 Antolín López-Viña
Antolín López-Viña Rocío M. Díaz Campos2*
Rocío M. Díaz Campos2* Andrea Trisan Alonso
Andrea Trisan Alonso Carlos Melero Moreno
Carlos Melero Moreno- 1Servicio de Neumología, Hospital Universitario Puerta de Hierro, Majadahonda, Madrid, Spain
- 2Servicio de Neumología, Hospital Universitario 12 de Octubre, Madrid, Spain
- 3Instituto de Investigación (i+ 12), Hospital Universitario 12 de Octubre, Madrid, Spain
In recent years, advances in knowledge of molecular mechanisms involved in asthma have changed uncontrolled severe asthma (USA) treatment, with the appearance of biological treatment. USA is a heterogeneous entity with different endotypes and phenotypes. Nowadays, the biological drugs approved with asthma indication are omalizumab, mepolizumab, reslizumab, benralizumab and dupilumab. Tezepelumab is approved by the Food and Drug Administration (FDA) in the United States and, recently, by the European Medicines Agency (EMA). All these biological drugs have shown their efficacy in clinical trials, especially in reducing exacerbations, improving asthma control, quality of life, pulmonary function, and withdrawing systemic corticosteroids or at least reducing their daily dose, with some differences between them. Except for mepolizumab and reslizumab, biological drugs have different targets and thus different therapeutic indications should be expected; however, in some patients, more than one drug could be indicated, making the election more difficult. Because there are no direct comparisons between biological drugs, some biomarkers are used to choose between them, but they are not unbeatable. In this article, an algorithm to choose the first biological drug in a specific patient is proposed based on different study results and patient’ characteristics.
Introduction
Severe asthma (SA) requires high doses of inhaled corticosteroids (ICS) associated with another controller medication [long-acting beta 2 adrenergic agonists (LABA) and/or long-acting anticholinergic (LAMA)] to be controlled or despite that remains uncontrolled. Therapeutic adherence, comorbidities, and triggers must be evaluated before (1).
Uncontrolled severe asthma (USA) is considered when SA remains uncontrolled despite high doses of ICS and LABA or oral corticosteroids (OCS), for at least, 6 months in 1 year without any other cause than disease severity (1).
Although the USA is approximately 5% of the asthmatic population (2), it accounts for more than half of asthma costs and is responsible for daily symptoms, frequent exacerbations, and hospitalizations (3, 4). OCS adverse events (AE) must be considered (5, 6).
SA is a heterogeneous syndrome considering allergy presence, symptoms onset, airway obstruction severity, treatment response, and prognosis. Recently, SA is considered biologically heterogeneous with differentiated subtypes characterized by different pathophysiological mechanisms so endotypes or molecular phenotypes are defined (7–11). There are two endotypes: high T2 and low T2.
High T2 endotype is driven by T2 cytokines (IL-4, IL-5, and IL-13), eosinophils, alarmins [IL-25, IL-33, and thymic stromal lymphoprotein (TSLP)], and IgE. There are two groups of patients with high T2 SA: early-onset allergic asthma and late-onset eosinophil asthma (12–14).
There are different biomarkers to identify high T2 inflammation (15–18): blood and sputum eosinophils, exhaled fraction of nitric oxide (FeNO).
Clinical practice guidelines (19–21) based on different studies determine as cut-off points: blood eosinophils ≥150/µl, and/or FeNO ≥ 20ppb, and/or induced sputum (IS) eosinophils ≥2%. IgE cannot be considered a T2 biomarker, although it is used to calculate omalizumab’s dose, but an allergic prick test or specific IgE determination can.
Low T2 endotype mechanism knowledge is poor, and no biomarkers for its identification are available (22). It is characterized by neutrophilic or pauci-granulocytic inflammation (7).
Advances in knowledge of T2 asthma molecular mechanisms have led to the appearance of monoclonal antibodies (MA) which target immunoglobulins and cytokines implicated in the inflammatory cascade (23). Nowadays, biological drugs approved by regulatory agencies in the United States (FDA) and Europe (EMA) are Omalizumab (MA that blocks IgE union to its receptor for allergic asthma), mepolizumab and reslizumab (anti-IL-5 MA for eosinophilic asthma), benralizumab (antagonist of the α subunit of IL-5 receptor for eosinophilic asthma), and dupilumab (directed against the α subunit of IL-4 receptor which is a common receptor for IL-4 and IL-13). Tezepelumab [anti-alarmin directed against the thymic stromal lymphopoietin (TSLP)] has shown its efficacy in the USA approved by FDA, and recently, by EMA.
Clinical trials and real-world studies, with T2 USA patients, have shown MAs' efficacy in reducing exacerbations, improving asthma control, pulmonary function, and withdrawing or at least reducing OCS daily dose.
A great response variability is seen in clinical practice, from super-responders (no symptoms, no exacerbations) to sub-optimal or no responders at all. To make precision medicine, it would be ideal to know which MA is the best for each patient, but no head-to-head comparisons are available while indirect comparisons (24–28) are but with low value mainly because of arbitrarily inclusion criteria.
The best scenario would be to have predictor markers of good or bad response to MA but until they are available the MA election would be based on asthma patients’ characteristics.
This article will revise different biomarkers studies that could predict MA response in T2 asthma patients, differences in MA clinical trials, and their impact on comorbidities. Also, the importance of treatment goals for each patient, the patient’s age, and the patient’s treatment preferences with the aim to propose an algorithm to choose the first MA in a specific patient.
Possible biomarkers
Blood eosinophil count
Is the most frequent biomarker used to predict therapeutic response to all MA. Its determination is cheap, minimally invasive, and easy to obtain. Although it has some drawbacks as temporary fluctuations in time (29) and its reduction with some drugs mainly OCS. Repeated determinations improve its sensibility. In patients taking OCS is recommended to reduce the dose and realize different determinations (30).
Response to anti-IL5/IL5Rα MA is better with more eosinophils in the blood.
Exacerbation reduction with mepolizumab is better with more than 300 blood eosinophils/µl and almost nil under 150 eosinophils/µl (31, 32). With reslizumab, a response is almost nil with less than 400 eosinophils/µl (33), while benralizumab’s efficacy is better with more than 300 blood eosinophils/µl (34). With dupilumab (35, 36), there is a better response with more than 300 eosinophils/µl.
EXTRA (37) post hoc analysis with omalizumab showed a better response with more than 300 eosinophils/µl, although this result was not seen in other studies.
Tezepelumab’s efficacy is better with more than 150 eosinophils/µl, although it has shown benefits in patients without eosinophilia (38).
Sputum eosinophils
The “gold standard” test to diagnose T2 asthma is the presence of eosinophils in sputum. The relationship between an increase in exacerbations and more eosinophils in sputum has been demonstrated (39, 40). Some factors such as cost, availability and time, make it difficult to use this biomarker, so it is available only in some hospitals.
In clinical practice, eosinophils in sputum are not validated to choose a MA although they could be used to evaluate treatment response. Data exists about the persistence of eosinophils in sputum in non-responder patients treated with mepolizumab, indicating T2 residual inflammation, so a switch to reslizumab (41) could be an option (weight dose calculated).
FeNO
FeNO is a non-invasive parameter of epithelial damage and bronchial T2 phenotype associated with eosinophil inflammation. It is related to different T2 citoquines, mainly with IL13.
FeNO does not predict anti-eosinophil MA (anti IL5/IL5Rα) response. No differences are seen in patients’ responses with high or low FeNO.
Exacerbation reduction with dupilumab (36) is greater with FeNO values ≥ 25ppb so it is used as a response biomarker.
Omalizumab’s response was better with FeNO ≥ 24ppb in the EXTRA study (37), although this result was not shown in other studies.
Exacerbation reduction with tezepelumab is also predicted by FeNO values (38).
Blood IgE
Blood IgE cannot be considered a T2 inflammation biomarker. A relationship between IgE level and atopic asthma exists, although high blood IgE levels can be seen in patients with non-atopic asthma (42).
Omalizumab’s dose is calculated considering blood IgE level but exacerbation reduction is independent of IgE values (43).
Dupilumab was effective in allergic and non-allergic asthma patients in the QUEST study, even with high blood IgE level (>700 IU/ml), so dupilumab could be used in allergic asthma with blood IgE level >1,500 IU/ml (44).
Blood IgE level does not predict response to anti-IL5 MA.
Periostin
Periostin is a protein detected in peripheral blood and secreted by epithelial cells in response to IL4/IL13. Initially, it arose a lot of expectations as a response detector mainly for anti-IL13 MA. Periostin is associated with tissue remodeling in asthma and does not always correlate with eosinophils and other biomarkers (45). Nowadays, the interest in periostin as a response predictor has decreased.
Differences between MA in pivotal studies
Omalizumab
Clinical trials (46–50), meta-analysis (51), and real-world studies (52, 53) have shown Omalizumab's efficacy in ≥ 6 years old USA patients with sensitization for at least one perennial allergen and IgE blood levels from 30 to 1,500 IU/l. Exacerbations reduction, asthma control improvement, and moderate and inconsistent pulmonary function improvement have been demonstrated. Data about OCS reduction or withdrawal is contradictory (Table 1).
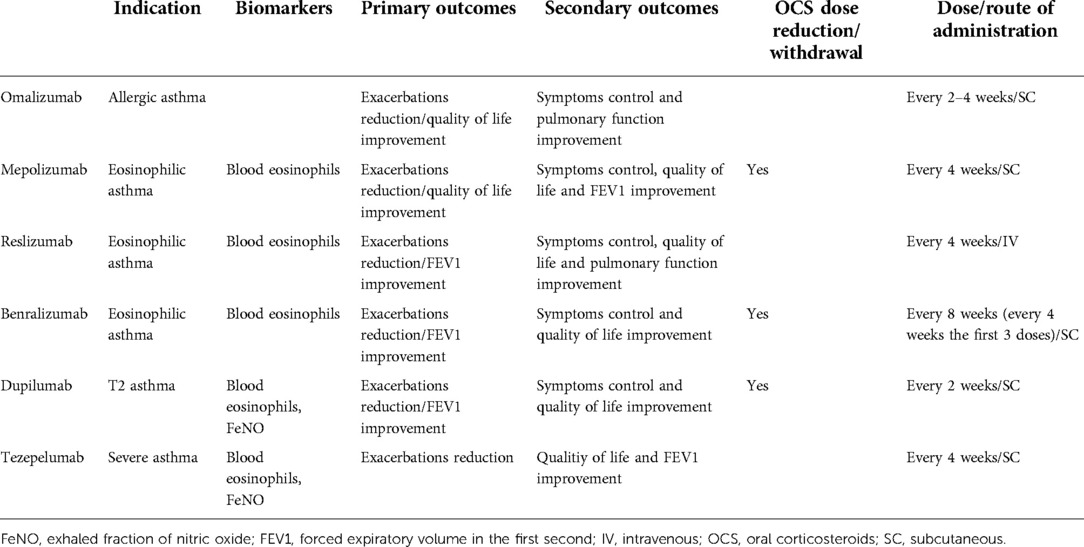
Table 1. Monoclonal antibodies’ results differences.
Mepolizumab
Exacerbations reduction (54–56), OCS dose reduction (57, 58), improvement in quality of life (54, 56, 57), asthma control (56, 57), and forced expiratory volume in the first second (FEV1) (56) have been shown in clinical trials with USA patients treated with mepolizumab.
Mepolizumab’s efficacy is better with more blood eosinophils as has been shown in pivotal clinical trial extension studies (31).
Reslizumab
Exacerbation reduction has been shown in clinical trials (59, 60) although in one (60) of them was only seen in the patient subgroup with 400 blood eosinophils/µl. Improvement in FEV1, asthma control, quality of life, and pulmonary function parameters [forced vital capacity (FVC) and forced mid-expiratory flow (FEF25–75)] have been shown in clinical trials (59, 61).
Benralizumab
Clinical trials’ primary endpoints have demonstrated exacerbations reduction (62, 63) in patients with ≥300 eosinophils/µl, FEV1 improvement (64, 65), and OCS dose reduction (66).
Clinical trials’ secondary endpoints have shown asthma control (62, 63) and quality of life (67) improvement.
Dupilumab
Exacerbations reduction (36, 38) and OCS dose reduction (35) have been shown in clinical trials’ primary endpoints.
Clinical trials’ secondary endpoints have shown FEV1, asthma control, and quality of life improvement (36, 38, 69).
Exacerbation reduction and FEV1 improvement are greater in dupilumab patients treated with ≥300 blood eosinophils/µl and FeNO ≥ 25ppb (70).
Tezepelumab
Exacerbation reduction (38, 71) in patients with >300 blood eosinophils/µl (38) has been shown in clinical trials’ primary outcome and FEV1 and quality of life improvement (38, 71) in clinical trials’ secondary endpoints. Exacerbation reduction has been shown in patients without eosinophilia, in clinical trials, so it could be indicated in low T2 USA.
MA impact in frequent comorbidities in asthma patients
Omalizumab
Omalizumab’s efficacy in chronic rhinosinusitis with nasal polyps (72) was evaluated in two phase 3 clinical trials that showed endoscopic and nasal congestion improvement. It is also indicated in chronic urticaria with proven efficacy (73–76) (Table 2).
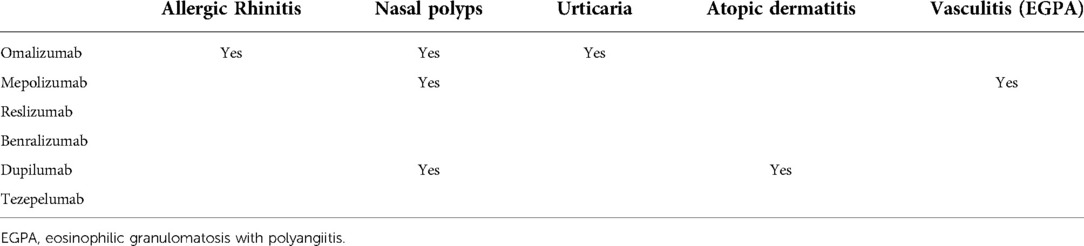
Table 2. Monoclonal antibodies’ efficacy in different comorbidities.
Asthma patients with allergic rhinitis treated with immunotherapy have fewer systemic reactions and more probability to obtain the maintenance dose with omalizumab (76).
Mepolizumab
A clinical trial (77) that included patients with nasal polyps refractory to medical and surgical treatment showed polyp endoscopic reduction, nasal obstruction, and symptom improvement with mepolizumab.
Mepolizumab’s efficacy is also proven in eosinophilic granulomatosis with polyangiitis (EGPA) (78) and hypereosinophilic syndrome (79).
Reslizumab
No clinical trials are available on efficacy in comorbidities but an open-label study showed its efficacy in reducing OCS in EGPA.
Benralizumab
Benralizumab reduces nasal obstruction and improves smell, compared with placebo, with little impact on the quality of life in patients with nasal polyps (80).
There are few case reports about benralizumab’s use in EGPA.
Dupilumab
Dupilumab has shown its efficacy in severe atopic dermatitis (81) and was first approved with this indication.
Three clinical trials (82) have shown dupilumab’s efficacy in patients with chronic rhinosinusitis with nasal polyps in reducing polyps' size, and improving symptoms and quality of life, mainly in those patients with asthma.
Other factors that can influence MA choice
Treatment aims
Therapeutic goals with MA could be different from a clinical point of view. The main objective used to be exacerbation reduction (all MA have shown their efficacy in this aspect) but other goals could be asthma control or pulmonary function improvement or reduction/withdrawal of OCS.
Symptoms control
Dupilumab (36, 38) is the MA that best controls symptoms in clinical trials. Although, extension and real-world studies have shown an improvement with all MA measured by questionnaires (83, 84).
Pulmonary function
Benralizumab, reslizumab and dupilumab showed greater improvement in pulmonary function in clinical trials (36, 59, 64, 65, 68).
OCS reduction
Not all the MA have shown their efficacy in reducing/withdrawing OCS. Mepolizumab, benralizumab and dupilumab have shown their efficacy in this aspect in clinical trials and real-world studies (36, 57, 58, 66).
Possible AE
No remarkable AE has been described with any MA except injection site reactions, headache and general malaise. Dupilumab can produce transitory peripheral eosinophilia (69) (4%–13%).
Patient’s age
Mepolizumab is indicated in USA patients ≥6 years old, dupilumab ≥12 years old, benralizumab and reslizumab ≥18 years old.
Patients’ choice
Patients’ choice (85) always must be considered taking into account administration frequency, route of administration, and AE.
Pregnancy
Omalizumab (86) is the only MA with studies that showed no complications during pregnancy.
Algorithm to choose the best MA in a specific patient
Once the MA indication is done, after we have proven that uncontrolled asthma or OCS need is due to disease severity (20, 21), we have to identify if the patient has an allergic or late-onset eosinophilic asthma because many MA can be used in both cases, and sometimes they can be overlapped, which make more difficult the MA choice.
We propose an algorithm for the MA choice considering clinical characteristics and biomarkers in a specific patient (Figure 1).
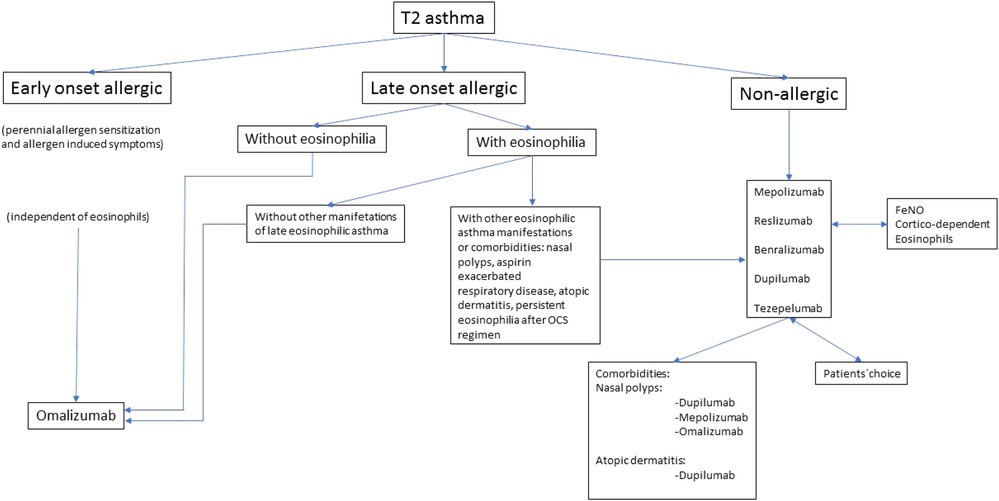
Figure 1. Algorithm to choose a monoclonal antibody.
In clinical practice, we will find scenarios where the choice of the MA will be easy. In an early onset allergic USA patient, independently of blood eosinophil count, omalizumab will be the first choice while in a late onset non-allergic USA patient with eosinophilia, an anti-IL5/IL5Rα, or dupilumab will be considered.
In early-onset allergic asthma with eosinophilia could be used an anti-IL5/IL5Rα, dupilumab or tezepelumab, but the main reason to choose in first place omalizumab is more years of experience. Early onset and allergy-induced symptoms predict a good response to omalizumab (87).
In our opinion, in late-onset allergic asthma patients (with perennial allergen sensitization and associated symptoms) without eosinophilia, omalizumab is the MA of choice. Although, tezepelumab could be considered.
In late-onset allergic USA patients with eosinophilia, the choice is more difficult. In this case, we must evaluate which factor have more impact on asthma control: allergy or eosinophilia. If no other late-onset eosinophilic manifestations are present, omalizumab is the MA of choice. When other eosinophilic asthma manifestations exist (nasal polyps, aspirin-exacerbated respiratory disease [AERD], atopic dermatitis or if eosinophilia persists after a short term of OCS) (88), anti IL5/IL5Rα or dupilumab would be recommended.
In non-allergic asthma, omalizumab is not indicated, while an anti-IL5/IL5Rα, dupilumab, or tezepelumab could be considered. No head-to-head studies are available, so we must consider the response predictor factors evaluated in clinical trials, meta-analysis, post hoc and real-world studies. In many cases, it will not be possible to make a high recommendation for a specific MA but different factors, described previously in this article, such as blood eosinophil count, FeNO, OCS use and comorbidities should be considered in the choice of the best MA.
Another factor to be considered is the patient’s age. Mepolizumab is indicated in USA patients ≥6 years old, dupilumab ≥12 years old, benralizumab and reslizumab ≥18 years old.
Local availability is another factor to consider. In some communities and hospitals, all the MA are not available.
Patient’s choice is the most important factor in many cases once MA’s frequency, route of administration, self-administration possibility and AE are explained.
Data from clinical trials and real-world studies showed that many patients had a good response to MA. But a good response is not always obtained, so a close follow-up must be performed mainly looking for exacerbations reduction, OCS reduction/withdrawal, symptoms, and pulmonary function improvement. A tool that combines all these parameters have been proposed (89) and may be of interest in clinical practice. If a good response is not obtained, a MA switch is recommended, but previously other causes of non-response must be ruled out such as poor adherence to ICS.
Discussion
Monoclonal antibodies’ efficacy indicated in T2 USA has been demonstrated in clinical trials. Real-world studies’ results corroborated, even improved, them. But no head-to-head MA comparisons are available so evidence-based MA’s choice is not possible.
Clinical trials have similarities and differences that can be helpful in MA’s choice, but with poor evidence as they included different populations and used different methodologies.
Considering all these aspects, MA’s choice must take into account the different biomarkers available and patients’ characteristics.
USA included late-onset allergic and eosinophilic asthma with different mechanisms and different therapeutic targets. The first step in MA’s choice is to know the patient’s type of T2 severe asthma but sometimes it is difficult because there is an overlap of the two subtypes.
Clinical practice guidelines (19–21) and experts’ opinions (18, 83, 84, 88, 90) proposed algorithms to choose MA based on biomarkers mainly FeNO and blood or sputum eosinophil count. The algorithm we propose in this article tries to guide the MA election in each case as we do in clinical practice. Sometimes the MA election will not be the best and we will have to switch the MA.
The first step in our algorithm is to classify the patient according to the age of asthma onset and allergy presence, then eosinophilia presence must be considered.
Omalizumab would be indicated in early and late-onset allergic asthma without eosinophilia (although other MA could be chosen) mainly based on years of experience compared with other MA.
Late-onset allergic asthma with eosinophilia, represents the T2 subtypes overlap. In this case must be considered the factor that mainly influences asthma control (allergy presence or eosinophilia) evaluating the presence of other characteristics or comorbidities of late-onset eosinophilic asthma such as nasal polyps, atopic dermatitis, aspirin-exacerbated respiratory disease. Omalizumab would be indicated if these characteristics are not present but if they are, MA for eosinophilic asthma would be considered. Oishi et al. (88) proposed in overlapped patients (allergic and eosinophilic) to indicate a short OCS regimen and evaluate eosinophil response. If eosinophils disappeared, allergy probably would be the most important factor, and omalizumab would be indicated.
MA election in USA non-allergic T2 is a multifactorial process based on biomarkers, steroid dependence, and comorbidities. In our opinion, in clinical practice, generally is easy to choose a MA. Other factors to consider are MA availability and patients' preferences.
The main weakness of the algorithm we propose is that is based in our opinion and clinical experience as no head-to-head MA comparisons are available.
In conclusion, in USA is important to choose the best MA in each patient although sometimes is difficult as no direct comparisons are available and all recommendations are based on experts' opinions. MA election must be based on multiple factors including patients’ preferences.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
ALV, CM, RDC and AT contributed to conception and design of the study and wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. (2014) 43:343–73. doi: 10.1183/09031936.00202013
2. Hekking P-PW, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. (2015) 135:896–902. doi: 10.1016/j.jaci.2014.08.042
3. Melero Moreno C, Quirce S, Huerta A, Uría E, Cuesta M. Economic impact of severe asthma in Spain: multicentre observational longitudinal study. J Asthma. (2019 Aug) 56(8):861–71. doi: 10.1080/02770903.2018.1499035
4. Kerkhof M, Tran TN, Soriano JB, Golam S, Gibson D, Hillyer EV, Price DB. Healthcare resource use and costs of severe, uncontrolled eosinophilic asthma in the UK general population. Thorax 2018;73:116–24. doi: 10.1136/thoraxjnl-2017-210531
5. Zazzali JL, Broder MS, Omachi TA, Chang E, Sun GH, Raimundo K. Risk of corticosteroid-related adverse events in asthma patients with high oral corticosteroid use. Allergy Asthma Proc. (2015) 36:268–74. doi: 10.2500/aap.2015.36.3863
6. Sullivan PW, Ghushchyan VH, Globe G, Schatz MJ. Oral corticosteroid exposure and adverse effects in asthmatic patients. Allergy Clin Immunol. (2018) 141:110–6. doi: 10.1016/j.jaci.2017.04.009
7. Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med. (2012) 18:716–25. doi: 10.1038/nm.2678
8. Woodruff PG, Modrek B, Choy DF, Jia G, Abbas AR, Ellwanger A, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med. (2009) 180:388–95. doi: 10.1164/rccm.200903-0392OC
9. Fahy JV. Type 2 inflammation in asthma–present in most, absent in many. Nat Rev Immunol. (2015) 15:57–65. doi: 10.1038/nri3786
10. Lambrecht BN, Hammad H, Fahy JV. Immunity. Cytokines Asthma. (2019) 50:975–91. doi: 10.1016/j.immuni.2019.03.018
11. Lötvall J, Akdis CA, Bacharier LB, Bjermer L, Casale TB, Custovic A, et al. Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. J Allergy Clin Immunol. (2011) 127:355–60. doi: 10.1016/j.jaci.2010.11.037
12. Kaur R, Chupp GJ. Phenotypes and endotypes of adult asthma: moving toward precision medicine. Allergy Clin Immunol. (2019) 144:1–12. doi: 10.1016/j.jaci.2019.05.031
13. Peebles RS Jr, Aronica MA. Proinflammatory pathways in the pathogenesis of asthma. Clin Chest Med. (2019) 40:29–50. doi: 10.1016/j.ccm.2018.10.014
14. Israel E, Reddel HKN. Severe and difficult-to-treat asthma in adults. Engl J Med. (2017) 377:965–76. doi: 10.1056/NEJMra1608969
15. Parulekar AD, Diamant Z, Hanania NA. Role of T2 inflammation biomarkers in severe asthma. Curr Opin Pulm Med. (2016) 22:59–68. doi: 10.1097/MCP.0000000000000231
16. Godar M, Blanchetot C, de Haard H, Lambrecht BN, Brusselle G. Personalized medicine with biologics for severe type 2 asthma: current status and future prospects. MAbs. (2018) 10:34–45. doi: 10.1080/19420862.2017.1392425
17. Cirandi G, Tosca MA, Silvestri M, Ricciardolo LM. Inflammatory biomarkers in asthma endotypes and consequent personalized therapy. Expert Rev Clin Inmunol. (2017) 13:715–21. doi: 10.1080/1744666X.2017.1313117
18. Runnstrom M, Pitner H, Xu J, Lee FE, Kuruvilla M. Utilizing predictive inflammatory markers for guiding the use of biologicals in severe asthma. J Inflamm Res. (2022) 15:241–9. doi: 10.2147/JIR.S269297
19. Álvarez-Gutiérrez FJ, Blanco-Aparicio M, Plaza V, Cisneros C, García-Rivero JL, Padilla A, et al. Documento de consenso de asma grave en adultos. Actualización 2020. Open Respir Arch. (2020) 2:158–74. doi: 10.1016/j.opresp.2020.03.005
20. Adolescents and adults with difficult-to-treat and severe asthma © GINA 2021 www.ginasthma.org
22. Fitzpatrick AM, Chipps BE, Holguin F, Fitzpatrick AM, Chipps BE, Holguin F, Woodruff PG. T2-”Low” asthma: overview and management strategies. J Allergy Clin Immunol Pract. (2020) 8:452–63. doi: 10.1016/j.jaip.2019.11.006
23. Brusselle GG, Koppelman GH. N biologic therapies for severe asthma. Engl J Med. (2022) 386:157–71. doi: 10.1056/NEJMra2032506
24. Cockle SM, Stynes G, Gunsoy NB, Parks D, Alfonso-Cristancho R, Wex J, et al. Comparative effectiveness of mepolizumab and omalizumab in severe asthma: an indirect treatment comparison. Respir Med. (2017) 123:140–8. doi: 10.1016/j.rmed.2016.12.009
25. Iftikhar IH, Schimmel M, Bender W, Swenson C, Amrol D. Comparative efficacy of anti IL-4, IL-5 and IL-13 drugs for treatment of eosinophilic asthma: a network meta-analysis. Lung. (2018) 196:517–30. doi: 10.1007/s00408-018-0151-5
26. Bourdin A, Husereau D, Molinari N, Golam S, Siddiqui Mohd K, Lindner L, et al. Matching-adjusted indirect comparison of benralizumab versus interleukin-5 inhibitors for the treatment of severe asthma: a systematic review. Eur Respir J. (2018) 52:1801393. doi: 10.1183/13993003.01393-2018
27. Busse W, Chupp G, Nagase H, Albers FC, Doyle S, Shen Q, et al. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: indirect treatment comparison. J Allergy Clin Immunol. (2019) 143:190–200. e20. doi: 10.1016/j.jaci.2018.08.031
28. Bateman ED, Khan AH, Xu Y, Guyot P, Chao J, Kamat S, et al. Pairwise indirect treatment comparison of dupilumab versus other biologics in patients with uncontrolled persistent asthma. Respir Med. (2022) 191:105991. doi: 10.1016/j.rmed.2020.105991
29. Corren J, Du E, Gubbi A, Vanlandinham R. Variability in blood eosinophil counts in patients with eosinophilic asthma. J Allergy Clin Immunol Pract. (2021) 9:1224–31. doi: 10.1016/j.jaip.2020.10.033
30. Ortega H, Gleich G, Mayer B, Yancey S. Reproducibility of a single blood eosinophil measurement as a biomarker in severe eosinophilic asthma. Ann Am Thorac Soc. (2015) 12:1896–7. doi: 10.1513/AnnalsATS.201507-443LE
31. Ortega HG, Yancey SW, Mayer B, Gunsoy NB, Keene ON, Bleecker ER, et al. Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: a secondary analysis of the DREAM and MENSA studies. Lancet Respir Med. (2016) 4:549–56. doi: 10.1016/S2213-2600(16)30031-5
32. Albers FC, Licskai C, Chanez P, Bratton D, Bradford ES, Yaney SW, et al. Baseline blood eosinophil count as a predictor of treatment response to the licensed dose of mepolizumab in severe eosinophilic asthma. Respir Med. (2019) 159:105806. doi: 10.1016/j.rmed.2019.105806
33. Corren J, Weinstein S, Janka L, Zangrilli J, Garin M. Phase 3 study of reslizumab in patients with poorly controlled asthma: effects across a broad range of eosinophil counts. Chest. (2016) 150:799–810. doi: 10.1016/j.chest.2016.03.018
34. Bleecker ER, Wechsler ME, FitzGerald JM, Menzies-Gow A, Wu Y, Hirsch I, et al. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. Eur Respir J. (2018) 52:1800936. doi: 10.1183/13993003.00936-2018
35. Rabe KF, Nair P, Brusselle G, Maspero J, Castro M, Sher L, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. (2018) 378:2475–85. doi: 10.1056/NEJMoa1804093
36. Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. (2018) 378:2486–96. doi: 10.1056/NEJMoa1804092
37. Hanania NA, Wenzel S, Rosén K, Hsieh H-J, Mosesova S, Choy D, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med. (2013) 187:804–11. doi: 10.1164/rccm.201208-1414OC
38. Menzies-Gow A, Corren J, Bourdin A, Chupp G, Israel E, Wechsler ME, et al. Tezepelumab in adults and adolescents with severe, uncontrolled asthma. N Engl J Med. (2021) 13(384):1800–9. doi: 10.1056/NEJMoa2034975
39. Denlinger LC, Phillips BR, Ramratnam S, Ross K, Bhakta NR, Cardet JC, et al. Inflammatory and comorbid features of patients with severe asthma and frequent exacerbations. Am J Respir Crit Care Med. (2017) 195:302–13. doi: 10.1164/rccm.201602-0419OC
40. Katz LE, Gleich GJ, Hartley BF, Yancey SW, Ortega HG. Blood eosinophil count is a useful biomarker to identify patients with severe eosinophilic asthma. Ann Am Thorac Soc. (2014) 11(4):531–6. doi: 10.1513/AnnalsATS.201310-354OC
41. Mukherjee M, Aleman Paramo F, Kjarsgaard M, Salter B, Nair G, Nicola LaVigne N, et al. Weight-adjusted intravenous reslizumab in severe asthma with inadequate response to fixed-dose subcutaneous mepolizumab. Am J Respir Crit Care Med. (2018) 197:38–46. doi: 10.1164/rccm.201707-1323OC
42. Beeh KM, Ksoll M, Buhl R. Elevation of total serum immunoglobulin E is associated with asthma in nonallergic individuals. Eur Respir J. (2000) 16:609–14. doi: 10.1034/j.1399-3003.2000.16d07.x
43. Bousquet J, Cabrera P, Berkman N, Buhl R, Holgate S, Wenzel S, et al. The effect of treatment with omalizumab, an anti-IgE antibody, on asthma exacerbations and emergency medical visits in patients with severe persistent asthma. Allergy. (2005) 60:302–8. doi: 10.1111/j.1398-9995.2004.00770.x
44. Corren J, Castro M, O’Riordan T, Hanania NA, Pavord ID, Quirce S, et al. Dupilumab efficacy in patients with uncontrolled, moderate-to-severe allergic asthma. J Allergy Clin Immunol Pract. (2020) 8:516–26. doi: 10.1016/j.jaip.2019.08.050
45. Izuhara K, Ohta S, Ono J. Using periostin as a biomarker in the treatment of asthma. Allergy Asthma Immunol Res. (2016) 8:491–8. doi: 10.4168/aair.2016.8.6.491
46. Humbert M, Beasley R, Ayres J, Slavin R, Hébert J, Bousquet J, et al. Benefits of omalizumab as add-on therapy in patients with severe persistent asthma who are inadequately controlled despite best available therapy (GINA 2002 step 4 treatment): iNNOVATE. Allergy. (2005) 60:309–16. doi: 10.1111/j.1398-9995.2004.00772.x
47. Busse W, Corren J, Lanier BQ, McAlary M, Fowler-Taylor A, Cioppa GD, et al. Omalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthma. J Allergy Clin Immunol. (2001) 108:184–90. 114. doi: 10.1067/mai.2001.117880
48. Soler M, Matz J, Townley R, Buhl R, O'Brien J, Fox H, et al. The anti-IgE antibody omalizumab reduces exacerbations and steroid requirement in allergic asthmatics. Eur Respir J. (2001) 18:254–61. 115. doi: 10.1183/09031936.01.00092101
49. Holgate S, Chuchalin A, Hebert J, Lötvall J, Persson GB, Chung KF, et al. Efficacy and safety of a recombinant anti-immunoglobulin E antibody (omalizumab) in severe allergic asthma. Clin Exp Allergy. (2004) 34:632–8. 116. doi: 10.1111/j.1365-2222.2004.1916.x
50. Vignola A, Humbert M, Bousquet J, Boulet LP, Hedgecock S, Blogg M, et al. Efficacy and tolerability of anti-immunoglobulin E therapy with omalizumab in patients with concomitant allergic asthma and persistent allergic rhinitis: sOLAR. Allergy. (2004) 59:709–17. doi: 10.1111/j.1398-9995.2004.00550.x
51. Normansell R, Walker S, Milan SJ, Walters EH, Nair P. Omalizumab for asthma in adults and children. Cochrane Database Syst Rev. (2014) 1:CD003559. doi: 10.1002/14651858.CD003559.pub4
52. Alhossan A, Lee CS, MacDonald K, Abraham I. “Real-life” effectiveness studies of omalizumab in adult patients with severe allergic asthma: metaanalysis. J Allergy Clin Immunol Pract. (2017) 5:1362–70. 125. doi: 10.1016/j.jaip.2017.02.002
53. Bousquet J, Humbert M, Gibson PG, Kostikas K, Jaumont X, Pfister P, et al. Real-world effectiveness of omalizumab in severe allergic asthma: a meta-analysis of observational studies. J Allergy Clin Immunol Pract. (2021) 9:2702–14. doi: 10.1016/j.jaip.2021.01.011
54. Haldar P, Brightling CE, Hargadon B, Gupta S, Monteiro W, Sousa A, et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med. (2009) 360:973–84. 41. doi: 10.1056/NEJMoa0808991
55. Pavord ID, Korn S, Howarth P, Bleecker ER, Buhl R, Keene ON, et al. Mepolizumab for severe eosinophilic asthma (DREAM): a multicentre, double-blind, placebo-controlled trial. Lancet. (2012) 380:651–9. doi: 10.1016/S0140-6736(12)60988-X
56. Ortega HG, Liu MC, Pavord ID, Brusselle GG, FitzGerald JM, Chetta A, et al. MENSA Investigators. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. (2014) 371:1198–207. doi: 10.1056/NEJMoa1403290
57. Nair P, Pizzichini MM, Kjarsgaard M, Inman MD, Efthimiadis A, Pizzichini E, et al. Mepolizumab for prednisone-dependent asthma with sputum eosinophilia. N Engl J Med. (2009) 360:985–93. 42. doi: 10.1056/NEJMoa0805435
58. Bel EH, Wenzel SE, Thompson PJ, Prazma CM, Keene ON, Yancey SW, et al. SIRIUS Investigators. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N Engl J Med. (2014) 371:1189–97. doi: 10.1056/NEJMoa1403291
59. Castro M, Zangrilli J, Wechsler ME, Bateman ED, Brusselle GG, Bardin P, et al. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir Med. (2015) 3:355–66. doi: 10.1016/S2213-2600(15)00042-9
60. Bernstein JA, Virchow JC, Murphy K, Maspero JF, Jacobs J, Adir Y, et al. Effect of fixed-dose subcutaneous reslizumab on asthma exacerbations in patients with severe uncontrolled asthma and corticosteroid sparing in patients with oral corticosteroid-dependent asthma: results from two phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir Med. (2020) 8:461–74. doi: 10.1016/S2213-2600(19)30372-8
61. Bjermer L, Lemiere C, Maspero J, Weiss S, Zangrilli J, Germinaro M. Reslizumab for inadequately controlled asthma with elevated blood eosinophil levels: a randomized phase 3 study. Chest. (2016) 150:789–98. doi: 10.1016/j.chest.2016.03.032
62. Bleecker ER, FitzGerald JM, Chanez P, Papi A, Weinstein SF, Barker P, et al.; SIROCCO study investigators. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting b2-agonists (SIROCCO): a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. (2016) 388:2115–27. 54. doi: 10.1016/S0140-6736(16)31324-1
63. FitzGerald JM, Bleecker ER, Nair P, Korn S, Ohta K, Lommatzsch M, et al.; CALIMA study investigators. Benralizumab, an antiinterleukin-5 receptor a monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. (2016) 388:2128–41. 55. doi: 10.1016/S0140-6736(16)31322-8
64. Ferguson GT, FitzGerald JM, Bleecker ER, Laviolette M, Bernstein D, LaForce C, et al. Benralizumab for patients with mild to moderate, persistent asthma (BISE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. (2017) 5:568–76. doi: 10.1016/S2213-2600(17)30190-X
65. Panettieri RA, Welte T, Shenoy KV, Korn S, Jandl M, Kerwin EM, et al. Onset of effect, changes in airflow obstruction and lung volume, and health-related quality of life improvements with benralizumab for patients with severe eosinophilic asthma: phase IIIb randomized, controlled trial (SOLANA). J Asthma Allergy. (2020) 13:115–26. doi: 10.2147/JAA.S240044
66. Nair P, Wenzel S, Rabe KF, Bourdin A, Lugogo NL, Kuna P, et al. ZONDA Trial investigators. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. (2017) 376:2448–58. doi: 10.1056/NEJMoa1703501
67. Harrison TW, Chanez P, Menzella F, Canonica GW, Louis R, Cosio BG, et al. Onset of effect and impact on health-related quality of life, exacerbation rate, lung function, and nasal polyposis symptoms for patients with severe eosinophilic asthma treated with benralizumab (ANDHI): a randomised, controlled, phase 3b trial. Lancet Respir Med. (2021) 9:260–74. doi: 10.1016/S2213-2600(20)30414-8
68. Wenzel S, Ford L, Pearlman D, Spector S, Sher L, Skobieranda F, et al. Dupilumab in persistent asthma with elevated eosinophil levels. N Engl J Med. (2013) 368:2455–66. doi: 10.1056/NEJMoa1304048
69. Wenzel S, Castro M, Corren J, Maspero J, Wang L, Zhang B, et al. Dupilumab efficacy and safety in adults with uncontrolled persistent asthma despite use of medium-to-high-dose inhaled corticosteroids plus a long-acting β2 agonist: a randomised double-blind placebo-controlled pivotal phase 2b dose-ranging trial. Lancet. (2016) 388(10039):31–44. doi: 10.1016/S0140-6736(16)30307-5
70. Bacharier LB, Maspero JF, Katelaris CH, Fiocchi AG, Gagnon R, de Mir I, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. Engl J Med. (2021) 385(24):2230–40. doi: 10.1056/NEJMoa2106567
71. Corren J, Parnes JR, Wang L, Mo M, Roseti SL, Griffiths JM, et al. Tezepelumab in adults with uncontrolled asthma. N Engl J Med. (2017) 377(10):936–46. doi: 10.1056/NEJMoa1704064
72. Gevaert P, Omachi TA, Corren J, Mullol J, Han J, Lee SE, et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. Allergy Clin Immunol. (2020) 146:595–605. doi: 10.1016/j.jaci.2020.05.032
73. Kaplan A, Ledford D, Ashby M, Canvin J, Zazzali JL, Conner E, et al. Omalizumab in patients with symptomatic chronic idiopathic/spontaneous urticaria despite standard combination therapy. J Allergy Clin Immunol. (2013) 132:101–9. doi: 10.1016/j.jaci.2013.05.013
74. Maurer M, Rosen K, Hsieh HJ, Saini S, Grattan C, Gimenez-Arnau A, et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria. N Engl J Med. (2013) 368:924–35. doi: 10.1056/NEJMoa1215372
75. Saini SS, Bindslev-Jensen C, Maurer M, Grob JJ, Bulbul Baskan E, Bradley MS, et al. Efficacy and safety of omalizumab in patients with chronic idiopathic/spontaneous urticaria who remain symptomatic on h1 antihistamines: a randomized, placebo controlled study. J Invest Dermatol. (2015) 135:67–75. doi: 10.1038/jid.2014.306
76. Kuehr J, Brauburger J, Zielen S, Schauer U, Kamin W, Von Berg A, et al. Efficacy of combination treatment with anti-IgE plus specific immunotherapy in polysensitized children and adolescents with seasonal allergic rinitis. J Allergy Clin Immunol. (2002) 109:274–80. doi: 10.1067/mai.2002.121949
77. Han JK, Bachert C, Fokkens W, Desrosiers M, Wagenmann M, Lee SE, et al. Mepolizumab for chronic rhinosinusitis with nasal polyps (SYNAPSE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Respir Med. (2021) 9:1141–53. doi: 10.1016/S2213-2600(21)00097-7
78. Wechsler ME, Akuthota P, Jayne D, Khoury P, Klion A, Langford CA, et al. Mepolizumab or placebo for eosinophilic granulomatosis with polyangiitis. N Engl J Med. (2017) 376:1921–32. doi: 10.1056/NEJMoa1702079
79. Roufosse F, Kahn JE, Rothenberg ME, Wardlaw AJ, Klion AD, Kirby SY, et al. Efficacy and safety of mepolizumab in hypereosinophilic syndrome: a phase III, randomized, placebo-controlled trial. J Allergy Clin Immunol. (2020) 146:1397–405. doi: 10.1016/j.jaci.2020.08.037
80. Bachert C, Han JK, Desrosiers MY, Gevaert P, Heffler E, Hopkins C, et al. Efficacy and safety of benralizumab in chronic rhinosinusitis with nasal polyps: a randomized, placebo-controlled trial. J Allergy Clin Immunol. (2022) 149:1309–17. doi: 10.1016/j.jaci.2021.08.030
81. Simpson EL, Bieber T, Guttman-Yassky E, Beck LA, Blauvelt A, Cork MJ, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. (2016) 375:2335–48. doi: 10.1056/NEJMoa1610020
82. Bachert C, Han JK, Desrosiers M, Wagenmann M, Lee SE, Smith SG, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet. (2019) 394:1638–50. doi: 10.1016/S0140-6736(19)31881-1
83. Brusselle GG, Koppelman GHN. Biologic therapies for severe asthma. Engl J Med. (2022) 386:157–71. doi: 10.1056/NEJMra2032506
84. Pavord ID, Hanania NA, Corren JJ. Controversies in allergy: choosing a biologic for patients with severe asthma. Allergy Clin Immunol Pract. (2022) 10:410–9. doi: 10.1016/j.jaip.2021.12.014
85. Bukstein DA Jr, Guerra DG. Severe asthma and biologics: data are good, listening to patients is better. Ann Allergy Asthma Immunol. (2021) 127:285–6. doi: 10.1016/j.anai.2021.05.017
86. Namazy JA, Blais L, Andrews EB, Scheuerle AE, Cabana MD, Thorp JM, et al. Pregnancy outcomes in the omalizumab pregnancy registry and a disease-matched comparator cohort. J Allergy Clin Immunol. (2020) 145:528–36. doi: 10.1016/j.jaci.2019.05.019
87. Kavanagh JE, Hearn AP, Jackson DJ. A pragmatic guide to choosing biologic therapies in severe asthma. Breathe (Sheff). (2021) 17(4):210144. doi: 10.1183/20734735.0144-2021
88. Oishi K, Matsunaga K. Three-step algorithm for biological therapy targeted IgE and IL-5 in severe asthma. ImmunInflamm Dis. (2018) 6:374–6. doi: 10.1002/iid3.233
89. Pérez de Llano L, Dávila I, Martínez-Moragón E, Domínguez-Ortega J, Almonacid C, Colás C, et al. Development of a tool to measure the clinical response to biologic therapy in uncontrolled severe asthma: the FEV1, exacerbations, oral corticosteroids, symptoms score. J Allergy Clin Immunol Pract. (2021) 9:2725–31. doi: 10.1016/j.jaip.2021.01.033
Keywords: T2 severe asthma, monoclonal antibodies, biomarkers, exacerbations, systemic corticosteroid
Citation: López-Viña A, Díaz Campos RM, Trisan Alonso A and Melero Moreno C (2022) Uncontrolled severe T2 asthma: Which biological to choose? A biomarker-based approach. Front. Allergy 3:1007593. doi: 10.3389/falgy.2022.1007593
Received: 30 July 2022; Accepted: 11 October 2022;
Published: 14 November 2022.
Edited by:
Apostolos Bossios, Karolinska University Hospital, SwedenReviewed by:
Mona Al-Ahmad, Kuwait University, Kuwait© 2022 López-Viña, Díaz Campos, Trisán Alonso and Melero Moreno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rocío M. Díaz Campos cm9jaW9tZGM4MEBnbWFpbC5jb20=
Specialty Section: This article was submitted to Asthma, a section of the journal Frontiers in Allergy