 Lubnaa Hossenbaccus
Lubnaa Hossenbaccus Sophia Linton
Sophia Linton Rashi Ramchandani
Rashi Ramchandani Alyssa G. Burrows
Alyssa G. Burrows Anne K. Ellis
Anne K. Ellis
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Allergy , 17 March 2022
Sec. Rhinology
Volume 3 - 2022 | https://doi.org/10.3389/falgy.2022.828091
This article is part of the Research Topic Insights in Rhinology: 2021/22 View all 9 articles
The prevalence of cat allergen-induced AR is increasing worldwide, prompting its study using controlled methodology. Three general categories of allergen exposure models currently exist for the study of cat allergen-induced AR: natural exposure cat rooms, allergen exposure chambers (AEC), and nasal allergen challenges (NAC). We evaluated existing literature surrounding the use of these models to study cat allergen induced AR using online research databases, including OVID Medline, Embase, and Web of Science. We report that natural exposure cat rooms have been important in establishing the foundation for our understanding of cat allergen-induced AR. Major limitations, including variable allergen ranges and differing study designs highlight the need for a more standardized protocol. In comparison, AECs are an exceptional model to mimic real-world allergen exposure and study long-term implications of AR with large sample sizes. Existing AECs are limited by heterogeneous facility designs, differing methods of cat allergen distribution, and issues surrounding cost and accessibility. Conversely, NACs allow for smaller participant cohorts for easier biological sampling and are ideal for phase I, phase 2 or proof-of-concept studies. NACs generally have a standardized protocol and are less expensive compared to AECs. Nevertheless, NACs solely capture acute allergen exposure and have the further limitation of using allergen extracts rather than natural allergen. As the use of combined controlled methodologies is sparse, we recommend concurrent use of AECs and NACs to study short- and long-term effects of AR, thereby providing a more holistic representation of cat allergen-induced AR.
Pet dander is a major source of indoor allergen and a common cause of perennial allergic rhinitis (AR). The prevalence of cat allergen-induced AR specifically, caused by domestic cats (Felis domesticus), is increasing worldwide (1–5). There are 10 unique allergens that have been identified originating from cats found in the saliva, pelt, or urine, with Fel d 1 being the primary culprit of AR (6–8). In sensitized patients, exposure to cat allergens trigger an immunoglobulin E (IgE)-mediated inflammatory response in the nose, resulting in the characteristic symptoms of AR including sneezing, itchy nose, nasal pruritus, and congestion.
In the study of AR, controlled methodologies aim to regulate exposure of the target allergen while minimizing the effect of extraneous variables (Figure 1). Historically, natural exposures were conducted, where participants were placed in an environment where they were exposed to the allergen of interest for a certain period. For cat allergen-induced AR, cat rooms were used extensively. While allowing for natural exposure, such models involve a wide range of allergen concentrations, sometimes resulting in higher levels than are normally observed in a home setting (9, 10). In contrast, allergen exposure chambers (AEC) mimic natural exposure while controlling all environmental variables, allowing for more precise and controlled distribution of allergen. They are specialized facilities, requiring trained staff, and are limited in number (11). AECs are ideal for representing longer-lasting exposures to allergen, whereas the nasal allergen challenge (NAC) is an acute and localized model (12). NAC protocols may vary, though it offers the opportunity to provide personalized doses of allergen intranasally to participants and extensive biological sampling (13). AEC and NAC models are useful for investigating disease pathophysiology and for the evaluation of AR therapies.
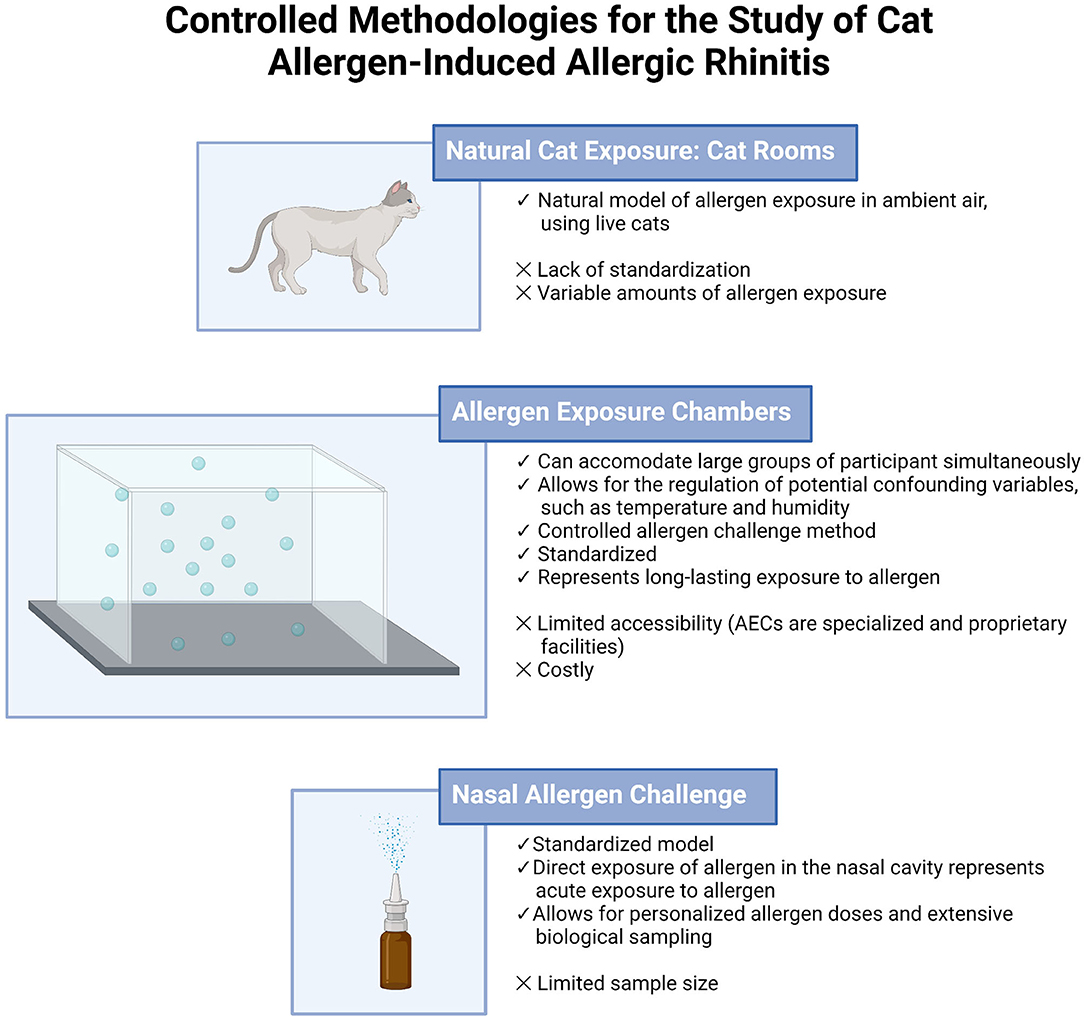
Figure 1. Comparison of models used in the investigation of cat allergy.
In this review, we performed a literature search using online databases, including OVID Medline, Embase and Web of Science and have summarized the current state of the literature on studying cat allergen-induced AR using controlled clinical methodologies.
Cat rooms draw upon the natural mode of allergen exposure in ambient air (14). Generally, they are small, constructed rooms containing one to two neutered cats who live in the space for several days; sometimes a litter box is also kept in the room. Depending on the study design, the cats are either kept in their cages or are free to roam around when participants are in the room (15–21). Most studies include the vigorous shaking of a blanket at a certain time interval to disturb the allergen (15–18, 20–22). In a study by Berkowitz et al., their cat exposure room shared the same ventilation supply as a cat shelter containing 80 cats. To aerosolize the cat allergen, they vigorously shook the cats' bedding before participant entry and at 15-min intervals (22). Generally, Fel d 1 concentrations in cat rooms are measured using enzyme linked immunosorbent assays (ELISA) (Table 1). The natural cat exposure experimental model has been used to evaluate the pathophysiology of cat allergen-induced AR, pharmacotherapies, and sublingual (SLIT) and subcutaneous (SCIT) allergen-specific immunotherapy (AIT) options for patients.
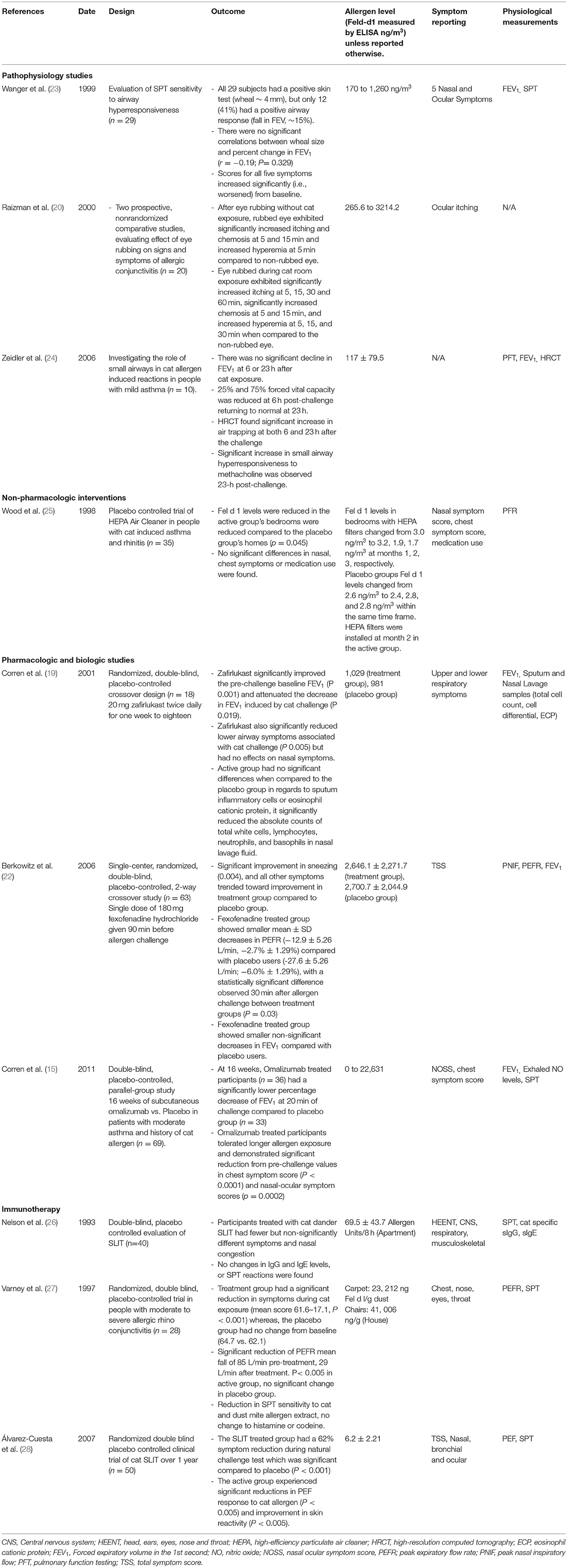
Table 1. Summary of cat room studies.
A handful of studies using cat rooms have investigated the physiological impact of cat allergen exposure in sensitized participants. Wagner et al. evaluated the correlation between skin testing reactivity and fall in forced expiratory volume in one second (FEV1) in cat sensitized individuals (23). They reported no significant correlations between the wheal size and percent change in FEV1 (r = −0.19; P = 0.329). All five symptom scores recorded (itchy/watery eyes, rhinorrhea, cough, nasal congestion) were worse compared to baseline after cat exposure (P < 0.001; P = 0.003). Zeilder et al. investigated the involvement of the small airways (<2 μm in diameter) in the late allergic asthmatic response induced by natural exposure to inhaled cat allergen (24). They reported that 20% of Fel d 1 particles were <6 μm while 7% were <3.2 μm. At 6 h following challenge, there was a borderline significant decline of FEV1 and a significant decline of forced expiratory flow from 25 to 75% of forced vital capacity at 6 h, which was undetectable at 23 h. High-resolution computed tomography found a significant increase in air trapping at both 6 and 23 h after the challenge. Additionally, a significant increase in small airway hyperresponsiveness to methacholine was observed 23-h post-challenge. These results demonstrate worsening of small airway obstruction at 6- and 23-h post-cat exposure.
Ocular symptoms have also been evaluated in participants with allergic conjunctivitis before, during, and after cat exposure (20). Eye rubbing during cat room exposure resulted in significantly increased itching, chemosis, and hyperemia compared to the non-rubbed eye. Prolonged redness and itchiness were also observed during cat exposure compared to eye rubbing without cat exposure. This study demonstrated that eye rubbing may play a role in ocular signs and symptoms in cat allergen allergic conjunctivitis and encouraging patients to stop rubbing their eyes may improve their clinical course.
The primary approach to AR management, following allergen avoidance, is pharmacotherapy, characterized by antihistamines, corticosteroids, leukotriene receptor antagonists, and combination therapies. In this section, we explore pharmacotherapies and biological agents for AR evaluated using cat rooms.
Berkowitz et al. evaluated fexofenadine hydrochloride, an H1 antagonist, in a single-center, randomized, double-blind, placebo-controlled, 2-way crossover study (n = 63) using ventilated air from a cat shelter housing 80 cats (22). Participants were given a 180 mg dose of fexofenadine hydrochloride and after 90 min, were exposed to cat allergen in the cat room. At 30 min post-challenge, the treatment group also had a significantly less (P = 0.03) mean (± SD) decreases in peak expiratory flow rate (PEFR) (−12.9 ± 5.26 L/min, −2.7% ± 1.29%) compared to placebo (−27.6 ± 5.26 L/min; −6.0% ± 1.29%). At 60 min post-onset of cat allergen exposure, participants in the treatment group had significant improvements in sneezing (p = 0.004) and all other symptoms trended toward improvement compared to the placebo group. Only the placebo group experienced a significant mean (± SD) decrease in FEV1 of −0.041 ± 0.015 L/s (P = 0.007) compared with their pre-challenge baseline values, suggesting a protective effect for antihistamine, fexofenadine.
In a randomized, double-blind, placebo-controlled, cross-over study, zafirlukast, an oral leukotriene receptor antagonist, was evaluated (19). Participants (n = 18) were given 20 mg zafirlukast twice daily for one week before an allergen challenge. After cat exposure, participants who had received zafirlukast had significantly attenuated decrease in FEV1 compared with placebo (−15.1 ± 2.7 vs. −25.1 ± 2.7, P = 0.019). Symptom scores decreased by 38% in the treatment group compared to the placebo; both wheezing (P = 0.004) and chest tightness (P = 0.0019) were significantly reduced, although it is worthwhile to recognize that a validated AR symptom scoring system was not used. Nasal lavage fluid revealed significantly fewer total cells and absolute counts of lymphocytes, neutrophils, monocytes, and basophils but no significant differences in the absolute or percentage values of eosinophils or eosinophil cationic proteins (ECP). Overall, this study demonstrated the effectiveness of zafirlukast at reducing acute pulmonary responses to cat exposure, though a longer duration of treatment may be needed to evaluate biological changes.
A newer treatment approach for AR involves omalizumab, an anti-IgE monoclonal antibody that is widely used to treat allergic asthma through the inhibition of IgE binding to the FcER1 receptor on mast cells and basophils. In a natural cat exposure study, omalizumab was administered at a dose of 0.008 mg/kg/IgE [IU/mL] every 2 weeks or 0.016 mg/kg/IgE [IU/mL] every 4 weeks (based on body weight and baseline serum total IgE levels) for 16 weeks (15). Some participants had cats in their homes whereas others did not and were randomized accordingly. Omalizumab-treated participants had a 44% improvement in the area under the curve (AUC) of the percentage decrease from pre-challenge FEV1 during a 60-min cat chamber exposure compared to the placebo-treated patients (15.2% per hour vs. 27.3% per hour, P = 0.0009). At 16 weeks, significant reductions in chest symptom scores (P < 0.0001), nasal ocular symptom scores (NOSS) (P = 0.0002), and skin prick reactivity (P < 0.0001) were observed in the treatment group. Omalizumab-treated participants tolerated a median of 50 min in the cat room whereas the placebo group tolerated a median of 22 min (p = 0.0006). Across the three sites that this study was conducted, the Fel d 1 allergen varied greatly, specifically site 3 (Mississauga, ON), which had large variations and higher concentrations when compared to sites 1 and 2 and between their placebo (178 to 6,445 ng/m3) and treatment group (19 to 4,744 ng/m3). Omalizumab was shown to significantly reduce symptom scores and improve FEV1 upon allergen exposure after 16 weeks of treatment however, results should be interpreted cautiously given the inconsistencies in allergen exposure.
SLIT and SCIT options for cat allergen-induced AR have been evaluated using the cat room model, with Fel d 1 being commonly used in the AIT protocols.
A SCIT regimen of 100 units every two weeks to a maintenance dose of 100,000 units (15 μg of Fel d 1) given every four weeks was evaluated in a double-blind placebo-controlled trial in 28 patients by Varney et al. The exact duration of treatment is unclear. All participants were brought to a house where three cats had lived for over 8 years and Fel d 1 concentrations were measured from carpets and chairs (Table 1). The SCIT treatment group had a significant reduction in symptoms during cat exposure (P < 0.001) whereas, the placebo group had no change when compared to baseline. A significant reduction in decreased PEFR (P < 0.005) was found only in the active group, with a reduction in SPT sensitivity to cat extract. Together these results suggest that cat-specific SCIT therapy successfully reduced symptoms, PEFR, and SPT reactivity as evaluated in a natural exposure model (27).
Nelson et al. conducted a 105-day double-blind, placebo-controlled evaluation of SLIT therapy to 4,500,000 allergy units of cat extract in 40 patients with AR with and without asthma after cat exposure (26). At the end of the course of treatment, participants were brought to an apartment that had cat dander for a 90-min exposure. Following exposure, participants treated with cat dander SLIT had fewer but non-significantly different symptoms and nasal congestion. Additionally, no changes in IgG and IgE levels or skin prick testing reactions were observed. This study was critiqued by Bousquet et al. in a letter to the editor, specifically that the SLIT treatment duration was likely not long enough to make a definitive conclusion about the treatment efficacy (29).
Following this, Alvarez-Cuesta et al., conducted a double-blind, placebo-controlled study to evaluate the effectiveness of SLIT on 50 patients over one year. During the SLIT build-up phase, the accumulated dose was 1.7 μg of Fel d 1. The total accumulated dose during the entire length of the study was 17.1 μg of Fel d 1, patients were instructed to keep the SLIT mixture under their tongue for 2 min prior to swallowing. Patients were advised to avoid cat exposure. After one year of treatment, the SLIT treated group had a 62% symptom reduction during natural challenge test (i.e. cat room), which was significant compared to placebo (P < 0.001). The active group also experienced significant reductions in PEF response to cat allergen (P < 0.005) and improvement in skin reactivity (P < 0.005) (28).
A non-pharmacological high-efficiency particulate air (HEPA) filter intervention was investigated using a natural exposure model in 35 cat-sensitized people with asthma and rhinitis who owned one or more cats (25). Fel d 1 concentrations were measured in participant's bedrooms at baseline, 1, 2, and 3 months. Participants were randomized and blinded to either receive an active HEPA filters or a non-active filter. Although a significant reduction in Fel d 1 concentrations in bedrooms was found between the active and non-active groups at months 2 and 3 (p = 0.045), the reduction in allergen levels in the bedroom was insufficient at decreasing medication use, and chest and nasal symptom scores. HEPA filters may be valuable in reducing allergen levels, however allergen levels outside the bedroom likely impact patients' disease response.
Exposure to cat allergen through cat rooms was sufficient to induce AR symptoms in cat-sensitized individuals with and without asthma and those with rhinoconjunctivitis. This model adequately assessed the benefits of pharmacological therapies, immunotherapies, and physiological changes due to cat exposure. However, the lack of standardization in the design and execution of cat rooms is of concern. Cat rooms have varying amounts of allergen exposure between room designs and the range of allergen within the same room throughout the experiment is variable. In the cat room studies, various symptom questionnaires and biological measurements were employed, making it difficult to compare results between studies (Table 1). While natural cat allergen exposure room having produced useful insights on cat allergen-induced AR, there is a need to standardize the design and execution of cat allergen exposure with a more robust clinical model.
AECs are controlled clinical models of AR that allow for a large participant population to be simultaneously exposed to a specified allergen concentration, with the regulation of all variables including, but not limited to, temperature and humidity (30). Keeping the current COVID-19 pandemic in mind, modifications to the protocol can be implemented to ensure safety of all participants and staff involved, such as ensuring all participants are double vaccinated, a negative PCR test result from 48 to 72 h prior to the study visit, negative rapid antigen testing upon arrival at the study site, and masking until the allergen challenge starts. While controlled, AECs in many ways simulate real-world exposure to cat allergen, especially as the allergen is usually aerosolized and moves in particle clusters with a diameter of <5 microns (8). A comparative study by Haya et al. found that in naturalistic environments, blanket shaking produced larger dander particles (2–40 μm), while expulsions from vacuum cleaners produced smaller sized particles (1–20 μm) (31). In AECs, the spread of allergen is enhanced by the presence of fans; this model provides an unique method of simulating real-world cat allergen exposure (32, 33).
AECs have been used to study participants' biological responses to cat allergen-induced AR. Sicherer et al. found that exposure to cat allergen through an AEC reduced participants FEV1, which is reflective of typical allergen bronchoprovocation (34). Interestingly, the bronchoprovocation responses observed in the AEC were used to identify patients with asthma, suggesting its usefulness in studying a spectrum of allergic manifestations associated with cat allergens. A validation study by Marcelo et al. found that levels of cat dander on the walls and floors of an exposure chamber were comparable to levels seen in residences (21). This highlights the usefulness of AECs, in that the levels of cat allergen in the controlled facility are shown to be akin to real-world exposures.
AECs have also been used to evaluate AR therapies, specifically AIT peptides. Patel et al. used an environmental exposure chamber in a double- blind placebo design to measure the efficacy and safety of Fel d 1-derived peptide antigen desensitization (Cat-PAD) 1-year after the start of treatment. Nasal and ocular symptoms were effectively measured to ultimately provide evidence for the novel treatment (35). Similar outcomes were observed in a study by Couroux et al. where anti-synthetic peptide immuno-regulatory epitopes were tested. The AECs employed in each of the studies provided an effective method to measure a variety biological symptom data for AR, rhinoconjunctivitis and asthma manifestations (36). Furthermore, Hafner et al. tested CAT-PAD 4-weeks apart measuring participants TNSS score in 30-min intervals. Relative to the placebo, CAT-PAD decreased participants TNSS during the treatment period and two-years post-treatment (37). Notably, cat allergen peptide immunotherapy studies using AECs were also able to deduce the mechanisms associated with immunotherapy. For instance, a study by Worm et al. found that Fel d 1 can overlap with several MHC binding regions. This sheds light on binding affinity of developed Fel d 1 peptides and subsequently assisted in determining appropriate dosing for allergen immunotherapy (38). Mechanism-related data in a non-AEC study using T cell peptides for Fel d 1 by Oldfield et al. revealed that specifically post-immunotherapy, cat allergen sensitized participants exhibited decreased levels of pro-inflammatory interleukin levels, notably interleukin (IL)-4 and IL-13 relative to the placebo (39). The AEC model allows for a vast array of investigations in a regulated experimental setting.
The outcomes of AEC studies have not been directly compared to cat rooms. They similarly involve aerosolizing cat allergen to be spread across a large space, however in cat rooms, the allergen is directly from the animal source, whereas in AECs, the cat allergen is generally purified. While AECs are more controlled, much validation work is required to ensure effective allergen distribution and the maintenance of consistent protocols across various AECs. As they are specialized and proprietary facilities, AECs are limited in number worldwide and are costly. This highlights the need for a more accessible and cost-effective model in the study of cat allergies.
NAC and their various protocols have been extensively studied in the context of seasonal allergens and house dust mite, though there is limited data in the literature concerning the effects of cat allergen exposure. Recently, a couple of robust NAC studies have been published which detail biological outcomes after a cat allergen NAC.
Scadding et al. used a previously validated grass pollen NAC protocol to study the effects of cat allergen NAC and saw local and systemic Th2-driven inflammatory responses among their participants (40). Cat allergen dilutions were administered in a titrated fashion ranging 500 to 10,000 bioequivalent allergen unit (BAU)/ml, until the participants reached a TNSS score of 8. Each participant received one 100 μl spray to each nostril at 10-min intervals. Post-NAC, they saw a dose-response in symptoms and elevated levels of nasal fluid tryptase at 5 min after challenge. Levels of eotaxin, IL-4,−5,−9, and−13 were also increased at 8 h. Surface expression of CD63 and CD107a was evaluated to measure peripheral basophil activation and were found to be greater at 6 h than at baseline, both in the presence and absence of in vitro allergen stimulation.
The standardized NAC protocol developed by the Allergic Rhinitis–Clinical Investigator Collaborative project (AR-CIC), part of the Allergy, Genes and the Environment Networks for Centres of Excellence resembles the protocol developed by Scadding et al. The AR-CIC protocol differs slightly in that a titration challenge (doses ranging from 4.9 to 5,000 BAU/ml) is performed one week before administration of a single-dose NAC (41). The allergen dose administered was either a cumulative dose (from the lowest to the qualifying concentration dose) or a qualifying concentration dose (100 μl of the qualifying concentration). Both cohorts saw neutrophils, increased at 1 and 2 h after NAC; eosinophils, decreased at 1 and 2 h after NAC; lymphocytes, increased at 6 h after NAC; and the neutrophil/lymphocyte ratio, increased at 1 and 2 h after NAC. This group also identified seven clusters of immune gene expression patterns after NAC and some clusters were associated with clinical symptoms or immune cell frequencies. These findings suggest there may be systemic immune response signatures in whole peripheral blood post-NAC.
Doherty et al. studied Type 2 innate lymphoid cells (ILC2s) using the NAC model with cat allergen (42). A titrated-NAC was conducted using increasing concentrations of cat allergen extract (4, 40, 400 BAU/ml) administered 10-min apart. Post-NAC, they saw an increased percentage of peripheral blood ILC2s that express the chemoattractant receptor homologous molecule expressed on Th2 lymphocytes (CRTH2). However, the role of increased peripheral blood ILC2s after NAC remains unclear.
Paterniti et al. compared the magnitude of cat allergen-induced basophil histamine release (BHR) to NAC and other biological outcomes (43). They also administered a titration challenge at 10-min intervals with doses of 10, 100, and 1,000 BAU/ml in participants with cat allergy. A positive NAC was defined as 5 total sneezes. They saw that a positive cat allergen-induced BHR is associated with higher cat-specific IgE levels, a higher cat-specific to total IgE ratio and is predictive of a positive cat-induced NAC. Sánchez et al. recently evaluated levels of IgE sensitization and symptom production in atopic and non-atopic participants using NACs with pet allergen extracts (44). They reported that significantly more allergic participants were sensitized to one or more cat allergen components compared to the control group (p = 0.05), with Fel d 1-specific IgE concentrations, in particular, being higher. IgE sensitization was not associated with a positive NAC outcome, however, those with higher IgE concentrations had increased probability of a positive challenge. These findings reinforce the need for better tools to effectively predict clinical outcomes to pet allergens.
Lastly, the NAC model has been used to compare the clinical presentation of cat allergen-induced AR with other allergens. In 2017, Steacy et al. compared the symptoms produced by ragweed and cat-NACs using the AR-CIC methodology (45). They saw that cat-allergic participants required a significantly higher dose to achieve the qualifying criteria of TNSS ≥ 8 and a %PNIF fall ≥60% during screening compared to ragweed-allergic participants. Both groups of allergic participants had the same peak TNSS post-challenge, however, the peak %PNIF fall was achieved at 15 min for cat-allergic participants and 30-min post-challenge. An important caveat to this study was that cat-allergic participants were required to live with a cat to participate in this study and ragweed-allergic participants were challenged out of season. This study suggests clinical differences in the presentation of AR against seasonal and perennial allergens, which may be useful to inform treatment practices.
The biological outcomes of an NAC with cat allergen, described above, can be used as surrogate outcome measures in clinical trials. In the past 10 years, several trials investigating new pharmacotherapies and immunotherapy options for cat-allergy have been performed using the NAC as a model for cat-allergen exposure. These data build on previous research using NACs to evaluate onset of action and duration of efficacy for many therapeutics. Previously, Ewbank et al. performed a double-blind, placebo-controlled immunotherapy dose-response study with standardized cat extract and used a titrated NAC with cat hair extract to evaluate biological responses to treatment (46). A similar study by Nanda et al. assessed the long-term immunological response to reaching maintenance in immunotherapy (47). They also used a titrated NAC with cat hair and dander extract and saw the symptoms, nasal cytokines, and serum TGF-β levels at 5 weeks is predictive of the response at 1 year. These studies demonstrate the use of NAC in cat immunotherapy trials.
The effect of omalizumab on basophil and mast cell responses were evaluated using a cat NAC. This double-blind, placebo-controlled trial involved a baseline, mid-study, and final NAC with blood sampling to measure basophil histamine release (BHR) and basophil IgE/FcεRI measurements. The dosage of omalizumab was 0.016 mg/kg/IgE every 4 weeks. Eckman et al. saw a significant mean reduction in BHR and in mean combined nasal symptom scores by mid-study NAC (~4 weeks) compared to baseline suggesting basophils may play a role in the acute NAC response (48).
The use of Cat-PAD, a new form of immunotherapy for cat allergy, has been investigated using a cat NAC. In 2018, Neighbour et al. aimed to outline biomarkers of efficacy for Cat-PAF using AR-CIC NAC methodology (49). Participants underwent a baseline titrated NAC, followed by four intradermal injections of 6 nmol of Cat-PAD every 4-weeks and a final NAC. They saw a significant reduction in TNSS and PNIF after treatment. In 2020, Kim et al. used the same methodology to measure the clinical response to Cat-PAD at the same dosing (50). Post-NAC blood differential cell counts, transcriptomic profiles, and symptoms were compared before and after treatment. Total nasal symptom score (TNSS) post-NAC was significantly reduced after treatment as well as frequencies of neutrophils, lymphocytes, and monocytes. There was also a significant neutrophil to lymphocyte ratio (NLR) reduction at baseline, and 1 and 2 h-post NAC, after Cat-PAD treatment. IL-1β had a significantly lower RNA expression after treatment and IFN-y had significantly higher RNA levels post-NAC after treatment. This group also saw changes in clustered gene expression patterns after treatment: integrin subunit alpha E (ITGAE, CD103), CD180 (LY64), neural cell adhesion molecule 1 (NCAM1, CD56), C-C motif chemokine receptor 7 (CCR7, CD197), and leucine-rich repeat neuronal 3. These findings suggest that peripheral blood biomarkers could serve as predictors of treatment efficacy.
Recently, a phase 1b, randomized, double-blind, placebo-controlled proof-of-mechanism study was conducted to evaluate the therapeutic potential of monoclonal IgG antibodies (REGN1908-1909), administered subcutaneously, for cat allergy. Orengo et al. used an NAC with cat hair extract to measure the TNSS AUC from pre-treatment challenge to day 8 challenge (51). They saw TNSS AUC from baseline to day 8 NAC significantly decrease in patients receiving a single dose of REGN1908-1909 (600 mg) compared to placebo. They also saw a clinically meaningful reduction in TNSS AUC up to 85 days after the first dose. Finally, REGN1908-1909 was well-tolerated by participants (52). Another group, Shamji et al., also performed at phase 1b study of REGN1908-1909 using an NAC with cat hair extract followed by extensive biological sampling. NAC was conducted on Study Days 8, 29, 57, and 85 using a titration protocol. Following treatment, significantly decreased levels of IL-4, IL-5, IL-13, TARC, and RANTES were observed in nasal fluid samples post-NAC (Day 8). Likewise, they saw inhibitory activity in the treatment group, measured as cat allergen-IgE complexes bound to B cells. Together, these data demonstrate proof of principle that a single dose of REGN1908-1909 can reduce symptoms in patients with cat allergy.
As cat rooms are not validated and standardized, they are challenging to compare between studies and with AEC and NAC studies. To our knowledge, the first comparison of cat allergen NACs and a cat exposure room was in 1997 by Sicherer et al. (34). They conducted an NAC using filter paper disks containing up to 50 μl of allergen at the following concentrations: 50, 500, and 5000 BAU/ml until a FEV1 fall of 20% was reached. Participants also sat for 1-h in a cat-exposure room for an environmental allergen challenge (EAC), which contained 2 female cats, where Fel d 1 levels ranged from 289 to 9,349 ng/m3 per session. The challenges were separated at least 1 week. They saw that nasal symptom scores during the EAC were correlated with those post-NAC. However, this study is limited by a small sample size (n = 13) and the large variation in Fel d 1 exposure levels in the EAC sessions.
The clinical and biological comparability of the NAC and AEC has also not been investigated thoroughly, especially with cat allergens. In 2019, Tenn et al. compared clinical outcomes from EEU and NAC studies using ragweed and reported the induction of symptoms of similar severity between the models, though with differing temporal patterns (53). More recently, in 2020, Larson et al. conducted a randomized trial comparing the NAC and environmental exposure chamber (EEC) (54). Participants received either an NAC followed by a 2-day challenge in an EEC (Group A) or a 2-day challenge in an EEC followed by NAC (Group B). A washout period of 28-days separated each challenge type. In the NAC, a single dose of 0.87 μg total Fel d1 was administered whereas the EEC phase lasted 3 h with an exposure of 10 to 500 ng/m3 Fel d 1 allergen. They saw that symptoms with NAC peaked earlier (15-min and 30-min) than EEC (>1 h) and had overall reduced magnitude of response. They also observed strong NAC and EEC correlations when the allergen exposure-induced changes in IL-5 and IL-13 when expressed as 2- to 8-h AUCs. Similarly, differentially expressed genes showed a similar magnitude of change with each challenge and the changes were highly correlated. Together, these data suggest that clinical outcomes of the NAC and EEC are temporally different but induce similar immunologic responses. However, this study is limited by sample size, the lack of a non-allergic control group, and that the total dose administered in the two challenges differed significantly.
AECs and NACs represent the future of research on cat allergen-induced AR as standardized and reproducible controlled methodologies. AECs generally model allergen exposure over the course of hours whereas NACs, through a sudden burst of allergen extract into the nose, are more representative of acute exposure. In everyday life, cat allergen exposure can variably be short-term, such as on public transportation, or long-term, as in one's home environment if a cat is kept as a pet (55). Both circumstances may cause the triggering of AR symptoms in sensitized individuals, hence, for the complete understanding of cat allergen-induced AR, both modes of exposure need to be considered. As explored in the previous section, only a few studies evaluate the two through the AEC and NAC, however with certain limitations, so there exists the need for better comparisons between the models to improve our understanding of the pathophysiology of cat allergen-induced AR, with larger sample sizes and standardized protocols.
In this review, we discuss three models to study cat allergies including natural exposure cat rooms, AECs, and NACs. In comparison to cat rooms, the use of AECs and NACs to investigate cat allergen-induced AR are limited. While these models have been extensively used in pharmacological studies of AR, there is a paucity of data investigating the biological outcomes of cat allergies using an AEC or NAC. Existing studies are limited by their small sample size, lack of controls, non-standardized protocol, and specified dosing methodology. Given the rising incidence, it is pivotal to develop an appropriate and controlled study model to study cat allergen-induced AR. Based on the review of existing literature, the consideration of which model to employ when studying cat allergen-induced AR depends on study objectives, cost, and resource accessibility. Given their similarity to real-world exposure, we recommend using a combination of AEC and NAC to evaluate participants AR response at different timepoints. This would provide valuable information about the acute and long-term effects of allergen exposure to better understand the full spectrum of cat allergen-induced AR.
LH, SL, RR, and AB wrote and edited the manuscript. AE ensured critical revision of the manuscript. All authors read and approved the final manuscript.
AE has participated in advisory boards for Abbvie, ALK Abello, AstraZeneca, Aralez, Bausch Health, Circassia Ltd., GSK, LEO Pharma, Merck, Novartis, Pfizer; has been a speaker for ALK Abello, Aralez, AstraZeneca, CSL Behring, Medexus, Novartis, Mylan, Pfizer, Sanofi and Takeda. Her institution has received research grants from ALK Abello, Aralez, AstraZeneca, Bayer LLC, Circassia, Green Cross, Merck, Medexus, Pfizer, Novartis, Sanofi, and Regeneron. She has also served as an independent consultant to Bayer LLC and Regeneron.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AEC, allergen exposure chambers; AIT, Allergen Specific Immunotherapy; AR, allergic rhinitis; AR-CIC, Allergic Rhinitis–Clinical Investigator Collaborative project; AUC, area under the curve; BHR, basophil histamine release; Cat-PAD, Cat-peptide antigen desensitization; CRTH2, chemoattractant receptor homologous molecule expressed on Th2 lymphocytes; EAC, environmental allergen challenge; ECP, eosinophil cationic proteins; EEC, Environmental Allergen Chamber; ELISA, Enzyme-Linked Immunosorbent Assay; FDA, Food & Drug Administration; FEV1, Forced expiratory volume in the 1st second; HEPA, high-efficiency particulate air; IgE, immunoglobulin E; IL, interleukin; ILC2s, Type 2 innate lymphoid cells; NAC, nasal allergen challenge; NOSS, nasal ocular symptom scores; PEFR, peak expiratory flow rate; SCIT, Subcutaneous Immunotherapy; SLIT, Sublingual Immunotherapy; TNSS, total nasal symptom score.
1. Bousquet PJ, Chinn S, Janson C, Kogevinas M, Burney P, Jarvis D. Geographical variation in the prevalence of positive skin tests to environmental aeroallergens in the European Community Respiratory Health Survey I. Allergy. (2007) 62:301–9. doi: 10.1111/j.1398-9995.2006.01293.x
2. Rancé F. Allergie aux phanères animaux chez l'enfant. Arch Pédiatrie. (2006) 13:584–6. doi: 10.1016/j.arcped.2006.03.031
3. Linneberg A, Nielsen NH, Madsen F, Frølund L, Dirksen A, Jørgensen T. Increasing prevalence of specific IgE to aeroallergens in an adult population: Two cross-sectional surveys 8 years apart: The Copenhagen Allergy Study. J Allergy Clin Immunol. (2000) 106:247–52. doi: 10.1067/mai.2000.108312
4. Arbes SSJ, Gergen PJ, Elliott L, Zeldin DC. Prevalences of positive skin test responses to 10 common allergens in the US population: results from the third National Health and Nutrition Examination Survey. J Allergy Clin Immunol. (2005) 116:377–83. doi: 10.1016/j.jaci.2005.05.017
5. Heinzerling L, Frew AJ, Bindslev-Jensen C, Bonini S, Bousquet J, Bresciani M, et al. Standard skin prick testing and sensitization to inhalant allergens across Europe – a survey from the GA2LEN network*. Allergy. (2005) 60:1287–300. doi: 10.1111/j.1398-9995.2005.00895.x
6. Løwenstein H, Lind P, Weeke B. Identification and clinical significance of allergenic molecules of cat origin. Part of the DAS 76 study. Allergy. (1985) 40:430–41. doi: 10.1111/j.1398-9995.1985.tb02682.x
7. Anderson MC, Baer H. Allergenically active components of cat allergen extracts - PubMed. J Immunol. (1981) 127:972–5.
8. Bonnet B, Messaoudi K, Jacomet F, Michaud E, Fauquert JL, Caillaud D, et al. An update on molecular cat allergens: Fel d 1 and what else? Chapter 1: Fel d 1, the major cat allergen Allergy, Asthma. Clin Immunol. (2018) 14:1–9. doi: 10.1186/s13223-018-0239-8
9. Wood RA, Eggleston PA. The effects of intranasal steroids on nasal and pulmonary responses to cat exposure. Am J Respir Crit Care Med. (1995) 151:315–20. doi: 10.1164/ajrccm.151.2.7842184
10. Wood RA, Laheri AN, Eggleston PA. The aerodynamic characteristics of cat allergen. Clin Exp Allergy. (1993) 23:733–9. doi: 10.1111/j.1365-2222.1993.tb00360.x
11. Pfaar O, Bergmann K-C, Bonini S, Compalati E, Domis N, de Blay F, et al. Technical standards in allergen exposure chambers worldwide – an EAACI Task Force Report. Allergy. (2021) 76:3589–612. doi: 10.1111/all.14957
12. Ramchandani R, Linton S, Hossenbaccus L, Ellis AK. Comparing the nasal allergen challenge and environmental exposure unit models of allergic rhinitis. Ann Allergy, Asthma Immunol. (2021) 127:163–4. doi: 10.1016/j.anai.2021.04.012
13. Ellis AK, Soliman M, Steacy L, Boulay MÈ, Boulet LP, Keith PK, et al. The Allergic Rhinitis - Clinical Investigator Collaborative (AR-CIC): Nasal allergen challenge protocol optimization for studying AR pathophysiology and evaluating novel therapies. Allergy, Asthma Clin Immunol. (2015) 11:1–10. doi: 10.1186/s13223-015-0082-0
14. Day JH, Ellis AK, Rafeiro E, Ratz JD, Briscoe MP. Experimental models for the evaluation of treatment of allergic rhinitis. Ann Allergy Asthma Immunol. (2006) 96:263–78. doi: 10.1016/S1081-1206(10)61235-5
15. Corren J, Wood RA, Patel D, Zhu J, Yegin A, Dhillon G, et al. Effects of omalizumab on changes in pulmonary function induced by controlled cat room challenge. J Allergy Clin Immunol. (2011) 127:398–405. doi: 10.1016/j.jaci.2010.09.043
16. Kelly S, Yang J, Karsh J, Marcelo J, Santone B, Mehri R, et al. Validation of air sampling technique for control of Fel d1 levels in cat allergen exposure chamber. Allergy. (2018) 73:543–543. doi: 10.1111/all.13539
17. Solomon E, Fukuyama T, Sampson M, Baeumer W, Chan S, Falbo J, et al. P078 Methods for homogenizing Feld1 levels in a cat allergen exposure chamber. Ann Allergy, Asthma Immunol. (2017) 119:S32. doi: 10.1016/j.anai.2017.08.118
18. Kelly SM, Marcelo J, Falbo J, Ly K, Yang J, Karsh J, et al. Stabilizing Fel d1 levels in a cat allergen exposure chamber. J Allergy Clin Immunol. (2018) 141:AB126. doi: 10.1016/j.jaci.2017.12.401
19. Corren J, Spector S, Fuller L, Minkwitz M, Mezzanotte W. Effects of zafirlukast upon clinical, physiologic, and inflammatory responses to natural cat allergen exposure. Ann Allergy Asthma Immunol. (2001) 87:211–7. doi: 10.1016/S1081-1206(10)62228-4
20. Raizman MB, Rothman JS, Maroun F, Rand WM. Effect of eye rubbing on signs and symptoms of allergic conjunctivitis in cat-sensitive individuals. Ophthalmology. (2000) 107:2158–61. doi: 10.1016/S0161-6420(00)00461-9
21. Marcelo J, Kelly S, Yang J, Karsh J, Mehri R, Santone B, et al. Validation of cat allergen exposure chamber for patients with perennial allergic rhinitis to cats. Allergy. (2018) 142. doi: 10.26226/morressier.5acdc65ad462b8029238da47
22. Berkowitz RB, Braker S, Lutz C, Jones P, Meeves S, Qiu C, et al. Efficacy of fexofenadine in the prophylactic control of cat allergen-induced allergic rhinitis. Ann Allergy Asthma Immunol. (2006) 96:327–33. doi: 10.1016/S1081-1206(10)61243-4
23. Wanger JS, Dockhorn RJ. Correlation of cat-hair (Fel d1) prick skin test to airway response using a live-cat-room challenge model. Allergy Asthma Proc. (1999) 20:371–6. doi: 10.2500/108854199778251735
24. Zeidler MR, Goldin JG, Kleerup EC, Kim HJ, Truong DA, Gjertson DW, et al. Small airways response to naturalistic cat allergen exposure in subjects with asthma. J Allergy Clin Immunol. (2006) 118:1075–81. doi: 10.1016/j.jaci.2006.06.042
25. Wood RA, Johnson EF, Van Natta ML, Pei Hua, Chen, Eggleston PA. A placebo-controlled trial of a HEPA air cleaner in the treatment of cat allergy. Am J Respir Crit Care Med. (1998) 158:115–20. doi: 10.1164/ajrccm.158.1.9712110
26. Nelson HS, Oppenheimer J, Vatsia GA, Buchmeier A. A double-blind, placebo-controlled evaluation of sublingual immunotherapy with standardized cat extract. J Allergy Clin Immunol. (1993) 92:229–36. doi: 10.1016/0091-6749(93)90166-D
27. Varney VA, Edwards J, Tabbah K, Brewster H, Mavroleon G, Frew AJ. Clinical efficacy of specific immunotherapy to cat dander: a double-blind placebo-controlled trial. Clin Exp Allergy. (1997) 27:860–7. doi: 10.1046/j.1365-2222.1997.1220903.x
28. Álvarez-Cuesta E, Berges-Gimeno P, Mancebo EG, Fernández-Caldas E, Cuesta-Herranz J, Casanovas M. Sublingual immunotherapy with a standardized cat dander extract: evaluation of efficacy in a double blind placebo controlled study. Allergy. (2007) 62:810–7. doi: 10.1111/j.1398-9995.2007.01365.x
29. Bousquet J, Michel FB, Creticos PS. Sublingual immunotherapy for cat allergy. J Allergy Clin Immunol. (1995) 95:920. doi: 10.1016/S0091-6749(95)70140-0
30. Pfaar O, Calderon MA, Andrews CP, Angjeli E, Bergmann KC, Bønløkke JH, et al. Allergen exposure chambers: harmonizing current concepts and projecting the needs for the future - an EAACI Position Paper. Allergy. (2017) 72:1035–42. doi: 10.1111/all.13133
31. Haya L, Mehri R, Ogrodnik N, Kelly SM, Falbo J, Yang J, et al. Aerosolization of cat dander in a naturalistic exposure chamber. J Allergy Clin Immunol. (2019) 143:AB122. doi: 10.1016/j.jaci.2018.12.370
32. Zahradnik E, Raulf M. Respiratory allergens from furred mammals: environmental and occupational exposure. Vet Sci. (2017) 4:38. doi: 10.3390/vetsci4030038
33. Almqvist C, Larsson PH, Egmar AC, Hedrén M, Malmberg P, Wickman M. School as a risk environment for children allergic to cats and a site for transfer of cat allergen to homes. J Allergy Clin Immunol. (1999) 103:1012–7. doi: 10.1016/S0091-6749(99)70172-7
34. Sicherer SH, Wood RA, Eggleston PA. Determinants of airway responses to cat allergen: Comparison of environmental challenge to quantitative nasal and bronchial allergen challenge. J Allergy Clin Immunol. (1997) 99:798–805. doi: 10.1016/S0091-6749(97)80014-0
35. Patel D, Couroux P, Hickey P, Salapatek AM, Laidler P, Larché M, et al. Fel d 1-derived peptide antigen desensitization shows a persistent treatment effect 1 year after the start of dosing: a randomized, placebo-controlled study. J Allergy Clin Immunol. (2013) 131:103–9.e1-7. doi: 10.1016/j.jaci.2012.07.028
36. Couroux P, Patel D, Armstrong K, Larché M, Hafner RP. Fel d 1-derived synthetic peptide immuno-regulatory epitopes show a long-term treatment effect in cat allergic subjects. Clin Exp Allergy. (2015) 45:974–81. doi: 10.1111/cea.12488
37. Hafner R, Couroux P, Armstrong K, Patel D, Larche M, Haumann B. Two year persistent treatment effect in reducing nasal symptoms of cat allergy after 4 doses of Cat-PAD, the first in a new class of synthetic peptide immuno-regulatory epitopes. Clin Transl Allergy. (2013) 3:O7. doi: 10.1186/2045-7022-3-S2-O7
38. Worm M, Lee HH, Kleine-Tebbe J, Hafner RP, Laidler P, Healey D, et al. Development and preliminary clinical evaluation of a peptide immunotherapy vaccine for cat allergy. J Allergy Clin Immunol. (2011) 127:89–97, 97.e1–14. doi: 10.1016/j.jaci.2010.11.029
39. Oldfield WLG, Larché M, Kay AB. Effect of T-cell peptides derived from Fel d 1 on allergic reactions and cytokine production in patients sensitive to cats: a randomised controlled trial. Lancet (London, England). (2002) 360:47–53. doi: 10.1016/S0140-6736(02)09332-7
40. Scadding GW, Eifan A, Penagos M, Dumitru A, Switzer A, Mcmahon O, et al. Local and systemic effects of cat allergen nasal provocation. Clin Exp Allergy. (2015) 45:613–23. doi: 10.1111/cea.12434
41. Kim YW, Singh A, Shannon CP, Thiele J, Steacy LM, Ellis AK, et al. Investigating immune gene signatures in peripheral blood from subjects with allergic rhinitis undergoing nasal allergen challenge. J Immunol. (2017) 199:3395–405. doi: 10.4049/jimmunol.1700378
42. Doherty TA, Scott D, Walford HH, Khorram N, Lund S, Baum R, et al. Allergen challenge in allergic rhinitis rapidly induces increased peripheral blood type 2 innate lymphoid cells that express CD84. J Allergy Clin Immunol. (2014) 133:1203–1205.e7. doi: 10.1016/j.jaci.2013.12.1086
43. Paterniti M, Kelly DC, Eckman JA, Sterba PM, Hamilton RG, Bochner BS, et al. Cat allergen-induced blood basophil reactivity in vitro predicts acute human nasal allergen challenge responses in vivo. Clin Exp Allergy. (2011) 41:963–9. doi: 10.1111/j.1365-2222.2011.03719.x
44. Sánchez A, Cardona R, Munera M, Calvo V, Tejada-Giraldo M, Sánchez J. Nasal provocation test with cat and dog extracts: results according to molecular components. Pulm Med. (2020) 2020:1–10. doi: 10.1155/2020/6365314
45. Steacy LM, Thiele J, Soliman M, Ellis AK. A comparison of the difference in symptom scores between seasonal and perennial allergens using the Nasal Allergen Challenge method. J Allergy Clin Immunol. (2017) 139:AB161. doi: 10.1016/J.JACI.2016.12.529
46. Ewbank PA, Murray J, Sanders K, Curran-Everett D, Dreskin S, Nelson HS, et al. double-blind, placebo-controlled immunotherapy dose-response study with standardized cat extract. J Allergy Clin Immunol. (2003) 111:155–61. doi: 10.1067/mai.2003.41
47. Nanda A, O'Connor M, Anand M, Dreskin SC, Zhang L, Hines B, et al. Dose dependence and time course of the immunologic response to administration of standardized cat allergen extract. J Allergy Clin Immunol. (2004) 114:1339–44. doi: 10.1016/j.jaci.2004.08.049
48. Eckman JA, Sterba PM, Kelly D, Alexander V, Liu MC, Bochner BS, et al. Effects of omalizumab on basophil and mast cell responses using an intranasal cat allergen challenge. J Allergy Clin Immunol. (2010) 125:889–895.e7. doi: 10.1016/j.jaci.2009.09.012
49. Neighbour H, Soliman M, Steacy LM, Hickey P, Forbes B, Larché M, et al. The Allergic Rhinitis Clinical Investigator Collaborative (AR-CIC): verification of nasal allergen challenge procedures in a study utilizing an investigational immunotherapy for cat allergy. Clin Transl Allergy. (2018) 8:15. doi: 10.1186/s13601-018-0198-7
50. Kim YW, Tonti E, Hickey P, Ellis AK, Neighbour H, Larché M, et al. Immunological changes in peripheral blood following nasal allergen challenge in subjects with allergic rhinitis pre- and post-peptide immunotherapy: An open-label clinical study. Allergy. (2021) 76:1907–11. doi: 10.1111/all.14710
51. Orengo JM, Radin AR, Kamat V, Badithe A, Ben LH, Bennett BL, et al. Treating cat allergy with monoclonal IgG antibodies that bind allergen and prevent IgE engagement. Nat Commun. (2018) 9:1–15. doi: 10.1038/s41467-018-03636-8
52. Shamji MH, Singh I, Layhadi JA, Ito C, Karamani A, Kouser L, et al. Passive prophylactic administration with a single dose of Anti–Fel d 1 monoclonal antibodies REGN1908–1909 in cat allergen–induced allergic rhinitis: a randomized, double-blind, placebo-controlled clinical trial. Am J Respir Crit Care Med. (2021) 204:23–33. doi: 10.1164/rccm.202011-4107OC
53. Tenn MW, Steacy LM, Adams DE, Walker TJ, Ellis AK. Comparison of allergic rhinitis outcomes of the environmental exposure unit and nasal allergen challenge model. Ann Allergy, Asthma Immunol. (2019) 123:105–6.e1. doi: 10.1016/j.anai.2019.04.003
54. Larson D, Patel P, Salapatek AM, Couroux P, Whitehouse D, Pina A, et al. Nasal allergen challenge and environmental exposure chamber challenge: A randomized trial comparing clinical and biological responses to cat allergen. J. Allergy Clin Immunol. (2020) 145:1585–97. doi: 10.1016/j.jaci.2020.02.024
Keywords: cat allergies, allergen exposure chamber (AEC), nasal allergen challenge, natural exposure model, allergic rhinitis (AR), Fel d 1 exposure
Citation: Hossenbaccus L, Linton S, Ramchandani R, Burrows AG and Ellis AK (2022) Study of Cat Allergy Using Controlled Methodology—A Review of the Literature and a Call to Action. Front. Allergy 3:828091. doi: 10.3389/falgy.2022.828091
Received: 02 December 2021; Accepted: 31 January 2022;
Published: 17 March 2022.
Edited by:
Glenis Kathleen Scadding, University College London Hospitals NHS Foundation Trust, United KingdomReviewed by:
Jorge Sánchez, University of Antioquia, ColombiaCopyright © 2022 Hossenbaccus, Linton, Ramchandani, Burrows and Ellis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne K. Ellis, YW5uZS5lbGxpc0BraW5nc3RvbmhzYy5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.