 Maria Isabel Sánchez-Hernández1*
Maria Isabel Sánchez-Hernández1* Eduardo Gismera-Tierno2
Eduardo Gismera-Tierno2 Jesus Labrador-Fernández2
Jesus Labrador-Fernández2 José Luis Fernández-Fernández2
José Luis Fernández-Fernández2- 1Business Management and Sociology Department, School of Economics and Business Administration, University of Extremadura, Badajoz, Spain
- 2Ethics and Sustainability Department, School of Economics, Comillas Pontifical University, Madrid, Spain
Health religious organizations tend to offer individual attention to patients in line with their spiritual character and, at the same time, the highest service quality. This study puts the attention on the nurse-patient relationship and empirically explores a theoretical model that links nurses’ suffering at work with personal’s willingness to engage in a therapeutic and spiritual relationship with patients and the consequent effect on quality. Data has been collected in the city of Madrid (Spain) in the month of June 2019 in Santa Elena Clinic. An analytical case-study based on Partial Least Squares (PLS) path modeling is the chosen method to verify the cause-effect hypothesized relationships. This study contributes to the current academic literature by providing new knowledge and empirical evidence on the topic of the future of work in health religious organizations. The main conclusion is the necessary inclusion of suffering, even in good places to work, as a key indicator for a better management. Results should be a useful source of information for practitioners that seek to implement better human management systems in these organizations.
Introduction
Poor knowledge exists concerning the effects of suffering at work on health and occupational safety (Tetrick and Quick, 2003). Although researchers are becoming increasingly interested in understanding suffering at work such as Gismera et al. (2019), and companies start to be conscious about the organizational problems associated is an unexplored topic. The current human management systems do not directly address this problem, and there is a lack of evidence regarding how to manage suffering in organizations.
Religious health care institutions, most of them Catholic in Spain, are communities of healing, but also communities of compassion. That means that the service offered is not limited to the clinical treatment of the disease (physical dimension). In addition, religious health care institutions embrace the psychological, social and spiritual dimensions of the patients and the medical expertise is combined with spiritual forms of care to minimize human suffering. The encounter of Christians with human suffering is taken on a positive meaning through the redemptive power of Jesus’ suffering and death. At this respect, the United States Conference of Catholic Bishops (2001) highlighted “healing and compassion as a continuation of Christ’s mission and suffering as a participation in the redemptive power of Christ’s passion, death, and resurrection.” Going beyond the achievement of service quality, that is a general business goal (Lee et al., 2000; Glickman et al., 2007) to develop a close relationship with patients is considered the central aspect of health religious organizations. Consequently, measuring and managing the suffering in the workplace seems to be more important in this type of organizations, devoted to mitigate the suffering of others from the physical and the spiritual dimensions, than in other non-religious.
This study explores a structural model that links suffering at work with personal’s willingness to engage in a therapeutic and spiritual relationship. Data was collected in Madrid in the month of June 2019 in Santa Elena Clinic. Partial Least Squares (PLS) path modeling is the chosen analytical method to test the model and identify cause-effect relationships. This study will contribute to the academic literature by providing new knowledge and empirical evidence on the topic and a very useful source of information for practitioners that seek to implement better human management systems in health religious organizations.
Theoretical Framework
Suffering at work has been recently defined as a destabilizing and unpleasant psychological experience arising when the employee runs into insuperable and tenacious barriers, after having used up all his or her available resources trying to improve the organization of work with regards to quality and safety (Bontemps et al., 2018). According to the Psychodynamics Theory (PT) of work and organizations, a person’s working experience undergoes the same intrapsychic conflicts as other aspects of life. Czander (1993) pointed out that the traditional view of system man/woman is that he/she is motivated by the need for material goods (economic matters) but the psychoanalytic perspective defends the neurotic condition of all human beings conditioned by shadowy wishes and fears. Under this theory, Diamond and Allcorn (2003) defined organizations as processes of human behavior that are considered as experiential and perceptual systems dominated by unconscious schemes (Prins, 2006). The workplace has been conceptualized as psychological space and a meaningful workplace implies a good relationship employee-organization in terms of dedication, loyalty and commitment (Chalofsky, 2003; Glomb et al., 2011) where spirituality has a relevant role (Steenkamp and Basson, 2013). Some recent works exist devoted to the study of these topics within the context of religious organizations (Ariza-Montes et al., 2017, 2019; Ortiz-Gómez et al., 2020).
Most human beings are inclined to avoid suffering (Connelly, 2009). The recommendation of Diamond and Allcorn (2003) for human resources managers is to bring into the workplace those things that contribute to making work a meaningful experience that will contribute to the employees’ mental health. In the same vain, and following some authors from the field of coaching such as Briner (1999), de Vries (2004), Peltier (2011) in this research the argument is made that unconscious dynamics related to job satisfaction, but also suffering at work, causes a significant impact on organizations and, in addition, on service quality (Ellinger et al., 2011).
Job satisfaction is a complex and multifaceted construct (Judge and Kinger, 2007). Locke (1976) defined job satisfaction as a “pleasurable or positive emotional state resulting from the appraisal of one’s job or job experiences.” In general terms, job satisfaction is reflected on the positive perception of professional achievement (Gazioglu and Tansel, 2006) related to motivation (Tzeng, 2002; Egan et al., 2004), spiritual well-being (Duggleby et al., 2009) psychological well-being (Munir et al., 2012; Burton et al., 2017), recognition (Ernst et al., 2004; Clarke and Mahadi, 2017), and pride for a given work activity (Utriainen and Kyngäs, 2009). It has been also recognized that satisfaction at work is reflected in the opportunity to express feelings and opinions to colleagues and supervisors and different experiences at work such as solidarity, cooperation or the possibility of using creativity at work (Noon et al., 2013; Guillén et al., 2015). In this context, although job satisfaction in the health care field is considered a significant element of health service quality (Snipes et al., 2005; Mosadeghrad, 2014; Choi et al., 2016), it is still largely understudied.
In general terms, traditionally medical literature has contained few studies that specifically address suffering (Cassell, 1982) and most authors who have tried to define suffering argued for its complementarity with the term pain (Egnew, 2005). However, the study of human suffering has advanced considerably in the last years (Coulehan, 2018). Some authors such as Montoya-Juarez et al. (2013) defined suffering as a state of pain more or less permanent, experienced by the subject within a specific society and culture, when facing a perceived threat as capable of destroying their own physical or psychosocial integrity, and before which they feel vulnerable and helpless.
Suffering in the workplace is probably a more common occurrence than expected in everyday life. As individuals of the first quarter of the 21st century, we spend much of our time around the professional side, in the bosom of business organizations of one kind or another and of the most diverse sectors. The suffering of human beings can not be subtracted from us. In fact, suffering at work represents a condition that drives worker mobilization against inconsistencies experienced at work and may even trigger mental disease.
It coul be said that the workplace itself is a source of suffering. Probably, this is more accurate in specific professions in front-office, assuming risks and/or dealing with high responsibilities. Suffering at the workplace can be evaluated through the experience of exhaustion that is caused by the perception of stress (Quick and Henderson, 2016) dissatisfaction (Häggström et al., 2005), insecurity or fear (Probst and Lawler, 2006; Cheng and Chan, 2008).
However, that is a fact in all sectors and job positions when the increase of competition and the derived new forms of work organization are even causing harm employees’ mental health (Hirigoyen, 2008). At this respect, Quick and Henderson (2016) reviewed the evidence concerning the health risks associated with occupational stress. Their arguments and final conclusions, that were developed from roots in preventive medicine and public health, highlighted the application of preventive management. In the interests of both, employee well-being and company performance, suffering at work must be taken seriously by Human Resources Managers, especially in the service sector, because it is expected that it will impact the final quality of the service provided.
Moving to the specific reality of suffering at work in staff nurses, the work of Elpern et al. (2005) about moral distress in a medical intensive care unit is a good example. The author identifies frequent and intense contexts where nurses suffer at work dealing with specific treatments for terminally ill patients and related technical and moral/ethical decisions. In academic literature, other authors have analyzed nursing and suffering at work focusing the attention on work stress (Taylor et al., 1999; Adeb-Saeedi, 2002; Dominguez-Gomez and Rutledge, 2009) burnout (Malach-Pines, 2000; Alimoglu and Donmez, 2005; Pompili et al., 2006; Khamisa et al., 2013) or both, in relation to the environment and the working conditions (Jennings, 2008).
Service quality has been deeply studied in academic literature originally from the Nordic School (Chowdhary and Prakash, 2007; Gummesson et al., 2012) and especially in health services (Isaac et al., 2010; Kitapci et al., 2014; Meesala and Paul, 2018). Once the existence of suffering at work in organizations has been recognized, it must be managed in health religious clinics and the quality of the healthcare service must be guaranteed.
To sum up, satisfied personnel in religious health-care organizations would develop a trusting and connected relationship with patients. Thus, we can expect high levels of nurse-patient relationship (Moyle, 2003; Mok and Chiu, 2004; Ward et al., 2009) and high levels of service quality (Landrum et al., 2009). However, poor knowledge exists concerning the effects of nurses’ suffering at work on service quality, basically because the current human management systems do not directly address this problem. Trying to contribute to fill the gap, this study contributes to the topic with new insights.
Materials and Methods
Design
An analytical case-study based on primary data was carried on. The case-study had three differentiated steps. Firstly, the Santa Elena Clinic was selected for being considered a best place to work. To verify this assumption nurses’ satisfaction at work was measured throughout an ad hoc anonymous self-administered questionnaire.
Secondly, the study analyzed the causal effect between nurse-patient relationship and the quality of the service provided (Model A). Finally, suffering at work was included to test the effect on the process of attending the patients and attaining the goal of high service quality (Model B).
Figure 1 shows the theoretical model A and B on the basis of this study representing the following hypotheses:
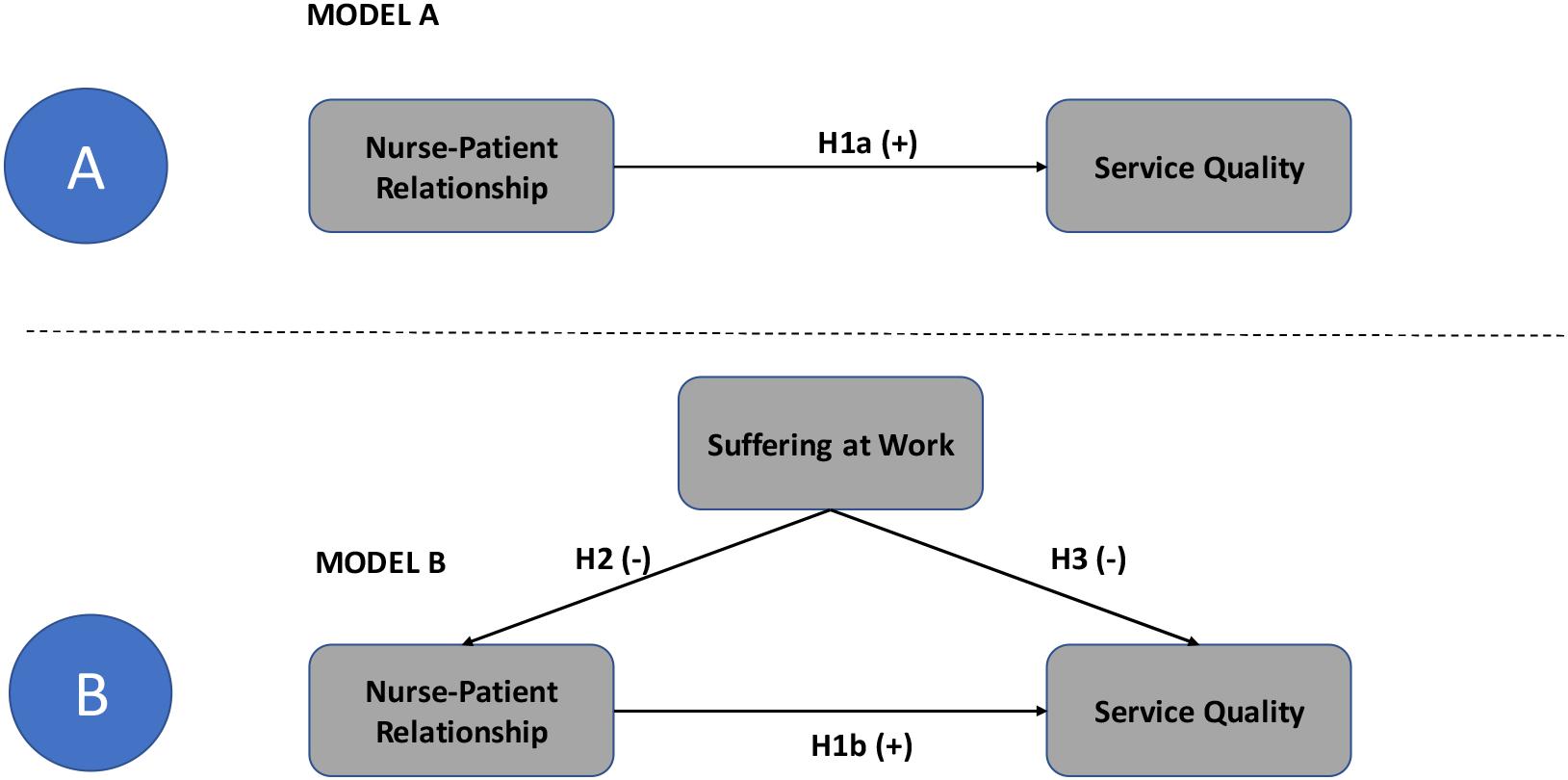
Figure 1. Theoretical Models (A,B).
H1: Nurse-Patient Relationship has a direct and positive impact on service quality.
H2: Suffering at work has a direct and negative impact on nurse-patient relationship.
H3: Suffering at work has a direct and negative impact on service quality.
Participants and Procedures
Catholic Hospitals of Madrid is the first non-lucrative health group in the city of Madrid in Spain. One of its members is Santa Elena Clinic, a Catholic health organization that has been run for more than half a century by the Religious Society of Saint José from Gerona. In all the centers the patient receives an individual attention in line with the human and spiritual character of the religious organization based on the maximum respect for the person and for life. This work is carried out with high level of dedication and love by religious, volunteers and professionals.
A total of 140 nurses were contacted in Santa Elena Clinic in Madrid, in the month of June 2019. A pilot test was carried out in order to check that the survey would be appropriately interpreted by the respondent. A final sample of 102 valid questionnaires were collected. Table 1 presents the study’s technical data sheet.
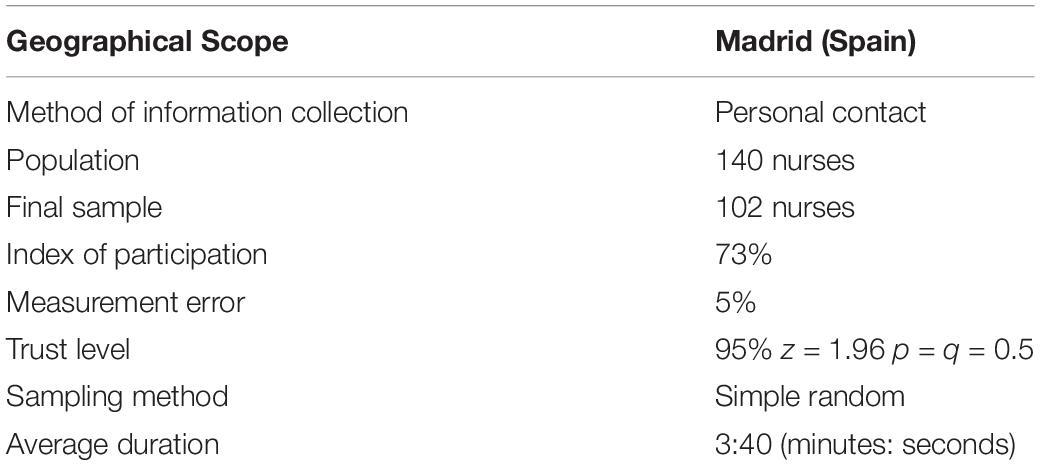
Table 1. Technical data sheet.
Data Analysis Methods
Descriptive statistics first, and structural equations modeling (SEM) later, have been used considering it very suitable for our research interests following Czander (1993). Concretely we want to highlight two reasons: because the constructs under study and the relationships between them, are really new; and both, the theoretical model and the relative measures, are not very well formed and generally accepted in the academic literature.
Structural equations modeling has been selected as the appropriate methodological tool considering that it offers the possibility to combine and compare theory with empirical data, performing multiple regressions between several latent variables to provide causal scientific explanations that go beyond the description and the association. In the present study, it has been applied the software developed by Ringle et al. (2005) denominated Smart-PLS (Partial Least Squares). PLS focuses on the explanation of variance using ordinary least squares, this technique is suited for the investigation of relationships in a predictive rather than a confirmatory fashion (Fornell and Bookstein, 1982). As a multivariate variance-based technique, PLS estimates path models involving latent constructs indirectly observed by multiple indicators. Furthermore, PLS is not sensitive to the assumptions of normality.
After verifying high levels of job satisfaction in the nurse-staff, a step-by-step analysis was conducted to offer a thorough analysis. In the first step, the focus was on the relationship between nurse-patient relationship and service quality. Subsequently, suffering at work was introduced, and the full structural model was assessed.
Measures and Instrument
An ad hoc questionnaire was elaborated to inquire into the nurse’s perceptions concerning different constructs, with responses on a 5-point Likert scale. According to previous literature review, satisfaction at work was measured with the following six items: Satisfaction with professional achievements (S1); Proud to work here (S2); Freedom of expression to both, colleagues and bosses (S3); Trust in co-workers (S4); Feelings of solidarity and cooperation at work (S5); Possibility to be creative at work (S6). Nurse-patient relationship was measured throughout four items: Understanding the patients’ needs (NPR1); Displaying caring actions and caring attitudes (NPR2); Providing holistic care (NPRN3); Acting as the patient’s advocate (NPR4). Service Quality was measured throughout two items, Affective and therapeutic dimensions: Willingness to listen patients and to assist them to talk about their fears, anxieties and problems (SQ1); Willingness to help patients and provide prompt service (SQ2). Finally, suffering at work was measured with a direct and single item; Fear and insecurity at work (SFF).
Ethical Considerations
Health is a matter of public interest. Putting the focus on human resources management in health institutions, the study has been guided by considerations of social justice and decent work, seeking for sustainable job positions and guaranteeing the agreement of managers to perform the analysis and, at the same time, the anonymity for participants.
Results
After verifying 3.9 average on job satisfaction on the sample, we considered the validity of the scales and the reliability of the measurement Model A and B (the inner models). The purpose was to analyze whether the theoretical concepts were properly measured by the observed items. This analysis was carried out for the two attributes validity (measuring what one really wanted to measure) and reliability (whether the process is stable and consistent). To this end we proceeded to calculate the reliability of individual items, the internal consistency or reliability of the scales and the analysis of the average variance extracted obtaining satisfactory results (Table 2).
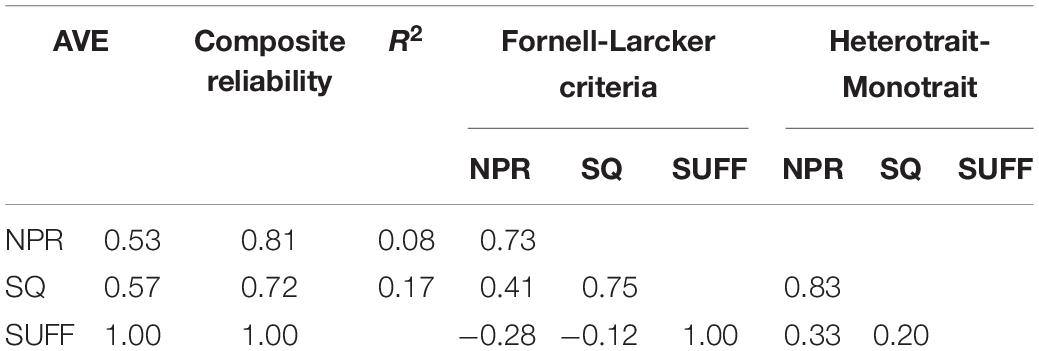
Table 2. Main results.
After the satisfactory evaluation of the measurement models it was necessary to carry out a correct interpretation of the structural models in order to verify whether these models considered the proposed relationships between the latent variables. A structural model estimates the assumed causal and linear covariance relationships among exogenous and endogenous latent constructs. Figure 2 shows graphically the main results from Models A and B.
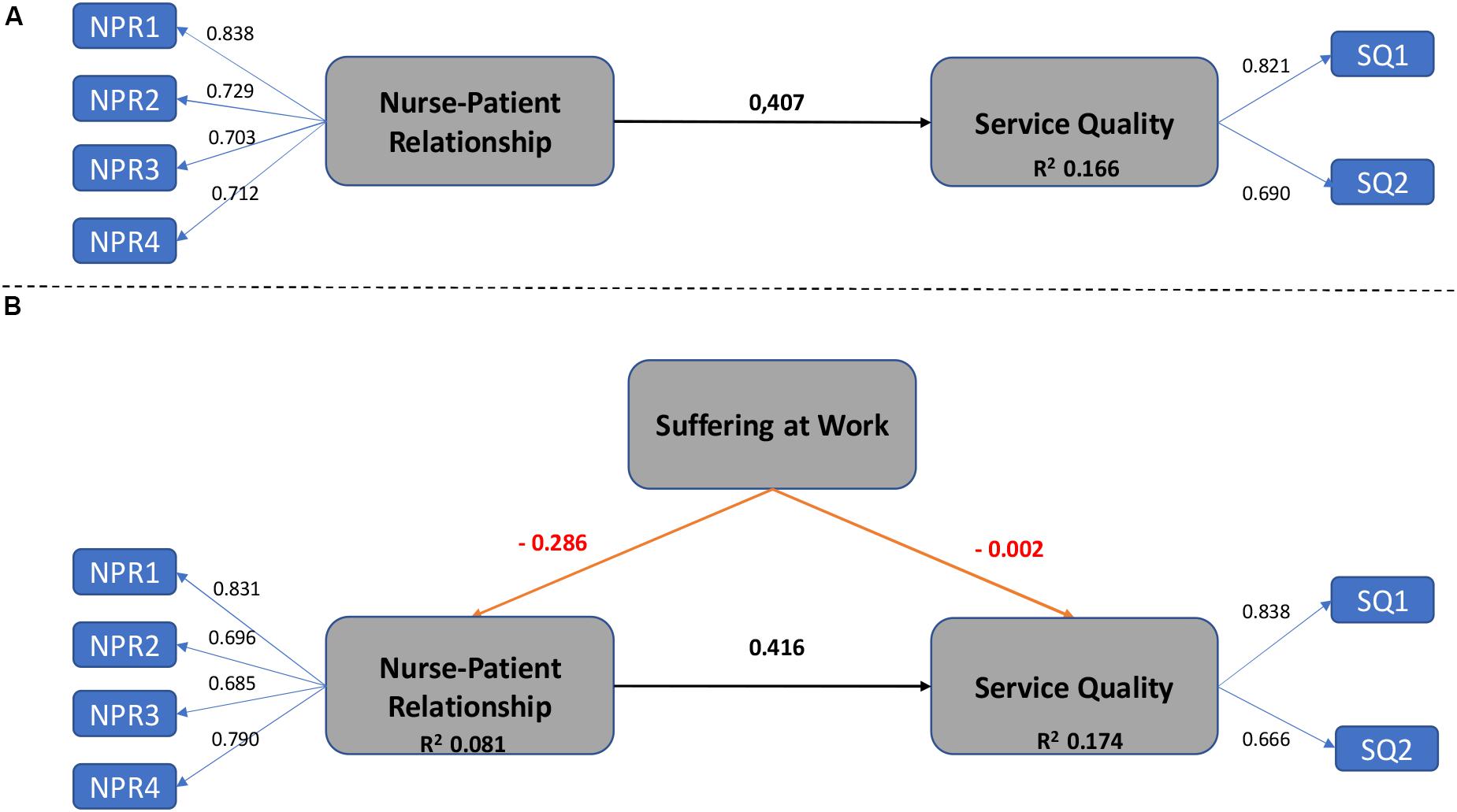
Figure 2. Main results: Models (A,B).
To conclude the analysis, Table 3 shows the hypotheses testing after bootstrap procedure. It was confirmed that the nurse-patient relationship is positively related to service quality but the consideration of suffering at work reduce the positive impact. At the same time, it was verified the significant but negative relation between suffering and both, the nurse-patient relationship and the service quality as was previously hypothesized.
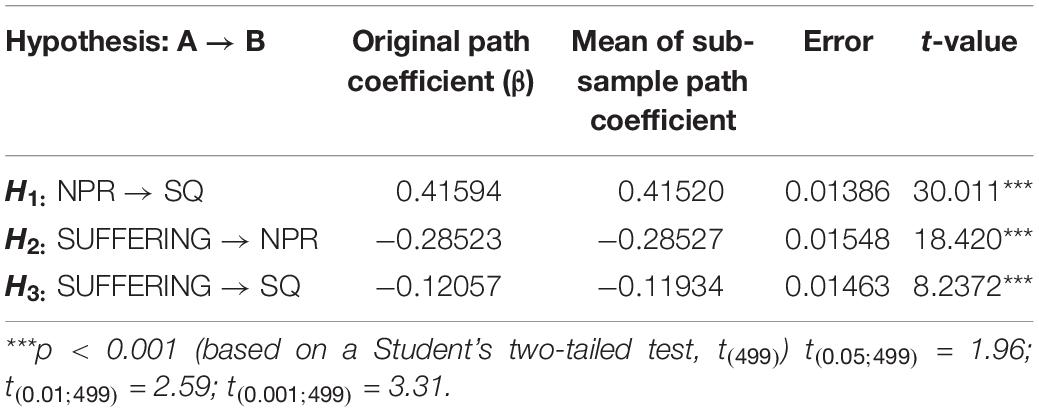
Table 3. Hypotheses testing.
Discussion and Conclusion
Health religious organizations offer professional and spiritual attention to their patients but suffering at the workplace exists, and often at the cost of service quality. In this work the nurse-patient relationship has been empirically explored through two complementary models. The first hypothesis of the study was verified in Model A when testing the direct and positive link between nurse-patient relationship and service quality. The results obtained from the second model, Model B, served for a twofold purpose.
On the first hand, it confirms that suffering at work exists even in good places to work for, and even in religious organizations such as Santa Elena Clinic, with high levels of job satisfaction in their staff. That is in line to the consideration of suffering in the workplace as a more common occurrence than expected. On the second hand, results from Model B confirm previous works defending that suffering causes a significant impact on organizations (Briner, 1999; de Vries, 2004; Peltier, 2011). In our case, and confirming our hypotheses, there is a negative impact of suffering on nurse-patient relationship and also on service quality.
We can conclude that health-care personal in religious clinics, will have difficulties in meeting the needs of their patients and providing the best service to them if their own needs are not previously met as well. The novelty of this work is the study of suffering at work in a specific institution where, a priori, nurse-patient interaction is spiritual and therapeutically good, job satisfaction of nurses is high, and the organization presents high service quality standards. Even in this situation, suffering at work appears and negatively impacts both constructs, nurse-patient relationship and service quality. Thus, human resources responsible in healthcare institutions have to start considering measuring and managing suffering at work in order to improve the places to work for and the quality of their care systems.
The results of this research contribute to the literature on suffering at work among nursing staff in healthcare religious organizations by enhancing the understanding of its influence on the nurse-patient relationship and the final health service quality. This study offers new policy insight for healthcare human resource managers who seek to increase service quality among their nursing staff. Managers grasping the importance of suffering at work affecting the well-being of nurses will be more likely to gain improved service quality.
Some recommendations in terms of the Human Resources Management policies in health religious organizations emerge. Assuming that behavior is often the result of conscious and unconscious mental processes, suffering at work must be taken into account when managing personnel to guarantee the quality of the final service. In line with, it should be highly innovative the implementation of questionnaires. The first reason should be accepting a visibility tool for managing suffering. The tool will measure the potential imbalance between what the nurse has to do and what is receiving from its immediate environment causing suffering.
Secondly, the implementation of an appropriate system to measure suffering at work will serve for understanding the phenomena, and for helping nurses to reflect on their emotions when attending patients in order to improve the final healthcare quality system. In the same line, other highly recommended tool according to literature review should be the implementation of mindfulness programs at work (Glomb et al., 2011) because mindfulness training has been shown to be effective in reducing suffering and enhancing psychological wellbeing (Burton et al., 2017) because health religious organizations must be “healthy organizations” as well.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
MS-H searched and reviewed the study, analyzed the data, wrote the manuscript, and supervised research process. EG-T performed the data collection. EG-T, JL-F, and JF-F critically reviewed the manuscript. All authors contributed to data interpretation and approved the final version of the manuscript for submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to extend our sincere thanks to the Management Team of the participating hospital (Clínica Santa Elena) for their valuable collaboration and all the nurses who participated in this study. We are also grateful to the Comillas Pontifical University Chair in Economics and Business Ethics, the Regional Government of Extremadura (Research group SEJ021 and Project IB16024 by the VI Action Plan 2017–2020) and the European Funds (FSE and FEDER). Furthermore, we would like to thank the reviewers who contributed their valuable time and effort to improve the article’s quality with much appreciated suggestions and comments.
References
Adeb-Saeedi, J. (2002). Stress amongst emergency nurses. Austr. Emerg. Nurs. J. 5, 19–24. doi: 10.1016/s1328-2743(02)80015-3
Alimoglu, M. K., and Donmez, L. (2005). Daylight exposure and the other predictors of burnout among nurses in a University Hospital. Int. J. Nurs. Stud. 42, 549–555. doi: 10.1016/j.ijnurstu.2004.09.001
Ariza-Montes, A., Giorgi, G., Leal-Rodríguez, A., and Ramírez-Sobrino, J. (2017). Authenticity and subjective wellbeing within the context of a religious organization. Front. Psychol. 8:1228. doi: 10.3389/fpsyg.2017.01228
Ariza-Montes, A., Leal-Rodríguez, A. L., Ramírez-Sobrino, J., and Molina-Sánchez, H. (2019). Safeguarding health at the workplace: a study of work engagement, authenticity and subjective wellbeing among religious workers. Intern. J. Environ. Res. Public Health 16:3016. doi: 10.3390/ijerph16173016
Bontemps, S., Barlet-Ghaleb, C., Mediouni, Z., Besse, C., Bonsack, C., Wild, P., et al. (2018). Long title: protocol for evaluating a consultation for suffering at work in french-speaking Switzerland. Contemp. Clin. Trials Commun. 9, 71–76. doi: 10.1016/j.conctc.2017.12.002
Briner, R. B. (1999). The neglect and importance of emotion at work. Eur. J. Work Organ. Psychol. 8, 323–346. doi: 10.1080/135943299398212
Burton, A., Burgess, C., Dean, S., Koutsopoulou, G. Z., and Hugh-Jones, S. (2017). How effective are mindfulness-based interventions for reducing stress among healthcare professionals? A systematic review and meta-analysis. Stress Health 33, 3–13. doi: 10.1002/smi.2673
Cassell, E. J. (1982). The nature of suffering and the goals of medicine. New Engl. J. Med. 306, 639–645.
Chalofsky, N. (2003). An emerging construct of meaningful work. Hum. Resour. Dev. Intern. 6, 69–83. doi: 10.1080/1367886022000016785
Cheng, G. H. L., and Chan, D. K. S. (2008). Who suffers more from job insecurity? A meta-analytic review. Appl. Psychol. 57, 272–303. doi: 10.1111/j.1464-0597.2007.00312.x
Choi, S. L., Goh, C. F., Adam, M. B. H., and Tan, O. K. (2016). Transformational leadership, empowerment, and job satisfaction: the mediating role of employee empowerment. Hum. Resour. Health 14:73.
Chowdhary, N., and Prakash, M. (2007). Prioritizing service quality dimensions. Manag. Serv. Q. Intern. J. 17, 493–509. doi: 10.1108/09604520710817325
Clarke, N., and Mahadi, N. (2017). The significance of mutual recognition respect in mediating the relationships between trait emotional intelligence, affective commitment and job satisfaction. Pers. Individ. Differ. 105, 129–134. doi: 10.1016/j.paid.2016.09.028
Connelly, J. E. (2009). The avoidance of human suffering. Perspect. Biol. Med. 52, 381–391. doi: 10.1353/pbm.0.0095
Coulehan, J. (2018). “Suffering, hope, and healing,” in Handbook of Pain And Palliative Care, ed. R. J. Moore (Cham: Springer), 739–753. doi: 10.1007/978-3-319-95369-4_35
Czander, W. M. (1993). The Psychodynamics Of Work And Organizations: Theory And Application. New York, NY: Guilford Press.
de Vries, M. K. (2004). Organizations on the couch: a clinical perspective on organizational dynamics. Eur. Manag. J. 22, 183–200.
Diamond, M., and Allcorn, S. (2003). The cornerstone of psychoanalytic organizational analysis: psychological reality, transference and counter-transference in the workplace. Hum. Relat. 56, 491–514. doi: 10.1177/0018726703056004005
Dominguez-Gomez, E., and Rutledge, D. N. (2009). Prevalence of secondary traumatic stress among emergency nurses. J. Emerg. Nurs. 35, 199–204. doi: 10.1016/j.jen.2008.05.003
Duggleby, W., Cooper, D., and Penz, K. (2009). Hope, self-efficacy, spiritual well-being and job satisfaction. J. Adv. Nurs. 65, 2376–2385. doi: 10.1111/j.1365-2648.2009.05094.x
Egan, T. M., Yang, B., and Bartlett, K. R. (2004). The effects of organizational learning culture and job satisfaction on motivation to transfer learning and turnover intention. Hum. Resour. Dev. Q. 15, 279–301. doi: 10.1002/hrdq.1104
Egnew, T. R. (2005). The meaning of healing: transcending suffering. Ann. Fam. Med. 3, 255–262. doi: 10.1370/afm.313
Ellinger, A. D., Ellinger, A. E., Bachrach, D. G., Wang, Y. L., and Elmadağ Baş, A. B. (2011). Organizational investments in social capital, managerial coaching, and employee work-related performance. Manag. Learn. 42, 67–85. doi: 10.1177/1350507610384329
Elpern, E. H., Covert, B., and Kleinpell, R. (2005). Moral distress of staff nurses in a medical intensive care unit. Am. J. Crit. Care 14, 523–530. doi: 10.4037/ajcc2005.14.6.523
Ernst, M. E., Franco, M., Messmer, P. R., and Gonzalez, J. L. (2004). Nurses’ job satisfaction, stress, and recognition in a pediatric setting. Pediatr. Nurs. 30, 219–228.
Fornell, C., and Bookstein, F. L. (1982). Two structural equation models: LISREL and PLS applied to consumer exit-voice theory. J. Mark. Res. 19, 440–452. doi: 10.1177/002224378201900406
Gazioglu, S., and Tansel, A. (2006). Job satisfaction in britain: individual and job related factors. Appl. Econ. 38, 1163–1171. doi: 10.1080/00036840500392987
Gismera, E., Fernández, J. L., Labrador, J., and Gismera, L. (2019). Suffering at work: a challenge for corporate sustainability in the spanish context. Sustainability 11:4152. doi: 10.3390/su11154152
Glickman, S. W., Baggett, K. A., Krubert, C. G., Peterson, E. D., and Schulman, K. A. (2007). Promoting quality: the health-care organization from a management perspective. Int. J. Qual. Health Care 19, 341–348. doi: 10.1093/intqhc/mzm047
Glomb, T. M., Duffy, M. K., Bono, J. E., and Yang, T. (2011). Mindfulness at work. Res. Pers. Hum. Resour. Manag. 30, 115–157.
Guillén, M., Ferrero, I., and Hoffman, W. M. (2015). The neglected ethical and spiritual motivations in the workplace. J. Bus. Ethics 128, 803–816. doi: 10.1007/s10551-013-1985-7
Gummesson, E., Mele, C., Polese, F., Gummesson, E., and Grönroos, C. (2012). The emergence of the new service marketing: nordic school perspectives. J. Serv. Manag. 23, 479–497. doi: 10.1108/09564231211260387
Häggström, E., Skovdahl, K., Fläckman, B., Kihlgren, A. L., and Kihlgren, M. (2005). Work satisfaction and dissatisfaction–caregivers’ experiences after a two-year intervention in a newly opened nursing home. J. Clin. Nurs. 14, 9–19. doi: 10.1111/j.1365-2702.2004.00977.x
Hirigoyen, M. F. (2008). Las Nuevas Soledades: El reto de las Relaciones Personales En El Mundo De Hoy. Barcelona: Paidós Ibérica.
Isaac, T., Zaslavsky, A. M., Cleary, P. D., and Landon, B. E. (2010). The relationship between patients’ perception of care and measures of hospital quality and safety. Health Serv. Res. 45, 1024–1040. doi: 10.1111/j.1475-6773.2010.01122.x
Jennings, B. M. (2008). “Work stress and burnout among nurses: role of the work environment and working conditions,” in Patient Safety and Quality: An Evidence Based Handbook for Nurses, ed. R. G. Hughes (Rockville, MD: Agency for Healthcare Research and Quality), 137–158.
Judge, T. A., and Kinger, R. (2007). “Job satisfaction: subjective well-being at work,” in The Science Of Subjective Well-Being, eds M. Eid and R. Larsen (New York, NY: Guilford Publications).
Khamisa, N., Peltzer, K., and Oldenburg, B. (2013). Burnout in relation to specific contributing factors and health outcomes among nurses: a systematic review. Intern. J. Environ. Res. Public Health 10, 2214–2240. doi: 10.3390/ijerph10062214
Kitapci, O., Akdogan, C., and Dortyol, I. T. (2014). The impact of service quality dimensions on patient satisfaction, repurchase intentions and word-of-mouth communication in the public healthcare industry. Proc. Soc. Behav. Sci. 148, 161–169. doi: 10.1016/j.sbspro.2014.07.030
Landrum, H., Zhang, X., Prybutok, V., and Peak, D. (2009). Measuring IS system service quality with SERVQUAL: users’ perceptions of relative importance of the five SERVPERF dimensions. Inform. Sci. 12:426.
Lee, H., Delene, L. M., Bunda, M. A., and Kim, C. (2000). Methods of measuring health-care service quality. J. Bus. Res. 48, 233–246.
Locke, E. A. (1976). “The nature and causes of job satisfaction,” in Handbook of Industrial And Organizational Psychology, ed. M. D. Dunnette (Chicago: Rand McNally), 1297–1349.
Malach-Pines, A. (2000). Nurses’ burnout: an existential psychodynamic perspective. J. Psychosoc. Nurs. Ment. Health Serv. 38, 23–31.
Meesala, A., and Paul, J. (2018). Service quality, consumer satisfaction and loyalty in hospitals: thinking for the future. J. Retail. Consum. Serv 40, 261–269. doi: 10.1016/j.jretconser.2016.10.011
Mok, E., and Chiu, P. C. (2004). Nurse–patient relationships in palliative care. J. Adv. Nurs. 48, 475–483. doi: 10.1111/j.1365-2648.2004.03230.x
Montoya-Juarez, R., Garcia-Caro, M. P., Campos-Calderon, C., Schmidt-RioValle, J., Gomez-Chica, A., Marti-García, C., et al. (2013). Psychological responses of terminally ill patients who are experiencing suffering: a qualitative study. Int. J. Nurs. Stud. 50, 53–62. doi: 10.1016/j.ijnurstu.2012.08.016
Mosadeghrad, A. M. (2014). Factors influencing healthcare service quality. Intern. J. Health Policy Manag. 3, 77–89. doi: 10.15171/ijhpm.2014.65
Moyle, W. (2003). Nurse–patient relationship: a dichotomy of expectations. Intern. J. Ment. Health Nurs. 12, 103–109. doi: 10.1046/j.1440-0979.2003.00276.x
Munir, F., Nielsen, K., Garde, A. H., Albertsen, K., and Carneiro, I. G. (2012). Mediating the effects of work–life conflict between transformational leadership and health-care workers’ job satisfaction and psychological wellbeing. J. Nurs. Manag. 20, 512–521. doi: 10.1111/j.1365-2834.2011.01308.x
Noon, M., Blyton, P., and Morrell, K. (2013). The Realities Of Work: Experiencing Work And Employment In Contemporary Society. London: Macmillan International Higher Education.
Ortiz-Gómez, M., Ariza-Montes, A., and Molina-Sánchez, H. (2020). Human values and work engagement: the mediating role of authenticity among workers in a spanish religious organization. Front. Psychol. 11:76. doi: 10.3389/fpsyg.2017.076
Peltier, B. (2011). The Psychology Of Executive Coaching: Theory And Application. Milton Park: Taylor & Francis.
Pompili, M., Rinaldi, G., Lester, D., Girardi, P., Ruberto, A., and Tatarelli, R. (2006). Hopelessness and suicide risk emerge in psychiatric nurses suffering from burnout and using specific defense mechanisms. Arch. Psychiatr. Nurs. 20, 135–143. doi: 10.1016/j.apnu.2005.12.002
Prins, S. (2006). The psychodynamic perspective in organizational research: making sense of the dynamics of direction setting in emergent collaborative processes. J. Occup. Organ. Psychol. 79, 335–355. doi: 10.1348/096317906x105724
Probst, T. M., and Lawler, J. (2006). Cultural values as moderators of employee reactions to job insecurity: the role of individualism and collectivism. Appl. Psychol. Intern. Rev. 55, 234–254. doi: 10.1111/j.1464-0597.2006.00239.x
Quick, J. C., and Henderson, D. F. (2016). Occupational stress: preventing suffering, enhancing wellbeing. Intern. J. Environ. Res. Public Health 13:459. doi: 10.3390/ijerph13050459
Snipes, R. L., Oswald, S. L., LaTour, M., and Armenakis, A. A. (2005). The effects of specific job satisfaction facets on customer perceptions of service quality: an employee-level analysis. J. Bus. Res. 58, 1330–1339. doi: 10.1016/j.jbusres.2004.03.007
Steenkamp, P. L., and Basson, J. S. (2013). A meaningful workplace: framework, space and context. HTS Teol. Stud. 69, 1–9.
Taylor, S., White, B., and Muncer, S. (1999). Nurses’ cognitive structural models of work-based stress. J. Adv. Nurs. 29, 974–983. doi: 10.1046/j.1365-2648.1999.00980.x
Tetrick, L. E., and Quick, J. C. (2003). “Prevention at work: public health in occupational settings,” in Handbook of Occupational Health Psychology, eds J. C. Quick and L. E. Tetrick (Worcester, MA: American Psychological Association), 3–17. doi: 10.1037/10474-001
Tzeng, H. M. (2002). The influence of nurses’ working motivation and job satisfaction on intention to quit: an empirical investigation in Taiwan. Int. J. Nurs. Stud. 39, 867–878. doi: 10.1016/s0020-7489(02)00027-5
United States Conference of Catholic Bishops (2001). Ethical and Religious Directives for Catholic Health Care Services, 4th Edn, Washington, DC: United States Conference of Catholic Bishops.
Utriainen, K., and Kyngäs, H. (2009). Hospital nurses’ job satisfaction: a literature review. J. Nurs. Manag. 17, 1002–1010. doi: 10.1111/j.1365-2834.2009.01028.x
Keywords: health, hospitals, quality, nurse-patient relationship, religious organizations, suffering
Citation: Sánchez-Hernández MI, Gismera-Tierno E, Labrador-Fernández J and Fernández-Fernández JL (2020) Encountering Suffering at Work in Health Religious Organizations: A Partial Least Squares Path Modeling Case-Study. Front. Psychol. 11:1424. doi: 10.3389/fpsyg.2020.01424
Received: 31 March 2020; Accepted: 27 May 2020;
Published: 23 June 2020.
Edited by:
Antonio Ariza-Montes, Universidad Loyola Andalucía, SpainReviewed by:
Luísa Carvalho, Instituto Politecnico de Setubal (IPS), PortugalNuria Huete-Alcocer, University of Castilla–La Mancha, Spain
Maria Conceição Rego, University of Evora, Portugal
Copyright © 2020 Sánchez-Hernández, Gismera-Tierno, Labrador-Fernández and Fernández-Fernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Isabel Sánchez-Hernández, aXNhbmNoZXpAdW5leC5lcw==