 Justine Chouët1,2
Justine Chouët1,2 Guillaume Sacco2,3
Guillaume Sacco2,3 Spyridon N. Karras4David J. Llewellyn5Dolores Sánchez-Rodríguez6
Spyridon N. Karras4David J. Llewellyn5Dolores Sánchez-Rodríguez6 Cédric Annweiler2,3,7*
Cédric Annweiler2,3,7*- 1Department of Geriatric Medicine, Cholet Hospital, Cholet, France
- 2Department of Geriatric Medicine, Angers University Memory Clinic, Research Center on Autonomy and Longevity, Angers University Hospital, Angers, France
- 3UPRES EA 4638 and Health Faculty, University of Angers, Angers, France
- 4Division of Endocrinology and Metabolism, First Department of Internal Medicine, Medical School, Aristotle University of Thessaloniki, AHEPA University Hospital, Thessaloniki, Greece
- 5University of Exeter Medical School, Exeter, United Kingdom
- 6WHO Collaborating Centre for Public Health Aspects of Musculoskeletal Health and Aging, Division of Public Health, Epidemiology and Health Economics, University of Liege, Liege, Belgium
- 7Department of Medical Biophysics, Robarts Research Institute, Schulich School of Medicine and Dentistry, the University of Western Ontario, London, ON, Canada
Objective: Vitamin D is involved in brain health and function. Our objective was to determine whether the serum 25-hydroxyvitamin D (25OHD) concentration was associated with delirium in a case-control study of geriatric inpatients.
Methods: Sixty cases with delirium (mean ± SD, 84.8 ± 5.7years; 58.3% female) and 180 age- and gender-matched controls were enrolled in a geriatric acute care unit between 2012 and 2014. The diagnosis of delirium was made using the Confusion Assessment Method. Hypovitaminosis D was defined using consecutively the consensual threshold value of 50 nmol/L and a threshold value calculated from a sensitivity-specificity analysis. Age, gender, number of acute diseases, use of psychoactive drugs, season of testing, and serum concentrations of calcium, parathyroid hormone, creatinine, albumin, TSH, vitamin B9 and vitamin B12 were used as potential confounders.
Results: The 60 cases with delirium exhibited lower 25OHD concentration than 180 matched controls (35.4 ± 30.0 nmol/L vs. 45.9 ± 34.5 nmol/L, p = 0.035). Increased 25OHD concentration was associated with a decrease in delirium prevalence (OR = 0.99 [95CI: 0.98–0.99] per nmol/L of 25OHD, p = 0.038). The concentration distinguishing between cases and controls with the best sensitivity-specificity was found between 29.5 and 30.5 nmol/L. The regression models showed that delirium was associated with hypovitaminosis D defined either as 25OHD ≤ 50 nmol/L (OR = 2.37 [95CI: 1.07–5.25], p = 0.034) or as 25OHD ≤ 30 nmol/L (OR = 2.66 [95 CI: 1.30–5.45], p = 0.008).
Conclusions: Decreased serum 25OHD concentrations were associated with delirium among acute geriatric inpatients. The threshold concentration to differentiate between cases and controls was around 30 nmol/L.
Introduction
Clinical importance of hypovitaminosis D is linked to its high prevalence, estimated at more than one billion people around the word (1), and its health manifestations. Vitamin D is classically known for its regulatory function in phosphocalcic metabolism (2). A growing number of studies have also reported non-bone effects of vitamin D in the past decade, especially on brain health and function (3–5).
Hypovitaminosis D has been repeatedly associated with neurocognition (6), particularly with major neurocognitive disorders (7, 8) and accelerated cognitive decline (8, 9). However, epidemiological associations reported thus far mainly implied chronic neurocognitive disorders. In contrast, acute neurocognitive disorders such as delirium were only scarcely examined in this context.
Delirium is an acute neurocognitive disorder leading to greater morbidity (pressure ulcers, infectious diseases, fall risk, disability), complicated care course (prolonged hospital stays, more frequent readmissions, increased healthcare costs), and greater mid-term mortality (10–12). Pathophysiology of delirium remains not fully elucidated. Some risk factors are well identified, including the advance in age, male gender, history of chronic neurocognitive disorders or psychiatric conditions (11). However, these risk factors are unchangeable and cannot be targeted to prevent delirium. Thus, potential changeable risk factors are the matter of extensive research. Several hypotheses are proposed, mainly based on biological imbalance within the central nervous system (11). Considering the neurocognitive effects of vitamin D, we hypothesized that hypovitaminosis D could participate to the onset of delirium among older adults. The aim of the present study was to determine whether serum 25-hydroxyvitamin D (25OHD) concentration was associated with delirium among geriatric inpatients hospitalized in an acute care unit.
Methods
Design and Settings
We conducted a unicentric case-control study (1 case with delirium for 3 controls without delirium) in the geriatric acute care unit of the University Hospital of Angers, France, between 2012 and 2014. At the admission into the unit, participants received standardized clinical and neuropsychological assessments together with a blood test. The study was approved by the local ethics committee and the Commission nationale informatique et libertés (number 1408714).
Participants
All patients aged 70 years and older consecutively admitted between 2012 and 2014 in the unit were considered for inclusion in the study. Inclusion criterion for cases was the diagnosis of delirium according to the Confusion Assessment Method (CAM) (13). Controls exhibiting no diagnosis of delirium according to the CAM were matched by age and gender (ratio 3:1). All participants were affiliated to the French social insurance.
Data Collection
Delirium
Delirium was identified using the CAM (13), a standardized tool aiming to screening for delirium. A senior physician assessed four main criteria (a) acute onset and fluctuating course, (b) inattention, (c) disorganized thinking, (d) altered level of consciousness. Delirium was retained when criteria (a) and (b) associated to criteria (c) and/or (d) were retrieved. This assessment is quick and easy to use with good metrological performance (13, 14).
Serum 25-hydroxyvitamin D Concentration
Serum concentrations of 25OHD effectively reflect the stock of vitamin D in the body. Serum concentrations of 25OHD were measured at the time of the CAM test by radioimmunoassay (DiaSorin Inc., Stillwater, MN) in nmol/L (to convert to ng/mL, divide by 2.496). With this method, there is no interference with lipids, which is often observed in other non-chromatographic assays of 25OHD. The intra- and interassay precision were 5.2 and 11.3%, respectively. Hypovitaminosis D was successively defined using either the consensual threshold value of 50 nmol/L according to the World Health Organization and the National Institutes of Health definitions, or using a threshold value calculated from a sensitivity-specificity analysis to best fit the studied group.
Covariates
Age, gender, number of acute diseases, use of psychoactive drugs, season of testing, serum concentrations of calcium, parathyroid hormone, creatinine, albumin, thyroid-stimulating hormone (TSH), vitamins B9 and B12 were used as potential confounders. The number of acute diseases was assessed by a senior physician at the admission. Using psychoactive drugs (i.e., antidepressants or neuroleptics or anxiolytics) were determined from drug prescriptions at the admission. The season of testing were categorized as follows: Spring from March 21 to June 20, Summer from June 21 to September 20, Autumn from September 21 to December 20, and Winter from December 21 to March 20. All blood samples were analyzed using standardized laboratory methods at the University Hospital of Angers, France.
Number of Participants
Because the main objective of the study was descriptive, no calculation of number of subjects was required. However, to match a normal distribution of the data and to use parametric statistical tests, at least 30 participants were required in each group (i.e., n = 30 participants with delirium and n = 30 controls at least). To improve the power of the study, we chose to triple the number of controls (i.e., 3 controls per 1 case).
Statistics
The participants' characteristics were summarized using means and standard deviations (SD) or frequencies and percentages, as appropriate. Normality of data distribution was checked using skewness-kurtosis test. As the number of observations was higher than 40, comparisons were not affected by the shape of the error distribution and no transform was applied (15). Firstly, comparisons between cases with delirium and controls without delirium were performed using Student's t-test or the Chi-square test, as appropriate. Secondly, the serum 25OHD threshold value that best distinguished between cases and controls was determined by sensitivity analysis. Thirdly, a multiple logistic regression was used to examine the association between delirium (dependent variable) and serum 25OHD (independent variable), while adjusting for potential confounders. Finally, similar logistic models were used to examine the association between delirium and hypovitaminosis D defined either using the consensual threshold value of 50 nmol/L or using the threshold value calculated with the sensitivity analysis. P-values < 0.05 were considered significant. All statistics were performed using SPSS (v19.0, IBM Corporation, Chicago, IL).
Results
Sixty cases with delirium (mean ± SD, 84.8 ± 5.7years; 58.3% female) and 180 controls without delirium (84.8 ± 5.7 years; 58.3% female) were included in the study. The mean serum 25OHD concentration was 43.3 ± 33.7 nmol/L, and 67.5% of the studied group exhibited hypovitaminosis D ≤ 50 nmol/L. Serum 25OHD concentration was lower among cases compared to controls (respectively, 35.4 ± 30.0 nmol/L vs. 45.9 ± 34.5 nmol/L, p = 0.035), and hypovitaminosis D ≤ 50 nmol/L was also more frequent among cases compared to controls (p = 0.039) (Table 1).
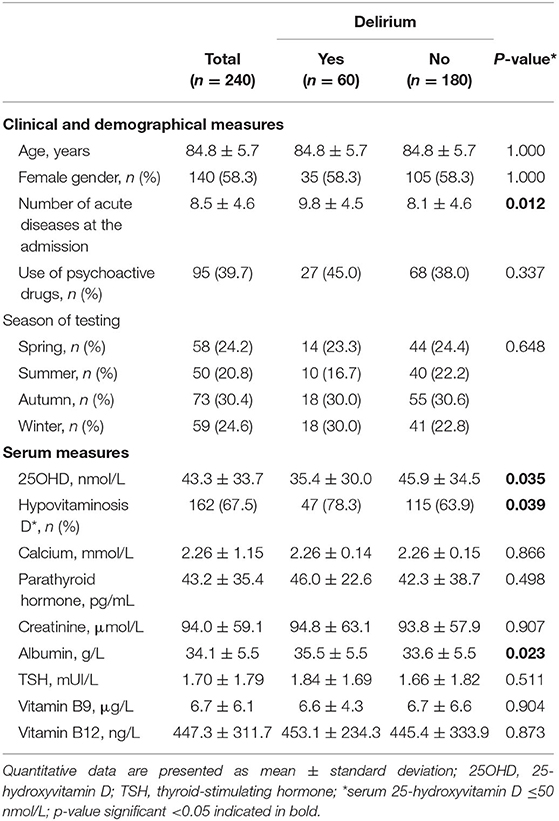
Table 1. Participants' characteristics and comparisons between cases with delirium (n = 60) and age- and gender-matched controls without delirium (n = 180).
Multiple logistic regression models showed that the increase in serum 25OHD was inversely associated to delirium (OR = 0.989 [95% confidence interval (CI): 0.979–0.999] by nmol/L of 25OHD, p = 0.038), even after adjusting for potential confounders (OR = 0.988 [95CI: 0.975–0.999] by nmol/L of 25OHD, p = 0.047) (Table 2).
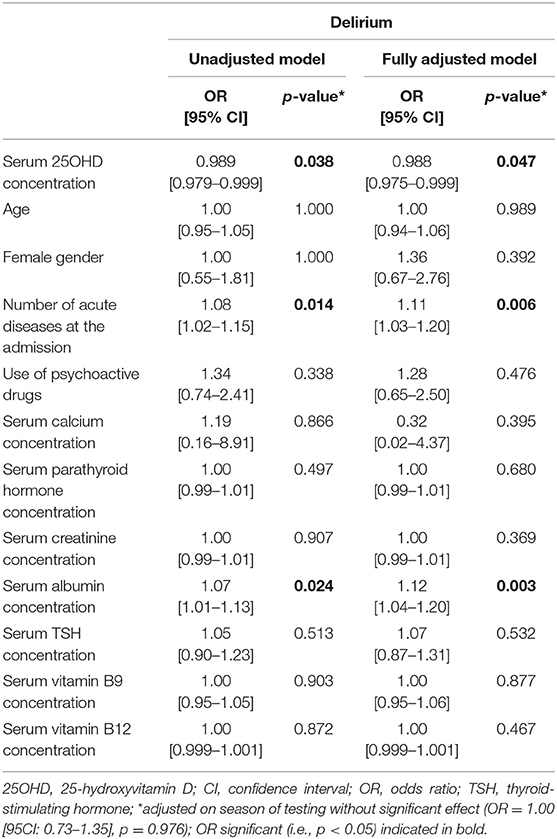
Table 2. Univariate and multiple logistic regression models assessing the cross-sectional association between serum 25-hydroxyvitamin D concentration (independent variable) and the diagnosis of delirium (dependent variable) after adjustment for potential confounders* (n = 240).
The best compromise between sensitivity and specificity to predict delirium was calculated for a 25OHD threshold between 29.5 nmol/L (Se = 0.60, Sp = 0.37) and 30.5 nmol/L (Se = 0.58, Sp = 0.35).
Hypovitaminosis D was associated with delirium whether using the consensual threshold of 50 nmol/L (OR = 2.37 [95CI: 1.07–5.25], p = 0.034) or using the calculated threshold of 30 nmol/L (OR = 2.66 [95CI: 1.30–5.45], p = 0.008) (Table 3). Increased number of acute diseases and serum albumin concentration were also associated with delirium (Tables 2, 3).
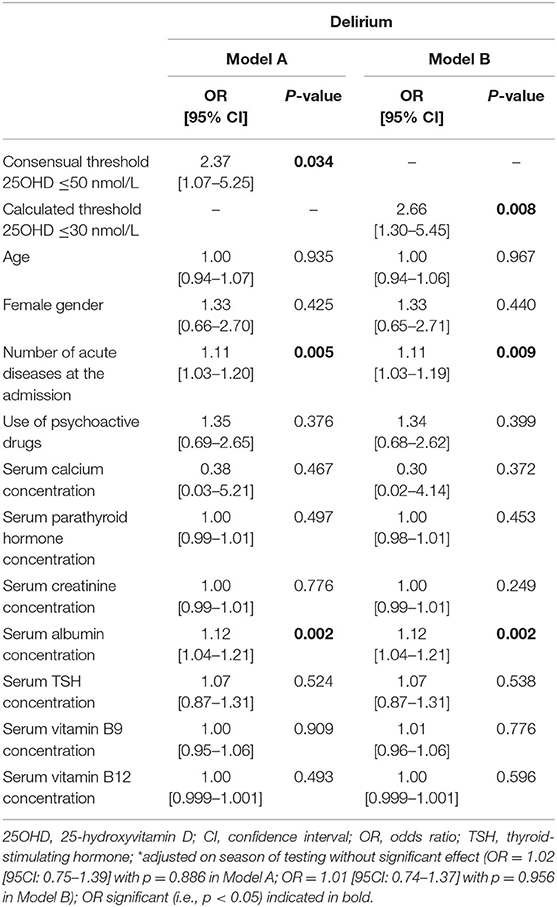
Table 3. Multiple logistic regression models* assessing the cross-sectional association between delirium and hypovitaminosis D defined using (A) consensual threshold of 50 nmol/L or (B) calculated threshold of 30 nmol/L (n = 240).
Discussion
Delirium was associated with decreased 25OHD concentrations among older adults hospitalized in geriatric acute care unit, independently of all studied potential confounders. Hypovitaminosis D (defined either by the consensual threshold of 50 nmol/L or by a population-based threshold of 30 nmol/L) was associated with delirium.
Our results are in accordance with the scarce previous literature. Ford et al. found hypovitaminosis D (ie, insufficiency <75 nmol/L or deficiency <25 nmol/L) in 66% of people diagnosed with delirium from three Canadian university hospitals (12). Similarly, in a cohort of more than 4,000 patients, Quraishi et al. reported that serum 25OHD concentration <25 nmol/L prior to hospitalization was associated with an increased risk of delirium during the hospital stay (16), which suggested that the vitamin D status could be a changeable risk factor for delirium acquired during hospitalization. In contrast, such association was not found within intensive care units (17). The divergence could be explained by the initial severity of the acute medical problem and by the different levels of care provided, which may overpass the effect of hypovitaminosis D on delirium risk, if any. Compared to previous literature, we provide here the first case-control study on this issue to our knowledge, which allowed us to calculate the threshold of serum 25HOD corresponding specifically to the onset of delirium among geriatric inpatients.
Delirium is an acute cognitive dysfunction. Most previous studies reported that hypovitaminosis D could be associated with increased risks of Alzheimer disease (AD) and related disorders (18, 19). One meta-analysis found a 2.4-fold higher risk of cognitive dysfunction among people with hypovitaminosis D compared to those without hypovitaminosis D (7). Moreover, patients with AD have lower serum 25OHD concentrations compared to those without AD (19). Such association was found both in the severe (20) but also in the prodromal stages of AD (21), just as if hypovitaminosis D contributed to the process of neurodegenerative dementia. Consistently, cohort studies confirmed that hypovitaminosis D precedes and predicts the onset of AD (7, 9). As a consequence, an international expert consensus concluded that hypovitaminosis D increased the risk of cognitive decline and dementia in older patients (8).
Mechanisms linking hypovitaminosis D to delirium are not fully elucidated. Vitamin D receptors were found in neurons and glial cells from brain areas that are essential to cognitive function (temporal cingular and orbital cortex, thalamus, nucleus accumbens, stria terminalis and amygdala) (22). By modifying the gene expression of various proteins, vitamin D modulates some effects that could influence neurophysiology and neuroprotection (4). With regards to neurophysiology, vitamin D regulates neurotrophic agents and controls cell differentiation and maturation (23). Vitamin D also regulates the gene expression of various neurotransmitters including acetylcholine, dopamine and serotonin (6). With regards to neuroprotection, vitamin D limits inflammatory changes associated with aging in hippocampus (24), prevents the accumulation of Aβ peptides by stimulating phagocytosis (25) and blood-brain barrier efflux transport (26). Moreover, vitamin D is involved in calcium homeostasis by regulating calcium channels (27). Vitamin D also protects the brain against glutamate toxicity (28) through anti-oxidant and anti-ischemic effects. As a consequence, hypovitaminosis D is associated with changes in brain volume (29), vascularization (30) and metabolism (31); all changes that may explain the greater risk of delirium in the case of hypovitaminosis D. Nevertheless, causality could not be deducted from our observational study, and delirium may actually be the expression of an altered cognitive status responsible for hypovitaminosis D because of disability and subsequent decreased food intakes and sun exposure.
We found a positive association between the number of acute diseases and delirium. This association could be explained on the one hand by the multifactorial origin of the delirium; most patients with delirium having multiple triggering factors independently of any previous major neurocognitive disorder (32). On the other hand, it is also possible that acute diseases were the consequences of delirium (11).
Our study presents some limitations. First, the case-control design of our study is less robust than a prospective longitudinal cohort study. Second, the CAM is a screening rather than a diagnostic tool despite very high metrological performance (14). Because of its 99% specificity (14), we assume all included patients effectively suffered from delirium. Third, our results cannot be generalized to all older adults due to the unicentric recruitment and the relatively limited number of participants. Fourth, although we were able to control for important characteristics that could modify the associations, residual potential confounders might still be present such as the ApoE genotype. Fifth, because 90% of frail elderly patients admitted into our hospital geriatric acute care unit suffer from major neurocognitive disorders, we did not use chronic neurocognitive disorders as a potential confounder here. Last, the use of an observational design precludes from inferring any causal inference.
Conclusions
We were able to report an association between serum 25OHD concentration and delirium in older adults hospitalized in a geriatric acute care unit, especially below 30 nmol/L. This result should be confirmed in larger longitudinal studies, preferentially on a variety of adult populations. Nevertheless, it provides new clues for better understanding the involvement of vitamin D in neurocognitive decline and acute failure illustrated by delirium. It also provides a scientific basis for conducting clinical trials to test the efficacy of vitamin D supplementation to prevent or improve the prognosis of delirium in older patients with initial serum 25OHD < 30 nmol/L.
Data Availability Statement
The datasets generated for this study are available on request from the corresponding author after notification and authorization of the competent authorities.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethical committee of Angers University Hospital. No patient and/or relatives objected to the use of their health, functional and biological data for research purposes.
Author Contributions
CA has full access to all data in the study, takes responsibility for the data, the analyses and interpretation, and has the right to publish any or all data, separate and apart from the attitudes of the sponsors, obtained funding, statistical expertise, administrative, technical, or material support, and study supervision. JC and CA: study concept and design. JC: acquisition of data. JC, GS, SK, DS-R, and CA: analysis and interpretation of data. JC, GS, and CA: drafting of the manuscript. SK, DL, and DS-R: critical revision of the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Authors wish to thank patients for their participation to the study.
References
2. Hossein-Nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo Clin Proc. (2013) 88:720–55. doi: 10.1016/j.mayocp.2013.05.011
3. Annweiler C, Allali G, Allain P, Bridenbaugh S, Schott A-M, Kressig RW, et al. Vitamin D and cognitive performance in adults: a systematic review. Eur J Neurol. (2009) 16:1083–9. doi: 10.1111/j.1468-1331.2009.02755.x
4. Annweiler C. Vitamin D in dementia prevention. Ann N Y Acad Sci. (2016) 1367:57–63. doi: 10.1111/nyas.13058
5. Landel V, Annweiler C, Millet P, Morello M, Féron F. Vitamin D, cognition and Alzheimer's disease: the therapeutic benefit is in the D-tails. J Alzheimers Dis. (2016) 53:419–44. doi: 10.3233/JAD-150943
6. Annweiler C, Schott A-M, Berrut G, Chauviré V, Le Gall D, Inzitari M, et al. Vitamin D and ageing: neurological issues. Neuropsychobiology. (2010) 62:139–50. doi: 10.1159/000318570
7. Etgen T, Sander D, Bickel H, Sander K, Förstl H. Vitamin D deficiency, cognitive impairment and dementia: a systematic review and meta-analysis. Dement Geriatr Cogn Disord. (2012) 33:297–305. doi: 10.1159/000339702
8. Annweiler C, Dursun E, Féron F, Gezen-Ak D, Kalueff AV, Littlejohns T, et al. “Vitamin D and cognition in older adults”: updated international recommendations. J Intern Med. (2015) 277:45–57. doi: 10.1111/joim.12279
9. Tilvis RS, Kähönen-Väre MH, Jolkkonen J, Valvanne J, Pitkala KH, Strandberg TE. Predictors of cognitive decline and mortality of aged people over a 10-year period. J Gerontol A Biol Sci Med Sci. (2004) 59:268–74. doi: 10.1093/gerona/59.3.M268
10. Gentric A, Le Deun P, Estivin S. [Prevention of delirium in an acute geriatric care unit]. Rev Med Intern. (2007) 28:589–93. doi: 10.1016/j.revmed.2007.04.004
11. Zarate-Lagune M, Lang P.O, Zekry D. [Delirium in old age. Difficulties in diagnosis.] Rev Méd Suisse. (2008) 4:2392–7.
12. Ford J, Hategan A, Bourgeois JA, Tisi DK, Xiong GL. Hypovitaminosis D in Delirium: a retrospective cross-sectional study. Can Geriatr J. (2013) 16:186–91. doi: 10.5770/cgj.16.79
13. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. (1990) 113:941–8. doi: 10.7326/0003-4819-113-12-941
14. Shi Q, Warren L, Saposnik G, Macdermid JC. Confusion assessment method: a systematic review and meta-analysis of diagnostic accuracy. Neuropsychiatr Dis Treat. (2013) 9:1359–70. doi: 10.2147/NDT.S49520
15. Rochon J, Gondan M, Kieser M. To test or not to test: preliminary assessment of normality when comparing two independent samples. BMC Med Res Methodol. (2012) 12:81. doi: 10.1186/1471-2288-12-81
16. Quraishi SA, Litonjua AA, Elias KM, Gibbons FK, Giovannucci E, Camargo CA, et al. Association between pre-hospital vitamin D status and hospital-acquired new-onset delirium. Br J Nutr. (2015) 113:1753–60. doi: 10.1017/S0007114515001245
17. Morandi A, Barnett N, Miller RR, Girard TD, Pandharipande PP, Ely EW, et al. Vitamin D and delirium in critically Ill patients: a preliminary investigation. J Crit Care. (2013) 28:230–5. doi: 10.1016/j.jcrc.2012.06.011
18. Annweiler C, Rolland Y, Schott AM, Blain H, Vellas B, Beauchet O. Serum vitamin D deficiency as a predictor of incident non-Alzheimer dementias: a 7-year longitudinal study. Dement Geriatr Cogn Disord. (2011) 32:273–8. doi: 10.1159/000334944
19. Annweiler C, Llewellyn DJ, Beauchet O. Low serum vitamin D concentrations in Alzheimer's disease: a systematic review and meta-analysis. J Alzheimers Dis. (2013) 33:659–74. doi: 10.3233/JAD-2012-121432
20. Annweiler C, Fantino B, Le Gall D, Schott A-M, Berrut G, Beauchet O. Severe vitamin D deficiency is associated with advanced-stage dementia in geriatric inpatients. J Am Geriatr Soc. (2011) 59:169–71. doi: 10.1111/j.1532-5415.2010.03166.x
21. Tot Babberich EDN, Gourdeau C, Pointel S, Lemarchant B, Beauchet O, Annweiler C. Biology of subjective cognitive complaint amongst geriatric patients: vitamin D involvement. Curr Alzheimer Res. (2015) 12:173–8. doi: 10.2174/1567205012666150204123504
22. Kalueff AV, Tuohimaa P. Neurosteroid hormone vitamin D and its utility in clinical nutrition. Curr Opin Clin Nutr Metab Care. (2007) 10:12–9. doi: 10.1097/MCO.0b013e328010ca18
23. Brown J, Bianco JI, McGrath JJ, Eyles DW. 1,25-dihydroxyvitamin D3 induces nerve growth factor, promotes neurite outgrowth and inhibits mitosis in embryonic rat hippocampal neurons. Neurosci Lett. (2003) 343:139–43. doi: 10.1016/S0304-3940(03)00303-3
24. Nissou M-F, Guttin A, Zenga C, Berger F, Issartel J-P, Wion D. Additional clues for a protective role of vitamin D in neurodegenerative diseases: 1,25-dihydroxyvitamin D3 triggers an anti-inflammatory response in brain pericytes. J Alzheimers Dis. (2014) 42:789–99. doi: 10.3233/JAD-140411
25. Masoumi A, Goldenson B, Ghirmai S, Avagyan H, Zaghi J, Abel K, et al. 1alpha,25-dihydroxyvitamin D3 interacts with curcuminoids to stimulate amyloid-beta clearance by macrophages of Alzheimer's disease patients. J Alzheimers Dis. (2009) 17:703–17. doi: 10.3233/JAD-2009-1080
26. Ito S, Ohtsuki S, Nezu Y, Koitabashi Y, Murata S, Terasaki T. 1α,25-Dihydroxyvitamin D3 enhances cerebral clearance of human amyloid-β peptide(1-40) from mouse brain across the blood-brain barrier. Fluids Barriers CNS. (2011) 8:20. doi: 10.1186/2045-8118-8-20
27. Brewer LD, Thibault V, Chen KC, Langub MC, Landfield PW, Porter NM. Vitamin D hormone confers neuroprotection in parallel with downregulation of L-type calcium channel expression in hippocampal neurons. J Neurosci. (2001) 21:98–108. doi: 10.1523/JNEUROSCI.21-01-00098.2001
28. Ibi M, Sawada H, Nakanishi M, Kume T, Katsuki H, Kaneko S, et al. Protective effects of 1 alpha,25-(OH)(2)D(3) against the neurotoxicity of glutamate and reactive oxygen species in mesencephalic culture. Neuropharmacology. (2001) 40:761–71. doi: 10.1016/S0028-3908(01)00009-0
29. Annweiler C, Annweiler T, Montero-Odasso M, Bartha R, Beauchet O. Vitamin D and brain volumetric changes: systematic review and meta-analysis. Maturitas. (2014) 78:30–9. doi: 10.1016/j.maturitas.2014.02.013
30. Annweiler C, Annweiler T, Bartha R, Herrmann FR, Camicioli R, Beauchet O. Vitamin D and white matter abnormalities in older adults: a cross-sectional neuroimaging study. Eur J Neurol. (2014) 21:1436–e95. doi: 10.1111/ene.12511
31. Annweiler C, Beauchet O, Bartha R, Hachinski V, Montero-Odasso M. Vitamin D and caudal primary motor cortex: a magnetic resonance spectroscopy study. PLoS ONE. (2014) 9:e87314. doi: 10.1371/journal.pone.0087314
Keywords: vitamin D, delirium, cognition, older adults, neuroendocrinology
Citation: Chouët J, Sacco G, Karras SN, Llewellyn DJ, Sánchez-Rodríguez D and Annweiler C (2020) Vitamin D and Delirium in Older Adults: A Case-Control Study in Geriatric Acute Care Unit. Front. Neurol. 11:1034. doi: 10.3389/fneur.2020.01034
Received: 27 December 2019; Accepted: 10 August 2020;
Published: 18 September 2020.
Edited by:
William Camu, Hôpital Gui De Chauliac, FranceReviewed by:
James Alan Bourgeois, Baylor Scott and White Health, United StatesWalter Serrano, University of Colima, Mexico
Copyright © 2020 Chouët, Sacco, Karras, Llewellyn, Sánchez-Rodríguez and Annweiler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cédric Annweiler, Y2VkcmljLmFubndlaWxlckBjaHUtYW5nZXJzLmZy