 Lærke Mygind
Lærke Mygind Eva Kjeldsted
Eva Kjeldsted Rikke Dalgaard Hartmeyer1
Rikke Dalgaard Hartmeyer1 Peter Bentsen
Peter Bentsen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol., 03 May 2019
Sec. Environmental Psychology
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.00943
This article is part of the Research TopicHuman-Nature Interactions: Perspectives on Conceptual and Methodological IssuesView all 21 articles
In this systematic review, we summarized and evaluated the evidence for effects of, and associations between, immersive nature-experience on mental, physical, and social health promotion outcomes. Immersive nature-experience was operationalized as non-competitive activities, both sedentary and active, occurring in natural environments removed from everyday environments. We defined health according to the World Health Organization's holistic and positive definition of health and included steady-state, intermediate, and health promotion outcomes. An electronic search was performed for Danish, English, German, Norwegian, and Swedish articles published between January 2004 and May 2017. Manual approaches, e.g., bibliographies from experts, supplemented the literature search. Data were extracted from 461 publications that met the inclusion criteria. To assess the status and quality of the evidence for health promotion effects of immersive nature-experience, we focused on the subset of studies based on controlled designs (n = 133). Outcome level quality of the evidence was assessed narratively. Interventions most often involved adventure-based activities, short-termed walking, and seated relaxation in natural environments. We found positive effects on a range of health promotion outcomes grouped under psychological wellbeing (n = 97; ≈55% positive; ≈13% mixed; ≈29% non-significant; 2% negative); psychosocial function (n = 67; ≈61% positive; ≈9% mixed; ≈30% non-significant); psychophysiological stress response (n = 50; ≈58% positive; ≈18% mixed; ≈24% non-significant), and cognitive performance (n = 36; ≈58% positive; ≈6% mixed; ≈33% non-significant; 3% negative); and social skills and relationships (n = 34; ≈70% positive; ≈7% mixed; ≈22% non-significant). Findings related to outcomes categorized under physical health, e.g., risk of cardiovascular disease, were less consistent (n = 51; ≈37% positive; ≈28% mixed; ≈35% non-significant). Across the types of interventions and outcomes, the quality of the evidence was deemed low and occasionally moderate. In the review, we identify, discuss, and present possible solutions to four core methodological challenges associated with investigating immersive nature-experience and health outcomes: (1) intervention and program complexity; (2) feasibility and desirability of randomization; (3) blinding of participants and researchers; and (4) transferability and generalizability. The results of the review have been published as a popular-scientific report and a scientific research overview, both in Danish language.
Nature may be an affordable, upstream health promotion intervention (Maller et al., 2006) and is widely considered to enhance mental, physical, and social health (Hartig et al., 2011, 2014; Twohig-Bennett and Jones, 2018). However, there are countless ways, situations, and contexts in which nature may be encountered, visited, or used, which in turn may lead to varying health outcomes. While reviews have synthesized the wealth of predominantly correlational literature exploring nature contact and benefits for health (Bowler et al., 2010; Bratman et al., 2012; Hartig et al., 2014; Twohig-Bennett and Jones, 2018), the evidence is both diverse and dispersed. In agreement with Tillmann et al. (2018), we argue that a distinction between types of nature interaction is needed when assessing the evidence, and that existing reviews concerning nature and health have tended to compile interventions that are highly heterogenous (e.g., Twohig-Bennett and Jones, 2018). This approach involves a risk of obscuring the conditions under which contact with nature may or may not promote health outcomes. The consequences are simplified conclusions, reduced interpretational value, and potentially inappropriate health promotion recommendations.
Indicatively, Tillmann et al. (2018) found that that the ratio of positive to non-significant findings varied across three types of nature contact: exposure, i.e., direct and passive or non-specified encounters with natural environments and elements; accessibility, i.e., the likelihood of encountering or interacting with nature; and engagement, i.e., direct, intentional and sustained contact with nature. Exposure to nature and natural elements was most consistently associated with benefits for child and adolescent mental health, whereas accessibility to greenspace and direct engagement with nature provided more mixed results. The difference between the types of contact with nature could be caused by method-related issues or actual differences in achieved outcomes. For example, it is possible that there is a more widespread use of rigorously controlled designs and experimental conditions for exposure-type studies than for accessibility- and engagement-type studies. In this is the case, a focused effort to identify method weaknesses and to improve the quality of the research with consideration and adaptation to the type of nature contact is warranted. However, it is also possible that passive exposure to nature more often provides beneficial outcomes than direct engagement or accessibility to greenspace. This suggests that under some conditions or during specific activities, contact with nature is more likely to have health promoting outcomes than others. This highlights a need for an increased awareness to the context and type of activity involved with nature contact and the circumstances under which positive health promotion outcomes are obtained.
In this systematic review, we focused on the Scandinavian tradition of friluftsliv, which includes concepts such as “outdoor life,” “outdoor recreation and education,” or “adventure recreation and education,” but with an emphasis on achieving a closeness to nature during the activity (Gelter, 2000; Sandell, 2003; Bentsen et al., 2009a). While the tradition is considered to be philosophically rooted in an industrialized, Scandinavian setting, activities in nature which encourage the feeling of being away from everyday life and immersion in the experience is practiced more widely (Gelter, 2000; Sandell, 2003; Bentsen et al., 2009a). These criteria are theorized to be fundamental to, for example, restorative experiences according to the Attention Restoration Theory (Kaplan, 1995) which has inspired much research, in both natural and manmade environments, outside of Scandinavia. However, existing reviews of friluftsliv, henceforth termed “immersive nature-experience,” were mainly oriented toward Scandinavian practice and published in Scandinavian languages (Sandell, 2004; Schantz and Silvander, 2004). Although highly informative, these reviews were based on narrative identification, quality appraisal, and syntheses of the literature. From a medical, best-evidence paradigm point of view, the quality of the evidence was of low quality (Sandell, 2004; Schantz and Silvander, 2004). In these reviews, the research field anno 2004 was described as vast and interdisciplinary, dominated by qualitative and quantitative, correlational research. Therefore, the aim of this systematic review was to provide an updated, comprehensive overview of the existing research literature about the effects of immersive nature-experience and both mental, physical, and social health promotion outcomes.
Three main research questions frame this systematic review: (1) What types of immersive nature-experience and (2) health outcomes have been investigated, and (3) how do different types of immersive nature-experience influence or associate with mental, physical, and social health promotion outcomes.
We did not consider it meaningful or possible to evaluate the participants' acute and individual experience of being away or closeness to nature in the identified studies. Therefore, we operationalized some, perhaps arbitrary, conditions under which the nature experience should take place for the nature experience to be considered immersive: Inspired by Bentsen et al. (2009a), immersive nature-experience was operationalized as non-competitive activities, both sedentary and active, occurring in public natural environments removed from everyday environments. This, for example, did not include activities in sports fields with greenery, competitive sports in natural environments or transport to and from work or school through natural environments. While private gardens may promote health and afford activities in which individuals may immerse themselves in as well as experience a sense of closeness with nature, they are not removed from everyday life settings. Being away is a central experiential element of the type of immersive nature-experience under review, and we therefore excluded garden-based activities unless they occurred in settings removed from the participants' day-to-day life. All motorized activities in natural environments were excluded. We argue that a strength of this approach involves including nature-based interventions and programs that are more comparable in terms of content, e.g., activities and experiential character of the nature contact, situation, e.g., deliberate visits to nature, and activation of pathways, e.g., direct, multisensory contact with nature, to improved health (Kuo, 2015). To differentiate between contexts and situations of the immersive nature-experience in relation to health promotion outcomes, we divided the individual studies in three rough categories, namely recreation, health and social, and education. These are described in more detail in the methods section.
We defined health according to the World Health Organization's holistic and positive definition of health. Health promotion denotes the process of providing structures and empowering people to exert control over the determinants of health and risk factors (Nutbeam, 1998; Marmot, 2005). In other words, health promotion includes actions directed toward supporting active and healthy living and facilitating supportive environments (Nutbeam, 1998). Inspired by the outcome classification by Nutbeam (1998), we included health and social outcomes, e.g., quality of life and health status, but also proximal outcomes that influence health outcomes, i.e., intermediate health outcomes and health promotion outcomes. Intermediate health outcomes represent the determinants of health outcomes, e.g., lifestyle choices and actions. Health promotion outcomes reflect modulations of those personal, social and environmental factors which are means to improving people's control, e.g., improved health literacy, and thereby changing the determinants of health (intermediate health outcomes). Health literacy could, for example, be specified as physical literacy, which is defined as a person's capacities and attitude for engagement in physical activities (Edwards et al., 2018). In other words, this review covers not only narrowly defined health outcomes, such as functional independence or physical and mental health status, but also actions, e.g., physical activity (PA) and diet, and perceptions, e.g., self-concept and health literacy, that are involved in the process of health promotion. The focus of this review will be individual-oriented outcomes, not environmental or community level outcomes, although these are relevant in evaluations of health promotion interventions more broadly. While we maintain an analytical distinction between mental, physical, and social health promotion outcomes for communicative purposes, these are highly interdependent and developments in one outcome is likely to influence others.
The results of the literature search have previously been published as a popular-scientific report (Mygind et al., 2018a) and a scientific research overview (Mygind et al., 2018b), both in Danish language.
The systematic review was inspired by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009) (for PRISMA checklist, please see Supplementary Material A). The review protocol can be accessed on the PROSPERO register of systematic reviews (ID: CRD42017057988)1.
Publications were included if reporting on health promotion outcomes of immersive nature-experience (please see the introduction for the definition of immersive nature-experience and health promotion outcomes). We applied no restrictions pertaining to quality of the studies or population characteristics. To assess the status of the evidence concerning effects of the interventions, we focused our analysis on the subset of studies that included a control group. Since little research based on randomized trials was found, we included non-randomized controlled research with attention to the biases involved with this type of research.
We included existing reviews when all included studies investigated immersive nature-experience and health. In some cases, reviews of exposure to nature more broadly were included if it was possible to extract findings related to immersive nature-experience specifically (e.g., Haluza et al., 2014). We included studies that had been published in Danish, English, German, Norwegian, and Swedish language between January 2004 and May 2017. The latter of these criteria was chosen to extend the knowledge from previous reviews about immersive nature-experience and health, which included studies published before 2004 (Sandell, 2004; Schantz and Silvander, 2004).
Six electronic databases were searched using a generic search string that was adapted to the individual electronic databases (for the generic search string, see Supplementary Material B). These included Dissertation Abstracts, ERIC, PsycINFO, Scopus, SPORTDiscus, and Web of Science. We obtained additional literature on selected websites, through contributions from experts and by searching the reference lists in identified relevant publications.
Identified literature was screened by pairs of two individual reviewers (LM, EK, RH, and EM) by reading through titles and abstracts. Subsequently, full-text eligibility was determined by two independent reviewers. Disagreements were settled through discussion between the two reviewers. If an agreement could not be made, a third reviewer (PB or LM) made the final decision. Please see Figure 1 for PRISMA flow chart.
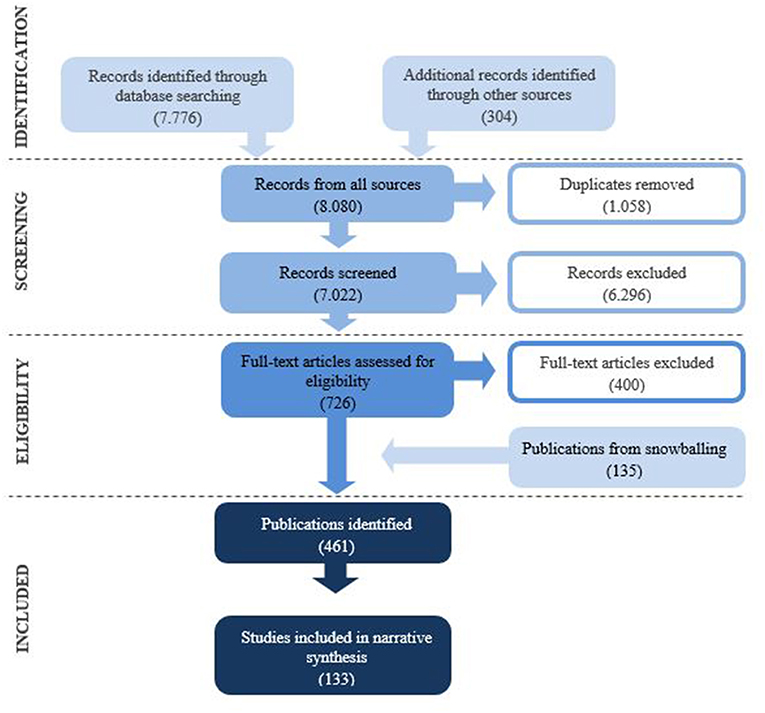
Figure 1. Flow chart.
Two reviewers screened titles and abstracts of 7,022 identified citations, excluding 6,296 publications that were outside the scope of the review. Main reasons for excluding studies at this stage were that studies either investigated only health outcomes, but not immersive nature-exposure, or immersive nature-exposure, but not health.
Subsequently, two reviewers assessed 726 publications in their full length. At this level, studies of types of nature-exposure that did not fall under the definition of immersive nature-experience were excluded. This, for example, included gardening activities (e.g., Sato and Conner, 2013) and school ground greening (e.g., Dyment and Bell, 2008), but also studies in which the place or uses of the natural environments could not be identified (e.g., Zhang et al., 2015). Additional reasons for excluding studies included specifications that, for example, activities occurred indoors (e.g., Siegel et al., 2015); that full-texts could not be obtained (e.g., Jelley, 2005); or the body of the text was written in languages not spoken by members of the review team (e.g., de Assis Pimentel, 2008).
The inclusion of publications identified through snowballing (n = 135) resulted in 461 publications included in the systematic review. Within these 461 publications, 489 individual studies were represented since some publications included more individual studies.
Data were obtained from the literature by a single investigator (LM and EK) using the same generic data extraction form. Data extracted from the literature included: study information (i.e., publication year, authors, and country in which the study was performed); study sample (i.e., sample size, sex, participant characteristics, e.g., information relating to any diagnoses, sociodemographic, or particular group affiliation, and age); study design [inspired by (Ryan et al., 2013)]; activity; duration of exposure; characteristics of natural and control conditions; outcome measures; and reported results. This information is displayed in Tables 1–3.
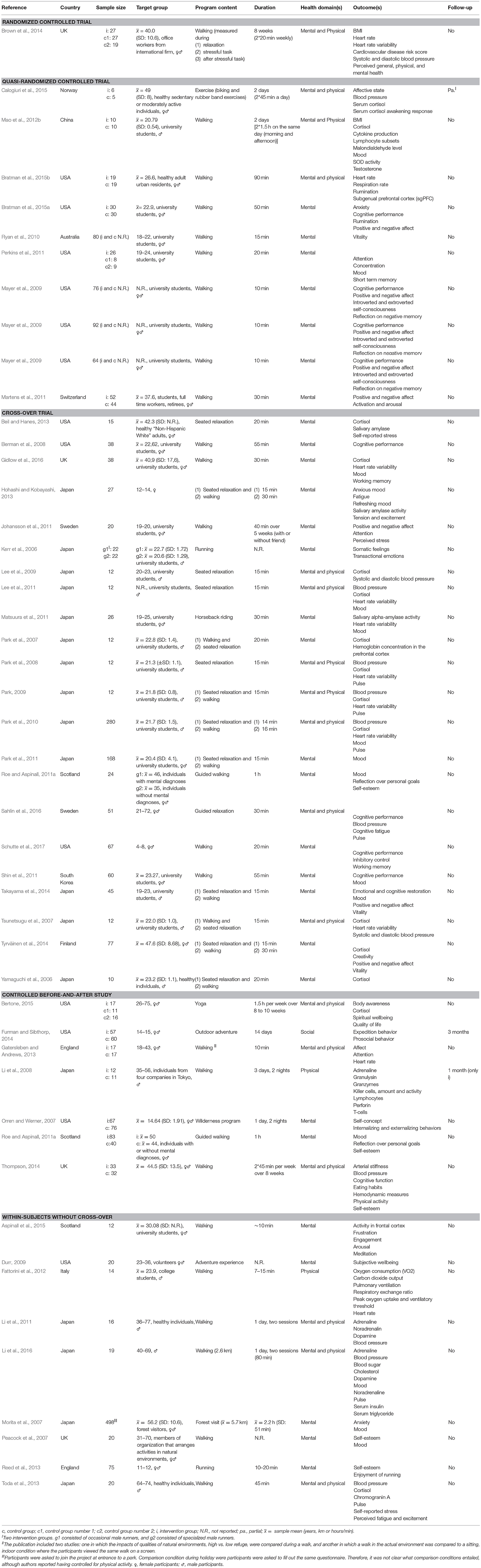
Table 1. Study characteristics, recreation.
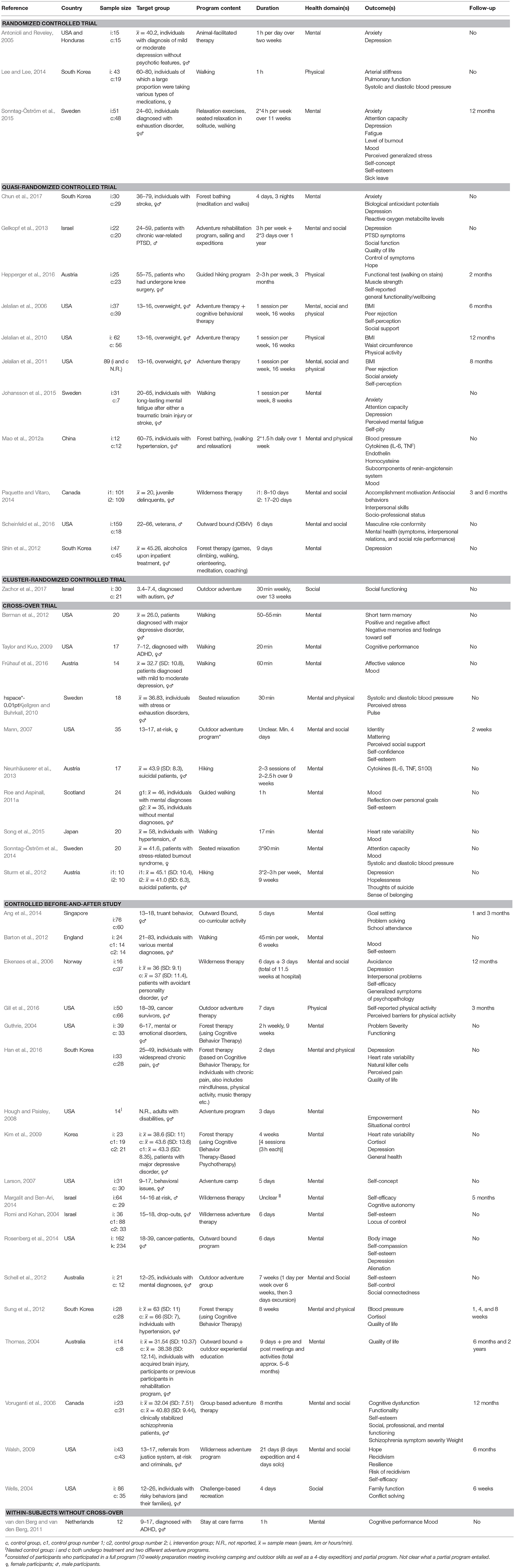
Table 2. Study characteristics, health and social.
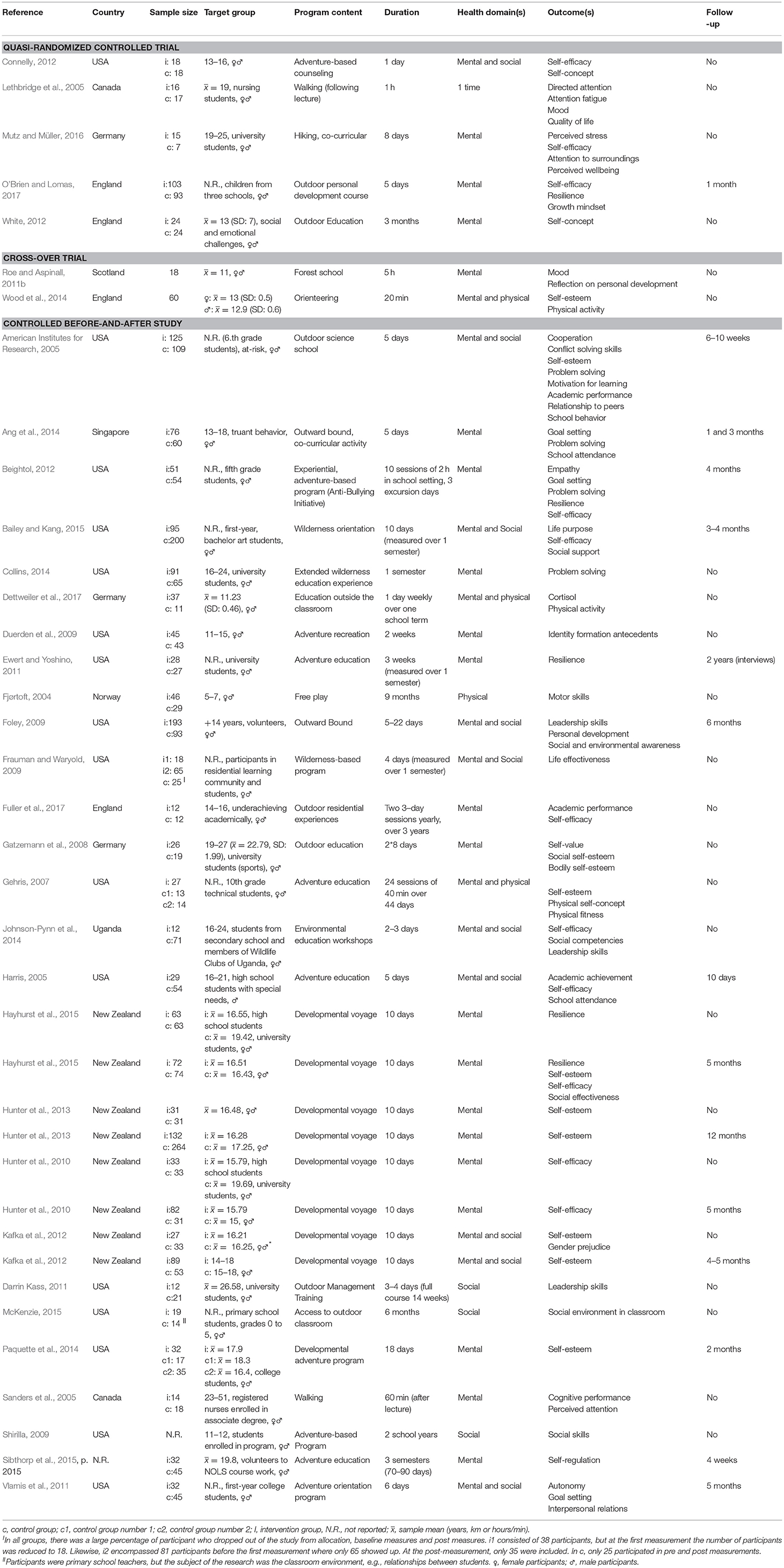
Table 3. Study characteristics, education.
According to the context in which the nature-experience was inscribed, studies were divided into three sectors: (1) recreation; (2) social and health; and (3) day care and education. The first category included types of interventions and programs that occurred during healthy participants' free time, e.g., outside school or work hours. The second category encompassed types of interventions and programs that were used as a form of treatment or offer for specific ill, vulnerable or socially disadvantaged populations. The last category included studies that investigated interventions that were integrated in educational practice, e.g., education outside the classroom (EOtC), or add-ons to educational programs, e.g., semester-start courses or adventure education.
Given the wealth of identified literature and limited resources, we did not systematically assess risk of bias of the individual studies. Risk of bias for individual studies was narratively described. Special attention was given to selection bias related to appropriate randomization of group allocation. In the absence of randomization, we assessed whether recruitment strategies were likely to result in systematic differences between intervention and control groups, and whether sufficient information was provided to ascertain that groups were comparable. Other risk of bias focus areas included ascertainment bias, face-validity of constructs, carry-over effects, as well as attrition, verification, and reporting bias. Lastly, we considered whether power calculations were reported and if sample sizes seemed appropriate. The nature of the interventions makes it impossible to blind participants and instructors to group allocation which might introduce performance bias. However, if this was the only potential source of bias identified, we did not downgrade the quality of evidence at an outcome level. To provide a rough indication of level of evidence, studies were categorized according to the Cochrane Collaboration Study Design Guide (Ryan et al., 2013) from which typical potential sources of bias for the individual types of designs may deduced.
Additionally, we considered the strength of the quantitative, controlled evidence at an outcome level: if most of the studies were randomized, large-scale and without apparent issues relating to bias, we considered the quality of the evidence high. If randomization had been used in most of the studies, but the number of participants was limited, or other issues relating to bias were likely, we considered the quality moderate. If the evidence primarily was based on non-randomized studies, or there were apparent, serious issues relating to bias that could skew the results, we considered the quality of evidence low. If, for example, the effects of immersive nature-experience on psychophysiological stress response was based on a number of non-randomized studies and a few sufficiently powered, appropriately randomized cross-over trials, the quality of the evidence would be considered high. However, if the randomized studies were based on small samples, the quality would be rated moderate. If we additionally found that the studies did not cross-over and counter-balance the order of the exposures, and a carry-over effect would be likely to affect the investigated outcomes, further reductions in the overall assessment of the quality of evidence would be made.
Given the heterogeneity of outcomes and interventions, we did not consider meta-analyses appropriate. Results for individual outcomes were therefore not quantitatively synthesized but summarized by sector, health domain, and results and described narratively in the text (Green et al., 2006). Results were divided into four categories: (1) Intervention had significant positive effect on outcome; (2) intervention had significant positive or non-significant effect on subsets of outcome; (3) findings were non-significant; and (4) intervention had significant negative effect on outcome. Mixed findings thus indicated that subsets of the constructs or markers used to measure the same outcome displayed significantly positive changes, but other subsets were non-significant. For example, in a study investigating the effects of immersive nature-experience on mood, individual subscales that contribute to overall mood were considered subscales and not individual constructs. We did not come across any studies in which some subsets were negatively affected and some non-significant or positive and do therefore not include this category. In the text, we present findings according to the categories relating to type of intervention under the three sectors, i.e., recreation, health and social, and education.
The included studies mainly derived from USA (n = 174), UK (n = 63), Denmark (n = 32), Japan (n = 28), Australia (n = 24), Norway (n = 19), Canada (n = 18), New Zealand (n = 15), Sweden (n = 14), South Korea (n = 10), Austria (n = 7), Germany (n = 5), and Switzerland (n = 5). Other countries represented were Finland, Israel, Italy, Iran, Malaysia, Croatia, Bulgaria, Peru, Tanzania, Uganda, and Brazil.
Amongst the 489 included studies, ≈5% were existing reviews (n = 23), ≈23% qualitative analyses (n = 115), ≈13% a combination of quantitative and qualitative analyses (n = 62), and ≈59% quantitative analyses (n = 289). Amongst the 315 studies including quantitative analyses, ≈42% involved control groups or conditions (n = 133), e.g., randomized controlled-trials, randomized cross-over trials, and controlled before-and-after studies, and ≈69% of the quantitative studies (n = 218) did not involve a control group or condition, e.g., before-and-after and case studies. See Tables 1–3 for characteristics of the individual quantitative, controlled studies and Supplementary Material C for a full list of references for qualitative and observational, quantitative studies.
Participants included healthy adults, adolescents and children as well as populations with behavioral or emotional disturbances [e.g., Attention Deficit/Hyperactivity Disorder (ADHD) or depression], substance abuse issues, delinquent behaviors, social disadvantage, or who were overweight. Amongst all the identified research, ≈28% included only child and adolescent populations (n = 129) under the age of 18.
Results were grouped under psychological wellbeing (n = 97; ≈55% positive; ≈13% mixed; ≈29% non-significant; 2% negative); psychosocial function (n = 67; ≈61% positive; ≈9% mixed; ≈30% non-significant); psychophysiological stress response (n = 50; ≈58% positive; ≈18% mixed; ≈24% non-significant); cognitive performance (n = 36; ≈58% positive; ≈6% mixed; ≈33% non-significant; 3% negative); social skills and relationships (n = 34; ≈70% positive; ≈7% mixed; ≈22% non-significant); and physical health, e.g., risk of cardiovascular disease (n = 51; ≈37% positive; ≈28% mixed; ≈35% non-significant). See Table 4 for results from all outcomes groups, divided by sector, and Supplementary Material D for all individual outcomes. Table 4, for example, shows that we found 57 studies in which positive results were reported, 22 that reported mixed results, 31 non-significant results, and one negative results on mental health outcomes within the recreation sector.
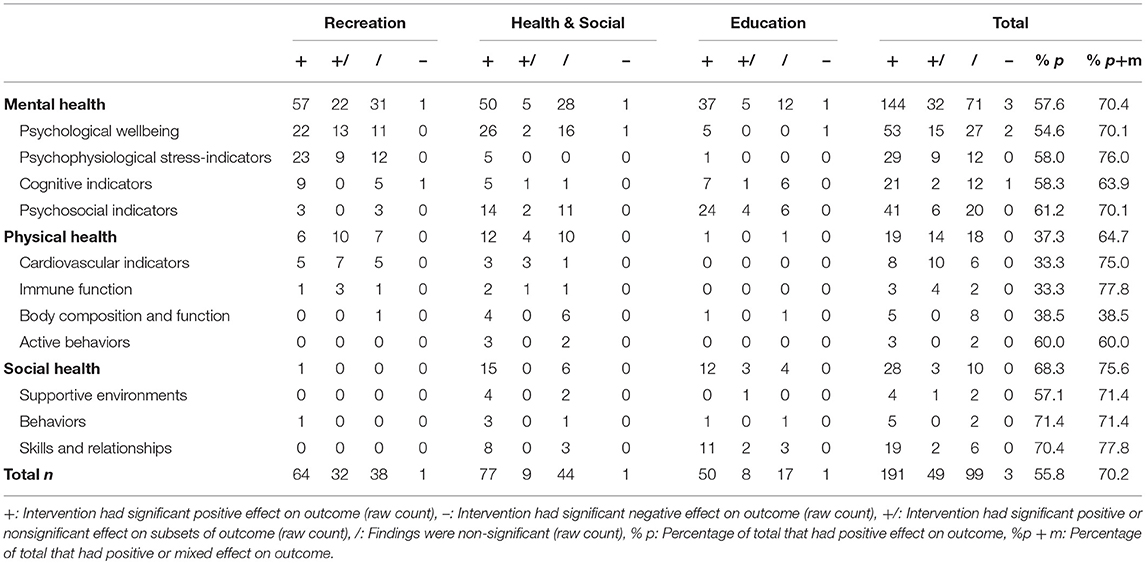
Table 4. Outcomes across sectors and health domains.
In the following, findings are presented in relation to types of interventions and programs categorized by sector, i.e., recreation, health and social, or education, and domain, i.e., mental, physical, and social health. Any identified meta-analyses and reviews are presented first, followed by supplementary, individual studies.
Recreational immersive nature-experience encompassed free-time activities and programs in which healthy participants partook voluntarily. The most common type of activities included short-termed walks or seated relaxation. These activities were sometimes practiced more times over several days in conjunction with cognitive or behavioral therapy. This was often termed shinrin-yuko or forest bathing. We found 168 studies that explored relationships between recreational immersive nature-experience and health of which ≈82% (n = 138) included mental, ≈52% physical (n = 88), and ≈17% social health (n = 29) outcomes. Seven reviews addressed various forms of nature-experience in the recreational sector and presented the literature in a manner allowing for extraction of results from studies relating to immersive nature-experience (Thompson, 2006; Bischoff et al., 2007; Tsunetsugu et al., 2010; Bratman et al., 2012; Voutselas, 2012; Konijnendijk et al., 2013; Haluza et al., 2014).
Below, we focus on reviews and studies that were based quantitative, controlled analyses given the wealth of material. Please see Table 1 for a full summary of quantitative, controlled analyses from the recreational sector.
Several distinct psychological wellbeing constructs were investigated in the identified literature: positive and negative affect; perceived stress; vitality; quality of life; mental and spiritual wellbeing; anxiety; rumination; internalizing and externalizing behaviors, and mood states. Overall, the number of interventions that had a positive (n = 22) or mixed effect on these outcomes (n = 13) outweighed the number of non-significant findings (n = 11) (see Table 4 for the distribution of positive, negative, mixed, and non-significant findings for the individual outcomes). Mixed findings indicate that subsets of the constructs used to measure the outcome displayed significantly positive changes, but not all. Mixed findings were frequent for the outcome mood states. This is discussed further in the following. Given the predominant use of non-randomized designs with small sample sizes and the dispersion of the findings between and, for the outcome mood states, within the distinct outcome constructs, strong conclusions could not be accumulated, and the quality of the evidence was considered low. Below, we provide examples of the interventions and findings.
Levels of self-reported positive affect were increased relatively more for participants when they walked in natural environments compared to urban environments (Mayer et al., 2009; Johansson et al., 2011; Martens et al., 2011; Takayama et al., 2014; Tyrväinen et al., 2014; Bratman et al., 2015a; Calogiuri et al., 2015), but the same could generally not be observed for negative affect (Mayer et al., 2009; Johansson et al., 2011; Martens et al., 2011; Takayama et al., 2014; Bratman et al., 2015a). Roe and Aspinall (2011a) observed that participants with and without mental diagnoses reported decreased stress and enhanced happiness. This was supported in two other studies evaluating the effects of short-termed walks for healthy adults (Beil and Hanes, 2013; Toda et al., 2013). In another study, no significant stress reducing effects was reported (Johansson et al., 2011). Quality of life and spiritual wellbeing was not found to differ following weekly yoga practice over a period of 8 to 10 weeks in natural environments compared to indoors (Bertone, 2015).
Mixed findings stemmed from studies of the effects of short-termed immersive nature-experience on self-reports of transient mood states, encompassing anxiety, anger, vigor, fatigue, depression, and confusion subscales. Here, we treat these subscales as distinct parts of mood, not as individual constructs. Twelve studies investigated effects of short-termed, i.e., 15 min to 2 days (Peacock et al., 2007; Park et al., 2010, 2011; Lee et al., 2011; Matsuura et al., 2011; Perkins et al., 2011; Shin et al., 2011; Mao et al., 2012b; Hohashi and Kobayashi, 2013; Takayama et al., 2014; Li et al., 2016), and 8 weeks of repeated short-termed recreational immersive nature-experience (Thompson, 2014). In all studies, it was reported that some constructs relating to these mood states were improved, although some subscales remained unchanged. No individual constructs consistently changed across the studies. For example, across short exposures in 14 different types of forests, Park et al. (2011) found that all subscales, except for the construct depression, were improved in comparison to exposures to various urban environments. Comparatively, Peacock et al. (2007) found that anger, confusion, depression, and anxiety were relatively more improved, while no such difference could be observed for vigor and fatigue. Likewise, upon an 8 week program, reductions in anxiety and depression were observed, but not the other mood states (Thompson, 2014). The findings relating to individual, distinct mood states seem to point in various directions. As such, immersive nature-experience may improve mood, but the finer distinctions remain unclear.
We found that positive findings (n = 23) only just outweighed mixed (n = 9) and insignificant (n = 12) findings across all psychophysiological indicators of stress, i.e., heart rate variability; cortisol; adrenaline; noradrenaline; dopamine; salivary amylase; and cortisol awakening response2. More uncommon approaches to measuring acute stress response included activity in the frontal cortex and hemoglobin concentration in the prefrontal area of the brain. The studies were mainly designed as randomized, cross-over trials with small samples. Most of the studies (n = 13) included university students of which most were male (85% of the studies). Based on the types of designs and sample sizes used, we considered the overall quality of the evidence moderate. The investigated types of interventions are elaborated in the following and may be supplemented by results from the health and social sectors which are reviewed in section Psychophysiological stress-indicators.
Short-termed walking or seated relaxation in natural environments was frequently (n = 9) found to reduce psychophysiological stress indicators (Lee et al., 2009, 2011, 2014; Park et al., 2010; Li et al., 2011, 2016; Mao et al., 2012b; Toda et al., 2013; Aspinall et al., 2015) more than the same activities in control conditions. Amongst these studies, Toda et al. (2013) compared a physically active natural environment condition with a sedentary indoor condition. As such, results may have been affected by differences relating to differences of PA and not the conditions as such. Six studies also investigating the effects of short-termed walking or seated relaxation reported mixed (Park et al., 2007, 2008; Tsunetsugu et al., 2007; Park, 2009; Calogiuri et al., 2015; Lee et al., 2015) and eight insignificant findings (Yamaguchi et al., 2006; Matsuura et al., 2011; Beil and Hanes, 2013; Hohashi and Kobayashi, 2013; Brown et al., 2014; Tyrväinen et al., 2014; Bertone, 2015; Gidlow et al., 2016), but none directly negative outcomes of the programs.
Calogiuri et al. (2015) found that some, but not all, stress-indicators were improved more upon work day breaks involving green exercise (i.e., biking and rubber band exercises) compared to when the same exercises were performed indoors. Brown et al. (2014) did not find an influence of walking in natural environments during breaks in the work day. Likewise, Matsuura et al. (2011) did not find differences in stress-indicators upon a short horseback ride in natural environments compared to an indoor simulator.
A number of distinct cognitive indicators were investigated within the recreation sector: cognitive task performance; creativity; attention; concentration; inhibitory control; working memory; and short-term memory. Positive findings marginally outweighed (n = 9), negative (n = 1), and non-significant findings (n = 5). The included studies were designed as randomized cross-over trials with small samples, and the overall quality of evidence was considered moderate.
Short-termed walking in natural environments was frequently found to enhance cognitive performance more than the same activities in control conditions (Berman et al., 2008; Mayer et al., 2009; Shin et al., 2011; Sahlin et al., 2016). Indicators of creativity (Tyrväinen et al., 2014) and working memory (Gidlow et al., 2016) were likewise enhanced more after walking in natural environments compared to urban control conditions. One study reported that no differences relating to attention, concentration, and working memory could be observed when comparing three contexts, i.e., one natural and two built environments (Perkins et al., 2011), and another that participants performed worse in an attention task after a walk in a park (Johansson et al., 2011). We found one study conducted with children in which it was found that preschool children responded more quickly in an attention task following a walk in natural environments compared to urban environments (Schutte et al., 2017), but no differences could be observed relating to regulative control and verbal working memory.
Findings within the recreation sector related to cardiovascular indicators, i.e., acute changes in blood pressure and cardiovascular disease risk factors, were more often absent (n = 5) or mixed (n = 7) than positive (n = 5). The included studies were mainly designed as randomized, cross-over trials with small samples. Based on the types of designs and sample sizes used, we considered the overall quality of the evidence moderate.
Acute reductions in blood pressure were most often mixed (n = 6) or insignificant (n = 2): only three studies reported larger reductions in blood pressure after exposure to natural than comparison environments. Haluza et al. (2014) reviewed partially overlapping studies using blood pressure measures, amongst other physiological indicators, and echoed the finding. In addition to studies reviewed by Haluza et al. (2014) and Mao et al. (2012b) found that ET-1, a so-called vasoconstrictor involved with the progression of cardiovascular disease, was reduced subject to two walks in natural environments, but not urban environments amongst a small sample of healthy adults. Likewise, Thompson found that arterial stiffness and hemodynamic measures, both associated with cardiovascular risk of disease, were improved differentially following an 8 week walking program (Thompson, 2014). Another indicator of the occurrence and development of cardiovascular disease, platelet activation, was not significantly different (Mao et al., 2012b), nor was the Framingham cardiovascular disease risk score (Brown et al., 2014).
Four controlled studies investigated the effects of short-termed immersive nature-experience on outcomes related to immune function, i.e., so-called oxidative stress (i.e., the disturbance in the balance between the production of free radicals and antioxidant defenses), pro-inflammatory cytokines (i.e., signaling molecules that mediate innate immune response), and leukocyte or white blood cell subsets. The evidence for impacts of immersive nature-experience on the immune system in healthy subjects was spread over many indicators related to oxidative stress, pro-inflammatory cytokines, and leukocyte subsets. Findings were positive (n = 1) or mixed (n = 4). The included studies were based on between- and within-subjects designs and included small samples, and the overall quality of evidence was considered low to moderate.
Programs of 3 days including one or two walks in forested areas a day were found to have positive effects on a number of immune function indicators, but some subsets were unchanged. study (Li et al., 2008): Leukocyte subsets, i.e., the number of CD3+ cells; granulsyn; granzymes A/B expressing cells; natural killer cells; and perforin, were increased post nature-programs, but not after the same walking activities in urban environments. However, differences in overall white blood cell counts were non-significant. Another study identified no significant effects on immunoglobin A (Tsunetsugu et al., 2007). A quasi-randomized trial (Mao et al., 2012b) included reports of a vast number of immune function indicators: levels of serum pro-inflammatory cytokines were reduced in the forest group; indicators of oxidative stress status were mixed, i.e., levels of malondialdehyde was decreased, but T-SOD not significantly different; and the distribution of leukocyte subsets was likewise mixed, i.e., the levels of B-lymphocytes were increased, but the percentage of natural killer cells; T; T-helper; and T-suppressor lymphocytes were not significantly different.
In the absence of controlled studies relating to social health in the recreation sector, we here discuss findings from observational studies. Konijnendijk et al. (2013) reviewed research on the benefits of recreational use of urban parks, including aspects such as social interaction, collective efficacy, and sense of community. The review included mainly correlational studies of which only three studies explicitly addressed immersive nature-experience as defined in the present review. The scarcity of relevant literature identified in this review corresponds with our review. These studies, two qualitative and one observational, quantitative, indicated that adults and children alike considered that urban green space was a place that enhanced social support and social interaction. The authors of the review found that the field of research was limited and deemed the certainty of the evidence weak, as studies were mainly qualitative or observational (Konijnendijk et al., 2013). Due to the use of designs with no control group, the quality of the evidence for the outcomes related to supportive environments, i.e., social interaction and support, was low.
One hundred-and-seventeen studies investigated health outcomes of immersive nature-experience in the social and health sectors of which ≈86% included mental (n = 147), ≈52% physical (n = 89), and ≈36% social health (n = 62) outcomes. Thirteen reviews addressed various forms of nature-experience in social and health sectors and presented the literature in a manner allowing for extraction of results from studies relating to immersive nature-experience (Bedard, 2004; Wendell, 2004; Bischoff et al., 2007; Grinde and Patil, 2009; Shanahan et al., 2009; Annerstedt and Währborg, 2011; Lubans et al., 2012; Bowen and Neill, 2013; Ejbye-Ernst, 2013; Norton, 2014; Poulsen et al., 2015; Bettmann et al., 2016; Fernee et al., 2017). Programs were similar in content to those of recreational immersive nature-experience but were targeted and adapted to a range of unhealthy, disadvantaged, or at-risk populations. Intense and demanding expeditions in wild or urban nature or short-and-longer termed primitive camp-based experiences were a predominant type of activity within the sector. Please see Table 2 for a full summary of quantitative, controlled analyses from the social and health sectors.
A vast range of outcomes related to psychological wellbeing were investigated in the health and social sector. Some measures represented clinical assessments, i.e., symptoms of psychopathology; schizophrenia; depression; anxiety; and post-traumatic stress disorder (PTSD). Others related to more generalized or non-clinical assessments of positive and negative affect; stress; mood states; depressive states; fatigue; level of burnout; anxiety; thoughts of suicide; negative memories and feelings toward self; quality of life; general wellbeing; and internalizing and externalizing behaviors. Most findings were positive (n = 26). One study indicated that fatigue was improved more during the comparison condition, which included a mindfulness course (Johansson et al., 2015). Two studies in the sector reported mixed and 16 non-significant findings. The quality of the evidence was considered low to moderate and is discussed further in the following.
Sustained expedition or base camp adventure experiences in natural environments were commonly used in a variety of social and health care contexts and applied amongst diverse target groups. In a comprehensive meta-analysis based primarily on observational studies, Bowen and Neill (2013) reported that outdoor behavioral health care was associated with moderate effect sizes for psychological state and level of mental functioning, an aggregate measure of parameters such as anxiety and locus of control (g = 0.5). However, associations were absent at follow-up. Participants were most commonly male, between age 10 and 17, resided in USA, identified as at-risk and Caucasian (Bowen and Neill, 2013). Populations were characterized as abuse victims; adjudicated youth; behaviorally disordered; disabled; educationally disengaged; emotionally disturbed; having mental health issues; having physical issues (exemplified by brain injury or weight-loss); and substance abusers. The authors observed a substantial level of heterogeneity in the outcome estimates across the individual original studies and found that study, program and, participant characteristics partially explained the variance. Age was highlighted as a singular predictor that influenced the achieved associations: older participants, who more often volunteered to participate than younger participants, achieved larger improvements. Therefore, despite the vastness of the research, the generalizability of the results is questionable. Since subsequent controlled studies have supported the positive findings (e.g., Gelkopf et al., 2013; Scheinfeld et al., 2016), we considered the quality of the evidence for positive associations and effects on psychological wellbeing of adventure experiences in nature low to moderate amongst adolescent and adult populations.
Short-termed seated relaxation and walking in natural environments was found to improve various indicators of self-reported wellbeing. Patients diagnosed with mild to moderate depression reported improved mood indicators and affective valences upon a 60 min walk compared to indoor biking and resting (Frühauf et al., 2016). However, affective valences did not differ significantly from the indoor active control group. Patients with major depressive disorder reported higher levels of positive affect, but similar levels of negative affect, after a 50–55 min of walking in natural environments compared to urban environments (Berman et al., 2012). Likewise, women diagnosed with exhaustion disorder reported improved mood indicators upon three 1.5 h long sessions of seated relaxation in a forest compared to an urban environment (Sonntag-Öström et al., 2015). Mood indicators were likewise higher after 90 min of seated relaxation in three different natural environments compared to a parking lot in an urban area amongst patients with stress-related burnout syndrome (Sonntag-Öström et al., 2014). Amongst two different groups of individuals with and without mental diagnoses, 1 h of guided walking in a natural environment compared to urban environments resulted in higher ratings of mood, with the largest effect sizes observed amongst individuals with mental diagnoses (Roe and Aspinall, 2011a). Similar effects were found for mood indicators amongst hypertensive males after 17 min of walking in a natural environment (Song et al., 2015), compared to urban environments. Thirty minutes of seated relaxation in a forest was found to reduce perceived stress amongst individuals with stress or exhaustion disorders, although no more than the indoor control condition which involved watching a slideshow of the same forest environment (Kjellgren and Buhrkall, 2010). The quality of the evidence was considered moderate being based both randomized and non-randomized controlled designs and small study samples.
Interventions of longer duration with repeated exposures were also investigated. Participants with various mental diagnoses displayed improved mood indicators following a 6-week walking program in natural urban and rural environments, but changes were no larger than two control groups who underwent alternative treatments (social activities and swimming) (Barton et al., 2012). For individuals diagnosed with hypertension, two daily sessions with seated relaxation and walking in forests over a week improved mood indicators more than the same activities in an urban environment did (Mao et al., 2012a).
Patients characterized as high-risk suicidal reported lower levels of depression and hopelessness after a 9 week program with triweekly hikes compared to a waitlist control group (Sturm et al., 2012). Individuals with mental fatigue following acquired brain injury did not report improved anxiety or depression after 8 weeks of weekly 1.5 h walks in a park compared to participants taking part in face-to-face or online mindfulness courses (Johansson et al., 2015).
Two days of forest therapy in conjunction with cognitive behavior therapy provided small effects on self-reported depression and perceived pain amongst individuals with widespread chronic pain (Han et al., 2016). A similar 4-week forest therapy program provided larger reductions in depressive symptoms than a no treatment control and alternative treatment hospital-based control group for patients with major depressive disorder (Kim et al., 2009). Depression and anxiety decreased amongst patients with chronic stroke who partook in a 4 day forest bathing intervention, while no such changes could be observed in the control group who performed similar activities in an urban environment (Chun et al., 2017). Likewise, alcoholics' depression ratings decreased after a 9 day forest therapy camp with no changes occurring in the control group (Shin et al., 2012). The reviewed wellbeing indicators were multifarious, and the included studies covered a range of populations. As such, across various wellbeing measures, immersive nature-experience seemed to be beneficial, but the finer distinctions remained uncertain. The quality of the evidence was considered low to moderate.
There was a vast amount of research indicating that outdoor behavioral health care improved psychosocial parameters (Cason and Gillis, 1994; Hattie et al., 1997; Wilson and Lipsey, 2000; Bedard, 2004; Bowen and Neill, 2013; Bettmann et al., 2016)3. The identified psychosocial outcomes represented interrelated yet different phenomena, such as identity formation; confidence; autonomy; locus of control; empowerment; resilience; daily functioning; and self-compassion, -efficacy, -esteem, -concept, -perception, -pity, and -control. Overall, outcomes were often improved (n = 14), but many were non-significant (n = 11) or mixed (n = 2). Due to the predominant use of pre-post designs with no randomization and the dispersion of outcomes, the quality of evidence for these outcomes was considered low.
Bowen and Neill (2013) reported that outdoor behavioral health care was associated with moderate increase in self-concept, which was an aggregate measure of, amongst other parameters, self-efficacy and self-control (g = 0.3). Bedard (2004) compared changes in self-esteem and self-concept in delinquent youth, who participated in outdoor behavioral health care with delinquent youth who engaged in standard processes of probation or rehabilitation. Outdoor behavioral health care was considerably more favorable.
As was observed amongst healthy populations (see section Psychophysiological stress-indicators), short-termed walking or seated relaxation in natural environments was found to reduce psychophysiological stress-indicators, i.e., heart rate variability and cortisol. Amongst the included studies, measures were exclusively found to be improved (n = 5). The studies in the social and health sector investigating psychophysiological stress-indicators were mainly designed as controlled before-and-after studies with small samples. Only one study was a cross-over trial. We considered the quality of evidence low to moderate. However, if findings from healthy populations may be translated to the populations included in this section, the evidence could be considered moderate. Examples of interventions and outcomes are provided in the following.
In a randomized cross-over trial, walking for 17 min increased heart rate variability more than the same activities in control conditions for middle-aged males with pre-hypertensive or stage 1 hypertension (Song et al., 2015). Longer-term forest therapy likewise enhanced psychophysiological stress indicators amongst individuals with hypertension (Sung et al., 2012), major depressive disorder (Kim et al., 2009), and chronic pain (Han et al., 2016).
Identified outcomes representing cognitive indicators included cognitive performance; attention capacity; short term memory; and goal setting. These were predominantly improved (n = 5), but some were mixed (n = 1) or non-significant (n = 1). Interventions included short-termed walks and seated relaxation, and sustained expeditions and adventure programs. Quality of evidence is discussed in relation to these types of interventions below.
In the meta-analysis described in section Psychological wellbeing, Bowen and Neill (2013) reported that participation in sustained expeditions and adventure programs was associated with moderate improvements in school achievement, e.g., academic performance in English, Math, and Reading (g = 0.41). Associations were absent at follow-up. The research was based on studies about outdoor behavioral health care and behaviorally unadjusted adolescents in schools. Therefore, these findings are also relevant to the education sector (section Psychological and psychophysiological wellbeing indicators). The cognitive parameters were scattered and based on mainly observational studies. Given that the studies were based on a wealth of types of designs, many of which utilized poor or no control groups, the quality of the evidence was deemed low.
As was observed amongst healthy populations (see section Cognitive indicators), walking or sitting in nature provided larger acute enhancements in cognitive indicators than the same activity in control conditions: patients diagnosed with major depressive disorder displayed an enhanced short term memory upon walking in a park relatively to an urban environment (Berman et al., 2012). Likewise, women diagnosed with exhaustion disorder (Sonntag-Öström et al., 2015) had improved attention capacity upon three 1.5 h long sessions of seated relaxation in a forest compared to an urban environment. Patients diagnosed with mild to moderate depression participated in an 11 week program consisting of relaxation exercises, seated relaxation in solitude, and walking in a forest environment (Frühauf et al., 2016). Here, it was found that attention capacity was increased after single forest visits, but there was no effect found for the rehabilitation period as a whole when comparing measures to a waitlist control group (Frühauf et al., 2016). Amongst children diagnosed with ADHD (Taylor and Kuo, 2009), acute increases in cognitive performance after a 20 min walk in a natural environment compared to an urban environment. These studies were designed as randomized cross-over trials and one as a randomized controlled trial (RCT), thereby providing a moderate quality of evidence.
Physical health in the social and health sector was investigated using diverse indicators of bodily function, i.e., pulmonary function; progress in walking rehabilitation; muscle strength; sick leave; perceived pain; and body composition measures, i.e., body-mass index (BMI) and waist circumference. Cardiovascular indicators, i.e., blood pressure and biomarkers of cardiovascular disease risk, and immune function indicators, i.e., oxidative stress, pro-inflammatory cytokines, and leukocyte subsets, were also used. Lastly, various indicators relating to PA were applied (n = 5). Most of the studies found that individual outcomes were improved (n = 14), but quite a few reported mixed (n = 4) and non-significant (n = 10) findings. Given that the evidence was predominantly based on observational or controlled pre-post studies without allocation randomization, the quality of the evidence was deemed low.
In the abovementioned meta-analysis, Bowen and Neill (2013) concluded that outdoor behavioral health care was associated with a small effect size related to the participants' bodily function and physical health, exemplified by changes in weight and so-called somatic health (g = 0.32). However, associations had decreased at follow-up (g = 0.23). A substantial level of heterogeneity in the outcome estimates across the original studies was observed. Hence, the understanding of the mechanisms that cause the observed changes were limited and generalization should be practiced with caution. While the meta-analysis (Bowen and Neill, 2013) primarily was based on observational studies, subsequent experimental, controlled studies have supported the conclusions: outdoor behavioral health care interventions contributed to an enhancement of PA and reductions of the participants' BMI (although no larger than an alternative PA intervention), but improvements were absent at follow-up (Jelalian et al., 2010, 2011). Caution should be taken in interpreting these results since changes in weight and BMI provide inaccurate measures of unhealthy body fat and general bodily health.
Most studies in the social and health sector indicated positive social health outcomes (n = 15), although some reported non-significant findings (n = 6). The outcomes were spread over a number of measures, for example relating to the participants' social environment, i.e., family function; social support; alienation; and sense of belonging. Social behavior outcomes included antisocial behaviors; social avoidance; and ability to maintain socio-professional status. Lastly, social skills and relationships included outcomes social cognition and functioning; amount of conflict; and interpersonal relationships and problems. Given that the studies utilized a vast number of outcomes and were based on non-randomized designs, the evidence was deemed low to moderate.
In addition to, and partly overlapping with, the results from the above mentioned original studies, Bowen and Neill (2013) concluded that outdoor behavioral health care interventions associated with the participants' social development (g = 0.42), e.g., alienation and social skills, and family development (g = 0.36), e.g., parent-child relationship and family functioning. Associations were absent by follow-up. Across five original studies, Bedard (2004) found that interpersonal competencies and behavioral change in delinquent youth was positively influenced by participation in outdoor behavioral health care, and that this form of treatment was preferable to standard processes of probation or rehabilitation. Most of the studies on which the reviews were based used non-controlled designs and the quality of evidence was considered low to moderate.
The effects of nature-based sustained expedition or base camp adventure experiences on risky health behaviors were also investigated. Bowen and Neill (2013) collapsed substance use with other parameters, such as recidivism and home behavior, into one behavior-oriented outcome category, and found that the observed associations (g = 0.41) remained at follow-up, although reduced (g = 0.21). Due to the predominant use of non-controlled designs, the evidence was considered low quality.
The final sector, immersive nature-experience used in educational context, encompassed 172 individual studies ≈72% included mental (n = 124), ≈16% physical (n = 27), and ≈58% social health (n = 100) outcomes. Three reviews addressed various forms of nature-experience in the education sector and presented the literature in a manner allowing for extraction of results from the studies relating to immersive nature-experience (Furie, 2011; Daniel et al., 2014; Cooley et al., 2015). Adventure education was the main type of activity. Other types of activities included green breaks from teaching and various types of educational activities taking place in natural environments. Please see Table 3 for a full summary of quantitative, controlled analyses from the education and daycare sectors.
The dominant type of mental health category in the education sector was psychosocial indicators. Positive findings (n = 24) outweighed mixed (n = 4) and non-significant (n = 6) findings. Frequent outcomes were self-efficacy; self-esteem; and resilience. Other outcomes that were used on a more sporadic basis included self-concept; life effectiveness; sense of identity; autonomy; self-regulation; and the development of a so-called Growth Mindset which is a form of openminded or adaptive thinking. Given that the research was based mainly on small samples and controlled designs with no group allocation randomization, the evidence for the outcomes was considered low quality.
The main type of intervention was sustained adventure-based experiences in natural environments. Adventure education programs ranging from four to ~90 days of varying intensity were found to increase psychosocial indicators such as self-esteem (Romi and Kohan, 2004; Mann, 2007; Kafka et al., 2012; Hunter et al., 2013; Hayhurst et al., 2015), self-efficacy (Hunter et al., 2010; Connelly, 2012; Fuller et al., 2017), self-concept (White, 2012), and resilience (Hayhurst et al., 2015) more than comparison conditions. A few studies in the education sector reported mixed effects on the psychosocial outcomes. For example, Gehris (2007) found that 44 days of adventure education improved the 10th grade pupils' self-esteem more than the control group that had undergone a health education programme, but not more than the control group that participated in a PA program. No effect on self-concept could be observed following the same program in comparison to either control group (Gehris, 2007).
Effects of extra- and co-curricular and curriculum-integrated immersive nature-experience on problem solving; goal setting; attention capacity; and academic performance were investigated. Overall, positive effects of the interventions (n = 7) were almost matched by the number of non-significant findings (n = 6), with one study displaying mixed effects. Since the studies used small samples and did not randomize allocation to groups, the evidence was considered low quality.
Extra- and co-curricular immersive nature-experience for adolescents and young adults provided some positive and non-significant findings. For examples, adventure education as a co-curricular activity for adolescents with truant behavior was found to improve goal setting but not problem solving (Ang et al., 2014) and weekly sessions of outdoor residential experiences improved academically underachieving adolescents' academic performance (Fuller et al., 2017).
Whereas extra- and co-curricular adventure education was usually oriented toward shorter or longer durations of time removed from everyday life, included studies also addressed the potentials of outdoor activities in nature that were inscribed in educational practices. Studies, for example, investigated whether a break from lectures in the form of a 1 h walk in natural environments would increase the capacity to direct attention of undergraduate nursing students (Lethbridge et al., 2005) and diploma-prepared nursing students enrolled in a baccalaureate nursing program (Sanders et al., 2005). Results were inconclusive: in both studies, comparison groups, who did not participate in any form of restorative experience, also increased directed attention scores. In consequence, it seems the results indicated a learning effect rather than an effect of walking in a natural environment. This, however, did not imply inefficacy of natural environments to induce attention restoration, but rather a method weakness related to repeated use of measurement instruments that were not developed for such use. Amongst children, it was found that a 5-day science teaching program in a forest lead to improvements in motivation and attention capacity, as well as academic performance, amongst elementary school children in comparison to similar children who went to school as usual (American Institutes for Research, 2005). Research on EOtC in natural environments, a more long-termed, curriculum-integrated approach than the 5 day science teaching program, resulted in similar findings indicated by an observational study (Mygind, 2005).
The number of outcomes categorized under psychological wellbeing (positive effects: n = 5, negative effect: n = 1) and psychophysiological stress-indicators (positive effect: n = 1) was limited and we therefore present them together. Included outcomes were mood states; quality of life; mental wellbeing; purpose in life; self-reported stress; and the psychophysiological indicator of stress response, cortisol. Being based on mainly non-randomized study designs and small sample sizes, the evidence was considered low quality.
Interventions ranged from breaks from studying in natural environments (Lethbridge et al., 2005) and curriculum-integrated forest school (Roe and Aspinall, 2011b) to co-curricular hiking trips (Mutz and Müller, 2016). For example, nursing students reported increased mood states and quality of life (Lethbridge et al., 2005). Likewise, children who participated in 5 h of forest school reported improved mood (Roe and Aspinall, 2011b). Cortisol levels, indicative of stress response, were decreased when elementary school students partook in EOtC over 1 year in comparison to typical classroom-based education (Dettweiler et al., 2017).
Interestingly, a 10-day wilderness orientation experience was associated with a decrease in first-year university students' sense of purpose in life (Bailey and Kang, 2015). The authors argued that occurrences unrelated to the program caused the decline in sense of life purpose (Bailey and Kang, 2015). This is probable since outcomes were measured before and after the first semester at university (and not the program), a time of substantial stimuli and rapid development. Furthermore, the study was based on a nonequivalent controlled pre-post design in which participants self-selected into intervention and control groups. As such, the design would be susceptible to influence from these exogenous factors.
We found a limited number of studies about physical health promotion outcomes within the education sector. We identified only two which were based on controlled designs. In these motor skills and physical fitness was assessed. We therefore discuss the observational literature within the sector related to physical health. Considering the scarcity of controlled studies and the use of small samples, the quality of the evidence for these outcomes was considered low.
There were indications that outdoor activities in nature that were integrated in pedagogical practice can enhance preschool-aged children's PA and motor skills. Motor skills are believed to be an important predictor of later life PA (Larsen et al., 2015; Lima et al., 2017a,b). In a preschool context, children's motor skills improved more when participating in daycare taking place in a forest environment compared to children who went to a traditional kindergarten (Fjørtoft, 2004). The observation was supported by an observational study (Vigsø and Nielsen, 2006).
Indicators of PA were mainly used as an acute and highly context-dependent indicator of bodily movement during immersive nature experience. As such, perhaps unsurprisingly, no studies compared PA before and after interventions. Research on EOtC in natural environments, a form of recurring nature-integrated teaching that stems from Scandinavia (Bentsen et al., 2009b; Jordet, 2010), was consistently found to encourage higher levels of moderate to vigorous PA (MVPA) than traditional, classroom-based teaching (Grønningsæter et al., 2007; Mygind, 2007, 2016; Dettweiler et al., 2017). For example, children were estimated to spend 11.5 min longer in MVPA per 2 h unit, averaged over three seasons (Dettweiler et al., 2017).
Social health promotion outcomes within the education sector were most often oriented toward social skills and relationships, i.e., cooperation skills; social competence; amount of conflict and conflict resolution skills; peer relations; interpersonal relations; and knowledge about bullying. Other outcomes included perceived social support; bullying; and school attendance. Mostly, interventions had significant positive effects on outcomes (n = 12). Some cases were mixed (n = 3) or non-significant (n = 4). The quality of the evidence was considered low and is discussed further in relation to the main types of interventions in the following.
A review and three subsequently published original studies reported that various aspects of cooperation skills, such as trust in the group, responsibility, leadership and mutual aid, were improved after both short and long term outdoor education interventions (Frauman and Waryold, 2009; Ewert and Overholt, 2010; Harun and Salamuddin, 2010; White, 2012; Cooley et al., 2015). The review (Cooley et al., 2015) included four controlled studies, two of which were published within the time frame reviewed in the present systematic review (Harun and Salamuddin, 2010; Vlamis et al., 2011), as well as qualitative and observational studies which are not discussed here. The studies included children, adolescents, and adults. While the studies reported promising developments in cooperation skills pre to post programs, the transferability of the skills to everyday life remained uncertain. These types of outdoor education interventions were also found to associate with reduced gender-based prejudice (Kafka et al., 2012) and an increase in knowledge about bullying amongst adolescents, although no direct effect on bullying was observed (Furie, 2011). Effects of adventure-based pre-orientation courses for first-year university students on social competencies (Frauman and Waryold, 2009), social support (Bailey and Kang, 2015), and interpersonal relations (Vlamis et al., 2011) were mixed. The quality of the evidence for effects relating to cooperation skills, gender-based prejudice, bullying, knowledge about bullying, social competences, social support, and interpersonal relations was considered low.
Research on immersive nature-experience integrated into pedagogical and didactical practice provided mixed results. Elementary school students, who took part in a 5-day outdoor science school intervention, rated their conflict resolution and cooperative skills higher than waitlist controls (American Institutes for Research, 2005). Likewise, teachers estimated that the intervention group improved their conflict resolution skills, peer relations, and behavior in class more than the waitlist controls. Over the course of a 6-month outdoor class intervention, McKenzie (2015) could not observe any differences in teacher-reported changes in the quality of peer relations (i.e., friction and cohesion between students) between the intervention and control group. Furthermore, McKenzie (2015) did not report differences between competition orientation and the amount of problems in the class. The intervention and control groups were not completely comparable: students were recruited from different schools and differed in terms of ratio of ethnic minorities and socio-economy with more poor and ethnic minority backgrounds in the intervention group. In supplementary observational studies, it was indicated that participation in EOtC was associated with making more friends and higher levels of social wellbeing (Mygind, 2005, 2009). The used study designs in conjunction with small sample sizes provided the background for considering the quality of the evidence low.
The aims of this systematic review were to investigate (1) what types of immersive nature-experience, (2) which health promotion outcomes had been investigated, and (3) how immersive nature-experience influenced or associated with mental, physical, and social health outcomes. Here, we briefly summarize the key findings relating to (1) prominent types of immersive nature-experience and (2) the most commonly investigated outcomes and associated findings. To provide an overview across the three sectors used above, we also (3) discuss the two main types of immersive nature-experience, short-termed walks, and seated relaxation and adventure-based activities, and associated findings. Since these activities were more often found in the recreational or social and health sectors, we also briefly discuss findings from the educational sector. Lastly, we elaborate on the development of the body of research before discussing strengths and limitations of the present work.
Within the recreational sector, the most common type of activity included short-termed walks or seated relaxation, frequently termed shinrin-yuko or forest bathing. In the social and health sector, interventions were similar in content to those of recreational immersive nature-experience, but targeted and adapted to a range of unhealthy, disadvantaged, or at-risk populations. The main type of intervention was sustained expeditions and adventure programs in which participants were challenged mentally and physically through activities in natural environments. In the educational sector, adventure education was predominant, but other types of activities included green breaks from teaching and various types of educational activities taking place in natural environments, e.g., forest school or EOtC.
Use of immersive nature-experience was most frequently positively, or positively and non-significantly, associated with mental, social, and physical health outcomes. We found conditional support for positive effects on a range of health promotion outcomes grouped under psychological wellbeing (n = 97; ≈55% positive; ≈13% mixed; ≈29% non-significant; 2% negative); psychosocial function (n = 67; ≈61% positive; ≈9% mixed; ≈30% non-significant); psychophysiological stress response (n = 50; ≈58% positive; ≈18% mixed; ≈24% non-significant), and cognitive performance (n = 36; ≈58% positive; ≈6% mixed; ≈33% non-significant; 3% negative); and social skills and relationships (n = 34; ≈70% positive; ≈7% mixed; ≈22% non-significant). Findings related to outcomes categorized under physical health, e.g., risk of cardiovascular disease, were less consistent (n = 51; ≈37% positive; ≈28% mixed; ≈35% non-significant). Only three studies indicated a negative impact of immersive nature-experience on cognitive performance (Johansson et al., 2011), life purpose (Bailey and Kang, 2015), and fatigue (Johansson et al., 2015). Across the sectors, mental health outcomes were the dominant type of outcome. Since these were often psychosocial in character, e.g., self-esteem or self-concept, many mental health outcomes could also be categorized as social health outcomes.
Across the recreational and social and health sectors, walking, and seated relaxation in natural environments was most frequently found to enhance aspects of wellbeing; reduce stress; and enhance cognitive performance. However, wellbeing measures were diverse and aspects of wellbeing, e.g., individual scales relating to depressive or anxious moods, were not consistently improved. Likewise, the connection between exposure to natural environments while walking or during seated relaxation and acute reductions in psychophysiological indicators of stress was somewhat obscured by a relatively high proportion of mixed or insignificant findings. Much of the research focused on adults, especially university students.
It may seem surprising that the amount of research identified within the field of attention restoration was not larger. In a recent meta-analysis, Ohly et al. (2016) concluded that across 31 studies, some cognitive measures (i.e., Digit Span Forward, Digit Span Backward, and Trial Making Test B) were improved upon exposure to visual representations of natural environments, exposures to natural environments, and views to natural environments. As such, many of these studies were not eligible for inclusion in the present review of immersive nature-experience. However, the findings may supplement the studies identified in the present review.
Intense and demanding expeditions in wild or urban nature or primitive camp-based experiences targeted toward behavioral change, or personal or social development, appeared to have immediate effects on psychosocial indicators; the ability to engage in social contexts; cooperation skills; family development; behavior (e.g., substance abuse and crime); and physical health (e.g., changes in body weight) across a range of populations. There were indications that behavioral changes endured at follow-up. The activities were mainly inscribed in the educational or social and health sectors. The activities, pedagogies, and places of the programs under investigation were generally poorly described which hinders transfer and reproducibility of the study results. The evidence for the effects of outdoor behavioral health care and outdoor education amongst children is limited, perhaps because the practice is more common amongst adolescents and young adults. For example, the abovementioned meta-analysis (Bowen and Neill, 2013) included only four studies addressing (unspecified) impacts of outdoor education and outdoor behavioral health care amongst children under the age of 9 years.
Use of immersive nature-experience in educational contexts, e.g., schools or kindergartens, was positively associated with mental, social, and physical health outcomes. The research was mainly based on correlational studies that were spread over a range of outcomes and contexts, and we therefore considered the quality of the evidence low. Recent large-scale EOtC studies have supplied that 3 h of weekly EOtC increased boys' MVPA (Schneller et al., 2017a) and girls light PA (Schneller et al., 2017b) considerably over a full 7-day week when compared to students in a traditional classroom setting. Furthermore, the children who participated in EOtC over the course of 1 year maintained a higher level of motivation for school (Bølling et al., 2018). The studies were based on types of EOtC that did not exclusively occur in natural environments, but also other informal learning settings. Subsequent analyses will investigate whether the environments had differential impacts (Nielsen, 2016).
In agreement with previous reviews about immersive nature-experience, or friluftsliv, we found that the body of research was characterized by a considerable volume and interdisciplinary breadth (Sandell, 2004; Schantz and Silvander, 2004). The main focus of previous reviews was on Scandinavian literature, but attempts were made in previous reviews to also include research published in English language (Sandell, 2004; Schantz and Silvander, 2004). While contributions from outside of Scandinavia predominantly derived from USA at the time of the previous reviews, we unearthed a considerable body of literature from Asian countries relating to the phenomenon of forest bathing or, in Japanese, shinrin-yuko.
In previous reviews, the authors reflected upon a development from a culture of practicing immersive nature-experience for the sake of the experience itself toward a more commodified, outcome-driven culture (Sandell, 2004; Schantz and Silvander, 2004). In response to discussions concerning whether this development was within the spirit of immersive nature-experience, Sandell (2004) argued that the continuous growth of immersive nature-experience into other sectors of everyday life should be encouraged and investigated. In the present review, we focused exclusively on health promotion outcomes related to immersive nature-experience within discrete sectors, and the work may thus be considered a continuation and concretization of the outcome-driven focus. While the intermediate health promotion outcomes of immersive nature-experience were discussed in the previous reviews within the context of public health potentials, the main sectors in which immersive nature-experience was practiced were recreational or educational. Perhaps as a consequence of the observed expansion of research and practice of immersive nature-experience, our review differs by including and discussing immersive nature-experience used as an explicit treatment modality, in particular relating to mental and emotional disorders. The present review thus builds on, adds to, and nuances existing insights, rather than presenting a radical paradigm shift in our understanding of the health promotion outcomes of immersive nature-experience.
Direct comparison between health promotion outcomes of immersive nature-experience and non-immersive experience is difficult to make due to the use of varying definitions, categorization, and descriptions of nature contact in the literature (Hartig et al., 2014) as well as pooling of different types of nature-experience in individual reviews (e.g., Twohig-Bennett and Jones, 2018). However, there is empirical evidence to support that the character of the nature contact influences achieved effects. In a recently published meta-analysis (Stevenson et al., 2018), for example, cognitive indicators, e.g., working memory, cognitive flexibility, and attentional control, were found to be significantly higher following direct experience of natural environments compared to indirect exposures, e.g., viewing photos or videos of natural environments. Since our review focused exclusively on direct, immersive contact with natural environments, our results do not allow inferences about this type of nature contact compared with others, e.g., incidental, accumulated exposure due to transport through or views to neighborhood greenery. However, our results suggest that across all outcomes positive effects of immersive nature-experiences occur most consistently for social health [percentage positive (%p) = 68.3%, percentage positive and mixed (%p + m) = 75.6%) compared to mental (%p = 57.6%, %p + m = 70.4%) and physical health (%p = 43.9%, %p + m = 70.2). This suggests that immersive nature-experience might be well-suited for promoting, in particular, social behaviors, skills, and relationships, as well as psychosocial parameters. Since the outcome-level quality assessments were predominantly low, there is some uncertainty regarding the findings. Consequently, subsequent high-quality findings could change the impression made and the knowledge is premature as a background for recommendations for practice.
Although the research connected to physical health was inconsistent, this does not necessarily imply inefficacy. Firstly, the results should be interpreted with attention to the condition that some interventions were compared to active control groups (e.g., Jelalian et al., 2010) and others to waitlist or “treatment as usual” control groups (e.g., Fjørtoft, 2004). Results are influenced by this due to the comparative nature of the research. Secondly, studies in the physical health domain often used many distinct physiological markers to characterize the same phenomenon or closely related phenomena, for example, immune function. If one or more the individual markers were not significantly improved, we categorized the effect as mixed. This might have differentially influenced the physical health domain since many studies in the domain used several markers for the same phenomenon. Mixed findings indicate that positive effects were observed, but interpretation requires caution: Using many markers to address one outcome might be effective for identifying significant effects. In one study (Mao et al., 2012b), for example, six leukocyte subsets were investigated, alongside a number of other physiological indicators. However, in conjunction with small sample sizes, the vast number of variables introduces the risk of finding a significant effect by chance, i.e., type I mistakes. Thirdly, the intermediate health promotion indicator frequently and consistently associated with natural environments, PA (Konijnendijk et al., 2013), was mostly used in observational studies. Furthermore, there is a considerable field of epidemiological research connecting accessibility to green space with PA which was outside the scope of this review. It is well-documented that increased PA and decreased sedentary time reduces obesity, risk of NCDs, such as cardiovascular disease and diabetes, and morbidity (Lee et al., 2012; Ekelund et al., 2016), irrespective of the place where PA takes place. Recently, a connection between PA and cancer has also been established (Monninkhof et al., 2007; Wolin et al., 2009; Speck et al., 2010) and there is sound evidence that PA, in natural outdoor environments or elsewhere, has a direct effect on cognitive function and mental health (Biddle and Asare, 2011). There are indications that PA in natural environments has additional benefits to mental health compared to PA indoors or in urban settings (Bowler et al., 2010), as the present review also suggests. As such, immersive nature-experiences may also contribute to overall PA levels.
In the following, we discuss strengths and limitations in the reviewed literature. On this basis, we formulate methodological focus points from which the research field may grow further. Although we focused exclusively on immersive nature-experience and distinguished between types of designs; sectors (e.g., recreation, education, or treatment); and health outcomes, the research was spread across diverse intervention characteristics (e.g., activity, pedagogical and instructional approach, duration or type of natural environment); target groups (e.g., adults and children); and control conditions (e.g., no treatment, short nature exposure, and alternative treatment). As such, we did not consider the research suited for meta-analyses, which, we argue, requires more streamlining to avoid simplified conclusions and recommendations. Elsewhere, the inappropriateness of compiling research conducted with adults and children, for example, with the aim to generalize findings without regard to the target group has been addressed (Tillmann et al., 2018). The aim of this review was to accumulate and evaluate the research relating to specific types of nature-based activity. Therefore, we chose to include both child and adult populations and only distinguish between target groups narratively. Subsequent in-depth analyses of the research pertaining to children will follow.
We did not conduct systematic appraisal of risk of bias in the individual studies. Although we assessed studies according to design and apparent methodological issues, potential sources of bias may have been overlooked. For subsets of the review (psychophysiological outcomes and the literature addressing health promotion outcomes for children and adolescents), we have subsequently performed systematic risk of bias and quality appraisals. The systematic assessments made correspond well with the overall narrative assessments made in this review. Furthermore, we included both randomized and non-randomized controlled studies. The latter type of design is by some considered an inappropriate source for inferences relating to effects (Ryan et al., 2013; Gottfredson et al., 2015). We acknowledge the criticisms that can be raised toward this type of design but chose to include this research due to the scarcity of randomized studies. Since the type of design is so widespread in the reviewed literature, results should be interpreted with care and function only as conditional evidence of effects: Findings may be subject to bias and future rigorous studies might provide other results.
Across the types of interventions and outcomes, the quality of the evidence was deemed low; low to moderate; and occasionally moderate. In many studies, sample sizes were small and possibly underpowered which introduces a risk of small-study effects, i.e., inflated effect sizes and false positives as well as negatives (Schwarzer et al., 2015). Most of the studies identified through the literature searches were qualitative (23.3%, n = 114), observational, quantitative (34.6%, n = 169), or a mix of qualitative and observational, quantitative (10.2%, n = 50). However, in comparison to previous reviews that focused exclusively on immersive nature-experience (Sandell, 2004; Schantz and Silvander, 2004), a growth in quantitative, controlled studies may be discernible. However, since the exact numbers of quantitative, controlled studies were not clear in previous reviews, the comparison is speculative. While previous reviews did not apply systematic quality appraisal methods, the quality of the research was considered low (Sandell, 2004; Schantz and Silvander, 2004). In comparison, the quality of the research included in the present review was most often low or low to moderate, and occasionally moderate at an outcome level. As such, it is possible that a development in the quality has occurred. Still, the knowledge base remains only a conditional basis for effect inference and premature as a basis on which to formulate recommendations for practice. It should be emphasized that the intention behind the interventions was not necessarily health promotion, nor for all original studies to provide gold-standard evidence for health promotion effects of the interventions. However, following the broad and holistic conceptualization of health promotion applied in the present review, we deemed the outcomes relevant for health promotion. We appreciate that some of the outcomes could also have been conceptualized in terms of wellbeing or functioning, which in some cases may have been more in line with the original intentions.
Immersive nature-experience as a subject presents certain core challenges for the conduct of research of the type that is, from a medical, gold-standard point of view, of high quality: (1) immersive nature-experience involves complex interactions between individual subjective experience, activities, pedagogies, and places that are difficult to operationalize and measure in quantitative terms, (2) immersive nature-experiences are often inscribed in real-life contexts in which it is not feasible or desirable to randomize participant allocation, (3) blinding of participants and personnel from group allocation and condition is often not possible, (4) given the complexity of the research subject, transferability between studies and generalizability is challenging. A number of methodological focus points and tools could be used to enhance the quality and transferability of the studies.
The first challenge requires a substantial effort put into formulating a program theory, i.e., identification of intervention input; activities; outputs; intermediate outcomes; and long-term outcomes, and theory of change, i.e., a description of how and why the desired change is expected, pertaining to the specific type of immersive nature-experience and health outcome (Gottfredson et al., 2015). Kuo (2015) and Hartig et al. (2014) reviewed the existing research about nature exposure, in a broad sense, and various health outcomes, and formulated distinct pathways through which exposure to nature could influence health outcomes. The formulated pathways provide handy starting points for formulating theories of change for future studies, but should, at the minimum, be adapted to the specific target group; type of immersive nature-experience; and health outcome. Correspondingly, Hartig et al. (2014) highlighted a need for theory to guide research on which types of nature, and which qualities of those types of nature, are relatively effective for particular outcomes. Based on a review of empirical findings, Kuo (2015) suggested that some pathways are more central or effective than others, and shared Supplementary Materials from which additional pathways may be formulated. Here, we would add that the way the natural environments are “activated” and used, and the social or pedagogical processes that it affords, and not only the types and characteristics of the nature, should be considered in theories of change. The first challenge also necessitates the use of process evaluation to describe and, when possible, quantify the actual implementation of the intervention or mechanisms of action. Recent methodological innovations involved monitoring exposure to EOtC by intervention and comparison teachers (Bølling et al., 2018) and highly increased the understanding of the intervention and findings. The monitoring tool did not concern pedagogical practice or qualities of the environments. Future tools could attempt to also address these aspects.
In the reviewed studies, group allocation was often performed by convenience: participants were often recruited amongst individuals who had self-selected into the programs or who had been directed to the program by, for example, their therapist, teacher, or social worker. Furthermore, sociodemographic group comparability, e.g., age, gender, ethnicity, socioeconomic status (SES), or other relevant background variables of intervention and control groups, was seldom thoroughly described and analyzed. In contrast, the randomized controlled trial is commonly considered the gold-standard that provides the highest quality evidence (Gottfredson et al., 2015). While well-conducted randomization is often possible and provides studies with strong internal validity, it may not always be feasible, ethical, or acceptable, for example, when the subjects are very vulnerable or nested in schools or communities (Gottfredson et al., 2015; Frieden, 2017). Alternatively, regression discontinuity designs and comparison time series designs may provide unbiased estimates of intervention effects, where randomization is not practical or possible (Gottfredson et al., 2015). Other types of quasi-experimental designs that maximize feasibility and acceptability for use in prevention research, which in turn increases ecological validity, includes dynamic wait-listed designs, stepped wedge, or regression point displacement designs (Fok et al., 2015; Wyman et al., 2015). We did not identify any such designs amongst the included studies. Furthermore, the usefulness of experimental research may be increased if supported and supplemented by large, high quality cohort studies (Frieden, 2017). This would also contribute to understandings of nature impacts in a life-course perspective (Hartig et al., 2014). We argue, that an increased detail of reporting about, and general attention to, group allocation generation (preferably randomized, when feasible and ethical) and intervention and control group comparability (including, as a minimum, sociodemographic information such as age, gender, ethnicity, and SES) would significantly improve the quality of evidence.
In clinical research, blinding of participants and personnel from treatment is a fundamental tool to avoid performance bias. Elsewhere, the issues relating to blinding in the context of interventions in which environments and visual representations are a core component have been discussed (Brussoni et al., 2015; Ohly et al., 2016). Although full blinding is not possible, researchers could consider blinding participants and personnel from research aims and questions. In general, studies did not address the extent to which participants or personnel were aware of research aims and questions. As such, this may represent the detail of reporting rather than conduct. We suggest that researchers use blinding of participants and personnel from research aims and questions, to the extent that it is ethically valid. Furthermore, we recommend that the manner of blinding is reported clearly.
The fourth challenge requires an increased transparency and detail in reporting that is currently piecemeal in the reviewed literature: in general, activities; pedagogies; and types and qualities of the natural environments of the interventions and programs under investigation were not presented in sufficient detail. This hinders reproducibility and generalizability of the study results, and ultimately accumulation of solid evidence. The issue transferability and generalizability relates to that of cultural specificity in practices of immersive nature-experience and was also identified by Sandell (2004). Given that practices are culturally and geographically bounded, descriptions of these conditions, approaches, and underlying assumptions should to be described carefully. This challenge could be addressed in a systematic manner by utilizing intervention description checklists, for example the Template for Intervention Description and Replication (TIDieR) (Hoffmann et al., 2014). Using such a checklist will provide a transparency about basic intervention and program information pertaining to, for example, intervention delivery, e.g., physical or informational materials and procedures used; provision, e.g., profession, expertise, and specific training of key intervention providers; mode, e.g., face-to-face or group or alone; location, e.g., place and infrastructure; and intensity, e.g., number of sessions, duration, and schedule. Naturally, the checklist is generic in character and, depending on the specific type of activity and the cultural and geographical context, further description is warranted. For example, information about the intended type and actual practice of pedagogical or psychological approach used, e.g., positive psychology or cognitive-therapy, should be included. Likewise, thorough description of the intervention and control environments are also needed, for example, type of landscape, vegetation, elevation, and season.
In addition to these four methodological challenges and suggestions for solutions, the utility of immersive nature-experience as an affordable, upstream health promotion approach (Maller et al., 2006) would be strongly solidified by supplying studies with cost-effectiveness information (Hartig et al., 2014; Gottfredson et al., 2015). In agreement with Hartig et al. (2014), we suggest that future studies consider reporting cost-effectiveness information, or, in the absence of the resource or skill required, the costs related to interventions (Gottfredson et al., 2015).
The aim of this systematic review was to summarize and evaluate the evidence for effects of, and associations between, immersive nature experience on mental, physical, and social health. We identified 461 publications including 489 individual studies that met the inclusion criteria. Most studies were qualitative or observational, quantitative. Amongst 133 quantitative analyses in which control groups or conditions had been utilized, we found conditional support for effects of various immersive nature-experience on a range of outcomes: psychological wellbeing (n = 97; ≈55% positive; ≈13% mixed; ≈29% non-significant; 2% negative); psychosocial function (n = 67; ≈61% positive; ≈9% mixed; ≈30% non-significant); psychophysiological stress response (n = 50; ≈58% positive; ≈18% mixed; ≈24% non-significant), and cognitive performance (n = 36; ≈58% positive; ≈6% mixed; ≈33% non-significant; 3% negative); and social skills and relationships (n = 34; ≈70% positive; ≈7% mixed; ≈22% non-significant). Findings related to outcomes categorized under physical health, e.g., risk of cardiovascular disease, were less consistent (n = 51; ≈37% positive; ≈28% mixed; ≈35% non-significant). Walking and seated relaxation in natural environments was most frequently found to enhance aspects of psychological wellbeing, reduce psychophysiological stress, and enhance cognitive performance. Intense and demanding expeditions in wild or urban nature or primitive camp-based experiences targeted toward behavioral change, or personal or social development, promoted psychosocial indicators, the ability to engage in social contexts, cooperation skills, family development, behavior (e.g., substance abuse and crime) across a range of populations.
Across the types of interventions and outcomes, the quality of the evidence was deemed low and occasionally moderate and therefore only serves as a conditional basis for inferences about effects. Based on the main reasons for considering the quality of the evidence low, we discussed four core methodological challenges identified in the reviewed literature and provided tools to address these challenges in future studies: Given the complexity of pathways between immersive nature-experience and health outcomes, studies should develop and be guided by theories of change and develop logic models for the individual immersive nature-experience and health outcome under question. Furthermore, an increased detail of reporting about, and general attention to, group allocation generation (randomized, when ethical and feasible); intervention and control group comparability (including sociodemographic information); blinding (participants, personnel, and outcome assessors); and recruitment and sampling would increase interpretability and quality of the research. Finally, further use of process evaluation and systematic intervention description is warranted. An additional focus point for future research that could provide a strong argument for immersive nature-experience as a health promotion initiative involves reporting costs related to the intervention and, when possible, cost-efficiency.
LM, PB, and EM designed and planned the systematic review. LM, EK, and RH performed electronic and supplementary literature searches. All authors contributed to literature screening, full-text eligibility assessments, and data extraction. LM and EK analyzed the literature and wrote up an early paper draft. All authors contributed to the final manuscript.
The research is funded by a grant from The Danish Outdoor Council, Denmark (ID#105821).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.00943/full#supplementary-material
1. ^http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017057988
2. ^Heart rate is sometimes used as an indicator of stress-related phenomena. However, heart rate is subject to a multitude of physiologic cardiac functions and therefore not an interpretationally robust measure of stress.
3. ^The majority of the original studies included in the meta-analyses by Bedard (2004) and Bettmann et al. (2016) were also included in the meta-analysis by Bowen and Neill (2013). Since the reviews by Bedard (2004) and Bettmann et al. (2016) focused on different target groups, the overlap between these two reviews was insubstantial: only one original study was included in both. The references (Cason and Gillis, 1994; Hattie et al., 1997; Wilson and Lipsey, 2000) pertain to reviews published previously to the period covered in this review, but were obtained when snowballing references and provide a supplement to the more recent reviews and meta-analysis.
American Institutes for Research (2005). Effects of Outdoor Education Programs for Children in California. Sacramento, CA: The California Department of Education.
Ang, R. P., Farihah, N., Lau, S. (2014). An outcome evaluation of the implementation of the outward bound Singapore five-day “intercept” program. J. Adolesc. 37, 771–778. doi: 10.1016/j.adolescence.2014.05.003
Annerstedt, M., Währborg, P. (2011). Nature-assisted therapy: systematic review of controlled and observational studies. Scand. J. Public Health 39, 371–388. doi: 10.1177/1403494810396400
Antonioli, C., Reveley, M. A. (2005). Randomised controlled trial of animal facilitated therapy with dolphins in the treatment of depression. BMJ 331:1231. doi: 10.1136/bmj.331.7527.1231
Aspinall, P., Mavros, P., Coyne, R., Roe, J. (2015). The urban brain: analysing outdoor physical activity with mobile EEG. Br. J. Sports Med. 49:272–276. doi: 10.1136/bjsports-2012-091877
Bailey, A. W., Kang, H.-K. (2015). Modeling the impact of wilderness orientation programs on first-year academic success and life purpose. J. Adv. Educ. Outdoor Learn. 15, 209–223. doi: 10.1080/14729679.2014.949809
Barton, J., Griffin, M., Pretty, J. (2012). Exercise-, nature- and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect. Public Health 132, 89–96. doi: 10.1177/1757913910393862
Bedard, R. M. (2004). Wilderness Therapy Programs for Juvenile Delinquents: A Meta-Analysis Ph.D., Colorado State University. Retrieved from: http://search.proquest.com.ep.fjernadgang.kb.dk/docview/305206094/abstract/84BAE653EE62446EPQ/1
Beightol, J. (2012). Adventure education and resilience enhancement. J. Exp. Educ. 35, 307–325. doi: 10.1177/105382591203500203
Beil, K., Hanes, D. (2013). The influence of urban natural and built environments on physiological and psychological measures of stress- a pilot study. Int. J. Environ. Res. Public Health 10, 1250–1267. doi: 10.3390/ijerph10041250
Bentsen, P., Andkjær, S., Ejbye-Ernst, N. (2009a). Friluftsliv: Natur, Samfund og Pædagogik. Copenhagen: Munksgaard Danmark.
Bentsen, P., Mygind, E., Randrup, T. B. (2009b). Towards an understanding of udeskole : education outside the classroom in a Danish context. Education 37, 29–44. doi: 10.1080/03004270802291780
Berman, M. G., Jonides, J., Kaplan, S. (2008). The cognitive benefits of interacting with nature. Psychol. Sci. 19, 1207–1212. doi: 10.1111/j.1467-9280.2008.02225.x
Berman, M. G., Kross, E., Krpan, K. M., Askren, M. K., Burson, A., Deldin, P. J., et al. (2012). Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 140, 100–105. doi: 10.1016/j.jad.2012.03.012
Bertone, Z. J. (2015). Escaping the Matrix: A Quantitative Study of the Integration of Yogic Practice in Nature. Institute of Transpersonal Psychology. Retrieved from: http://search.proquest.com/openview/2b79b71772d3f28eafccd9c71932e674/1?pq-origsite=gscholar&cbl=18750&diss=y (accessed May 3, 2017).
Bettmann, J. E., Gillis, H. L., Speelman, E. A., Parry, K. J., Case, J. M. (2016). A meta-analysis of wilderness therapy outcomes for private pay clients. J. Child Fam. Stud. 25, 2659–2673. doi: 10.1007/s10826-016-0439-0
Biddle, S. J., Asare, M. (2011). Physical activity and mental health in children and adolescents: a review of reviews. Br. J. Sports Med. 45, 886–895. doi: 10.1136/bjsports-2011-090185
Bischoff, A., Marcussen, J., Reiten, T. (2007). Friluftsliv Og Helse: En Kunnskapsoversikt. Högskolen i Telemark. Institutt for idrett og friluftslivsfag.
Bølling, M., Otte, C. R., Elsborg, P., Nielsen, G., Bentsen, P. (2018). The association between education outside the classroom and students' school motivation: results from a one-school-year quasi-experiment. Int. J. Educ. Res. 89, 22–35. doi: 10.1016/j.ijer.2018.03.004
Bowen, D. J., Neill, J. T. (2013). A meta-analysis of adventure therapy outcomes and moderators. Open Psychol. J. 6, 28–53. doi: 10.2174/1874350120130802001
Bowler, D. E., Buyung-Ali, L. M., Knight, T. M., Pullin, A. S. (2010). A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 10:456. doi: 10.1186/1471-2458-10-456
Bratman, G. N., Daily, G. C., Levy, B. J., Gross, J. J. (2015a). The benefits of nature experience: improved affect and cognition. Landsc. Urban Plan. 138, 41–50. doi: 10.1016/j.landurbplan.2015.02.005
Bratman, G. N., Hamilton, J. P., Daily, G. C. (2012). The impacts of nature experience on human cognitive function and mental health: nature experience, cognitive function, and mental health. Ann. N. Y. Acad. Sci. 1249, 118–136. doi: 10.1111/j.1749-6632.2011.06400.x
Bratman, G. N., Hamilton, J. P., Hahn, K. S., Daily, G. C., Gross, J. J. (2015b). Nature experience reduces rumination and subgenual prefrontal cortex activation. Proc. Natl. Acad. Sci. U.S.A. 112, 8567–8572. doi: 10.1073/pnas.1510459112
Brown, D. K., Barton, J. L., Pretty, J., Gladwell, V. F. (2014). Walks4Work: assessing the role of the natural environment in a workplace physical activity intervention. Scand. J. Work Environ. Health 40, 390–399. doi: 10.5271/sjweh.3421
Brussoni, M., Gibbons, R., Gray, C., Ishikawa, T., Sandseter, E. B., Bienenstock, A., et al. (2015). What is the relationship between risky outdoor play and health in children? A systematic review. Int. J. Environ. Res. Public Health 12, 6423–6454. doi: 10.3390/ijerph120606423
Calogiuri, G., Evensen, K., Weydahl, A., Andersson, K., Patil, G., Ihlebæk, C., et al. (2015). Green exercise as a workplace intervention to reduce job stress. Results from a pilot study. Work 53, 99–111. doi: 10.3233/WOR-152219
Cason, D., Gillis, L. H. L. (1994). A meta-analysis of outdoor adventure programming with adolescents. J. Exp. Educ. 17, 40–47. doi: 10.1177/105382599401700109
Chun, M. H., Chang, M. C., Lee, S.-J. (2017). The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 127, 199–203. doi: 10.3109/00207454.2016.1170015
Collins, R. H. (2014). The Effect of An Extended Wilderness Education Experience on Ill-Structured Problem-Solving Skill Development in Emerging Adult Students. Retrieved from: http://search.proquest.com/openview/4799de27b7f7d50c01e617cb5482932e/1?pq-origsite=gscholar&cbl=18750&diss=y (accessed May 30, 2017).
Connelly, J. (2012). Adventure-Based Counseling and Self-Efficacy with High School Freshmen. Regent University, VA: ProQuest LLC.
Cooley, S. J., Burns, V. E., Cumming, J. (2015). The role of outdoor adventure education in facilitating groupwork in higher education. High. Educ. 69, 567–582. doi: 10.1007/s10734-014-9791-4
Daniel, B., Bobilya, A. J., Kalisch, K., McAvoy, L. (2014). Autonomous student experiences in outdoor and adventure education. J. Exp. Educ. 37, 4–17. doi: 10.1177/1053825913518892
Darrin Kass, C. G. (2011). Learning to lead at 5,267 feet: an empirical study of outdoor management training and MBA students' leadership development. J. Leadersh. Educ. 10, 41–62. doi: 10.12806/V10/I1/RF3
de Assis Pimentel, G. G. (2008). Aspectos socioculturais na percepção da qualidade de vida entre praticantes de esportes de aventura. Revista Salud Pública 10, 561–570. doi: 10.1590/S0124-00642008000400006
Dettweiler, U., Becker, C., Auestad, B. H., Simon, P., Kirsch, P. (2017). Stress in school. Some empirical hints on the circadian cortisol rhythm of children in outdoor and indoor classes. Int. J. Environ. Res. Public Health 14:475. doi: 10.3390/ijerph14050475
Duerden, M. D., Widmer, M. A., Taniguchi, S. T., McCoy, J. K. (2009). Adventures in identity development: the impact of adventure recreation on adolescent identity development. Identity 9, 341–359. doi: 10.1080/15283480903422806
Durr, L. I. (2009). Optimal challenge: the impact of adventure experiences on subjective well-being. J. Exp. Educ. 31, 451–455. doi: 10.1177/105382590803100319
Dyment, J. E., Bell, A. C. (2008). Grounds for movement: green school grounds as sites for promoting physical activity. Health Educ. Res. 23, 952–962. doi: 10.1093/her/cym059
Edwards, L. C., Bryant, A. S., Keegan, R. J., Morgan, K., Cooper, S.-M., Jones, A. M. (2018). “Measuring” physical literacy and related constructs: a systematic review of empirical findings. Sports Med. 48, 659–682. doi: 10.1007/s40279-017-0817-9
Eikenaes, I., Gude, T., Hoffart, A. (2006). Integrated wilderness therapy for avoidant personality disorder. Nord. J. Psychiatry 60, 275–281. doi: 10.1080/08039480600790093
Ejbye-Ernst, N. (2013). Natur og Sociale Indsatser. Retrieved from Red Barnet website: http://doczz.net/doc/6984858/natur-og-sociale-indsatser (accessed June 22, 2017).
Ekelund, U., Steene-Johannessen, J., Brown, W. J., Fagerland, M. W., Owen, N., Powell, K. E., et al. (2016). Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 388, 1302–1310. doi: 10.1016/S0140-6736(16)30370-1
Ewert, A., Overholt, J. R. (2010). Fostering Leadership through a Three-Week Experience: Does Outdoor Education Make a Difference? Retrieved from https://www.academia.edu/2113299/Fostering_Leadership_through_a_Three-Week_Experience_Does_Outdoor_Education_Make_a_Difference (accessed October 8, 2017).
Ewert, A., Yoshino, A. (2011). The influence of short-term adventure-based experiences on levels of resilience. J. Adv. Educ. Outdoor Learn. 11, 35–50. doi: 10.1080/14729679.2010.532986
Fattorini, L., Pittiglio, G., Federico, B., Pallicca, A., Bernardi, M., Rodio, A. (2012). Workload comparison between hiking and indoor physical activity. J. Strength Condition. Res. 26, 2883–2889. doi: 10.1519/JSC.0b013e318242a61e
Fernee, C. R., Gabrielsen, L. E., Andersen, A. J., Mesel, T. (2017). Unpacking the black box of wilderness therapy: a realist synthesis. Qual. Health Res. 27, 114–129. doi: 10.1177/1049732316655776
Fjørtoft, I. (2004). Landscape as playscape: the effects of natural environments on children's play and motor development. Child. Youth Environ. 14, 21–44.
Fok, C. C., Henry, D., Allen, J. (2015). Research designs for intervention research with small samples II: stepped wedge and interrupted time-series designs. Prevent. Sci. 16, 967–977. doi: 10.1007/s11121-015-0569-4
Foley, J. M. (2009). Measuring student learning outcomes on Outward Bound courses and associated independent variables (Colorado State University). Retrieved from: http://search.proquest.com/openview/1626f18c6a454a801a78185195cbcf58/1?pq-origsite=gscholar&cbl=18750&diss=y (accessed June 2, 2017).
Frauman, E., Waryold, D. (2009). Impact of a wilderness orientation program on college student's life effectiveness. J. Outdoor Recreat. Educ. Leadersh. 1, 189–207. doi: 10.7768/1948-5123.1018
Frieden, T. R. (2017). Evidence for health decision making - beyond randomized, controlled trials. N. Engl. J. Med. 377, 465–475. doi: 10.1056/NEJMra1614394
Frühauf, A., Niedermeier, M., Elliott, L. R., Ledochowski, L., Marksteiner, J., Kopp, M. (2016). Acute effects of outdoor physical activity on affect and psychological well-being in depressed patients-a preliminary study. Ment. Health Phys. Act. 10, 4–9. doi: 10.1016/j.mhpa.2016.02.002
Fuller, C., Powell, D., Fox, S. (2017). Making gains: the impact of outdoor residential experiences on students' examination grades and self-efficacy. Educ. Rev. 69, 232–247. doi: 10.1080/00131911.2016.1199538
Furie, J. (2011). Adventure Based Counseling as an Intervention for Bullying. Alliant International University. Retrieved from: https://media-proquest-com.ep.fjernadgang.kb.dk/media/pq/classic/doc/2484132611/fmt/ai/rep/NPDF?cit%3Aauth=Furie%2C+Jessica&cit%3Atitle=Adventure+based+counseling+as+an+intervention+for+bullying&cit%3Apub=ProQuest+Dissertations+and+Theses&cit%3Avol=&cit%3Aiss=&cit%3Apg=&cit%3Adate=2011&ic=true&cit%3Aprod=ProQuest&_a=ChgyMDE3MDgwOTE2MDUzNTkxODo3NDM1OTgSBTk4MjQwGgpPTkVfU0VBUkNIIg4xMzAuMjI2LjIyOS4xNioFMTg3NTAyCTg5NzkxOTU4MDoNRG9jdW1lbnRJbWFnZUIBMFIGT25saW5lWgJGVGIDUEZUagoyMDExLzAxLzAxcgoyMDExLzEyLzMxegCCASlQLTEwMDcxMDYtMTA0MTYtQ1VTVE9NRVItMTAwMDAyNTUtNTA0NTg3NZIBBk9ubGluZcoBSE1vemlsbGEvNS4wIChXaW5kb3dzIE5UIDYuMTsgV09XNjQ7IHJ2OjU0LjApIEdlY2tvLzIwMTAwMTAxIEZpcmVmb3gvNTQuMNIBFkRpc3NlcnRhdGlvbnMgJiBUaGVzZXOaAgdQcmVQYWlkqgIoT1M6RU1TLVBkZkRvY1ZpZXdCYXNlLWdldE1lZGlhVXJsRm9ySXRlbbICJjIwMTcwODA5MTYwNTM1OTE4Ojc0MzU5ODoxNTAyMjk0NzU3MDczugIpUC0xMDA3MTA2LTEwNDE2LUNVU1RPTUVSLTEwMDAwMjU1LTUwNDU4NzXKAhNEaXNzZXJ0YXRpb24vVGhlc2lz0gIBWeICAPICAA%3D%3D&_s=zE02LuW5kO8P6tlh%2B7wNMJvDI%2FM%3D
Furman, N., Sibthorp, J. (2014). The development of prosocial behavior in adolescents: a mixed methods study from NOLS. J. Exp. Educ. 37, 160–175. doi: 10.1177/1053825913489105
Gatersleben, B., Andrews, M. (2013). When walking in nature is not restorative? The role of prospect and refuge. Health Place 20, 91–101. doi: 10.1016/j.healthplace.2013.01.001
Gatzemann, T., Schweizer, K., Hummel, A. (2008). Effectiveness of sports activities with an orientation on experiential education, adventure-based learning and outdoor-education. Kineziologija 40, 147–153.
Gehris, J. S. (2007). A Quantitative and Qualitative Investigation of the Effects of Adventure Education on High School Students. Philadelphia, PA: Temple University.
Gelkopf, M., Hasson-Ohayon, I., Bikman, M., Kravetz, S. (2013). Nature adventure rehabilitation for combat-related posttraumatic chronic stress disorder: a randomized control trial. Psychiatry Res. 209, 485–493. doi: 10.1016/j.psychres.2013.01.026
Gelter, H. (2000). Friluftsliv: the Scandinavian philosophy of outdoor life. Can. J. Environ. Educ. 5, 77–92.
Gidlow, C. J., Jones, M. V., Hurst, G., Masterson, D., Clark-Carter, D., Tarvainen, M. P., et al. (2016). Where to put your best foot forward: psycho-physiological responses to walking in natural and urban environments. J. Environ. Psychol. 45, 22–29. doi: 10.1016/j.jenvp.2015.11.003
Gill, E., Goldenberg, M., Starnes, H., Phelan, S. (2016). Outdoor adventure therapy to increase physical activity in young adult cancer survivors. J. Psychosoc. Oncol. 34, 184–199. doi: 10.1080/07347332.2016.1157718
Gottfredson, D. C., Cook, T. D., Gardner, F. E., Gorman-Smith, D., Howe, G. W., Sandler, I. N., et al. (2015). Standards of evidence for efficacy, effectiveness, and scale-up research in prevention science: next generation. Prevent. Sci. 16, 893–926. doi: 10.1007/s11121-015-0555-x
Green, B. N., Johnson, C. D., Adams, A. (2006). Writing narrative literature reviews for peer-reviewed journals: secrets of the trade. J. Chiropr. Med. 5, 101–117. doi: 10.1016/S0899-3467(07)60142-6
Grinde, B., Patil, G. G. (2009). Biophilia: does visual contact with nature impact on health and well-being? Int. J. Environ. Res. Public Health 6, 2332–2343. doi: 10.3390/ijerph6092332
Grønningsæter, I., Hallås, O., Kristiansen, T., Nævdal, F. (2007). Fysisk aktivitet hos 11 - 12-åringar i skulen. Tidsskriftet Den Norske Legeforeng. Retrieved from: https://tidsskriftet.no/2007/11/originalartikkel/fysisk-aktivitet-hos-11-12-aringar-i-skulen
Guthrie, H. (2004). Adventure Therapy for Children With Mental Disorders: A Treatment Outcome Study (The University of Akron). Retrieved from: https://media-proquest-com.ep.fjernadgang.kb.dk/media/pq/classic/doc/845722061/fmt/ai/rep/SPDF?cit%3Aauth=Guthrie%2C+Heather&cit%3Atitle=Adventure+therapy+for+children+with+mental+disorders%3A++A+treatment+outcome+study&cit%3Apub=ProQuest+Dissertations+and+Theses&cit%3Avol=&cit%3Aiss=&cit%3Apg=&cit%3Adate=2004&ic=true&cit%3Aprod=ProQuest+Dissertations+%26+Theses+Global&_a=ChgyMDE3MDgxNzEzNDIzMzQ0ODo1NzgzODgSBTk4MjQwGgpPTkVfU0VBUkNIIg4xMzAuMjI2LjIyOS4xNioFMTg3NTAyCTMwNTIwODQ3NToNRG9jdW1lbnRJbWFnZUIBMFIGT25saW5lWgJGVGIDUEZUagoyMDA0LzAxLzAxcgoyMDA0LzEyLzMxegCCASlQLTEwMDg3NDktMTA0MTYtQ1VTVE9NRVItMTAwMDAyMDUtMzk2NTY3NZIBBk9ubGluZcoBSE1vemlsbGEvNS4wIChXaW5kb3dzIE5UIDYuMTsgV09XNjQ7IHJ2OjU0LjApIEdlY2tvLzIwMTAwMTAxIEZpcmVmb3gvNTQuMNIBFkRpc3NlcnRhdGlvbnMgJiBUaGVzZXOaAgdQcmVQYWlkqgIoT1M6RU1TLVBkZkRvY1ZpZXdCYXNlLWdldE1lZGlhVXJsRm9ySXRlbbICJjIwMTcwODE3MTM0MjMzNDQ4OjU3ODM4ODoxNTAyOTc3NzM1MjgzugIpUC0xMDA4NzQ5LTEwNDE2LUNVU1RPTUVSLTEwMDAwMjA1LTM5NjU2NzXKAhNEaXNzZXJ0YXRpb24vVGhlc2lz0gIBWeICAPICAA%3D%3D&_s=69dz7cAD9vCGlJk%2BlALfln%2FToWo%3D
Haluza, D., Schönbauer, R., Cervinka, R. (2014). Green perspectives for public health: a narrative review on the physiological effects of experiencing outdoor nature. Int. J. Environ. Res. Public Health 11, 5445–5461. doi: 10.3390/ijerph110505445
Han, J.-W., Choi, H., Jeon, Y.-H., Yoon, C.-H., Woo, J.-M., Kim, W. (2016). The effects of forest therapy on coping with chronic widespread pain: physiological and psychological differences between participants in a forest therapy program and a control group. Int. J. Environ. Res. Public Health 13:255. doi: 10.3390/ijerph13030255
Harris, J. P. (2005). The Impact of an Experiential/Adventure Intervention on Male Adolescents With Special Needs. Ph.D. thesis, Colorado State University. Retrieved from: http://search.proquest.com.ep.fjernadgang.kb.dk/docview/305009349/abstract/15D80F9B311F41C4PQ/1
Hartig, T., Mitchell, R., de Vries, S., Frumkin, H. (2014). Nature and health. Annu. Rev. Public Health 35, 207–228. doi: 10.1146/annurev-publhealth-032013-182443
Hartig, T., van den Berg, A. E., Hagerhall, C. M., Tomalak, M., Bauer, N., Hansmann, R., et al. (2011). “Health benefits of nature experience: psychological, social and cultural processes,” in Forests, Trees and Human Health, eds K. Nilsson, M. Sangster, C. Gallis, T. Hartig, S. de Vries, K. Seeland, and J. Schipperijn (Dordrecht: Springer), 127–168. doi: 10.1007/978-90-481-9806-1_5
Harun, M. T., Salamuddin, N. (2010). Cultivating personality development through outdoor education programme: the Malaysia experience. Procedia Soc. Behav. Sci. 9, 228–234. doi: 10.1016/j.sbspro.2010.12.141
Hattie, J., Marsh, H. W., Richards, G. (1997). Adventure education and outward bound: out-of-class experiences that make a lasting difference. Rev. Educ. Res. 67, 47–87. doi: 10.3102/00346543067001043
Hayhurst, J., Hunter, J. A., Kafka, S., Boyes, M. (2015). Enhancing resilience in youth through a 10-day developmental voyage. J. Adv. Educ. Outdoor Learn. 15, 40–52. doi: 10.1080/14729679.2013.843143
Hepperger, C., Gföller, P., Hoser, C., Ulmer, H., Fischer, F., Schobersberger, W., et al. (2016). The effects of a 3-month controlled hiking programme on the functional abilities of patients following total knee arthroplasty: a prospective, randomized trial. Knee Surgery Sports Traumatol. Arthrosc. 25, 3387–3395. doi: 10.1007/s00167-016-4299-3
Hoffmann, T. C., Glasziou, P. P., Boutron, I., Milne, R., Perera, R., Moher, D., et al. (2014). Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 348:g1687. doi: 10.1136/bmj.g1687
Hohashi, N., Kobayashi, K. (2013). The effectiveness of a forest therapy (shinrin-yoku) program for girls aged 12 to 14 years: a crossover study. Stress Sci. Res. 28, 82–89. doi: 10.5058/stresskagakukenkyu.28.82
Hough, M., Paisley, K. (2008). An empowerment theory approach to adventure programming for adults with disabilities. Ther. Recreation J. 42, 89–102.
Hunter, J. A., Hayhurst, J., Kafka, S., Boyes, M., Ruffman, T., O'Brien, K., et al. (2013). Elevated self-esteem 12 months following a 10-day developmental voyage: elevated self-esteem. J. Appl. Soc. Psychol. 43, 1956–1961. doi: 10.1111/jasp.12132
Hunter, J. A., Kafka, S., Hayhurst, J., Clark, H., Dickerson, D., Harold, G., et al. (2010). Increased self-efficacy following a ten-day developmental voyage. J. Child Adolesc. Mental Health 22, 63–65. doi: 10.2989/17280583.2010.496943
Jelalian, E., Lloyd-Richardson, E. E., Mehlenbeck, R. S., Hart, C. N., Flynn-O'Brien, K., Kaplan, J., et al. (2010). Behavioral weight control treatment with supervised exercise or peer-enhanced adventure for overweight adolescents. J. Pediatr. 157, 923–928.e1. doi: 10.1016/j.jpeds.2010.05.047
Jelalian, E., Mehlenbeck, R. S., Lloyd-Richardson, E. E., Birmaher, V., Wing, R. R. (2006). “Adventure therapy” combined with cognitive-behavioral treatment for overweight adolescents. Int. J. Obesity 30, 31–39. doi: 10.1038/sj.ijo.0803069
Jelalian, E., Sato, A., Hart, C. N. (2011). The effect of group-based weight-control intervention on adolescent psychosocial outcomes: perceived peer rejection, social anxiety, and self-concept. Children's Health Care 40, 197–211. doi: 10.1080/02739615.2011.590391
Jelley, S. (2005). Outdoor education physical activities : a primary prevention for adolescent male obesity. (Abstract). J. Sci. Med. Sport 8(4 Suppl.):91. doi: 10.1016/S1440-2440(17)30656-4
Johansson, B., Bjuhr, H., Karlsson, M., Karlsson, J.-O., Rönnbäck, L. (2015). Mindfulness-Based Stress Reduction (MBSR) delivered live on the internet to individuals suffering from mental fatigue after an acquired brain injury. Mindfulness 6, 1356–1365. doi: 10.1007/s12671-015-0406-7
Johansson, M., Hartig, T., Staats, H. (2011). Psychological Benefits of Walking: moderation by company and outdoor environment: environmental moderation of walking benefits. Appl. Psychol. Health Well-Being 3, 261–280. doi: 10.1111/j.1758-0854.2011.01051.x
Johnson-Pynn, J. S., Johnson, L. R., Kityo, R., Lugumya, D. (2014). Students and scientists connect with nature in Uganda, East Africa. Int. J. Environ. Sci. Educ. 9, 311–327. doi: 10.12973/ijese.2014.217a
Jordet, A. N. (2010). Klasserommet Utenfor. Tilpasset Oppl a Ering i et Utvidet L a Eringsrom. Retrieved from: http://realfag.eventweb.no/NTEVENT/Realfag2011.nsf/DocsB/E8FB8ECEBD906C69C1257811003D59D7/$FILE/Klasserommet_utenfor-informasjonsbrosjyre.pdf
Kafka, S., Hunter, J. A., Hayhurst, J., Boyes, M., Thomson, R. L., Clarke, H., et al. (2012). A 10-day developmental voyage: converging evidence from three studies showing that self-esteem may be elevated and maintained without negative outcomes. Soc. Psychol. Educ. 15, 571–601. doi: 10.1007/s11218-012-9177-3
Kaplan, S. (1995). The restorative benefits of nature: toward an integrative framework. J. Environ. Psychol. 15, 169–182. doi: 10.1016/0272-4944(95)90001-2
Kerr, J. H., Fujiyama, H., Sugano, A., Okamura, T., Chang, M., Onouha, F. (2006). Psychological responses to exercising in laboratory and natural environments. Psychol. Sport Exerc. 7, 345–359. doi: 10.1016/j.psychsport.2005.09.002
Kim, W., Lim, S.-K., Chung, E.-J., Woo, J.-M. (2009). The effect of cognitive behavior therapy-based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiatry Investig. 6:245. doi: 10.4306/pi.2009.6.4.245
Kjellgren, A., Buhrkall, H. (2010). A comparison of the restorative effect of a natural environment with that of a simulated natural environment. J. Environ. Psychol. 30, 464–472. doi: 10.1016/j.jenvp.2010.01.011
Konijnendijk, C. C., Annerstedt, M., Nielsen, A. B., Maruthaveeran, S. (2013). Benefits of Urban Parks: A Systematic Review. A Report for IPFRA. Retrieved from IFPRA website: http://curis.ku.dk/ws/files/44944034/ifpra_park_benefits_review_final_version.pdf
Kuo, M. (2015). How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 6:1093. doi: 10.3389/fpsyg.2015.01093
Larsen, L. R., Kristensen, P. L., Junge, T., Rexen, C. T., Wedderkopp, N. (2015). Motor performance as predictor of physical activity in children: the CHAMPS study-DK. Med. Sci. Sports Exerc. 47, 1849–1856. doi: 10.1249/MSS.0000000000000604
Larson, B. A. (2007). Adventure camp programs, self-concept, and their effects on behavioral problem adolescents. J. Exp. Educ. 29, 313–330. doi: 10.1177/105382590702900304
Lee, I.-M., Shiroma, E. J., Lobelo, F., Puska, P., Blair, S. N., Katzmarzyk, P. T. (2012). Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 380, 219–229. doi: 10.1016/S0140-6736(12)61031-9
Lee, J., Park, B.-J., Ohira, T., Kagawa, T., Miyazaki, Y. (2015). Acute effects of exposure to a traditional rural environment on urban dwellers: a crossover field study in terraced farmland. Int. J. Environ. Res. Public Health 12, 1874–1893. doi: 10.3390/ijerph120201874
Lee, J., Park, B.-J., Tsunetsugu, Y., Kagawa, T., Miyazaki, Y. (2009). Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. Forest Res. 24, 227–234. doi: 10.1080/02827580902903341
Lee, J., Park, B.-J., Tsunetsugu, Y., Ohira, T., Kagawa, T., Miyazaki, Y. (2011). Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 125, 93–100. doi: 10.1016/j.puhe.2010.09.005
Lee, J., Tsunetsugu, Y., Takayama, N., Park, B.-J., Li, Q., Song, C., et al. (2014). Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Complement. Alternat. Med. 2014:834360. doi: 10.1155/2014/834360
Lee, J.-Y., Lee, D.-C. (2014). Cardiac and pulmonary benefits of forest walking versus city walking in elderly women: a randomised, controlled, open-label trial. Eur. J. Integr. Med. 6, 5–11. doi: 10.1016/j.eujim.2013.10.006
Lethbridge, K., Yankou, D., Andrusyszyn, M.-A., and American Holistic Nurses' Association Education Provider Committee (2005). The effects of a restorative intervention on undergraduate nursing students' capacity to direct attention. J. Holistic Nurs. 23, 323–347. doi: 10.1177/0898010105279610
Li, Q., Kobayashi, M., Kumeda, S., Ochiai, T., Miura, T., Kagawa, T., et al. (2016). Effects of forest bathing on cardiovascular and metabolic parameters in middle-aged males. Evid. Based Complement. Alternat. Med. 2016:e2587381. doi: 10.1155/2016/2587381
Li, Q., Morimoto, K., Kobayashi, M., Inagaki, H., Katsumata, M., Hirata, Y., et al. (2008). Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 21, 117–127. doi: 10.1177/039463200802100113
Li, Q., Otsuka, T., Kobayashi, M., Wakayama, Y., Inagaki, H., Katsumata, M., et al. (2011). Acute effects of walking in forest environments on cardiovascular and metabolic parameters. Eur. J. Appl. Physiol. 111, 2845–2853. doi: 10.1007/s00421-011-1918-z
Lima, R. A., Pfeiffer, K., Larsen, L. R., Bugge, A., Moller, N. C., Anderson, L. B., et al. (2017b). Physical activity and motor competence present a positive reciprocal longitudinal relationship across childhood and early adolescence. J. Phys. Activity Health 14, 440–447. doi: 10.1123/jpah.2016-0473
Lima, R. A., Pfeiffer, K. A., Bugge, A., Møller, N. C., Andersen, L. B., Stodden, D. F. (2017a). Motor competence and cardiorespiratory fitness have greater influence on body fatness than physical activity across time. Scand. J. Med. Sci. Sports 27, 1638–1647. doi: 10.1111/sms.12850
Lubans, D. R., Plotnikoff, R. C., Lubans, N. J. (2012). Review: a systematic review of the impact of physical activity programmes on social and emotional well-being in at-risk youth: review of physical activity programmes for at-risk youth. Child Adolesc. Ment. Health 17, 2–13. doi: 10.1111/j.1475-3588.2011.00623.x
Maller, C., Townsend, M., Pryor, A., Brown, P., St. Leger, L. (2006). Healthy nature healthy people: ‘contact with nature' as an upstream health promotion intervention for populations. Health Promot. Int. 21, 45–54. doi: 10.1093/heapro/dai032
Mann, M. J. (2007). The Influence of Project Challenge on Levels of Psychosocial Development and Resilence in Adolescent Girls at Risk for Delinquency. University of Florida. Retrieved from: http://etd.fcla.edu/UF/UFE0021251/mann_m.pdf
Mao, G.-X., Cao, Y.-B., Lan, X.-G., He, Z.-H., Chen, Z.-M., Wang, Y.-Z., et al. (2012a). Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 60, 495–502. doi: 10.1016/j.jjcc.2012.08.003
Mao, G.-X., Lan, X.-G., Cao, Y.-B., Chen, Z. M., He, Z.-H., Lv, Y.-D., et al. (2012b). Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 25, 317–324. doi: 10.3967/0895-3988.2012.03.010
Margalit, D., Ben-Ari, A. (2014). The effect of wilderness therapy on adolescents' cognitive autonomy and self-efficacy: results of a non-randomized trial. Child Youth Care Forum 43, 181–194. doi: 10.1007/s10566-013-9234-x
Marmot, M. (2005). Social determinants of health inequalities. Lancet 365, 1099–1104. doi: 10.1016/S0140-6736(05)74234-3
Martens, D., Gutscher, H., Bauer, N. (2011). Walking in “wild” and “tended” urban forests: the impact on psychological well-being. J. Environ. Psychol. 31, 36–44. doi: 10.1016/j.jenvp.2010.11.001
Matsuura, A., Nagai, N., Funatsu, A., Irimajiri, M., Yamazaki, A., Hodate, K. (2011). Comparison of the short-term effects of horse trekking and exercising with a riding simulator on autonomic nervous activity. Anthrozoös 24, 65–77. doi: 10.2752/175303711X12923300467401
Mayer, F. S., Frantz, C. M., Bruehlman-Senecal, E., Dolliver, K. (2009). Why is nature beneficial? The role of connectedness to nature. Environ. Behav. 41, 607–643. doi: 10.1177/0013916508319745
McKenzie, E. A. (2015). Access to an Outdoor Classroom and Changes in Classroom Environment: Elementary School Teachers' Perspectives. Ph.D., thesis, Oklahoma State University. Retrieved from: https://search.proquest.com/docview/1820070929/abstract/FE2E86B0785B4BAFPQ/1
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Monninkhof, E. M., Elias, S. G., Vlems, F. A., van der Tweel, I., Schuit, A. J., Voskuil, D. W., et al. (2007). Physical activity and breast cancer: a systematic review. Epidemiology 18, 137–157. doi: 10.1097/01.ede.0000251167.75581.98
Morita, E., Fukuda, S., Nagano, J., Hamajima, N., Yamamoto, H., Iwai, Y., et al. (2007). Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 121, 54–63. doi: 10.1016/j.puhe.2006.05.024
Mutz, M., Müller, J. (2016). Mental health benefits of outdoor adventures: results from two pilot studies. J. Adolesc. 49, 105–114. doi: 10.1016/j.adolescence.2016.03.009
Mygind, E. (2005). Udeundervisning i Folkeskolen: et Casestudie om en Naturklasse på Rødkilde Skole og Virkningerne af en Ugentlig Obligatorisk Naturdag på Yngste Klassetrin i Perioden 2000-2003. Copenhagen: Museum Tusculanum Press.
Mygind, E. (2007). A comparison between children's physical activity levels at school and learning in an outdoor environment. J. Adv. Educ. Outdoor Learn. 7, 161–176. doi: 10.1080/14729670701717580
Mygind, E. (2009). A comparison of childrens' statements about social relations and teaching in the classroom and in the outdoor environment. J. Adv. Educ. Outdoor Learn. 9, 151–169. doi: 10.1080/14729670902860809
Mygind, E. (2016). Physical activity during learning inside and outside the classroom. Health Behav. Policy Rev. 3, 455–467. doi: 10.14485/HBPR.3.5.6
Mygind, L., Hartmeyer, R., Kjeldsted, E., Mygind, E., Bentsen, P. (2018a). Viden om Friluftslivs Effekter på Sundhed-Resultater fra en Systematisk Forskningsoversigt, 40. Copenhagen. Retrieved from The Danish Outdoor Council website: https://www.friluftsraadet.dk/publikationer
Mygind, L., Kjeldsted, E., Hartmeyer, R., Mygind, E., Bentsen, P. (2018b). Forskningsoversigt Over Effekter af Friluftsliv på Mental, Fysisk og Social Sundhed, 330. Copenhagen. Retrieved from The Danish Outdoor Council website: https://www.friluftsraadet.dk/publikationer
Neunhäuserer, D., Sturm, J., Baumgartlinger, M. M., Niederseer, D., Ledl-Kurkowski, E., Steidle, E., et al. (2013). Hiking in suicidal patients: neutral effects on markers of suicidality. Am. J. Med. 126, 927–930. doi: 10.1016/j.amjmed.2013.05.008
Nielsen, G. (2016). A quasi-experimental cross-disciplinary evaluation of the impacts of education outside the classroom on pupils' physical activity, well-being and learning: the TEACHOUT study protocol. BMC Public Health 16:1117. doi: 10.1186/s12889-016-3780-8
Norton, C. L. (2014). Adventure therapy with youth. J. Exp. Educ. 37, 46–59. doi: 10.1177/1053825913518895
Nutbeam, D. (1998). Evaluating health promotion-progress, problems and solutions. Health Promot. Int. 13, 27–44. doi: 10.1093/heapro/13.1.27
O'Brien, K., Lomas, T. (2017). Developing a growth mindset through outdoor personal development: can an intervention underpinned by psychology increase the impact of an outdoor learning course for young people? J. Adv. Educ. Outdoor Learn. 17, 133–147. doi: 10.1080/14729679.2016.1232199
Ohly, H., White, M. P., Wheeler, B. W., Bethel, A., Ukoumunne, O. C., Nikolaou, V., et al. (2016). Attention restoration theory: a systematic review of the attention restoration potential of exposure to natural environments. J. Toxicol. Environ. Health Part B Crit. Rev. 19, 305–343. doi: 10.1080/10937404.2016.1196155
Orren, P. M., Werner, P. D. (2007). Effects of brief wilderness programs in relation to adolescents' race. J. Exp. Educ. 30, 117–133. doi: 10.1177/105382590703000203
Paquette, J., Vitaro, F. (2014). Wilderness therapy, interpersonal skills and accomplishment motivation: impact analysis on antisocial behavior and socio-professional status. Resid. Treat. Child. Youth 31, 230–252. doi: 10.1080/0886571X.2014.944024
Paquette, L., Brassard, A., Guérin, A., Fortin-Chevalier, J., Tanguay-Beaudoin, L. (2014). Effects of a developmental adventure on the self-esteem of college students. J. Exp. Educ. 37, 216–231. doi: 10.1177/1053825913498372
Park, B.-J. (2009). Physiological effects of forest recreation in a young conifer forest in Hinokage Town, Japan. Silva Fennica 43:213. doi: 10.14214/sf.213
Park, B.-J., Furuya, K., Kasetani, T., Takayama, N., Kagawa, T., Miyazaki, Y. (2011). Relationship between psychological responses and physical environments in forest settings. Landsc. Urban Plan. 102, 24–32. doi: 10.1016/j.landurbplan.2011.03.005
Park, B.-J., Tsunetsugu, Y., Ishii, H., Furuhashi, S., Hirano, H., Kagawa, T., et al. (2008). Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in a mixed forest in Shinano Town, Japan. Scand. J. Forest Res. 23, 278–283. doi: 10.1080/02827580802055978
Park, B.-J., Tsunetsugu, Y., Kasetani, T., Hirano, H., Kagawa, T., Sato, M., et al. (2007). Physiological effects of shinrin-yoku (taking in the atmosphere of the forest)-using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 26, 123–128. doi: 10.2114/jpa2.26.123
Park, B.-J., Tsunetsugu, Y., Kasetani, T., Kagawa, T., Miyazaki, Y. (2010). The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 15, 18–26. doi: 10.1007/s12199-009-0086-9
Peacock, J., Hine, R., Pretty, J. (2007). The Mental Health Benefits of Green Exercise Activities and Green Care. Colchester, UK: Mind.
Perkins, S., Searight, H. R., Ratwik, S. (2011). Walking in a natural winter setting to relieve attention fatigue: a pilot study. Psychology 2, 777–780. doi: 10.4236/psych.2011.28119
Poulsen, D. V., Stigsdotter, U. K., Refshage, A. D. (2015). Whatever happened to the soldiers? Nature-assisted therapies for veterans diagnosed with post-traumatic stress disorder: a literature review. Urban Forest. Urban Green. 14, 438–445. doi: 10.1016/j.ufug.2015.03.009
Reed, K., Wood, C., Barton, J., Pretty, J. N., Cohen, D., Sandercock, G. R. (2013). A repeated measures experiment of green exercise to improve self-esteem in UK school children. PLoS ONE 8:e69176. doi: 10.1371/journal.pone.0069176
Roe, J., Aspinall, P. (2011a). The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place 17, 103–113. doi: 10.1016/j.healthplace.2010.09.003
Roe, J., Aspinall, P. (2011b). The restorative outcomes of forest school and conventional school in young people with good and poor behaviour. Urban Forest. Urban Green. 10, 205–212. doi: 10.1016/j.ufug.2011.03.003
Romi, S., Kohan, E. (2004). Wilderness programs: principles, possibilities and opportunities for intervention with dropout adolescents. Child Youth Care Forum 33, 115–136. doi: 10.1023/B:CCAR.0000019634.47226.ab
Rosenberg, R. S., Lange, W., Zebrack, B., Moulton, S., Kosslyn, S. M. (2014). An outdoor adventure program for young adults with cancer: positive effects on body image and psychosocial functioning. J. Psychosoc. Oncol. 32, 622–636. doi: 10.1080/07347332.2014.936652
Ryan, R., Hill, S., Broclain, D., Oliver, S., Prictor, M., and Cochrane Consumers, et al. (2013). Study Design Guide. Retrieved from: https://figshare.com/articles/Study_design_guide/6818900
Ryan, R. M., Weinstein, N., Bernstein, J., Brown, K. W., Mistretta, L., Gagné, M. (2010). Vitalizing effects of being outdoors and in nature. J. Environ. Psychol. 30, 159–168. doi: 10.1016/j.jenvp.2009.10.009
Sahlin, E., Lindegård, A., Hadzibajramovic, E., Grahn, P., Vega Matuszczyk, J., Ahlborg, G. (2016). The influence of the environment on directed attention, blood pressure and heart rate-an experimental study using a relaxation intervention. Landsc. Res. 41, 7–25. doi: 10.1080/01426397.2014.982079
Sandell, K. (2003). Begreppet Friluftsliv - som en Trebent Pall. Argaladei, 1. Garphyttan. Retrieved from: http://www.argaladei.nu/gamla/index.html%3Fsida=tidskrift_arkiv_2003-1a.html
Sandell, K. (2004). Friluftslivets värden. En Internationell Forskningsutblick. Arbetsrapport, 20. Retrieved from: https://docplayer.se/10224160-Friluftslivets-varden.html
Sanders, C. M., Yankou, D., Andrusyszyn, M.-A. (2005). Attention and restoration in post-RN students. J. Contin. Educ. Nurs. 36, 218–225. doi: 10.3928/0022-0124-20050901-08
Sato, I., Conner, T. S. (2013). The quality of time in nature: how fascination explains and enhances the relationship between nature experiences and daily affect. Ecopsychology 5, 197–204. doi: 10.1089/eco.2013.0026
Schantz, P., Silvander, U. (2004). Forskning Och Utbildning Inom Friluftsliv : Utredning Och Förslag. Retrieved from: http://gih.diva-portal.org/smash/record.jsf?pid=diva2:537 (accessed September 27, 2017).
Scheinfeld, D. E., Rochlen, A. B., Russell, M. L. (2016). The impact of outward bound programming on psychosocial functioning for male military veterans. Psychol. Men Masculinity. 18, 400–408. doi: 10.1037/men0000066
Schell, L., Cotton, S., Luxmoore, M. (2012). Outdoor adventure for young people with a mental illness: outdoor adventure for young people. Early Interv. Psychiatry 6, 407–414. doi: 10.1111/j.1751-7893.2011.00326.x
Schneller, M. B., Duncan, S., Schipperijn, J., Nielsen, G., Mygind, E., Bentsen, P. (2017a). Are children participating in a quasi-experimental education outside the classroom intervention more physically active? BMC Public Health 17:523. doi: 10.1186/s12889-017-4430-5
Schneller, M. B., Schipperijn, J., Nielsen, G., Bentsen, P. (2017b). Children's physical activity during a segmented school week: results from a quasi-experimental education outside the classroom intervention. Int. J. Behav. Nutr. Phys. Act. 14:80. doi: 10.1186/s12966-017-0534-7
Schutte, A. R., Torquati, J. C., Beattie, H. L. (2017). Impact of urban nature on executive functioning in early and middle childhood. Environ. Behav. 49, 3–30. doi: 10.1177/0013916515603095
Schwarzer, G., Carpenter, J. R., Rücker, G. (2015). “Small-study effects in meta-analysis,” in Meta-Analysis With R, eds G. Schwarzer, J. R. Carpenter, and G. Rücker (Cham: Springer), 107–141. doi: 10.1007/978-3-319-21416-0_5
Shanahan, L., McAllister, L., Curtin, M. (2009). Wilderness adventure therapy and cognitive rehabilitation: joining forces for youth with TBI. Brain Injury 23, 1054–1064. doi: 10.3109/02699050903421115
Shin, W. S., Shin, C. S., Yeoun, P. S. (2012). The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 17, 73–76. doi: 10.1007/s12199-011-0215-0
Shin, W. S., Shin, C. S., Yeoun, P. S., Kim, J. J. (2011). The influence of interaction with forest on cognitive function. Scand. J. Forest Res. 26, 595–598. doi: 10.1080/02827581.2011.585996
Shirilla, P. (2009). Adventure-based programming and social skill development in the lives of diverse youth: perspectives from two research projects. J. Exp. Educ. 31, 410–414. doi: 10.1177/105382590803100310
Sibthorp, J., Collins, R., Rathunde, K., Paisley, K., Schumann, S., Pohja, M., et al. (2015). Fostering experiential self-regulation through outdoor adventure education. J. Exp. Educ. 38, 26–40. doi: 10.1177/1053825913516735
Siegel, S. R., Robinson, J. M., Johnston, S. A., Lindley, M. R., Pfeiffer, K. A. (2015). Health-related fitness and energy expenditure in recreational youth rock climbers 8-16 years of age. Int. J. Exerc. Sci. 8:8.
Song, C., Ikei, H., Kobayashi, M., Miura, T., Taue, M., Kagawa, T., et al. (2015). Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: a pilot study. Int. J. Environ. Res. Public Health 12, 2687–2699. doi: 10.3390/ijerph120302687
Sonntag-Öström, E., Nordin, M., Dolling, A., Lundell, Y., Nilsson, L., Slunga Järvholm, L. (2015). Can rehabilitation in boreal forests help recovery from exhaustion disorder? The randomised clinical trial ForRest. Scand. J. Forest Res. 30, 732–748. doi: 10.1080/02827581.2015.1046482
Sonntag-Öström, E., Nordin, M., Lundell, Y., Dolling, A., Wiklund, U., Karlsson, M., et al. (2014). Restorative effects of visits to urban and forest environments in patients with exhaustion disorder. Urban Forest. Urban Green. 13, 344–354. doi: 10.1016/j.ufug.2013.12.007
Speck, R. M., Courneya, K. S., Mâsse, L. C., Duval, S., Schmitz, K. H. (2010). An update of controlled physical activity trials in cancer survivors: a systematic review and meta-analysis. J. Cancer Survivor. 4, 87–100. doi: 10.1007/s11764-009-0110-5
Stevenson, M. P., Schilhab, T., Bentsen, P. (2018). Attention restoration theory II: a systematic review to clarify attention processes affected by exposure to natural environments. J. Toxicol. Environ. Health B 21, 227–268. doi: 10.1080/10937404.2018.1505571
Sturm, J., Plöderl, M., Fartacek, C., Kralovec, K., Neunhäuserer, D., Niederseer, D., et al. (2012). Physical exercise through mountain hiking in high-risk suicide patients. A randomized crossover trial: mountain hiking in high-risk suicide patients. Acta Psychiatr. Scandinav. 126, 467–475. doi: 10.1111/j.1600-0447.2012.01860.x
Sung, J., Woo, J.-M., Kim, W., Lim, S.-K., Chung, E.-J. (2012). The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 34, 1–7. doi: 10.3109/10641963.2011.618195
Takayama, N., Korpela, K., Lee, J., Morikawa, T., Tsunetsugu, Y., Park, B.-J., et al. (2014). Emotional, restorative and vitalizing effects of forest and urban environments at four sites in Japan. Int. J. Environ. Res. Public Health 11, 7207–7230. doi: 10.3390/ijerph110707207
Taylor, A. F., Kuo, F. E. (2009). Children with attention deficits concentrate better after walk in the park. J. Atten. Disord. 12, 402–409.
Thomas, M. (2004). The potential unlimited programme: an outdoor experiential education and group work approach that facilitates adjustment to brain injury. Brain Injury 18, 1271–1286. doi: 10.1080/02699050410001698776
Thompson, C. W. (2006). Free-Range Teenagers: The Role of Wild Adventure Spaces in Young Peoples' Lives. Final report. Retrieved from Natural England website: https://www.academia.edu/874769/free-range_teenagers_the_role_of_wild_adventure_space_in_young_peoples_lives_final_report
Thompson, J. E. S. (2014). The Impact of an 8-Week Green-Exercise Programme on Systemic Health, and on Markers Associated with Cardiovascular Disease Risk. Cardiff, UK: Cardiff Metropolitan University. Retrieved from: https://repository.cardiffmet.ac.uk/handle/10369/7526
Tillmann, S., Tobin, D., Avison, W., Gilliland, J. (2018). Mental health benefits of interactions with nature in children and teenagers: a systematic review. J Epidemiol Community Health 2018:210436. doi: 10.1136/jech-2018-210436
Toda, M., Den, R., Hasegawa-Ohira, M., Morimoto, K. (2013). Effects of woodland walking on salivary stress markers cortisol and chromogranin A. Complement. Ther. Med. 21, 29–34. doi: 10.1016/j.ctim.2012.11.004
Tsunetsugu, Y., Park, B.-J., Ishii, H., Hirano, H., Kagawa, T., Miyazaki, Y. (2007). Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 26, 135–142. doi: 10.2114/jpa2.26.135
Tsunetsugu, Y., Park, B.-J., Miyazaki, Y. (2010). Trends in research related to “Shinrin-yoku” (taking in the forest atmosphere or forest bathing) in Japan. Environ. Health Prev. Med. 15, 27–37. doi: 10.1007/s12199-009-0091-z
Twohig-Bennett, C., Jones, A. (2018). The health benefits of the great outdoors: a systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 166, 628–637. doi: 10.1016/j.envres.2018.06.030
Tyrväinen, L., Ojala, A., Korpela, K., Lanki, T., Tsunetsugu, Y., Kagawa, T. (2014). The influence of urban green environments on stress relief measures: a field experiment. J. Environ. Psychol. 38(Supplement C), 1–9. doi: 10.1016/j.jenvp.2013.12.005
van den Berg, A. E., van den Berg, C. G. (2011). A comparison of children with ADHD in a natural and built setting: nature and ADHD. Child Care Health Dev. 37, 430–439. doi: 10.1111/j.1365-2214.2010.01172.x
Vlamis, E., Bell, B. J., Gass, M. (2011). Effects of a college adventure orientation program on student development behaviors. J. Exp. Educ. 34, 127–148. doi: 10.1177/105382591103400203
Voruganti, L. N., Whatham, J., Bard, E., Parker, G., Babbey, C., Ryan, J., et al. (2006). Going beyond: an adventure-and recreation-based group intervention promotes well-being and weight loss in schizophrenia. Can. J. Psychiatry 51, 575–580. doi: 10.1177/070674370605100905
Voutselas (2012). Physiological and metabolic responses to hiking: a meta-analysis toward health benefits. Gazzetta Medica Ital. 171, 653–9. Retrieved from: http://www.minervamedica.it/en/journals/gazzetta-medica-italiana/article.php?cod=R22Y2012N05A0653
Walsh, M. A. (2009). Wilderness Adventure Programming as an Intervention for Youthful Offenders: Self-efficacy, Resilience, and Hope for the Future. Ph.D., University of Minnesota. Retrieved from: http://search.proquest.com.ep.fjernadgang.kb.dk/docview/304939123/abstract/E62884E17C7D47AEPQ/1
Wells, M. S. (2004). Grubs and grasshoppers: challenge-based recreation and the collective efficacy of families with at-risk youth. Fam. Relat. 53, 326–333. doi: 10.1111/j.0197-6664.2003.0009.x
Wendell, N. S. (2004). Wilderness Therapy as a Viable Treatment for Emotionally and Behaviorally Disturbed Children and Adolescents. Psy.D., Spalding University. Retrieved from: http://search.proquest.com.ep.fjernadgang.kb.dk/docview/305056653/abstract/9F673CC1E4DE4252PQ/1
White, R. (2012). A sociocultural investigation of the efficacy of outdoor education to improve learner engagement. Emot. Behav. Difficulties 17, 13–23. doi: 10.1080/13632752.2012.652422
Wilson, S. J., Lipsey, M. W. (2000). Wilderness challenge programs for delinquent youth: A meta-analysis of outcome evaluations. Eval. Program Plann. 23, 1–12. doi: 10.1016/S0149-7189(99)00040-3
Wolin, K. Y., Yan, Y., Colditz, G. A., Lee, I.-M. (2009). Physical activity and colon cancer prevention: a meta-analysis. Br. J. Cancer 100, 611–616. doi: 10.1038/sj.bjc.6604917
Wood, C., Sandercock, G., Barton, J. (2014). Interactions between physical activity and the environment to improve adolescent self-esteem: a randomised controlled trial. Int. J. Environ. Health 7, 144–155. doi: 10.1504/IJENVH.2014.067359
Wyman, P. A., Henry, D., Knoblauch, S., Brown, C. H. (2015). Designs for testing group-based interventions with limited numbers of social units: the dynamic wait-listed and regression point displacement designs. Prevent. Sci. 16, 956–966. doi: 10.1007/s11121-014-0535-6
Yamaguchi, M., Deguchi, M., Miyazaki, Y. (2006). The effects of exercise in forest and urban environments on sympathetic nervous activity of normal young adults. J. Int. Med. Res. 34, 152–159. doi: 10.1177/147323000603400204
Zachor, D. A., Vardi, S., Baron-Eitan, S., Brodai-Meir, I., Ginossar, N., Ben-Itzchak, E. (2017). The effectiveness of an outdoor adventure programme for young children with autism spectrum disorder: a controlled study. Dev. Med. Child Neurol. 59, 550–556. doi: 10.1111/dmcn.13337
Keywords: friluftsliv (outdoor life), green exercise, green space, therapy, social ecology
Citation: Mygind L, Kjeldsted E, Hartmeyer RD, Mygind E, Bølling M and Bentsen P (2019) Immersive Nature-Experiences as Health Promotion Interventions for Healthy, Vulnerable, and Sick Populations? A Systematic Review and Appraisal of Controlled Studies. Front. Psychol. 10:943. doi: 10.3389/fpsyg.2019.00943
Received: 23 October 2018; Accepted: 09 April 2019;
Published: 03 May 2019.
Edited by:
Juergen Beckmann, Technische Universität München, GermanyReviewed by:
Susana Alves, Çankaya University, TurkeyCopyright © 2019 Mygind, Kjeldsted, Hartmeyer, Mygind, Bølling and Bentsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lærke Mygind, bGFlcmtlLm15Z2luZC5ncm9lbmZlbGR0QHJlZ2lvbmguZGs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.