 Andreia Veloso
Andreia Veloso Selene G. Vicente
Selene G. Vicente Marisa G. Filipe
Marisa G. Filipe- Faculty of Psychology and Education Sciences, Centre for Psychology, University of Porto, Porto, Portugal
Problems with executive functions (EF) are hallmark characteristics of Attention Deficit/Hyperactivity Disorder (ADHD). Therefore, this review analyzed the efficacy of cognitive training for EF in reducing ADHD symptomatology and improving educational, interpersonal, and occupational outcomes in children and adolescents with this disorder. A systematic search, using a PICO (population/participant, intervention/indicator, comparator/control, outcome) framework was carried out. From 2008 to 2018, resorting to EBSCOhost, the following databases were searched: Academic Search Complete, ERIC, MEDLINE with Full Text, PsycARTICLES, PsycINFO, and Psychology and Behavioral Sciences Collection. Twenty-two studies were included in this review. Of the 18 studies that reported performance-based measures of EF, 13 found improvements and five did not. Overall, 17 studies showed positive transfer effects on ADHD symptomatology, EF, academic improvement, reduced off-task behavior, and/or enhanced social skills. Of the nine studies that performed follow-up sessions, seven concluded that the treatment effects were maintained over time. In sum, results showed that cognitive training can be an effective intervention for children and adolescents with ADHD and might be a complementary treatment option for this disorder.
Attention Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder marked by persistent symptoms of inattention, hyperactivity, and/or impulsivity (American Psychiatric Association, 2013). Children diagnosed with this disorder present difficulties in the ability to pay attention, restrain movements, inhibit impulses, and regulate behavior (Roberts et al., 2015) that affect communication, daily living, and socialization (Weyandt and Gudmundsdottir, 2015). Importantly, according to the literature, these difficulties arise from deficits in executive functioning (e.g., Rapport et al., 2001; Sonuga-Barke, 2003; Willcutt et al., 2005; Nigg, 2006; Barkley, 2015).
Even though there is no agreed-upon definition, executive functions (EF) can be viewed as a multidimensional construct that encapsulates higher-order cognitive processes responsible for guiding, directing, and managing cognitive, emotional, and behavioral functions, particularly during novel problem situations (Gioia et al., 2000). There are several cognitive processes associated with EF, but the major elements include anticipation, goal selection, planning, initiation, self-regulation, mental flexibility, attention, and utilization of feedback (Anderson, 2002). These processes develop throughout childhood and adolescence and are invaluable to the cognitive, behavioral, emotional, and social functioning of the individual (Anderson, 2002), originating a variety of difficulties when impaired (Brown, 2013).
Consequently, EF has been broadly investigated in individuals with ADHD and, even though results have been incongruous, studies showed poor performance of children with ADHD on EF tasks when compared to typically developing peers (e.g., Nigg et al., 2002; Willcutt et al., 2005). For instance, a meta-analytic review composed of 83 studies evaluated the validity of the EF theory in this population and observed that children with ADHD display significant deficits in inhibitory control, vigilance, working memory, and planning (Willcutt et al., 2005). A few studies also found difficulties in processing speed (Nigg et al., 2002; Lawrence et al., 2004; Pasini et al., 2007; Yáñez-Téllez et al., 2012), cognitive flexibility (Lawrence et al., 2004; Geurts et al., 2005; Yáñez-Téllez et al., 2012), and sustained attention (Nigg et al., 2002; Trani et al., 2011; Yáñez-Téllez et al., 2012). Thus, problems with EF seem to be hallmark characteristics of this disorder.
Treatment options for ADHD are limited and, frequently, involve the prescription of psychostimulant medication as a first line treatment (Yildiz et al., 2011). Improvements in behavior, attention, interpersonal interactions, cognition (Biederman and Spencer, 2008), and EF (e.g., Barnett et al., 2001; Swanson et al., 2011) reinforce the short-term efficacy of psychostimulant medication, of which methylphenidate and dextroamphetamine are the most prescribed (Rabipour and Raz, 2012). Nevertheless, the limitations of such medication (e.g., short-term effects, unknown long-term effects, side-effects such as insomnia and lack of appetite) prompt parents and professionals to look for another treatment options (Rabipour and Raz, 2012). Thus, efforts have been made to develop non-pharmacological interventions that decrease ADHD symptomatology, and cognitive training has been considered a potential intervention. As reported by Vinogradov et al. (2012), due to brain plasticity, cognitive training can strengthen and develop essential brain networks and underlying cognitive processes by exposing the brain to well-defined learning tasks, resulting in more adaptive behaviors across contexts.
The tasks presented in cognitive training interventions vary extensively, are usually conferred as games, and can be presented through a computer or pen and paper format, aiming to improve a plethora of abilities such as working memory, attention, inhibitory control, planning, and cognitive flexibility. As it is important to keep the child engaged, motivated, and practicing at a level that is in accordance with or slightly above their current abilities (Diamond, 2012; Rapport et al., 2013), this training is usually adaptive (i.e., the difficulty of the task is adjusted to the performance of the child; Rapport et al., 2013). Thus, it has been proposed that cognitive training can reduce ADHD symptomatology and improve functioning by addressing the neuropsychological deficits thought to mediate its pathophysiology (Cortese et al., 2015).
A meta-analytic review carried out by Cortese et al. (2015) examined the effects of cognitive training on ADHD symptomatology, neuropsychological deficits, and academic skills in children and adolescents with ADHD. The authors concluded that there were significant effects of training on ADHD symptoms when considering unblinded raters. Yet, these results were drastically reduced when analyses were limited to trials with active control groups or where raters were blind to treatment conditions. Additionally, significant performance improvements in objective measures of visual and verbal working memory were reported, while there were no effects on inhibition or attention. However, these effects of training on working memory did not extend to academic outcomes. Other reviews found similar results (e.g., Karch et al., 2013; Rapport et al., 2013; Sonuga-Barke et al., 2013). However, the majority of the studies included in these previous reviews focused on a single EF, such as working memory, inhibitory, and attention (or a combination of these). Given that children with ADHD display a diverse set of EF deficits, and training multiple EF might be a more effective strategy than focusing on a single EF domain (Dovis et al., 2015), a systematic literature review focusing on the training of multiple EF domains is lacking.
As it has been proposed that cognitive training for improving executive functioning can reduce ADHD symptomatology (e.g., Cortese et al., 2015), our main aim is to update and extend the findings of previous systematic reviews and meta-analyses, characterizing the current literature on cognitive training interventions for EF in children and adolescents diagnosed with ADHD. We, thus, examine the outcomes within the included studies to determine the efficacy of cognitive training assessed by performance-based measures of EF and behavioral/EF questionnaires. Additionally, we intended to evaluate the transfer effects (i.e., generalization of training effects to other non-trained tasks) and possible maintenance of gains reported in each study. As such, we developed the following research question using the PICO framework: In children and adolescents with ADHD, is cognitive training for EF, compared to other types of intervention, typically developing controls, or placebo, effective in developing executive functioning, reducing symptomatology, and improving educational, interpersonal and/or occupational outcomes? (cf. Table 1).
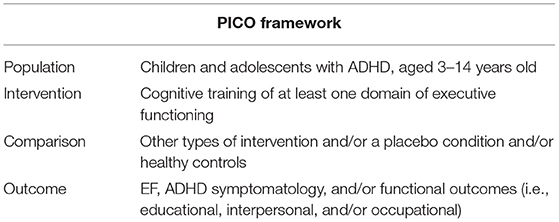
Table 1. PICO (population/participant, intervention/indicator, comparator/control, outcome) framework.
Methods
Search Strategy
The systematic literature search was conducted between January and February 2018, resorting to EBSCOhost (Academic Search Complete, ERIC, MEDLINE with Full Text, PsycARTICLES, PsycINFO and Psychology and Behavioral Sciences Collection). The search keywords were operationalized using a Population/Participant, Intervention/Indicator, Comparator/Control, Outcome(s) (PICO) search framework (cf. Table 1). Focusing on the last 10 years (2008–2018), the keywords executive function* OR executive functioning AND cognitive training OR intervention* AND Attention Deficit Hyperactivity Disorder OR ADHD were used to conduct the search. Every reference was, then, conveyed to Mendeley and Rayyan, a website developed to assist systematic review authors to perform study selection (Ouzzani et al., 2016), and duplicates were removed. Every study was initially identified by title and abstract, according to the inclusion criteria. Figure 1 details the process of study selection.
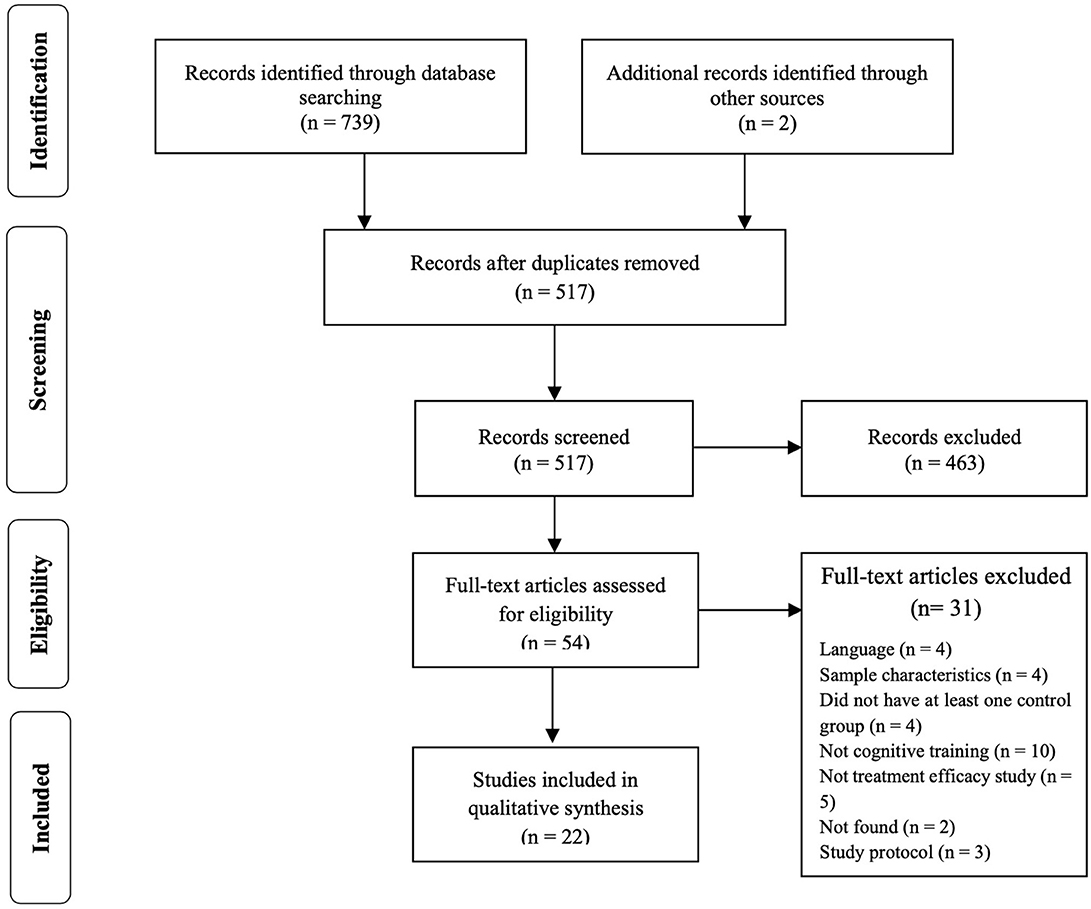
Figure 1. Preferred Reporting Items in Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of selection of studies.
Inclusion and Exclusion Criteria
In order to be included in this review, studies had to: (1) include children with ADHD aged 3–14 years; (2) include a cognitive intervention/training focusing on one or more components of EF; (3) include an active and/or a passive control condition; (4) include measures of EF, ADHD symptomatology, academic achievement and/or interpersonal relationship quality as outcomes; and (5) be published in English.
Reasons for exclusion entailed: (1) reviews, meta-analysis, dissertations, book chapters, and study protocols; (2) studies involving different intervention technics (e.g., mindfulness, neurofeedback); (3) studies focused on different neurodevelopmental disorders (e.g., learning difficulties, Autism Spectrum Disorder) or clinical groups (e.g., Neurofibromatosis); (4) studies including different age ranges (e.g., adults); (5) studies that do not include at least one outcome measure of EF, ADHD symptomatology, academic achievement and/or interpersonal relationship quality; and (6), papers not published in English.
Studies were not excluded if children presented comorbid diagnoses or maintained the course of pharmacological treatment during interventions.
After screening each study by title and abstract, the full texts were analyzed and included if they fulfilled the stipulated criteria. Two additional studies (Green et al., 2012; Johnstone et al., 2012) were hand-searched and included in this review.
Risk of Bias (Quality) Assessment
In order to assess the risk of bias of the included studies, the Cochrane Collaboration tools were used, namely the RoB 2.0 (Sterne et al., 2019) for the randomized trials and the ROBINS-I (Sterne et al., 2016) for the non-randomized trials. The RoB 2.0 assesses five domains of bias, specifically: (1) bias due to randomization, (2) bias due to deviations from intended intervention, (3) bias due to missing data, (4) bias due to outcome measurement, and (5) bias due to selection of reported result. The ROBINS-I, one the other hand, assesses: (1) bias due to confounding, (2) bias due to selection of participants, (3) bias in classification of interventions, (4) bias due to deviation from intended intervention, (5) bias due to missing data, (6) bias in measurement of outcomes, and (7) bias in selection of the reported result. Risk of bias was independently assessed by AV and MF and disagreements were resolved through discussion. Figures 2–5, designed with the robvis web app (McGuiness, 2019), depict the plots obtained from these analyses.
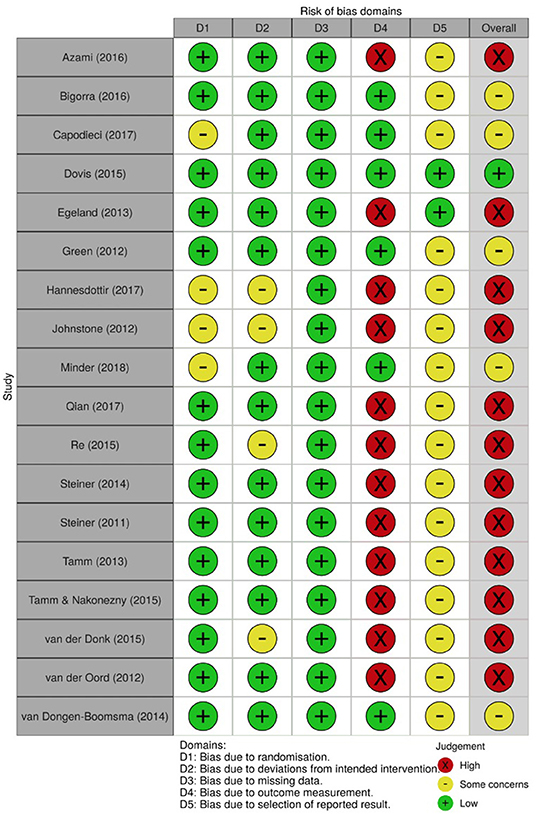
Figure 2. Risk of bias summary for all randomized trials included.
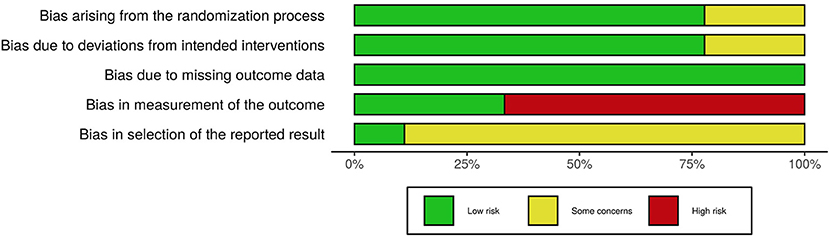
Figure 3. Risk of bias graph for all randomized trials included.
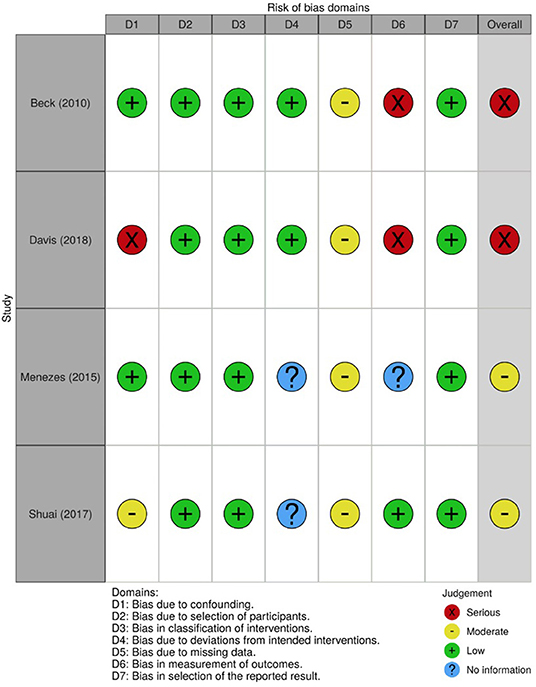
Figure 4. Risk of bias summary for all non-randomized trials included.
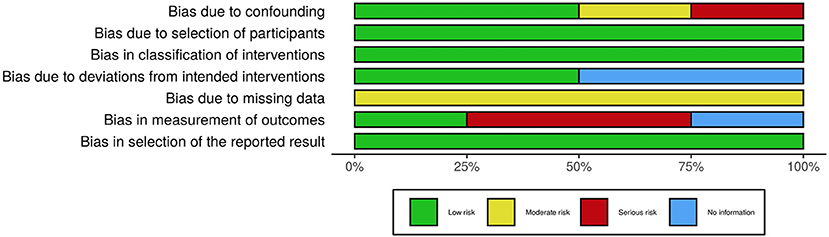
Figure 5. Risk of bias graph for all non-randomized trials included.
Data Extraction
Data obtained from each study encompassed sample characteristics, study design, settings, intervention materials, outcome measures, and main findings.
Results
Trial Flow
A total of 739 articles were identified from the databases using the search strategy previously reported. Two additional references were hand-searched and included in this review. Two hundred and twenty-four duplicates were removed, and 517 articles were assessed by title and abstract. Of these, 463 reports were excluded since they did not fulfill the predetermined criteria. Hence, 54 papers were included and their full-text analyzed, of which 22 met inclusion criteria. Again, in Figure 1, the study selection process is presented in a PRISMA flow diagram (Moher et al., 2009).
General Study Characteristics
The age range of the participants included in each study varied extensively and most of the studies analyzed children aged between 3 and 12 years old (cf. Table 2).
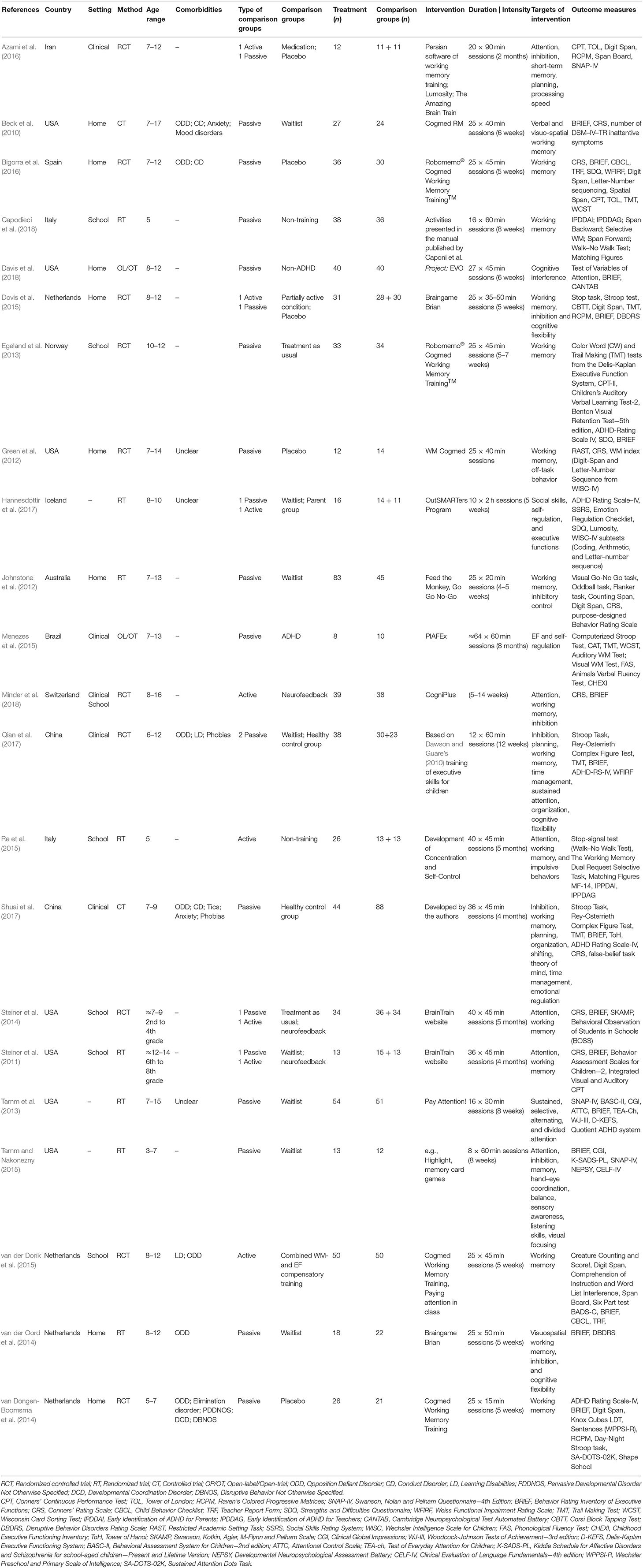
Table 2. Study and intervention characteristics.
Sample groups were composed by children diagnosed with ADHD and their typically developing peers. Twelve studies included samples of participants with no comorbidities and seven studies included children with comorbid diagnosis such as Opposition Defiant Disorder (ODD), Conduct Disorder (CD), Learning Disabilities (LD), Anxiety and/or Tics, Mood Disorders, Phobias and/or Elimination Disorders. Three studies did not detail whether they included or excluded participants with comorbidities (cf. Table 2).
Regarding research design, 10 studies were randomized controlled trials, eight were randomized trials, two were open-label/open-trial designs, and two were non-randomized controlled trials (cf. Table 2). In regard to control groups, three of these studies compared the performance of the experimental groups only with active control groups (i.e., medication, non-adaptive training, different intervention) and 14 included passive control groups (i.e., waitlist, healthy control group, normal school activities, treatment as usual) (cf. Table 2). Furthermore, to assess outcomes, eight studies included informants blind to study conditions (i.e., uninformed regarding which people belong to a particular group). One study included only blinded teachers (Beck et al., 2010) and three included blinded classroom observers (Green et al., 2012; Steiner et al., 2014; Minder et al., 2018). In three studies all informants were blind, either parents, teachers, and/or clinicians (van Dongen-Boomsma et al., 2014; Dovis et al., 2015; Bigorra et al., 2016). Lastly, one study used blind clinician assessments (Tamm and Nakonezny, 2015) and another blinded researchers and participants (Green et al., 2012). The remainder fourteen studies used unblinded informants.
Seven studies included in this review were carried out in the USA and 10 in Europe. Two studies were carried out in China, one in Brazil, one in Iran, and one in Australia (cf. Table 2). Eight interventions were conducted at home, six took place in school settings, and four in clinical settings. One study was carried out both in school and clinical settings (Minder et al., 2018). This information was not explicitly stated in three studies. When interventions took place at home, parents where usually the ones providing support during sessions. At school, the intervention was either delivered by teachers, clinicians, or trained research assistants. In regard to the clinical setting, most of the programs were employed by clinicians, but it was not possible to gather precise information in three of these investigations.
Nine of the 22 included studies were published between 2010 and 2014, while five studies were published in 2015, two in 2016, three in 2017, and three in 2018 (cf. Table 2).
Type of Intervention
The duration of interventions varied extensively. The number of the training sessions varied from 8 to 64, and each session lasted from 15 min to 2 h (average of 52 min). The amount of time participants spent in training ranged between 375 and 3,840 min (average of 1,096 min per intervention).
Two types of intervention materials were considered: computerized (Beck et al., 2010; Steiner et al., 2011, 2014; Green et al., 2012; Johnstone et al., 2012; Egeland et al., 2013; van der Oord et al., 2014; van Dongen-Boomsma et al., 2014; Dovis et al., 2015; Azami et al., 2016; Bigorra et al., 2016; Davis et al., 2018; Minder et al., 2018) and non-computerized cognitive training (Tamm et al., 2013; Menezes et al., 2015; Re et al., 2015; Tamm and Nakonezny, 2015; Hannesdottir et al., 2017; Qian et al., 2017; Shuai et al., 2017; Capodieci et al., 2018). One study used both types of intervention in order to compare their efficacy (van der Donk et al., 2015).
Regarding the computerized training, the majority of the studies employed some variation of the Cogmed software. Additional websites and software encompass the Persian software of working memory training, Project: Evo, Braingame Brian, CogniPlus, the Brain Train website, and others. Further programs and activities, without computerized characteristics, feature the activities presented in the manual published by Caponi and collaborators, the OutSMARTers program, PIAFEx, a training program based on Dawson and Guare's training of executive skills for children, and other activities. One study did not specify the training program used during the intervention but provided some insights about its characteristics (Shuai et al., 2017).
Targets of Intervention
As previously stated, there is no universally accepted definition of EF and, therefore, there is no agreement concerning the elements incorporated in this construct. Consequently, there is extensive variability in the domains of intervention across studies, and, in total, 16 EF were considered. Five of these 16 domains were targeted more frequently, specifically: attention (n = 8), inhibition (n = 8), working memory (n = 16), planning (n = 3), and cognitive flexibility (n = 4). Other components of executive functioning addressed by interventions incorporate organization, processing speed, short-term memory, self/emotional regulation, time management, and theory of mind (cf. Table 2).
Outcome Measures
A variety of measures were used across studies to measure EF, as detailed in Table 3. These measures can be subdivided into two categories: (1) performance-based neuropsychological measures (i.e., computer-oriented or pen-paper tasks) and (2) behavioral and EF questionnaires (under the perspective of parents, teachers, clinicians and/or significant others).
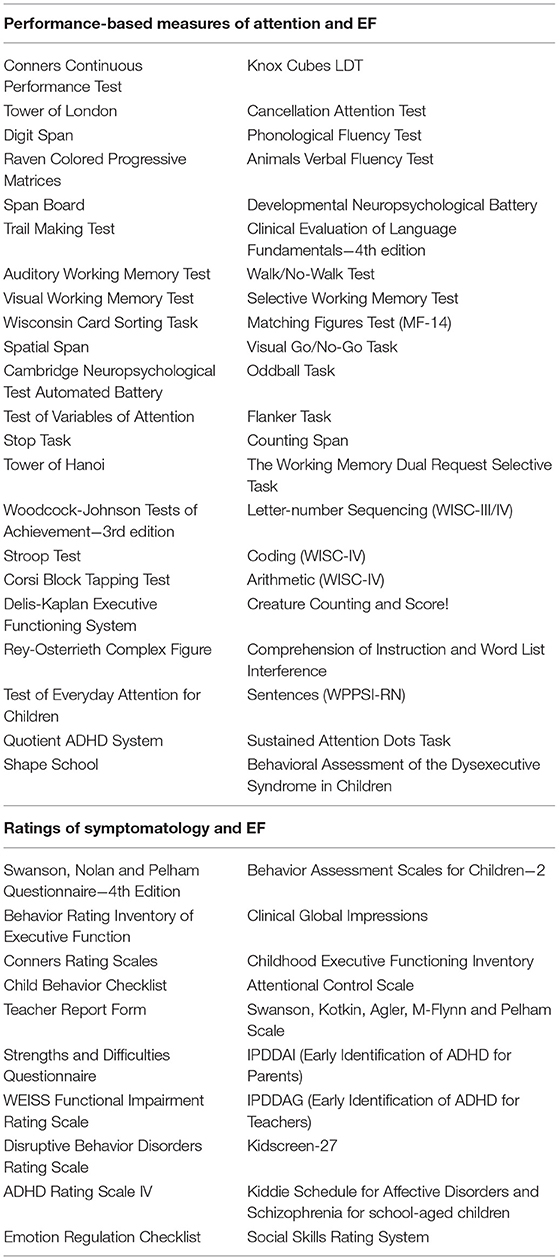
Table 3. Performance-based measures and questionnaires employed across studies.
Within the 22 studies, 44 performance-based measures were used to assess particular aspects of EF. Of these 44 measures, 10 were adopted in three or more studies, respectively: (1) Conners' Continuous Performance Test, (2) Trail Making Test, (3) Wisconsin Card Sorting Task, (4) Delis-Kaplan Executive Functioning System, (5) Stroop Test, (6) Rey-Osterrieth Complex Figure, (7) Digit Span, (8) Raven Colored Progressive Matrices, (9) Developmental Neuropsychological Assessment Battery, and (10) Letter-Number Sequencing. It is important to note, however, that not all studies included in this review used performance-based measures to verify the efficacy of their intervention.
Furthermore, within the 20 ratings employed, five were widely used across studies, specifically: (1) Behavior Rating Inventory of Executive Functions, (2) Conners' Rating Scales, (3) Swanson, Nolan, and Pelham Questionnaire−4th edition, (4) Strengths and Difficulties Questionnaire, and (5) ADHD Rating Scale-IV.
Effects of Intervention
Data for EF outcomes were examined in each study in order to determine the efficacy of the interventions, and details are outlined in Table 4. Of the 22 studies included in this review, 14 reported improvements in performance-based measures of EF (Green et al., 2012; Johnstone et al., 2012; Egeland et al., 2013; Tamm et al., 2013; Dovis et al., 2015; Menezes et al., 2015; Re et al., 2015; van der Donk et al., 2015; Azami et al., 2016; Bigorra et al., 2016; Shuai et al., 2017; Capodieci et al., 2018; Davis et al., 2018), four didn't resort to these measures to evaluate the outcomes (Beck et al., 2010; Steiner et al., 2014; van der Oord et al., 2014; Minder et al., 2018), four were unable to find significant differences between groups (van Dongen-Boomsma et al., 2014; Tamm and Nakonezny, 2015; Hannesdottir et al., 2017; Qian et al., 2017), and one was unclear regarding its findings (Steiner et al., 2011). In the 14 studies that presented positive results in performance-based measures, improvements were reported for attention (Johnstone et al., 2012; Tamm et al., 2013; van der Donk et al., 2015; Azami et al., 2016; Bigorra et al., 2016; Davis et al., 2018), working memory (Green et al., 2012; Dovis et al., 2015; Menezes et al., 2015; Re et al., 2015; van der Donk et al., 2015; Shuai et al., 2017; Capodieci et al., 2018; Davis et al., 2018), inhibition (Dovis et al., 2015; Menezes et al., 2015; van der Donk et al., 2015; Azami et al., 2016; Bigorra et al., 2016; Davis et al., 2018), visuospatial short-term memory (Dovis et al., 2015; Azami et al., 2016), verbal short-term memory (Azami et al., 2016), attentional control (Re et al., 2015; Capodieci et al., 2018), interference control (Dovis et al., 2015; Shuai et al., 2017), impulsiveness (Re et al., 2015; Capodieci et al., 2018), processing speed (Egeland et al., 2013; Shuai et al., 2017), shifting (Shuai et al., 2017), planning (Tamm et al., 2013; Shuai et al., 2017), and reasoning (Azami et al., 2016). The effect sizes reported ranged from small to large (cf. Table 4 for detailed results).
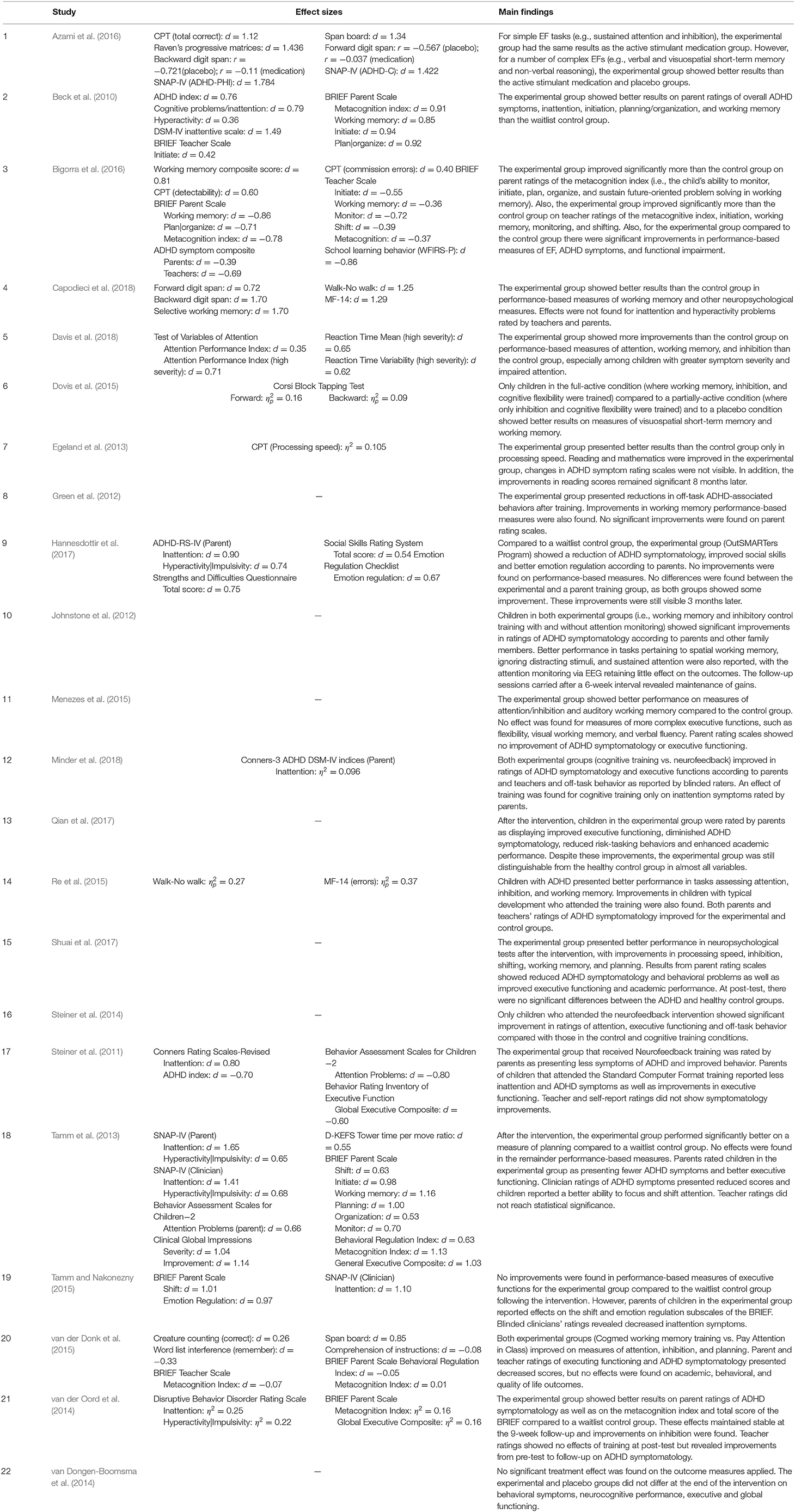
Table 4. Results of included studies.
Regarding the ability of cognitive training to trigger change in day-to-day life (i.e., transfer effects; Toplak et al., 2008), 11 studies have shown decreases in parent and/or teacher ratings of ADHD symptomatology and 11 studies conveyed reductions on EF difficulties according to informants, with small to large effect sizes (cf. Table 4). Studies also stated improvements in social skills (Hannesdottir et al., 2017; Qian et al., 2017), progress in academic performance (Egeland et al., 2013; Qian et al., 2017; Shuai et al., 2017), and reduced off-task behavior (Green et al., 2012; Minder et al., 2018; cf. Table 4). In the matter of the assessment of EF behaviors in everyday environments, informants reported positive changes in working memory (Beck et al., 2010; Tamm et al., 2013; Tamm and Nakonezny, 2015; Bigorra et al., 2016; Shuai et al., 2017), initiation (Beck et al., 2010; Tamm et al., 2013; Shuai et al., 2017), planning/organization (Beck et al., 2010; Tamm et al., 2013; Tamm and Nakonezny, 2015; Shuai et al., 2017), monitoring (Tamm et al., 2013; Bigorra et al., 2016; Shuai et al., 2017), shifting (Tamm et al., 2013; Bigorra et al., 2016), inhibition (Tamm and Nakonezny, 2015; Shuai et al., 2017), emotional control (Shuai et al., 2017), the metacognition (Tamm et al., 2013; van der Oord et al., 2014; van der Donk et al., 2015; Bigorra et al., 2016; Shuai et al., 2017; Minder et al., 2018) and behavioral regulation indexes (Tamm et al., 2013; van der Donk et al., 2015; Shuai et al., 2017; Minder et al., 2018), and the global executive composite (Steiner et al., 2011; Tamm et al., 2013; van der Oord et al., 2014; Shuai et al., 2017).
Of these 22 studies, 13 did not analyze the possible maintenance of gains through follow-up sessions. Of the nine studies that performed follow-up sessions, seven concluded that the gains observed at the end of the intervention were maintained throughout time (Beck et al., 2010; Johnstone et al., 2012; Egeland et al., 2013; van der Oord et al., 2014; van der Donk et al., 2015; Bigorra et al., 2016; Hannesdottir et al., 2017).
In order to assess if study design had implications in the results obtained across studies, a qualitative comparison of the results obtained in randomized (n = 18) vs. non-randomized (n = 4) trials was conducted. On one hand, randomized studies reported, more often than non-randomized trials, improvements in ratings (≃33 vs. ≃25%) as well as in performance-based measures and ratings combined (≃33 vs. ≃25%). On the other hand, non-randomized trials reported improvements only in performance-based measures more frequently than randomized studies (≃50 vs. ≃22%).
As previously reported, seven studies contemplated in this review included samples of children with comorbid diagnoses. A qualitative comparison of the results obtained by these studies showed that, comparatively to studies that included children with an ADHD diagnosis only, a higher proportion of studies with included comorbid diagnoses reached improvements in ratings (≃43 vs. ≃25%) and performance-based measures in combination with ratings (≃43 vs. ≃25%). Also, in samples without comorbid diagnoses, improvements were found more frequently only in performance-based measures (≃42%).
Discussion
The first aim of this study was to update and extend the findings of previous reviews, characterizing the current literature on cognitive training interventions for EF in children and adolescents diagnosed with ADHD between 3 and 14 years of age. A total of 741 articles were identified and, after duplicates removal, 517 articles were analyzed. Twenty-two studies were eligible for inclusion. Regarding the characteristics of the included studies, it is useful to highlight important methodological features. Studies tend to include individuals diagnosed with ADHD and other comorbid disorders (i.e., ODD, CD, LD, Anxiety and/or Tics, Mood Disorders, Phobias, and/or Elimination Disorders). Regarding research designs, the majority of the included studies were randomized trials, but a few non-randomized studies were also included as they fulfilled the pre-established inclusion criteria. Also, although all studies included control groups, unblinded outcomes assessments were performed frequently. Most of the research was conducted in USA and Europe in home, school, and/or clinical settings. Regarding intervention programs, computerized but also non-computerized programs were frequently employed. The most frequent EF domains targeted by interventions were attention, inhibition, working memory, planning, and cognitive flexibility.
Our second aim was to assess whether cognitive training was effective in ADHD as evaluated by performance-based measures of EF and/or behavioral/EF questionnaires. Results showed that most of the studies that used performance-based measures demonstrated efficacy in improving one or more domains of EF in children and adolescents. Study design appears to have implications in the results obtained across studies, as a qualitative comparison of the results obtained in randomized and non-randomized trials showed that randomized studies reported, more often than non-randomized trials, improvements in ratings as well as in performance-based measures and ratings combined. Conversely, non-randomized trials reported improvements only in performance-based measures more frequently than randomized studies.
Furthermore, we intended to evaluate the transfer of gains (i.e., the generalization of training effects to other non-trained tasks). Regarding these transfer effects, research has shown decreases in parent and/or teacher ratings of ADHD symptomatology, social skills improvements, and reductions in EF dysfunction in daily life. Additionally, improvements in academic performance and reduced off-task behavior (i.e., task disengagement to engage in unrelated behaviors) were reported. In spite of these results showing that cognitive training can be an effective intervention for children and adolescents with ADHD, our conclusions should be interpreted considering limitations of the included studies as discussed below.
As previously mentioned, several studies integrated in this review included participants with associated comorbidities. In fact, Efron et al. (2016) found that in a sample of 132 diagnosed children, aged 4–7 years, 39% had one comorbidity and 37% had more than one comorbidity. According to the authors, ODD (53%), Anxiety Disorder (23.5%), LD (15.9%), and Language Disorder (14.4%) were the most common comorbidities across individuals with ADHD. Similar results have been reported by Reale et al. (2017). The authors found that of the 1,919 subjects evaluated, 66% had at least one comorbid diagnosis, while only 34% presented just ADHD. Among the most common comorbid diagnosis were LD (56%), Sleep Disorders (23%), ODD (20%), and Anxiety Disorders (12%). Therefore, it is clear that the majority of children diagnosed with ADHD have, at least, one comorbid disorder.
The comparison of the results obtained by the included studies in this review demonstrated that a higher proportion of studies that included comorbid diagnoses reached improvements in ratings and performance-based measures in combination with ratings. Contrarily, in samples without comorbid diagnoses, improvements were found more frequently only in performance-based measures. These results suggest that, for children with comorbidities, improvements perceived by informants in daily life were more frequent. In fact, as discussed by Diamond (2012), children with greater difficulties on executive functioning may benefit the most from any intervention focusing on its training. As children with comorbid diagnoses usually present with higher levels of symptomatology and EF problems, they may have more room for improvement than children presenting with one single diagnosis (Flook et al., 2010). As such, individuals with different comorbidities may respond differently to specific treatments, have differing clinical correlates, and/or demonstrate unique clinical outcomes what might influence results obtained across studies. So, additional studies should group ADHD individuals into more homogenous subgroups based on comorbid patterns.
Regarding control groups, in order to consider that differences between the groups may be accounted to effects of the intervention, researchers should compare the performance of an experimental group and a control group that “accounts for improvements caused by factors other than the treatment” (i.e., an active control group; Boot et al., 2013). In line with these theoretical assumptions, assessing the efficacy of interventions by comparing the performance between a treated group and a non-treated group (i.e., treatment as usual, waitlist, typical development) would not be appropriate since both groups have different expectations (Boot et al., 2013), influencing results on outcome measurements. In fact, of the studies included in this review, three reported active control groups and five used both active and passive control groups. Nevertheless, the majority of the comparison groups were passive (n = 14), and these considerations should be taken into account while interpreting these results.
Another limitation of most of the studies conducted is the lack of transfer effects when the efficacy of the intervention is assessed by blinded raters. Even though this was confirmed across the majority of studies that included unblinded informants, positive results should also be highlighted. Beck et al. (2010) and Bigorra et al. (2016) assessed treatment efficacy through blinded raters and found significant results. Beck et al. (2010) found slight improvements in the initiate scale of the BRIEF—Teacher Form, even though these only approached significance. Bigorra et al. (2016) found significant improvements in several subscales of the BRIEF—Teacher and Parent Forms, with small to large effect sizes. The authors also found significant improvements in ADHD symptoms according to both teachers and parents. These results show that blind raters are able to detect changes in everyday situations following cognitive training interventions. Nevertheless, more studies using blind raters are needed in order to provide a better understanding of the effects of cognitive training.
For future studies, there are a number of additional issues that researchers must address to support empirical evidence for the implementation of EF training as a complementary intervention for individuals with ADHD. Specifically, a well-designed intervention should (a) randomize participants into the experimental and control groups; (b) match participants in variables that might account for differences between groups other than the treatment (e.g., age, comorbidity); (c) control for participants and informants expectations through blinding and assessment of expectations prior to the beginning of the intervention to control for possible placebo effects; (d) compare the performance of the experimental group to both active and passive control groups; and (e) use both performance-based measures and ratings of EF and behavior to assess the interventions' efficacy.
Notwithstanding, this review represents an important contribution as it includes a wider range of studies (i.e., different designs and interventions), having important clinical and educational implications, as it demonstrates the feasibility and positive effects of conducting EF training with children and adolescents with ADHD in a variety of contexts.
In sum, our results showed that cognitive training can be an effective intervention for children and adolescents with ADHD and might be considered a complement of psychostimulant medication. Nonetheless, conclusions should be interpreted with caution due to important methodological limitations. However, the available evidence certainly justifies the allocation of resources to evaluate the efficacy of EF interventions, since they carry the promise of reducing ADHD symptomatology and improving academic, interpersonal, and occupational outcomes.
Author Contributions
AV and MF contributed to the conception and design of the work. AV prepared the first draft of the manuscript. MF revised the manuscript critically for important intellectual content. MF and SV revised the last version of the manuscript.
Funding
This research was supported by the M2S Project funded through the Operational Programme for Competitiveness and Internationalization, supported by FEDER and national funds allocated to the Portuguese Foundation for Science and Technology (NORTE-01-0145-FEDER-028404).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Arlington, VA: American Psychiatric Publishing.
Anderson, P. (2002). Assessment and development of executive function (EF) during childhood. Child Neuropsychol. 8, 71–82. doi: 10.1076/chin.8.2.71.8724
Azami, S., Moghadas, A., Sohrabi-Esmrood, F., Nazifi, M., Mirmohamad, M., Hemmati, F., et al. (2016). A pilot randomized controlled trial comparing computer-assisted cognitive rehabilitation, stimulant medication, and an active control in the treatment of ADHD. Child Adolesc. Mental Health 21, 217–224. doi: 10.1111/camh.12157
Barkley, R. A., (ed.). (2015). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 4th Edn. New York, NY: Guilford Press.
Barnett, R., Maruff, P., Vance, A., Luk, E. S. L., Costin, J., Wood, C., et al. (2001). Abnormal executive function in Attention Deficit Hyperactivity Disorder: the effect of stimulant medication and age on spatial working memory. Psychol. Med. 31, 1107–1115. doi: 10.1017/S0033291701004172
Beck, S. J., Hanson, C. A., Puffenberger, S. S., Benninger, K. L., and Benninger, W. B. (2010). A controlled trial of working memory training for children and adolescents with ADHD. J. Clin. Child Adolesc. Psychol. 39, 825–836. doi: 10.1080/15374416.2010.517162
Biederman, J., and Spencer, T. J. (2008). Psychopharmacological interventions. Child Adolesc. Psychiatr. Clin. N. Am. 17, 439–458. doi: 10.1016/j.chc.2007.12.001
Bigorra, A., Garolera, M., Guijarro, S., and Hervás, A. (2016). Long-term far-transfer effects of working memory training in children with ADHD: a randomized controlled trial. Eur. Child Adolesc. Psychiatr. 25, 853–867. doi: 10.1007/s00787-015-0804-3
Boot, W. R., Simons, D. J., Stothart, C., and Stutts, C. (2013). The pervasive problem with placebos in psychology: why active control groups are not sufficient to rule out placebo effects. Perspect. Psychol. Sci. 8, 445–454. doi: 10.1177/1745691613491271
Brown, T. E. (2013). A New Understanding of ADHD in Children and Adults: Executive Function Impairments. New York, NY: Routledge.
Capodieci, A., Gola, M. L., Cornoldi, C., and Re, A. M. (2018). Effects of a working memory training program in preschoolers with symptoms of attention-deficit/hyperactivity disorder. J. Clin. Exp. Neuropsychol. 40, 17–29. doi: 10.1080/13803395.2017.1307946
Cortese, S., Ferrin, M., Brandeis, D., Buitelaar, J., Daley, D., Dittmann, R. W., et al. (2015). Cognitive training for attention-deficit/hyperactivity disorder: meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials. J. Am. Acad. Child Adolesc. Psychiatr. 54, 164–174. doi: 10.1016/j.jaac.2014.12.010
Davis, N. O., Bower, J., and Kollins, S. H. (2018). Proof-of-concept study of an at-home, engaging, digital intervention for pediatric ADHD. PLoS ONE 13:e0189749. doi: 10.1371/journal.pone.0189749
Dawson, P., and Guare, R. (2010). Executive Skills in Children and Adolescents: A Practical Guide to Assessment and Intervention, 2nd Edn. New York, NY: Guilford Press.
Diamond, A. (2012). Activities and programs that improve children's executive functions. Curr. Dir. Psychol. Sci. 21, 335–341. doi: 10.1177/0963721412453722
Dovis, S., Van der Oord, S., Wiers, R. W., and Prins, P. J. M. (2015). Improving executive functioning in children with ADHD: training multiple executive functions within the context of a computer game. A randomized double-blind placebo controlled trial. PLoS ONE 10, 10:e0121651. doi: 10.1371/journal.pone.0121651
Efron, D., Bryson, H., Lycett, K., and Sciberras, E. (2016). Children referred for evaluation for ADHD: comorbidity profiles and characteristics associated with a positive diagnosis. Child Care Health Dev. 42, 718–724. doi: 10.1111/cch.12364
Egeland, J., Aarlien, A. K., Saunes, B.-K., Aarlien, A. K., and Saunes, B.-K. (2013). Few effects of far transfer of working memory training in ADHD: a randomized controlled trial. PLoS ONE 8, 1–9. doi: 10.1371/journal.pone.0075660
Flook, L., Smalley, S. L., Kitil, M. J., Galla, B. M., Kaiser-Greenland, S., Locke, J., et al. (2010). Effects of mindful awareness practices on executive functions in elementary school children. J. Appl. School Psychol. 26, 70–95. doi: 10.1080/15377900903379125
Geurts, H. M., Verté, S., Oosterlaan, J., Roeyers, H., and Sergeant, J. A. (2005). ADHD subtypes: do they differ in their executive functioning profile? Arch. Clin. Neuropsychol. 20, 457–477. doi: 10.1016/j.acn.2004.11.001
Gioia, G. A., Guy, S. C., Isquith, P. K., and Kenworthy, L. (2000). Behavior Rating Inventory of Executive Function. Florida, FL: PAR.
Green, C. T., Long, D., Green, D., Iosif, A., Dixon, J., Miller, M., et al. (2012). Will working memory training generalize to improve off-task behavior in children with attention-deficit/hyperactivity disorder? Neurotherapeutics 9, 639–648. doi: 10.1007/s13311-012-0124-y
Hannesdottir, D. K., Ingvarsdottir, E., and Bjornsson, A. (2017). The OutSMARTers program for children with ADHD: a pilot study on the effects of social skills, self-regulation, and executive function training. J. Atten. Disord. 21, 353–364. doi: 10.1177/1087054713520617
Johnstone, S. J., Roodenrys, S., Blackman, R., Johnston, E., Loveday, K., Mantz, S., et al. (2012). Neurocognitive training for children with and without AD/HD. ADHD Atten. Deficit Hyperactivity Disord. 4, 11–23. doi: 10.1007/s12402-011-0069-8
Karch, D., Albers, L., Renner, G., Lichtenauer, N., and Von Kries, R. (2013). The efficacy of cognitive training programs in children and adolescents. Dtsch. Arztebl. Int. 110, 643–652. doi: 10.3238/arztebl.2013.0643
Lawrence, V., Houghton, S., Douglas, G., Durkin, K., Whiting, K., and Tannock, R. (2004). Executive function and ADHD: a comparison of children's performance during neuropsychological testing and real-world activities. J. Atten. Disord. 7, 137–149. doi: 10.1177/108705470400700302
McGuiness, L. A. (2019). robvis: An R Package and Web Application for Visualizing Risk-of-Bias Assessments. Retrieved from: https://github.com/mcguinlu/robvis (accessed December 13, 2019).
Menezes, A., Dias, N. M., Trevisan, B. T., Carreiro, L. R. R., Seabra, A. G., and Gotuzo, R. A. (2015). Intervention for executive functions in attention deficit and hyperactivity disorder. Arq. Neuro Psiquiatr. 73, 227–236. doi: 10.1590/0004-282X20140225
Minder, F., Zuberer, A., Eis, D., Drechsler, R., Brandeis, D., and Drechsler, R. (2018). Informant-related effects of neurofeedback and cognitive training in children with ADHD including a waiting control phase: a randomized-controlled trial. Eur. Child Adolesc. Psychiatr. 27, 1055–1066. doi: 10.1007/s00787-018-1116-1
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Ann. Int. Med. 151, 264–270. doi: 10.7326/0003-4819-151-4-200908180-00135
Nigg, J. T. (2006). What Causes ADHD? Understanding What Goes Wrong and Why. New York, NY: The Guilford Press.
Nigg, J. T., Blaskey, L. G., Huang-Pollock, C. L., and Rappley, M. D. (2002). Neuropsychological executive functions and DSM-IV ADHD subtypes. J. Am. Acad. Child Adolesc. Psychiatr. 41, 59–66. doi: 10.1097/00004583-200201000-00012
Ouzzani, M., Hammady, H., Fedorowicz, Z., and Elmagarmid, A. (2016). Rayyan—a web and mobile app for systematic reviews. Syst. Rev. 5:210. doi: 10.1186/s13643-016-0384-4
Pasini, A., Paloscia, C., Alessandrelli, R., Porfirio, M. C., and Curatolo, P. (2007). Attention and executive functions profile in drug naive ADHD subtypes. Brain Dev. 29, 400–408. doi: 10.1016/j.braindev.2006.11.010
Qian, Y., Chen, M., Shuai, L., Cao, Q.-J., Yang, L., and Wang, Y.-F. (2017). Effect of an ecological executive skill training program for school-aged children with Attention Deficit Hyperactivity Disorder: a randomized controlled clinical trial. Chin. Med. J. 130, 1513–1522. doi: 10.4103/0366-6999.208236
Rabipour, S., and Raz, A. (2012). Training the brain: fact and fad in cognitive and behavioral remediation. Brain Cogn. 79, 159–179. doi: 10.1016/j.bandc.2012.02.006
Rapport, M. D., Chung, K.-M., Shore, G., and Isaacs, P. (2001). A conceptual model of child psychopathology: implications for understanding Attention Deficit Hyperactivity Disorder and treatment efficacy. J. Clin. Child Adolesc. Psychol. 30, 48–58. doi: 10.1207/S15374424JCCP3001_6
Rapport, M. D., Orban, S. A., Kofler, M. J., and Friedman, L. M. (2013). Do programs designed to train working memory, other executive functions, and attention benefit children with ADHD? A meta-analytic review of cognitive, academic, and behavioral outcomes. Clin. Psychol. Rev. 33, 1237–1252. doi: 10.1016/j.cpr.2013.08.005
Re, A. M., Capodieci, A., and Cornoldi, C. (2015). Effect of training focused on executive functions (attention, inhibition, and working memory) in preschoolers exhibiting ADHD symptoms. Front. Psychol. 6:1161. doi: 10.3389/fpsyg.2015.01161
Reale, L., Bartoli, B., Cartabia, M., Zanetti, M., Costantino, M. A., Canevini, M. P., et al. (2017). Comorbidity prevalence and treatment outcome in children and adolescents with ADHD. Eur. Child Adolesc. Psychiatr. 26, 1443–1457. doi: 10.1007/s00787-017-1005-z
Roberts, W., Milich, R., and Barkley, R. A. (2015). “Primary symptoms, diagnostic criteria, subtyping, and prevalence of ADHD,” in Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 4th Edn. eds R. A. Barkley (New York, NY: Guilford Press), 51–80.
Shuai, L., Daley, D., Wang, Y.-F., Zhang, J.-S., Kong, Y.-T., Tan, X., et al. (2017). Executive function training for children with Attention Deficit Hyperactivity Disorder. Chin. Med. J. 130:549. doi: 10.4103/0366-6999.200541
Sonuga-Barke, E. J. S. (2003). The dual pathway model of AD/HD: an elaboration of neuro-developmental characteristics. Neurosci. Biobehav. Rev. 27, 593–604. doi: 10.1016/j.neubiorev.2003.08.005
Sonuga-Barke, E. J. S., Brandeis, D., Cortese, S., Daley, D., Ferrin, M., Holtmann, M., et al. (2013). Nonpharmacological interventions for ADHD: systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatr. 170, 275–289. doi: 10.1176/appi.ajp.2012.12070991
Steiner, N. J., Frenette, E. C., Rene, K. M., Brennan, R. T., and Perrin, E. C. (2014). Neurofeedback and cognitive attention training for children with attention-deficit hyperactivity disorder in schools. J. Dev. Behav. Pediatr. 35, 18–27. doi: 10.1097/DBP.0000000000000009
Steiner, N. J., Sheldrick, R. C., Gotthelf, D., and Perrin, E. C. (2011). Computer-based attention training in the schools for children with Attention Deficit/Hyperactivity Disorder: a preliminary trial. Clin. Pediatr. 50, 615–622. doi: 10.1177/0009922810397887
Sterne, J. A., Hernán, M. A., Reeves, B. C., Savovi,ć, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 355:i4919. doi: 10.1136/bmj.i4919
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., et al. (2019). RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366:l4898. doi: 10.1136/bmj.l4898
Swanson, J., Baler, R. D., and Volkow, N. D. (2011). Understanding the effects of stimulant medications on cognition in individuals with attention-deficit hyperactivity disorder: a decade of progress. Neuropsychopharmacology 36, 207–226. doi: 10.1038/npp.2010.160
Tamm, L., Epstein, J. N., Peugh, J. L., Nakonezny, P. A., and Hughes, C. W. (2013). Preliminary data suggesting the efficacy of attention training for school-aged children with ADHD. Dev. Cogn. Neurosci. 4, 16–28. doi: 10.1016/j.dcn.2012.11.004
Tamm, L., and Nakonezny, P. A. (2015). Metacognitive executive function training for young children with ADHD: a proof-of-concept study. ADHD Atten. Deficit Hyperactivity Disord. 7, 183–190. doi: 10.1007/s12402-014-0162-x
Toplak, M. E., Connors, L., Shuster, J., Knezevic, B., and Parks, S. (2008). Review of cognitive, cognitive-behavioral, and neural-based interventions for attention-deficit/hyperactivity disorder (ADHD). Clin. Psychol. Rev. 28, 801–823. doi: 10.1016/j.cpr.2007.10.008
Trani, M., Di, Casini, M. P., Capuzzo, F., Gentile, S., Bianco, G., Menghini, D., et al. (2011). Executive and intellectual functions in attention-deficit/hyperactivity disorder with and without comorbidity. Brain Dev. 33, 462–469. doi: 10.1016/j.braindev.2010.06.002
van der Donk, M., Hiemstra-Beernink, A.-C., Tjeenk-Kalff, A., van der Leij, A., and Lindauer, R. (2015). Cognitive training for children with ADHD: a randomized controlled trial of Cogmed working memory training and ‘paying attention in class’. Front. Psychol. 6:1081. doi: 10.3389/fpsyg.2015.01081
van der Oord, S., Ponsioen, A. J., Geurts, H. M., Ten Brink, E. L., and Prins, P. J. (2014). A pilot study of the efficacy of a computerized executive functioning remediation training with game elements for children with ADHD in an outpatient setting: outcome on parent- and teacher-rated executive functioning and ADHD behavior. J. Attent. Disord. 18, 699–712. doi: 10.1177/1087054712453167
van Dongen-Boomsma, M., Vollebregt, M. A., Buitelaar, J. K., and Slaats-Willemse, D. (2014). Working memory training in young children with ADHD: a randomized placebo-controlled trial. J. Child Psychol. Psychiatr. 55, 886–896. doi: 10.1111/jcpp.12218
Vinogradov, S., Fisher, M., and de Villers-Sidani, E. (2012). Cognitive training for impaired neural systems in neuropsychiatric illness. Neuropsychopharmacology 37, 43–76. doi: 10.1038/npp.2011.251
Weyandt, L. L., and Gudmundsdottir, B. G. (2015). “Developmental and neuropsychological deficits in children with ADHD,” in Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 4th Edn. ed R. A. Barkley (New York, NY: Guilford Press), 116–139.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., and Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol. Psychiatr. 57, 1336–1346. doi: 10.1016/j.biopsych.2005.02.006
Yáñez-Téllez, G., Romero-Romero, H., Rivera-García, L., Prieto-Corona, B., Bernal-Hernández, J., Marosi-Holczberger, E., et al. (2012). Cognitive and executive functions in ADHD. Actas Esp. Psiquiatr. 40, 293–298.
Keywords: attention deficit/hyperactivity disorder, ADHD, cognitive training, executive functions, intervention, review
Citation: Veloso A, Vicente SG and Filipe MG (2020) Effectiveness of Cognitive Training for School-Aged Children and Adolescents With Attention Deficit/Hyperactivity Disorder: A Systematic Review. Front. Psychol. 10:2983. doi: 10.3389/fpsyg.2019.02983
Received: 24 September 2019; Accepted: 16 December 2019;
Published: 14 January 2020.
Edited by:
Daniela Smirni, University of Palermo, ItalyReviewed by:
Carmen Berenguer, University of Valencia, SpainMarie Geurten, University of Liège, Belgium
Copyright © 2020 Veloso, Vicente and Filipe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreia Veloso, YW5kcmVpYXZlbG9zb0BmcGNlLnVwLnB0
†These authors share last authorship