
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Psychol. , 19 February 2019
Sec. Psychology for Clinical Settings
Volume 10 - 2019 | https://doi.org/10.3389/fpsyg.2019.00277
This article is part of the Research Topic Psychosocial Interventions for Suicide Prevention View all 12 articles
 Pablo Méndez-Bustos1*
Pablo Méndez-Bustos1* Raffaella Calati2,3
Raffaella Calati2,3 Francisca Rubio-Ramírez1
Francisca Rubio-Ramírez1 Emilie Olié2,4,5
Emilie Olié2,4,5 Philippe Courtet2,4,5
Philippe Courtet2,4,5 Jorge Lopez-Castroman2,6
Jorge Lopez-Castroman2,6Background: Suicidal behavior is a major public health concern worldwide, and the interest in the development of novel and more efficient treatment strategies and therapies to reduce suicidal risk is increasing. Some recent studies have summarized the results of randomized clinical trials (RCTs) assessing the efficacy of psychotherapeutic tools designed to treat patients at suicidal risk. However, observational studies, which reflect real-world effectiveness and may use original approaches, have not been reviewed.
Method: The aim of this study is to systematically review the available scientific evidence issued from observational studies on the clinical effectiveness of psychotherapeutic tools designed to treat patients at suicide risk. We have thus performed a systematic search of PubMed and Web of Science databases.
Results: Out of 1578 papers, 40 original observational studies fulfilled our selection criteria. The most used psychotherapeutic treatments were dialectical behavioral therapy (DBT, 27.5%) and cognitive behavioral therapy (CBT, 15.0%) in patients with a diagnosis of borderline personality disorder (32.5%) and depression (15.0%). Despite the between-study heterogeneity, interventions lead to a reduction in suicidal outcomes, i.e., suicidal ideation (55.0%) and suicide attempts (37.5%). The content and reporting quality varied considerably between the studies.
Conclusion: DBT and CBT are the most widely used psychotherapeutic interventions and show promising results in existing observational studies. Some of the included studies provide innovative approaches. Group therapies and internet-based therapies, which are cost-effective methods, are promising treatments and would need further study.
Suicide is a global public health problem causing about one million deaths every year according to the World Health Organization (World Health Organization, 2018). Although the most relevant risk and protective factors associated with suicidal behavior have been identified (Table 1), the global suicide rates have remained relatively stable in the last years.
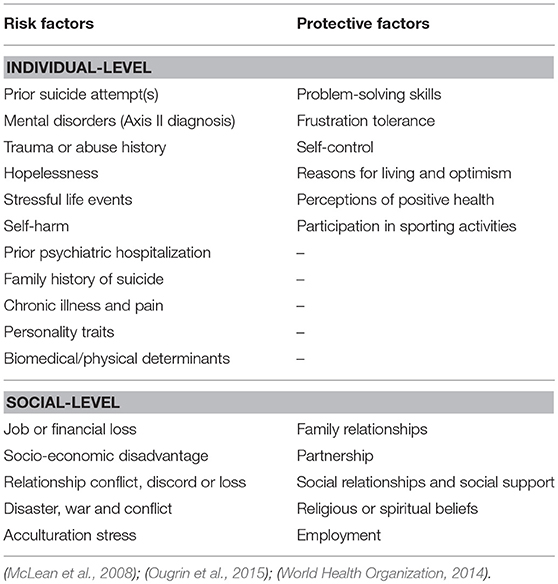
Table 1. Risk and protective factors associated with suicidal behavior.
One essential drawback for reducing suicide and suicide attempts is the lack of clear evidence on interventional programs directed to the population at risk (e.g., patient with suicide attempt history). Besides, knowledge about the efficacy of existing interventions is limited by the paucity of randomized clinical trials (RCTs) (Miller et al., 2017). Some interventions have shown to be efficacious, but the integration and dissemination of these programs in common clinical practice has proven to be an arduous task (Comtois and Linehan, 2006). The role of psychotherapy in suicide prevention is recognized but insufficient (Schneider, 2012). Current evidence supports especially the efficacy of Cognitive Behavioral Therapy (CBT) or Dialectical Behavioral Therapy (DBT), with a particular interest of problem-solving strategies (McMain et al., 2009; Rudge et al., 2017; Weinstein et al., 2017; Calati et al., 2018). Intensive outpatient support therapy, even if unspecific, is also a mainstay of suicide prevention guidelines (Mann et al., 2005; Zalsman et al., 2016). However, the evidence supporting these therapies and how to apply them is still scarce. Further research is needed to sustain existing results and design treatment plans contributing to a better treatment approach for the suicidal patient in different contexts, such as emergency room, primary care or inpatient units (Comtois and Linehan, 2006).
The creation of evidence-based guidelines for psychotherapy in suicide prevention is needed to improve the outcomes, especially in vulnerable groups presenting major social, psychiatric, or psychological risk factors (Valtonen et al., 2006; Rihmer, 2007; Fountoulakis et al., 2009; Rogers et al., 2018). Ideally, intervention strategies could follow a consensual methodology to ensure the coherence and comparability of results.
The aim of the current study is: (1) to systematically review observational studies exploring the effect of psychotherapeutic programs in the prevention of suicidal behaviors, (2) to describe the quality of this literature, (3) to identify innovative approaches, and (4) to propose recommendations for future observational research in this area. We planned to include only observational studies in order to assess literature that is not covered by recently published systematic reviews and meta-analyses (Sledge et al., 2014; Calati and Courtet, 2016; Hawton et al., 2016; Meerwijk et al., 2016; Krysinska et al., 2017; Leavey and Hawkins, 2017; Calati et al., 2018). Observational studies may help to assess the effectiveness of a psychotherapeutic strategy (Nallamothu et al., 2008), while RCTs are not necessarily representative of real-world situations because of their detailed inclusion and exclusion criteria (Faraoni and Schaefer, 2016). Thus, results from both RCTs (efficacy) and observational studies (effectiveness) provide valid evidence to improve clinical practice (Shadish et al., 2000; Berger et al., 2012).
A systematic review was performed to identify the available published data on psychotherapeutic strategies addressing suicidal behavior. A broad free text search was made using the terms (psychotherap* OR psychosoc* OR psychologic* OR acceptance and commitment therapy OR cognitive behavior* therapy OR cognitive therapy OR dialectical behavior therapy OR dialectical behavior therapy OR interpersonal psychotherapy OR mentalization based treatment OR mindfulness OR problem solving therapy OR schema-focused therapy OR transference-focused psychotherapy) AND (effectiveness OR efficac*) AND (suicid*) for PubMed and Web of Science. Potentially relevant papers in all languages until March 2018 were accessed to review full texts. Additional articles were obtained through citation tracking of reviews/opinion articles and original papers. The titles, abstracts, and studies identified in the literature search were assessed by two reviewers (PMB and FRR). All studies matching the inclusion criteria were reviewed by the authors and disagreements were settled through discussion.
In this review we included only observational studies in populations presenting suicidal ideation, suicide plans, or suicide attempts and informing about the effect of a psychotherapeutic approach, either individual or group therapy, in terms of suicidal outcomes. Concerning suicidal outcomes we referred to established nomenclature (Turecki and Brent, 2015). In particular, suicidal ideation refers to thoughts about taking action to end one's life, while suicide attempt is a self-inflicted potentially injurious behaviour with a non-fatal outcome and with the intention to die (De Leo et al., 2006). Only papers in English, French, Spanish or Portuguese were included. A flow diagram summarizing the selection process can be found in Figure 1.
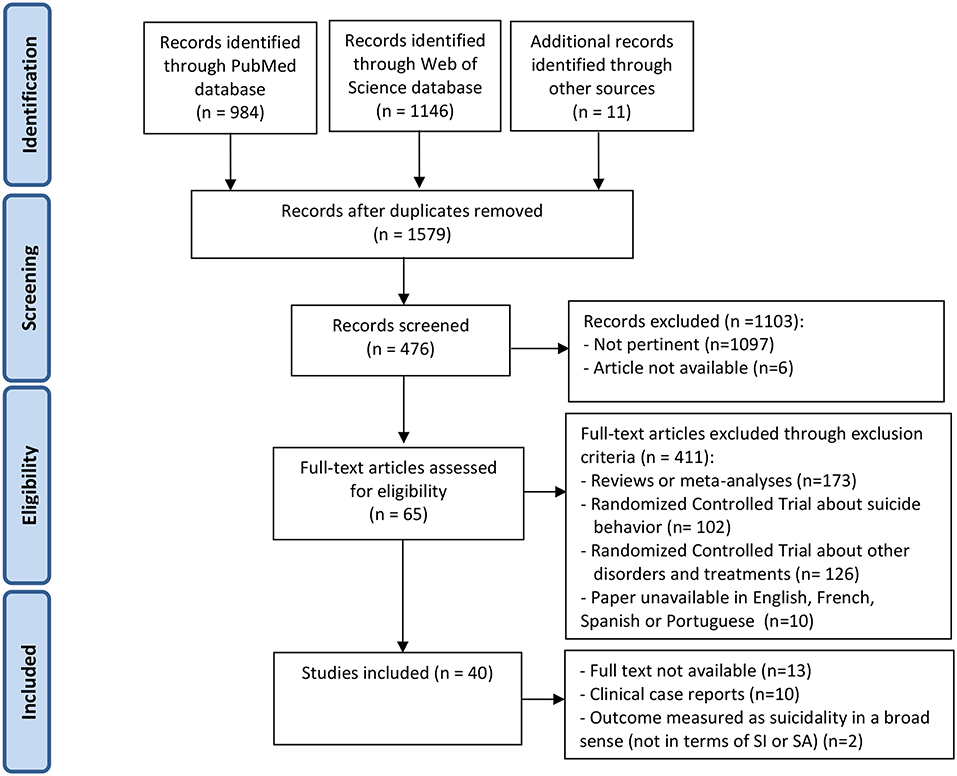
Figure 1. PRISMA flow diagram summarizing the systematic literature review and its results.
All articles that focused on deliberate self-harm or non-suicidal self-injury, as opposed to suicidal behavior, were excluded. Systematic reviews, meta-analyses, randomized controlled trials and reports of clinical case studies were also excluded.
One independent reviewer (FRR) supervised by a senior reviewer (PMB) extracted the relevant data using a predesigned data extraction form. Disagreement between the two reviewers was solved by referring to two additional reviewers (JLC and RC). From each selected original observational study, the following data was extracted: sample size, gender, mean age, psychiatric diagnoses, psychotherapeutic strategy, duration, number of weekly sessions, follow up after therapy, assessment scales, main results, and methodological quality rating.
We assessed the methodological quality of papers using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies created by the US National Heart, Lung, and Blood Institute (NHLBI) (NIH, 2018). This tool measures 14 different criteria which are then used to give each study an overall quality rating which is classified in good, fair, or poor. Two authors (PMB and FRR) applied this tool, they independently evaluated the items as “yes,” “no,” “not applicable,” “cannot determine” or “not reported.” This method was used to guide the quality rating of each study. In case of disagreement, consensus was reached through discussion. Based on previous articles (Koppen et al., 2016; Carbia et al., 2018) and our own assessment, we used the following threshold scores for the classification of the studies: good (>11), fair (6–9) and poor (<6).
A total of 40 papers were identified as meeting the inclusion criteria (Figure 1). A detailed description of the studies can be found in Tables 2, 3. Studies focused on suicidal ideation (n = 23, 57.5%) or suicide attempts (n = 17, 42.5%) in adult or adolescent samples. A large majority reported a decrease either in suicidal ideation (22/23) or suicide attempts (15/17).
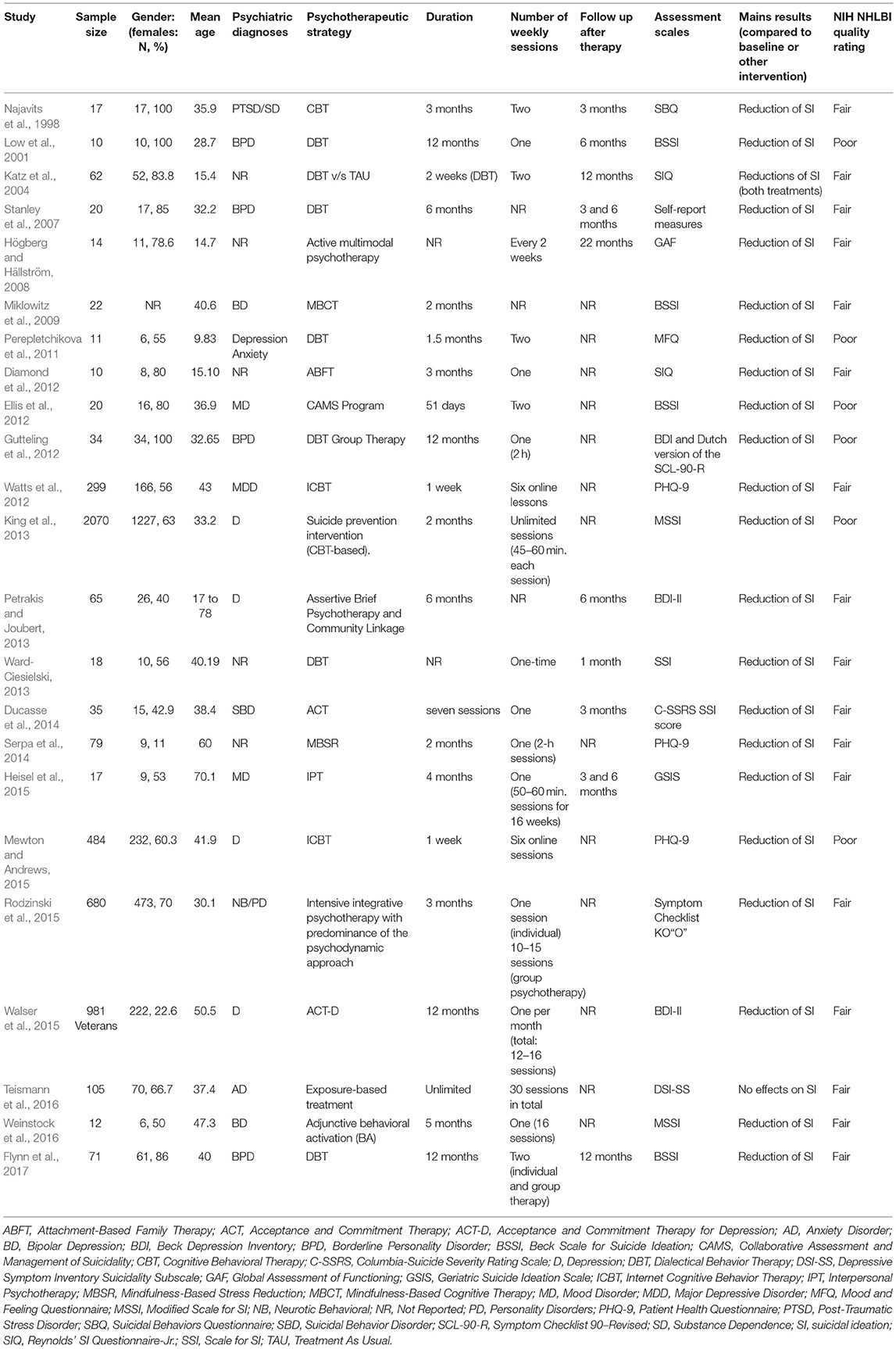
Table 2. Description of studies reporting the effects of psychotherapy on suicide ideation.
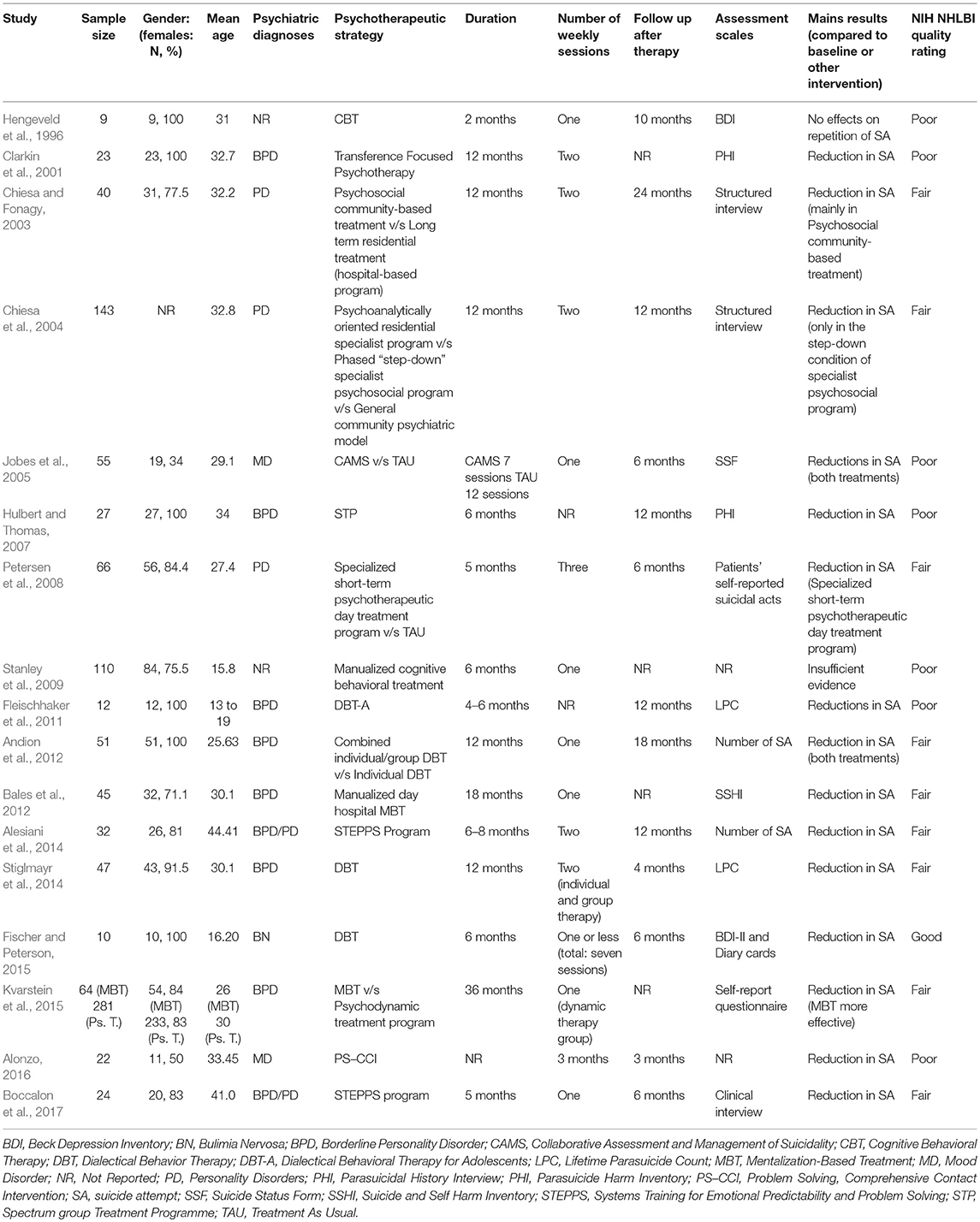
Table 3. Description of studies reporting the effects of psychotherapy on suicide attempts.
The most frequently reported interventions consisted on DBT or CBT. The remaining interventions used strategies based on miscellaneous approaches such as interpersonal psychotherapy, psychodynamic oriented therapy and family therapy.
The studies focused on patients with the following mental disorders: borderline personality disorder (n = 13, 32.5%), depression (n = 6, 15%), mood disorders (n = 4, 10%), and personality disorders (n = 3, 7.5%). Only the study by Ducasse et al. (2014) considered suicidal behavior disorder, the diagnostic category proposed in DSM-5 (American Psychiatric Association, 2013).
Psychotherapies were heterogeneous in terms of their intensity (duration of intervention, number of sessions). The duration varied between 1 and 2 weeks (n = 3, 7.5%), 2–3 months (n = 8, 20%), 4–8 months (n = 11, 27.5%), 12–18 months (n = 10, 25%), and one that extended over a period of 36 months (2.5%). Three studies (7.5%) did not report the duration. Most interventions planned one (n = 16, 40%) or two sessions per week (n = 10, 25%). Follow-up after therapy was reported in 57.5% of the studies. Follow-up length varied from 1 month (n = 1, 2.5%), 3–6 months (n = 12, 30%), 10–18 months (n = 8, 20%) and 2–3 years (n = 2, 5%). Many studies compared only assessments before and after therapy (n = 1 7, 42.5%).
Twenty-three studies were assessed. Results were positive overall, with a decrease of suicidal ideation rates in 95.7% of them. The most used psychotherapeutic treatments were DBT (n = 7, 30.4%) and CBT (n = 4, 17.4%). Interventions generally followed a weekly pattern (n = 12, 52.2%).
Two naturalistic interventions were focused on internet-based CBT to address suicidal ideation in depressed patients recruited by their primary care physician (Watts et al., 2012; Mewton and Andrews, 2015). The brief intervention consisted in six online sessions but the reported positive results, with a decrease in both suicidal ideation and depression levels from baseline, suggest the utility of this method in terms of cost and accessibility for the patients. Perepletchikova et al. (2011) applied an intensive version of DBT (2 weekly sessions during 6 weeks) to 11 children presenting mood symptoms and obtained good results: suicidal ideation and depressive symptoms decreased, while coping strategies improved. Heisel et al. (2015) performed a pilot study including 16 sessions of weekly interpersonal therapy for older adults. Compared to baseline assessments, suicidal ideation was lower at the end of the treatment and 6 months later. Petrakis and Joubert (2013) applied a brief assertive psychotherapy by social workers to 57 patients attending the emergency department. Patients, independently of their diagnosis, received a comprehensive evaluation, and linkage to community services was proactively encouraged to minimize drop-outs. In this program, psychosocial improvements were associated with a reduction in the level of depression and suicidal ideation, but the specifics of the therapy are not described. Another study by Högberg and Hällström (2008) used the active multimodal psychotherapy, an integrative approach combining different psychotherapeutic techniques in a case series of 14 suicidal adolescents. The approach comprised mood charting, psycho-education, well-being practice and trauma resolution (including eye movement desensitization and reprocessing).
Of note, two studies used exclusively group interventions and four combined both individual and group interventions. A very complete Irish program delivered individual and group DBT weekly sessions, as well as phone coaching and follow-up visits, for borderline personality disorder patients during 12 months (Flynn et al., 2017). Gutteling et al. (2012) also found that group DBT could be used to reduce suicidal ideation and depressive symptoms in borderline personality disorder. In general, group interventions were effective in reducing suicidal ideation and improving several other outcomes related to mental health.
Seventeen studies examined the effect of interventions in reducing subsequent suicide attempts. Most of them provided positive results (n = 15, 88.2%), frequently using DBT methods (n = 4, 23.5%) and weekly sessions (n = 8, 47.0%).
The Collaborative Assessment and Management of Suicidality (CAMS) was compared to treatment as usual (TAU) in a small sample of suicidal outpatients (Jobes et al., 2005). A reduction in suicidality (including any suicidal behavior or suicidal thought) was found in both groups at the end of treatment but CAMS achieved similar results in a significantly lower number of sessions. Interestingly, CAMS was also associated with decreased medical health care utilization 6 months after the treatment.
Some psychosocial programs combined social interventions and psychoanalytic therapy (individual and group-focused) to improve the social functioning of patients with personality disorders. These programs included a step-down period of limited duration offering biweekly therapy in small groups, meetings with community nurses and psychiatric consultations. Participants were also encouraged to create social bounds in the community, which was considered by the authors as particularly useful in reducing the risk of suicide attempts (Chiesa and Fonagy, 2003; Chiesa et al., 2004).
Another program, named Systems Training for Emotional Predictability and Problem Solving (STEPPS) and combining CBT elements and skills training with a systems component, was found to reduce suicide attempts in personality disorders patients (Alesiani et al., 2014; Boccalon et al., 2017). STEPPS was also associated with better emotional regulation, fewer hospitalizations and suicide attempts 6 months after the end of the treatment (Boccalon et al., 2017). Finally, the delivery of a manualized problem-solving and comprehensive contact intervention (PS-CCI) to mood-disordered patients found a decrease in both suicidal ideation and suicide attempts 3 months later (Alonzo, 2016). The intervention was delivered in emergency settings and included an educative interview about problem-solving, the sending of a personalized postcard and a telephone call 3 months later.
The large majority of the studies (n = 26) was qualified as “fair” at the quality assessment. Only one was scored “good” while 13 studies were considered “poor.” The most common caveats were the lack of sample size justification, not describing precisely the features of participants, showing weaknesses in the statistical methodology and making only pre- and post-test evaluations (with no further assessment).
Clinical decision-making regarding patients with suicidal risk is largely based on the experience of health care providers, rather than international guidelines. Suicidal patients are heterogeneous, and frequently non-adherent to treatment or follow-up. Since this variability is unlikely to be reflected in RCTs, we have tried to synthesize data from observational studies to complete the results of previous reviews and meta-analyses. The results seem to confirm the effectiveness of psychotherapeutic interventions for the management and reduction of suicidal risk. However, there is a lack of methodological consensus on how to apply these interventions, which limits the generalizability of the findings. In this domain, many observational studies, similarly to RCTs (Witt et al., 2018), do not offer detailed information about the components of psychotherapeutic interventions, such as the number of sessions, their frequency, the duration of follow-up, or the clinical features of the sample. Of note, some strategies, such as internet-based therapies, group therapy or community settings for the treatment, might prove particularly cost-effective.
According to our results, CBT and DBT appear to be the most used and effective psychotherapeutic interventions for patients presenting suicidal ideation or suicide attempts, even in the short-term. For instance, 1-week internet-based CBT (Watts et al., 2012; Mewton and Andrews, 2015) and a short 2-month CBT program to reduce suicide risk in primary care patients (King et al., 2013) were both effective in reducing suicidal ideation. Another short-term intervention (seven sessions) addressing suicidal behavior disorder with Acceptance and Commitment Therapy showed a decrease in both the frequency and intensity of suicidal ideation (Ducasse et al., 2014). Of note, no other study focused on the diagnostic category of suicidal behavior disorder, which is associated with the risk of attempting suicide in the short-term. To consider suicidal behavior as a trans-diagnostic entity could help to more accurately evaluate the effect of psychotherapeutic interventions.
However, the range of potential psychotherapeutic interventions for suicide prevention is not limited to CBT and DBT. Mindfulness-based strategies, integrative programs, CAMS, STEPPS, or PS-CCI, just to mention some, are promising possibilities. Besides, most studies were conducted in adults, but some interventions have shown promising results in extreme ages, such as DBT adapted for children (Perepletchikova et al., 2011) and interpersonal therapy for older adults (Heisel et al., 2015).
Luoma et al. (2002) found that ~45% of suicide victims had contact with primary care in the month prior to their death and 77% in the year before suicide. Since so far the evidence sustaining targeted psychotherapeutic interventions for patients at suicide risk is still scarce, a research effort to establish effective interventions is needed. Some interventions need to be tested in independent and larger samples to verify their utility before translation into common clinical practice could be considered (Glenn et al., 2015). Group CBT for the prevention of repeated suicide attempts is currently being compared to individual supportive therapy by our team in a multicenter randomized clinical trial (clinicaltrials.gov registration: NCT02664701). Indeed, the setting of the therapy (individual vs. group) does not appear to predict the outcome for several mental disorders (Pomini, 2004) and the group setting provides important pragmatic advantages, such as a more efficient use of human resources dedicated to patient care and subsequent cost savings.
According to the quality assessment, reviewed studies present frequent weaknesses at the methodological level. These deficits comprise mainly a restricted evaluation of the sample, a vague description of the intervention, the non-justification of the sample size, the lack of a blinded outcome assessment, and a limited time frame to examine the association between exposure and outcome. In addition, adjustment for relevant confounders, such as educational level, depression severity, or the concomitant use of psychotropic treatment, was not considered in the majority of the studies. A reassessment several weeks or months after the end of the psychotherapy is also needed to ascertain the duration of the effect. Importantly, the cost-effectiveness of psychotherapeutic programs, such as short programs and group psychotherapy, could be compared to pharmacological approaches or non-specific support therapy. Our review uncovers a high heterogeneity in type and intensity of psychotherapeutic programs to reduce suicidal behavior. A quite wide range of psychotherapeutic strategies may be efficacious to prevent suicidal behavior but the benefits of their application in real clinical conditions (effectiveness) is not yet clear. We also need to differentiate the specific effect of psychotherapy from the non-specific effect of any treatment implying intensive contact and follow-up with a physician, such as supportive therapy provided by a general practitioner. Stronger evidence regarding the specific aspects of psychotherapy that reduce the suicide risk is thus needed.
Both RCTs and observational studies provide relevant information for the interpretation of the efficacy and effectiveness of therapeutic strategies applied to different populations. Future observational studies in this area should provide precise measurements of the exposure, as well as a detailed description of the components of psychotherapeutic interventions and the outcome variables of interest. Additional recommendations include a consensual terminology, notifying patients of the potential risks of therapies during the informed consent process, and clear procedures for monitoring and reporting side effects (Guidi et al., 2018; Rozental et al., 2018).
In summary, further research is still needed to discern how to improve psychotherapeutic strategies in suicide prevention. Replication by independent groups of successful programs is particularly important to ensure generalizability of the findings (Miklowitz and Taylor, 2006; Glenn et al., 2015; Zalsman et al., 2016). Psychotherapeutic interventions seem to have a positive effect in patients with suicidal ideation and suicide attempts, but it is not yet possible to identify the most effective/efficacious psychotherapeutic approach. This is partly due to the very high number of interconnected factors that should be assessed, i.e., patient-clinician-treatment related factors. Artificial intelligence could be one further promising tool to answer to this complex question.
PM-B, JL-C, and RC conceived and designed the study and drafted the manuscript. PM-B and FR-R managed the literature searches and analyses. All authors revised the article critically and read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This study was supported by Fondo Nacional de Desarrollo Científico y Tecnológico (Fondecyt) del Gobierno de Chile (FONDECYT N°11170342).
Alesiani, R., Boccalon, S., Giarolli, L., Blum, N., and Fossati, A. (2014). Systems Training for Emotional Predictability and Problem Solving (STEPPS): program efficacy and personality features as predictors of drop-out - an Italian study. Compr. Psychiatry 55, 920–927. doi: 10.1016/j.comppsych.2014.01.003
Alonzo, D. (2016). Suicidal individuals and mental health treatment: a novel approach to engagement. Community Ment. Health J. 52, 527–533. doi: 10.1007/s10597-015-9980-3
American Psychiatric Association (2013). The Diagnostic and Statistical Manual of Mental Disorders, DSM-5. Washington, DC: American Psychiatric Association.
Andion, O., Ferrer, M., Matali, J., Gancedo, B., Calvo, N., Barral, C., et al. (2012). Effectiveness of combined individual and group dialectical behavior therapy compared to only individual dialectical behavior therapy: a preliminary study. Psychotherapy 49, 241–250. doi: 10.1037/a0027401
Bales, D., van Beek, N., Smits, M., Willemsen, S., Busschbach, J. J., Verheul, R., et al. (2012). Treatment outcome of 18-month, day hospital mentalization-based treatment (MBT) in patients with severe borderline personality disorder in the Netherlands. J. Pers. Disord. 26, 568–582. doi: 10.1521/pedi.2012.26.4.568
Berger, M. L., Dreyer, N., Anderson, F., Towse, A., Sedrakyan, A., and Normand, S. L. (2012). Prospective observational studies to assess comparative effectiveness: the ISPOR good research practices task force report. Value Health 15, 217–230. doi: 10.1016/j.jval.2011.12.010
Boccalon, S., Alesiani, R., Giarolli, L., and Fossati, A. (2017). Systems training for emotional predictability and problem solving program and emotion dysregulation: a pilot study. J. Nerv. Ment. Dis. 205, 213–216. doi: 10.1097/NMD.0000000000000640
Calati, R., and Courtet, P. (2016). Is psychotherapy effective for reducing suicide attempt and non-suicidal self-injury rates? Meta-analysis and meta-regression of literature data. J Psychiatr Res. 79, 8–20. doi: 10.1016/j.jpsychires.2016.04.003
Calati, R., Courtet, P., and Lopez-Castroman, J. (2018). Refining suicide prevention: a narrative review on advances in psychotherapetic tools. Curr. Psychiatry Rep. 20:14. doi: 10.1007/s11920-018-0876-0
Carbia, C., López-Caneda, E., Corral, M., and Cadaveira, F. (2018). A systematic review of neuropsychological studies involving young binge drinkers. Neurosci. Biobehav. Rev. 90, 332–349. doi: 10.1016/j.neubiorev.2018.04.013
Chiesa, M., and Fonagy, P. (2003). Psychosocial treatment for severe personality disorder - 36-month follow-up. Br. J. Psychiatry 183, 356–362. doi: 10.1192/bjp.183.4.356
Chiesa, M., Fonagy, P., Holmes, J., and Drahorad, C. (2004). Residential versus community treatment of personality disorders: a comparative study of three treatment programs. Am. J. Psychiatry 161,1463–1470. doi: 10.1176/appi.ajp.161.8.1463
Clarkin, J. F., Foelsch, P. A., Levy, K. N., Hull, J. W., Delaney, J. C., and Kernberg, O. F. (2001). The development of a psychodynamic treatment for patients with Borderline Personality Disorder: a preliminary study of behavioral change. J. Pers. Disord. 15, 487–495. doi: 10.1521/pedi.15.6.487.19190
Comtois, K. A., and Linehan, M. M. (2006). Psychosocial treatments of suicidal behaviors: a practice-friendly review. J. Clin. Psychol. 62, 161–170. doi: 10.1002/jclp.20220
De Leo, D., Burgis, S., Bertolote, J. M., Kerkhof, A. J. F. M., and Bille-Brahe, U. (2006). Definitions of suicidal behavior lessons learned from the WHO/EURO multicentre study. Crisis 27, 4–15. doi: 10.1027/0227-5910.27.1.4
Diamond, G. M., Diamond, G. S., Levy, S., Closs, C., Ladipo, T., and Siqueland, L. (2012). Attachment-based family therapy for suicidal lesbian, gay, and bisexual adolescents: a treatment development study and open trial with preliminary findings. Psychotherapy 49,62–71. doi: 10.1037/a0026247
Ducasse, D., Rene, E., Beziat, S., Guillaume, S., Courtet, P., and Olie, E. (2014). Acceptance and commitment therapy for management of suicidal patients: a pilot study. Psychother. Psychosom. 83, 374–376. doi: 10.1159/000365974
Ellis, T. E., Green, K. L., Allen, J. G., Jobes, D. A., and Nadorff, M. R. (2012). Collaborative assessment and management of suicidality in an inpatient setting: results of a pilot study. Psychotherapy 49, 72–80. doi: 10.1037/a0026746
Faraoni, D., and Schaefer, S. T. (2016). Randomized controlled trials vs. observational studies: why not just live together? BMC Anesthesiol. 16, 102. doi: 10.1186/s12871-016-0265-3
Fischer, S., and Peterson, C. (2015). Dialectical behavior therapy for adolescent binge eating, purging, suicidal behavior, and non-suicidal self-injury: a pilot study. Psychotherapy 52, 78–92. doi: 10.1037/a0036065
Fleischhaker, C., Bohme, R., Sixt, B., Bruck, C., Schneider, C., and Schulz, E. (2011). Dialectical Behavioral Therapy for Adolescents (DBT-A): a clinical trial for patients with suicidal and self-injurious Behavior and Borderline Symptoms with a one-year Follow-up. Child Adolesc. Psychiatry Ment. Health 5:3. doi: 10.1186/1753-2000-5-3
Flynn, D., Kells, M., Joyce, M., Corcoran, P., Gillespie, C., Suarez, C., et al. (2017). Standard 12 month dialectical behaviour therapy for adults with borderline personality disorder in a public community mental health setting. Borderline Pers. Disord Emot Dysregul. 4:19. doi: 10.1186/s40479-017-0070-8
Fountoulakis, K. N., Gonda, X., Siamouli, M., and Rihmer, Z. (2009). Psychotherapeutic intervention and suicide risk reduction in bipolar disorder: a review of the evidence. J. Affect. Disord. 113, 21–29. doi: 10.1016/j.jad.2008.06.014
Glenn, C. R., Franklin, J. C., and Nock, M. K. (2015). Evidence-based psychosocial treatments for self-injurious thoughts and behaviors in youth. J. Clin. Child Adolesc. Psychol. 44, 1–29. doi: 10.1080/15374416.2014.945211
Guidi, J., Brakemeier, E. L., Bockting, C. L. H., Cosci, F., Cuijpers, P., Jarrett, R. B., et al. (2018). Methodological recommendations for trials of psychological Interventions. Psychother Psychosom. 87, 276–284. doi: 10.1159/000490574
Gutteling, B. M., Montagne, B., Nijs, M., and van den Bosch, L. M. (2012). Dialectical behavior therapy: is outpatient group psychotherapy an effective alternative to individual psychotherapy? Preliminary conclusions. Compr Psychiatry 53, 1161–1168. doi: 10.1016/j.comppsych.2012.03.017
Hawton, K., Witt, K. G., Taylor Salisbury, T. L., Arensman, E., Gunnell, D., Hazell, P., et al. (2016). Psychosocial interventions for self-harm in adults. Cochrane Database Syst Rev. 5:CD012189. doi: 10.1002/14651858.CD012189
Heisel, M. J., Talbot, N. L., King, D. A., Tu, X. M., and Duberstein, P. R. (2015). Adapting interpersonal psychotherapy for older adults at risk for suicide. Am. J. Geriatr. Psychiatry 23, 87–98. doi: 10.1016/j.jagp.2014.03.010
Hengeveld, M. W., Jonker, D. J., and Rooijmans, H. G. (1996). A pilot study of a short cognitive-behavioral group treatment for female recurrent suicide attempters. Int. J. Psychiatry Med. 26, 83–91. doi: 10.2190/1q2g-gn44-fata-tt4j
Högberg, G., and Hällström, T. (2008). Active multimodal psychotherapy in children and adolescents with suicidality: description, evaluation and clinical profile. Clin. Child Psychol. Psychiatry 13, 435–448. doi: 10.1177/1359104507088348
Hulbert, C., and Thomas, R. (2007). Public sector group treatment for severe personality disorder: a 12-month follow-up study. Australas. Psychiatry 15, 226–231. doi: 10.1080/10398560701317101
Jobes, D. A., Wong, S. A., Conrad, A. K., Drozd, J. F., and Neal-Walden, T. (2005). The collaborative assessment and management of suicidality versus treatment as usual: a retrospective study with suicidal outpatients. Suicide Life Threat. Behav. 35, 483–497. doi: 10.1521/suli.2005.35.5.483
Katz, L. Y., Cox, B. J., Gunasekara, S., and Miller, A. L. (2004). Feasibility of dialectical behavior therapy for suicidal adolescent inpatients. J. Am. Acad. Child Adolesc. Psychiatry 43, 276–282. doi: 10.1097/00004583-200403000-00008
King, K., Bassilios, B., Reifels, L., Fletcher, J., Ftanou, M., Blashki, G., et al. (2013). Suicide prevention: evaluation of a pilot intervention in a primary care context. J. Ment. Health 22, 439–448. doi: 10.3109/09638237.2013.815334
Koppen, I. J. N., Kuizenga-Wessel, S., Saps, M., Di Lorenzo, C., Benninga, M. A., Faridi, S., et al. (2016). Functional defecation disorders and excessive body weight: a systematic review. Pediatrics 138:e20161417. doi: 10.1542/peds.2016-1417
Krysinska, K., Batterham, P. J., and Christensen, H. (2017). Differences in the effectiveness of psychosocial interventions for suicidal ideation and behaviour in women and men: a systematic review of randomized controlled trials. Arch. Suicide Res. 21, 12–32. doi: 10.1080/13811118.2016.1162246
Kvarstein, E. H., Pedersen, G., Urnes, O., Hummelen, B., Wilberg, T., and Karterud, S. (2015). Changing from a traditional psychodynamic treatment programme to mentalization-based treatment for patients with borderline personality disorder - Does it make a difference? Psychol. Psychother.Theory Res. Pract. 88, 71–86. doi: 10.1111/papt.12036
Leavey, K., and Hawkins, R. (2017). Is cognitive behavioural therapy effective in reducing suicidal ideation and behaviour when delivered face-toface or via e-health? A systematic review and meta-analysis. Cogn. Behav. Ther. 46, 353–374. doi: 10.1080/16506073.2017.1332095
Low, G., Jones, D., Duggan, C., Power, M., and MacLeod, A. (2001). The treatment of deliberate self-harm in borderline personality disorder using dialectical behaviour therapy: a pilot study in a high security hospital. Behav. Cogn. Psychother. 29, 85–92. doi: 10.1017/S1352465801001096
Luoma, J. B., Martin, C. E., and Pearson, J. L. (2002). Contact with mental health and primary care providers before suicide: a review of the evidence. Am. J. Psychiatry 159, 909–916. doi: 10.1176/appi.ajp.159.6.909
Mann, J. J., Apter, A., Bertolote, J., Beautrais, A., Currier, D., Haas, A., et al. (2005). Suicide prevention strategies: a systematic review. JAMA, 294, 2064–2074. doi: 10.1001/jama.294.16.2064
McLean, J., Maxwell, M., Platt, S., Harris, F., and Jepson, R. (2008). Risk and Protective Factors for Suicide and Suicidal Behaviour: A Literature Review. Edinborough: Scottish Government Social Research.
McMain, S. F., Links, P. S., Gnam, W. H., Guimond, T., Cardish, R. J., Korman, L., et al. (2009). A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. Am J Psychiatry 166, 1365–1374. doi: 10.1176/appi.ajp.2009.09010039
Meerwijk, E. L., Parekh, A., Oquendo, M. A., Allen, I. E., Franck, L. S., and Lee, K. A. (2016). Direct versus indirect psychosocial and behavioural interventions to prevent suicide and suicide attempts: a systematic review and meta-analysis. Lancet Psychiatry 3, 544–554. doi: 10.1016/S2215-0366(16)00064-X
Mewton, L., and Andrews, G. (2015). Cognitive behaviour therapy via the internet for depression: a useful strategy to reduce suicidal ideation. J. Affect. Disord. 170, 78–84. doi: 10.1016/j.jad.2014.08.038
Miklowitz, D. J., Alatiq, Y., Goodwin, G. M., Geddes, J. R., Fennell, M. J. V., Dimidjian, S., et al. (2009). A pilot study of mindfulness-based cognitive therapy for bipolar disorder. Int. J. Cogn. Ther. 2, 373–382. doi: 10.1521/ijct.2009.2.4.373
Miklowitz, D. J., and Taylor, D. O. (2006). Family-focused treatment of the suicidal bipolar patient. Bipolar Disord. 8, 640–651. doi: 10.1111/j.1399-5618.2006.00320.x
Miller, I. W., Camargo, C. A. Jr, Arias, S. A., Sullivan, A. F., Allen, M. H., Goldstein, A. B., et al. (2017). Suicide prevention in an emergency department population: the ED-SAFE study. JAMA Psychiatry 74, 563–570. doi: 10.1001/jamapsychiatry.2017.0678
Najavits, L. M., Weiss, R. D., Shaw, S. R., and Muenz, L. R. (1998). “Seeking safety”: outcome of a new cognitive-behavioral psychotherapy for women with posttraumatic stress disorder and substance dependence. J. Trauma. Stress 11, 437–456.
Nallamothu, B. K., Hayward, R. A., and Bates, E. R. (2008). Beyond the randomized clinical trial: the role of effectiveness studies in evaluating cardiovascular therapies. Circulation 118, 1294–1303. doi: 10.1161/CIRCULATIONAHA.107.703579
NIH (2018). Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (Accessed November 7, 2018).
Ougrin, D., Tranah, T., Stahl, D., Moran, P., and Rosenbaum, J. (2015). Therapeutic interventions for suicide attempts and self-harm in adolescents: systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 54, 97–107.e2. doi: 10.1016/j.jaac.2014.10.009
Perepletchikova, F., Axelrod, S. R., Kaufman, J., Rounsaville, B. J., Douglas-Palumberi, H., and Miller, A. L. (2011). Adapting dialectical behaviour therapy for children: towards a new research agenda for paediatric suicidal and non-suicidal self-injurious behaviours. Child Adolesc. Mental Health 16, 116–121. doi: 10.1111/j.1475-3588.2010.00583.x
Petersen, B., Toft, J., Christensen, N. B., Foldager, L., Munk-Jörgensen, P., Lien, K., et al. (2008). Outcome of a psychotherapeutic programme for patients with severe personality disorders. Nord. J. Psychiatry 62, 450–456. doi: 10.1080/08039480801984271
Petrakis, M., and Joubert, L. (2013). A social work contribution to suicide prevention through assertive brief psychotherapy and community linkage: use of the Manchester Short Assessment of Quality of Life (MANSA). Soc. Work Health Care 52, 239–257. doi: 10.1080/00981389.2012.737903
Pomini, V. (2004). Les thérapies cognitivo-comportementales de groupe dans le traitement des troubles anxieux ont-elles un avantage sur les traitements individuels? Santé Ment. Québec 29, 115–126. doi: 10.7202/008825ar
Rihmer, Z. (2007). Suicide risk in mood disorders. Curr. Opin. Psychiatry 20, 17–22. doi: 10.1097/YCO.0b013e3280106868
Rodzinski, P., Sobanski, J. A., Rutkowski, K., Cyranka, K., Murzyn, A., Dembinska, E., et al. (2015). Effectiveness of therapy in terms of reduction of intensity and elimination of suicidal ideation in day hospital for the treatment of neurotic and behavioral disorders. Psychiatr. Pol. 49, 489–502. doi: 10.12740/PP/29837
Rogers, A. H., Short, N. A., Robles, Z., Bakhshaie, J., Viana, A., Schmidt, N. B., et al. (2018). Identifying the rol of sociodemographuc factors in major depressive disorder and suicidality among Spanish-speaking Latino patients in a federally qualified health center. Cogn. Behav. Ther. 6, 1–15. doi: 10.1080/16506073.2018.1445123
Rozental, A., Bennett, S., Forsstr?m, D., Ebert, D. D., Shafran, R., Andersson, G., et al. (2018). Targeting procrastination using psychological treatments: a systematic review and meta-analysis. Front. Psychol. 9:1588. doi: 10.3389/fpsyg.2018.01588
Rudge, S., Feigenbaum, J. D., and Fonagy, P. (2017). Mechanisms of change in dialectical behaviour therapy and cognitive behaviour therapy for borderline personality disorder: a critical review of the literature. J. Ment. Health doi: 10.1080/09638237.2017.1322185. [Epub ahead of print].
Schneider, B. (2012). Behavioural therapy of suicidality. Eur. Arch. Psychiatry Clin. Neurosci. 262(Suppl. 2), 123–128. doi: 10.1007/s00406-012-0351-6
Serpa, J. G., Taylor, S. L., and Tillisch, K. (2014). Mindfulness-based stress reduction (MBSR) reduces anxiety, depression, and suicidal ideation in veterans. Med. Care 52, S19–S24. doi: 10.1097/MLR.0000000000000202
Shadish, W. R., Navarro, A. M., Matt, G. E., and Phillips, G. (2000). The effects of psychological therapies under clinically representative conditions: a meta-analysis. Psychol. Bull. 126, 512–529. doi: 10.1037/0033-2909.126.4.512
Sledge, W., Plakun, E. M., Bauer, S., Brodsky, B., Caligor, E., Clemens, N. A., et al. (2014). Psychotherapy for suicidal patients with borderline personality disorder: an expert consensus review of common factors across five therapies. Borderline Pers. Disord. Emot. Dysregul. 1:16. doi: 10.1186/2051-6673-1-16
Stanley, B., Brodsky, B., Nelson, J. D., and Dulit, R. (2007). Brief Dialectical Behavior Therapy (DBT-B) for suicidal behavior and non-suicidal self-injury. Arch. Suicide Res. 11, 337–341. doi: 10.1080/13811110701542069
Stanley, B., Brown, G., Brent, D., Wells, K., Poling, K., Curry, J., et al. (2009). Cognitive Behavior Therapy for Suicide Prevention (CBT-SP): treatment model, feasibility and acceptability. J. Am. Acad. Child Adolesc. Psychiatry 48, 1005–1013. doi: 10.1097/CHI.0b013e3181b5dbfe
Stiglmayr, C., Stecher-Mohr, J., Wagner, T., Meiβner, J., Spretz, D., Steffens, C., et al. (2014). Effectiveness of dialectic behavioral therapy in routine outpatient care: the Berlin Borderline Study. Borderline Pers. Disord. Emot. Dysregul. 1:20. doi: 10.1186/2051-6673-1-20
Teismann, T., Forkmann, T., Rath, D., Glaesmer, H., and Margraf, J. (2016). Perceived burdensomeness and suicidal ideation in adult outpatients receiving exposure therapy for anxiety disorders. Behav. Res. Ther. 85, 1–5. doi: 10.1016/j.brat.2016.07.011
Turecki, G., and Brent, D. A. (2015). Suicide and suicidal behaviour. Lancet 387, 1227–1239. doi: 10.1016/S0140-6736(15)00234-2
Valtonen, H. M., Suominen, K., Mantere, O., Leppamaki, S., Arvilommi, P., and Isometsa, E. T. (2006). Prospective study of risk factors for attempted suicide among patients with bipolar disorder. Bipolar Disord. 8(5 Pt 2), 576–585. doi: 10.1111/j.1399-5618.2006.00341.x
Walser, R. D., Garvert, D. W., Karlin, B. E., Trockel, M., Ryu, D. M., and Taylot, C. B. (2015). Effectiveness of acceptance and commitment therapy in treating depression and suicidal ideation in veterans. Behav. Res. Ther. 74, 25–31. doi: 10.1016/j.brat.2015.08.012
Ward-Ciesielski, E. F. (2013). An Open Pilot Feasibility study of a brief dialectical behavior therapy skills–based intervention for suicidal individuals. Suicide Life Threat. Behav. 43, 324–335. doi: 10.1111/sltb.12019
Watts, S., Newby, J. M., Mewton, L., and Andrews, G. (2012). A clinical audit of changes in suicide ideas with internet treatment for depression. BMJ Open 2:e001558. doi: 10.1136/bmjopen-2012-001558
Weinstein, S. M., Cruz, R. A., Isaia, A. R., Peters, A. T., and West, A. E. (2017). Child- and family-focused cognitive behavioral therapy for pediatric bipolar disorder: applications for suicide prevention. Suicide Life Threat Behav. doi: 10.1111/sltb.12416
Weinstock, L. M., Melvin, C., Munroe, M. K., and Miller, I. W. (2016). Adjunctive behavioral activation for the treatment of bipolar depression: a proof of concept trial. J. Psychiatr. Pract. 22, 149–158. doi: 10.1097/PRA.0000000000000142
Witt, K., Pache de Moraes, D., Taylor, T., Arensman, E., Gunnell, D., Hazel, P., et al. (2018). Treatment as usual (TAU) as a control condition in trials of cognitive behavioural-based psychotherapy for self-harm: impact of content and quality on outcomes in a systematic review. J. Affect. Disord. 235, 434–447. doi: 10.1016/j.jad.2018.04.025
World Health Organization (2014). Preventing Suicide: A Global Imperative. Available online at: http://www.who.int/mental_health/suicide-prevention/world_report_2014/en (Accessed November 3, 2018).
World Health Organization (2018). WHO Suicide Data. Available online at: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/. (Accessed February 15, 2018).
Keywords: effectiveness, psychotherapy, suicide attempt (SA), suicidal ideation (SI), systematic review
Citation: Méndez-Bustos P, Calati R, Rubio-Ramírez F, Olié E, Courtet P and Lopez-Castroman J (2019) Effectiveness of Psychotherapy on Suicidal Risk: A Systematic Review of Observational Studies. Front. Psychol. 10:277. doi: 10.3389/fpsyg.2019.00277
Received: 10 June 2018; Accepted: 28 January 2019;
Published: 19 February 2019.
Edited by:
Sayyed Mohsen Fatemi, Harvard University, United StatesReviewed by:
Domenico De Berardis, Azienda Usl Teramo, ItalyCopyright © 2019 Méndez-Bustos, Calati, Rubio-Ramírez, Olié, Courtet and Lopez-Castroman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Méndez-Bustos, cC5tZW5kZXpiQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.