
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Psychol. , 20 December 2018
Sec. Human-Media Interaction
Volume 9 - 2018 | https://doi.org/10.3389/fpsyg.2018.02508
This article is part of the Research Topic Assessing the Therapeutic Uses and Effectiveness of Virtual Reality, Augmented Reality and Video Games for Emotion Regulation and Stress Management View all 11 articles
 Barbara Atzori1*
Barbara Atzori1* Hunter G. Hoffman2*
Hunter G. Hoffman2* Laura Vagnoli3
Laura Vagnoli3 David R. Patterson4Wadee Alhalabi5,6Andrea Messeri7
David R. Patterson4Wadee Alhalabi5,6Andrea Messeri7 Rosapia Lauro Grotto1,8
Rosapia Lauro Grotto1,8Background: Venipuncture is described by children as one of the most painful and frightening medical procedures.
Objective: To evaluate the effectiveness of Virtual Reality (VR) as a distraction technique to help control pain in children and adolescents undergoing venipuncture.
Methods: Using a within-subjects design, fifteen patients (mean age 10.92, SD = 2.64) suffering from oncological or hematological diseases received one venipuncture with “No VR” and one venipuncture with “Yes VR” on two separate days (treatment order randomized). “Time spent thinking about pain”, “Pain Unpleasantness”, “Worst pain” the quality of VR experience, fun during the venipuncture and nausea were measured.
Results: During VR, patients reported significant reductions in “Time spent thinking about pain,” “Pain unpleasantness,” and “Worst pain”. Patients also reported significantly more fun during VR, and reported a “Strong sense of going inside the computer-generated world” during VR. No side effects were reported.
Conclusion: VR can be considered an effective distraction technique for children and adolescents’ pain management during venipuncture. Moreover, VR may elicit positive emotions, more than traditional distraction techniques. This could help patients cope with venipuncture in a non-stressful manner. Additional research and development is needed.
For many children, venipuncture is one of the most frightening aspects of visiting a hospital (Duff, 2003; Caprilli and Messeri, 2006). Experiencing pain and anxiety during medical procedures can result in several negative consequences, such as higher levels of fear. Unpleasant early medical experiences can affect patients’ perception of healthcare, can increase pain and suffering during subsequent medical visits, and can reduce preventative healthcare, affecting lifelong health (El-Housseiny et al., 2014). Developing expectations of pain (e.g., via memories for previous painful medical procedure experiences, Noel et al., 2015) can increase how much pain patientsexperience during a procedure, via top-down amplification of neural signals coming into the brain from the pain receptors (Fields, 2018). For patients with chronic diseases, venipuncture can be particularly painful and stressful (Bisogni et al., 2014). Adequate pain management is especially important for patients who receive multiple venipunctures. Indeed, untreated pain can have damaging effects on future pain perceptions and can provoke negative psychological effects (Weisman et al., 1998) and a simple procedure, such as venipuncture, could represent an additional stressor in an already critical condition.
Traditional distraction techniques (e.g., reading books or listening to music) are some of the most common psychological strategies for the reduction of procedural pain and anticipatory anxiety during venipuncture (Birnie et al., 2018).
Birnie et al. (2018) conducted a Cochrane Review of Psychological interventions for needle-related procedural pain and distress in children and adolescents (5550 participants). The studies evaluated in Birnie et al’s (2018) review included venipuncture, intravenous insertion, and vaccine injections in patients aged two to 19 years. The most common psychological interventions were distraction (n = 32 studies) and only two VR distraction studies were included in Birnie et al’s Cochrane review.
Virtual Reality (VR) is showing promise as an innovative distraction technique for pain management among children undergoing medical procedures (Hoffman, 1998; Hoffman et al., 2000a; Bailey and Bailenson, 2017; Atzori et al., 2018b,c). VR reduces the cognitive component of pain (time spent thinking about pain), but also reduces the affective component (pain unpleasantness) and the sensory component (worst pain), as consistently shown in studies with adult and pediatric participants with burn injuries (Hoffman, 1998; Hoffman et al., 2000a,b, 2011; Atzori et al., 2018a; Soltani et al., 2018). Unlike traditional distractions, VR allows the user to be immersed in a computer-generated environment, wearing a Head Mounted Display (HMD), or similar goggles, that occlude the patient’s view of the hospital treatment room and blocks sounds of the real environment (Hoffman, 2004). The user can also interact with the VR environment, if the software allows it (Hoffman et al., 2006; Won et al., 2017). Although the mechanism(s) of how VR reduces pain are still under investigation, Hoffman and colleagues applied the Eccleston and Crombez (1999) Attention Pain Theory to explain how VR can reduce the perception of pain. Attention is required to feel pain, but the illusion of being in a virtual environment and the patients’ interaction with the objects in the virtual world reduce the amount of attentional resources the patient’s brain has available to attend to the painful stimulus, thus reducing conscious pain perception (Hoffman et al., 2004a). Much of VR’s therapeutic power is derived from its ability to divert attention away from painful medical interventions. Moreover, in addition to reducing pain, patients report having fun during burn wound care when playing VR (Hoffman et al., 2004b). The immersiveness of the VR systems, such as the quality of the helmet, and the patients’ ability to interact with objects in the virtual world, influence how much VR reduces pain in adults (Hoffman et al., 2004c, 2006; Wender et al., 2009). Moreover, as converging objective evidence, fMRI brain scan studies have shown reduced activity of the brain areas involved in pain perception in healthy adult volunteers distracted with VR during a brief painful thermal stimulus (Hoffman et al., 2004b, 2007).
There is a growing interest in using VR for distraction among children and adolescents; however, to date most clinical studies on VR analgesia have included burn patients during physical therapy (Carrougher et al., 2009) or during burn wound cleaning (Das et al., 2005; Maani et al., 2011; Hoffman et al., 2014; Dascal et al., 2017). VR has also emerged as a useful intervention for procedural pain in patients suffering from chronic diseases, such as cancer patients’ support during medical treatments (Chirico et al., 2016) and pain management during invasive procedures in pediatric cancer patients (Wint et al., 2002; Gershon et al., 2003, 2004; Wolitzky et al., 2005). Results exploring the use of VR distraction during needle related procedures have been encouraging, but mixed. Several studies have shown the predicted pattern, but non-significant reductions in patients’ pain during painful cancer treatment procedures for children. For example, in a non-immersive VR study by Sanders Wint et al. (2002), patients watched a traditional movie via see-through glasses, and found no significant reduction in cancer patients’ ratings of pain during venipuncture. A small early study using a relatively low tech VR goggles, did not find significant reduce patients pain during IV placement (Gold et al., 2006). Similarly, using early low tech VR technology, although they found some encouraging patterns, Gershon et al. (2004) found no significant reduction in patients’ pain during port placement. Due in part to recent dramatic increases in the availability of immersive VR equipment (e.g., Hoffman et al., 2014), there is growing interest in using VR as a non-pharmacologic analgesic. Gold and Mahrer (2017) recently published a large definitive clinical study exploring the use of immersive VR using untethered Oculus VR goggles, and found significant reductions in pain during blood draws. Using tethered Oculus VR DK2 goggles, Piskorz and Czub (2018) found significant reductions in pain during blood draws in children with kidney problems.
The aim of the present study was to investigate VR effectiveness as a distraction technique for pain management in children and adolescents with onco-hematological diseases undergoing venipuncture. Based on the Eccleston and Crombez (1999) interpretative model, we predicted that patients would focus their attentional resources on VR, and would have less attentional resources available to process incoming pain signals, with the result of reduced pain perception during venipuncture. We expected that patients interacting with VR during venipuncture would report less pain (“pain unpleasantness”, “time spent thinking about pain” and “worst pain”) compared to “treatment as usual”. The current study is the first to measure how much fun patients experienced during venipuncture, during No VR vs. during Yes VR. We predicted that patients would report significantly higher levels of fun during VR (a surrogate measure of positive affect), compared with the standard care (no VR), without side effects (Sharar et al., 2016).
From February 2014 to July 2016, patients attending the Service of Pediatric Oncology and Hematological Diseases of an Italian Children’s hospital participated. Children and adolescents who needed to undergo venipuncture twice in a year, for intravenous placement during chemotherapy, transfusions, magnetic resonance or blood analysis were recruited. Patients were selected according to the following criteria based on the existent literature (Won et al., 2017; Atzori et al., 2018a): children and adolescents who were able to understand Italian language, complete the tests, wear the helmet and interact with the VR environment, without any physical or psychological impairments. Patients with a venous access already inserted, with a diagnosis of epilepsy, not accompanied by their legal guardians, older than 17 years old and younger than 7 years old were excluded. Moreover, patients who wanted their own distraction tool (i.e., a book, a videogame or mp3-player) during the venipuncture, were excluded.
Seventeen patients met the inclusion criteria. However, one of them withdrew because he decided to use his own distraction technique and another patient withdrew because he didn’t want to use VR during the second venipuncture (the reason was not indicated). A total of 15 patients (66.7% males, 33.3% females; mean age 10.92, SD = 2.64, see Table 1) took part in the study. All patients had previously received at least one venipuncture by nurses of the Service of Pediatric Oncology and Hematological Diseases and none of patients was at the first access. No patient reported pain before the beginning of the procedure. No patient had previously used VR before the study and all participants were familiar with the wireless mouse. All patients underwent two venipunctures on two different days: one venipuncture with No VR, and one venipuncture with Yes VR on a second visit (treatment order randomized). The mean time between the first and the second venipuncture was 26.6 days (± 24.5).
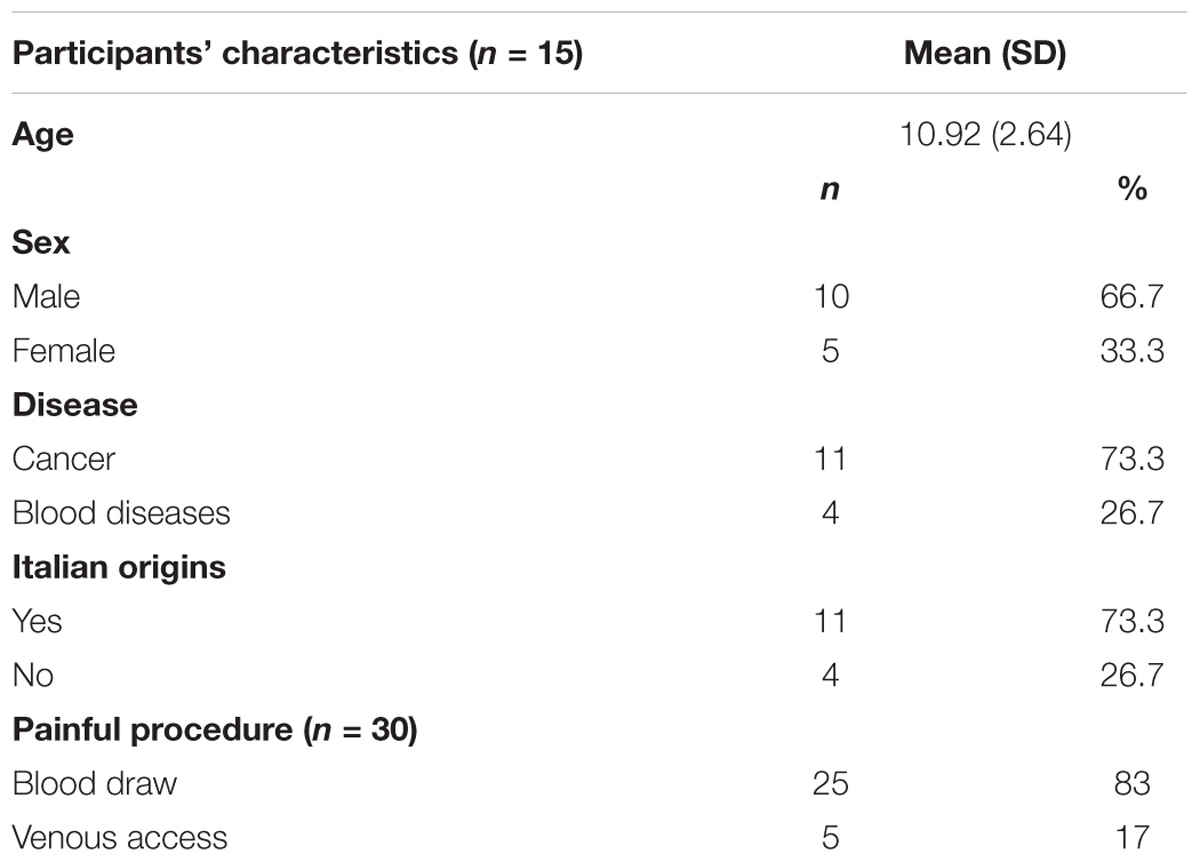
Table 1. Demographic, clinical and procedural characteristics.
This research was conducted in accordance with the Declaration of the World Medical Association1. The protocol was accepted by the Ethical Committee of the Hospital and the study was approved by the physicians and the nurses of the Service of Pediatric Oncology and Hematological Diseases and conducted in collaboration with the Pediatric Psychology Service and the Pain Therapy Service. Patients meeting the inclusion criteria were approached in the waiting room by a psychologist before the procedure in order to inform the families and get the signed written informed consent form by the patient’s caregivers. The written informed consent was obtained from all the parents of the participants. All participants provided written informed consent/assent in accordance with the Declaration of Helsinki. The study was described to the parents/guardians. If the parent/guardian’s gave permission, the research team then explained the study to the child in age-appropriate language, to see if the child was willing to participate in the study. Both children and their parents were encouraged to ask questions. Before the procedure began, patients and their caregivers were next escorted to the treatment room, and then the nurse arrived.
Using a within-subjects design, patients were assigned to the control condition (“No VR”) or the experimental condition (“Yes VR”) (treatment order randomized). Patients underwent the second venipuncture using the distraction technique not used the first time. The “No VR” control condition consisted of non-medical conversation by the nurse who performed the venipuncture (standard of care). In the “Yes VR” condition, patients interacted with VR during venipuncture. Before the nurse arrived, patients had 5 min to learn how to use the VR system. The helmet and the earphones included in the VR system were worn at the arrival of the nurse for the procedure and removed after the procedure. In both conditions, during the venipuncture, the patient, a nurse, the patient’s parent/caregiver and the psychologist researcher were present. After the procedure, the nurse left the room and patients completed the self-report questionnaire (pain ratings). No reward was given to patients for participating.
At the end of the procedure, patients filled out a brief self-report questionnaire aimed to evaluate the pain, the quality of the VR experience, nausea and fun. Patients responded by giving a 0–10 score on a horizontal Visual Analogue Scale (VAS; Price et al., 1994; Bailey et al., 2012). Pain, evaluated in its cognitive component (time spent thinking about pain), affective component (pain unpleasantness) and sensory component (worst pain) (Pagé et al., 2012), fun and nausea (Hoffman et al., 2004a) were evaluated in both conditions (“No VR” vs. “Yes VR”, within subjects). The quality of VR experience was investigated only in the “Yes VR” condition asking patients what extent did they feel like they went into the virtual world, and how real did the VR objects seem. The included questions were based on those used in previous studies (Hoffman et al., 2004a; Atzori et al., 2018b) and they were translated from English language into Italian language using the back-translation method, one of the most commonly used methods for cross-cultural translation (Maneesriwongul and Dixon, 2004). The total time for the procedure was comparable in both conditions. The time was measured from the positioning of the tourniquet to the needle extraction.
The VR equipment consisted of a VR helmet, the Personal 3D Viewer Sony: HMZ T-2, supported by a laptop, that allowed the interaction with the VR environment. The helmet had a 45° diagonal field of view, 1280 x 720 pixels per eye, latex-free earphones to provide acoustic isolation and it was suitable for both younger and older children. The VR software used was Snow World2, one of the most frequently employed VR environments, specifically designed to promote distraction from procedural pain (Hoffman et al., 2001). In SnowWorld, patients “go into” an icy canyon, where they throw snowballs at penguins, snowmen and other characters in VR, using a wireless mouse with the hand not employed in the venipuncture. SnowWorld was previously used in studies evaluating VR effectiveness for pain reduction in burn patients and during dental procedures. This is the first study in which this virtual environment is applied during venipuncture in patients with oncological and blood diseases.
A t-test for paired samples was adopted to compare pain, nausea and fun levels and the total time for the procedure between the “No VR” condition and the “Yes VR” condition. A researcher not involved in data collection carried out data analysis using the statistical Software SPSS. Based on the a priori assumption that the differences could only be in one direction, results were considered significant when associated with p-values less than 0.05, one tailed.
As reported in Table 2, when patients underwent venipuncture, their mean pain levels were significantly lower during VR, compared with pain levels during “No VR”, for all the three pain components: “Time spent thinking about pain” during “No VR” mean = 3.23 (SD = 2.98) vs. during “Yes VR” mean = 1.33 (SD = 1.05), p < 0.05, Cohen’s d = 0.62, moderate effect size; “Pain unpleasantness” during “No VR” mean = 3.27 (SD = 3.43) vs. during “Yes VR” mean = 0.93 (SD = 1.16), p < 0.01, Cohen’s d = 0.70 moderate effect size; “Worst pain” during “No VR” mean = 3.60 (SD = 3.00) vs. during “Yes VR” mean = 2.00 (SD = 1.20), p < 0.05, Cohen’s d = 0.51, moderate effect size.
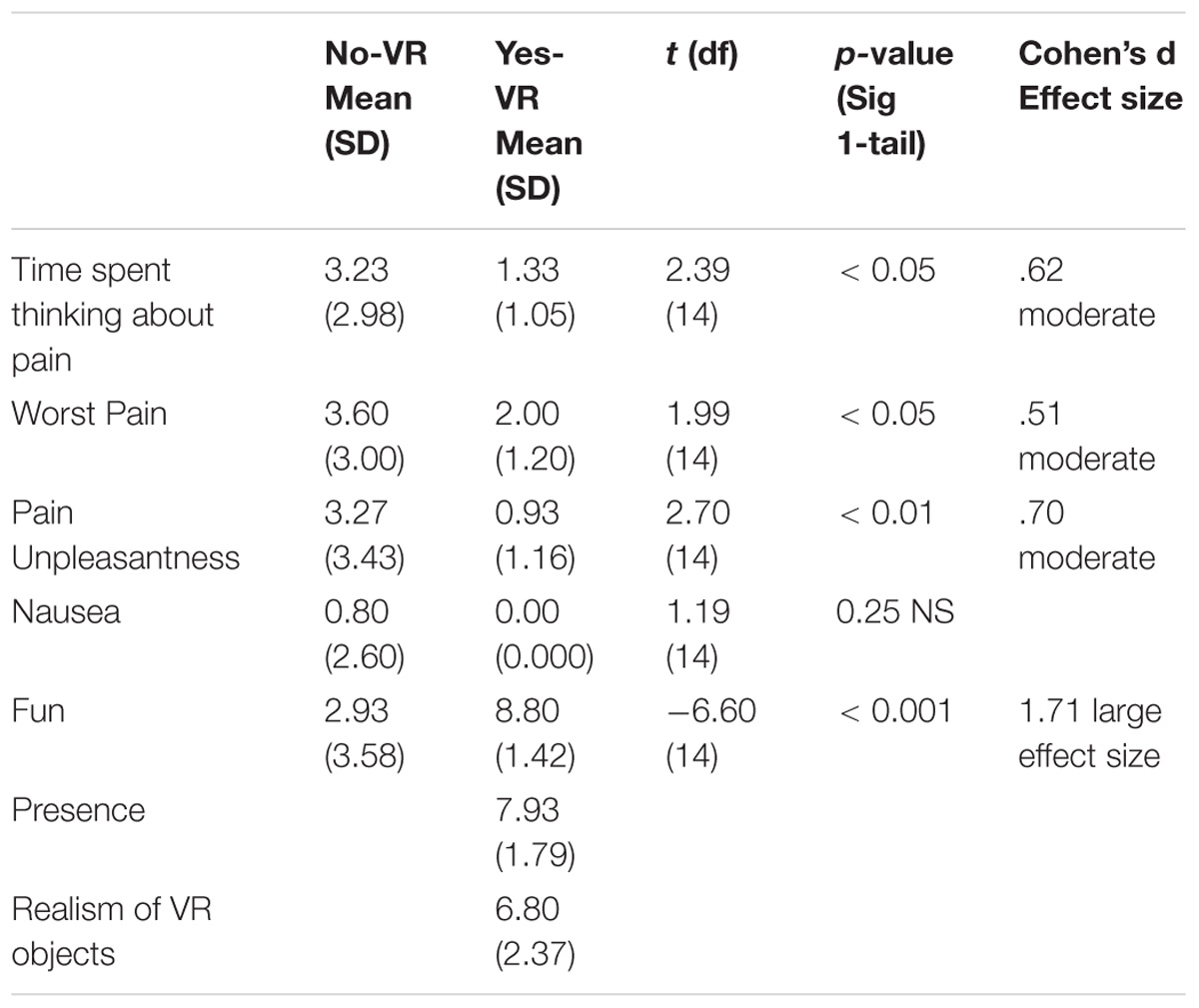
Table 2. Means (Standard Deviation) in “No-VR” condition vs. “Yes-VR” condition.
Patients distracted by VR reported a mean presence score of 7.93 (SD = 1.79), corresponding to “strong sense of going inside the computer generated world”, and a mean realism of VR objects score of 6.80 (SD = 2.37), corresponding to “Moderately real.”
Patients rated “fun” during the venipuncture as “mildly fun” during No VR, vs. “pretty fun” during VR. A significant difference for fun levels emerged between the two conditions: during “No VR” mean = 2.93 (SD = 3.58) vs. “Yes VR” mean = 8.80, SD = 1.42; t(14) = −6.60, p < 0.0001, Cohen’s d = 1.71, large effect size. No significant differences emerged for nausea levels between the two conditions (p > 0.05 NS): no patient reported nausea during the interaction with VR. During the “Yes VR” condition the mean of the total time of the procedure was 3.09 min (SD = 1.81) vs. 4.45 (SD = 3.50) during the “No VR” condition. The pattern of results showed the venipuncture took less time during VR vs. during No VR; however, the differences were not significant (p > 0.05, NS).
As shown in Figures 1, 2 when males and females were analyzed separately, both males and females showed the predicted pattern of results (lower pain during VR compared to standard of care No VR).
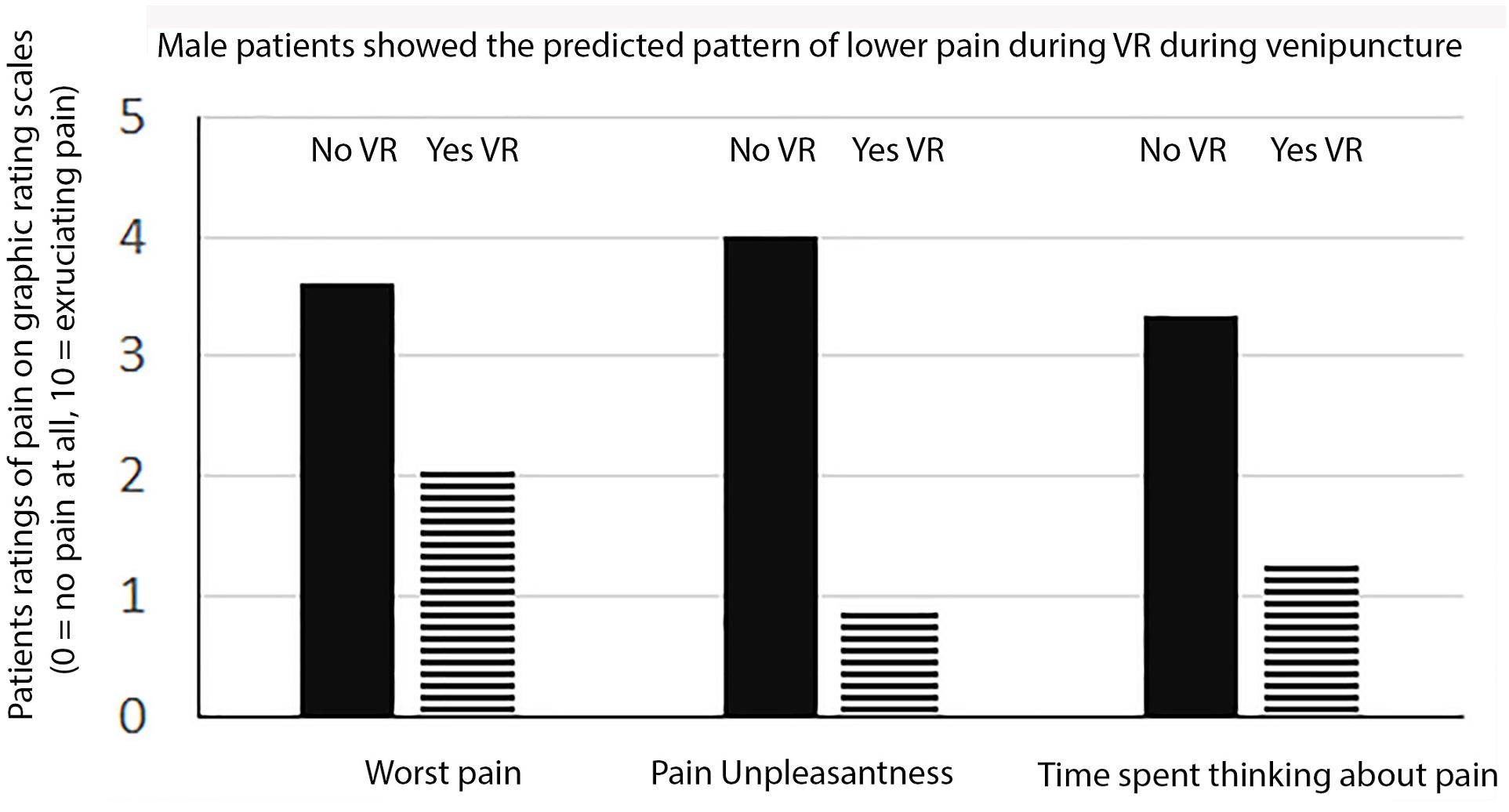
Figure 1. Male patients ratings of pain.
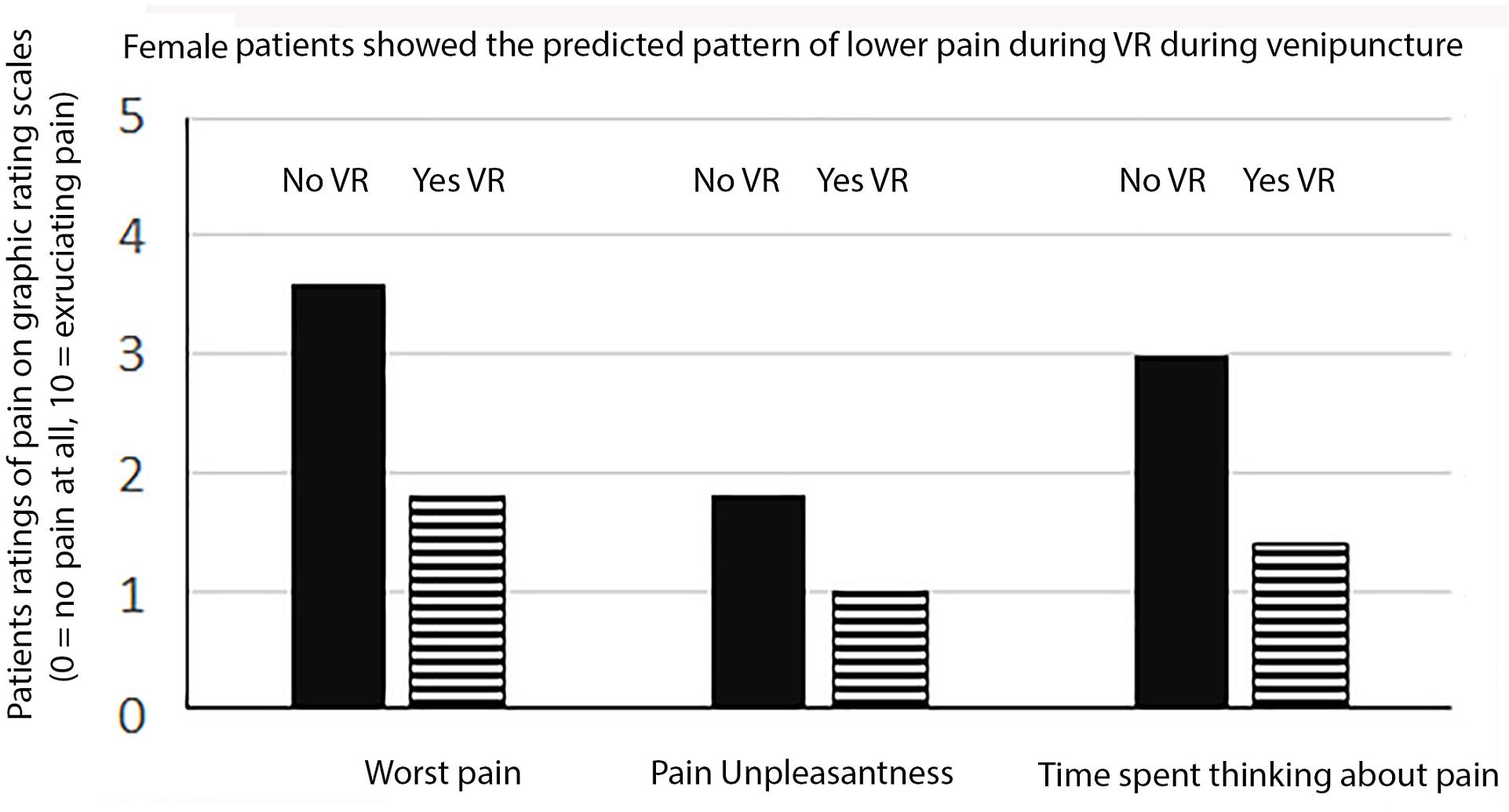
Figure 2. Female patients ratings of pain.
Based on the Eccleston and Crombez (1999) Interruption of Attention and Pain model, pain requires attention, and humans have limited attentional resources, we predicted that patients would focus their attention on VR, and would have fewer attentional resources available to focus on the painful stimulus, so patients would feel less pain. As predicted, children and adolescent patients reported significant reductions in pain unpleasantness, reported spending significantly less time thinking about their pain during venipuncture and reported significantly lower intensity of pain during VR. As predicted, children and adolescent patients reported significantly more fun when they used VR during their venipuncture. In the current study, patients experienced a strong illusion of presence and rated the virtual objects as “moderately real” looking. According to these results, the current VR system including the Sony HMZ-T2 helmet and the VR software SnowWorld, could be considered suitable for clinical applications with children and adolescents, promoting a medium-high quality virtual experience, without side effects. A higher quality helmet could potentially promote even better analgesia, as suggested by the literature (Hoffman et al., 2006).
The current study has some important limitations. Firstly, the sample size is small. Future studies with a larger sample are needed, and should also evaluate how much VR distraction reduces anxiety. Another limitation of the current study is the use of standard of care as a control group. Because the current study used standard of care as the control group, the difference between the groups may simply be due to the use of a distraction technique rather than to the specific use of VR. Addition research comparing VR to a more conventional distraction technique such as listening to music, is needed before any firm conclusions can about whether VR is unusually distracting.
According to Gold et al. (2007), not only the attentional demanding, but also the elicitation of positive emotion may contribute to VR analgesia (e.g., Sharar et al., 2016). The isolation from the medical setting (helmet blocking the patients view of the hospital room) and the possibility to be immersed in a pleasant activity makes VR a strong distraction technique, in particular for younger patients. The current study compared VR distraction with treatment as usual (non-medical conversation).
Future studies should compare VR to other distraction techniques during venipuncture, and should further explore the role of emotional activation in VR analgesia. For example, in future studies the VR condition should be compared to another simpler form of distraction such as having the children listen to an audiotape while undergoing the venipuncture treatment. And a study comparing immersive VR to augmented reality glassescould be interesting. Moreover, patients interacted with Snow World, a virtual environment specifically designed for procedural pain management, in particular for burn patients. In future studies, environments designed for the specific kind of procedure and patient’s characteristics (i.e., age, gender, cognitive abilities) are recommended.
Future studies may explore whether personality aspects of the child, such as catastrophizing, fear of pain, as well as parents’ anxiety, and patients’ memory for previous painful procedures (Noel et al., 2015) influence how much pain children experience during medical procedures (e.g., De Castro Morais Machado et al., 2018).
This study contributes to a growing literature that supports the use of immersive VR distraction for pain control. The current study evaluated the effectiveness of VR to control pain (in its affective, sensory and cognitive components) and to promote fun during venipuncture in pediatric patients with cancer and blood diseases. Younger patients suffering from chronic diseases (i.e., cancer and blood diseases), who spend much time in hospital and need several painful and stressful medical procedures, could particularly benefit from this distraction. In the future, VR systems could also let patients have social interaction (Won et al., 2017) and the quality of VR experiences will be more and more attentional demanding. VR distraction may also offer new opportunities for socialization and social support, especially for those patients in isolation or hospitalized for long periods.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
This study was supported by NIH grants R01GM042725 and R01AR054115 to DP, and by Effat University Research and Consultancy Institute, Jeddah, Saudi Arabia, and the Mayday Fund. Thanks to the support of Foundation Cassa di Risparmio di Firenze.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Thanks to Foundation Cassa di Risparmio di Firenze. Special thanks to A.T.C.R.U.P.
Atzori, B., Hoffman, H. G., Vagnoli, L., Messeri, A., and Grotto, R. L. (2018a). “Virtual Reality as Distraction Technique for Pain Management in Children and Adolescents,” in Encyclopedia of Information Science and Technology, Fourth Edition, ed. M. Khosrow-Pour (New York, NY: Idea Group Inc.), 5955–5965.
Atzori, B., Vagnoli, L., Messeri, A., and Lauro Grotto, R. (2018b). “Virtual Reality for Pain Management Among Children and Adolescents: Applicability in Clinical Settings and Limitations,” in Universal Access in Human-Computer Interaction. Virtual, Augmented, and Intelligent Environments. UAHCI 2018. Lecture Notes in Computer Science, eds M. Antona and C. Stephanidis (Cham: Springer).
Atzori, B., Hoffman, H. G., Vagnoli, L., Patterson, D. R., Alhalabi, W., Messeri, A., Lauro Grotto, R. et al. (2018c). Virtual reality analgesia during venipuncture in pediatric patients with onco-hematological diseases. Front. Psychol. 9:2508. doi: 10.3389/fpsyg.2018.02508
Bailey, B., Gravel, J., and Daoust, R. (2012). Reliability of the visual analog scale in children with acute pain in the emergency department. Pain 153, 839–842. doi: 10.1016/j.pain.2012.01.006
Bailey, J. O., and Bailenson, J. N. (2017). Considering virtual reality in children’s lives. J. Child. Media 11, 107–113. doi: 10.1080/17482798.2016.1268779
Birnie, K. A., Noel, M., Chambers, C. T., Uman, L. S., and Parker, J. A. (2018). Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 10:CD005179. doi: 10.1002/14651858.CD005179.pub4
Bisogni, S., Dini, C., Olivini, N., Ciofi, D., Giusti, F., Caprilli, S., et al. (2014). Perception of venipuncture pain in children suffering from chronic diseases. BMC Res. Notes 7:735. doi: 10.1186/1756-0500-7-735
Caprilli, S., and Messeri, A. (2006). Animal-assisted activity at a. meyer children’s hospital: a pilot study. Evid. Based Complement. Alternat. Med. 3, 379–383. doi: 10.1093/ecam/nel029
Carrougher, G. J., Hoffman, H. G., Nakamura, D., Lezotte, D., Soltani, M., Leahy, L., et al. (2009). The effect of virtual reality on pain and range of motion in adults with burn injuries. J. Burn Care Res. 30, 785–791. doi: 10.1097/BCR.0b013e3181b485d3
Chirico, A., Lucidi, F., De Laurentiis, M., Milanese, C., Napoli, A., and Giordano, A. (2016). Virtual reality in health system: beyond entertainment. a mini-review on the efficacy of VR during cancer treatment. J. Cell. Physiol. 231, 275–287. doi: 10.1002/jcp.25117
Das, D. A., Grimmer, K. A., Sparnon, A. L., McRae, S. E., and Thomas, B. H. (2005). The efficacy of playing a virtual reality game in modulating pain for children with acute burn injuries: a randomized controlled trial [ISRCTN87413556]. BMC Pediatr. 5:1. doi: 10.1186/1471-2431-5-1
Dascal, J., Reid, M., Ishak, W. W., Spiegel, B., Recacho, J., Rosen, B., et al. (2017). Virtual reality and medical inpatients: a systematic review of randomized, controlled trials. Innovat. Clin. Neurosci. 14:14.
De Castro Morais Machado, G., Van Wijk, A., van der Heijden, G., and Costa, L. R. (2018). Does parental anxiety, coping, and pain catastrophizing influence child behavior during sedation? Pediatri. Dent. 15, 365–369.
Duff, A. J. A. (2003). Incorporating psychological approaches into routine paediatric venepuncture. Arch. Dis. Child. 88, 931–937. doi: 10.1136/adc.88.10.931
Eccleston, C., and Crombez, G. (1999). Pain demands attention: a cognitive–affective model of the interruptive function of pain. Psychol. Bull. 125:356. doi: 10.1037/0033-2909.125.3.356
El-Housseiny, A. A., Alamoudi, N. M., Farsi, N. M., and El Derwi, D. A. (2014). Characteristics of dental fear among Arabic-speaking children: a descriptive study. BMC Oral Health 22:118. doi: 10.1186/1472-6831-14-118
Fields, H. L. (2018). How expectations influence pain. Pain 159(Suppl. 1), S3–S10. doi: 10.1097/j.pain.0000000000001272
Gershon, J., Zimand, E., Lemos, R., Rothbaum, B. O., and Hodges, L. (2003). Use of virtual reality as a distractor for painful procedures in a patient with pediatric cancer: a case study. CyberPsychol. Behav. 6, 657–661. doi: 10.1089/109493103322725450
Gershon, J., Zimand, E., Pickering, M., Rothbaum, B. O., and Hodges, L. (2004). A pilot and feasibility study of virtual reality as a distraction for children with cancer. J. Am. Acad. Child Adolesc. Psychiatry 43, 1243–1249. doi: 10.1097/01.chi.0000135621.23145.05
Gold, J. I., Belmont, K. A., and Thomas, D. A. (2007). The neurobiology of virtual reality pain attenuation. CyberPsychol. Behav. 10, 536–544. doi: 10.1089/cpb.2007.9993
Gold, J. I., Kim, S. H., Kant, A. J., Joseph, M. H., and Rizzo, A. S. (2006). Effectiveness of virtual reality for pediatric pain distraction during IV placement. CyberPsychol. Behav. 9, 207–212. doi: 10.1089/cpb.2006.9.207
Gold, J. I., and Mahrer, N. E. (2017). Is virtual reality ready for prime time in the medical space? A randomized control trial of pediatric virtual reality for acute procedural pain management. J. Pediatr. Psychol. 43, 266–275. doi: 10.1093/jpepsy/jsx129
Hoffman, H. (1998). Cyberpsychology & behavior. CyberPsychol. Behav. 1, 195–200. doi: 10.1089/cpb.1998.1.195
Hoffman, H. G. (2004). Virtual-reality therapy. Sci. Am. 291, 58–65. doi: 10.1038/scientificamerican0804-58
Hoffman, H. G., Chambers, G. T., Meyer, III. W. J., Arceneaux, L. L., Russell, W. J., Seibel, E. J., et al. (2011). Virtual reality as an adjunctive non-pharmacologic analgesic for acute burn pain during medical procedures. Ann. Behav. Med. 41, 183–191. doi: 10.1007/s12160-010-9248-7
Hoffman, H. G., Doctor, J. N., Patterson, D. R., Carrougher, G. J., and Furness, T. A. III. (2000a). Virtual reality as an adjunctive pain control during burn wound care in adolescent patients. Pain 85, 305–309. doi: 10.1016/S0304-3959(99)00275-4
Hoffman, H. G., Meyer, W. J. III., Ramirez, M., Roberts, L., Seibel, E. J., Atzori, B., et al. (2014). Feasibility of articulated arm mounted oculus rift virtual reality goggles for adjunctive pain control during occupational therapy in pediatric burn patients. Cyberpsychol. Behav. Soc. Netw. 17, 397–401. doi: 10.1089/cyber.2014.0058
Hoffman, H. G., Patterson, D. R., and Carrougher, G. J. (2000b). Use of virtual reality for adjunctive treatment of adult burn pain during physical therapy: a controlled study. Clin. J. Pain 16, 244–250. doi: 10.1097/00002508-200009000-00010
Hoffman, H. G., Patterson, D. R., Carrougher, G. J., Nakamura, D., Moore, M., Garcia-Palacios, A., et al. (2001). The effectiveness of virtual reality pain control with multiple treatments of longer durations: a case study. Int. J. Hum. Comput. Interact. 13, 1–12. doi: 10.1207/S15327590IJHC1301_1
Hoffman, H. G., Patterson, D. R., Magula, J., Carrougher, G. J., Zeltzer, K., Dagadakis, S., et al. (2004a). Water-friendly virtual reality pain control during wound care. J. Clin. Psychol. 60, 189–195.
Hoffman, H. G., Richards, T. L., Coda, B., Bills, A. R., Blough, D., Richards, A. L., et al. (2004b). Modulation of thermal pain-related brain activity with virtual reality: evidence from fMRI. Neuroreport 15, 1245–1248.
Hoffman, H. G., Sharar, S. R., Coda, B., Everett, J. J., Ciol, M., Richards, T., et al. (2004c). Manipulating presence influences the magnitude of virtual reality analgesia. Pain 111, 162–168.
Hoffman, H. G., Richards, T. L., Van Oostrom, T., Coda, B. A., Jensen, M. P., Blough, D. K., et al. (2007). The analgesic effects of opioids and immersive virtual reality distraction: evidence from subjective and functional brain imaging assessments. Anesth. Analg. 105, 1776–1783. doi: 10.1213/01.ane.0000270205.45146.db
Hoffman, H. G., Seibel, E. J., Richards, T. L., Furness, T. A., Patterson, D. R., and Sharar, S. R. (2006). Virtual reality helmet display quality influences the magnitude of virtual reality analgesia. J. Pain 7, 843–850. doi: 10.1016/j.jpain.2006.04.006
Maani, C. V., Hoffman, H. G., Morrow, M., Maiers, A., Gaylord, K., McGhee, L. L., et al. (2011). Virtual reality pain control during burn wound debridement of combat-related burn injuries using robot-like arm mounted VR goggles. J. Trauma 71(1 Suppl.), S125–S130. doi: 10.1097/TA.0b013e31822192e2
Maneesriwongul, W., and Dixon, J. K. (2004). Instrument translation process: a methods review. J. Adv. Nurs. 48, 175–186. doi: 10.1111/j.1365-2648.2004.03185.x
Noel, M., Rabbitts, J. A., Tai, G. G., and Palermo, T. M. (2015). Remembering pain after surgery: a longitudinal examination of the role of pain catastrophizing in children’s and parents’ recall. Pain 156, 800–808. doi: 10.1097/j.pain.0000000000000102
Pagé, M. G., Katz, J., Stinson, J., Isaac, L., Martin-Pichora, A. L., and Campbell, F. (2012). Validation of the numerical rating scale for pain intensity and unpleasantness in pediatric acute postoperative pain: sensitivity to change over time. J. Pain 13, 359–369. doi: 10.1016/j.jpain.2011.12.010
Piskorz, J., and Czub, M. (2018). Effectiveness of a virtual reality intervention to minimize pediatric stress and pain intensity during venipuncture. J. Spec. Pediatr. Nurs. 23:e12201. doi: 10.1111/jspn.12201
Price, D. D., Bush, F. M., Long, S., and Harkins, S. W. (1994). A comparison of pain measurement characteristics of mechanical visual analogue and simple numerical rating scales. Pain 56, 217–226. doi: 10.1016/0304-3959(94)90097-3
Sharar, S. R., Alamdari, A., Hoffer, C., Hoffman, H. G., Jensen, M. P., and Patterson, D. R. (2016). Circumplex model of affect: a measure of pleasure and arousal during virtual reality distraction analgesia. Games Health J. 5, 197–202. doi: 10.1089/g4h.2015.0046
Soltani, M., Drever, S. A., Hoffman, H. G., Sharar, S. R., Wiechman, S. A., Jensen, M. P., and Patterson, D. R. (2018). Virtual reality analgesia for burn joint flexibility: a randomized controlled trial. Rehabil Psychol. 63, 487–494. doi: 10.1037/rep0000239
Weisman, S. J., Bernstein, B., and Schechter, N. L. (1998). Consequences of inadequate analgesia during painful procedures in children. Arch. Pediatr. Adolesc. Med. 152, 147–149. doi: 10.1001/archpedi.152.2.147
Wender, R., Hoffman, H. G., Hunner, H. H., Seibel, E. J., Patterson, D. R., and Sharar, S. R. (2009). Interactivity influences the magnitude of virtual reality analgesia. J. Cyber Ther. Rehabil. 2, 27-33.
Wint, S. S., Eshelman, D., Steele, J., and Guzzetta, C. E. (2002). Effects of distraction using virtual reality glasses during lumbar punctures in adolescents with cancer. Oncol. Nurs. Forum 29, E8–E15. doi: 10.1188/02.ONF.E8-E15
Wolitzky, K., Fivush, R., Zimand, E., Hodges, L., and Rothbaum, B. O. (2005). Effectiveness of virtual reality distraction during a painful medical procedure in pediatric oncology patients. Psychol. Health 20, 817–824. doi: 10.1080/14768320500143339
Keywords: virtual reality, children, adolescents, pain, pediatric cancer, distraction
Citation: Atzori B, Hoffman HG, Vagnoli L, Patterson DR, Alhalabi W, Messeri A and Lauro Grotto R (2018) Virtual Reality Analgesia During Venipuncture in Pediatric Patients With Onco-Hematological Diseases. Front. Psychol. 9:2508. doi: 10.3389/fpsyg.2018.02508
Received: 01 October 2018; Accepted: 26 November 2018;
Published: 20 December 2018.
Edited by:
Federica Pallavicini, Università degli Studi di Milano Bicocca, ItalyReviewed by:
Karel Allegaert, University Hospitals Leuven, BelgiumCopyright © 2018 Atzori, Hoffman, Vagnoli, Patterson, Alhalabi, Messeri and Lauro Grotto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara Atzori, cHNpY29iLmF0em9yaUBnbWFpbC5jb20= Hunter G. Hoffman, aG9vbnRhaXJAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.