
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Allergy , 25 August 2023
Sec. Rhinology
Volume 4 - 2023 | https://doi.org/10.3389/falgy.2023.1223427
This article is part of the Research Topic 2022 in Review: Rhinology View all 8 articles
 Shaimaa Albloushi1,†
Shaimaa Albloushi1,† Mona Al-Ahmad1,2*†
Mona Al-Ahmad1,2*†
Introduction: Despite well-defined clinical phenotypes of chronic rhinitis, the underlying in-depth pathophysiological mechanism, particularly with reference to the involvement of immune mediators, genetic, and environmental factors, are still not fully understood. Therefore, our aim was to give updated information on the pathogenesis of allergic rhinitis (AR), with an emphasis on the role of cytokines in adults aged 18 years and above. Additionally, we investigated the impact of genetic and environmental factors in the pathogenesis of AR.
Results: A search in various databases identified 1,178 records, and 18 studies were ultimately selected from January 2018 to April 2023. The total sample size in our studies was 4,317, with 2,186 in the experimental and 2,131 in control groups, respectively. The mean age was 33.4 years, with 43% were male, while 57% were female. According to the selected studies, various factors, including immune mediators, particularly cytokines, genetic, and environmental factors, were identified in the development of AR.
Conclusion: The selected studies presented findings on different factors and sub-factors in the pathogenesis of AR, making it a challenge for us to compare their results. However, based on our findings, researchers can link our identified factors to potential therapies for AR.
In order to effectively treat a disease, understanding its true underlying mechanism is essential (1). Unfortunately, for many chronic diseases, these mechanisms are not fully understood, which leads to a reliance on symptom-based management. Chronic rhinitis is one such disease (2). It refers to inflammation of the nasal mucosa that persists for a minimum of 12 weeks each year (3). Allergic rhinitis (AR) and non-allergic rhinitis (NAR) are two well-recognized subgroups of rhinitis (4).
The pathogenesis of chronic rhinitis is linked to immune mediators, environmental, genetic, and epigenetic factors. However, the available data is insufficient to draw definitive conclusions about the involvement of these factors particularly in AR (5). The available data have focused on the role of environment, genetics, and epigenetics in the pathogenesis of AR. The development of AR in individuals with atopic tendencies is believed to be strongly influenced by their exposure to various external environmental factors (6). Other than environmental factors, various genes associated with immune-related diseases, such as allergic and autoimmune disorders, are also involved (7).
The prevalence of AR varies among studies due to the lack of an acceptable definition for both conditions (8, 9). A review by Savoure et al. reported a wide range of prevalence, varying from 1% to 63% from 184 studies. The overall median prevalence rates of unspecified rhinitis, and AR, were 29.4% and 18.1%, respectively (9). The severity of chronic rhinitis, particularly AR symptoms, is associated with lower quality of life. A large Spanish cohort study concluded that AR symptoms have a considerable impact on the quality of life and sleep quality for all patients with AR (10).
However, despite well-defined clinical phenotypes of chronic rhinitis, the underlying pathophysiological mechanism, particularly with reference to the involvement of cytokines, genetic, and environmental factors, is still not fully understood (2). The significance of cytokines in AR is considered more significant among these factors. Cytokines possess roles that depend on the context and determine their usual physiological function. However, when cytokine pathways become dysregulated or chronically activated, they can disrupt the equilibrium of tissues, moving away from a state of balanced stability toward immunopathology associated with disease (11). The aim of the review was to give updated information on the pathogenesis of AR at the molecular level, with an emphasis on the role of cytokines in adults aged 18 years and above. Additionally, we investigated the impact of genetic and environmental factors in the pathogenesis of AR.
On May 02, 2023, a literature search was conducted based on PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The search included relevant articles published between 2018 and 2023 in PubMed, Scopus, Wiley online library, and Google Scholar. Keywords such as Rhinitis, Chronic rhinitis, Allergic rhinitis, Non-Allergic Rhinitis, Pathophysiology, Etiology, Mechanism, Environmental factors, Epigenetic factors, Inflammatory Mediators, Inflammatory Biomarkers, Cytokines, Interleukin, Interferon, Chemokines, and Immune mediators were used in various combinations. The searches were conducted separately for each primary database using Boolean operators (AND) and (OR) in combination with Medical Subject Subheadings (MeSH) terms and key text words.
Our inclusion criteria include controlled trials that investigated the role of cytokines, genetic factors, and environmental factors in the pathogenesis of AR. Experimental or animal studies, non-English language studies, non-peer-reviewed studies, conference abstracts, papers, letters, and unpublished manuscripts were excluded. Likewise, studies that investigated the pathogenesis for coexistence of AR with other diseases were also excluded.
The potential studies were initially screened based on their abstracts and article titles. Subsequently, full-text articles of potential studies were evaluated by two independent researchers. Any discrepancies were discussed until a consensus was reached to ensure the accuracy of the research. We utilized descriptive statistics, such as mean and median, to obtain summary measures.
A search was conducted in databases as well as other sources like relevant journals and bibliographic searches, resulting in the identification of 1,178 records. After a screening process based on titles, abstracts, and full-text articles, 103 articles were screened. Out of the 103 articles, 85 were excluded for not meeting the inclusion criteria, such as not being a controlled trial, involving patients under 18 years of age, studied only the correlation of different factors in the pathogenesis of AR with drugs, or was centered on the pathogenesis non-allergic rhinitis or mixed rhinitis. In the end, 14 studies from January 2018 to April 2023 were ultimately selected. These studies were chosen based on their relevance to immune mediators i.e., cytokines, genetic factors, and environmental factors in the pathogenesis of AR. The PRISMA flow chart in Figure 1 illustrates the selection process of the studies.
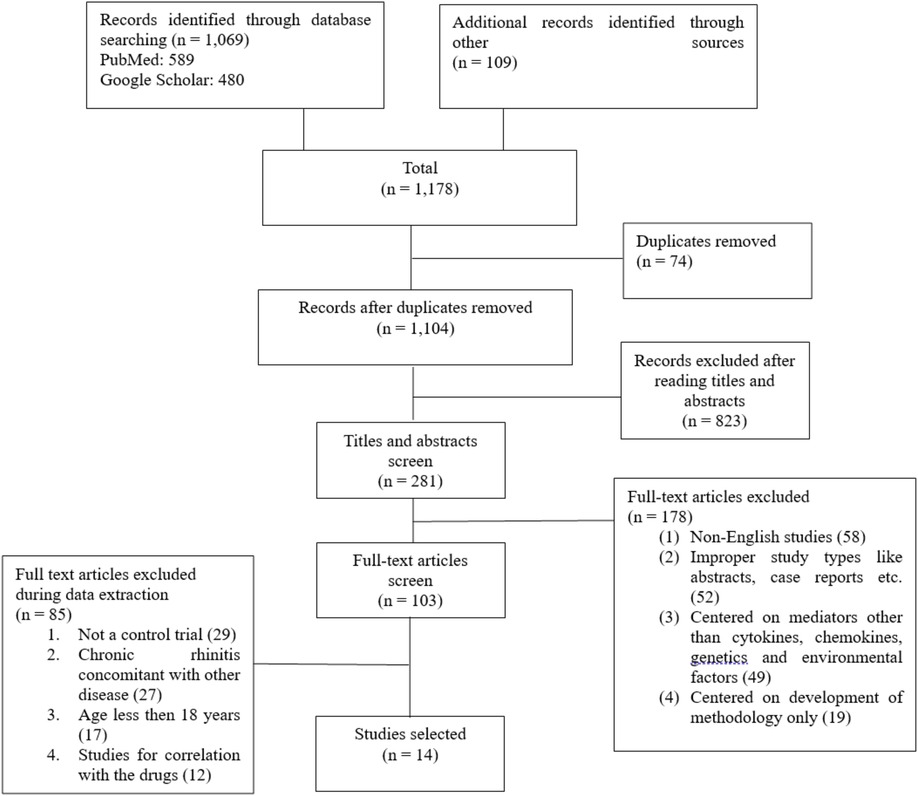
Figure 1. PRISMA flowchart for the searching and screening studies.
The studies selected for analysis comprised of seven conducted in China, three in Iran, and one each in Turkey, Malaysia, Romania, and Australia. Out of the 14 selected studies, four were cross-sectional, five were case-control, two were comparative studies, and three were genome-wide association studies (GWAS). The total sample size for these studies was 4,317, with 2,186 in the experimental and 2,131 in the control groups, respectively. The mean age was 33.4 years with 43% were male, while 57% were female. Various diagnostic criteria were used for the diagnosis of AR, including clinical examination, allergic rhinitis and its impact on asthma (ARIA) guidelines (12), and skin prick tests, among others. The detailed analysis of the characteristics of the selected studies are presented in Tables 1–3.
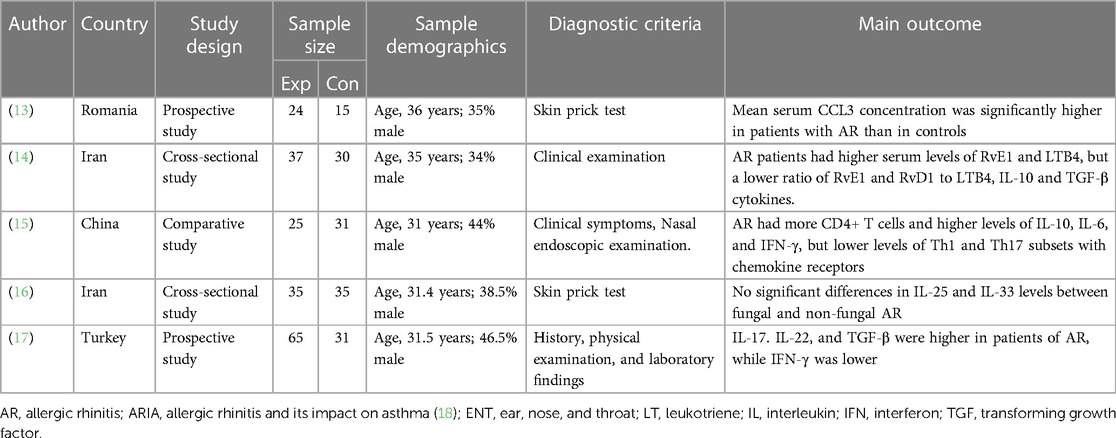
Table 1. Investigation of immune mediators in AR: characteristics of included studies.
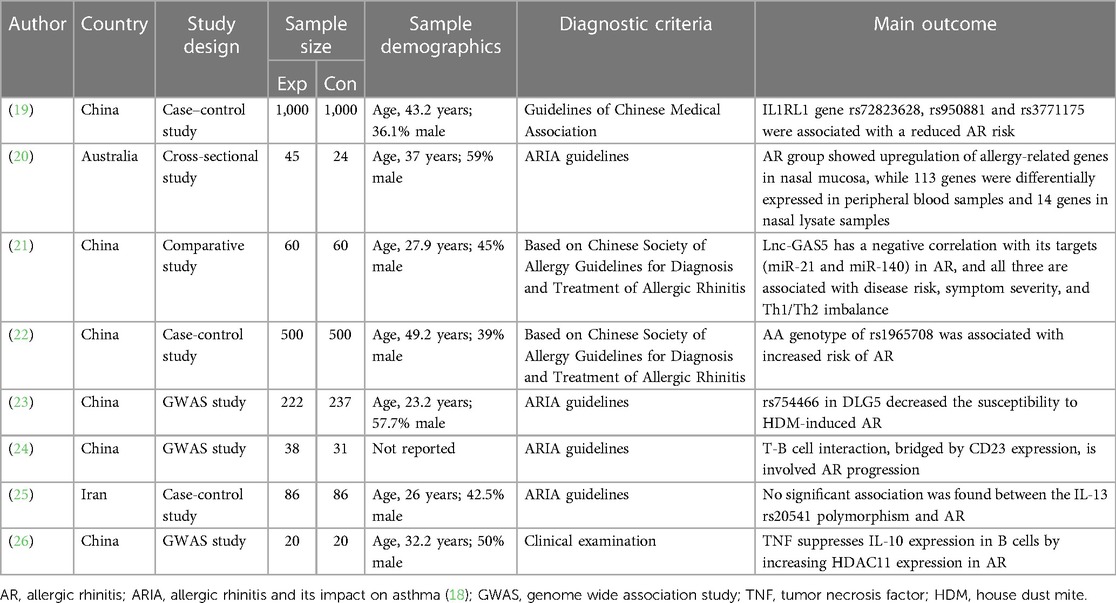
Table 2. Investigation of genetic factors in AR: characteristics of included studies.

Table 3. Investigation of Environmental factors in AR: characteristics of included studies.
Due to the heterogeneity in the outcomes of the selected studies, we divided the analysis into three subheadings to ensure a comprehensive evaluation as.
While various immune mediators have been reported to play a role in the pathogenesis of AR, it is not feasible to cover all of them in a single study. Though we mainly focused on essential mediators of cytokines, along with subtypes for our analysis. However, we also considered other relevant mediators in our study if considered important. We identified five studies from 2018 to 2023 that focused on these immune mediators in the pathogenesis of AR.
The outcomes of these five studies on the pathogenesis of AR indicate that patients with AR had higher serum levels of CCL3, RvE1, and LTB4, but a lower ratio of RvE1 and RvD1 to LTB4, IL-10, and TGF-β cytokines. Additionally, AR patients had more CD4+ T cells and higher levels of IL-10, IL-6, and IFN-γ, but lower levels of Th1 and Th17 subsets with chemokine receptors. There were no significant differences in IL-25 and IL-33 levels between fungal and non-fungal AR. Furthermore, IL-17, IL-22, and TGF-β levels were higher in patients with AR, while IFN-γ levels were lower compared to the control group (13–17). The outcomes of our selected studies regarding the role of immune mediators in pathogenesis of AR are presented in Table 1.
There were ten studies that focused on the genetic pathogenesis of AR. Due to the wide range of genetic and epigenetic factors studied, it was not possible to draw a single conclusion for any particular factor in the pathogenesis of AR. The research showed a link between the IL1RL1 gene markers rs72823628, rs950881, and rs3771175, and a lower likelihood of AR. In the AR group, genes connected to allergies were more active in nasal tissue, with 113 genes exhibiting differential expression in peripheral blood samples and 14 genes in nasal lysate samples. Long non-coding RNA GAS5 (lnc-GAS5) showed an inverse relationship with its targets (miR-21 and miR-140) in AR, all of which correlated with disease risk, symptom severity, and Th1/Th2 imbalance. The AA genotype of rs1965708 was associated with a heightened AR risk. The expression of CST1, TFF3, ITLN1, and rs754466 in DLG5 were linked to lower susceptibility to house dust mite-induced AR. T-B cell interaction, bridged by CD23 expression, was involved in AR progression. However, no significant association was found between the IL-13 rs20541 polymorphism and AR (19–26). The outcomes of our selected studies regarding the role of genetic factors in the pathogenesis of AR are presented in Table 2.
We identified only one study that examined the impact of environmental factors in relation to AR. This study assessed the mRNA expression levels of various tight junctions, including occludin (OCLN), claudin-3 and −7 (CLDN3 and CLDN7), desmoglein 3 (DSG3), and thymic stromal lymphopoietin (TSLP) in 30 individuals with Allergic Rhinitis (AR) and 30 non-allergic controls. The research found a significantly lower expression of OCLN, CLDN3, and CLDN7 transcripts in AR sufferers compared to the non-allergic control group. However, no noticeable variances were seen in the DSG3 or TSLP transcript expression between the two groups. The study also revealed an association between urban areas and decreased OCLN expression, and a correlation between second-hand smoke exposure and lower CLDN7 expression in AR patients. Ultimately, the conclusion was drawn that decreased expression of OCLN and CLDN7, connected to urban settings and second-hand smoke exposure, may be contributing to the impaired nasal epithelial barrier seen in AR patients, supporting recent studies positing air pollution as a possible cause of AR (28).
Chronic rhinitis, and AR in particular, is a major global health concern that affects approximately 400 million people worldwide. The prevalence of AR has been on the rise due to increased urbanization and exposure to environmental pollutants, which are believed to be among the leading causes of the disease. Developing effective therapies for chronic rhinitis requires a thorough understanding of its complex pathophysiology, including various contributing factors (1). Therefore, it is essential to review the complex pathogenesis of AR, considering multiple factors to identify potential drug targets for successful treatment.
Although literature reviews on AR are available, many of them are focused on either single pathology or based on a single pathogenic factor only (29, 30, 31). Our systematic review, on the other hand, takes a comprehensive approach to understand the pathogenesis of AR by considering multiple factors. This is one of the first reviews to adopt such a comprehensive approach. Our selected studies exhibit heterogeneity; therefore, a meta-analysis could not be performed. However, the broad overview of multiple factors in the pathogenesis of chronic rhinitis offers detailed information for researchers to understand its complex mechanism.
In our study, we have identified several cytokines that were reported in the included studies for their involvement in the pathogenesis of AR. The findings from the studies indicate that individuals with AR tend to have elevated levels of certain immune mediators such as CCL3, RvE1, LTB4, CD4+ T cells, IL-10, IL-6, IL-17, IL-22, and TGF-β, but reduced levels of the RvE1 and RvD1 ratio to LTB4, Th1 and Th17 subsets with chemokine receptors, and IFN-γ (13–17).
The role of Cytokines and Chemokines was described in various previous studies. AR is categorized as a type 2 inflammation mediated disease. The pathology of AR involves interleukins 4, 5, and 13, which play significant roles (32). The type 2 inflammatory response is provoked by both the innate immune system, which is activated by pollutants or viral or fungal infections and involves type 2 innate lymphoid cells (ILC2), and the adaptive immune system, which is stimulated by allergen exposure and involves type 2 T-helper (Th2) cells. Both ILC2 and Th2 cells release type-2 cytokines like interleukin IL-4, IL-5, and IL-13, playing diverse roles in the inflammatory cascade. IL-4 and IL-13 cause B-cell class switching and IgE production, provoke the discharge of pro-inflammatory substances, disrupt barriers, and encourage tissue remodeling. In addition, IL-13 prompts an increase in goblet cells leading to excess mucus production (33, 34).
Furthermore, there are indications that the pathophysiology of AR may encompass other pathways, specifically involving the regulation of Th2 cytokine responses by cytokines expressed in the epithelial cells. These cytokines include thymic stromal lymphopoietin, IL-25, and IL-33 (33). In addition to IL-4, IL-5, IL-13, IL-25, and IL-33, a range of other immune mediators contribute to the pathophysiology of AR. In the case of viral infections, elevated levels of various inflammatory cytokines, including IL-1β, IL-6, IL-7, IL-17, IFN-γ, IL-8, TNFα, and GM-CSF are observed, alongside IL-4 and IL-5. Similarly, during the allergy season, the levels of IL-4 and IL-10 decrease in nasal fluid. However, both cytokines demonstrate an increase in concentration 5 h after a nasal allergen challenge conducted outside the allergy season (35). We have also found a decrease in Th17 levels, which is in line with a previous review conducted by Fan et al., suggesting a negative correlation between Th17 and the occurrence of AR. The proposed mechanism is that regulatory B cells play a role in inhibiting the differentiation and proliferation of primary T cells into Th17 cells by facilitating the release of IL-10 and IL-35. As a result, this leads to a reduction in Th17 cells, a decrease in IL-17 secretion, and the alleviation of symptoms in individuals with AR (36).
Chemokine (C-C motif) ligand 3 (CCL3), also known as macrophage inflammatory protein 1-alpha (MIP-1-alpha), is a protein that in humans is encoded by the CCL3 gene and plays a role in inflammatory responses through binding to the receptors CCR1, CCR4 and CCR5 (37). CCL3 stimulates the movement of monocytes and T lymphocytes, although its impact varies among different T cell subsets. For instance, CCL3 primarily drives chemotaxis in B lymphocytes and activated CD8 T cells. This cytokine also prompts the chemotaxis of natural killer (NK) cells. Moreover, CCL3 acts as a chemoattractant for eosinophils and encourages basophils to discharge histamine. Additionally, CCL3 triggers the expression of ICAM-1, the degranulation of mast cells, and the production of tumor necrosis factor alpha (TNF-a), IL-1, and IL-6 (38). In their 2020 study, Berghi and colleagues discovered a notable elevation in the average serum CCL3 levels among patients suffering from Allergic Rhinitis (AR), compared to those in control groups. This finding can be associated with the significant function that CCL3 plays in sparking inflammation in cases of AR.
Endogenous lipid mediators known as Resolvins, specifically Resolvin E1 (RvE1) and Resolvin D1 (RvD1), are identified for their positive influence on resolving inflammation (39). RvE1 has the capability to bind to BLT-1, a receptor with a high affinity for leukotriene B4 (LTB4), which results in the suppression of LTB4-driven immune cell recruitment to inflamed areas. This binding action mitigates the LTB4-induced mobilization of immune cells to inflammation sites, indicating a competition between RvE1 and LTB4 for BLT-1 binding, with RvE1 functioning as a BLT-1 antagonist (40). In a 2020 study conducted by Lotfi and his team, they found that the lower ratios of RvE1 and RvD1 to LTB4 suggest an imbalance in the production of these mediators in AR patients. They suggested that the findings indicate a possibility that LTB4 might be dominating RvE1 in terms of BLT-1 binding, leading to impaired resolution of airway inflammation, and consequently contributing to the development of chronic airway inflammation. Overall, it appears that the increase in RvE1 is a critical action of the immune system to actively resolve allergic airway inflammation, though this effort remains insufficient. Notably, the study also found that serum levels of both IL-10 and TGF-β were significantly decreased in AR patients compared to healthy individuals, which is comparable to findings from a murine study conducted by Oner and associates in (41), where they demonstrated that RvE1 inhibited IL-10 synthesis by Th17 cells. Conversely, their study also revealed that RvE1 increased the production of TGF-β by dendritic cells.
Similar to the focus on cytokines, most of our studies also concentrated on examining the role of genetic factors, specifically in AR. The findings indicated an increase in the expression of allergy-related genes in the nasal mucosa, CD23 expression during T-B cell interaction, and TNF-induced HDAC11 expression. However, the IL1RL1 gene variants, namely rs72823628, rs950881, and rs3771175, were associated with a lower risk of developing AR (19–26). A review by Choi et al. reported multiple genetic and epigenetic factors, some of which were consistent with our findings (29). Lastly, regarding environmental factors, the selected study observed the effect of environmental factors in pathogenesis, and demonstrated an indirect relation between the expression of OCLN and CLDN7 to air pollution (27).
Our review has some limitations that should be addressed in future research. Firstly, the studies included in our review varied in terms of their objectives, methodology, and findings. Similarly, the studies focused on different sub-factors, making it difficult to compare their results. Therefore, future studies should focus on one aspect at a time to obtain more conclusive results. Furthermore, based on our findings, researchers should link these mechanisms to potential therapies for AR and mixed rhinitis.
Various factors, including immune mediators particularly cytokines, genetic, and environmental factors, are involved in the development of AR. However, the studies presented findings on different factors and sub-factors, making it challenging for us to compare their results. Therefore, future studies should focus on one aspect at a time to obtain more conclusive results. Additionally, researchers should connect these mechanisms to potential treatments for AR and mixed rhinitis based on our findings.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Nur Husna SM, Tan H-TT, Md Shukri N, Mohd Ashari NS, Wong KK. Allergic rhinitis: a clinical and pathophysiological overview. Front Med. (2022) 9:940. doi: 10.3389/fmed.2022.874114
2. Liva GA, Karatzanis AD, Prokopakis EP. Review of rhinitis: classification, types, pathophysiology. J Clin Med. (2021) 10:14. doi: 10.3390/jcm10143183
3. Reitsma S, Subramaniam S, Fokkens WWJ, Wang Y. Recent developments and highlights in rhinitis and allergen immunotherapy. Allergy. (2018) 73(12):2306–13. doi: 10.1111/all.13617
4. Wise SK, Lin SY, Toskala E, Orlandi RR, Akdis CA, Alt JA, et al. International consensus statement on allergy and rhinology: allergic rhinitis. Int Forum Allergy Rhinol. (2018) 8:108–352. doi: 10.1002/alr.22073
5. Lal D, Brar T, Ramkumar SP, Li J, Kato A, Zhang L. Genetics and epigenetics of chronic rhinosinusitis. J Allergy Clin Immunol. (2023) 151:848–68. doi: 10.1016/j.jaci.2023.01.004
6. Meng Y, Wang C, Zhang L. Recent developments and highlights in allergic rhinitis. Allergy. (2019) 74(12):2320–8. doi: 10.1111/all.14067
7. Liu G, Liu F. Bach2: a key regulator in Th2-related immune cells and Th2 immune response. J Immunol Res. (2022) 2022:14883. doi: 10.1155/2022/2814510
8. Chong SN, Chew FT. Epidemiology of allergic rhinitis and associated risk factors in Asia. World Allergy Organ J. (2018) 11(1):17. doi: 10.1186/s40413-018-0198-z
9. Savouré M, Bousquet J, Jaakkola JJK, Jaakkola MS, Jacquemin B, Nadif R. Worldwide prevalence of rhinitis in adults: a review of definitions and temporal evolution. Clin Transl Allergy. (2022) 12(3):e12130. doi: 10.1002/clt2.12130
10. Muñoz-Cano R, Ribó P, Araujo G, Giralt E, Sanchez-Lopez J, Valero A. Severity of allergic rhinitis impacts sleep and anxiety: results from a large Spanish cohort. Clin Transl Allergy. (2018) 8:23. doi: 10.1186/s13601-018-0212-0
12. Bousquet J, Bachert C, Canonica GW, Casale TB, Cruz AA, Lockey RJ, et al. Unmet needs in severe chronic upper airway disease (SCUAD). J Allergy Clin Immunol. (2009) 124(3):428–33. doi: 10.1016/j.jaci.2009.06.027
13. Berghi O, Dumitru M, Caragheorgheopol R, Tucureanu C, Simioniuc-Petrescu A, Sfrent-Cornateanu R, et al. The relationship between chemokine ligand 3 and allergic rhinitis. Cureus. (2020) 12(4):e7783. doi: 10.7759/cureus.7783
14. Lotfi R, Davoodi A, Mortazavi SH, Gorgin Karaji A, Tarokhian H, Rezaiemanesh A, et al. Imbalanced serum levels of resolvin E1 (RvE1) and leukotriene B4 (LTB4) in patients with allergic rhinitis. Mol Biol Rep. (2020) 47(10):7745–54. doi: 10.1007/s11033-020-05849-x
15. Yu X, Wang M, Cao Z. Reduced CD4(+)T cell CXCR3 expression in patients with allergic rhinitis. Front Immunol. (2020) 11:581180. doi: 10.3389/fimmu.2020.581180
16. Abbasi R, Zomorodian K, Zare Shahrabadi Z, Saadat F, Nabavizadeh SH, Esmaeilzadeh H, et al. IL-25 and IL-33 serum levels are not associated with the type of allergen causing allergic rhinitis. Iran J Immunol. (2019) 16(4):321–6. doi: 10.22034/iji.2019.80283
17. Bayrak Degirmenci P, Aksun S, Altin Z, Bilgir F, Arslan IB, Colak H, et al. Allergic rhinitis and its relationship with IL-10, IL-17, TGF-β, IFN-γ, IL 22, and IL-35. Dis Markers. (2018) 2018:9131432. doi: 10.1155/2018/9131432
18. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens W, Togias A, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008. Allergy. (2008) 63:8–160. doi: 10.1111/j.1398-9995.2007.01620.x
19. Li Z, Ren J, Zhang J, Wang X, Liu Y, Wang Q. Association between IL1RL1 gene polymorphisms and allergic rhinitis risk in the Chinese Han population. J Clin Lab Anal. (2022) 36(11):e24747. doi: 10.1002/jcla.24747
20. Watts AM, West NP, Smith PK, Cripps AW, Cox AJ. Adult allergic rhinitis sufferers have unique nasal mucosal and peripheral blood immune gene expression profiles: a case–control study. Immun Inflamm Dis. (2022) 10(1):78–92. doi: 10.1002/iid3.545
21. Song J, Wang T, Chen Y, Cen R. Long non-coding RNA growth arrest-specific 5 and its targets, microRNA-21 and microRNA-140, are potential biomarkers of allergic rhinitis. J Clin Lab Anal. (2021) 35(10):e23938. doi: 10.1002/jcla.23938
22. Yin X, Wang B, Yan Z, Hu L, Zhang X. Association between SP-A rs1965708 gene polymorphism and allergic rhinitis risk in Chinese population. J Clin Lab Anal. (2021) 35(7):e23828. doi: 10.1002/jcla.23828
23. Chen M, Zheng R, Li F, Xin JY, Chen SL, Zhu XJ, et al. Genetic variants in hippo pathway genes are associated with house dust mite-induced allergic rhinitis in a Chinese population. Clin Transl Allergy. (2021) 11(10):e12077. doi: 10.1002/clt2.12077
24. Yao Y, Wang N, Chen CL, Pan L, Wang ZC, Yunis J, et al. CD23 Expression on switched memory B cells bridges T-B cell interaction in allergic rhinitis. Allergy. (2020) 75(10):2599–612. doi: 10.1111/all.14288
25. Shirkani A, Mansouri A, Hosseini RF, Azad FJ, Mahmoudian RA, Montazer M, et al. The role of interleukin-4 and 13 gene polymorphisms in allergic rhinitis: a case control study. Rep Biochem Mol Biol. (2019) 8(2):111.31832433
26. Shao JB, Luo XQ, Wu YJ, Li MG, Hong JY, Mo LH, et al. Histone deacetylase 11 inhibits interleukin 10 in B cells of subjects with allergic rhinitis. Int Forum Allergy Rhinol. (2018) 8:1274–83. doi: 10.1002/alr.22171
27. Nur Husna SM, Siti Sarah CO, Tan HT, Md Shukri N, Mohd Ashari NS, Wong KK. Reduced occludin and claudin-7 expression is associated with urban locations and exposure to second-hand smoke in allergic rhinitis patients. Sci Rep. (2021) 11(1):1245. doi: 10.1038/s41598-020-79208-y
28. Nur Husna SM, Md Shukri N, Tuan Sharif SE, Tan HTT, Mohd Ashari NS, Wong KK. IL-4/IL-13 axis in allergic rhinitis: elevated serum cytokines levels and inverse association with tight junction molecules expression. Front Mol Biosci. (2022) 9:819772. doi: 10.3389/fmolb.2022.819772
29. Choi BY, Han M, Kwak JW, Kim TH. Genetics and epigenetics in allergic rhinitis. Genes. (2021) 12(12):2004. doi: 10.3390/genes12122004
30. Meng Y, Wang C, Zhang L. Diagnosis and treatment of non-allergic rhinitis: focus on immunologic mechanisms. Expert Rev Clin Immunol. (2021) 17(1):51–62. doi: 10.1080/1744666X.2020.1858804
31. Nur Husna SM, Tan H-TT, Md Shukri N, Mohd Ashari NS, Wong KK. Nasal epithelial barrier integrity and tight junctions disruption in allergic rhinitis: overview and pathogenic insights. Front Immunol. (2021) 12:663626. doi: 10.3389/fimmu.2021.663626
32. Scadding G. Cytokine profiles in allergic rhinitis. Curr Allergy Asthma Rep. (2014) 14:1–8. doi: 10.1007/s11882-014-0435-7
34. Maspero J, Adir Y, Al-Ahmad M, Celis-Preciado CA, Colodenco FD, Giavina-Bianchi P, et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Res. (2022) 8:3. doi: 10.1183/23120541.00576-2021
35. Baumann R, Rabaszowski M, Stenin I, Tilgner L, Scheckenbach K, Wiltfang J, et al. Comparison of the nasal release of IL-4, IL-10, IL-17, CCL13/MCP-4, and CCL26/eotaxin-3 in allergic rhinitis during season and after allergen challenge. Am J Rhinol Allergy. (2013) 27(4):266–72. doi: 10.2500/ajra.2013.27.3913
36. Fan K, Jin L, Yu S. Roles of regulatory B cells in the pathogenesis of allergic rhinitis. Allergol Immunopathol. (2022) 50(5):7–15. doi: 10.15586/aei.v50i5.615
37. Menten P, Wuyts A, Van Damme J. Macrophage inflammatory protein-1. Cytokine Growth Factor Rev. (2002) 13(6):455–81. doi: 10.1016/S1359-6101(02)00045-X
38. Cook DN. The role of MIP-1α in inflammation and hematopoiesis. J Leukoc Biol. (1996) 59:61–6. doi: 10.1002/jlb.59.1.61
39. Liu C, Fan D, Lei Q, Lu A, He X. Roles of resolvins in chronic inflammatory response. Int J Mol Sci. (2022) 23:14883. doi: 10.3390/ijms232314883
40. Im DS. Omega-3 fatty acids in anti-inflammation (pro-resolution) and GPCRs. Prog Lipid Res. (2012) 51(3):232–7. doi: 10.1016/j.plipres.2012.02.003
Keywords: allergic rhinitis, cytokines, pathogenesis, genetic factor, enviromental factors
Citation: Albloushi S and Al-Ahmad M (2023) Exploring the latest understanding on the role of immune mediators, genetic and environmental factors in pathogenesis of allergic rhinitis: a systematic review. Front. Allergy 4:1223427. doi: 10.3389/falgy.2023.1223427
Received: 16 May 2023; Accepted: 14 August 2023;
Published: 25 August 2023.
Edited by:
Glenis Kathleen Scadding, University College London, United KingdomReviewed by:
Lei Cheng, Nanjing Medical University, China© 2023 Albloushi and Al-Ahmad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mona Al-Ahmad bW9uYS5hbGFobWFkQGt1LmVkdS5rdw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.