
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Allergy, 05 May 2023
Sec. Food Allergy
Volume 4 - 2023 | https://doi.org/10.3389/falgy.2023.1101247
 Gregory D. Gooding1*
Gregory D. Gooding1* Jennifer L. Protudjer2,3,4,5,6
Jennifer L. Protudjer2,3,4,5,6 Sofianne Gabrielli1
Sofianne Gabrielli1 Pasquale Mulé1Greg Shand1Xun Zhang1
Pasquale Mulé1Greg Shand1Xun Zhang1 Christine McCusker1
Christine McCusker1 Francisco J. Noya1Maria Harvey1Mélodie Chalifour1Catherine Sicard4
Francisco J. Noya1Maria Harvey1Mélodie Chalifour1Catherine Sicard4 Elissa Abrams2,3Jacques-Alexandre Amiel7Thanh-Thao Ngo4Andre Bonnici4
Elissa Abrams2,3Jacques-Alexandre Amiel7Thanh-Thao Ngo4Andre Bonnici4 Noni MacDonald8Moshe Ben-Shoshan1
Noni MacDonald8Moshe Ben-Shoshan1  on behalf of the COVERS Group
on behalf of the COVERS Group
Background: We aimed to determine vaccine hesitancy and the main barriers associated with the 2019 novel coronavirus, SARS-CoV-2 (COVID-19) vaccination among families of children diagnosed with food/drug/environmental allergies.
Methods: Between May and June 2021, we approached 146 families seen at the outpatient allergy clinic at the Montreal Children's Hospital and a community allergy practice were invited to complete an anonymous online survey on COVID-19 and vaccination attitudes and behaviour. Uni and multivariable logistic regressions were compared to estimate factors associated with vaccine hesitancy.
Results: Among all patients, 24.1% reported vaccine hesitancy. The large majority of parents (95.2%) believed that vaccines work. The most common barrier to vaccination was fear of adverse side effects (57.0%). One-third of participants (31.5%) reported that a history of food, venom and drug allergy was a contraindication for COVID-19 vaccination. Fifty-nine (60.8%) participants stated that the dissemination of additional information would increase their willingness to be vaccinated. Most (96.9%) parents reported that their children's vaccinations were up to date. Hesitant families were more likely to be parents of children aged 6–10 years, be of Asian descent, report that mRNA vaccines are riskier than traditional vaccines, and report that the vaccine should not be given if the child has a history of allergic reaction to vaccines.
Conclusion: Vaccine hesitancy exists mainly among certain ethnic groups and families with young children. Allergies to food, venom and drug allergy are commonly perceived as contraindications for COVID-19 vaccination. Knowledge translation activities addressing parental concerns will help increase vaccination rates.
The implementation of COVID-19 vaccinations is suggested to play a crucial role in pandemic control. Yet, COVID-19 vaccination rates remain variable and suboptimal globally, ranging from <5% to 99% (1).
In children, vaccines may reduce the risk for developing severe disease manifestations, such as multisystem inflammation syndrome (MIS-C), high susceptibility to persistent COVID-19, and transmission of certain variants (2–4).
It is especially important to assess hesitancy among children with known food/drugs/aeroallergen allergies given that vaccination was listed as a contraindication for patients with food or drugs allergy and as a precaution in patients with aeroallergy according to recommendations by the Medicines and Healthcare Products Regulatory Agency (MHPRA) regulates medicines (5). We aimed to determine vaccine hesitancy and the main barriers associated with COVID-19 vaccination among families of children diagnosed with food, venom or drug allergies.
Parents of children at the allergy clinic at the Montreal Children's Hospital and a community allergy practice, in Montreal, Canada, were invited, in person, to complete a survey, available in either French or English, on COVID-19 and vaccination attitudes and behaviour. The questionnaire was developed by a multidisciplinary team composed of nurses, physicians, pharmacists and researchers. Parents were queried on age, sex of both parent and child, ethnicity, education level, history of vaccination of their child, parental willingness to vaccinate their child, and potential barriers for vaccination. The questionnaire was developed in English, then validated among 8 families and translated per World Health Organization guidelines for the translation of instruments, prior to distribution (6). Families provided informed consent and assent (in children at least 7 years old). Data were analysed with R (version 4.0.0). Descriptive statistics were used for reporting demographic factors (age, sex, ethnicity, education level). Uni - and multivariable logistic regressions were compared to estimate factors associated with vaccine hesitancy. Ethics approval for this study was granted by the McGill University Health Centre Research Ethics Board.
Between May and June 2021, 146 families were approached and all consented to participate in our anonymous survey (Supplementary Table 1). The largest group (26%) of children were 6–10 years old (range: 0–18 + years). The majority of parents (55.2%) were 40–49 years old (range: 20–60 + years) and had at least college education (83.6%). Among participants 110 (75.3%) indicated they would vaccinate their children for COVID-19 (95%CI: 67.9%, 82.4%). The large majority of parents 139 (95.2%) believed that vaccines work.
Among all patients, thirty-five (24.1%) reported vaccine hesitancy. Fifty-six parents (38.4%) reported hesitancy regarding vaccinating a child that had already been diagnosed with COVID-19 and over half (61.6%) had concerns regarding vaccination in pregnant women. Eighty-five (58.2%) reported hesitancy regarding vaccine safety for lactating women and/or their children. One-third of parents (34.9%) were hesitant about the safety of mRNA vaccines compared to other types of vaccines. Compared to non-hesitant families, vaccine-hesitant families were more likely to be parents of children aged 6–10 years (OR: 2.24, 95% CI: 1.04, 4.86), be of Asian descent (OR: 4.52, 95% CI: 1.56, 13.10), report that mRNA vaccines are riskier (OR: 2.43, 95% CI: 1.05, 5.61), and report a history of allergic reaction to vaccines as a contraindication (OR: 4.65, 95%CI: 1.51, 14.31) (Table 1).
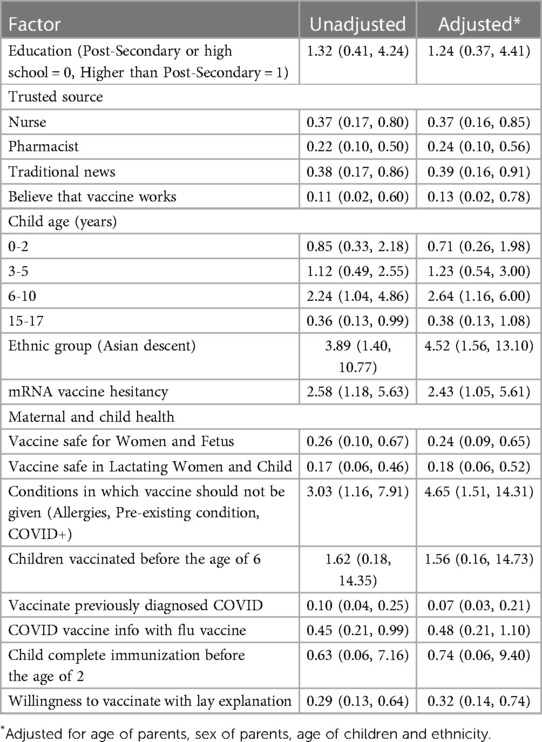
Table 1. Univariable and multivariable analyses (OR, 95%CI) of factors associated with vaccine hesitancy.
Fear of side effects was identified as the most common primary barrier to vaccination (57.0%). The majority of parents (60.3%) stated that receiving information regarding the safety of administration for the COVID-19 vaccine at the same time as other vaccines such as the seasonal influenza injection would increase their likelihood to get vaccinated.
To our knowledge, we conducted the first Canadian study to assess COVID-19 vaccine hesitancy among families. Our findings reveal that 24% of parents are hesitant regarding child vaccination. Parents of younger children and parents of Asian descent were more likely to be hesitant.
Our findings have particular importance given the ever-changing landscape of the pandemic. In October 2021 children aged 10–19 years accounted for almost 15% of all newly reported cases of COVID-19 (4). It is important to note that morbidity and mortality are reported to be particularly increased among adolescents with underlying illnesses—such as diabetes, cancer, HIV, and obesity (4). The majority of families of children with food, drug or, venom allergies reported that they would appreciate lay educational tools addressing their concerns, mainly the risk of side effects. Indeed, numerous studies suggest that some of the most effective interventions that succeed in reducing vaccination hesitancy are those that aim to increase vaccine knowledge (7).
Over half of our sample ranked fear of side effects as the most important barrier to vaccination despite the fact that data reveal that benefits associated with COVID-19 vaccination and booster shots largely outweigh the risks (8). Current literature states that mRNA vaccines are safe and effective for the vast majority of the population (8). Of note, at the time of our study, regulatory bodies were not yet investigating the safety of vaccines in children aged 0–5 years which could explain why parents of these age groups were hesitant. Of particular interest, one-third of participants indicated a history of food, drug, venom, or environmental allergy as contraindications to vaccination. In Canada, the National Advisory Council on Immunizations (NACI) and the Canadian Society of Allergy and Immunology (CSACI) has stated that the vaccine is contraindicated only in persons with a history of anaphylaxis to the COVID-19 vaccine or a vaccine excipient (9).
A limitation is that the small validation group and that families recruited at the allergy clinic are more likely to be concerned regarding side effects it is possible that we overestimated vaccine hesitancy. Interestingly, a study among French-speaking health care workers in France, parts of Belgium and Quebec revealed a similar percentage of vaccine hesitancy (10).
Vaccine hesitancy is not negligible; our data suggests that it exists mainly among certain ethnic groups and for young children. Despite current evidence, allergies to food, venom and drug allergy are often perceived contraindications for COVID-19 vaccination. Knowledge translation activities such as educational videos will increase vaccination rates among children and contribute to better control of the COVID-19 pandemic.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by McGill University Health Centre Research Institute. The patients/participants provided their written informed consent to participate in this study.
In accordance with the Annals’ Guide for Authors we confirm that the following authors meet 4 the requirements approved by the International Committee of Medical Journal Editors (ICMJE). All authors have done the following: (1) made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) drafted the article or reviewed it critically for important intellectual content; (3) given final approval of the version to be published; and (4) agrees to be accountable for all aspects of the work related to its accuracy or integrity. All authors contributed to the article and approved the submitted version.
This project was supported by the McGill Interdisciplinary Initiative in Infection and Immunity (MI4). The Grant is held and administered at The Research Institute of the McGill University Health Centre.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/falgy.2023.1101247/full#supplementary-material.
1. Mathieu E, Ritchie H, Ortiz-Ospina E, Roser M, Hasell J, Appel C, et al. Coronavirus pandemic (COVID-19). Our World in Data. (2020) 5(7):947–53.
2. Kabeerdoss J, Pilania RK, Karkhele R, Kumar TS, Danda D, Singh S. Severe COVID-19, multisystem inflammatory syndrome in children, and Kawasaki disease: immunological mechanisms, clinical manifestations and management. Rheumatol Int. (2021) 41(1):19–32. doi: 10.1007/s00296-020-04749-4
3. Ludvigsson JF. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. (2020) 109(6):1088–95. doi: 10.1111/apa.15270
4. Lima DGS, Figueiredo TMR, Pereira YTG, Almino MAFB, Pereira LM, de Menezes HL, et al. The effects of the silence on South African children and adolescents against a global alert on the newly identified coronavirus variant: omicron. J Pediatr Nurs. (2021) 65:e5–6. doi: 10.1016/j.pedn.2021.11.032
5. Ortega Rodríguez NR, Audícana Berasategui MT, de la Hoz Caballer B, Valero Santiago A. The century of mRNA vaccines: cOVID-19 vaccines and allergy. J Investig Allergol Clin Immunol. (2021) 31(1):89–91. doi: 10.18176/jiaci.0665
6. Process of translation and adaptation of instruments | World Health Organization. Available from: https://www.mhinnovation.net/sites/default/files/files/WHO%20Guidelines%20on%20Translation%20and%20Adaptation%20of%20Instruments.docx (cited January 19, 2022).
7. Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson HJ, Eskola J, et al. Strategies for addressing vaccine hesitancy—a systematic review. Vaccine. (2015) 33(34):4180–90. doi: 10.1016/j.vaccine.2015.04.040
8. Anand P, Stahel VP. Review the safety of COVID-19 mRNA vaccines: a review. Patient Saf Surg. (2021) 15(1):1–9. doi: 10.1186/s13037-020-00273-3
9. Archive 22: Recommendations on the use of COVID-19 vaccines (2021) - Canada.ca. Available from: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/recommendations-use-covid-19-vaccines.html (cited January 1, 2022).
Keywords: allergy, children, family, COVID-19, vaccine hesitancy, knowledge translation
Citation: Gooding GD, Protudjer JL, Gabrielli S, Mulé P, Shand G, Zhang X, McCusker C, Noya FJ, Harvey M, Chalifour M, Sicard C, Abrams E, Amiel J-A, Ngo T-T, Bonnici A, MacDonald N and Ben-Shoshan M (2023) COVID vaccine evaluation of barriers and resources among families of children with diagnosed allergies. Front. Allergy 4:1101247. doi: 10.3389/falgy.2023.1101247
Received: 17 November 2022; Accepted: 22 March 2023;
Published: 5 May 2023.
Edited by:
Lucien Harthoorn, Clasado Biosciences Ltd, JerseyReviewed by:
Amir Hamzah Abdul Latiff, Pantai Hospital Kuala Lumpur, Malaysia© 2023 Gooding, Protudjer, Gabrielli, Mulé, Shand, Zhang, McCusker, Noya, Harvey, Chalifour, Sicard, Abrams, Amiel, Ngo, Bonnici, MacDonald and Ben-Shoshan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gregory D. Gooding Z3JlZ29yeWRnb29kaW5nQGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Food Allergy, a section of the journal Frontiers in Allergy
Abbreviations: CSACI, Canadian Society of Allergy and Clinical Immunology; MHPRA, Medicines and Healthcare Products Regulatory Agency; MIS-C, multisystem inflammation syndrome; NACI, National Advisory Council on Immunizations; OR, odds ratio; 95%CI, 95% confidence intervals.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.