 Yolanda Quiles
Yolanda Quiles Maria José Quiles
Maria José Quiles Eva León
Eva León Javier Manchón
Javier Manchón- Department of Behavioral Sciences and Health, Miguel Hernández University, Elche, Spain
People’s beliefs about their illness have been shown to affect their adjustment. The aim of this study was to describe illness perception in adolescent patients with anorexia nervosa (AN) and assess its relationship with socio-emotional and academic adjustment following Leventhal’s Self-Regulation Model. Thirty-four female AN patients, with a mean age of 15.76 (SD = 2.00), completed the Revised Illness Perception Questionnaire (IPQ-R), the Psychosocial Adjustment to Illness Scale (PAIS) and the Hospital Anxiety and Depression Scale (HAD). Adolescent anorexia patients perceived that they had control over their illness and treatment would improve their condition. However, they also believed that it was highly distressing, going to last a long time and would have serious consequences. As for the causes of the disorder, they were attributed primarily to a specific eating disorder and psychological factors. The results showed that anorexia patients’ illness perceptions were related to socio-emotional and academic adjustment. In this sense, identity with the illness was associated with a worse academic adjustment, while emotional representation was associated with a worse emotional and social adjustment. These findings highlight how important it is for patients’ beliefs about their disease to be considered in the treatment of anorexia. In this respect, clinicians treating these patients should consider how certain beliefs affect their academic and socio-emotional adjustment. It would be interesting for patients to become aware of how these beliefs influence the strategies they use to cope with their disease as well as their adjustment to it.
Introduction
Anorexia nervosa (AN) is a chronic and complex mental illness with serious physical and social consequences (Patel et al., 2016). Its prevalence ranges between 4 and 6% for women and under 1% in the case of men (DSM-5, American Psychiatric Association, 2013; Ward et al., 2019). It is characterized by a high resistance to treatment with serious family and social repercussions, including the highest mortality rate of any psychiatric illness (López and Treasure, 2011; Ward et al., 2019). Young women make up the majority of people with AN, with an average illness duration of about 6 years (Schmidt et al., 2016).
Anorexia nervosa is diagnostically defined by abnormal eating behavior and distorted attitudes toward body weight and shape (DSM-5). It has a high impact on patients’ quality of life, affecting their physical and psychological health as well as having important consequences for their academic and social functioning (Treasure et al., 2015).
Data suggest that AN is associated with atypical social and emotional functioning (Harrison et al., 2010; Patel et al., 2016). In this sense, negative social experiences (such as derogatory comments, negative feedback, and pressure) can be stressors that trigger the disease (Hutchinson and Rapee, 2007; Quiles et al., 2013), and during its most acute phase, patients can experience isolation and loneliness (Levine, 2012). It is also known that socio-communicative difficulties are maintaining factors for these patients (Patel et al., 2016; Schmidt and Treasure, 2006). Recently, Cardi et al. (2018) identified three specific factors that might be involved in the onset and maintenance of AN: fear of negative evaluation, perceived lack of social competence and early experiences of submissiveness.
Academic performance is another important trigger in AN patients. Although reported premorbid characteristics for these patients include high levels of academic performance and extreme perfectionism, when the illness becomes entrenched, cognitive decline and impaired concentration can accompany starvation and depression (Maxwell et al., 2011). This impaired neurocognitive functioning present in AN patients (Weider et al., 2015; Kucharska et al., 2019) leads to difficulties in different neuropsychological capacities, such as attention, working memory, long-term learning, autobiographical memory, processing speed, problem solving, or information processing (Oltra et al., 2012). Data suggests that this could be a consequence of the illness per se or could arise from intensified underlying traits for AN (Lang et al., 2016). On the one hand, the personal self-demand that characterizes these patients is associated with high pressure to obtain excellent academic results; and on the other hand, if patients identify themselves as “AN patients” their performance also worsens. However, academic performance can be affected by school stress too (Espíndola and Blay, 2009).
Cognitive difficulties are not the only factor that could influence academic performance (Yanover and Thompson, 2008), discrepancies between actual and ideal self-perceptions, what the patient would really like to be and how they really feel, are also a core symptom. These differences are related to poor school grades, low self-esteem and depressive symptoms (Ferguson et al., 2010). In fact, individuals with AN report that the social and psychological consequences of the disorder are more important than physical ones (Dovydaitiene and Maslauskiene, 2013). Thus, during the recovery process, it is important to consider the extent to which patients consider that the disease hinders their daily functioning (Tchanturia et al., 2012).
There is scarce research on illness perception with respect to AN (Jansen, 2016). It is perceived as a chronic illness with strong negative consequences (Holliday et al., 2005), and AN patients typically have a high number of symptoms that are difficult to control, cure, and understand. These perceptions are very important because patients with a strong belief in treatment control are more likely to report a better psychological adjustment and appear to have better academic performance, family relationships, and global adjustment (Quiles et al., 2007a). It is therefore apparent that illness perception is related to treatment outcomes, which can interfere with recovery. Moreover, AN is often seen as linked to an individual’s identity and difficult to give up (Higbed and Fox, 2010), and patients tend to perceive their illness as chronic and difficult to be treated. This perception of chronicity and severity is related to the impression that the eating disorder is untreatable (Stockford et al., 2007). Apart from this, illness perception also affects family and social relationships.
The aim of this study was to describe illness perception in adolescent AN patients and assess its relationship with socio-emotional and academic adjustment following Leventhal’s Self-Regulation Model (Leventhal et al., 1984, 1997, 2003). This is a very useful model to understand the way that AN patients understand and cope to the illness. It hypothesizes that individuals create mental representations of illness based on five dimensions (illness identity, timeline, consequences, causes, and controllability/curability).
Materials and Methods
Participants
A total of 34 female AN nervosa outpatients attending a specialized unit for eating disorders were recruited. Patients have a primary DSM-IV diagnosis of AN (restrictive type = 30; purging type = 4). Participants’ age ranged from 12 to 19 (Mean = 15.76 years, SD = 2.00). The patients had a mean illness duration of 25.82 months (SD = 18.62), and they were receiving psychological and nutritional treatment.
Variables and Instruments
Sociodemographic and Clinical Characteristics
Patients’ sociodemographic data and clinical characteristics were collected through the completion of an ad hoc questionnaire. This sought information concerning ages and relevant clinical data for the study (diagnosis and history of the problem).
Illness Perception
Patients’ perceptions of eating disorder were assessed using the specific eating disorders dimension from the Spanish version (Quiles et al., 2007b) of the Revised Illness Perception Questionnaire (IPQ-R; Moss-Morris et al., 2002). This questionnaire measures participants’ illness beliefs in eight dimensions: identity, timeline (individual’s beliefs about the course of the illness), consequences, cause, cyclical timeline, control, cure, and emotional representations. It is divided into three sections: the identity and causal dimensions are presented in two separate sections, while the remaining dimensions are presented together in one section. The cause subscale consists of four components: psychological cause, ED specified cause, risk cause, and external cause. The internal consistency for the subscales in the Spanish version of this questionnaire range from α = 0.55 to α = 0.85. For this study, McDonald’s omega for the subscales ranged from ω = 0.62 (cyclical timeline subscale) to ω = 0.86 (identity subscale).
Psychosocial Adaptation
The PAIS (Psychosocial Adjustment to Illness Scale, Derogatis, 1986) was used to assess adjustment to illness. The PAIS comprises 45 items, each of which contains four statements scored on a 4-point scale ranging from 0 (no problem) to 3 (many difficulties). Higher scores indicate more difficulties. The scale is designed to provide information on global adjustment as well as adjustment in specific areas. In this study, we have assessed these areas: educational and social adjustment, family relationships and psychological distress. The Spanish version of this questionnaire has adequate psychometric properties (from α = 0.70 to α = 0.90) (Neipp, 2005; Portillo et al., 2019). For this study, McDonald’s omega ranged from ω = 0.74 (educational adjustment) to ω = 0.91 (social adjustment).
Anxiety and Depression
The HAD (Hospital Anxiety and Depression Scale; Zigmond and Snaith, 1983) is a 14-item scale that assesses anxiety and depression, requiring answers on a 4-point scale. In this questionnaire, patients rate the degree to which they have experienced these symptoms over the previous week. The internal consistency, calculated with the Cronbach’s alpha coefficient for the Spanish version was 0.80 in the anxiety subscale and 0.76 in the depression subscale (Terol et al., 2007). For this study, McDonald’s omega for the subscales was ω = 0.73 and ω = 0.86, respectively.
Procedure
Patients were recruited from the Eating Disorder Unit of a public Hospital in the province of Alicante (Spain). Patients were included in the study if they were outpatients. Exclusion criteria were: borderline personality disorder, psychosis, current alcohol, substance dependence, or serious medical condition. This information was provided by the Eating Disorder Unit. These patients were handed information about the study during their treatment sessions. All patients and their relatives gave written informed consent for participation. Patients were interviewed in the Eating Disorder Unit by a qualified health psychologist after one of their treatment sessions.
Data Analysis
A cross-sectional design was used for this study. Data were analyzed using IBM SPSS v.25. to obtain frequencies and data descriptions for mean and minimum and maximum standard deviation. A one-way ANOVA was carried out to determine the differences in illness perception scores according to illness duration. For relation analysis, we used the Pearson correlation coefficient, and a stepwise multiple regression procedure was conducted to examine the relation between illness perception and socio-emotional and academic adjustment. Prior to the analysis, the assumptions of normality, homoscedasticity and independence were tested. The three assumptions were met.
Results
Illness Perception
Identity Subscale
Illness identity refers to statements regarding beliefs about the illness label and the link with symptoms. The mean for symptoms experienced by the patients was 6.85 (SD = 2.94). The two most frequently experienced symptoms were “weight loss” (94.1%) and “irregularities in menstruation” (88.2%). The two least frequently experienced symptoms were “wheeziness,” “sore eyes” and “stiff joints.” Results for this subscale are given in Table 1.
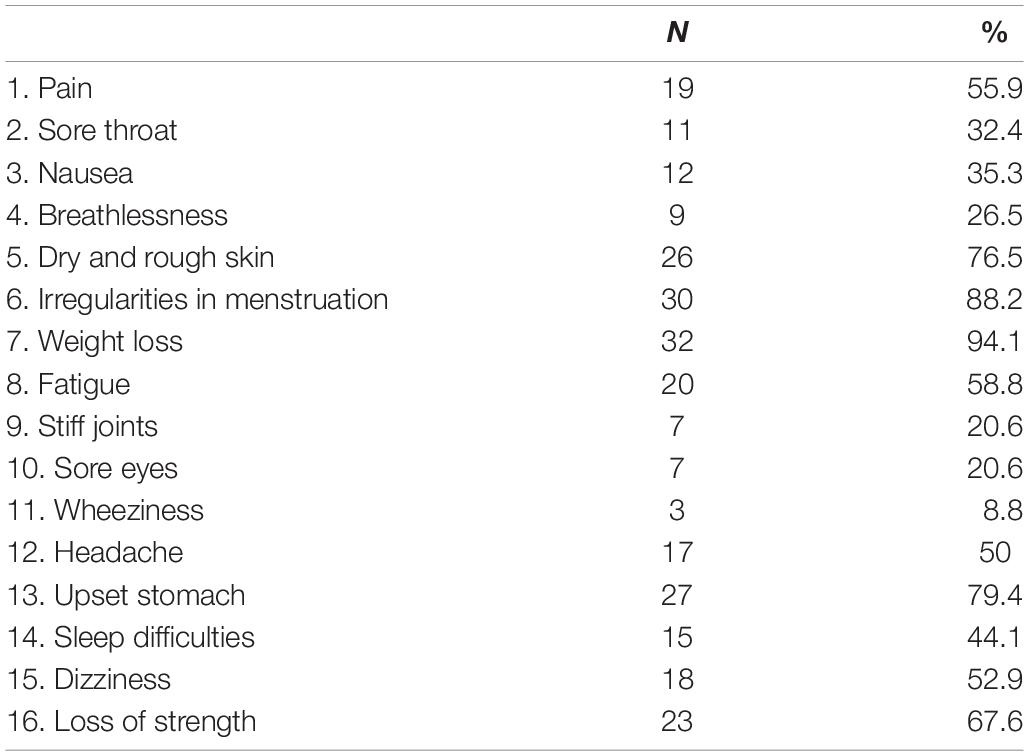
Table 1. Identity subscale: frequency of experienced symptoms.
Consequences, Control, Cure, Timeline, Emotional Representation and Cyclical Timeline Subscales
Illness perception of the sample is described in Table 2. The mean scores for these dimensions would suggest that these patients’ perception of their illness is that it was highly distressing, they had control over it, it was going to last a long time, and it had serious consequences. A one-way ANOVA comparing illness perception according to illness duration revealed that AN patients with a shorter average illness duration (≤1 year), perceived their illness with less serious consequences (M = 10; SD = 3.36) than patients with a longer illness duration (≥2 years) (M = 12.5; SD = 1.67) (F = 4.06, p < 0.05).
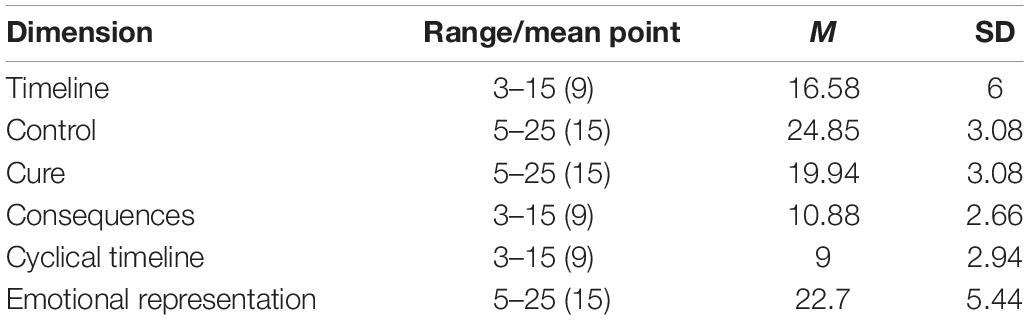
Table 2. Means and standard deviations of illness perception dimensions.
Causal Subscale
These patients showed higher scores in “specified ED factor” (M = 23.52; SD = 6.35) and “psychological factor” (M = 20.26; SD = 6.19). By contrast, the lowest scores were in “external cause factor” (M = 6; SD = 2.65) and in “risk factor” (M = 12.61; SD = 4). The factors that were most frequently identified as the cause of anorexia were low self-esteem and own behavior, followed by the need to be perfect, while the least frequently identified factors were alcohol, germen or virus and smoking. A one-way ANOVA comparing the type of causes to which they attributed their illness according to illness duration revealed that AN patients with the shortest average illness duration (≤6 months), attributed their disease to causes of the specific ED factor to a lesser extent (M = 18.00; SD = 6.00) than the group with the longest evolution time (≥4 years) (M = 28.8; SD = 5.8) (F = 3.85, p < 0.05).
Relationships Between Illness Perception and Socio-Emotional and Academic Adjustment
The Pearson correlation analyses showed that “identity” was associated with psychological distress (r = 0.48, p < 0.01), academic adjustment (r = 0.51, p < 0.01), family relationships (r = 0.45, p < 0.01), anxiety (r = 0.40, p < 0.05), and depression (r = 0.36, p < 0.05). Emotional representation was associated with psychological distress (r = 0.68, p < 0.001), anxiety (r = 0.50, p < 0.01), depression (r = 0.54, p < 0.01), family relationships (r = 0.43, p < 0.05), and with social (r = 0.36, p < 0.05) and academic (r = 0.38, p < 0.05) adjustment.
The timeline dimension was associated with psychological distress (r = 0.42, p < 0.01) and anxiety (r = 0.36, p < 0.05). ED specified causes were associated with family relationships (r = 0.38, p < 0.05) and with anxiety (r = 0.39, p < 0.05).
The results of the regression analyses are shown in Table 3.
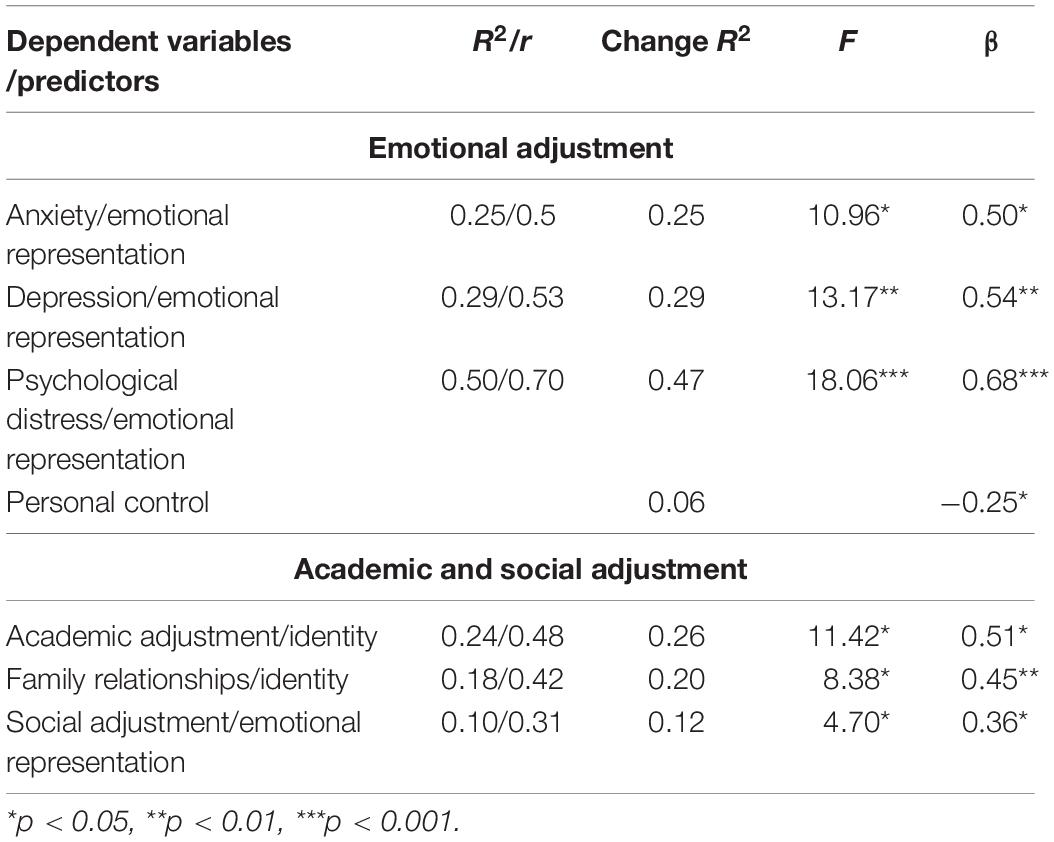
Table 3. Stepwise multiple regression analyses: the relation between illness perception and socio-emotional and academic adjustment.
“Emotional representation” was the most significant illness perception dimension related to emotional adjustment. It contributed to 25% of the variance in anxiety, 29% in depression, and 47% in psychological distress.
With respect to academic adjustment, “identity” contributed to 24% of the variance, while “emotional representation” explained 10% of the variance, which was the same as in social adjustment.
Discussion
Illness perception in adolescent AN patients may not coincide with the clinical conception of this disorder, and their understanding of this illness and its causes, consequences, duration, and treatment effectiveness may significantly influence their recovery process. The results of this study showed that adolescent AN patients reported experiencing a moderate number of physical symptoms and believed that they had control over their disease and that the treatment was effective for their recovery. However, they also believed that their illness was going to last a long time and that it had serious consequences. The most commonly reported causes were attributed to the “specified ED factor” (refers to items that have been identified in research as core causes related to the onset of EDs) and “psychological factor,” such as low self-esteem and the need to be perfect. AN patients with longer duration of the illness perceived more physical and psychological complications.
This research has shown that AN patients’ illness perceptions are related to socio-emotional and academic adjustment. One area of concern is the extent to which negative emotional responses to AN negatively influence patients’ socio-emotional adjustment. These results are in line with Leventhal’s Self-Regulation Model, which asserts that emotional representation is a determining factor in an individual’s emotional response to their disease (Leventhal et al., 1980). In this context, high levels of illness-related distress (emotional representation) are associated with anxiety, depression, psychological distress and worse social functioning. Thus, these unpleasant emotions will affect patients’ social adjustment and therefore deteriorate their social relations. If an individual is afraid and insecure or perceives any situation as a threat or danger, it is difficult for them to relate to others, and consequently, these feelings can lead to social isolation, which is a key maintaining factor of the disorder (Kan and Treasure, 2019; Meneguzzo et al., 2020).
Illness identity or the tendency to attribute symptoms to AN was associated with academic adjustment, since these symptoms can become a signal to patients that their AN is active or progressing, leading to anxiety (Leventhal et al., 2003). Literature has shown that high levels of anxiety reduce learning efficiency by decreasing attention, concentration and retention, with the consequent deterioration in school performance (Van Ameringen et al., 2003; Visu-Petra et al., 2014; Respondek et al., 2017). For this reason, it is very important to treat anxiety that comes from identifying symptoms because decreased school performance negatively affects marks as well as adolescent students’ self-esteem (Nguyen et al., 2019).
This study highlights that illness perception is a key factor to be considered and one that should be included in the treatment of anorexia. In this sense, interventions designed to address illness perception can improve adjustment in these patients. Despite the importance of patients’ beliefs as well as their views of their symptoms and illness, they are not fully discussed in consultations. The results of the psychological treatment of AN may improve if the therapist addresses patients’ perceptions of identity and the emotional state of these patients.
Clinicians supporting adolescent AN patients’ adjustment should consider that some illness beliefs are associated with their academic and socio-emotional adjustment. It would be interesting for these patients to become aware of how these beliefs influence the strategies they use to cope with their disease as well as their adjustment to it.
This research has produced clear findings, but a number of limitations need to be considered, as sample size and the low reliability of some subscales, as cyclical timeline subscale of the IPQ-R. The results of the study might be influenced by the fact that at the time of the study all patients were in outpatient treatment. Therefore, it is likely that the results cannot be generalized to other patient samples. This was a cross-sectional study, so it would be important to carry out a longitudinal study to find out how illness perception changes in response to experience with one’s illness.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by University Miguel Hernández. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
YQ, MQ, and EL developed the design of the research. YQ and JM performed the data analyses. MQ, EL, and JM wrote the first draft. All authors contributed and reviewed the final draft. All authors participated in the development of the study and approved the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors are grateful to the patients with anorexia who agreed to participate in the study, as well to the professionals from the Eating Disorders Unit (UTCA) of the University Hospital of Sant Joan d’Alacant (Spain).
References
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn, Washington, DC: American Psychiatric Association.
Cardi, V., Mallorqui-Bague, N., Albano, G., Monteleone, A. M., Fernández-Aranda, F., and Treasure, J. (2018). Social difficulties as risk and maintaining factors in anorexia nervosa: a mixed-method investigation. Front. Psychiatr. 9:12. doi: 10.3389/fpsyt.2018.00012
Derogatis, L. R. (1986). The psychosocial adjustment to illness scale (PAIS). J. Psychosom. Res. 30, 77–91. doi: 10.1016/0022-3999(86)90069-3
Dovydaitiene, M., and Maslauskiene, I. (2013). Illness perception and motivation to recover in eating disorders. Proc. Soc. Behav. Sci. 84, 1217–1220. doi: 10.1016/j.sbspro.2013.06.731
Espíndola, C. R., and Blay, S. L. (2009). Anorexia nervosa’s meaning to patients: a qualitative synthesis. Psychopathology 42, 69–80. doi: 10.1159/000203339
Ferguson, G. M., Hafen, C. A., and Laursen, B. (2010). Adolescent psychological and academic adjustment as a function of discrepancies between actual and ideal self-perceptions. Youth Adol. 39, 1485–1497. doi: 10.1007/s10964-009-9461-5
Harrison, A., Sullivan, S., Tchanturia, K., and Treasure, J. (2010). Emotional functioning in eating disorders: attentional bias, emotion recognition and emotion regulation. Psychol. Med. 40, 1887–1897. doi: 10.1017/S0033291710000036
Higbed, L., and Fox, J. R. E. (2010). Illness perceptions in anorexia nervosa: a qualitative investigation. Br. J. Clin. Psychol. 49, 307–325. doi: 10.1348/014466509X454598
Holliday, J., Wall, E., Treasure, J., and Weinman, J. (2005). Perception of illness in anorexia nervosa: a comparison with other eating disorders and lay men and women. Int. J. Eat. Disord. 37, 50–56. doi: 10.1002/eat.20056
Hutchinson, D. M., and Rapee, R. M. (2007). Do friends share similar body image and eating problems? The role of social networks and peer influences in early adolescence. Behav. Res. Ther. 45, 1557–1577. doi: 10.1016/j.brat.2006.11.007
Jansen, A. (2016). Eating disorders need more experimental psychopatology. Behav. Res. Ther. 86, 2–10. doi: 10.1016/j.brat
Kan, C., and Treasure, J. (2019). Recent research and personalized treatment of anorexia nervosa. Psychiat. Clin. N. Am. 42, 11–19. doi: 10.1016/j.psc.2018.10.010
Kucharska, K., Kulakowska, D., Starzomska, M., Rybakowski, F., and Biernacka, K. (2019). The improvement in neurocognitive functioning in anorexia nervosa adolescents throughout the integrative model of psychotherapy including adolescents throughout the integrative cognitive remediation therapy. BMC Psychiatry 19:15. doi: 10.1186/s12888-018-1984-4
Lang, K., Treasure, J., and Tchanturia, K. (2016). Is inefficient cognitive processing in anorexia nervosa a family trait? A neuropsychological pilot study of mothers of offspring with a diagnosis of anorexia nervosa. World J. Biol. Psychiatr. 17, 258–265. doi: 10.3109/15622975.2015.1112035
Leventhal, H., Benyamini, Y., Brownlee, S., Diefenbach, M., Leventhal, E., Patrick-Miller, L., et al. (1997). “Illness representations: theoretical foundations,” in Perceptions of Health and Illness: Current Research and Applications, eds K. J. Petrie and J. Weiman (Amsterdam: Harwood Academic Publichers), 19–45.
Leventhal, H., Brissette, I., and Leventhal, A. (2003). “The self-regulation of health and illness behaviour,” in The Common-Sense Model Of Selfregulation Of Health And Illness, ed. L. D. Camero (New York, NY: Routledge), 42–65.
Leventhal, H., Meyer, D., and Nerenz, D. (1980). “The common sense representations of illness danger,” in Contributions to Medical Psychology, Vol. 2, ed. S. Rachman (Oxford: Pergamon Press).
Leventhal, H., Nerenz, D. R., and Steele, D. S. (1984). “Illness representations and coping with health threats,” in Handbook of Psychology and Health, eds A. Baum, S. E. Taylor, and J. E. Singer (Hillsdale, N.J: Erlbaum), 219–252.
Levine, M. P. (2012). Loneliness and eating disorders. J. Psychol. 146, 243–257. doi: 10.1080/00223980.2011.606435
López, C., and Treasure, J. (2011). Trastornos de la conducta alimentaria en adolescentes: descripción y manejo. Rev. Méd. Clín. Cond. 22, 85–97. doi: 10.1016/S0716-8640(11)70396
Maxwell, M., Thornton, L. M., Root, T. L., Pinheiro, A. P., Strober, M., Brandt, H., et al. (2011). Life beyond the eating disorder: education, relationships, and reproduction. Int. J. Eat. Disord. 44, 225–232. doi: 10.1002/eat.20804
Meneguzzo, P., Collantoni, E., Bonello, E., Busetto, P., Tenconi, E., and Favaro, A. (2020). The predictive value of the early maladaptive schemas in social situations in anorexia nervosa. Eur. Eat. Disord. Rev. 28, 318–331. doi: 10.1002/erv.2724
Moss-Morris, R., Weinman, J., Petrie, K. J., Horne, R., Cameron, L. D., and Buick, D. (2002). The revised illness perception questionnaire (IPQ-R). Psychol. Health 17, 1–16. doi: 10.1080/08870440290001494
Neipp, M. C. (2005). Control And Coping Beliefs In Women With Breast Cancer In The Follow-Up Stage, Doctoral thesis, Miguel Hernandez University, Spain.
Nguyen, D. T., Wright, E. P., Dedding, C., Pham, T. T., and Bunders, J. (2019). Low self-esteem and its association with anxiety, depression, and suicidal ideation in vietnamese secondary school students: a cross-sectional study. Front. Psychiatry 10:698. doi: 10.3389/fpsyt.2019.00698
Oltra, R., Espert, R., and Rojo, L. (2012). Neuropsicología y anorexia nerviosa. Hallazgos cognitivos y radiológicos. Neurología 27, 504–510. doi: 10.1016/j.nrl.2011.08.003
Patel, K., Tchanturia, K., and Harrison, A. (2016). An exploration of social functioning in young people with eating disorders: a qualitative study. PLoS One 7:e0159910. doi: 10.1371/journal.pone.0159910
Portillo, M. C., Ambrosio, L., Lanas, R., Navarta, M. V., Ursua, M., and Riveral, M. (2019). A pilot study on the Spanish version of the psychosocial adjustment to illness scale (PAIS-SR) with carers of people with Parkinson’s disease. Open J. Nurs. 6, 1262–1268. doi: 10.1002/nop2.329
Quiles, Y., Quiles, M. J., Pamies, L., Botella, J., and Treasure, J. (2013). Peer and family influence in eating disorders: a meta-analysis. Eur. Psychiatry 28, 199–206. doi: 10.1016/j.eurpsy.2012.03.005
Quiles, Y., Terol, M. C., Romero, C., and Pagán, G. (2007a). Illness perception in eating disorders and psychosocial adaptation. Eur. Eat. Disord. Rev. 15, 373–384. doi: 10.1002/erv.793
Quiles, Y., Terol, M. C., Tirado, S., and Beléndez, M. (2007b). Estructura factorial de la versión española del “cuestionario de percepción de enfermedad revisado” (IPQ-R) en pacientes con un trastorno del comportamiento alimentario y sus familiares. Cuadern. Med. Psicosom. Psiquiatr. Enlace 82, 9–22.
Respondek, L., Seufert, T., Stupnisky, R., and Nett, U. E. (2017). Perceived academic control and academic emotions predict undergraduate university student success: examining effects on dropout intention and achievement. Front. Psychol. 8:243. doi: 10.3389/fpsyg.2017.00243
Schmidt, U., and Treasure, J. (2006). Anorexia nervosa: valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. Br. J. Clin. Psychol. 45, 343–366. doi: 10.1348/014466505X53902
Schmidt, U., Adan, R., Boehm, I., Campbell, I. C., Dingemans, A., and Ehrlich, S. (2016). Eating disorders: the big issue. Lancet Psychiatry, 3, 313–315. doi: 10.1016/S2215-0366(16)00081-X
Stockford, K., Turner, H., and Cooper, M. (2007). Illness perception and its relationship to readiness to change in the eating disorders: a preliminary investigation. Br. Psychol. Soc 46, 139–154. doi: 10.1348/014466506X115786
Tchanturia, K., Davies, H., Harrison, A., Roberts, M., Nakazato, M., Schmidt, U., et al. (2012). Poor cognitive flexibility in eating disorders: examining the evidence using the Wisconsin cart sorting task. PLoS One 7:e28331.
Terol, M. C., López-Roig, S., Rodríguez-Marín, J., Pastor, M. A., Martín-Aragón, M., and Reig, J. (2007). Propiedades psicométricas de la Escala hospitalaria de ansiedad y Estrés (HAD) en población española. Anxiety Stress 13, 163–176.
Treasure, J., Zipfel, S., Micali, N., Wade, T., Stice, E., Claudino, A., et al. (2015). Anorexia nervosa. Nat. Rev. Dis. Primers 26:15074. doi: 10.1038/nrdp.2015.74
Van Ameringen, M., Mancini, C., and Farvolden, P. (2003). The impact of anxiety disorders on educational achievement. J. Anxiety Disord. 17, 561–571. doi: 10.1016/S0887-6185(02)00228-1
Visu-Petra, L., Stanciu, O., Benga, O., Miclea, M., and Cheie, L. (2014). Longitudinal and concurrent links between memory span, anxiety symptoms, and subsequent executive functioning in young children. Front. Psychol. 5:443. doi: 10.3389/fpsyg.2014.00443
Ward, Z. J., Rodriguez, P., Wright, D. R., Austin, S. B., and Long, M. W. (2019). Estimation of eating disorders prevalence by age and associations with mortality in a simulated nationally representative US Cohort. JAMA Netw. Open 2:e1912925. doi: 10.1001/jamanetworkopen.2019.12925
Weider, S., Indredavik, M. S., Lydersen, S., and Hestad, K. (2015). Neuropsychological function in patients with anorexia nervosa or bulimia nervosa. Int. J. Eat. Disord. 48, 397–405. doi: 10.1002/eat.22283
Yanover, T., and Thompson, J. K. (2008). Self-reported interference with academic academic functioning and eating disordered symptoms: associations with multiple dimensions of body image. Body Image 5, 326–328. doi: 10.1016/j.bodyim.2008.03.008
Keywords: anorexia nervosa, adolescents, illness perception, socio-emotional adjustment, academic adjustment
Citation: Quiles Y, Quiles MJ, León E and Manchón J (2020) Illness Perception in Adolescent Patients With Anorexia: Does It Play a Role in socio-Emotional and Academic Adjustment? Front. Psychol. 11:1730. doi: 10.3389/fpsyg.2020.01730
Received: 04 May 2020; Accepted: 23 June 2020;
Published: 21 July 2020.
Edited by:
José Manuel García-Fernández, University of Alicante, SpainReviewed by:
María Roncero, University of Valencia, SpainYolanda Pastor, Rey Juan Carlos University, Spain
Copyright © 2020 Quiles, Quiles, León and Manchón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria José Quiles, bWoucXVpbGVzQHVtaC5lcw==