v13.i25.3456
27. Feng C, Kim JH. Beyond avoidance: the psychosocial impact of food allergies. Clin Rev Allergy Immunol. (2019) 57(1):74–82. doi: 10.1007/s12016-018-8708-x
28. Chong AC, Diwakar L, Kaplan CM, Fox AT, Abrams EM, Greenhawt M, et al. Provision of food allergy care in the United Kingdom and United States: current issues and future directions. J Allergy Clin Immunol Pract. (2023) S2213–2198(23):00316-1. doi: 10.1016/j.jaip.2023.03.029
29. Gupta R, Holdford D, Bilaver L, Dyer A, Holl JL, Meltzer D. The economic impact of childhood food allergy in the United States. JAMA Pediatr. (2013) 167(11):1026–31. doi: 10.1001/jamapediatrics.2013.2376
30. Chua KP, Conti RM. Out-of-pocket spending among commercially insured patients for epinephrine autoinjectors between 2007 and 2014. JAMA Intern Med. (2017) 177(5):736–9. doi: 10.1001/jamainternmed.2017.0252
31. Treudler R, Simon JC. Overview of component resolved diagnostics. Curr Allergy Asthma Rep. (2013) 13(1):110–7. doi: 10.1007/s11882-012-0318-8
32. Nicolaou N, Poorafshar M, Murray C, Simpson A, Winell H, Kerry G, et al. Allergy or tolerance in children sensitized to peanut: prevalence and differentiation using component-resolved diagnostics. J Allergy Clin Immunol. (2010) 125(1):191–7.e1–13. doi: 10.1016/j.jaci.2009.10.008
33. Cabrera-Freitag P, Bermejo Becerro A, Abreu Ramírez MG, Álvarez-Perea A, Infante Herrero S, Fuentes-Aparicio V, et al. Allergy to strawberry in children from the Mediterranean area: is it really allergy? J Investig Allergol Clin Immunol. (2020) 30(4):283–5. doi: 10.18176/jiaci.0491
34. Baral VR, Hourihane JO. Food allergy in children. Postgrad Med J. (2005) 81(961):693–701. doi: 10.1136/pgmj.2004.030288
35. Tsakok T, Marrs T, Mohsin M, Baron S, du Toit G, Till S, et al. Does atopic dermatitis cause food allergy? A systematic review. J Allergy Clin Immunol. (2016) 137(4):1071–8. doi: 10.1016/j.jaci.2015.10.049
36. Al-Abri R, Al-Amri AS, Al-Dhahli Z, Varghese AM. Allergic rhinitis in relation to food allergies. Sultan Qaboos Univ Med J. (2018) 18(1):e30–3. doi: 10.18295/squmj.2018.18.01.005
37. Liu AH, Jaramillo R, Sicherer SH, Wood RA, Bock SA, Burks AW, et al. National prevalence and risk factors for food allergy and relationship to asthma: results from the National Health and Nutrition Examination Survey 2005–2006. J Allergy Clin Immunol. (2010) 126(4):798–806.e13. doi: 10.1016/j.jaci.2010.07.026
38. Justiz Vaillant AA, Modi P, Jan A. Atopy. In: Statpearls. Treasure Island: StatPearls Publishing (2023). 31194344. Available at: http://www.ncbi.nlm.nih.gov/books/NBK542187/ (Accessed April 26, 2023).
39. Carr RD, Berke M, Becker SW. Incidence of atopy in the general population. Arch Dermatol. (1964) 89(1):27–32. doi: 10.1001/archderm.1964.01590250033006
40. Oykhman P, Dookie J, Al-Rammahy H, de Benedetto A, Asiniwasis RN, LeBovidge J, et al. Dietary elimination for the treatment of atopic dermatitis: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. (2022) 10(10):2657–66.e8. doi: 10.1016/j.jaip.2022.06.044
41. Wollenberg A, Thomsen SF, Lacour JP, Jaumont X, Lazarewicz S. Targeting immunoglobulin E in atopic dermatitis: a review of the existing evidence. World Allergy Organ J. (2021) 14(3):100519. doi: 10.1016/j.waojou.2021.100519
42. Chong AC, Visitsunthorn K, Ong PY. Genetic/environmental contributions and immune dysregulation in children with atopic dermatitis. J Asthma Allergy. (2022) 15:1681–700. doi: 10.2147/JAA.S293900
43. Ramírez-Marín HA, Singh AM, Ong PY, Silverberg JI. Food allergy testing in atopic dermatitis. JAAD Int. (2022) 9:50–6. doi: 10.1016/j.jdin.2022.08.004
44. Skypala IJ, Hunter H, Krishna MT, Rey-Garcia H, Till SJ, du Toit G, et al. BSACI guideline for the diagnosis and management of pollen food syndrome in the UK. Clin Exp Allergy J Br Soc Allergy Clin Immunol. (2022) 52(9):1018–34. doi: 10.1111/cea.14208
Keywords: food allergy, strawberry, tomato, immunoglobulin E, pediatric
Citation: Chong AC, Izadi N, Chwa WJ and Tam JS (2023) Fruitful or unfruitful: strawberry and tomato specific immunoglobulin E testing at a tertiary pediatric center. Front. Allergy 4:1277631. doi: 10.3389/falgy.2023.1277631
Received: 14 August 2023; Accepted: 18 September 2023;
Published: 16 October 2023.
Edited by:
Richard L. Wasserman, Medical City Children’s Hospital, United StatesReviewed by:
Jay Lieberman, University of Tennessee Health Science Center (UTHSC), United States© 2023 Chong, Izadi, Chwa and Tam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan S. Tam anN0YW1AY2hsYS51c2MuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.