 Virginia Burgdorf
Virginia Burgdorf Marianna Szabó
Marianna Szabó Maree J. Abbott
Maree J. Abbott
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 06 June 2019
Sec. Psychology for Clinical Settings
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.01336
This article is part of the Research Topic Application of the Third Generation of Cognitive-Behavioral Approaches to Parenting View all 15 articles
Background: The psychological well-being of parents and children is compromised in families characterized by greater parenting stress. As parental mindfulness is associated with lower parenting stress, a growing number of studies have investigated whether mindfulness interventions can improve outcomes for families. This systematic review and meta-analysis evaluates the effectiveness of mindfulness interventions for parents, in reducing parenting stress and improving youth psychological outcomes.
Methods: A literature search for peer-reviewed articles and dissertations was conducted in accordance with PRISMA guidelines in the PsycInfo, Medline, PubMed, CINAHL, Web of Science, Cochrane Central Register of Controlled Trials, and ProQuest Dissertations & Theses databases. Studies were included if they reported on a mindfulness-based intervention delivered in person to parents with the primary aim of reducing parenting stress or improving youth psychological outcomes.
Results: Twenty-five independent studies were included in the review. Eighteen studies used a single group design and six were randomized controlled trials. Within-groups, meta-analysis indicated a small, post-intervention reduction in parenting stress (g = 0.34), growing to a moderate reduction at 2 month follow-up (g = 0.53). Overall, there was a small improvement in youth outcomes (g = 0.27). Neither youth age or clinical status, nor time in mindfulness training, moderated parenting stress or overall youth outcome effects. Youth outcomes were not moderated by intervention group attendees. Change in parenting stress predicted change in youth externalizing and cognitive effects, but not internalizing effects. In controlled studies, parenting stress reduced more in mindfulness groups than control groups (g = 0.44). Overall, risk of bias was assessed as serious.
Conclusions: Mindfulness interventions for parents may reduce parenting stress and improve youth psychological functioning. While improvements in youth externalizing and cognitive outcomes may be explained by reductions in parenting stress, it appears that other parenting factors may contribute to improvements in youth internalizing outcomes. Methodological weaknesses in the reviewed literature prevent firm conclusions from being drawn regarding effectiveness. Future research should address these methodological issues before mindfulness interventions for parents are recommended as an effective treatment option for parents or their children.
Parenting stress is associated with negative outcomes for parents and their children (Davis and Carter, 2008; Deater-Deckard et al., 2016). Recently, several studies have linked lower parenting stress with higher parental mindfulness (e.g., Parent et al., 2016; Campbell et al., 2017). Accordingly, a growing number of studies have delivered mindfulness-based interventions to parents, with the aim of reducing parenting stress and improving psychological outcomes for youth (e.g., Zhang et al., 2017; Jones et al., 2018). However, no quantitative synthesis of the literature on the effectiveness of such interventions is currently available. This review and meta-analysis was conducted to evaluate the effectiveness of mindfulness interventions for parents, in reducing parenting stress and improving youth psychological outcomes.
Parents who experience higher parenting stress report poorer psychological well-being (Lavee et al., 1996), more negative affect and less positive affect (Deater-Deckard et al., 2016), and lower marital quality (Robinson and Neece, 2015). In families characterized by greater parenting stress, children have more internalizing and externalizing problems (Huth-Bocks and Hughes, 2007; Davis and Carter, 2008; Robinson and Neece, 2015), poorer cognitive skills such as executive function (de Cock et al., 2017) and more social and interpersonal difficulties (Anthony et al., 2005). Greater parenting stress is also associated with negative parenting behaviors, including harsh discipline (Venta et al., 2016) and hostility (McMahon and Meins, 2012), which have been shown to contribute to poorer child and adolescent psychological outcomes (Rominov et al., 2016; Pinquart, 2017). Managing parenting stress is therefore important for the well-being of parents and their children. It has been suggested that incorporating mindfulness into the parent-child relationship may be one way of achieving this goal (Kabat-Zinn and Kabat-Zinn, 1997; Dumas, 2005; Duncan et al., 2009; Bögels et al., 2010).
In the context of contemporary Western psychology, mindfulness is typically described as a psychological process of bringing non-judgmental awareness to experiences occurring in the present moment (Kabat-Zinn, 2015). Individuals differ in their disposition for mindfulness but can develop their skills through regular practice (Kabat-Zinn, 2003, 2015; Baer et al., 2006). The application of mindfulness to parenting was first described by Kabat-Zinn and Kabat-Zinn (1997). These authors defined mindful parenting as paying non-judgmental, non-reactive attention to each moment and interaction with the child, such that the parent is aware of their child's needs in any moment. Building on this account, Duncan et al. (2009) developed a model of mindful parenting comprising five dimensions: listening to the child with full attention, non-judgmental acceptance of self and child, emotional awareness of self and child, self-regulation in parenting, and compassion for self and child. Mindful parents reduce their use of automatic but unhelpful ways of evaluating or interacting with their child, thus making way for more positive parent-child relationships (Dumas, 2005; Duncan et al., 2009). For example, mindfulness can assist parents to break a habitual pattern of automatically reacting with anger to a child's tantrum, which is likely to elicit further negative affect from the child (Dumas, 2005).
In light of these ideas, mindfulness-based interventions such as the 8-week Mindfulness-based Stress Reduction program (MBSR; Kabat-Zinn et al., 1992), have been offered to parents who experience high levels of stress, anxiety, or depression (Bazzano et al., 2015). Other researchers have adapted the MBSR program specifically to the parenting context (Bögels et al., 2014; Eames et al., 2015). These mindful parenting programs are based upon the same principles of mindfulness as MBSR and follow a similar session structure. MBSR for parents and mindful parenting programs both aim to improve outcomes for families, particularly reducing parenting stress (for example, Neece, 2014; Chaplin et al., 2018). However, mindful parenting programs focus specifically on the stressors faced by parents and the patterns of interaction they have with their children. For example, the well known “observing a raisin” exercise is used in MBSR to illustrate the concept of stepping out of automatic pilot. In one mindful parenting course (Bögels and Restifo, 2014), this exercise is followed by a homework practice in which parents mindfully observe their child, using the skills they learnt while observing a raisin.
In the past decade, a number of studies have explored the effects of both MBSR and mindful parenting interventions on parenting stress. Following MBSR programs, reductions in parenting stress were reported by parents of pre-school aged children with Autism Spectrum Disorder (ASD) and other developmental delays (Chan and Neece, 2018). In a similar clinical sample, the reductions in parenting stress were larger for the MBSR group than a waitlist control group (Neece, 2014). Mindful parenting interventions have been offered in community, as well as in clinical settings. In two small studies of community-recruited parents, no reduction in parenting stress was found following mindful parenting training (Maloney and Altmaier, 2007; Eames et al., 2015), whilst in a larger community study, a reduction was reported (Potharst et al., 2018). The difference in sample sizes may account for the contrasting findings in these studies. In the clinical context, parents of children and adolescents with a range of externalizing and internalizing disorders (Bögels et al., 2014; Ridderinkhof et al., 2017) reported both immediate and maintained reductions in parenting stress following mindful parenting interventions. In contrast, parents of children with Attention Deficit and Hyperactivity Disorder (ADHD) reported a moderate reduction in parenting stress only at 2 month follow-up (van der Oord et al., 2012). The majority of mindful parenting intervention studies have used a single group design. However, a small number of controlled studies have found mindful parenting groups report greater reductions in parenting stress than control groups, in community and clinical settings (Ferraioli and Harris, 2013; Lo et al., 2017a; Corthorn, 2018). In sum, although results are mixed, MBSR and mindful parenting interventions appear to be associated with reduced levels of parenting stress, both in community and clinical contexts.
Studies of MBSR and mindful parenting have also investigated outcomes for the children of parents who attended the interventions. Most studies investigated internalizing and externalizing symptoms, which are the most common psychological problems in youth (Bayer et al., 2008). A number of studies also examined cognitive and social domains of functioning, both of which are related to important longer term problems, such as poorer academic achievement (Malecki and Elliott, 2002; Daley and Birchwood, 2010). Following their parents' attendance at MBSR, pre-school aged children with ASD and other developmental delays showed significant improvements in cognitive, externalizing, and social outcomes (Neece, 2014; Lewallen and Neece, 2015). Following mindful parenting training, small to moderate reductions in youth internalizing problems have been reported by youth with a range of mental health problems and their parents (Bögels et al., 2014; Haydicky et al., 2015; Racey et al., 2017). In contrast, in a study involving 10 adolescents with ADHD, no significant improvements in adolescent internalizing problems were reported (van de Weijer-Bergsma et al., 2012). Similarly, externalizing problems have been reported to reduce after mindful parenting interventions by parents (Bögels et al., 2014; Meppelink et al., 2016) and youth (Bögels et al., 2008; Ridderinkhof et al., 2017) in some studies, but not in others (De Bruin et al., 2015; Jones et al., 2018). In relation to cognitive outcomes, parents have reported fewer attention problems (Ridderinkhof et al., 2017), but no reductions in metacognitive (Zhang et al., 2017) or learning problems (Haydicky et al., 2015). Finally, after mindful parenting interventions, youth social outcomes improved in some studies (Bögels et al., 2008; Haydicky et al., 2015) but not others (De Bruin et al., 2015; Jones et al., 2018). The results of the literature relating to youth outcomes are therefore mixed.
Considering the number of studies and the mixed results they report, a quantitative evaluation of the available data is needed. However, there are no published meta-analyses in this field of research. Further, although two narrative reviews have been conducted, neither of these focuses exclusively on mindfulness interventions delivered to parents. Harnett and Dawe (2012) reviewed 24 interventions incorporating mindfulness, for school students and their careers. Only two of those interventions were delivered to parents. Moreover, those two interventions were not primarily mindfulness interventions. Instead, they incorporated an element of mindfulness into existing behavioral skills programs. Townshend et al. (2016) reviewed seven randomized controlled trials (RCTs) of various interventions delivered to parents. Again, only two of the reviewed trials delivered interventions that were primarily mindfulness-based, while the others incorporated aspects of mindfulness in behavioral or emotion-coaching programs. A review focused upon mindfulness interventions for parents is therefore warranted. Accordingly, the aim of this review was to systematically and quantitatively evaluate the effectiveness of mindfulness interventions for parents. To reflect the range of outcomes covered in the existing literature, the outcomes of interest in this review were parenting stress, and youth functioning across internalizing, externalizing, cognitive, and social domains. Due to the noted similarities between mindful parenting interventions and other mindfulness-based interventions such as MBSR for parents, we amalgamated these studies into a single group and will refer to them together as “mindfulness interventions for parents.”
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and checklist (Moher et al., 2009) were used to guide the conduct and reporting of this review.
Studies were eligible for inclusion in the review if they reported on a mindfulness-based intervention delivered in person to parents, with a primary aim of reducing parenting stress or improving youth psychological outcomes. Studies that met this criterion that also delivered a parallel mindfulness intervention to a child of the participant parents were included. Studies were excluded if they reported on an intervention that was not a mindfulness-based intervention or if the intervention incorporated other forms of therapy or training such as behavioral parent training, acceptance and commitment therapy or cognitive therapy. Studies were also excluded if they used an individual case series or qualitative design.
A comprehensive literature search was conducted between 9 August and 11 October 2018, in the PsycInfo, Medline, PubMed, CINAHL, Web of Science, Cochrane Central Register of Controlled Trials and ProQuest Dissertations & Theses databases, for peer-reviewed articles and published dissertations indexed up to and including 30 September, 2018. In PsycInfo, we searched the database subject headings Mindfulness and Meditation, and the keywords mindful* and meditation, in combination with the subject headings Parenting, Parents, Parenting Style, Parenting Skills, Parental Attitudes, Parent Training, Childrearing Attitudes, Childrearing Practices, Family Intervention and Family Therapy and the key words parent*, child?rearing, family intervention*, and family therap*. For the search, no limitations were placed on the language in which the study was reported. The reference lists of included articles were also searched for relevant studies but no additional studies were identified in this way.
The database search was conducted by the first author. After removal of duplicates, a title and abstract screening of all articles was conducted by the first author to assess the studies against the eligibility criteria. One-third of the articles were also screened independently by a Masters-level graduate student in clinical psychology. A full-text review of the short-listed articles was then conducted independently by both the first author and the same graduate student, with 92% agreement between the two reviewers on the selection of studies for inclusion in the review.
All data was extracted by the first author. The data extracted from each study included participant characteristics, youth age and gender, parent and youth psychopathology, study design, and details of the intervention. These study details are presented in Table 1.
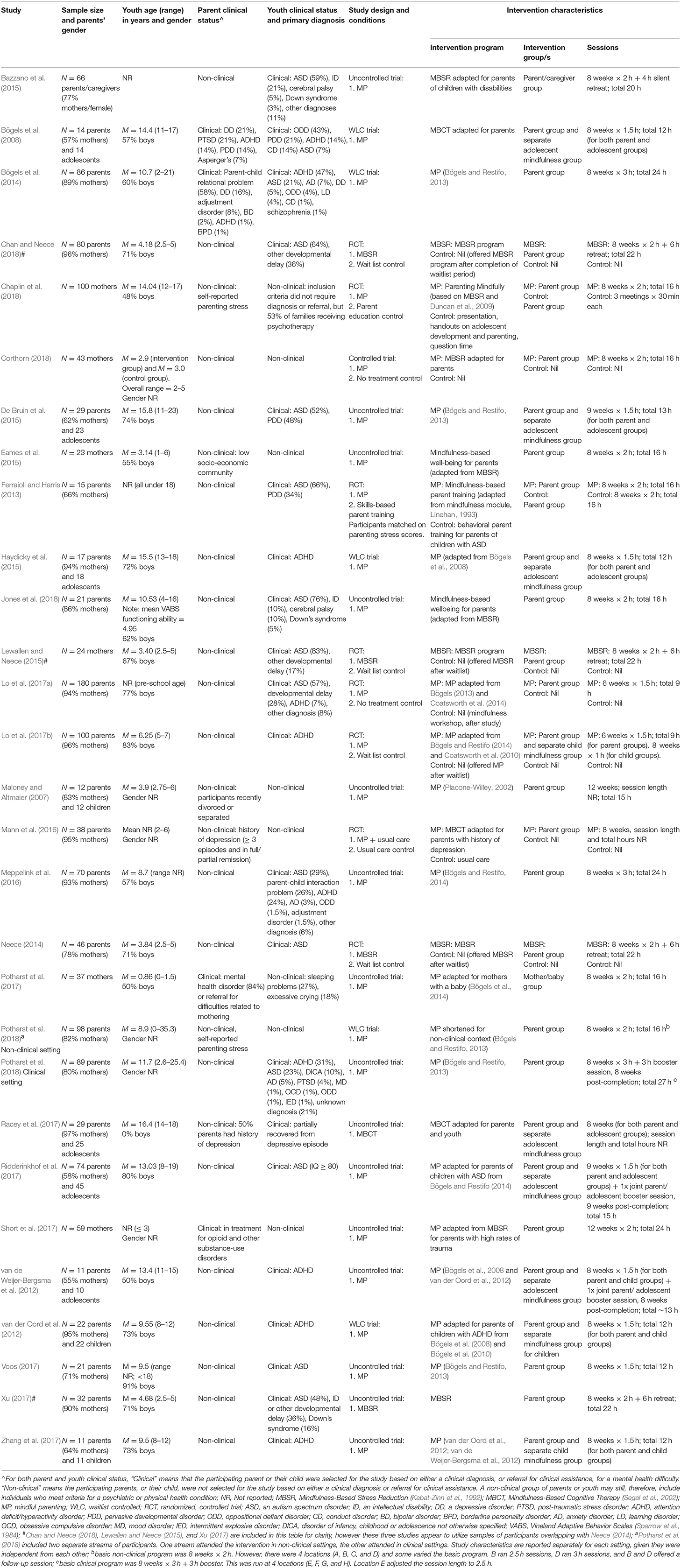
Table 1. Details of included studies.
Effect sizes reported by the study authors for parenting stress and youth psychological outcomes were also extracted and are included in Tables 2, 3, respectively.
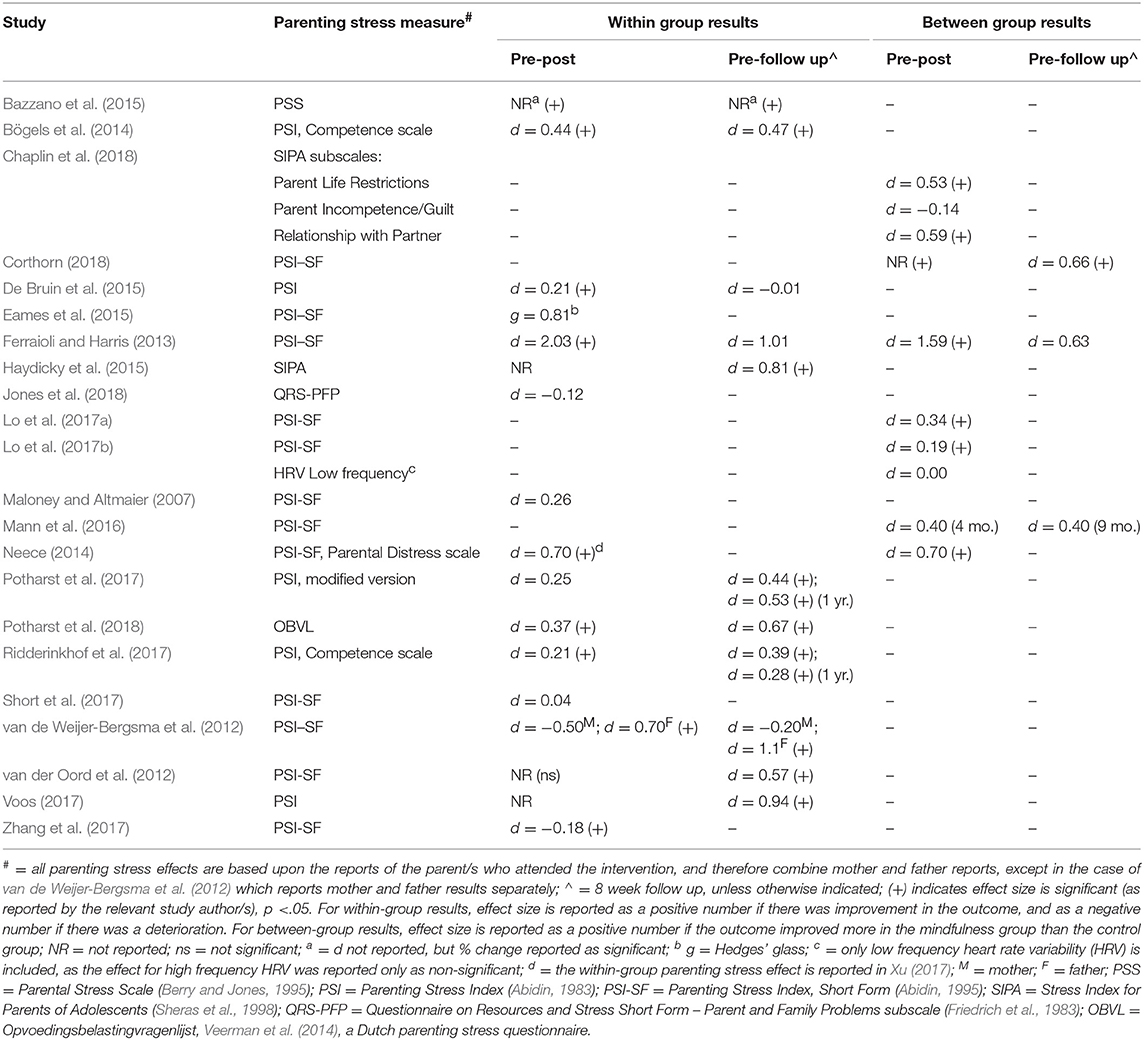
Table 2. Reported results of mindfulness intervention, for parenting stress.

Table 3. Reported results of mindfulness intervention, for youth psychological outcomes.
Quantitative data needed for calculation of effect sizes in the meta-analysis were also extracted. Where a study did not report the data required for calculation of effect sizes, they were requested by email from the corresponding author of the study. If no response was received, the study was included in the systematic review (in Tables 1–3), but not included in the quantitative analyses.
The meta-analysis was conducted using the Comprehensive Meta-Analysis program, version 3.0 (CMA). Two types of summary effect were calculated, using means and standard deviations whenever these were available, and statistics such as t and p when they were not. For studies reporting pre- and post-intervention outcome data, we calculated Hedges' g within-group effect sizes. For studies comparing outcomes of mindfulness and control groups, we calculated Hedges' g between-group differences in effect size. Hedges' g is a weighted mean effect size that corrects for potential bias due to small sample sizes (Hedges and Olkin, 1985). Cohen's guidelines that an effect size of 0.20 is small, 0.50 is moderate and 0.80 is large (Cohen, 1988) may be applied to both Cohen's d and Hedges' g effect sizes. For all analyses, a correlation of r = 0.70 was assumed between pre- and post-intervention measures (Rosenthal, 1993). Random-effects models were used for main effects analyses, to reflect the assumption that the true effect size would vary from study to study because study participants were drawn from different populations. Each summary effect reported in this paper is therefore an estimate of the mean of a distribution of true effects (Borenstein et al., 2009). Heterogeneity amongst studies in each main-effect analysis was assessed using the Q and I2 statistics. Q reflects the distance of each study from the summary effect. A significant Q-statistic indicates variance in true effects, rather than variance due only to random sampling error (Borenstein et al., 2009). I2 reflects the proportion of observed variance in effects that is due to heterogeneity, or variance in true effects (Higgins et al., 2003). Higgins et al. suggest that I2 values of 25, 50, and 75% indicate low, moderate, and high heterogeneity, respectively.
Several methodological issues arose in connection with the calculation of the summary effect size for parenting stress. All studies except one reported either a total parenting stress score or the score from a single parenting stress subscale. A parenting stress effect size was therefore calculated for each of these studies, using the single reported outcome score. However, Chaplin et al. (2018) reported separate data for three subscales of the Stress Index for Parents of Adolescents (SIPA; Sheras et al., 1998). Rather than including each of these three subscales as independent effects in the meta-analysis, the procedure described by Borenstein et al. (2009) was followed to create a single, composite effect for this study. Using a single effect ensures that additional weight is not given to this study, as would be the case if the subscales were treated as independent of each other. It also ensures that the precision of the summary effect is not over-estimated due to the positive correlations between each subscale (Borenstein et al., 2009). Under this procedure, the effects for each subscale were averaged to give a composite parenting stress effect size. To calculate the variance of the composite effect, a correlation between the subscales of r = 0.55 was used, based on the reported correlations between the three relevant subscales of r = 0.52–0.57 (Sheras et al., 1998). A similar issue arose in relation to the parenting stress reporter. Although the majority of studies presented data for a single parenting stress reporter, van de Weijer-Bergsma et al. (2012) reported separate data for mothers and fathers. As mothers and fathers were reporting their levels of stress in respect of the same adolescent, the mother and father effects were not independent. Accordingly, a composite mother/father effect size was calculated following the procedure described above, using a correlation between the two outcomes of r = 0.60. This r-value was chosen using the correlations between mother- and father-reports of child anxiety (r = 0.68) and parental rearing (rs between 0.39 and 0.49) reported in Bögels and van Melick (2004), as a guide. Finally, Potharst et al. (2018) reported data separately for parents participating in clinical and non-clinical settings. The effects reported for these two settings have been included separately in all analyses, as if they were data from two separate studies, because they are based on reports from independent groups of parents participating in independent settings.
Due to the limited number of studies reporting on specific youth psychological outcomes, a detailed quantitative analysis was not conducted in respect of each youth outcome covered by the reviewed studies. Instead, specific outcomes were grouped into internalizing, externalizing, cognitive, and social domains, as the reported outcomes all fell within one of these four domains of functioning. In addition, to provide a large enough pool of effects for moderator analyses to be conducted, a new “overall youth outcomes” variable was created. This variable was created by first calculating effect sizes for youth outcomes reported by parents and then calculating a single, composite parent-reported effect size for each study using the Borenstein et al. (2009) procedure described above, assuming a correlation between the outcomes within each study of r = 0.60. In studies reporting a broadband scale for youth outcomes (for example, “Internalizing problems”), the effect for the broadband scale was used in the calculation of the overall youth outcomes summary effect size. Where a study also reported data for the specific scales making up that broadband scale, specific scale effects were not included. In studies where no broadband scale was used, but more than one youth psychological outcome was reported (for example, anxiety and depression), then these were combined to form a composite effect. For studies reporting data for only one relevant youth outcome, then the effect size for that outcome was used for that study. For the two studies that reported separate youth outcome data for two parents or a parent and another family caregiver (van de Weijer-Bergsma et al., 2012; Lewallen and Neece, 2015), a composite parent-reported effect size was calculated using a correlation of r = 0.60 between the two parent or caregiver outcomes. The same two studies also included data from tutor reports on some outcomes. However, for consistency with the other studies, the tutor-reported data was not included in the calculation of the youth outcomes effect for those two studies. Data from youth-reported and objective tests of youth outcomes were also not used, as most studies did not include these data. The single youth outcome effect size for each study was then combined with the others to generate a summary, parent-reported overall youth outcome effect size.
Exploratory moderator analyses were conducted in relation to both parenting stress and overall youth outcomes. For potential categorical moderators, a mixed effects model was used (random-effects within subgroups and fixed-effects across subgroups). The variance of true effect sizes across studies (T2) was estimated by pooling within-group estimates of T2 for each subgroup and applying the common estimate to all studies. This method of estimating T2 is recommended by Borenstein et al. (2009) to increase the accuracy of the estimate, when the number of studies within any subgroup is low. Categorical moderators were tested only when there were four or more studies per subgroup (Fu et al., 2011). To test significance, the Q statistic was calculated between subgroups (QB). Random-effects meta-regression analyses were used to investigate the relationship between parent or youth outcomes and potential continuous moderators.
A risk of bias assessment was conducted for each included study. Bias is defined as the tendency for study results to vary from those that would have been obtained from a well-designed and run RCT on the same participant group (Sterne et al., 2016). The domains assessed for potential bias were confounding (for non-randomized studies only), selection, misclassification, performance, attrition, detection and reporting bias. For RCTs, the Cochrane Risk of Bias tool for Randomized Controlled Trials (Higgins et al., 2011) was used to assess selection bias. However, for all other domains, the Cochrane Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool (Sterne et al., 2016) was used, as that tool appeared more suited to assessing studies of psychological interventions where blinding of participants, researchers and outcome assessments are not possible. For the non-randomized studies, the ROBINS-I tool was used to assess all domains. All included studies were assessed for potential bias independently by both the first author and the graduate student who assisted with study selection. There was 94% agreement in bias ratings, with differences resolved by discussion.
Figure 1 shows the process of study selection and exclusion. The database searches identified 2,628 studies, 928 of which were duplicates. Forty-seven studies were retained after the title and abstract screening. Twenty-three of these studies were excluded based on the full text review, for the reasons set out in Figure 1. Of the 24 retained studies, three studies (Neece, 2014; Lewallen and Neece, 2015; Xu, 2017) appeared to be reporting data from an overlapping participant group. Confirmation was sought by email from the corresponding author but was not received. Lewallen and Neece (2015) and Xu (2017) reported on relevant outcomes that were not included in Neece (2014), but the outcome data for these two studies are reported in Table 3 under Neece (2014), to reflect the apparent non-independence of the outcomes reported in these two studies. When the initial search conducted in August 2018 was updated in October 2018, five additional studies were identified by the first author. Two of these, Chan and Neece (2018) and Neece et al. (2018), also appeared to report data from a group of participants overlapping with those used in Neece (2014). As these two new studies and Neece (2014) all reported on parenting stress, the parenting stress outcomes from Chan and Neece (2018) and Neece et al. (2018) were not included in this review. The child outcome reported by Chan and Neece (2018) was not included in Neece (2014), so this child outcome is reported in Table 3, also under Neece (2014). However, the child outcomes reported in Neece et al. (2018) were also reported in Neece (2014), so this study was not included in this review. Accordingly, 25 independent studies are included in this review.
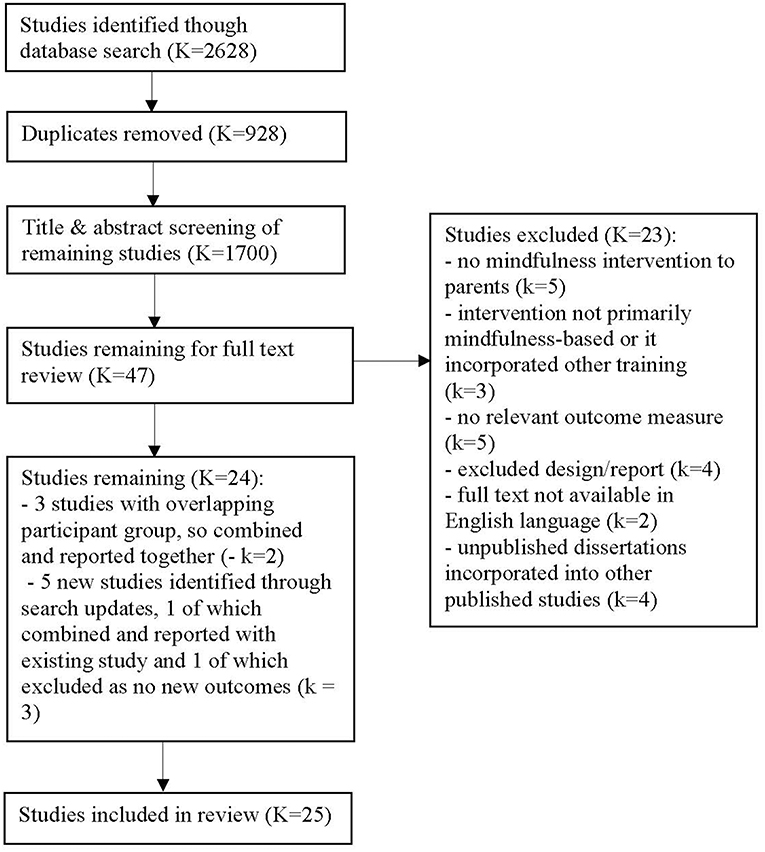
Figure 1. Flow diagram showing process of study selection.
Twenty-five independent studies reported on the effects of a mindfulness intervention for parents. Eighteen studies delivered mindful parenting interventions, five studies delivered MBSR or Mindfulness-based Cognitive Therapy (MBCT) interventions specifically adapted for parents, and four studies (which appeared to use overlapping participant groups) delivered MBSR to parents. Where adaptations were made to standard MBSR or MBCT programs to reflect the fact that the participants were parents, these adaptations were minor. For example, trainers encouraged participants to reflect on how key concepts of mindfulness, such as acceptance and non-reactivity, might apply to their interactions with their children.
All studies delivered the intervention in a group format. Sixteen studies delivered the intervention to parents (including one mother/infant group), while nine delivered parallel mindfulness training to both parents and their children (parents and children in separate groups). In all studies, the majority of participating parents (between 55 and 100%) were mothers. In relation to parental mental health, four studies involved parents referred for mental health treatment for their own mental health condition or parenting difficulties, while another six studies involved parents identified as being vulnerable to mental health difficulties due to socio-demographic factors or past psychiatric history, or who self-reported experiencing parenting stress. The remaining studies did not report on parental mental health status. In relation to youth mental health, the children of participating parents were identified as having mental health diagnoses or difficulties in 20 of the 25 studies. The mean age of children of participating parents ranged from 0.86 to 16.4 years, and 16 studies involved parents with children whose mean age was <12 years.
Sample sizes ranged from 11 to 180 participants. Of the 25 independent studies, 18 utilized a single group design and seven used a control group. Of the controlled trials, six were RCTs. Two RCTs used an active control group (skills-based parent training and parent education), while the remainder used passive controls such as waitlist or usual care groups. Individual session length ranged from 1.5 h (ten studies) to 3 h (three studies). Eight of the ten studies that delivered parallel parent and child interventions used the shorter 1.5 h sessions. The interventions were delivered over 6–12 weeks, and involved total hours of training between 9 and 27 h.
Nineteen studies reported data enabling a quantitative analysis of within-group parenting stress. Figure 2 shows the effect sizes for pre- to post-intervention change in parenting stress, with a summary Hedges' g = 0.34 (p < 0.001, 95% CI [0.23–0.45]). Heterogeneity was moderate to high (Q = 66.96, p = < 0.001, I2 = 70%). Figure 2 reports composite mother/father data for all studies where mothers and fathers participated. In the one study that reported mother and father outcomes separately, the authors found a significant, moderate to large reduction in parenting stress for fathers and a moderate but insignificant increase for mothers (van de Weijer-Bergsma et al., 2012). At first follow-up, which was generally 2 months post-intervention, the summary effect size for change in parenting stress was g = 0.53 (p < 0.001, 95% CI [0.45–0.61]) and heterogeneity was low (Q = 6.62, p = 0.76, I2 = 0%). The difference between pre-post and pre-follow up effect sizes was significant (QB = 7.32, df = 1, p = 0.007). Two studies also reported a 1-year post-intervention follow up. While no quantitative analysis was conducted for this time-point, the reported small to moderate reductions in parenting stress from pre-intervention remained significant [d = 0.53 in Potharst et al. (2017) and d = 0.28 in Ridderinkhof et al. (2017)].
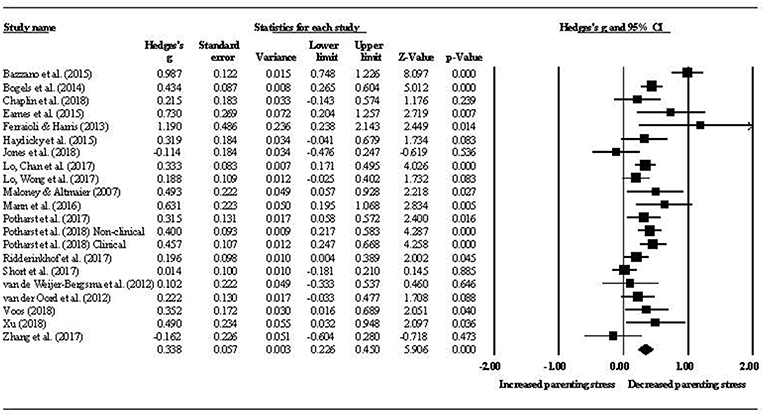
Figure 2. Pre- to post-intervention change in parenting stress.
Moderator analyses were conducted in relation to youth clinical status (clinical vs. non-clinical), youth age (child under 12 years vs. adolescent 12 years and over), and intervention groups (parent only mindfulness group vs. parallel parent and youth mindfulness groups). There were insufficient studies to conduct this analysis in respect of parent clinical status. No significant difference was found between the parenting stress effect sizes for parents attending a mindfulness program based on youth clinical status (g = 0.33, p < 0.001, 95% CI [0.19–0.48] for clinical youth and g = 0.35, p < 0.001, 95% CI [0.16–0.53] for non-clinical youth; QB = 0.01, df = 1, p = 0.906). Similarly, there was no difference in effects between parents of children (g = 0.31, p < 0.001, 95% CI [0.21–0.42]) and adolescents (g = 0.21, p = 0.005, 95% CI [0.06–0.35]) (QB = 1.33, df = 1, p = 0.248). However, the effect size for studies using parent-only intervention groups (g = 0.35, p < 0.001, 95% CI [0.24–0.46]) was greater than that for studies using parallel intervention groups (g = 0.18, p = 0.001, 95% CI [0.07–0.29]) (QB = 4.37, df = 1, p = 0.036). A meta-regression of total intervention hours on parenting stress effect size provided no evidence of a dose-response relationship between total hours spent in the mindfulness intervention and parenting stress (β = 0.01, SE = 0.01, p = 0.26).
Parenting stress was assessed by all studies as an outcome variable rather than as a potential mediator in the relationship between mindfulness in parenting and youth outcomes. One study (Haydicky et al., 2015) examined the direction of relationship between mindful parenting and parenting stress, by using cross-lagged panel correlations. Pre-test mindful parenting scores were significantly negatively correlated with post-test parenting stress [r(14) = −0.52, p = 0.02], but pre-test parenting stress was not significantly correlated with post-test mindful parenting [r(14) = −0.13, p = 0.311].
Five studies reported data enabling a comparison of post-intervention differences in parenting stress between mindfulness and control groups. The summary effect for the difference between these two groups indicated that the mindfulness groups experienced larger reductions in parenting stress than the control groups. This difference was of a small to moderate size (g = 0.44, p = 0.005, 95% CI [0.13–0.74]), with moderate heterogeneity (Q = 8.11, p = 0.087, I2 = 51%). Of these controlled studies, two compared a mindful parenting intervention with another active intervention. Ferraioli and Harris (2013) reported that mindful parenting resulted in a larger reduction in parenting stress than skills-based parent training (d = 1.59). Chaplin et al. (2018) reported that mindful parenting outperformed parent education, in two out of the three parenting stress domains measured (d = 0.53 and d = 0.59). Although not specifically about parenting stress, one study measured parents' heart rate variability and reported an effect of d = 0.00 for the comparison between the mindfulness and control groups (Lo et al., 2017b).
The summary effect sizes for the youth internalizing, externalizing, cognitive, and social domains are presented in Table 4. Post-intervention effect sizes for each domain were small, and all were maintained at 2-month follow-up.
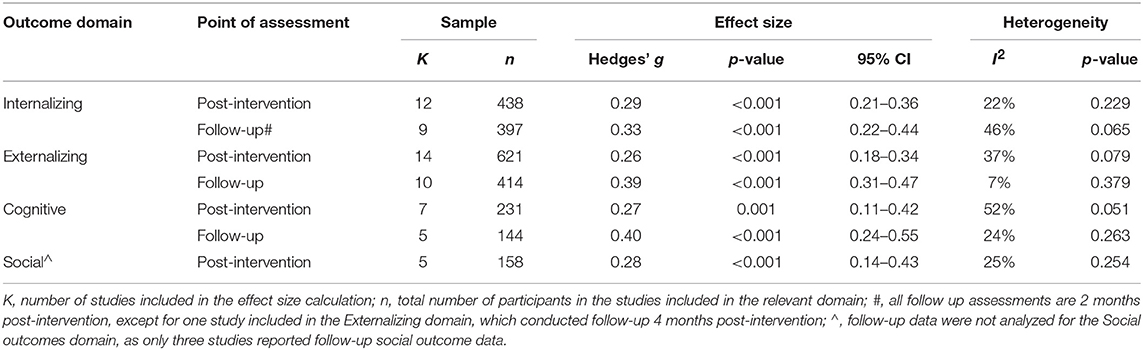
Table 4. Within-group effects for four youth outcome domains.
Figure 3 shows the effect sizes for overall youth outcomes. The summary effect size was g = 0.27 (p < 0.001, 95% CI [0.21–0.33]), with low to moderate heterogeneity (Q = 23.06, p = 0.147, I2 = 26%). At 2-month follow-up, the summary effect was g = 0.35 (p < 0.001, 95% CI [0.27–0.42]), with low heterogeneity (Q = 10.45, p = 0.402, I2 = 4%). There was no difference between pre-post and pre-follow up effects (QB = 2.53, df = 1, p = 0.112).
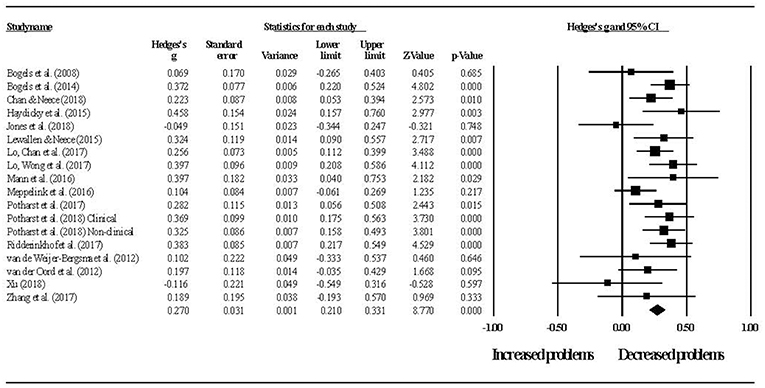
Figure 3. Pre- to post-intervention change in overall youth outcomes.
Despite the relatively low level of heterogeneity in youth outcome effects, moderator analyses were conducted in respect of youth age (child vs. adolescent) and intervention groups (parent only vs. parallel parent and youth groups). There were insufficient studies to conduct this analysis in respect of parent or youth clinical status. No differences were found in overall youth outcome effect sizes for children (g = 0.26, p < 0.001, 95% CI [0.20–0.33]) and adolescents (g = 0.30, p = 0.001, 95% CI [0.13–0.48]) (QB = 0.17, df = 1, p = 0.682) or for studies using parent only interventions (g = 0.26, p < 0.001, 95% CI [0.18–0.33]) and studies using parallel parent and youth interventions (g = 0.31, p < 0.001, 95% CI [0.21–0.41]) (QB = 0.71, df = 1, p = 0.399).
A meta-regression of total intervention hours on overall youth outcomes was conducted, but no evidence was found of a relationship between these two variables (β = 0.00, SE = 0.00, p = 0.844). For those studies reporting both parenting stress and youth outcome data, a series of meta-regressions were conducted to examine whether change in parenting stress predicted youth outcome effect sizes. Change in parenting stress predicted change in both youth externalizing (β = 0.48, SE = 0.21, p = 0.02) and cognitive outcomes (β = 1.13, SE = 0.56, p = 0.046), but not internalizing outcomes (β = −0.32, SE = 0.30, p = 0.282). The same analysis was not performed for the social domain as there were too few studies. Figures 4, 5 show the relationships between change in parenting stress and externalizing outcomes, and change in parenting stress and internalizing outcomes, respectively.
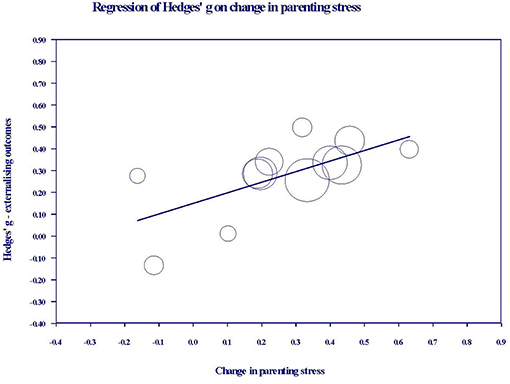
Figure 4. Bubble plot of youth externalizing outcome effects against change in parenting stress. Each bubble represents a study, and the diameter of each bubble is proportional to the study weight.
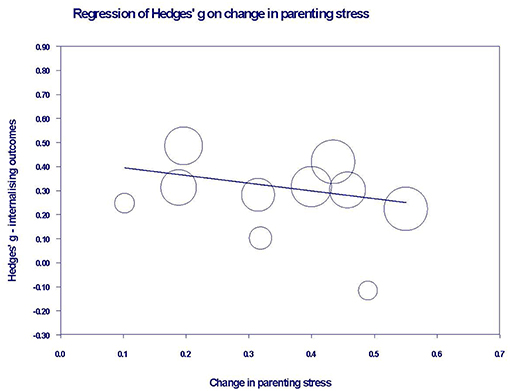
Figure 5. Bubble plot of youth internalizing outcome effects against change in parenting stress. Each bubble represents a study, and the diameter of each bubble is proportional to the study weight.
Insufficient data was available for a quantitative analysis of youth mindfulness, but the effects reported by five studies for this variable (see Table 3) ranged from d = −0.26 to d = 0.50. A small number of studies included objective measures of youth outcomes, such as attention tests. In two studies, the effects obtained in the attention tests were broadly in line with those obtained from self-reports. For example, in Bögels et al. (2008), the youth-reported effect for attention problems was d = 1.00, then d = 0.90 at follow up, while the effect reported based on the D2 Attention Test was d = 0.60, rising to d = 1.10 at follow up. Similarly, in van de Weijer-Bergsma et al. (2012), the youth-reported effect for attention problems was d = 0.50, while the computerized sustained attention task effects ranged between d = 0.20 and d = 0.40. In Zhang et al. (2017), the effects reported for several aspects of attention were variable. For example, the effects in various subtests of sustained attention ranged from d = −0.24 to d = 0.76.
Only one study reported mother and father data on youth outcomes separately (van de Weijer-Bergsma et al., 2012), and two studies obtained teacher reports of youth outcomes (Lewallen and Neece, 2015, reported in Table 3 under Neece, 2014; van de Weijer-Bergsma et al., 2012). Teacher-reported effects were similar to parent-reported effects in van de Weijer-Bergsma et al. However, in Lewallen and Neece, teachers reported significant improvements in all seven of the social domains measured, whereas parents reported significant improvements in only three domains.
No quantitative comparison of the effectiveness of mindfulness interventions to control groups for youth outcomes was performed, as data required for this analysis was only available for three studies. However, of the studies that reported a between-group effect, the mindfulness group outperformed wait list for externalizing problems in two out of five studies [d = 0.29 in Lo et al. (2017b) and d = 0.60 in Mann et al. (2016)] and for internalizing problems in one out of three studies [d = 0.46 in Lo et al. (2017b)]. There were no studies comparing mindfulness with an active control, for youth psychological outcomes.
To assess the impact of any publication bias on the observed effects in this review, the trim and fill method (Duval and Tweedie, 2000) was used to give unbiased estimates of effect size. For within-group parenting stress, the imputed summary effect size was g = 0.33, which was equal to the observed summary effect size of g = 0.33. As shown in Figure 6, the trim and fill analysis indicated that no studies were required to be trimmed in order for the funnel plot to be symmetric, that is for the impact of any publication bias to be removed. In relation to between-group parenting stress, the trim and fill analysis produced an imputed summary effect size of g = 0.32 (compared to the observed g = 0.35), with one study needing to fall on the left of the summary effect for plot symmetry. The impact of any publication bias in relation to parenting stress effects appears likely to be trivial.
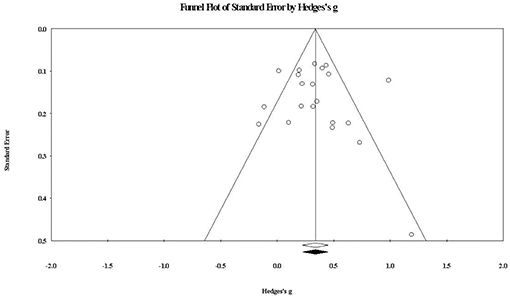
Figure 6. Funnel plot of standard error by within-group parenting stress effect sizes. The white diamond represents the observed summary effect size, while the black diamond represents the imputed summary effect size free of publication bias.
For within-group overall youth outcomes, the funnel plot at Figure 7 shows that one study would need to fall on the right side of the observed summary effect for plot symmetry. The imputed effect size was g = 0.281 (compared to the observed g = 0.276), again suggesting a trivial impact of publication bias.
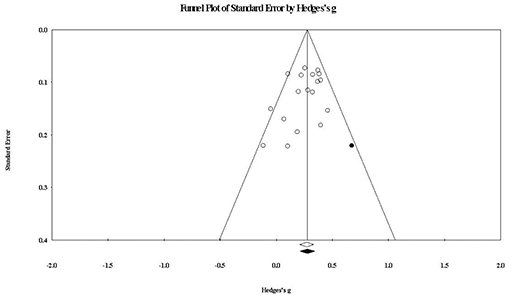
Figure 7. Funnel plot of standard error by within-group overall youth outcomes effect sizes. The black circle represents the effect size of the imputed study that would be required to remove publication bias. The white diamond represents the observed summary effect size, while the black diamond represents the imputed summary effect size free of publication bias.
Table 5 contains risk of bias assessments for each reviewed study. Overall, risk of bias was serious. For the non-randomized intervention studies, this was largely driven by the serious risk of confounding bias, which ROBINS-I notes may occur if any prognostic variable also predicts the intervention received by a participant. Due to the lack of randomization, it is considered likely to be an issue for most if not all non-randomized studies (Sterne et al., 2016). For both non-randomized studies and RCTs, the majority of studies were considered at serious risk of detection bias because of the reliance on subjective self- or parent-about-youth outcome reports, which are considered reasonably vulnerable to the influence of knowledge about the intervention. Bias due to potential misclassification was an issue in many studies, as most reports did not state their pre-intervention position as to the minimum number of sessions a participant would need to attend to be considered as having completed the intervention. Bias may be introduced if the minimum number of sessions was changed after the study commenced. Many studies also reported limited information regarding items such as session attendance rates of treatment completers, homework completion and instructor training, making it difficult to properly assess the risk of performance bias.
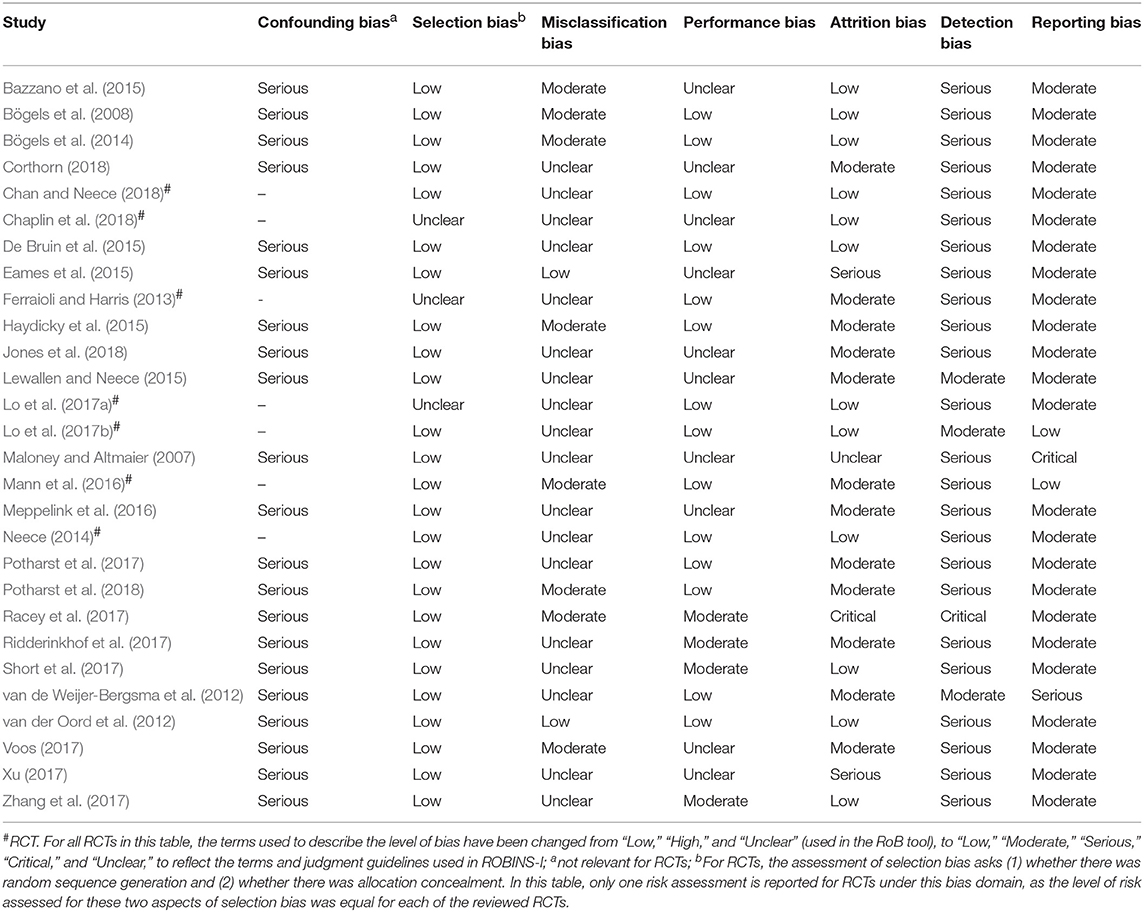
Table 5. Risk of bias assessment for reviewed studies.
This review examined 25 independent studies of mindfulness interventions delivered to parents. We systematically evaluated the effectiveness of these interventions in reducing parenting stress and improving youth psychological outcomes. The results of the review show that mindfulness interventions for parents are associated with small to moderate immediate and maintained reductions in parenting stress. Reductions in parenting stress are greater for parents who attend mindfulness intervention groups than for those who attend control groups. Results also show that mindfulness interventions for parents are associated with small immediate and maintained improvements for youth across internalizing, externalizing, cognitive, and social domains of psychological functioning. Improvements in youth externalizing and cognitive outcomes are predicted by reductions in parenting stress, but no relationship was found between youth internalizing outcomes and parenting stress. There were insufficient studies to test the relationship between parenting stress and social outcomes.
For parenting stress, the small within-group reduction (g = 0.34) obtained immediately after intervention rose to a moderate reduction (g = 0.53) 2 months later. This suggests that the positive impact on parenting stress of the mindfulness intervention continued after the intervention ended. Two studies also measured parenting stress 1 year after the intervention, both reporting the maintenance of small to moderate reductions in parenting stress at that point. The five controlled studies reviewed showed that mindfulness interventions have a small to moderate advantage (g = 0.44) over active and waitlist controls in reducing parenting stress. These results, together with the finding that pre-test mindful parenting scores are negatively correlated with post-test parenting stress, but not vice versa (Haydicky et al., 2015), provide initial evidence that mindfulness interventions for parents contribute to reduced parenting stress.
To place our findings regarding the parenting stress effect size into context, we sought to compare the current results against those obtained in other meta-analyses. We were unable to find meta-analyses of mindfulness or other interventions that aimed at lowering parenting stress specifically. However, Lundahl et al. (2006a) assessed parental emotional adjustment, which incorporated parenting stress. They reported a moderate within-group improvement in that outcome, in their review of parent programs to reduce child abuse. The post-intervention effect in that study (d = 0.53) was larger than in the present study (g = 0.34). This may have been because the measure of parental emotional adjustment included a number of negative emotional states, such as anger, in addition to parenting stress. It is therefore possible that the effect size was driven by improvements in emotional states other than parenting stress.
We also sought to compare the advantage we found for mindfulness interventions over control groups to that found for other parent interventions. Again, we were unable to find any published meta-analyses concerning parenting stress as a stand-alone outcome. However, Lundahl et al. (2006b) reviewed the effects of parent training programs on a composite parenting outcome, which included parenting stress. Lundahl et al. (2006b) defined behavioral training programs as those teaching parents to reinforce their children's positive behavior and ignore or punish poor behavior. Non-behavioral programs were defined as those that did not teach these specific skills, and included programs aimed at improving parent-child communication or altering child-related cognitions. Based on this definition, mindfulness interventions are non-behavioral programs, and indeed the advantage over controls in the present study (g = 0.44) is similar to that found by Lundahl et al. (2006b) for non-behavioral parent programs (d = 0.48). The advantage of behavioral programs over controls was slightly larger (d = 0.53).
Interestingly, this review also found that the reduction in parenting stress was greater at follow up than post-intervention. This is in contrast to the pattern reported for behavioral parent training by Lee et al. (2012), who found a reduced effect at follow-up for a composite parenting outcome that included parenting stress. Similarly, the effects of cognitive behavioral therapy for general stress are maintained at follow up, but not increased (Hofmann et al., 2012). The present results suggest, therefore, that mindfulness interventions provide durable outcomes for parents, and compare favorably in this respect to behavioral parent training and cognitive behavioral therapy.
Heterogeneity in relation to parenting stress is moderate to high, indicating variance in the true effect size across studies. Possible reasons for this variability were tested through categorical moderator analyses and meta-regression. The reduction in parenting stress was not moderated by either youth age or clinical status, or the length of the mindfulness course. This suggests that parents acquire generic skills in mindfulness programs lasting from 9 to 27 h, that they are able to apply in various parenting environments, and across their child's development. In contrast, the reduction in parenting stress was greater when the intervention was delivered only to parents, than when it was delivered to parallel parent and youth groups. This result was surprising, since it is reasonable to expect that training both parents and their children in mindfulness would contribute to better outcomes, given the bi-directionality of parent and child factors (Branje et al., 2010; Neece, 2014). To investigate this result further, the characteristics of the two subgroups were checked. Of the six studies in the parallel interventions subgroup, five involved youth diagnosed with ADHD. However, amongst the 15 studies in the parent-only intervention subgroup, only three involved parents whose children had been diagnosed with ADHD. Further, these three studies reported only 47, 31, and 7% of the parents' children as having ADHD. While no conclusion can be drawn, it is possible that the smaller reduction in parenting stress amongst parents in the parallel intervention subgroup is related to their child's diagnosis of ADHD, rather than the fact that both parents and their children received the intervention.
The results of our review show that mindfulness interventions for parents are associated with improved youth outcomes. The summary effects indicate small, within-group improvements in internalizing (g = 0.29), externalizing (g = 0.26), cognitive (g = 0.27), and social (g = 0.28) domains. These improvements are maintained after 2 months for the internalizing (g = 0.33), externalizing (g = 0.39), and cognitive (g = 0.40) domains. There were insufficient studies to conduct a follow-up analysis for the social domain. There were also insufficient controlled studies to conduct a quantitative comparison of intervention groups with controls, for any of the youth outcomes. The results reported by the few studies that included a control group are mixed, with mindfulness groups outperforming waitlist controls in some studies but not others, for both internalizing and externalizing outcomes.
This is the first published meta-analysis regarding the effectiveness of mindfulness interventions for parents in improving youth outcomes. There are, therefore, no equivalent studies to compare the effects found in the present review against. A review of mindfulness interventions delivered to children and adolescents in schools found within-group effects for emotional problems and cognitive performance of g = 0.31 and g = 0.68, respectively (Zenner et al., 2014). It is possible that the effects reported in that study were larger than those in the present review because the interventions were delivered directly to the children and adolescents, rather than to parents. Looking at other parent-focused interventions, a meta-meta-analysis of studies for treating youth with externalizing disorders obtained effects for youth outcomes (externalizing and internalizing problems combined) of d = 0.46 post-intervention and d = 0.49 at follow-up (Mingebach et al., 2018). The larger improvements found in that review may reflect the fact that the majority of reviewed studies involved behavioral parent training interventions. Mindfulness interventions for parents appear, therefore, to be associated with smaller improvements in youth outcomes than either behavioral parent training or mindfulness interventions for youth.
Heterogeneity in connection with youth outcomes is low to moderate. Mindfulness interventions for parents are associated with equally beneficial outcomes for children and adolescents, whether they attend mindfulness training in parallel with their parents or not, and regardless of the length of the mindfulness course. These results together suggest that even shorter mindfulness programs can result in changes to parental functioning that are positive for youth of any age. Meta-regressions were conducted to check whether change in parenting stress predicted youth outcomes. Greater reductions in parenting stress did predict greater improvements in youth externalizing and cognitive outcomes. This finding is consistent with previous studies showing that parenting stress is related to harsh, over-reactive parenting (Venta et al., 2016), and that harsh parenting predicts later youth behavior problems and poorer attentional regulation (Eisenberg et al., 1999; Rominov et al., 2016). Therefore, reductions in parenting stress may improve externalizing and cognitive outcomes.
Unlike externalizing and cognitive outcomes, reductions in parenting stress did not predict improvements in youth internalizing outcomes. There are a number of possible explanations for this. While youth externalizing problems can be aversive to parents and contribute to higher parenting stress (Eisenberg et al., 1999; Neece et al., 2012), youth internalizing problems tend to be subtle and non-aversive (Eisenberg et al., 1999). Accordingly, it is possible that parents of youth with internalizing problems have a lower baseline level of parenting stress than do parents of youth with externalizing problems. In this case, we would expect a mindfulness intervention for parents of youth with internalizing problems to have less of an impact on parenting stress. Any relationship between change in parenting stress and change in internalizing problems may therefore be too small to detect. Mindfulness interventions for parents could also affect youth internalizing outcomes through a pathway other than parenting stress. For example, greater parental warmth and acceptance toward children are associated with lower youth internalizing problems (Yap and Jorm, 2015). As mindful parenting involves compassion, emotional warmth, and non-judgmental acceptance toward a child (Duncan et al., 2009, 2015), mindfulness interventions may improve internalizing outcomes by promoting these attitudes in parents. Internalizing problems are also associated with difficulties with emotion regulation (Suveg and Zeman, 2004). For example, greater use by parents of adaptive emotion regulation strategies, such as cognitive reappraisal, are associated with lower youth anxiety (Wald et al., 2018). Since mindful parenting is also associated with greater parental self-regulation (Duncan et al., 2009; Ridderinkhof et al., 2017), mindfulness interventions could reduce youth internalizing problems by facilitating healthier forms of emotional regulation in parents.
There are several limitations affecting the strength of the evidence provided by both this review and the individual studies reviewed. At the review level, the number of studies available for inclusion is still small. For this reason, we treated studies of mindful parenting interventions and studies of other mindfulness-based interventions delivered to parents as a single group. However, it is not currently known whether these two types of mindfulness intervention have different outcomes for parents or youth, or whether they exert their effects through different pathways. The number of available studies also had implications for testing potential moderators, such as parent clinical status. It may also have affected our ability to detect significant moderators and covariates. For example, although we found no relationship between the length of the mindfulness course and either parenting stress or youth outcomes, some other meta-analyses have found dose-response relationships for a range of outcomes (Khoury et al., 2013; Zenner et al., 2014; cf. Vollestad et al., 2012). In general, due to the relatively small number of studies in this review, some caution should be applied to the interpretation of the moderator and meta-regression analyses. As more research is published on mindfulness interventions for parents, future reviews with greater power will provide more accurate information regarding significant moderators or covariates.
At the individual study level, small sample sizes are likely to have contributed to a lack of statistical power to detect significant effects in a number of studies. A scan of Tables 2, 3 reveals several moderate to large effects, both post-intervention and at follow-up, that are reported as non-significant. The availability of small samples may have been a reason for the single group design used in most of the reviewed studies. Due to the lack of randomization to intervention or control groups, we cannot conclude that the reported effects are caused by the mindfulness intervention. This is particularly the case for the various outcomes (anxiety, depression, well-being, rumination, and executive functioning) that significantly improved at follow up, but not immediately post-intervention. This longer term effect is consistent with the self-sustaining change proposed to be the result of mindfulness practice (Dumas, 2005). However, childhood is an ongoing period of development in which changes may occur in various domains of functioning over time, for many reasons. When more time has passed, it is more likely that extraneous variables may have contributed to changes in outcomes, making the causal link between the intervention and the effect more tenuous.
All studies were judged to have at least a serious risk of bias. Whilst this was partly due to the lack of randomization noted above, the subjective reporting of most outcomes in each study was also an issue. In the context of mindfulness interventions, which parents must invest a significant amount of time and effort to attend, relying on parent reports may increase the risk of detection bias. Although it is difficult to address this issue in studies in which many outcomes must be subjectively reported, obtaining reports from different sources, such as mothers, fathers, youth and teachers, and obtaining objective measures if possible, may give a more complete picture. For example, Lewallen and Neece (2015) found that teachers reported significant improvements in more social domains than parents did. This suggests that youth outcomes may differ across contexts. Similarly, the differences between mothers and fathers in post-intervention parenting stress (van de Weijer-Bergsma et al., 2012) might indicate a systematic difference in how mothers and fathers respond to a mindfulness intervention. Finally, assessment of treatment adherence and integrity was problematic in many studies, as limited information was reported regarding session attendance rates, homework completion or instructor training. Lack of detailed implementation-related data appears to be a common issue in connection with mindfulness interventions (Vollestad et al., 2012; Zou et al., 2018).
The results of this review show that further research on mindfulness interventions for parents is desirable. Future studies are needed to address the methodological limitations identified above. For example, there is evidence that variables such as therapist experience with mindfulness (Khoury et al., 2013), amount of home practice (Parsons et al., 2017) and total time of mindfulness training (Zenner et al., 2014) can moderate outcomes. Inclusion of more information on these variables would allow reviewers to investigate more potential moderators. In addition, randomizing participants to control and intervention groups would allow firmer conclusions to be drawn about whether mindfulness in parenting played a causal role in relevant outcomes.
Use of randomized controlled studies would also allow comparisons to be made between mindfulness interventions and other active interventions such as behavioral parent training. For youth with externalizing problems, behavioral parent training is an effective and widely used intervention (Dretzke et al., 2009). However, some parents, such as those with their own psychopathology, benefit less from behavioral parent training than others (Maliken and Katz, 2013). This may be because these parents find it difficult to apply new parenting skills in stressful situations with their child and revert to old patterns of responding in those situations (Siegel and Hartzell, 2004). Given its focus upon reducing parenting stress, mindfulness-based interventions might be of greater benefit to these families than behavioral parent training.
The majority of studies involved parents with children under 12 years, or parents managing youth externalizing problems. Very few studies included parents of youth with internalizing problems. It is therefore recommended that additional research be done in community samples or in clinical samples of families experiencing youth internalizing problems. As no relationship was found between parenting stress and youth internalizing outcomes, research with these samples could investigate whether mindfulness in parenting is associated with potential mediators other than parenting stress. These could include parental factors known to be associated with youth internalizing problems. Finally, relatively few studies examined outcomes for families with adolescents and only one of these (Corthorn, 2018) included parents of adolescents without a clinical diagnosis. Adolescence is associated with increased negative affect (Kim et al., 2001) and conflict (Laursen et al., 1998), and may be a time of potentially stressful change in the parent-child relationship (Duncan et al., 2009). Importantly, it is also a time when many psychological disorders are first diagnosed (Copeland et al., 2009). Research could usefully address the question of whether mindfulness interventions for parents of adolescents are effective as a preventive intervention for adolescent psychological problems.
The results of the present review show that mindfulness interventions for parents are associated with reduced parenting stress for parents of both children and adolescents. They are also associated with improved youth psychological functioning across internalizing, externalizing, cognitive, and social domains. Reduced parenting stress predicts improvement in youth externalizing and cognitive outcomes, but not youth internalizing outcomes. Methodological weaknesses in the available literature prevent firm conclusions from being drawn regarding the causal role of mindfulness training for parents in relation to each of these outcomes. Further research is recommended to address limitations in the current literature and questions raised by this review.
VB designed and conducted the review and meta-analysis and wrote the manuscript. MS and MA reviewed the design and collaborated on editing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank Avalon Tissue, Masters of Clinical Psychology student at The University of Sydney, for her contribution in reviewing the list of studies for inclusion, and conducting a risk of bias review of all included studies.
Abidin, R. R. (1995). Parenting Stress Index: Professional Manual 3rd ed. Odessa, FL: Psychological Assessment Resources Inc.
Achenbach, T. M. (1991a). Manual for the Youth Self-Report and 1991 Profile. Burlington: University of Vermont.
Achenbach, T. M. (1991b). Manual for the Child Behaviour Checklist/4-18 and 1991 Profile. Burlington: University of Vermont.
Anthony, L. G., Anthony, B. J., Glanville, D. N., Naiman, D. Q., Waanders, C., and Shaffer, S. (2005). The relationships between parenting stress, parenting behaviour and preschoolers' social competence and behaviour problems in the classroom. Infant Child Dev. 14, 133–154. doi: 10.1002/icd.385
Auyeung, B., Baron-Cohen, S., Wheelwright, S., and Allison, C. (2008). The autism spectrum quotient: children's version (AQ-Child). J. Autism Dev. Disord. 38, 1230–1240. doi: 10.1007/s10803-007-0504-z
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., and Toney, L. (2006). Using self-report assessment methods to explore facets of mindfulness. Assessment 13, 27–45. doi: 10.1177/1073191105283504
Bayer, J. K., Hiscock, H., Ukoumunne, O. C., Price, A., and Wake, M. (2008). Early childhood aetiology of mental health problems: a longitudinal population-based study. J. Child Psychol. Psychiatry, 49, 1166–1174. doi: 10.1111/j.1469-7610.2008.01943.x
Bazzano, A., Wolfe, C., Zylowska, L., Wang, S., Schuster, E., Barrett, C., et al. (2015). Mindfulness based stress reduction (MBSR) for parents and caregivers of individuals with developmental disabilities: a community-based approach. J. Child Family Stud. 24, 298–308. doi: 10.1007/s10826-013-9836-9
Bech, P., Olsen, L. R., Kjoller, M., and Rasmussen, N. (2003). Measuring well-being rather than the absence of distress symptoms: a comparison of the SF-36 Mental Health subscale and the WHO-5 Well-Being Scale. Int. J. Methods Psychiatr. Res. 12, 85–91. doi: 10.1002/mpr.145
Beck, A., Steer, R., and Brown, G. (1996). Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation.
Berry, J. O., and Jones, W. H. (1995). The parental stress scale: initial psychometric evidence. J. Soc. Personal Relation. 12, 463–472. doi: 10.1177/0265407595123009
Bögels, S. (2013). MYmind Mindfulness for Children and Adolescents With ADHD: Therapist's Manual. Amsterdam: University of Amsterdam.
Bögels, S. M., Hellemans, J., van Deursen, S., Romer, M., and van der Meulen, R. (2014). Mindful parenting in mental health care: effects on parental and child psychopathology, parental stress, parenting, coparenting and marital functioning. Mindfulness 5, 536–551. doi: 10.1007/s12671-013-0209-7
Bögels, S. M., Hoogstad, B., van Dun, L., de Schutter, S., and Restifo, K. (2008). Mindfulness training for adolescents with externalising disorders and their parents. Behav. Cogn. Psychother. 36, 193–209. doi: 10.1017/S1352465808004190
Bögels, S. M., Lehtonen, A., and Restifo, K. (2010). Mindful parenting in mental health care. Mindfulness 1, 107–120. doi: 10.1007/s12671-010-0014-5
Bögels, S. M., and Restifo, K. (2013). Mindful Parenting in Mental Health Care. New York, NY: Springer.
Bögels, S. M., and Restifo, K. (2014). Mindful Parenting: A Guide for Mental Health Practitioners. New York, NY: Springer.
Bögels, S. M., and van Melick, M. (2004). The relationship between child-report, parent self-report, and partner report of perceived parental rearing behaviours and anxiety in children and parents. Personal. Individ. Differ. 37, 1583–1596. doi: 10.1016/j.paid.2004.02.014
Borenstein, M., Hedges, L. V., Higgins, J. P. T., and Rothstein, H. R. (2009). Introduction to Meta-Analysis. Chichester: John Wiley.
Branje, S. J., Hale, W., Frijns, T., and Meeus, W. (2010). Longitudinal associations between perceived parent-child relationship quality and depressive symptoms in adolescence. J. Abnormal Child Psychol. 38, 751–763. doi: 10.1007/s10802-010-9401-6
Brown, K. W., and Ryan, R. M. (2003). The benefits of being present: mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 84, 822–848. doi: 10.1037/0022-3514.84.4.822
Brown, K. W., West, A. M., Loverich, T. M., and Biegel, G. M. (2011). Assessing adolescent mindfulness: validation of an adapted Mindful Attention Awareness Scale in adolescent normative and psychiatric populations. Psychol. Assess. 23, 1023–1033. doi: 10.1037/a0021338
Campbell, K., Thoburn, J. W., and Leonard, H. D. (2017). The mediating effects of stress on the relationship between mindfulness and parental responsiveness. Couple Family Psychol. 6, 48–59. doi: 10.1037/cfp0000075
Chan, N., and Neece, C. L. (2018). Parenting stress and emotion dysregulation among childrenwith developmental delays: the role of parenting behaviours. J. Child Family Stud. 2018:1219. doi: 10.1007/s10826-018-1219-9
Chaplin, T. M., Turpyn, C. C., Fischer, S., Martelli, A. M., Ross, C. E., Leichtweis, R. N., et al. (2018). Parenting-focused mindfulness intervention reduces stress and improves parenting in highly stressed mothers of adolescents. Mindfulness 2018:1026. doi: 10.1007/s12671-018-1026-9
Chorpita, B. F., Yim, L., Moffitt, C. E., Umemoto, L. A., and Francis, S. E. (2000). Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav. Res. Ther. 38, 835–855. doi: 10.1016/S0005-7967(99)00130-8
Coatsworth, J. D., Duncan, L. G., Berrena, E., Bamberger, K. T., Loeschinger, D., Greenberg, M. T., et al. (2014). “The mindfulness-enhanced strengthening families program: integrating brief mindfulness activities and parent training within an evidence-based prevention program,” in Mindfulness in Adolescence, eds E. Oberle and K. Schonert-Reichl (San Francisco, CA: Jossey-Bass), 45–58.
Coatsworth, J. D., Duncan, L. G., Greenberg, M. T., and Nix, R. L. (2010). Changing parents' mindfulness, child management skills and relationship quality with their youth: results from a randomised pilot intervention trial. J. Child Family Stud. 19, 203–217. doi: 10.1007/s10826-009-9304-8
Conners, C. K. (2015). Conners Continuous Performance Test 3rd ed (Conners CPT), Conners Continuous Auditory Test of Attention (Conners CATA) Manual. Canada: Multi-Health Systems Inc.
Constantino, J. N., and Gruber, C. P. (2005). Social Responsiveness Scale (SRS) Manual. Los Angeles, CA: Western Psychological Services.
Copeland, W. E., Shanahan, L., Costello, E. J., and Angold, A. (2009). Which childhood and adolescent psychiatric disorders predict which young adult disorders? Arch. General Psychiatry 66, 764–772. doi: 10.1001/archgenpsychiatry.2009.85
Corthorn, C. (2018). Benefits of mindfulness for parenting for mothers of preschoolers in Chile. Front. Psychol. 9:1443. doi: 10.3389/fpsyg.2018.01443
Daley, D., and Birchwood, J. (2010). ADHD and academic performance: why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom? Child Care Health Dev. 36, 455–464. doi: 10.1111/j.1365-2214.2009.01046.x
Davis, N. O., and Carter, A. S. (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: associations with child characteristics. J. Autism Dev. Disord. 38, 1278–1291. doi: 10.1007/s10803-007-0512-z
De Bruin, E. I., Blom, R., Smit, F. M. A., van Steensel, F. J. A., and Bögels, S. M. (2015). MYmind: mindfulness training for youngsters with autism spectrum disorders and their parents. Autism 19, 906–914. doi: 10.1177/1362361314553279
De Bruin, E. I., Sieh, D. S., Zijlstra, B. J., and Meijer, A. M. (2017). Chronic childhood stress: psychometric properties of the chronic stress questionnaire for children and adolescents (CSQ-CA) in three independent samples. Child Indic. Res. 2017:9478. doi: 10.1007/s12187-017-9478-3
De Bruin, E. I., Zijlstra, B. J., and Bögels, S. M. (2013). The meaning of mindfulness in children and adolescents: further validation of the Child and Adolescent Mindfulness Measure (CAMM) in two independent samples from the Netherlands. Mindfulness 2013:196. doi: 10.1007/s12671-013-0196-8
de Cock, E. S. A., Henrichs, J., Klimstra, T. A., Janneke, B. M. M. A., Vreeswijk, C., Meeus, W. H. J., et al. (2017). Longitudinal associations between parental bonding, parenting stress, and executive functioning in toddlerhood. J. Child Family Stud. 26, 1723–1733. doi: 10.1007/s10826-017-0679-7
De Sonneville, L. M. J. (1999). “Amsterdam neuropsychological tasks: a computer-aided assessment program,” in Cognitive Ergonomics, Clinical Assessment and Computer-assisted Learning: Computers in Psychology Vol. 6, eds B. P. L. M. den Brinker, P. J. Beek, A. N. Brand, S. J. Maarse, and L. J. M. Mulder (Lisse: Swets and Zeitlinger), 187–203.
Deater-Deckard, K., Li, M., and Bell, M. A. (2016). Multifaceted emotion regulation, stress and affect in mothers of young children. Cogn. Emot. 30, 444–457. doi: 10.1080/02699931.2015.1013087
Dretzke, J., Davenport, C., Frew, E., Barlow, J., Stewart-Brown, S., Bayliss, S., and Hyde, C. (2009). The clinical effectiveness of different parenting programmes for children with conduct problems: a systematic review of randomised controlled trials. Child Adolescent Psychiatry Mental Health 3:7. doi: 10.1186/1753-2000-3-7
Dumas, J. E. (2005). Mindfulness-based parent training: strategies to lessen the grip of automaticity in families with disruptive children. J. Clin. Child Adolescent Psychol. 34, 779–791. doi: 10.1207/s15374424jccp3404_20
Duncan, L. G., Coatsworth, J., and Greenberg, M. T. (2009). A model of mindful parenting: implications for parent-child relationships and prevention research. Clin. Child Family Psychol. Rev. 12, 255–270. doi: 10.1007/s10567-009-0046-3
Duncan, L. G., Coatsworth, J. D., Gayles, J. G., Geier, M. H., and Greenberg, M. T. (2015). Can mindful parenting be observed? Relations between observational ratings of mother–youth interactions and mothers' self-report of mindful parenting. J. Family Psychol. 29, 276–282. doi: 10.1037/a0038857
Duval, S., and Tweedie, R. (2000). Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-anaysis. Biometrics 56, 455–463. doi: 10.1111/j.0006-341X.2000.00455.x
Eames, C., Crane, R., Gold, E., and Pratt, S. (2015). Mindfulness-based wellbeing for socio-economically disadvantaged parents: a pre-post pilot study. J. Child. Serv. 10, 17–28. doi: 10.1108/JCS-09-2014-0040
Eisenberg, N., Fabes, R. A., Shepard, S. A., Guthrie, I. K., Murphy, B. C., and Reiser, M. (1999). Parental reactions to children's negative emotions: longitudinal relations to quality of children's social functioning. Child Dev. 70, 513–534. doi: 10.1111/1467-8624.00037
Ferraioli, S. J., and Harris, S. L. (2013). Comparative effects of mindfulness and skills-based parent training programs for parents of children with autism: feasibility and preliminary outcome data. Mindfulness 4, 89–101. doi: 10.1007/s12671-012-0099-0
Fresco, D. M., Moore, M., van Dulmen, M., Segal, Z., Ma, S., Teasdale, J., et al. (2007). Initial psychometric properties of the Experiences Questionnaire: validation of a self-report measure of decentring. Behav. Ther. 38, 234–246. doi: 10.1016/j.beth.2006.08.003
Friedrich, W. N., Greenberg, M. T., and Crnic, K. (1983). A short-form of the Questionnaire on Resources and Stress. Am. J. Mental Deficiency 88, 41–48.
Fu, R., Gartlehner, G., Grant, M., Shamliyan, T., Sedrakyan, A., Wilt, T. J., et al. (2011). Conducting quantitative synthesis when comparing medical interventions: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 64, 1187–1197. doi: 10.1016/jclinepi.2010.08.010
Goia, G. A., Isquith, P. K., Guy, S. C., and Kenworthy, L. (2000). Behaviour Rating Inventory of Executive Function (BRIEF): Professional Manual. Lutz: Psychological Assessment Resources.
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatry 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Gradisar, M., Lack, L., Richards, H., Harris, J., Gallasch, J., Boundy, M., et al. (2007). The flinders fatigue scale: preliminary psychometric properties and clinical sensitivity of a new scale for measuring daytime fatigue associated with insomnia. J. Clinical Sleep Med. 3, 722–728.
Gresham, F. M., and Elliott, S. N. (2008). Social Skills Improvement System Rating Scales. Minneapolis: NCS Pearson.
Harnett, P. H., and Dawe, S. (2012). The contribution of mindfulness-based therapies for children and families and proposed conceptual integration. Child Adolescent Mental Health 17, 195–208. doi: 10.1111/j.1475-3588.2011.00643.x
Haydicky, J., Shecter, C., Wiener, J., and Ducharme, J. M. (2015). Evaluation of MBCT for adolescents with ADHD and their parents: impact on individual and family functioning. J. Child Family Stud. 24, 76–94. doi: 10.1007/s10826-013-9815-1
Hedges, L. V., and Olkin, I. (1985). Statistical Methods for Meta-Analysis. San Diego, CA: Academic Press.
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The cochrane collaboration's tool for assessing risk of bias in randomised trials. Br. Med. J. 343, 1–9. doi: 10.1136/bmj.d5928
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. Br. Med. J. 6, 357–360. doi: 10.1136/bmj.327.7414.557
Hoffman, C., Crnic, K. A., and Baker, J. K. (2006). Maternal depression and parenting: implications for children's emergent emotion regulation and behavioral functioning. Parent. Sci. Pract. 6, 271–295. doi: 10.1207/s15327922par0604_1
Hofmann, S. G., Asnaani, A., Vonk, I. J., Sawyer, A. T., and Fang, A. (2012). The efficacy of cognitive behavioural therapy: a review of meta-analyses. Cogn. Ther. Res. 36, 427–440. doi: 10.1007/s10608-012-9476-1
Huth-Bocks, A. C., and Hughes, H. M. (2007). Parenting stress, parenting behavior, and children's adjustment in families experiencing intimate partner violence. J. Family Violence 23, 243–251. doi: 10.1007/s10896-007-9148-1
Jones, L., Gold, E., Totsika, V., Hastings, R. P., Jones, M., Griffiths, A., et al. (2018). A mindfulness parent wellbeing course: evaluation of outcomes for parents of children with autism and related disabilities recruited through special schools. Eur. J. Special Needs Educ. 33, 16–30. doi: 10.1080/08856257.2017.1297571
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present, and future. Clin. Psychol. 10, 144–156. doi: 10.1093/clipsy/bpg016
Kabat-Zinn, J., and Kabat-Zinn, M. (1997). Everyday Blessings. The Inner Work of Mindful Parenting. New York, NY: First Trade.
Kabat-Zinn, J., Massion, A. O., Kristeller, J., Peterson, L. G., Fletcher, K. E., Pbert, L., et al. (1992). Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. Am. J. Psychiatry 149:936. doi: 10.1176/ajp.149.7.936
Khoury, B., Lecomte, T., Fortin, G., Masse, M., Therien, P., Bouchard, V., et al. (2013). Mindfulness-based therapy: a comprehensive meta-analysis. Clin. Psychol. Rev. 33, 763–771. doi: 10.1016/j.cpr.2013.05.005
Kim, K. J., Conger, R. D., Lorenz, F. O., and Elder, G. H. (2001). Parent-adolescent reciprocity in negative affect and its relation to early adult social development. Dev. Psychol. 37, 775–790. doi: 10.1037/0012-1649.37.6.775
Laursen, B., Coy, K. C., and Collins, W. A. (1998). Reconsidering changes in parent-child conflict across adolescence: a meta-analysis. Child Dev. 69, 817–832. doi: 10.1111/j.1467-8624.1998.tb06245.x
Lavee, Y., Sharlin, S., and Katz, R. (1996). The effect of parenting stress on marital quality: an integrated mother-father model. J. Family Issues 17, 114–135. doi: 10.1177/019251396017001007
Lee, P., Niew, W., Yang, H., Chen, V. C., and Lin, K. (2012). A meta-analysis of behavioural parent training for children with attention deficit hyperactivity disorder. Res. Dev. Disabil. 33, 2040–2049. doi: 10.1016/j.ridd.2012.05.011
Lewallen, A. C., and Neece, C. L. (2015). Improved social skills in children with developmental delays after parent participation in MBSR: the role of parent-child relational factors. J. Child Family Stud. 24, 3117–3129. doi: 10.1007/s10826-015-0116-8
Linehan, M. M. (1993). Skills Training Manual for Treating Borderline Personality Disorder. New York, NY: Guilford Press.
Lo, H. H. M., Chan, S. K. C., Szeto, M. P., Chan, C. Y. H., and Choi, C. W. (2017a). A feasibility study of a brief mindfulness-based program for parents of preschool children with developmental disabilities. Mindfulness 8, 1665–1673. doi: 10.1007/s12671-017-0741-y
Lo, H. H. M., Wong, S. W. L., Wong, J. Y. H., Yeung, J. W. K., Snel, E., and Wong, S. Y. S. (2017b). The effects of family-based mindfulness intervention on ADHD symptomology in young children and their parents: a randomised control trial. J. Attention Disord. 2017:43330. doi: 10.1177/1087054717743330
Lundahl, B., Risser, H. J., and Lovejoy, M. C. (2006b). A meta-analysis of parent training: moderators and follow-up effects. Clin. Psychol. Rev. 26, 86–104. doi: 10.1016/j.cpr.2005.07.004
Lundahl, B., Nimer, J., and Parsons, B. (2006a). Preventing child abuse: a meta-analysis of parent training programs. Res. Soc. Work Pract. 16, 251–262. doi: 10.1177/1049731505284391
Luteijn, E., Luteijn, F., Jackson, S., Volkmar, F., and Mideraa, R. B. (2000). The children's social behaviour questionnaire for milder variants of PDD problems: evaluation of the psychometric characteristics. J. Autism Dev. Disord. 30, 317–330. doi: 10.1023/A:1005527300247
Lyubomirsky, S., and Lepper, H. S. (1999). A measure of subjective happiness. Soc. Indic. Res. 46:137. doi: 10.1023/A:1006824100041
Malecki, C. K., and Elliott, S. N. (2002). Children's social behaviours as predictors of academic achievement: a longitudinal analysis. School Psychol. Quart. 17, 1–23. doi: 10.1521/scpq.17.1.1.19902
Maliken, A. C., and Katz, L. F. (2013). Exploring the impact of parental psychopathology and emotion regulation on evidence-based parenting interventions: a transdiagnostic approach to improving treatment effectiveness. Clin. Child Family Psychol. Rev. 16, 173–186. doi: 10.1007/s10567-013-0132-4
Maloney, R., and Altmaier, E. (2007). An initial evaluation of a mindful parenting program. J. Clin. Psychol. 63, 1231–1238. doi: 10.1002/jclp.20395
Manly, T., Anderson, V., Nimmo-Smith, I., Turner, A., Watson, P., and Robertson, I. H. (2001). The differential assessment of children's attention: the Test of Everyday Attention for Children (TEA-Ch), normative sample and ADHD performance. J. Child Psychol. Psychiatry 42, 1065–1081. doi: 10.1017/S0021963001007909
Mann, J., Kuyken, W., O'Mahen, H., Ukoumunne, O. C., Evans, A., and Ford, T. (2016). Manual development and pilot randomised controlled trial of mindfulness-based cognitive therapy versus usual care for parents with a history of depression. Mindfulness 7, 1024–1033. doi: 10.1007/s12671-016-0543-7
McMahon, C. A., and Meins, E. (2012). Mind-mindedness, parenting stress, and emotional availability in mothers of preschoolers. Early Childhood Res. Quart. 27, 245–252. doi: 10.1016/j.ecresq.2011.08.002
Meijer, A. (2008). Chronic sleep reduction, functioning at school and school achievement in preadolescents. J. Sleep Res. 17, 395–405. doi: 10.1111/j.1365-2869.2008.00677.x
Meppelink, R., de Bruin, E. I., Wanders-Mulder, F. H., Vennik, C. J., and Bögels, S. M. (2016). Mindful parenting training in child psychiatric settings: heightened parental mindfulness reduces parents' and children's psychopathology. Mindfulness 7, 680–689. doi: 10.1007/s12671-016-0504-1
Meyer, T. J., Miller, M. L., Metzger, R. L., and Borkovec, T. D. (1990). Development and validation of the Penn State Worry Questionnaire. Behav. Res. Ther. 28, 487–495. doi: 10.1016/0005-7967(90)90135-6
Mingebach, T., Kamp-Becker, I., Christiansen, H., and Weber, L. (2018). Meta-meta-analysis on the effectiveness of parent-based interventions for the treatment of child externalising behaviour problems. PLoS ONE 13:e0202855. doi: 10.1371/journal.pone.0202855
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:97. doi: 10.1371/journal.pmed1000097
Neece, C. L. (2014). Mindfulness-based stress reduction for parents of young children with developmental delays: implications for parental mental health and child behaviour problems. J. Appl. Res. Intellect. Disabil. 27, 174–186. doi: 10.1111/jar.12064
Neece, C. L., Chan, N., Klein, K., Roberts, L., and Fenning, R. M. (2018). Mindfulness-based stress reduction for parents of children with developmental delays: understanding the experiences of Latino families. Mindfulness 2018:1011. doi: 10.1007/s12671-018-1011-3
Neece, C. L., Green, S. A., and Baker, B. L. (2012). Parenting stress and child behaviour problems: a transactional relationship across time. Am. J. Intellect. Dev. Disabil. 117, 48–66. doi: 10.1352/1944-7558-117.1.48
Neff, K. (2015). The self-compassion scale is a valid and theoretically coherent measure of self-compassion. Mindfulness 7, 264–274. doi: 10.1007/s12671-015-0479-3
Nolen-Hoeksema, S. (2000). The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J. Abnormal Psychol. 109, 504–511. doi: 10.1037/0021-843X.109.3.504
Parent, J., McKee, L. G., Rough, J. N., and Forehand, R. (2016). The association of parent mindfulness with parenting and youth psychopathology across three developmental stages. J. Abnormal Child Psychol. 44, 191–202. doi: 10.1007/s10802-015-9978-x
Parsons, C. E., Crane, C., Parsons, L. J., Fjorback, L. O., and Kuyken, W. (2017). Home practice in mindfulness-based cognitive therapy and mindfulness-based stress reduction: a systematic review and meta-analysis of participants' mindfulness practice and its association with outcomes. Behav. Res. Ther. 95, 29–41. doi: 10.1016/j.brat.2017.05.004
Pelham, W. E., Gnagy, E. M., Greenslade, K. E., and Milich, R. (1992). Teacher ratings of DSM-III-R symptoms for the disruptive behaviour disorders. J. Am. Acad. Child Adolescent Psychiatry 31, 210–218. doi: 10.1097/00004583-199203000-00006
Pinquart, M. (2017). Associations of parenting dimensions and styles with externalizing problems of children and adolescents: an updated meta-analysis. Dev. Psychol. 53, 873–932. doi: 10.1037/dev0000295
Placone-Willey, P. M. (2002). A Curriculum for Mindful Parenting: A Model Development Dissertation. Dissertations Abstracts International, 63(01), 568B (UMI No. 3040781).
Posner, M. I., and Petersen, S. E. (1990). The attention system of the human brain. Ann. Rev. Neurosci. 13, 25–42.
Potharst, E. S., Aktar, E., Rexwinkel, M., Rigterink, M, and Bögels, S. M. (2017). Mindful with your baby: feasibility, acceptability and effects of a mindful parenting group training for mothers and their babies in a mental health context. Mindfulness 8, 1236–1250. doi: 10.1007/s12671-017-0699-9
Potharst, E. S., Baartmans, J. M. D., and Bögels, S. M. (2018). Mindful parenting training in a clinical versus non-clinical setting: an explorative study. Mindfulness 2018:1021. doi: 10.1007/s12671-018-1021-1
Putnam, S. P., Helbig, A. L., Gartstein, M. A., Rothbart, M. K., and Leerkes, E. (2014). Development and assessment of short and very short forms of the Infant Behaviour Questionnaire-revised. J. Personal. Assess. 96, 445–458. doi: 10.1080/00223891.2013.841171
Racey, D. N., Fox, J., Berry, V. L., Blockley, K. V., Longridge, R. A., Simmons, J. L., et al. (2017). Mindfulness-based cognitive therapy for young people and their carers: a mixed-method feasibility study. Mindfulness 2017:842. doi: 10.1007/s12671-017-0842-7
Ridderinkhof, A., de Bruin, E. I., Blom, R., and Bögels, S. M. (2017). Mindfulness-based program for children with autism spectrum disorder and their parents: direct and long-term improvements. Mindfulness 2017:815. doi: 10.1007/s12671-017-0815-x
Robinson, E. A., Eyberg, S. M., and Ross, A. W. (1980). The standardisation of an inventory of child conduct problems. J. Clin. Child Psychol. 9, 22–29.
Robinson, M., and Neece, C. L. (2015). Marital satisfaction, parental stress, and child behavior problems among parents of young children with developmental delays. J. Mental Health Res. Intellect. Disabil. 8, 23–46. doi: 10.1080/19315864.2014.994247
Rominov, H., Giallo, R., and Whelan, T. A. (2016). Fathers' postnatal distress, parenting self-efficacy, later parenting behavior, and children's emotional-behavioral functioning: a longitudinal study. J. Family Psychol. 30, 907–917. doi: 10.1037/fam0000216
Segal, Z., Williams, J., and Teasdale, J. (2002). Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. New York, NY: Guildford Press.
Sheras, P. L., Abidin, R. R., and Konold, T. R. (1998). Stress Index for Parents of Adolescents (SIPA). Lutz: Psychological Assessment Resources Inc.
Shields, A., and Cicchetti, D. (1997). Emotion regulation among school-age children: the development and validation of a new criterion Q-sort scale. Dev. Psychol. 33, 906–916. doi: 10.1037/0012-1649.33.6.906
Short, V. L., Gannon, M., Weingarten, W., Kaltenbach, K., LaNoue, M., and Abatemarco, D. J. (2017). Reducing stress among mothers in drug treatment: a description of a mindfulness based parenting intervention. Matern. Child Health J. 21, 1377–1386. doi: 10.1007/s10995-016-2244-1
Siegel, D. J., and Hartzell, M. (2004). Parenting From the Inside Out: How a Deeper Self-Understanding Can Help You Raise Children Who Thrive. New York, NY: Penguin.
Sparrow, S., Balla, D. A., and Cicchetti, D. (1984). Vineland Adaptive Behaviour Scales. 2nd ed. Minneapolis, MN: Pearson.
Sterne, J. A., Hernan, M. A., Reeves, B. C., Savovic, J., Berkman, N. D., Viswanathan, M., et al. (2016). ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 355:i4919. doi: 10.1136/bmj.i4919
Suveg, C., and Zeman, J. (2004). Emotion regulation in children with anxiety disorders. J. Clin. Child Adolescent Psychol. 33, 750–759. doi: 10.1207/s15374424jccp3304_10
Swanson, J. M., Schuck, S., Porter, M. M., Carlson, C., Hartman, C. A., Sergeant, J. A., et al. (2012). Categorical and dimensional definitions and evaluations of symptoms or ADHD: History of the SNAP and the SWAN rating scales. Int. J. Educ. Psychol. Assess. 10, 51–70.
Townshend, K., Jordan, Z., Stephenson, M., and Tsey, K. (2016). The effectiveness of mindful parenting programs in promoting parents' and children's wellbeing: a systematic review. JBI Database Syst. Rev. Implement. Rep. 2016:2314. doi: 10.11124/JBISRIR-2016-2314
van de Weijer-Bergsma, E., Formsma, A. R., de Bruin, E. I., and Bögels, S. M. (2012). The effectiveness of mindfulness training on behavioural problems and attentional functioning in adolescents with ADHD. J. Child Family Stud. 21, 775–787. doi: 10.1007/s10826-011-9531-7
van der Oord, S., Bögels, S. M., and Peijnenburg, D. (2012). The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. J. Child Family Stud. 21, 139–147. doi: 10.1007/s10826-011-9457-0
Veerman, J. W., Kroes, G., De Meyer, R. E., Nguyen, L. M., and Vermulst, A. A. (2014). Opvoedingsbelasting in kaart gebracht. Een kennismaking Opvoedingsbelastingvragenlijst 2014:16. doi: 10.1007/s12452-014-0016-0
Venta, A., Velez, L., and Lau, J. (2016). The role of parental depressive symptoms in predicting dysfunctional discipline among parents at high-risk for child maltreatment. J. Child Family Stud. 25, 3076–3082. doi: 10.1007/s10826-016-0473-y
Vollestad, J., Nielsen, M. B., and Nielsen, G. H. (2012). Mindfulness- and acceptance-based interventions for anxiety disorders: a systematic review and meta-analysis. Br. J. Clin. Psychol. 51, 239–260. doi: 10.1111/j.2044-8260.2011.02024.x
Voos, A. C. (2017). An Initial Evaluation of the Mindful Parenting Group for Parents of Children with Autism Spectrum Disorder. (Doctoral thesis). Available from ProQuest Dissertations and Theses database. Record number 10634080.
Wald, N., Carthy, T., Shenaar-Golan, V., Tadmor-Zisman, Y., and Ziskind, M. (2018). Influence of maternal negative emotion reactivity and cognitive reappraisal on child anxiety disorder. Depress. Anxiety 35, 353–359. doi: 10.1002/da.22745
Xu, Y. (2017). Parental Stress, Emotion Regulation, Meta-Emotion, and Changes Following an MBSR Intervention. (Doctoral thesis). Available from ProQuest Dissertations and Theses database. Record number 10622067.
Yap, M. B. H., and Jorm, A. F. (2015). Parental factors associated with childhood anxiety, depression and internalising problems: a systematic review and meta-analysis. J. Affect. Disord. 175, 424–440. doi: 10.1016/j.jad.2015.01.050
Zenner, C., Herrnleben-Kurz, S., and Walach, H. (2014). Mindfulness-based interventions in schools: a systematic review and meta-analysis. Front. Psychol. 5:603. doi: 10.3389/fpsyg.2014.00603
Zhang, D., Chan, S. K. C., Lo, H. H. M., Chan, C. Y. H., Chan, J. C. Y., Ting, K. T., et al. (2017). Mindfulness-based intervention for Chinese children with ADHD and their parents: A pilot mixed-method study. Mindfulness 8, 859–872. doi: 10.1007/s12671-016-0660-3
Zou, L., Yeung, A., Quan, X., Boyden, S. D., and Wang, H. (2018). A systematic review and meta-analysis of mindfulness-based (baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 25:5020206. doi: 10.3390/ijerph15020206
Keywords: mindfulness, mindful parenting, parenting intervention, parenting stress, child externalizing, child internalizing, meta-analysis, systematic review
Citation: Burgdorf V, Szabó M and Abbott MJ (2019) The Effect of Mindfulness Interventions for Parents on Parenting Stress and Youth Psychological Outcomes: A Systematic Review and Meta-Analysis. Front. Psychol. 10:1336. doi: 10.3389/fpsyg.2019.01336
Received: 31 October 2018; Accepted: 22 May 2019;
Published: 06 June 2019.
Edited by:
Helena Moreira, University of Coimbra, PortugalReviewed by:
Eleonora Volpato, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyCopyright © 2019 Burgdorf, Szabó and Abbott. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virginia Burgdorf, dmlyZ2luaWEuYnVyZ2RvcmZAc3lkbmV5LmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.