
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychiatry , 01 March 2019
Sec. Psychological Therapy and Psychosomatics
Volume 10 - 2019 | https://doi.org/10.3389/fpsyt.2019.00070
This article is part of the Research Topic Brain-Metabolic Crossroads in Severe Mental Disorders – Focus on Metabolic Syndrome View all 11 articles
 Andrea Aguglia1,2*Paola Solano1,2Gabriele Giacomini1,2Matilde Caprino1,2Claudia Conigliaro1,2Miroslav Romano3Eugenio Aguglia3Gianluca Serafini1,2Mario Amore1,2
Andrea Aguglia1,2*Paola Solano1,2Gabriele Giacomini1,2Matilde Caprino1,2Claudia Conigliaro1,2Miroslav Romano3Eugenio Aguglia3Gianluca Serafini1,2Mario Amore1,2Evidence supports the existence of an association between dyslipidemia, psychiatric disorders, and suicide risk due to the effects of altered lipid profiles on serotoninergic neuron membranes. The aim of this study was to investigate the differences in c-reactive protein (CRP), thyroid functioning, total cholesterol, high lipoprotein density cholesterol (HDL-c), low-lipoprotein density cholesterol (LDL-c), and triglycerides (TG) serum levels in low lethality (LLSA) vs. high lethality suicide attempters (HLSA) within 24 h from the suicide attempt and inpatients who never attempted suicide (NAS). After attempting suicide, subjects were admitted to the emergency ward of the IRCCS Ospedale Policlinico San Martino and later to the section of Psychiatry from 1st August 2013 to 31st July 2018. Socio-demographic and clinical characteristics, serum lipids profile, CRP, and thyroid functioning were collected. The sample consisted of 133 individuals with a HLSA, 299 subjects with LLSA, and 200 patients NAS. HLSA subjects were more likely to be males and diagnosed as having a bipolar disorder. Furthermore, HLSA subgroup showed significantly lower total cholesterol and LDL-c levels and higher CRP serum levels compared to LLSA and control group, respectively. LLSA subgroup showed higher HDL-c levels compared to HLSA subgroup (no differences between HLSA and control group were observed). Additionally, the control group reported higher triglycerides levels compared to patients admitted to psychiatric ward for a suicide attempt. Only male gender, having a diagnosis of bipolar disorder, lower total cholesterol, and higher CRP serum levels predicted HLSA. Investigating the relation between dyslipidemia and the severity of suicide attempts may contribute to reveal the complex determinants underlying at-risk behaviors such as suicide, thus playing a relevant role in the possible prevention of this disabling phenomenon.
Suicide and non-fatal suicidal behaviors are major causes of mortality and morbidity worldwide. The World Health Organization (1) estimated that ~800,000 people die from suicide each year and a number from 10 to 20 times higher of individuals attempt suicide, indicating that both suicide and non-fatal suicidal behaviors need to be addressed as a real health priority. The variability in rates of suicidal behaviors within and between countries has been attributed to both population and individual risk factors, including economic status and cultural differences (2) that may significantly affect suicide risk.
Different explanatory models were developed in order to reveal the complex interplay between neurobiological factors such as genetic risk variables, altered serotonergic functioning, and stress responses potentially leading to suicidal behaviors (3, 4). Interestingly, two major dietary lipid classes, cholesterol, and polyunsaturated fatty acids (PUFAs), were significantly associated with higher suicide risk (5, 6). Consistent with the inflammation-related hypothesis of depression and suicidal behavior, C-reactive protein (CRP) blood levels were directly associated with the enhanced risk of attempting and committing suicide (7–9), suggesting that CRP may be a trait marker of suicidal behavior due to its pro-inflammatory effect together with its growing levels during acute inflammation (10). From a genetic perspective, genome-wide association studies (GWAS) identified a region on 2p25 that influences risk for attempting suicide and contains the ACP1 gene (11, 12) and polymorphisms in ACP1 which were found to modulate both protection and predisposition to dyslipidemia (13).
The association between low total cholesterol and cholesterol metabolites serum levels with higher suicide risk has been reported since 1990, when Muldoon et al. initially showed that treatments able to reduce cholesterol levels may attenuate the excess of suicidal behaviors and injury deaths in their sample (14). These results were confirmed by a wide body of literature showing significant associations between altered lipid profiles and higher suicide risk both in patients with specific psychiatric disorders as well as in non-clinical populations (15–21). Recently, Wu et al. conducted a large meta-analysis on 65 epidemiological studies, involving 510.392 participants, and investigated the association between serum lipid levels and “suicidality” subjects defined as individuals presenting suicidal ideation, suicide attempt, having threatened suicide, or death by suicide. Their findings showed that total cholesterol (TC) and low density lipoprotein cholesterol (LDL-c) levels were lower in suicidal patients than non-suicidal patients and healthy controls, high density lipoprotein cholesterol (HDL-c) levels were lower in suicidal patients relative to healthy controls, and triglycerides (TG) levels were lower in suicidal when compared to non-suicidal patients, respectively. Importantly, when the three groups were pooled, lower serum TC was associated with a 112% higher risk of suicidal behaviors (22).
Moreover, subjects who attempted suicide within a month from the blood tests had significantly lower TG and higher HDL-c levels than lifetime suicide attempters and those who never attempted suicide, with TG levels that were negatively associated with current suicidal behavior (23). However, other studies investigating a sample of inpatients with type 1 bipolar disorder and other psychiatric conditions failed to confirm these findings reporting no significant differences in lipid profiles between suicidal and non-suicidal subjects (24–26).
Recent studies investigated the role of cholesterol levels in violent vs. non-violent suicide attempts and showed that the former was significantly associated with lower cholesterol serum levels of ~30% than the latter (27–29). Moreover, two post-mortem studies showed significantly lower cholesterol levels in the pre-frontal-cortex (PFC) of violent suicide attempters and significantly higher cholesteryl-ester-hydrolase (LIPA) expression in violent suicide attempters when compared with non-violent suicide attempters (30, 31).
Given this background, in this study we investigated the differences in CRP, thyroid functioning, TC, HDL-c, LDL-c, and TG serum levels between low-lethality (LLSA) vs. high-lethality suicide attempts (HLSA) within 24 h from the suicide attempt and inpatients who never attempted suicide (NAS).
According to this main objective, we tested the following hypothesis: (a) lower total cholesterol, HDL-c, LDL-c, and TG serum levels determine HLSA instead of LLSA and NAS; (b) CRP levels are higher in HLSA instead of LLSA and NAS.
The present study was conducted in a sample of patients who were recruited at the section of Psychiatry of the IRCCS Ospedale Policlinico San Martino—Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal, and Child Health, University of Genoa, Italy, from 1st August 2013 to 31st July 2018.
The inclusion criteria were: (a) hospitalization in an emergency psychiatric ward for a suicide attempt; (b) aged over 18 years old; (c) the willingness to participate in the study by signing a written informed consent. The exclusion criteria were: (a) pregnancy or having just given birth; (b) having a positive history of acute neurological injury, such as neurodegenerative illnesses, mental retardation, loss of consciousness related to the presence of severe neurological conditions; (c) the assumption of lipid-lowering agents; (d) the refusal or inability to provide a valid consent prior to participate in the study.
A control group was also included in the sample and it was represented by admitted patients without a history of current and/or lifetime suicide attempts. The control group was matched for age, gender, occupational/marital status, and diagnosis to avoid any bias. We initially screened a sample of 703 patients; however, only 632 subjects voluntarily accepted to participate in the study by signing a written informed consent, the remaining individuals were lost due to lack of serum data or because they did not sign the required informed consent.
The study design was reviewed and approved by the local ethic committee.
Socio-demographic and clinical characteristics of the recruited patients were investigated during hospitalization through the standardized clinical chart and lifetime computerized medical record, used in Psychiatric Unit. The following patients' domains: age, gender, marital and occupational status, education level, suicide attempts, and suicide method were carefully investigated.
All available information have been cross-referred.
Psychiatric diagnoses were evaluated and set according to Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM 5) (32). Clinical evaluations were carried out by expert clinicians and carefully reviewed by a senior psychiatrist (with at least 10 years of clinical experience in inpatient clinical setting). If patients had more than one psychiatric diagnosis, the principal psychiatric condition as diagnosed by the treating psychiatrist, was recorded. According to previous published studies (33, 34), we grouped the diagnosis in four main categories: bipolar and related disorders, depressive disorders, schizophrenia, and related disorders, other psychiatric disorders.
Based on Schrijvers et al., we considered suicide as a process, for which suicidal behaviors can be broken down chronologically into “component parts,” beginning with the development of suicidal ideation, that progresses to planning, then putting thoughts and plans into action via attempts, and, if successful, culminating in completed suicide (35).
The term “suicidal lethality” has not yet been defined outside health literature. Beyond one publication describing suicide lethality as the lethality of the chosen suicide method (36), some theorists like Shneidman and Joiner conceptually identified suicide lethality “as a key ingredient of serious suicidality” (37, 38). We adopted Joiner's definition of suicide lethality, defined as “the acquired ability to enact lethal self-injury” (38). Within suicide lethality, the only individual intent is to perish as a result of the lethality of self-inflicted actions. Methods of suicide attempt were dichotomized in terms of lethality. Therefore, a high-lethality suicide attempt was defined as a suicide attempt that warranted hospitalization for at least 24 h and either treatment in a specialized unit (including intensive care unit, hyperbaric unit, or burn unit), surgery under general anesthesia, or extensive medical treatment (beyond gastric lavage, activated charcoal, or routine neurological observations), including antidotes for drug overdoses, telemetry, or repeated tests or investigations. Conversely, a low-lethality suicide attempt was defined as a suicide attempt that did not meet these criteria (39–46).
A routine blood examination was usually performed at hospital admission for all patients as a part of the clinical management routine. Blood samples were taken between 7:00 and 8:30 a.m. after patients had fasted for at least 10 h and after a psychiatric evaluation; patients who were not fasting were rescheduled. Blood exams included TC, TG, HDL-c, LDL-c, CRP serum levels, and TSH Reflex. Blood samples were drawn during the hospitalization in the Psychiatric Clinic and examined in the laboratory analysis of IRCCS Ospedale Policlinico San Martino, Genoa, Italy.
All statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA) with the value of statistical significance which was set at p < 0.05.
Socio-demographic and clinical characteristics of the subjects were represented as mean and standard deviation (SD) for continuous variables and as frequency and percentage regarding categorical variables. The Kolmogorov-Smirnov test was conducted to confirm whether all the investigated sample variables followed the normal distribution.
Firstly, the sample was divided in two subgroups according to the presence/absence of current suicide attempt. A statistical comparison between patients with and without current suicide attempt was performed to examine whether there were differences in terms of socio-demographic and diagnostic features. Thus, in order to avoid statistical bias, the two subgroups were matched for age, gender, marital/occupational status, and psychiatric diagnoses.
Subsequently, the subgroup of patients admitted for a current suicide attempt was divided according to the lethality of suicide attempts, identifying a subgroup with high-lethality of suicide attempts and a subgroup with low-lethality of suicide attempts. In order to analyze differences between these three subgroups, we used the Pearson χ2 test with Yates correction for the comparison of categorical variables, and ANOVA for continuous variables.
Lastly, a multinomial regression model was performed to detect the variables associated with the lethality of suicide attempt (dependent variable) and each of the other independent variables previously found associated in the statistical analyses. The probability of entering the equation was set at 0.05.
In our study we recruited a total sample of 632 patients, with a mean age of 49.69 ± 18.97 years old. Of the total sample, 478 subjects were females (75.6%) with an educational level of 11.06 ± 3.28 years. Four hundred and thirty-two subjects were recruited in the case-group and 200 in the control group. There were no statistically significant differences in socio-demographic and clinical characteristics (i.e., gender, age, marital status, educational level, working status, psychiatric diagnoses and pharmacological treatment) between the subgroup of patients who attempted suicide and the subgroup of patients who never attempted suicide (control group). Socio-demographic and clinical characteristics of the included subjects are summarized in Tables 1, 2.
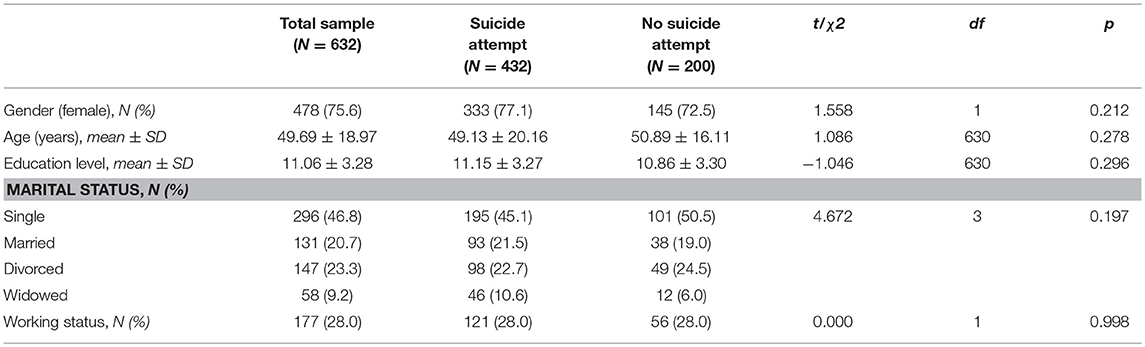
Table 1. Socio-demographic characteristics in the total sample and in the two subgroups.
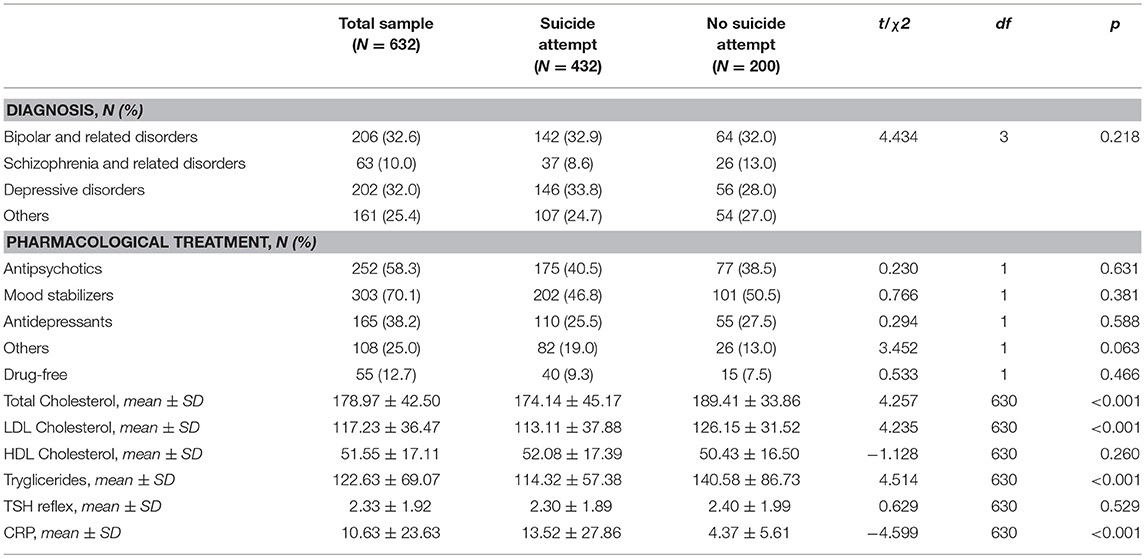
Table 2. Clinical characteristics in the total sample and in the two subgroups.
Regarding patients admitted for a suicide attempt, 133 individuals (30.8%) committed a HLSA while 299 subjects (69.2%) carried out a LLSA, respectively. The prevalence of the method used to attempt suicide is shown in Table 3.
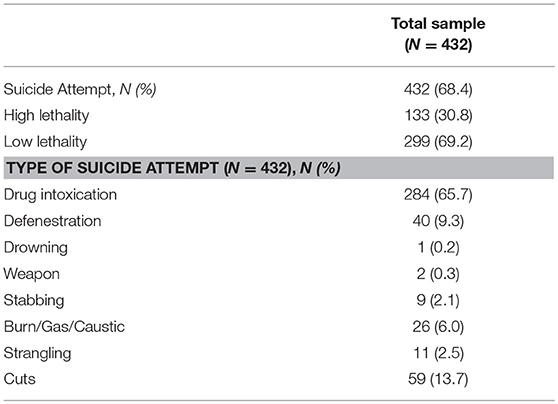
Table 3. Type of suicide according to lethality.
Considering socio-demographic and clinical features within the three subgroups, the HLSA subgroup was significantly associated with male gender (38.3 vs. 16.1 vs. 27.5%, p < 0.001) and diagnosis of bipolar disorder (41.4 vs. 29.1 vs. 32.0%, p = 0.007), compared to LLSA, and control group, respectively.
When the three subgroups were compared, the HLSA subgroup showed significantly lower total cholesterol levels (151.08 ± 40.90 vs. 184.40 ± 43.21 vs. 189.41 ± 33.88, p < 0.001) and LDL-c levels (99.55 ± 33.25 vs. 119.15 ± 38.30 vs. 126.15 ± 31.52, p < 0.001), and higher CRP serum levels (24.18 ± 38.69 vs. 8.78 ± 19.66 vs. 4.37 ± 5.61, p < 0.001) compared to LLSA and control group, respectively.
Furthermore, the LLSA subgroup showed higher HDL-c levels compared to HLSA subgroup (54.64 ± 16.59 vs. 46.31 ± 17.82, p < 0.001) (no differences between HLSA and control group were observed). Additionally, the control group reported higher triglycerides level compared to patients admitted for a suicide attempt. No differences in triglycerides levels between HLSA and LLSA were found). Additional differences are shown in Table 4.
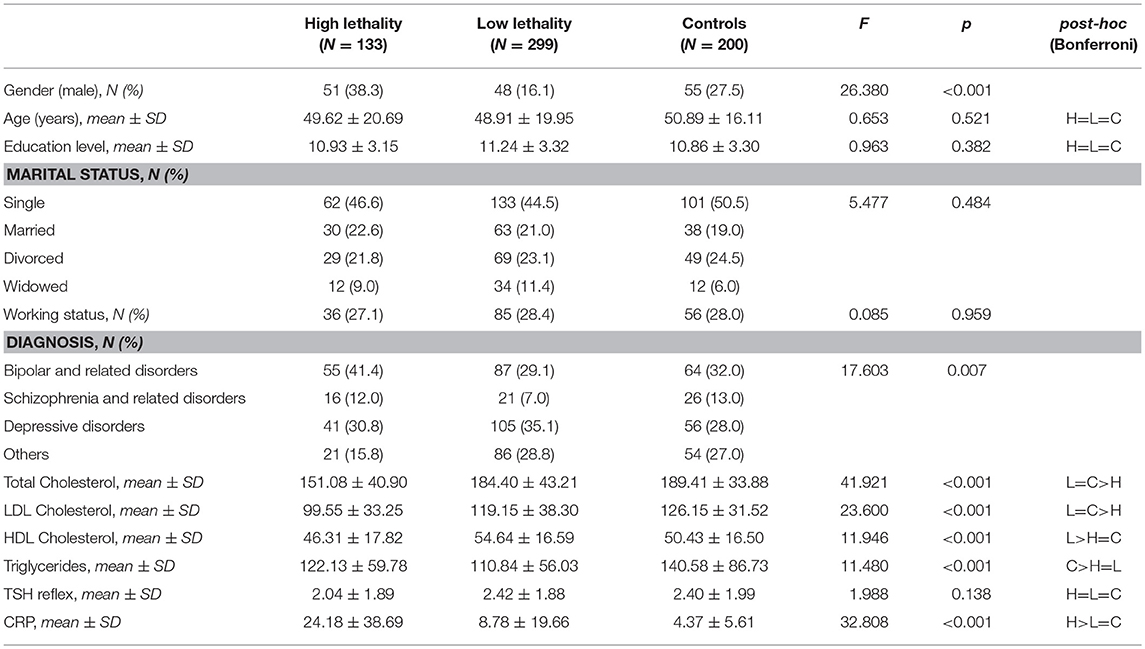
Table 4. Comparison among three subgroups according to the lethality of suicide attempt.
When the multinomial regression was performed, male gender, diagnosis of bipolar disorder, lower total cholesterol level, and higher CRP serum levels predicted HLSA (Table 5).
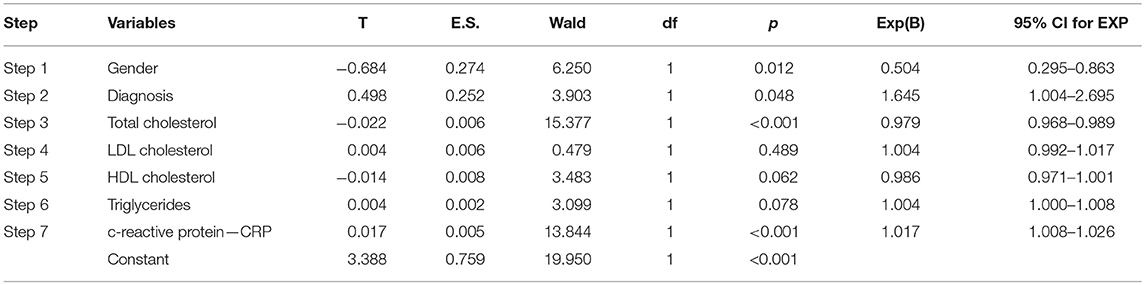
Table 5. Relationship between potential explanatory variables and lethality of suicide attempts: results from the logistic regression analysis.
The present study tested the association between lipid profile, CRP levels, and thyroid functioning in a relatively large sample of psychiatric inpatients who committed HLSA (133 subjects) vs. psychiatric inpatients who carried out LLSA (299 subjects) and a control group of psychiatric inpatients who never attempted suicide (200 subjects).
HLSA were more likely to be males and affected by bipolar disorder. This is consistent with previous findings showing that subjects with bipolar disorder presented a higher risk for attempting and committing suicide (47–49) and supported the higher lethality suicide among males irrespective from their psychiatric diagnosis (46, 49–51).
Our study showed that HLSA was clearly associated with lower total cholesterol and LDL-c, and higher CRP levels when compared with LLSA and controls. To the best of our knowledge, no previous studies investigated the association between suicide lethality and lipid profiles, though our results may be explained in the light of previous evidence showing that violent methods to attempt suicide were associated with lower total cholesterol levels (27).
The well-known cholesterol-serotonin hypothesis (52) may help to explain these results as lower total cholesterol levels may foster higher central neuroinflammation, thus altering the serotonergic system and leading to higher aggressiveness and impulsivity, especially among males (53). In the central nervous system, serotonin plays a role in the suppression of aggressive and harmful behaviors. There are several theories that may explain the potential effect of serum lipid profile (in particular cholesterol levels) on violent conduct and suicide risk. The most blamed mechanism is the reduction of brain serotonergic activity which is associated with the risk of attempting suicide. It has been hypothesized that cholesterol levels are associated with the lipid micro viscosity of serotonin receptors and transporters. Since reliable evidence shows that circulating levels of cholesterol—those that may be detected by routine blood tests as those used on the patients in the study—correlate with the role of stabilizer of cellular membrane functioning (6), and membrane cholesterol exchanges freely with cholesterol in the surrounding medium, low membrane cholesterol decreases the number of serotonergic receptors through the decreased lipid micro viscosity of the serotonergic receptor on the neuronal membrane (53, 54). This process could lead to a poorer suppression of impulsive and violent behaviors, such as suicidal behaviors (54). As a matter of fact, cholesterol is crucial for membrane stability and neurotransmission that include the alteration of membrane lipid raft structure by the proportions of cholesterol and n-3 PUFAs, affecting the functioning of membrane-bound proteins including serotonin receptors and transporters, and toll-like receptors (6, 55). Therefore, low levels of cholesterol might be responsible of increased n-6:n-3 PUFA ratio, thereby promoting neuroinflammation as n-3 PUFAs tend to exert anti-inflammatory properties, while n-6 PUFAs levels tend to show a pro-inflammatory activity, and disinhibit, albeit indirectly, two inflammatory intermediates such as nuclear factor kappa-light-chain-enhancer of activated B cells (NFκB) and peroxisome proliferator activated receptors (PPARs), respectively (56). The abnormal monoaminergic neurotransmission as well as neuroinflammation are two leading mechanisms which are evoked as biological pathways underlying suicidal behavior (6, 9, 55). Lower cholesterol levels are associated with greater impulsivity of suicide attempts and violent methods due to their effects on the serotonergic system. Indirect evidence suggests an association between attempt lethality and low-cholesterol levels on the basis of the relation between lethality and the choice of violent methods to attempt suicide (29).
Although, to the best of our knowledge, no studies investigated directly the association between CRP, cholesterol, and cholesterol metabolites serum levels and lethality of suicide attempts, interestingly, a recent study hypothesized a bridge between the well-known cholesterol metabolism process with its associated molecular pathways and the neurobiological underpinnings of suicide risk, by showing that the relation between total unesterified cholesterol and suicide risk was significantly mediated by ABCA-1-specific cholesterol efflux capacity (57).
Conversely, our results show no differences in total cholesterol and LDL-c levels between LLSA and controls, although ANOVA did not confirm these findings. The lack of differences concerning lipid profiles of LLSA and controls could be explained in the light of the method lethality used to attempt suicide. For instance, Lalovic et al. (30) reported no significant differences in cholesterol content between suicide victims and controls in specific brain regions such as the frontal cortex, amygdala, and hippocampus. However, when suicides were classified as violent or non-violent according to the used method, violent suicides were found to have lower gray-matter cholesterol content in the frontal cortex compared to non-violent suicides. Other authors (58), albeit in a small sample, reported no difference in the levels of total cholesterol and triglycerides among attempters and non-attempters.
Our findings show that TG were significantly higher in the control group than in LLSA and HLSA subgroups, among which no significant differences were reported. This is consistent with previous studies showing lower TG levels among suicide attempters when compared with controls without a positive history of suicide attempts (17, 20–22). Lower TG levels were reported in subjects who attempted suicide in the month before the survey compared with subjects who had suicidal ideation in the month before the survey and never suicidal controls (23).
Moreover, our findings do not show any differences regarding TG levels in LLSA and HLSA subgroups; to date, no previous studies investigated the possible association between the lethality of suicide attempts and TG levels. There are studies in the current literature that reported no differences in TG levels among violent vs. non-violent suicide attempts, though they did not consider the lethality of suicide attempts (25, 59).
Our study should be considered in the light of the following limitations; firstly, this is a cross-sectional study, and we cannot assess whether a decrease in TC or TG may have caused a mood episode with active suicidal ideation leading to suicide attempts, or if the presence of a mood episode originated a loss of appetite and a consequent loss of weight altering lipid profiles. Thus, given the main nature of this study, we could not evaluate the direct causal relation between suicidal behaviors and lipid profile. Moreover, our results could not be adjusted for the psychopharmacological medications that both cases and controls were taking when assessed and this may have influenced our findings. However, subjects taking lipid-lowering agents were not included in the sample. Thirdly, a detailed medical history, including careful information about the body mass index (BMI) was not available. Neither blood pressure nor glycaemic values were collected and, consequently, included in the analysis. However, we only included those subjects with stable clinical conditions apart from what was related to suicide attempts.
Our data suggest that low total cholesterol serum levels may increase the risk of HLSA and low triglycerides serum levels increase suicide risk—as well as low TC levels do—but they do not influence the lethality of the attempt. To the best of our knowledge, no previous studies have investigated TC and TG levels in respect to the lethality of suicide attempt. Therefore, further studies should focus on this association in order to confirm these preliminary results and shed light on the complex neurobiological mechanisms underlying suicidal behaviors.
AA: supervision data collection, writing protocol, statistical analyses, writing original draft; PS: writing original draft, designed the study; GG: writing protocol, conceived, and designed the study; MC, CC, and MR: data collection, revision of data literature; EA and MA: review and editing of the original draft, scientific advisor of the project; GS: designed the study, review, and editing of the original draft. All authors approved of the final draft of the manuscript before submission.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. World Health Organization. Preventing Suicide: A Global Imperative. Geneva: World Health Organization (2014).
3. Mann JJ, Waternaux C, Haas GL, Malone KM. Toward a clinical model of suicidal behavior in psychiatric patients. Am J Psychiatry. (1999) 156:181–9.
4. Oquendo MA, Sullivan GM, Sudol K, Baca-Garcia E, Stanley BH, Sublette ME, et al. Toward a biosignature for suicide. Am J Psychiatry. (2014) 171:1259–77. doi: 10.1176/appi.ajp.2014.14020194
5. Pompili M, Longo L, Dominici G, Serafini G, Lamis DA, Sarris J, et al. Polyunsaturated fatty acids and suicide risk in mood disorders: a systematic review. Progr NeuroPsychopharmacol Biol Psychiatry (2017) 74:43–56. doi: 10.1016/j.pnpbp.2016.11.007
6. Daray FM, Mann JJ, Sublette ME. How lipids may affect risk for suicidal behavior. J Psychiatr Res. (2018) 104:16–23. doi: 10.1016/j.jpsychires.2018.06.007
7. Loas G, Dalleau E, Lecointe H, Yon V. Relationships between anhedonia, alexithymia, impulsivity, suicidal ideation, recent suicide attempt, C-reactive protein and serum lipid levels among 122 inpatients with mood or anxious disorders. Psychiatry Res. (2016) 246:296–302. doi: 10.1016/j.psychres.2016.09.056
8. Dickerson F, Adamos M, Katsafanas E, Khushalani S, Origoni A, Savage C, et al. The association between immune markers and recent suicide attempts in patients with serious mental illness: a pilot study. Psychiatry Res. (2017) 255:8–12. doi: 10.1016/j.psychres.2017.05.005
9. Sudol K, Mann JJ. Biomarkers of suicide attempt behavior: towards a biological model of risk. Curr Psychiatry Rep. (2017) 19:31. doi: 10.1007/s11920-017-0781-y
10. Courtet P, Jaussent I, Genty C, Dupuy AM, Guillaume S, Ducasse D, et al. Increased CRP levels may be a trait marker of suicidal attempt. Eur Neuropsychopharmacol. (2015) 25:1824–31. doi: 10.1016/j.euroneuro.2015.05.003
11. Willour VL, Seifuddin F, Mahon PB, Jancic D, Pirooznia M, Steele J, et al. A genome-wide association study of attempted suicide. Mol Psychiatry. (2012) 17:433–44. doi: 10.1038/mp.2011.4
12. Pawlak J, Dmitrzak-Weglarz M, Wilkosc M, Szczepankiewicz A, Leszczynska-Rodziewicz A, Zaremba D, et al. Suicide behavior as a quantitative trait and its genetic background. J Affect Disord. (2016) 206:241–50. doi: 10.1016/j.jad.2016.07.029
13. Stanford SM, Bottini M, Bottini N. The role of LMPTP in the metabolic syndrome. In: Bence KK, editor. Protein Tyrosine Phosphatase Control of Metabolism. New York, NY; Heidelberg; Dordrecht; London: Springer (2015). p. 203–20.
14. Muldoon MF, Manuck SB, Matthews KA. Lowering cholesterol concentrations and mortality: a quantitative review of primary prevention trials. BMJ. (1990) 301:309–14.
15. Lee HJ, Kim YK. Serum lipid levels and suicide attempts. Acta Psychiatr Scand. (2003) 108:215–21. doi: 10.1034/j.1600-0447.2003.00115.x
16. Fiedorowicz JG, Coryell WH. Cholesterol and suicide attempts: a prospective study of depressed inpatients. Psychiatry Res. (2007) 152:11–20. doi: 10.1016/j.psychres.2006.09.003
17. Chang JC, Yen AM, Lee CS, Chen SL, Chiu SY, Fann JC, et al. Metabolic syndrome and the risk of suicide: a community-based integrated screening samples cohort study. Psychosom Med. (2013) 75:807–14. doi: 10.1097/PSY.0000000000000014
18. Aguglia A, Albert U, Maina G. Serum lipids and lifetime suicide attempts in patients with obsessive-compulsive disorder. J Obsessive Compuls Relat Disord. (2017) 15:1–6. doi: 10.1016/j.jocrd.2017.07.003
19. Messaoud A, Mensi R, Mrad A, Mhalla A, Azizi I, Amemou B, et al. Is low total cholesterol levels associated with suicide attempt in depressive patients? Ann Gen Psychiatry. (2017) 16:20. doi: 10.1186/s12991-017-0144-4
20. Ayesa-Arriola R, Canal Rivero M, Delgado-Alvarado M, Setién-Suero E, González-Gómez J, Labad J, et al. Low-density lipoprotein cholesterol and suicidal behaviour in a large sample of first-episode psychosis patients. World J Biol Psychiatry. (2018) 11:1–4. doi: 10.1080/15622975.2017.1414305
21. Segoviano-Mendoza M, Cárdenas-de la Cruz M, Salas-Pacheco J, Vázquez-Alaniz F, La Llave-León O, Castellanos-Juárez F, et al. Hypocholesterolemia is an independent risk factor for depression disorder and suicide attempt in Northern Mexican population. BMC Psychiatry. (2018) 18:7. doi: 10.1186/s12888-018-1596-z
22. Wu S, Ding Y, Wu F, Xie G, Hou J, Mao P. Serum lipid levels and suicidality: a meta-analysis of 65 epidemiological studies. J Psychiatry Neurosci. (2016) 41:56–69. doi: 10.1503/jpn.150079
23. Baek JH, Kang ES, Fava M, Mischoulon D, Nierenberg AA, Yu BH, et al. Serum lipids, recent suicide attempt and recent suicide status in patients with major depressive disorder. Progr NeuroPsychopharmacol Biol Psychiatry. (2014) 51:113–8. doi: 10.1016/j.pnpbp.2014.01.018
24. Ahmadpanah M, Haghighi M, Jahangard L, Borzoei S, Heshmati S, Bajoghli H, et al. No evidence for metabolic syndrome and lipid profile differences in patients suffering from bipolar I disorder with and without suicide attempts. Int J Psych Clin Pract. (2015) 19:168–73. doi: 10.3109/13651501.2015.1049277
25. Bartoli F, Crocamo C, Dakanalis A, Riboldi I, Miotto A, Brosio E, et al. Association between total serum cholesterol and suicide attempts in subjects with major depressive disorder: exploring the role of clinical and biochemical confounding factors. Clin Biochem. (2017) 50:274–8. doi: 10.1016/j.clinbiochem.2016.11.035
26. Perera S, Eisen RB, Bhatt M, Dennis BB, Bawor M, El-Sheikh W, et al. Exploring metabolic factors and health behaviors in relation to suicide attempts: a case-control study. J Affect Disord. (2018) 229:386–95. doi: 10.1016/j.jad.2017.12.060
27. Alvarez JC, Cremniter D, Gluck N, Quintin P, Leboyer M, Berlin I, et al. Low serum cholesterol in violent but not in non-violent suicide attempters. Psychiatry Res. (2000) 95:103–8. doi: 10.1016/S0165-1781(00)00171-2
28. Vevera J, Zukov I, Morcinek T, Papezova H. Cholesterol concentrations in violent and non-violent women suicide attempters. Eur Psychiatry. (2003) 18:23–7. doi: 10.1016/S0924-9338(02)00011-1
29. Ludwig B, Dwivedi Y. The concept of violent suicide, its underlying trait and neurobiology: a critical perspective. Eur Neuropsychopharmacol. (2018) 28:243–51. doi: 10.1016/j.euroneuro.2017.12.001
30. Lalovic A, Levy E, Luheshi G, Canetti L, Grenier E, Sequeira A, et al. Cholesterol content in brains of suicide completers. Int J Neuropsychopharmacol. (2007) 10:159–66. doi: 10.1017/S1461145706006663
31. Freemantle E, Mechawar N, Turecki G. Cholesterol and phospholipids in frontal cortex and synaptosomes of suicide completers: relationship with endosomal lipid trafficking genes. J Psychiatr Res. (2013) 47:272–9. doi: 10.1016/j.jpsychires.2012.10.019
32. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Publishing (2013).
33. Aguglia A, Borsotti A, Cuniberti F, Serafini G, Amore M, Maina G. The influence of sunlight exposure on hospitalization in emergency psychiatry. Chronobiol Int. (2017) 34:1413–22. doi: 10.1080/07420528.2017.1374286
34. Aguglia A, Borsotti A, Maina G. Bipolar disorders: is there an influence of seasonality or photoperiod? Rev Bras Psiquiatr. (2018) 40:6–11. doi: 10.1590/1516-4446-2016-2144
35. Schrijvers DL, Bollen J, Sabbe BG. The gender paradox in suicidal behavior and its impact on the suicidal process. J Affect Disord. (2012) 138:19–26. doi: 10.1016/j.jad.2011.03.050
36. Wu YW, Su YJ, Chen CK. Clinical characteristics, precipitating stressors, and correlates of lethality among suicide attempters. Chang Gung Med J. (2009) 32:543–52.
39. Beautrais AL. Suicides and serious suicide attempts: two populations or one? Psychol Med. (2001) 31:837–45. doi: 10.1017/S0033291701003889
40. Miller M, Azrael D, Hemenway D. The epidemiology of case fatality rates for suicide in the northeast. Ann Emerg Med. (2004) 43:723–30. doi: 10.1016/S0196064404000691
41. Chen VC, Cheng AT, Tan HK, Chen CY, Chen TH, Stewart R, et al. A community-based study of case fatality proportion among those who carry out suicide acts. Soc Psychiatry Psychiatr Epidemiol. (2009) 44:1005–11. doi: 10.1007/s00127-009-0021-9
42. Horesh N, Levi-Belz Y, Apter A. Medically serious versus non-serious suicide attempts: Relationships of lethality and intent to clinical and interpersonal characteristics. J Affect Disord. (2012) 136:286–93. doi: 10.1016/j.jad.2011.11.035
43. Huang YC, Wu YW, Chen CK, Wang LJ. Methods of suicide predict the risks and method-switching of subsequent suicide attempts: a community cohort study in Taiwan. Neuropsychiatr Dis Treat. (2014) 10:711–8. doi: 10.2147/NDT.S61965
44. Lee CY, Wu YW, Chen CK, Wang LJ. The rate of fatality and demographic characteristics associated with various suicide methods: a community-based study in Northern Taiwan. Crisis. (2014) 35:245–52. doi: 10.1027/0227-5910/a000266
45. Trakhtenbrot R, Gvion Y, Levi-Belz Y, Horesh N, Fischel T, Weiser M, et al. Predictive value of psychological characteristics and suicide history on medical lethality of suicide attempts: a follow-up study of hospitalized patients. J Affect Disord. (2016) 199:73–80. doi: 10.1016/j.jad.2016.03.054
46. Gvion Y, Levi-Belz Y. Serious suicide attempts: systematic review of psychological risk factors. Front Psychiatry. (2018) 9:56. doi: 10.3389/fpsyt.2018.00056
47. Schaffer A, Isometsä ET, Azorin JM, Cassidy F, Goldstein T, Rihmer Z, et al. A review of factors associated with greater likelihood of suicide attempts and suicide deaths in bipolar disorder: part II of a report of the International Society for Bipolar Disorders Task Force on Suicide in Bipolar Disorder. Aust N Z J Psychiatry. (2015) 49:1006–20. doi: 10.1177/0004867415594428
48. Johnston JAY, Wang F, Liu J, Blond BN, Wallace A, Liu J, et al. Multimodal neuroimaging of frontolimbic structure and function associated with suicide attempts in adolescents and young adults with bipolar disorder. Am J Psychiatry. (2017) 174:667–75. doi: 10.1176/appi.ajp.2016.15050652
49. Rihmer Z, Gonda X, Döme P. The assessment and management of suicide risk in bipolar disorder. In: Carvalho F, Vieta E, editors. The Treatment of Bipolar Disorder: Integrative Clinical Strategies and Future Directions. Oxford: Oxford University Press (2018) pp. 207–225.
50. Delpozo-Banos M, Hawton K, Gunnel D, Lloyd K, Scourfield J, Dennis M, et al. CHERISH: understanding suicide clusters through exploring self harm behaviours. Int J Population Data Sci. (2017) pp. 227–229. doi: 10.23889/ijpds.v1i1.247
51. Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Evidence-based national suicide prevention taskforce in Europe: a consensus position paper. Eur Neuropsychopharmacol. (2017) 27:418–21. doi: 10.1016/j.euroneuro.2017.01.012
52. Kaplan JR. Assessing the observed relationship between low cholesterol and violence-related mortality. Implications for suicide risk. Ann N Y Acad Sci. (1997) 836:57–80.
53. Tomson-Johanson K, Harro J. Low cholesterol, impulsivity and violence revisited. Curr Opin Endocrinol Diabetes Obes. (2018) 25:103–7. doi: 10.1097/MED.0000000000000395
54. Mann JJ. The serotoninergic system in mood disorders and suicidal behaviour. Phil Trans R Soc B. (2013) 368:20120537. doi: 10.1098/rstb.2012.0537
55. Allen JA, Halverson-Tamboli RA, Rasenick MM. Lipid raft microdomains and neurotransmitter signalling. Nat Rev Neurosci. (2007) 8:128–40. doi: 10.1038/nrn2059
56. Liu JJ, Green P, John Mann J, Rapoport SI, Sublette ME. Pathways of polyunsaturated fatty acid utilization: implications for brain function in neuropsychiatric health and disease. Brain Res. (2015) 1597:220–46. doi: 10.1016/j.brainres.2014.11.059
57. Knowles EEM, Curran JE, Meikle PJ, Huynh K, Mathias SR, Goring HHH, et al. Disentangling the genetic overlap between cholesterol and suicide risk. Neuropsychopharmacology. (2018) 43:2556–63. doi: 10.1038/s41386-018-0162-1
58. Pompili M, Innamorati M, Lester D, Girardi P, Tatarelli R. Nearly lethal resuscitated suicide attempters have no low serum levels of cholesterol and triglycerides. Psychol Rep. (2010) 106:785–90. doi: 10.2466/PR0.106.3.785-790
Keywords: suicide, lethality, dyslipidemia, cholesterol, -c reactive protein, metabolic profile, inflammation
Citation: Aguglia A, Solano P, Giacomini G, Caprino M, Conigliaro C, Romano M, Aguglia E, Serafini G and Amore M (2019) The Association Between Dyslipidemia and Lethality of Suicide Attempts: A Case-Control Study. Front. Psychiatry 10:70. doi: 10.3389/fpsyt.2019.00070
Received: 23 August 2018; Accepted: 30 January 2019;
Published: 01 March 2019.
Edited by:
Tomas Hajek, Dalhousie University, CanadaReviewed by:
Silvia Ferrari, University of Modena and Reggio Emilia, ItalyCopyright © 2019 Aguglia, Solano, Giacomini, Caprino, Conigliaro, Romano, Aguglia, Serafini and Amore. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Aguglia, andrea.aguglia@unito.it
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.