 Astrid Roeh1*
Astrid Roeh1* Rolf R. Engel1Moritz Lembeck1
Rolf R. Engel1Moritz Lembeck1 Benjamin Pross1*
Benjamin Pross1* Irina Papazova1Julia Schoenfeld2
Irina Papazova1Julia Schoenfeld2 Martin Halle2
Martin Halle2 Peter Falkai1Johannes Scherr2,3*
Peter Falkai1Johannes Scherr2,3* Alkomiet Hasan1,4*
Alkomiet Hasan1,4*- 1Department of Psychiatry and Psychotherapy, University Hospital, LMU Munich, Munich, Germany
- 2Department of Prevention and Sports Medicine, Klinikum Rechts der Isar, Technischen Universität München, Munich, Germany
- 3University Center for Preventive and Sports Medicine, Balgrist University Hospital, University of Zurich, Zurich, Switzerland
- 4Department of Psychiatry, Psychotherapy and Psychosomatics of the University Augsburg, Bezirkskrankenhaus Augsburg, University of Augsburg, Augsburg, Germany
Background: Endurance exercise in general and marathon running in particular have become increasingly popular over the past decades. Recent investigations about personality structures in this cohort and comparisons to non-active cohorts are lacking.
Methods: In the ReCaP study (Running effects on Cognition and Plasticity), a total of 100 marathon runners and 46 sedentary controls were recruited. After elimination of Minnesota Multiphasic Personality Inventory 2 Restructured Form (MMPI-2-RF) profiles with insufficient validity, 79 marathon runners (MA) and 27 sedentary controls (SC) remained for final analyses. Depressive symptoms were evaluated with Beck Depression Inventory (BDI) and Hamilton Depression Scale (HAMD).
Results: Marathon runners had lower scores in scales measuring somatic and cognitive complaints, stress, demoralization, hopelessness and distrust. Within the marathon group, committed runners exhibited hypomanic traits compared to regular runners.
Discussion and Conclusion: Personality differences could be summarized as (sub-)depressive personality traits in SC compared to MA rather than typical (sub-) depressive symptoms in the meaning of depressive disorders. Future studies should further evaluate cause and consequence of endurance training and hypomanic or euthymic symptoms, as a two-way interaction exists.
Trial Registration: http://apps.who.int/trialsearch/Trial2.aspx?TrialID=DRKS00012496.
Introduction
Endurance training and competitions like marathon running have become increasingly popular over the past decades. The beneficial effects of regular exercise training on the cardiovascular system are well-established (Praet and van Loon, 2009; Dimeo et al., 2012). In somatic and neuropsychiatric diseases, regular physical exercise has been shown to prevent depressive symptoms (Schuch et al., 2018; Roeh et al., 2019b) and improve cognitive symptoms (Buchman et al., 2012).
Regarding the psychological aspects of physical activity and especially of marathon running, consistent findings are lacking. Prior research aimed at identifying specific personality traits of committed runners. Different personality questionnaires and definitions were used, the most popular representing personality traits according to the Big Five Model or modifications (Goldberg, 1993). Committed marathon runners scored similar to the general population on the 16 personality factor (PF) questionnaire (McLeavey et al., 1984). It was assumed that (ultra-) marathon runners participate in the sport for several reasons, pointing toward specific personality traits (e.g., openness) in this cohort: a sense of achievement, a challenge, the opportunity to extend current capabilities, and the opportunity to socialize with other runners and meet people (Hashimoto et al., 2006). Committed athletes (11 h or more training per week) seem to be more extraverted than average sportsmen (less than 4 h training per week) (Egloff and Jan Gruhn, 1996).
Similar, but potentially even more pronounced personality traits regarding running-specific aspects, should be displayed in marathon and ultra-marathon runners. A systematic review of comparisons of ultra-marathon runners with the general population using various different questionnaires [e.g., NEO-Five Factor Inventory (NEO-FFI), Sensation Seeking Scale (SSS), Temperament and Character Inventory (TCI), Ten Item Personality Inventory (TIPI), Minnesota Multiphasic Personality Inventory (MMPI), Flow State Scale (FSS), State Trait Anxiety Inventory (STAI)] found conflicting evidence: in two studies the athletes were described as more self-motivated, more extraverted, open and experience-seeking and less disinhibited (N = 44 and 66 participants) (Rauch et al., 1988; Hughes et al., 2003); but other included studies found the ultra-marathon runners (N = 52 and 22 participants) to be more introverted and more self-transcendent and less cooperative and reward-dependent (Hashimoto et al., 2006; Freund et al., 2013; Roebuck et al., 2018). Another study showed no differences in ultra-marathon runners (N = 50) compared to non-runners using the Self-Motivation Inventory (SMI) and four subscales from the Philosophies of Human Nature (McCutcheon and Yoakum, 1983). In summary, consistent findings of personality traits in the (ultra-) marathon population are still lacking.
A recent narrative review on personality aspects (measured with, e.g., Cattell 16 Personality Factor Questionnaire, Karolinska Scales of Personality (KSP), adjective check list, The Self-Motivation Inventory (SMI), the Philosophies of Human Nature) of marathon runners described this population as having low scores in tension, depression, anger, fatigue and confusion, but high scores in vigor (Morgan and Costill, 1996; Nikolaidis et al., 2018). Many of the included studies and analyses were performed in the 1980s, a time where marathon running was not a trend sport. Moreover, the composition of the running cohort has changed over years from mainly young male to a mixed cohort with more women and aged runners today. This development results in a need for more comprehensive examinations of personality aspects in this newly reassembled cohort (Nikolaidis et al., 2018).
To the best of our knowledge, this is the first study to evaluate the personality traits of marathon runners with different subgroups (e.g., committed runners, sex, age) using the newly developed Minnesota Multiphasic Personality Inventory 2 Restructured Form (MMPI-2-RF) and compare them to age- and gender matched sedentary controls in an exploratory analysis. The revised form offers evaluations with regard to dimensional models of psychopathology and therefore improves categorization of symptoms.
With our design of exercise-specific subgroups in the marathon cohort and the sedentary control group we expect to be able to identify more specifically the personality traits in relation to daily activity. We hypothesized that persons who did marathon running or intend to do so will experience less distress and somatic complaints compared to the non-active group and that these traits will be more pronounced in the most committed runners.
Design and Methods
Subjects
The study population was part of the ReCaP trial (“Running effects on Cognition and Plasticity,” a longitudinal observational study of marathon runners who were registered for the Munich Marathon that took place on October 8th, 2017). The detailed study protocol was previously published (Roeh et al., 2019a).
A total of 146 participants (100 marathon group, 46 sedentary control group) were included in the trial. 116 participants (83 marathon group and 33 sedentary control group) filled out the MMPI-2-RF with less than 16 missing items.
Inclusion criteria for the marathon group (MA) contained an age range between 18 and 60 years, successful registration for Munich Marathon 2017, participants must have completed at least one half-marathon prior to the recent event, sufficient German language skills and written informed consent. Exclusion criteria contained relevant neurological, cardiac or psychiatric diseases, pregnancy and cannabis abuse, BMI > 30 kg/m2.
The sedentary control group (SC) was age- and gender matched with identical exclusion criteria. They were not included in case of participation in a marathon or half-marathon in earlier years. A sedentary lifestyle was defined as less than 25 min of physical activity per day (Cabrera de León et al., 2007). The participants of both groups filled out the questionnaires in person.
Ethics and Registration
The study proceedings agreed with Good Clinical Practice guidelines, the guiding principles of the Declaration of Helsinki 2008, and local laws and regulations. The study protocol had been approved by the ethics committees of both the Ludwig-Maximilians University Munich (approval reference number 17–148) and the Technical University Munich (approval reference number 218/17 S). The study was registered at WHO International Clinical Trials Research platform1 (registration number: DRKS00012496). All participants provided written informed consent prior to inclusion in the study.
Instruments
Personality Traits
Baseline values of personality aspects were assessed via the German translation of the Minnesota Multiphasic Personality Inventory 2 Restructured Form (MMPI-2-RF) (Moultrie and Engel, 2017). Table 1 provides an overview of all measured subscales.
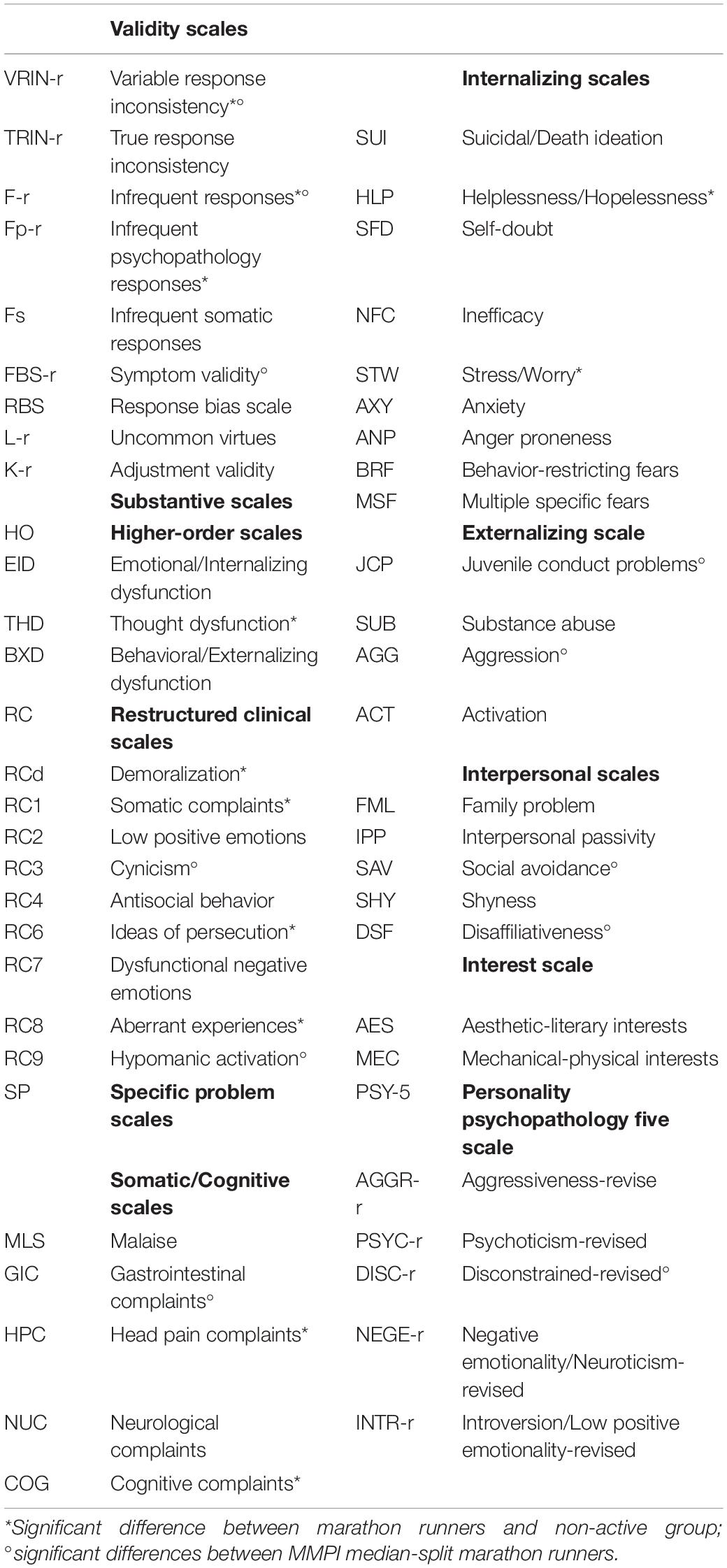
Table 1. MMPI-II RF overview of subscales.
Physical Activity Assessment
We used the International Physical Activity Questionnaire (IPAQ) to present detailed information about daily activity including physical exercise as well as physical activity in daily routines (e.g., usage of the bicycle for work) (Craig et al., 2003). The findings of the questionnaire show high correlation with activity measured with accelerometers (Mäder et al., 2006).
In the marathon runners, we further assessed the physical activity with training protocols about their training history in the 12 weeks prior to the marathon (including mean training kilometers per week and the mean weekly training duration). We collected information about their prior participations in marathon events with questionnaires. Moreover, we measured the endurance capacity with a spiroergometry (performed at visits −1 and 0). The main outcome parameter for our analyses was V02max [milliliters of oxygen used in 1 min per kilogram of body weight (mL/kg/min)].
Mood Questionnaires
Two rating scales for depressive symptoms were included for the here presented analyses. The self-rating scale Beck Depression Inventory (BDI) (Beck et al., 1961) and the observer-rating scale Hamilton Depression Scale (HAMD) (Hamilton, 1960).
Procedures
After comparisons of marathon group versus sedentary control group, we divided the marathon group in two activity-dependent subgroups for further analyses. In literature, no clear definitions of “committed runners” could be identified [one study used less than four and more than 11 weekly training hours (Egloff and Jan Gruhn, 1996)]. Thus, three different exploratory approaches with identical sample sizes were used in our sample: a median-split separation of the marathon population with the International Physical Activity Questionnaire (IPAQ) baseline score (Craig et al., 2003), a median-split separation with the individual marathon finishing time and a median-split separation with the spiroergometry performance expressed as VO2max.
Two further comparisons were included in the analysis: we compared male and female runners and younger and older participants (also using a median-split approach as we could not identify an established age separation in literature concerning the study question).
Statistical Analysis
As all participants were healthy (exclusion criterion of the study: relevant psychiatric disease), the inclusion criteria for final analyses were further restricted with the following validity scales: TRIN-r < 80T (one sedentary control group member (SC) and one marathon member (MA) were excluded); VRIN-r < 80T (one SC and two MA were excluded); F-r < 80T (two SC and one MA were excluded); Fp-r < 80T (5 SC and 3 MA were excluded). Some of these parameters referred to the same participants resulting in an exclusion of 10 participants (6 SC and 4 MA) for final analyses with 106 participants (79 MA, 27 SC) remaining.
All analyses were carried out in SPSS25 (IBM, Armonk, NY, United States), with a significance level of α = 0.05. Differences between groups were assessed using χ2-tests (Fisher’s exact test if> 20% of cells had an expected count < 5), two-sided independent t-tests and in cases of a violation of the normal distribution (Shapiro–Wilk Test, p < 0.05) with Mann–Whitney-U Test. For demographic data, BMI was normally distributed and for MMPI data, K_r, RC3, RC9 and AGGR_r were normally distributed (Shapiro–Wilk Test, p > 0.05).
Only complete datasets for a given dependent variable were analyzed (please see respective tables for the sample sizes for each variable). The tables show mean values and standard deviation.
Results
Baseline demographic results of the included participants and their comparison between marathon and sedentary control group are presented in Table 2. They were similar in educational status, age and gender. Significant differences were found in smoking habits and less pronounced in BMI values. The differences in IPAQ scores were expected due to inclusion criteria.
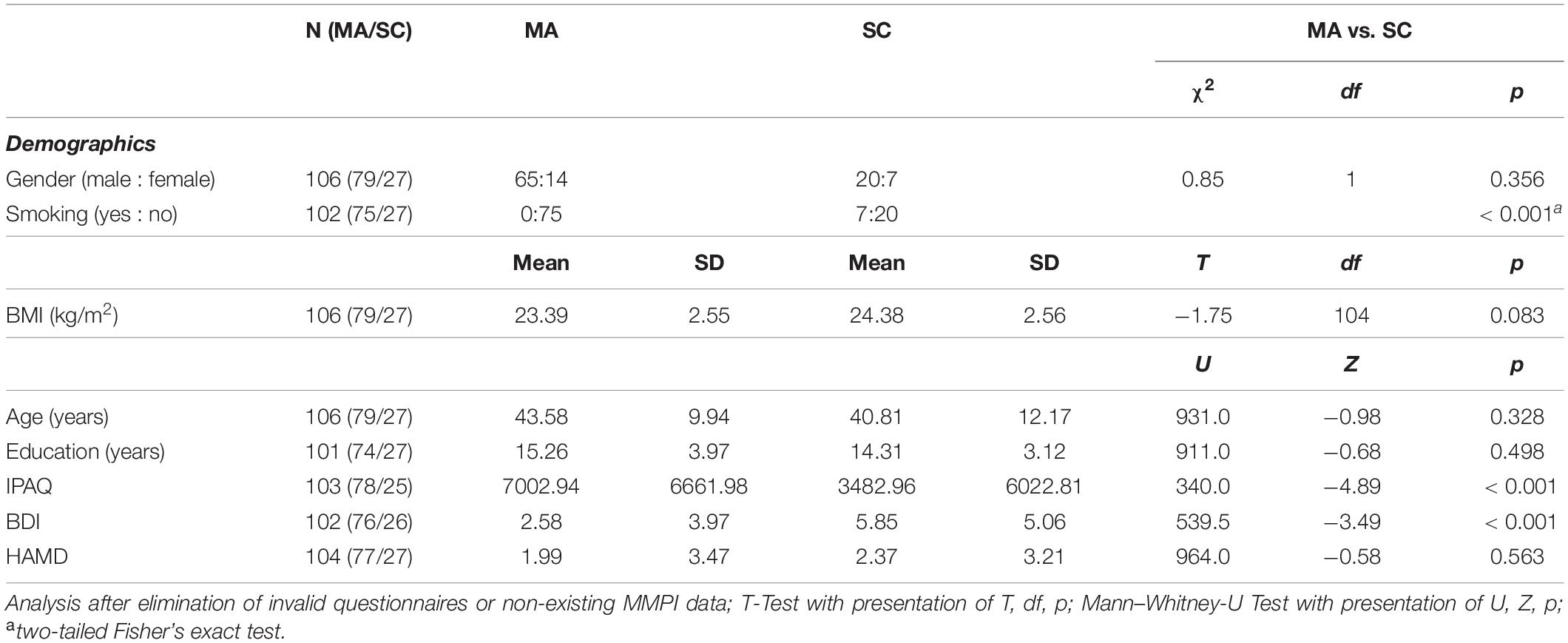
Table 2. Baseline characteristics of marathon group and sedentary controls, MA: marathon group, SC: Sedentary Controls.
Comparison Between Marathon Group and Sedentary Control Group
The results of both the validity and the clinical subscales of MMPI-2 RF with significant differences between both groups are presented in Table 3.
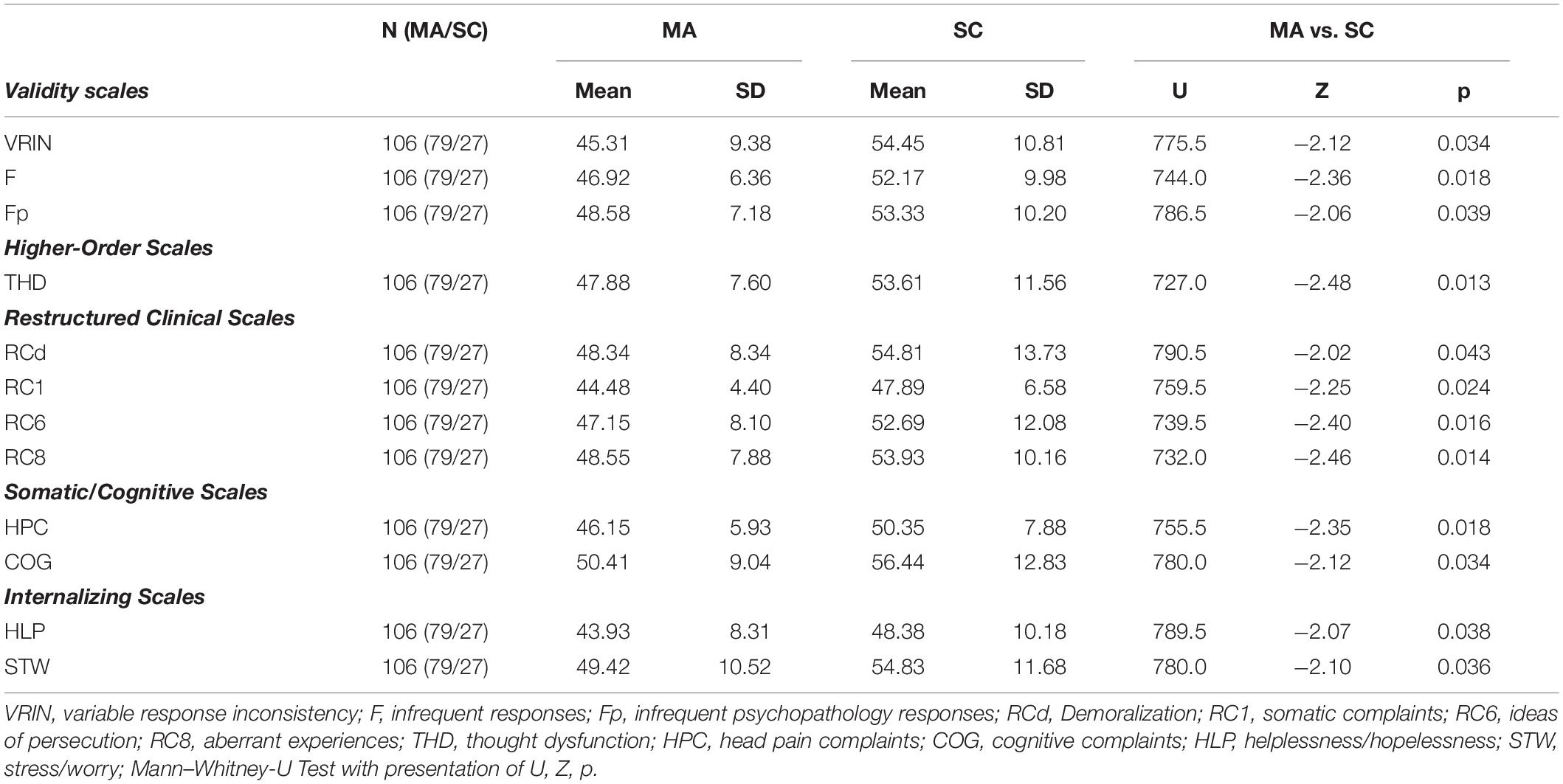
Table 3. Demographics of MMPI scales and comparison between MA (marathon group) and SC (sedentary controls).
Differences between both groups regarding BDI and HAMD scores are shown in Table 2, they only differed in BDI values (self-rating), not in HAMD values (observer-rating). All values were within normal ranges (cut-off for mild depressive disorder is nine points in BDI).
Comparison Within the Marathon Group
Of the 100 included participants, 71 finished the marathon with a median time of 231.84 min (range 167.65 – 346.82). Median instead of mean was presented because of median-split comparison. Of these, 60 provided sufficient MMPI-2 RF data. Of the 100 participants, 92 participants completed the baseline spiroergometry and 78 of this cohort provided sufficient MMPI-2 RF data. Median maximal oxygen uptake was 47.89 ml/kg/min (range 25.4 – 63.5). IPAQ baseline results of 92 participants resulted in a median of 4986.75 MET-minutes per week (Metabolic Equivalent) (range 910.00 – 42360.0). 78 participants remained after application of the above described validity and quality parameters. Of the 79 participants with sufficient MMPI 2 RF data, 77 provided more detailed information about their participation in prior marathon events: 59/77 had already participated in prior marathon events before Munich Marathon 2017 (all participants had prior experience in half marathons, see inclusion criteria). Mean training hours exclusively for running was 4.77 ± 2.27 per week (N = 64) with a mean weekly running frequency of 3.66 ± 1.33 (N = 68). Mean weekly training kilometers were 45.36 ± 21.20 (N = 69).
Results of the comparisons within the marathon population using the marathon finishing time or maximal oxygen uptake in the baseline spiroergometry showed no significant differences between both groups regarding personality aspects. Table 4 displays the personality parameters with significant differences between high- and low performers using the median-split comparison of the baseline IPAQ score. The respective scales were highlighted in Table 1 for better comparability. HAMD and BDI scores showed no significant differences in both median-split IPAQ and finishing time scores.
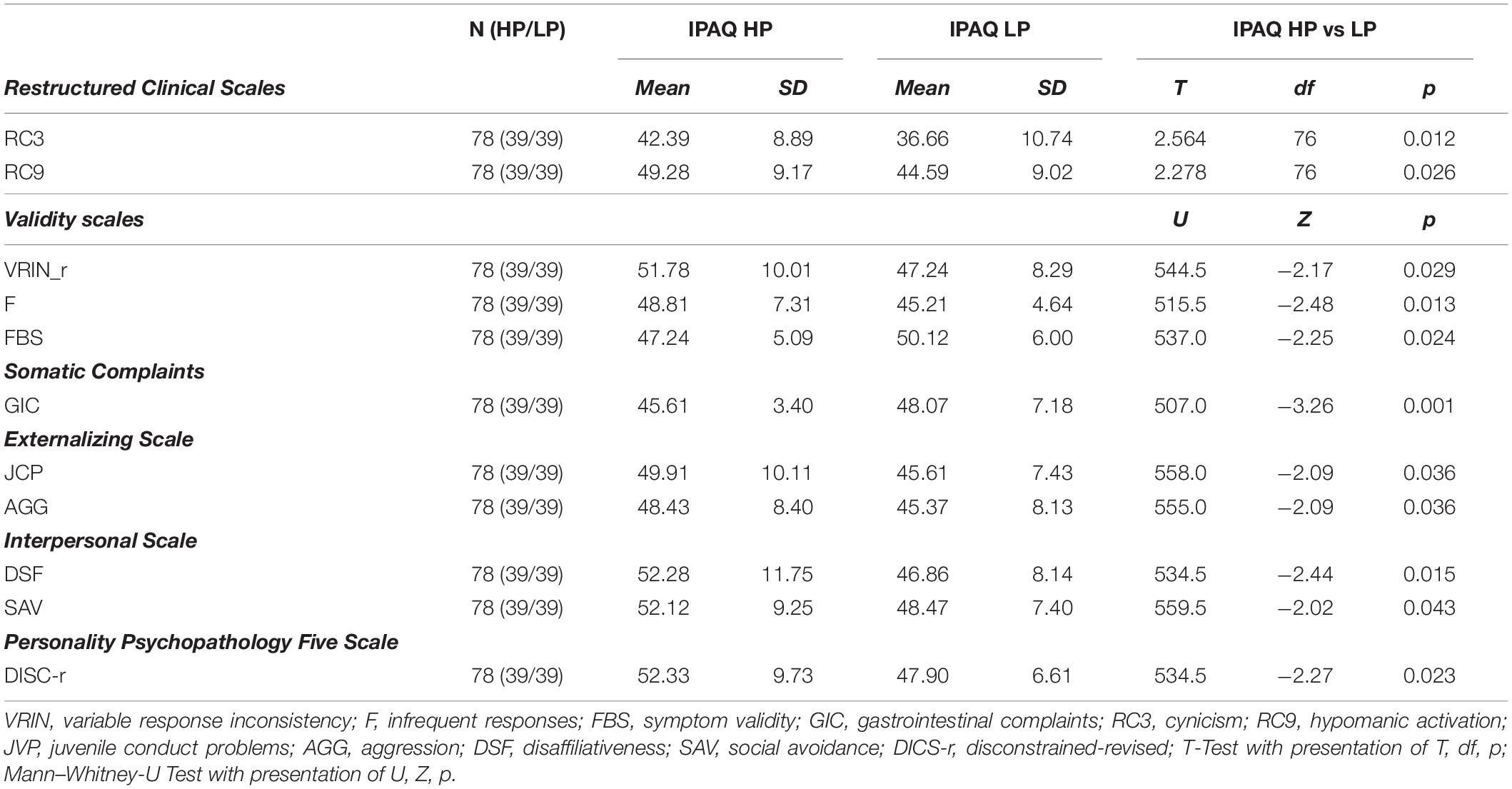
Table 4. Demographics of MMPI scales and comparison between IPAQ HP (high performer) and IPAQ LP (low performer).
To further investigate the effect of gender and age, we performed subsequent analyses. First, we compared the marathon group with regard to differences between male and female runners. Male and female runners (m:f = 65:14) showed differences in age (m:f = 45.14 ± 9.49 : 36.36 ± 9.0, U = 223.5, Z = −2.98, p = 0.002), BMI (m:f = 23.70 ± 2.53 : 21.96 ± 2.20, T = −2.38, df = 77, p = 0.016) and BDI (m:f = 2.0 ± 3.07 : 5.38 ± 3.15, U = 128.5, Z = −3.96, p < 0.001). Please see Table 5 for MMPI results of MMPI scales with male/female.
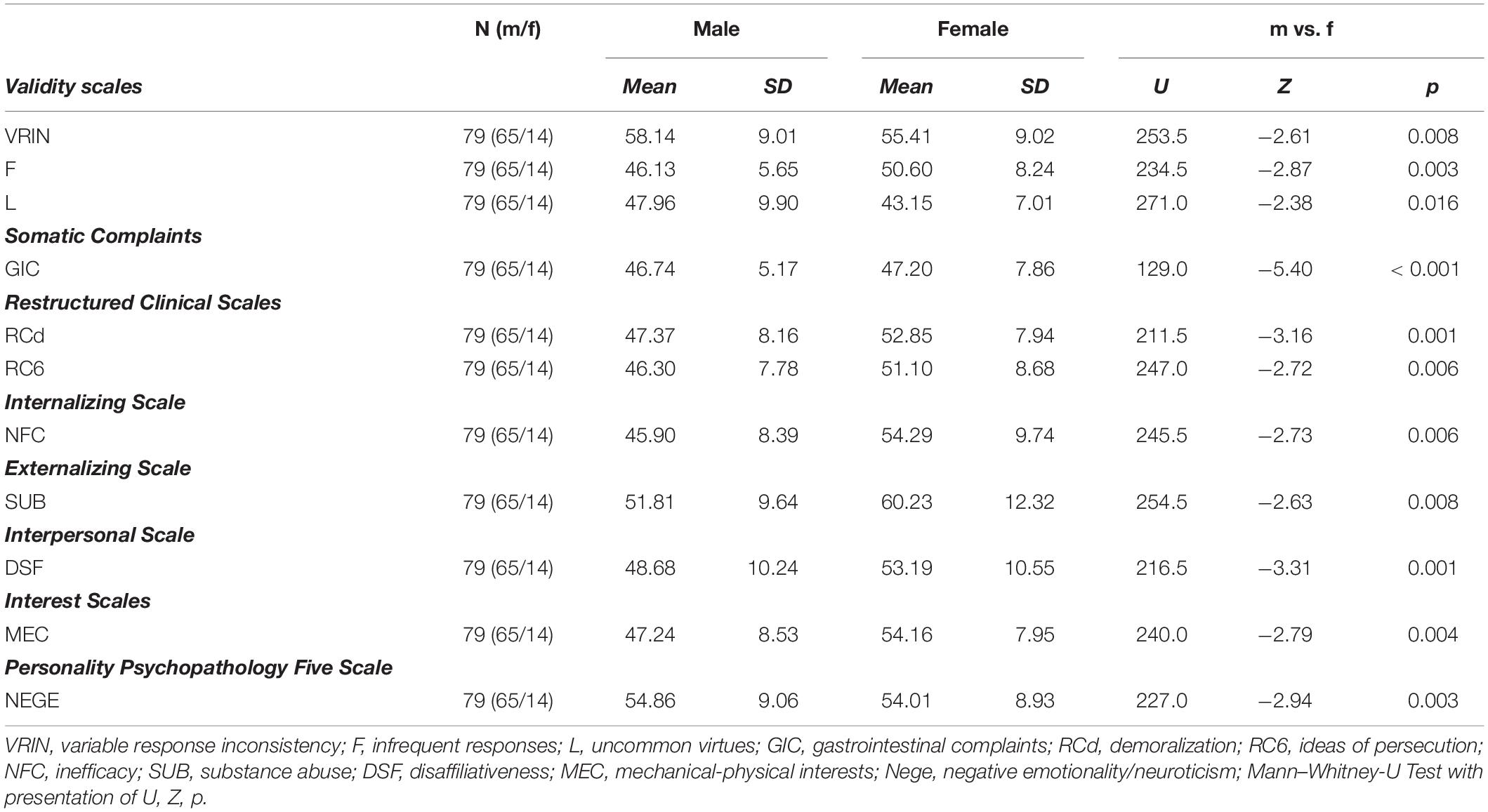
Table 5. Demographics of MMPI scales and comparison between males (m) and females (f) within the marathon group.
Next, we divided our marathon cohort with regard to age using a median-split. Median age of the marathon cohort was 44.0 years (range 23 – 60 years), the younger group was composed of participants aged 23 – 44 years (mean 35.0 ± 5.72 years) and the older group had an age range of 44.1 – 60 years (mean 52.38 ± 3.49 years). Younger and older participants (40:39) differed significantly with regard to the gender distribution [younger group f:m = 11:29 and older group f:m = 3:36, df = 1, p = 0.037 (two-tailed Fisher’s exact test)], but showed no significant differences in the other parameters (BMI, BDI, IPAQ, HAMD, education). Significant differences of MMPI parameters of this comparison are presented in Table 6.
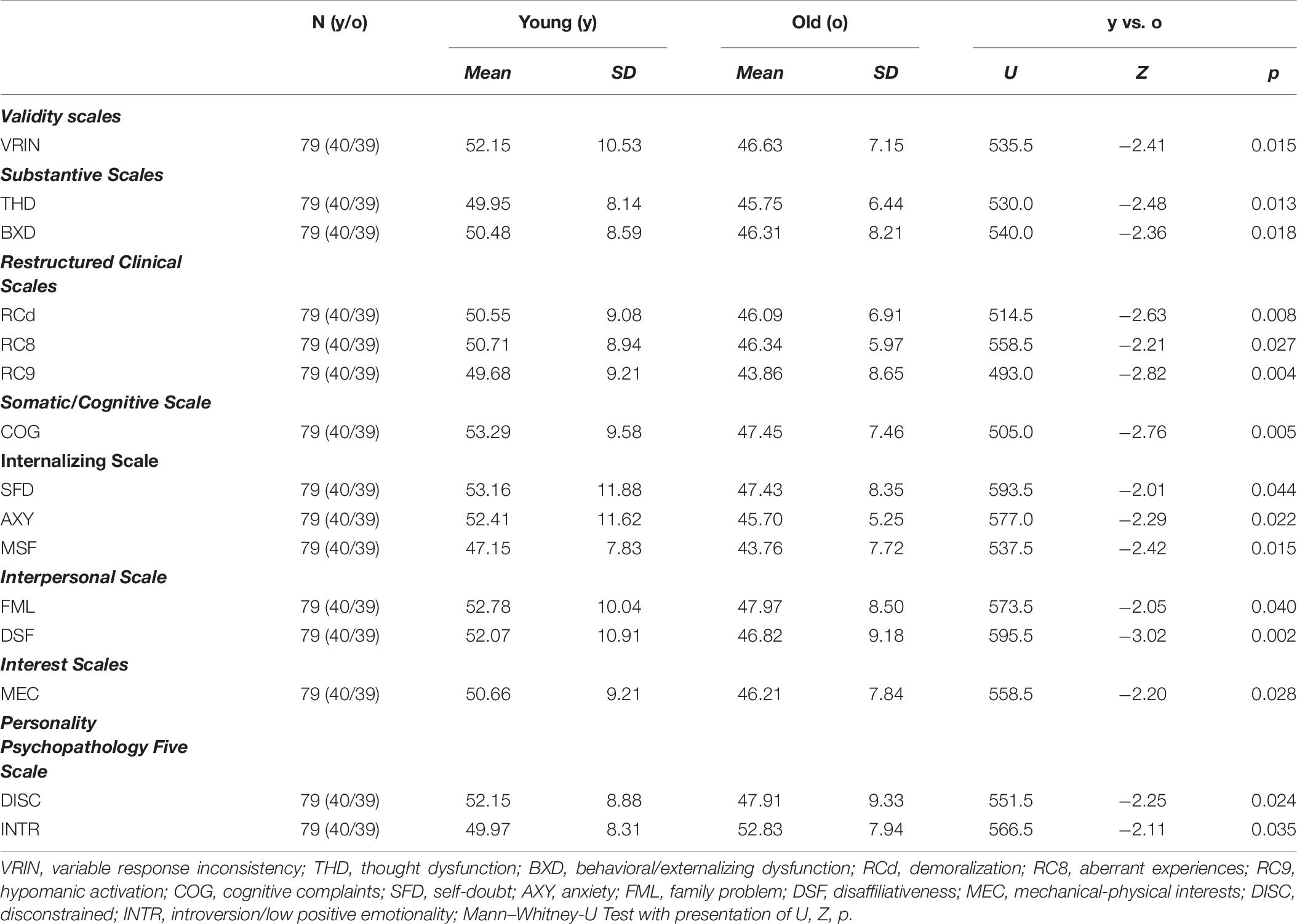
Table 6. Demographics of MMPI scales and comparison between younger (y, 23 – 44 years) and older marathon participants (o, 44.1 – 60 years).
Discussion
In our study, we compared marathon runners with an age- and gender-matched non-active control group in regard to personality aspects using the newly developed MMPI 2 RF (German translation).
We identified three superordinate groups of clinical subscales with differences between marathon runners and sedentary controls: Marathon runners seem to experience less physical and cognitive complaints, as their lower results in the subscales of somatic complaints, head pain complaints, cognitive complaints and thought dysfunction show.
Prior studies identified exercise and physical fitness as a public health resource (Gerber and Pühse, 2009) and exercise is recommended to maintain physical health (Garber et al., 2011), but the tendency toward complaining about physical and cognitive impairments (existing or non-existing) is also part of the personality and can be displayed with the described MMPI scales. The presented studies in our introduction about personality aspects in athletes and especially in (ultra-) marathon runners did not include items with regard to physical and cognitive complaints (Goldberg, 1993; McLeavey et al., 1984; Rauch et al., 1988; Egloff and Jan Gruhn, 1996; Hughes et al., 2003; Hashimoto et al., 2006; Freund et al., 2013).
Possible underlying mechanisms for our observation could be differences in pain perception: Previous studies found higher pain tolerance in endurance athletes [long-distance runners and triathletes, N = 86 (Egloff and Jan Gruhn, 1996), ultra-marathon runners, N = 11 (Freund et al., 2013)]. They argued that the personality trait of extraversion (increased in ultra-/marathon runners) could be associated with lower total resting levels of cortical arousals (Egloff and Jan Gruhn, 1996). As a result, higher levels of sensory stimulation are needed to induce positive/negative (e.g., pain perception) hedonic tone in extraverts. So the pain tolerance seems to be higher in extroverts due to this arousal deficit (Egloff and Jan Gruhn, 1996; Eysenck, 1967; Eysenck et al., 1982). It is still discussed whether the higher (physical) pain tolerance in endurance athletes like ultra-marathon runners is cause or consequence of the training (Freund et al., 2013).
Not only somatic, but also cognitive complaints were lower in our marathon runners compared to the non-active group.
This could be explained with improvements of cognitive function after endurance training due to, e.g., increased neuronal plasticity and better central vascularization (Voss et al., 2013). Moreover, other studies found an association of improved cognitive functioning after exercise in healthy adults (Gomez-Pinilla and Hillman, 2013; Kujach et al., 2018). Another possible explanation could be based on similar observations to the lower pain perception in marathon runners: the lower resting levels of cortical arousal could also lead to a lower sensation of not only somatic, but also cognitive deficits.
The lower results of aberrant experiences (ideas of persecution) point to a less distrustful personality of marathon runners.
When applying this finding to the personality traits in the big-five model, it would represent lower scores of openness, extraversion, conscientiousness, agreeableness and higher scores of neuroticism in the sedentary control group (Shi et al., 2018). Prior research indicated similar results (Hughes et al., 2003; Hashimoto et al., 2006; Freund et al., 2013; Roebuck et al., 2018). Again, this specific outcome was not measured in prior personality studies in athletes or specifically in (ultra-) marathon runners. A Finnish study included the Cynical Distrust Scale in a population-based study and found lower scores of distrust in the exercising group (frequency at least two or three times a week) (Hassmén et al., 2000) supporting our findings of less distrustful personalities in marathon runners. Less distrustful personalities are more open and experience-seeking and with that our results help clarify the conflicting findings of prior studies with ultra-marathon runners: they support two prior studies with similar findings of openness (Rauch et al., 1988; Hughes et al., 2003) and contradict other studies that found ultra-marathon runners to be more introverted (Hashimoto et al., 2006; Freund et al., 2013; Roebuck et al., 2018).
Our marathon runners exhibited lower scores of demoralization, helplessness/hopelessness and stress/worry compared to non-active controls. Prior studies described non-active groups as less self-motivated (Rauch et al., 1988; Hughes et al., 2003), pointing in the same direction without having examined the same scales. Most prior studies about personality traits used a variety of different questionnaires (often NEO-FFI or other questionnaires based on the “Big Five,” (Hughes et al., 2003; Hashimoto et al., 2006; Nikolaidis et al., 2018; Roebuck et al., 2018), so comparability to these studies is limited.
Interestingly, demoralization/helplessness/hopelessness and stress/worry are – beside others, including, e.g., concentration deficits – part of diagnostic criteria of depressive disorders and can coincide with somatic complaints (Kapfhammer, 2006). Regarding personality traits, these factors also contribute to the depressive personality disorder (or accentuation) (Vachon et al., 2009).
When applying these findings to clinical scenarios with psychiatric diagnoses, all three superordinate scales could be summarized with less depressive symptoms or less depressive personality traits in the broadest sense. In clinical practice, psychotic and depressive patients tend to score higher in neuroticism scales and lower in extraversion (Berenbaum and Fujita, 1994; Lewis et al., 2014) and therefore could exhibit similar personality traits.
To further analyze the possible depressive components and differentiate between personality traits and possible depressive disorders, we included the BDI and HAMD scales in our study. The self-rating BDI showed significantly higher scores in the sedentary controls compared to the marathon group (but still with values below the diagnostic cut-off for a manifest mild depressive disorder). The observer-rating scale HAMD on the other hand displayed no significant differences. This discrepancy between reported BDI and observed HAMD ratings has been linked to specific personality traits like high neuroticism and low extraversion in the big five model (Schneibel et al., 2012). This observation again supports earlier findings with higher scores of extraversion in endurance athletes and it points toward depressive personality traits more than objectifiable depressive symptoms in the meaning of depressive disorders (with no difference in HAMD scores between groups and overall values below diagnostic cut-offs in both scales).
We can conclude that we found traits of depressive personalities, but no depressive disorder, in the non-active group compared to the marathon runners.
In a second step we wanted to further analyze differences within the marathon runners (low versus high performer according to median IPAQ score) in order to possibly pronounce these findings. The “high performer” showed higher levels of hypomanic activation, cynicism, juvenile conduct problems, aggression, disaffiliativeness, social avoidance, disconstrained and lower levels of gastrointestinal complaints. Taken together, these traits point to a higher arousal in the high performer group and partly support the findings of prior studies of higher scores of vigor in marathon runners (Nikolaidis et al., 2018). All other scores, including the above described depressive personality traits were similar in both performance groups. This leads to the conclusion that there is a smooth transition between sedentary individuals with a (sub-)depressive personality, “regular runners” in between and hypomanic traits/increased psychological tension in committed runners.
Influence of Sex and Age
As described, the marathon cohorts of the last years consist of more female and aged runners compared to those studies conducted a few decades ago (Nikolaidis et al., 2018), so we performed additional analyses regarding the impact of gender and age on personality traits. Results have to be interpreted cautiously, as the included female runners were significantly younger than the included male runners. We found that the female runners had higher scores of gastrointestinal complaints, demoralization, ideas of persecution, inefficacy, substance abuse, disaffiliativeness and mechanical-physical interests. Prior studies of non-athletes identified remarkably high prevalence rates of gastric and intestinal complaints in women (Avramidou et al., 2018) and gender-differences were established in regard to depressive symptoms being more pronounced in female cohorts (with our higher results of demoralization, disaffiliativeness and inefficacy pointing in the same direction) (Salk et al., 2017). The higher scores of mechanical-physical interests and drug abuse as two personality items of MMPI were more unexpected. Usually, prevalence of drug abuse is higher in men (McHugh et al., 2018). Thus, it may be speculated (similar with mechanical-physical interests) that the here displayed higher scores in these MMPI items can either point to female marathon runners exhibiting some “male” attributes or that these differences are related to the younger mean age of women in our group. Especially, mechanical-physical interests overlap with the age-comparison (with higher scores in the younger group and in the female group with also a younger mean age), so this sex-difference can be explained more likely by age-differences.
In the age-comparison we further identified lower scores of thought dysfunction, behavioral/externalizing dysfunction, demoralization, aberrant experiences, hypomanic activation, cognitive complaints, self-doubt, anxiety, family problem, disaffiliativeness, mechanical-physical interests, disconstrained, introversion/low positive emotionality in the older cohort of marathon runners. Vice versa, the lower percentage of female participants in this cohort has to be taken into account for interpretation especially in the overlapping scales (disaffiliativeness, demoralization, mechanical-physical interests). Other than that, the older marathon cohort seems to have lower scores in the sub-depressive scales (thought dysfunction, self-doubt, anxiety, cognitive complaints) and as well in the vigor-scales (hypomanic activation, behavioral/externalizing dysfunction, family problems and disconstrained). Comparing these results of less sub-depressive symptoms in the male and in the older marathon cohort to one of our main findings (less sub-depressive characteristics in the marathon runners compared to sedentary controls), it may be speculated that the impact of the older runners overweighs the higher proportion of female runners in the younger group. As the composition of marathon groups is still changing, the impact of age and gender on personality analyses in marathon runners need to be explored in more detail in future studies.
As limitation, one should be aware that dichotomizing continuous variables using median split may result in the loss of information especially regarding individual differences. Thus, our analyses should be interpreted with caution (MacCallum et al., 2002).
Conclusion
This is the first study to evaluate personality traits in marathon runners with different performance groups and compare them to age and gender-matched sedentary controls using the newly developed MMPI-2-RF. We found that marathon runners experience less symptoms of somatic and cognitive complaints, less aberrant experiences and less hopelessness. We confirmed personality traits rather than objective depressive symptoms or disorders as underlying etiology. More committed runners did not present more pronounced traits, but higher levels of arousal. In our cohort that included more older runners and females compared to cohorts investigated some decades ago, the impact of these demographic variables explained in parts our personality findings. Future studies should further analyze the two-way interaction of depressive personality traits and endurance training to discriminate cause and effect.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethics committees of both the Ludwig-Maximilians University Munich Ethics committee (approval reference number 17-148) and the Technical University Munich (approval reference number 218/17 S). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AH, JoS, PF, ML, and AR conceptualized the study. AR and RE wrote the first draft of the manuscript. IP, BP, and JuS collected data. AR, AH, and RE made the statistical analyses. All authors revised the manuscript and approved of the final version. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank all participants of the trial and the whole ReCaP study group.
Footnotes
References
Avramidou, M., Angst, F., Angst, J., Aeschlimann, A., Rössler, W., and Schnyder, U. (2018). Epidemiology of gastrointestinal symptoms in young and middle-aged Swiss adults: prevalences and comorbidities in a longitudinal population cohort over 28 years. BMC Gastroenterol. 18:21. doi: 10.1186/s12876-018-0749-3
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., and Erbaugh, J. (1961). An inventory for measuring depression. Arch. Gen. Psychiatry 4, 561–571. doi: 10.1001/archpsyc.1961.01710120031004
Berenbaum, H., and Fujita, F. (1994). Schizophrenia and personality: exploring the boundaries and connections between vulnerability and outcome. J. Abnorm. Psychol. 103, 148–158. doi: 10.1037//0021-843X.103.1.148
Buchman, A. S., Boyle, P. A., Yu, L., Shah, R. C., Wilson, R. S., and Bennett, D. A. (2012). Total daily physical activity and the risk of AD and cognitive decline in older adults. Neurology 78, 1323–1329. doi: 10.1212/WNL.0b013e3182535d35
Cabrera de León, A., Rodríguez-Pérez, M. D. C., Rodríguez-Benjumeda, L. M., Anía-Lafuente, B., Brito-Díaz, B., and Muros de Fuentes, M. (2007). Sedentarismo: tiempo de ocio activo frente a porcentaje del gasto energético [Sedentary lifestyle: physical activity duration versus percentage of energy expenditure]. Revist. Espanola Cardiol. 60, 244–250.
Craig, C. L., Marshall, A. L., Sjöström, M., Bauman, A. E., Booth, M. L., Ainsworth, B. E., et al. (2003). International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35, 1381–1395. doi: 10.1249/01.MSS.0000078924.61453.FB
Dimeo, F., Pagonas, N., Seibert, F., Arndt, R., Zidek, W., and Westhoff, T. H. (2012). Aerobic exercise reduces blood pressure in resistant hypertension. Hypertension 60, 653–658. doi: 10.1161/HYPERTENSIONAHA.112.197780
Egloff, B., and Jan Gruhn, A. (1996). Personality and endurance sports. Pers. Individ. Differ. 21, 223–229. doi: 10.1016/0191-8869(96)00048-7
Eysenck, H. J. (1967). The Biological Basis Of Personality, 1st Edn, Springfield, IL: Charles C Thomas Pub Ltd.
Eysenck, H. J., Nias, D. K. B., and Cox, D. N. (1982). Sport and personality. Adv. Behav. Res. Therapy 4, 1–56. doi: 10.1016/0146-6402(82)90004-2
Freund, W., Weber, F., Billich, C., Birklein, F., Breimhorst, M., and Schuetz, U. H. (2013). Ultra-marathon runners are different: investigations into pain tolerance and personality traits of participants of the TransEurope FootRace 2009. Pain Pract. Offic. J. World Instit. Pain 13, 524–532. doi: 10.1111/papr.12039
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., Lee, I.-M., et al. (2011). American college of sports medicine position stand. quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med. Sci. Sports Exerc. 43, 1334–1359. doi: 10.1249/MSS.0b013e318213fefb
Gerber, M., and Pühse, U. (2009). Review article: do exercise and fitness protect against stress-induced health complaints? A review of the literature. Scand. J. Public Health 37, 801–819. doi: 10.1177/1403494809350522
Goldberg, L. R. (1993). The structure of phenotypic personality traits. Am. Psychol. 48, 26–34. doi: 10.1037/0003-066x.48.1.26
Gomez-Pinilla, F., and Hillman, C. (2013). The influence of exercise on cognitive abilities. Comprehens. Physiol. 3, 403–428. doi: 10.1002/cphy.c110063
Hamilton, M. (1960). A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 23, 56–62. doi: 10.1136/jnnp.23.1.56
Hashimoto, M., Hagura, N., Kuriyama, T., and Nishiyamai, M. (2006). Motivations and psychological characteristics of Japanese ultra-marathon runners using Myers-Briggs type indicator. Jpn. J. Health Hum. Ecol 72, 15–24. doi: 10.3861/jshhe.72.15
Hassmén, P., Koivula, N., and Uutela, A. (2000). Physical exercise and psychological well-being: a population study in Finland. Prevent. Med. 30, 17–25. doi: 10.1006/pmed.1999.0597
Hughes, S., Case, H. S., Stuempfle, K., and Evans, D. (2003). Personality profiles of iditasport ultra-marathon participants. J. Appl. Sport Psychol. 15, 256–261. doi: 10.1080/10413200305385
Kujach, S., Byun, K., Hyodo, K., Suwabe, K., Fukuie, T., Laskowski, R., et al. (2018). A transferable high-intensity intermittent exercise improves executive performance in association with dorsolateral prefrontal activation in young adults. Neuroimage 169, 117–125. doi: 10.1016/j.neuroimage.2017.12.003
Lewis, G. J., Bates, T. C., Posthuma, D., and Polderman, T. J. C. (2014). Core dimensions of personality broadly account for the link from perceived social support to symptoms of depression and anxiety. J. Pers. 82, 329–339. doi: 10.1111/jopy.12064
MacCallum, R. C., Zhang, S., Preacher, K. J., and Rucker, D. D. (2002). On the practice of dichotomization of quantitative variables. Psychol. Methods 7, 19–40. doi: 10.1037/1082-989x.7.1.19
Mäder, U., Martin, B. W., Schutz, Y., and Marti, B. (2006). Validity of four short physical activity questionnaires in middle-aged persons. Med. Sci. Sports Exerc. 38, 1255–1266. doi: 10.1249/01.mss.0000227310.18902.28
McCutcheon, L. E., and Yoakum, M. E. (1983). Personality attributes of ultramarathoners. J. Pers. Assess. 47, 178–180. doi: 10.1207/s15327752jpa4702_13
McHugh, R. K., Votaw, V. R., Sugarman, D. E., and Greenfield, S. F. (2018). Sex and gender differences in substance use disorders. Clin. Psychol. Rev. 66, 12–23. doi: 10.1016/j.cpr.2017.10.012
McLeavey, B. C., Corkery, M. B., and Cronin, T. E. (1984). The marathon runner: profile of health or vulnerable personality? Irish Med. J. 77, 37–39.
Morgan, W. P., and Costill, D. L. (1996). Selected psychological characteristics and health behaviors of aging marathon runners: a longitudinal study. Int. J. Sports Med. 17, 305–312. doi: 10.1055/s-2007-972852
Moultrie, J. K., and Engel, R. R. (2017). Empirical correlates for the minnesota multiphasic personality inventory-2-restructured form in a german inpatient sample. Psychol. Assess. 29, 1273–1289. doi: 10.1037/pas0000415
Nikolaidis, P. T., Rosemann, T., and Knechtle, B. (2018). A brief review of personality in marathon runners: the role of sex, age and performance level. Sports 6:99. doi: 10.3390/sports6030099
Praet, S. F. E., and van Loon, L. J. C. (2009). Exercise therapy in type 2 diabetes. Acta Diabetol. 46, 263–278. doi: 10.1007/s00592-009-0129-0
Rauch, T. M., Tharion, W. J., Strowman, S. R., and Shukitt, B. L. (1988). Psychological factors associated with performance in the ultramarathon. J. Sports Med. Phys. Fitness 28, 237–246.
Roebuck, G. S., Fitzgerald, P. B., Urquhart, D. M., Ng, S.-K., Cicuttini, F. M., and Fitzgibbon, B. M. (2018). The psychology of ultra-marathon runners: a systematic review. Psychol. Sport Exerc. 37, 43–58. doi: 10.1016/j.psychsport.2018.04.004
Roeh, A., Bunse, T., Lembeck, M., Handrack, M., Pross, B., Schoenfeld, J., et al. (2019a). Running effects on cognition and plasticity (ReCaP): study protocol of a longitudinal examination of multimodal adaptations of marathon running. Res. Sports Med. doi: 10.1080/15438627.2019.1647205 [Epub ahead of print].
Roeh, A., Kirchner, S. K., Malchow, B., Maurus, I., Schmitt, A., Falkai, P., et al. (2019b). Depression in somatic disorders: is there a beneficial effect of exercise? Front. Psychiatry 10:141. doi: 10.3389/fpsyt.2019.00141
Salk, R. H., Hyde, J. S., and Abramson, L. Y. (2017). Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol. Bull. 143, 783–822. doi: 10.1037/bul0000102
Schneibel, R., Brakemeier, E.-L., Wilbertz, G., Dykierek, P., Zobel, I., and Schramm, E. (2012). Sensitivity to detect change and the correlation of clinical factors with the Hamilton depression rating scale and the beck depression inventory in depressed inpatients. Psychiatry Res. 198, 62–67. doi: 10.1016/j.psychres.2011.11.014
Schuch, F. B., Vancampfort, D., Firth, J., Rosenbaum, S., Ward, P. B., Silva, E. S., et al. (2018). Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am. J. Psychiatry 175, 631–648. doi: 10.1176/appi.ajp.2018.17111194
Shi, J., Yao, Y., Zhan, C., Mao, Z., Yin, F., and Zhao, X. (2018). The relationship between big five personality traits and psychotic experience in a large non-clinical youth sample: the mediating role of emotion regulation. Front. Psychiatry 9:648. doi: 10.3389/fpsyt.2018.00648
Vachon, D. D., Sellbom, M., Ryder, A. G., Miller, J. D., and Bagby, R. M. (2009). A five-factor model description of depressive personality disorder. J. Personal. Disord. 23, 447–465. doi: 10.1521/pedi.2009.23.5.447
Keywords: personality, exercise, endurance training, marathon, MMPI
Citation: Roeh A, Engel RR, Lembeck M, Pross B, Papazova I, Schoenfeld J, Halle M, Falkai P, Scherr J and Hasan A (2020) Personality Traits in Marathon Runners and Sedentary Controls With MMPI-2-RF. Front. Psychol. 11:886. doi: 10.3389/fpsyg.2020.00886
Received: 22 October 2019; Accepted: 09 April 2020;
Published: 08 May 2020.
Edited by:
Costantino Balestra, Haute École Bruxelles-Brabant (HE2B), BelgiumReviewed by:
Pedro Gaspar, University of Coimbra, PortugalMing-Qiang Xiang, Guangzhou Sport University, China
Copyright © 2020 Roeh, Engel, Lembeck, Pross, Papazova, Schoenfeld, Halle, Falkai, Scherr and Hasan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Astrid Roeh, YXN0cmlkLnJvZWhAbWVkLnVuaS1tdWVuY2hlbi5kZQ==; Benjamin Pross, QmVuamFtaW4uUHJvc3NAbWVkLnVuaS1tdWVuY2hlbi5kZQ==; Johannes Scherr, Sm9oYW5uZXMuU2NoZXJyQG1yaS50dW0uZGU=; Alkomiet Hasan, YWxrb21pZXQuaGFzYW5AbWVkLnVuaS1tdWVuY2hlbi5kZQ==