
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Allergy , 13 December 2022
Sec. Rhinology
Volume 3 - 2022 | https://doi.org/10.3389/falgy.2022.1048385
This article is part of the Research Topic Insights in Rhinology: 2021/22 View all 9 articles
 An-Sofie Viskens1,2,†
An-Sofie Viskens1,2,† Tine Wils1,†
Tine Wils1,† Pauline Van Bulck3,†Leen Cools3
Pauline Van Bulck3,†Leen Cools3 Olivier Vanderveken2,4Peter W. Hellings1,3,5,6*
Olivier Vanderveken2,4Peter W. Hellings1,3,5,6*
Background: Up to 40% of patients with chronic rhinosinusitis (CRS) remain uncontrolled despite guidelines of care being available, with an enormous socio-economic impact. The reasons for uncontrolled disease can be arbitrarily divided into disease-related, diagnosis-related, treatment-related, and patient-related factors. The relative contribution of each factor in uncontrolled CRS remains speculative. This explorative study aimed at determining the factors responsible for uncontrolled CRS in a tertiary care center, thereby identifying the most commons reasons for uncontrolled disease in CRS.
Methods: Patients with uncontrolled CRS (n = 187) were asked to fill out a questionnaire and underwent a clinical examination at the outpatient clinic of the University Hospital of Leuven, Belgium. Two independent physicians evaluated the (multiple) reason(s) for uncontrolled disease.
Results: In uncontrolled CRS, 66% of patients showed two or more reasons for uncontrolled disease according to the physicians' evaluation. Disease-related factors (70%) were most often considered the reason for uncontrolled disease, followed by treatment- (45%), patient- (42%), and diagnosis- (32%) related factors.
Conclusion: In case of uncontrolled CRS, the different contributing factors to the uncontrolled nature need to be carefully addressed during diagnostic and therapeutic actions in order to define strategies to improve CRS care. Most uncontrolled CRS patients have multiple reasons contributing to their disease status, with disease-related factors being the most common factor.
Chronic rhinosinusitis (CRS) is an inflammatory condition of the nose and paranasal sinuses affecting up to 10,9% of the general population (1). Nasal endoscopy defines the major phenotypes, being CRS without (CRSsNP) and with nasal polyps (CRSwNP), while immune investigations reveal the endotypes (2, 3). Given the novel therapeutic options for CRSwNP, including biologicals, type 2 inflammation is getting progressively more associated with CRSwNP, as well as with comorbidities like asthma. However, underlying immune responses are not the only factor driving the multifactorial aetiology of CRS. Beside immune factors, also genetic, environmental, occupational, anatomic and iatrogenic factors contribute to the manifestation of CRS. In a single patient, it is often challenging to pinpoint one or multiple factors driving the chronicity of disease (4, 5). European and US guidelines can offer some guidance for symptomatic CRS care based on scientific evidence and level of control (6, 7). Nevertheless, not much is known about the different reasons underlaying uncontrolled CRS (8). Therefore, it is important to identify factors contributing to uncontrolled CRS allowing improvement of treatment strategies and patient care.
Disease control is defined as the disease state in which the patient subjectively does not experience symptoms anymore, or the remaining symptoms are not regarded as bothersome (4). More specifically, CRS patients are defined as controlled, partially controlled or uncontrolled according to the European Position Paper on Rhinosinusitis and Nasal Polyp (EPOS) criteria, where the degree of symptom reduction, the clinical mucosal aspect, the presence of adverse events, the need for systemic medication and the need for functional endoscopic sinus surgery objectively determine the disease control status (4). Despite multiple guidelines of care, it is estimated that up to 40% of patients with CRS continue to experience bothersome symptoms despite guideline-driven treatment, including functional endoscopic sinus surgery (5, 6, 9). A key reason for this lack of therapeutic success is our current limited understanding of the mechanisms underlaying uncontrolled CRS disease. Therefore, as stated above, it is important to identify all factors contributing to uncontrolled CRS. We have previously proposed to classify the reasons of uncontrolled CRS and AR into four major groups (Figure 1) (4): the disease-related, the treatment-related, the diagnosis-related and the patient-related factors.

Figure 1. Reasons for uncontrolled chronic rhinosinusitis hellings and colleagues reviewed and classified the reasons for uncontrolled chronic rhinosinusitis (CRS) in the following four groups: disease-related factors, diagnosis-related factors, patient-related factors, and treatment-related factors (Hellings et al., 2013).
Disease-related factors consist of factors that are contributing directly to the pathophysiology of CRS. This also includes environmental and life-style factors like occupational irritants, pollutants or cigarette smoke, which might contribute to the severity of CRS (10). Another example of a disease-related factor is a viral infection that predisposes some patients to recurrent bacterial rhinosinusitis episodes, thereby causing extensive damage to the ciliated cells and respiratory epithelium (e.g., Influenza, Adenovirus) (11, 12). Furthermore, also hormonal and genetic factors have been proposed to aggravate inflammation and the severity of upper airway diseases such as CRS (6). A real therapeutic challenge has been the severe chronic upper airway disease (SCUAD) patients as they are uncontrolled CRS patients with disease-related factors contributing to the severity of their disease. A better understanding of the prevalence and nature of all the contributing factors to their uncontrolled CRS state will therefore improve their treatment success (9, 11–13). Treatment-related issues of uncontrolled upper airway disease are linked with non-guideline based therapies consisting of (sub)optimal choice of treatment or an incorrect dose and route. Furthermore, also a lack of symptom-oriented treatment is categorized as a treatment-related factor. Diagnosis-related factors are factors that might be overlooked in an intial diagnosis that contribute to the uncontrolled disease state. For example, nasal hyperreactivity is a typical factor present in a subgroup of CRS patients, however it is often not diagnosed correctly (14). Other diagnosis-related factors include the presence of NSAID-exacerbated respiratory disease (N-ERD), structural nasal deformities, global airway dysfunction and systemic diseases or even an incorrect diagnosis of CRS. It is important to correctly diagnose these comorbidities as they have a significant impact on treatment strategy and patients need to be better informed about them. Lastly, patient-related factors consist of lack of compliance and treatment adherence, as well as the proper use of medication. A physician also needs to be attentive on how reliable the information given by the patient is.
The impact and prevalence of each of the four groups of factors responsible for uncontrolled disease will be evaluated in this study. The outcomes of this study will contribute to the improvement of treatment in uncontrolled CRS disease, as we will identify which factors contribute the most to uncontrolled disease. Better understanding of these factors will result in defined strategies to achieve disease control and increased quality of life (QoL) for patients, thereby reducing the socio-economic burden of uncontrolled CRS.
This academic observational trial was coordinated at the Department of Otorhinolaryngology, Head and Neck surgery of the University Hospital of Leuven, Belgium from 2016 until 2018, with analysis of data in 2021–2022. The study was evaluated and approved by the medical ethical commission of the university Hospital of Leuven (S57274). CRS patients were clinically examined by ENT specialists and asked to complete a questionnaire. The inclusion criteria were the following: an initial CRS diagnosis, a minimum of 17 years of age, a visual analogue scale (VAS) score of 5 or more for total sinus symptoms severity, and/or a SNOT-22 score of 35 or more despite previous or current medical/surgical treatment for their sino-nasal symptoms, and a minimum of two medical outpatient clinic visits for CRS in the last 5 years. Finally, to be eligible, the patient required at least 2 physician visits in the past for CRS to reduce the likelihood of including those without long-standing CRS or a false diagnosis of CRS. Exclusion criteria were being morbidly ill or recent sinus surgery (within the last 6 months).
A total of 200 uncontrolled CRS patients were screened of which 187 CRS patients met the inclusion criteria for evaluation of the reasons of uncontrolled CRS.
The initial diagnosis of uncontrolled CRS was assessed by ENT specialists (PVB and PH) at the University Hospital of Leuven based on CRS symptoms and clinical examination, including nasal endoscopy. All patients filled out a validated questionnaire which consisted of six parts:
• General information (age, gender, time to diagnosis of CRS, time to diagnosis, comorbidities, medication use, history of sinus surgery, and general health)
• Disease-related factors
• Diagnosis-related factors
• Treatment-related factors
• Patient-related factors
• The physician ‘s evaluation of the cause(s) for uncontrolled disease
The first five parts of the questionnaire were filled out by the patient. The last part of the questionnaire was completed by the physician after examination of the patient and then submitted to another physician who re-evaluated the reasons independently. Uncontrolled CRS was diagnosed using a VAS score of ≥5 and/or SNOT-22 score of ≥35 in combination with an evaluation of the nasal mucosa by nasal endoscopy (15).
The following symptoms on a VAS score were asked for further evaluation: total sino-nasal symptoms, nasal blockage, headache/facial pain, loss of smell, post-nasal drip (PND), runny nose, itchy eyes, itchy nose, sneezing, watery eyes, coughing, pressing sensation on the chest, dyspnoea, wheezing.
General information included age, gender, onset of complaints, diagnosis of CRS, comorbidities, and general health. The time to diagnosis was determined by asking patients to describe the date of onset of the CRS symptoms and the date of the confirmation by means of clinical examination and nasal endoscopy. They were also asked to write down their comorbidities, which were verified using the patients' medical history in their medical record. Subjects were also asked to mark the state of general health in terms of excellent, good, moderate, or bad.
Several factors can be responsible for a severe phenotype of CRS. All patients were asked if their symptoms were triggered by occupational and/or environmental factors, which could contribute to the severity of the symptoms. Their medical history with a comorbidity of a lower-airway disease (COPD, chronic bronchitis, and asthma) and also the presence of a hypersensitivity to aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs), was asked for. The patients were asked about nicotine abuse and the amount of smoking (packyears). Female sex hormones, which have been associated with more severe allergic inflammation, were evaluated by asking about oral contraceptives, pregnancy and menopause.
The ENT specialist reconsidered the diagnosis of uncontrolled CRS and associated comorbidities, by investigating concomitant anatomic nasal deformities, global airway dysfunction, presence of N-ERD and systemic diseases, by medical history and clinical examination. Anatomic deformities included perforation of the septum, significant septal deviation and nasal valve dysfunction. In context of associated comorbidities, the presence of associated airborne allergies e.g., hay fever or house dust mite allergy was evaluated. Airway allergies were diagnosed by means of a skin prick test, Immunocaps/RAST or verified in the patient's medical record if test results within the last 2 years were available. Medical history of a systemic disease [congenital or acquired immunodeficiency, congenital mucociliary dysfunction, primary ciliary dyskinesia, cystic fibrosis, systemic vasculitis, or granulomatous diseases (e.g., granulomatosis with polyangiitis and sarcoidosis)], dental disease and gastroesophageal reflux were asked and checked in the medical files.
Patients were asked about the current type of medication (e.g., nasal rinses, intranasal corticosteroids, antibiotics), dose, frequency, and route of administration were asked. The number of previous sinus operations was also questioned.
Patient-related factors including treatment adherence and correct medication use were questioned. Subjective factors like prejudices about treatment, fear of adverse events, and economic reasons were also asked. Patients were asked to report side effects. The doctor subjectively evaluated patient reliability.
Statistical analyses were performed with Graphpad Prism VI for Macintosh Version 8.4.3 (GraphPad Software Inc., San Diego, USA) by using the non-parametric Kruskal–Wallis test when comparing a single outcome between different groups. Prevalence differences in categorical variables (e.g., gender) were tested using the Pearson's chi squared test. A correlation analysis according to spearman was used to calculate a correlation between SNOT-22 score and the number of previous FESS operations. A statistical test was considered to be significant when p < 0.05.
A total of 187 included patients with uncontrolled CRS were evaluated. The mean age was 46.56 ± 2.08 years with equal distribution between males (51%) and females (49%) (Table 1). Only 26% were diagnosed with CRS within the first year of their symptoms. More than half of the patients (62%) had airway comorbidities of which 32% had concomitant allergies and 25% had co-morbid asthma, while 44% had systemic comorbidities and 7% had N-ERD. The mean total VAS score of sino-nasal symptoms was high (7.39 ± 1.78) (Table 2). The complaints perceived as most bothersome were nasal obstruction, postnasal drip, headache and anosmia. The total VAS score of sino-nasal symptoms correlated well with the average SNOT-22 score. Patients with a high VAS-score also had a high SNOT-22 score (Figure 2A). In our cohort, most patients (83%) had 1 or 2 FESS operations in the past (Table 1). The number of FESS operations only had a small positive correlation with the SNOT-22 score (p < 0,01; r = 0,24). Most patients with CRS had two (39%) possible reasons for their uncontrolled disease (Figure 2B). A single cause was present in 34% of the patients, three reasons were present in 22% of the patients and only 5% had four reasons for uncontrolled CRS. The most frequent reason for uncontrolled CRS was a disease-related factor (70%) (Figure 2C). Treatment-related factors (45%) were reported on the second place, followed by patients-related factors (42%) and diagnosis-related factors (32%) (Figure 2C).

Figure 2. Average VAS score, number, and percentage of reasons for uncontrolled disease (A) average VAS score of patients in each SNOT-22 score group. Data are shown as mean ± standard deviation. Kruskal-Wallis test was used for comparison between the different groups; *** p < 0.0001; ** p < 0.007 (B) Number of reasons for uncontrolled disease as assessed by an ear-nose-throat (ENT) specialists based on the questionnaire and clinical evaluation. (C) Observed prevalence of each factor contributing to uncontrolled disease. (D) Disease status according to the EPOS 2020 guidelines for CRS in the patient cohort. We analyzed our inclusion criteria for uncontrolled CRS disease against the corresponding, more recently published, EPOS guidelines for uncontrolled disease in CRS patients (Fokkens et al., 2020). The numbers represent the number of patients falling into the corresponding EPOS guideline category for controlled, partially or uncontrolled CRS.
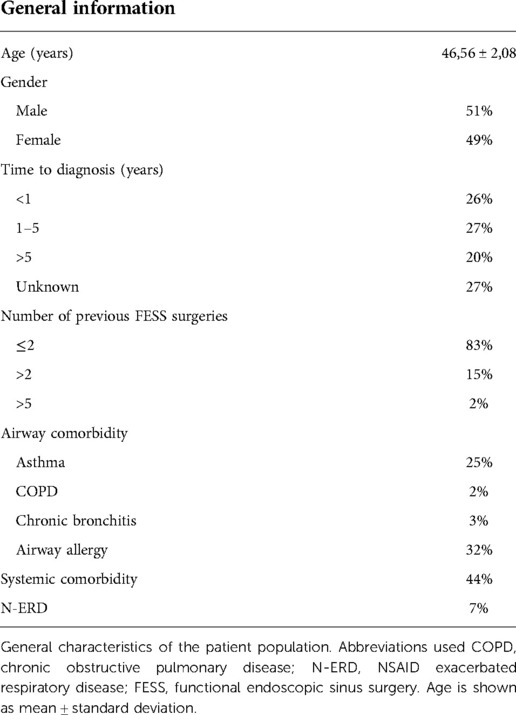
Table 1. General patient characteristics.
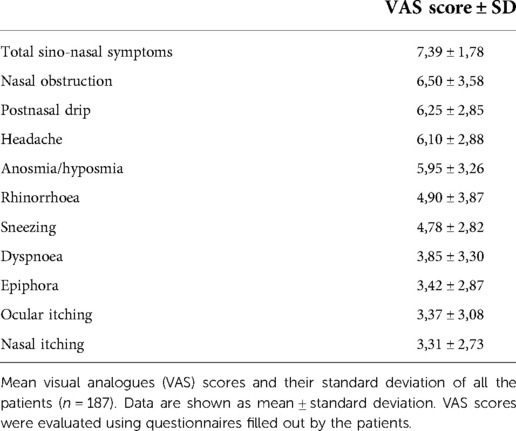
Table 2. Mean visual analogue (VAS) score.
Concerning the disease-related factors, 61% of the patients had an environmental factor, such as exposure to cold air, fog, a hobby (e.g., swimming or painting) or contact with their pet, contributing to their symptoms. Occupational factors were reported in 35% of the patients of which the most common occupations were office workers or teacher/day care centre operator. Lower airway disease was seen in a 30% of the patients of which the majority had asthma (25%) contributing to their uncontrolled CRS, while COPD and chronic bronchitis contributed in 2% and 3% of the cases, respectively. Furthermore, airborne allergies were present in 32% of our patient cohort. Other disease-related factors contributing to uncontrolled disease were genetic factors in 5% of the patients and smoking in 20% of the patients. Hormones and pregnancy were only relevant in one subject. (Table 3A).
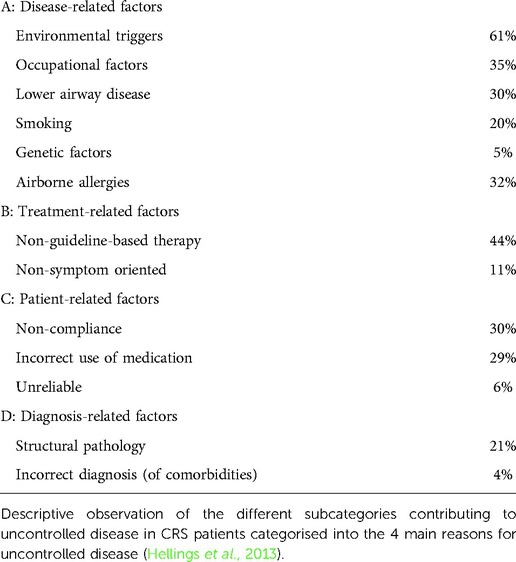
Table 3. Reasons for uncontrolled disease.
A total of 44% patients had non-guideline recommended therapy according to the EPOS guidelines (6). Of these patients 20% received maintenance treatment but not the required medication according to the EPOS guidelines and 24% didn't even receive any maintenance therapy at all and relied solely on rescue medication. Of all patients in the cohort, 59% received rescue medication at least one time within the last 3 months (Table 4). Only 11% of patients had a lack of symptom-oriented treatment. (Table 3B).
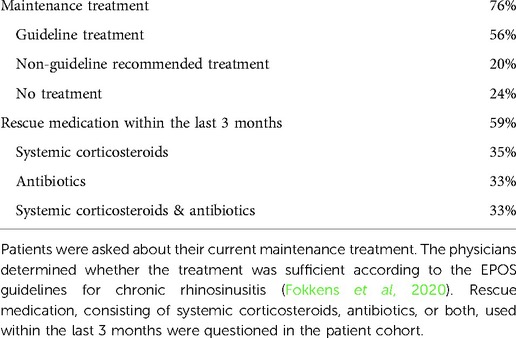
Table 4. Relevant medication use of the patients.
When looking at the patient-related factors, 30% of the patients suffered from uncontrolled disease due to poor treatment adherence. Furthermore, 29% used their medication incorrectly, while 6% of the patients were deemed unreliable by their physicians. Side effects of treatment occurred in 12% of patients. The most frequent side effects reported were sleepiness and epistaxis. Approximately 19% of the patients stopped their medical treatment for a certain amount of time, because they were tired of taking medication every day or didn't deem it necessary anymore (Table 3C).
In 21% of the patients, structural nasal pathology was identified as a diagnosis-related factor contributing to uncontrolled disease. Significant nasal septal deviation was seen in 11% of patients, nasal valve dysfunction in 6% and septal perforation in 3%. The initial diagnosis of CRS was incorrect in 4% of the patients who mostly had rhinitis medicamentosa or postnasal drip due to allergic or non-allergic rhinitis. (Table 3D).
During the course of this study, new EPOS guidelines (6) were published on defining (un)controlled CRS. We correlated our population of uncontrolled CRS patients with the new guidelines and saw that, as expected, more than 90% of these patients were also defined as uncontrolled according to the new EPOS guidelines (Figure 2D). Out of the 187 patients in our cohort, fifteen patients were defined as partially controlled, and one patient was classified as controlled according to the new EPOS guidelines. The controlled status according to the new EPOS guidelines of this one patient can be attributed to a low VAS score for specific CRS symptoms such as postnasal drip despite a high overall VAS score for total sino-nasal symptoms.
This study found that disease-related factors (SCUAD) were the most common factors underlaying uncontrolled disease in CRS patients followed by treatment-, patient-, and diagnosis- related factors. Most patients reported two or more reasons for poor CRS control. In addition, this study found that only 26% of patients were correctly diagnosed with CRS within one year after the start of their symptoms.
SCUAD was found in an astonishing 70% of the uncontrolled CRS population. These SCUAD patients represent a real therapeutic challenge for physicians because these disease-related factors are hard to modify or treat. For example, the environmental and occupational factors, which were the most common disease-related factors, cannot be that easily modified as other factors. Nevertheless, most of these SCUAD patients also had other factors contributing to their uncontrolled disease of which patient-related factors were the most common second factor. Other factors, and especially these patient-related factors, can be more easily managed compared to the disease-related factors (16). Therefore, it might be a therapeutic strategy to eliminate other factors as much as possible in these SCUAD patients, which can lead to better disease control.
Treatment-related factors are the second most common reason of uncontrolled CRS. Twenty-four percent of these patients didn't receive any maintenance treatment despite being recommended by the EPOS guidelines. Non-compliance was the most common reason of the patient-related factors, which is a known phenomenon in chronic diseases (17). Since 29% of patients did not use their medication correctly, there is a need to better educate the patients how to use their medication e.g., point the nozzle of the intranasal corticosteroid slightly outwards, away from the septum while spraying (18). Recent technologies, such as mobile applications, pave the way for improving patient-related factors. For example, mobile applications, such as “mySinusitisCoach” (19) can be specifically designed for better follow up of the patient's compliance and treatment adherence. Additionally, a mobile application can also contain tips and tricks, as well as videos on how to correctly use medication, therefore better educate the patient in how to use their medication (19, 20).
As expected, due to our inclusion criteria this study confirmed a high average VAS-score (7.39 ± 1.78) for total sino-nasal symptoms in uncontrolled CRS patients. The study also confirmed the classic symptoms of CRS (nasal obstruction, postnasal drip, headache and anosmia). A remarkable finding is that only 26% of patients were correctly diagnosed with CRS within one year after the start of their symptoms. However, confirmation of the above percentage with other studies in the future is necessary. In our cohort, 20% of the patients were smokers which is slightly higher than the national average of 12% (21). The number of patients who had concomitant asthma and/or airborne allergies were in line with current literature (22).
Current literature often describes the epidemiology of CRS and how to classify severe uncontrolled CRS patients (6, 8, 23). However, there is a lack of studies covering the actual reasons behind patients being uncontrolled after years and years of treatment (24). Therefore, our study, which defines the different factors important for uncontrolled disease, paves the way for the optimalisation of CRS care. As still up to 40% of CRS patients remain uncontrolled despite guideline-based treatments, a better characterisation of these four main factors in uncontrolled CRS patients will help to set up a patient-centred treatment plan, specifically managing an individual patients' needs.
One of the strengths of this study is the large number of patients despite being a monocentric study. Another strength is the appropriate clinical and anamnestic parameters to define uncontrolled disease. We defined CRS as uncontrolled if the VAS-score for total sino-nasal symptoms was 5 or more and/or if the SNOT-22 score was 35 or more. The former because a VAS score of 5 or more has been generally accepted in the field to significantly affect the QoL of the patients and has more recently also been incorporated in the latest EPOS guidelines and EUFOREA guidelines for severe uncontrolled CRS (6, 23). The latter because a SNOT-22 score of 35 or more was identified as the best cut-off for poorly controlled severe CRS patients (25). This SNOT-22 cut-off of 35 or more was also later confirmed by the recent EPOS and EUFOREA guidelines for severely uncontrolled CRS (6, 23). During the course of our study new EPOS guidelines (6) were published on defining (un)controlled CRS. Our correlation analysis showed that more than 90% of the patients in our cohort were still defined as having “uncontrolled CRS” according to the new guidelines. There was only one patient that, due to a low VAS-score for specific CRS symptoms, despite having a high overall VAS score for total sino-nasal symptoms, was deemed controlled according to the new criteria EPOS criteria (6).
Our study also has limitations. Although the VAS-score and SNOT-22 score were combined with an endoscopic evaluation of the nasal mucosa, we cannot deny that all these tests are rather subjective, and endoscopy is susceptible to interobserver variability. It would be more objective if a low-dose CT-scan was performed in all patients (26). In contrast, a strength of this study is that airborne allergies were objectified using a skin or RAST test. However, we did not discriminate between CRSwNP and CRSsNP, it could be interesting for future research to discriminate between these two phenotypes as this might reveal different contributing factors based on phenotype.
To conclude, the most common reason for uncontrolled CRS is related to the disease itself, followed by treatment-, patient-, and diagnostic related factors. However, most patients reported two or more reasons for poor CRS control. Therefore, it is important to properly identify the underlying reasons for uncontrolled disease in CRS patients and focus on easily manageable contributing factors to optimise CRS care.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethische commissie onderzoek UZ/KU Leuven. The patients/participants provided their written informed consent to participate in this study.
PVB, PH designed the work; ASV, TW, PVB, LC acquired and analyzed data; ASV, TW, PVB, OV, PH drafted, revised, and approved the manuscript; ASV, TW, PVB, LC, OV, PH agree to be accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
TW is a recipient of a PhD Fellowship from the Fund of Scientific research (FWO) (11L8922N)
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hastan D, Fokkens WJ, Bachert C, Newson RB, Bislimovska J, Bockelbrink A, et al. Chronic rhinosinusitis in Europe–an underestimated disease. A GA²LEN study. Allergy. (2011) 66(9):1216–23. doi: 10.1111/j.1398-9995.2011.02646.x
2. De Greve G, Hellings PW, Fokkens WJ, Pugin B, Steelant B, Seys SF. Endotype-driven treatment in chronic upper airway diseases. Clin Transl Allergy. (2017) 7:22. doi: 10.1186/s13601-017-0157-8
3. Hellings PW, Steelant B. Epithelial barriers in allergy and asthma. J Allergy Clin Immunol. (2020) 145(6):1499–509. doi: 10.1016/j.jaci.2020.04.010
4. Hellings PW, Fokkens WJ, Akdis C, Bachert C, Cingi C, Dietz de Loos D, et al. Uncontrolled allergic rhinitis and chronic rhinosinusitis: where do we stand today? Allergy. (2013) 68(1):1–7. doi: 10.1111/all.12040
5. van der Veen J, Seys SF, Timmermans M, Levie P, Jorissen M, Fokkens WJ, et al. Real-life study showing uncontrolled rhinosinusitis after sinus surgery in a tertiary referral centre. Allergy. (2017) 72(2):282–90. doi: 10.1111/all.12983
6. Fokkens WJ, Lund V, Hopkins C, Hellings PW. European position paper on rhinosinusitis and nasal polyps. Rhinology. (2020) 58(Suppl S29):1–464. doi: 10.4193/Rhin20.600
7. Orlandi RR, Kingdom TT, Smith TL, Bleier B, DeConde A, Luong AU, et al. International consensus statement on allergy and rhinology: rhinosinusitis 2021. Int Forum Allergy Rhinol. (2021) 11(3):213–739. doi: 10.1002/alr.22741
8. Hellings PW. SWOT analysis of chronic rhinosinusitis care anno 2022. J Allergy Clin Immunol. (2022) 10(6):1468–71. doi: 10.1016/j.jaip.2022.01.039
9. Prokopakis EP, Vlastos IM, Ferguson BJ, Scadding G, Kawauchi H, Georgalas C, et al. SCUAD And chronic rhinosinusitis. Reinforcing hypothesis driven research in difficult cases. Rhinology. (2014) 52(1):3–8. doi: 10.4193/Rhino13.049
10. Hox V, Delrue S, Scheers H, Adams E, Keirsbilck S, Jorissen M, et al. Negative impact of occupational exposure on surgical outcome in patients with rhinosinusitis. Allergy. (2012) 67(4):560–5. doi: 10.1111/j.1398-9995.2011.02779.x
11. Meena RS, Meena D, Aseri Y, Singh BK, Verma PC. Chronic rhino-sinusitis and asthma: concept of unified airway disease (UAD) and its impact in otolaryngology. Indian J Otolaryngol Head Neck Surg. (2013) 65(S2):338–42. doi: 10.1007/s12070-012-0495-8
12. Bernstein JM, Ballow M, Schlievert PM, Rich G, Allen C, Dryja D. A superantigen hypothesis for the pathogenesis of chronic hyperplastic sinusitis with massive nasal polyposis. Am J Rhinol. (2003) 17(6):321–6. doi: 10.1177/194589240301700601
13. Wu D, Bleier BS, Wei Y. Current understanding of the acute exacerbation of chronic rhinosinusitis. Front Cell Infect Microbiol. (2019) 9:9–15. doi: 10.3389/fcimb.2019.00415
14. Feijen J, Seys SF, Steelant B, Bullens DMA, Dupont LJ, García-Cruz M, et al. Prevalence and triggers of self-reported nasal hyperreactivity in adults with asthma. World Allergy Organ J. (2020) 13(6):100132. doi: 10.1016/j.waojou.2020.100132
15. Doulaptsi M, Prokopakis E, Seys S, Pugin B, Steelant B, Hellings P. Visual analogue scale for sino-nasal symptoms severity correlates with sino-nasal outcome test 22: paving the way for a simple outcome tool of CRS burden. Clin Transl Allergy. (2018) 8:32. doi: 10.1186/s13601-018-0219-6
16. Vennik J, Eyles C, Thomas M, Hopkins C, Little P, Blackshaw H, et al. Chronic rhinosinusitis: a qualitative study of patient views and experiences of current management in primary and secondary care. BMJ Open. (2019) 9(4):e022644. doi: 10.1136/bmjopen-2018-022644
17. Fernandez-Lazaro CI, García-González JM, Adams DP, Fernandez-Lazaro D, Mielgo-Ayuso J, Caballero-Garcia A, et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. (2019) 20(1):132. doi: 10.1186/s12875-019-1019-3
18. Rollema C, van Roon EN, de Vries TW. Inadequate quality of administration of intranasal corticosteroid sprays. J Asthma Allergy. (2019) 12:91–4. doi: 10.2147/JAA.S189523
19. Seys S, Bousquet J, Bachert C, Fokkens W, Agache I, Bernal-Sprekelsen M, et al. Mysinusitiscoach: patient empowerment in chronic rhinosinusitis using mobile technology. Rhinology. (2018) 56(3):209–215. doi: 10.4193/Rhin17.253
20. Claeys N, Teeling MT, Legrand P, Poppe M, Verschueren P, De Prins L, et al. Patients unmet needs in chronic rhinosinusitis with nasal polyps care: a patient advisory board statement of EUFOREA. Front Allergy. (2021) 2:761388. doi: 10.3389/falgy.2021.761388
21. Gisle L, Demarest S, Drieskens S. Gezondheidsenquete 2018: gebruik van tabak. Sciensano. (2018) 12–14.
22. Philpott CM, Erskine S, Hopkins C, Kumar N, Anari S, Kara N, et al. Prevalence of asthma, aspirin sensitivity and allergy in chronic rhinosinusitis: data from the UK National Chronic Rhinosinusitis Epidemiology Study. Respir Res. (2018) 19(1):129. doi: 10.1186/s12931-018-0823-y
23. Bachert C, Han JK, Wagenmann M, Hosemann W, Lee SE, Backer V, et al. EUFOREA Expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: definitions and management. J Allergy Clin Immunol. (2021) 147(1):29–36. doi: 10.1016/j.jaci.2020.11.013
24. Penttilä E, Sillanpää S, Vento SI, Myller J, Koskinen A, Hammarén-Malmi S, et al. Eosinophilia, asthma, NERD and the use of oral corticosteroids predict uncontrolled chronic rhinosinusitis with nasal polyps after surgery. Asian Pac J Allergy Immunol. (2021) [Online ahead of print]. doi: 10.12932/ap-310321-1102
25. Toma S, Hopkins C. Stratification of SNOT-22 scores into mild, moderate or severe and relationship with other subjective instruments. Rhinology. (2016) 54:129–33. doi: 10.4193/Rhino15.072
Keywords: chronic rhinosinusitis, uncontrolled disease, SCUAD, CRS therapy, contributing factors
Citation: Viskens A, Wils T, Van Bulck P, Cools L, Vanderveken O and Hellings PW (2022) Multiple reasons underlaying uncontrolled disease in the majority of chronic rhinosinusitis patients. Front. Allergy 3:1048385. doi: 10.3389/falgy.2022.1048385
Received: 19 September 2022; Accepted: 23 November 2022;
Published: 13 December 2022.
Edited by:
Cemal Cingi, Eskişehir Osmangazi University, TurkeyReviewed by:
Peter Valentin Tomazic, Medical University of Graz, Austria© 2022 Viskens, Wils, Van Bulck, Cools, Vanderveken and Hellings. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Peter Hellings cGV0ZXIuaGVsbGluZ3NAdXpsZXV2ZW4uYmU=
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Rhinology, a section of the journal Frontiers in Allergy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.