 Mimma Tafà
Mimma Tafà Luca Cerniglia
Luca Cerniglia Silvia Cimino
Silvia Cimino Giulia Ballarotto
Giulia Ballarotto Eleonora Marzilli
Eleonora Marzilli Renata Tambelli
Renata Tambelli- 1Department of Dynamic and Clinical Psychology, Sapienza Università di Roma, Rome, Italy
- 2Faculty of Psychology, Università Telematica Internazionale Uninettuno, Rome, Italy
Background: Several studies have suggested that the early loss of parents is a potentially traumatic experience, exposing adolescents to a higher risk for the onset of psychopathological symptoms. Furthermore, research has shown an association between the loss of a parent in childhood and subsequent physical illnesses, but much less attention has been given to the predictive role of loss in the development of physical illness in adolescence.
Methods: From a larger normative sample, we selected 418 early adolescents (and their surviving parents) each of whom had lost a parent in their first 3 years of life. We evaluate the offspring’s and parents’ psychopathological symptoms, dissociation, and physical problems over a 6-year period. Univariate and multivariate Cox proportional hazard regression analyses with time-dependent variables were used to examine the predictive values of the adolescents’ and surviving parents’ psychopathological symptoms, and youths’ demographic characteristics (sex and age) for the occurrence of physical illness during a 6-year period of follow-up.
Results: Independently of sex, the psychopathological risk of the surviving parents’ and adolescents’ affective problems and dissociation has been found to predict the occurrence of physical illnesses. Furthermore, dissociation was the most significant predictor of significant physical problems.
Conclusion: These results may be relevant and an addition to the previous literature, opening up new possibilities for prevention and intervention that are oriented toward greater support for children who have experienced the loss of one parent and for surviving parents.
Introduction
The death of a parent in the 1st year of a child’s life represents one of the most significant painful events in his or her emotional development (Haine et al., 2008), which may have short-term (Rostila and Saarela, 2011) and/or long-term consequences for mental health (Ellis et al., 2013), as well as causing physical illness (Bylund-Grenklo et al., 2016; Cipriano and Cipriano, 2017). Although the death of a parent is a potentially traumatic event when it happens in the evolutionary phases of development (Cimino et al., 2012b), research has underlined that when it occurs in the first 3 years of life, it has a greater impact on psychological and physical health (Abdelnoor and Hollins, 2004). However, within the Developmental Psychopathology framework, many studies have evidenced that the early experience of parental death need not lead to the development of mental and physical illness, emphasizing individuals’ resilience capacities (Lin et al., 2004; Ahern et al., 2008) and suggesting the importance of identifying risk factors that can influence short- and long-term outcomes (Luecken and Roubinov, 2012; Williams and Aber, 2016).
In spite of these results, only a few studies have been interested in the possible mechanisms underlying the associations between early parental loss and later mental and physical health, focusing on the quality of emotional-social support following the death (Schoenfelder et al., 2011). The present longitudinal study aims to understand better the link between parental death in infancy and physical illness during adolescence, considering the role played by youths’ and surviving parents’ psychological profiles.
Within the psychodynamic perspective (Freud, 1917; Abraham, 1924; Brown, 1966), the childhood loss of a love object was postulated as an important risk factor for later psychopathology. The attachment theory proposed by Bowlby (1980), and the psychoanalytic position proposed by Freud (1917) in relation to the relationship between object loss and future depression, suggested that unresolved childhood grief might have both immediate and long-term effects, increasing vulnerability to future psychopathological problems (Bowlby, 1960, 1973). Since then, there has been increase in the empirical work focusing on the impact of parental death experiences on an individual’s psychological wellbeing, suggesting that the loss of an attachment figure might be associated with a higher risk of developing a wide range of later psychopathologies, such as panic disorder and phobia (Kendler et al., 1992), depression (Brown and Harris, 1978; Harris et al., 1986), and anxiety (Faravelli et al., 1985; Bifulco et al., 1987), especially when the death of a parent was experienced during an early stage of life. In this field, the pioneering studies by Spitz (1945) and Spitz and Wolf (1946) were among the first observations of the impact of early prolonged emotional deprivation on infants’ psychological and physical wellbeing, reporting the presence of both severe mental adverse outcomes (such as acute anxiety, distress, depression, and withdrawal) and a progressive physical deterioration, including frequent illnesses, motor delay, loss of weight, eczema, and, in some cases, even death. Furthermore, these studies suggested that parental loss in itself did not lead to later negative outcomes. Rather, other antecedent and concomitant risk factors associated with bereavement might influence physical and psychopathological health during the lifespan, including the quality of subsequent parental care (Breier et al., 1988) and a socio-economically disadvantaged status (Harris et al., 1986).
From a developmental point of view, as suggested by studies by Brent et al. (2012) and Feigelman et al. (2017), adolescence represents a particular risk stage for the onset of psychopathological symptoms among children who have experienced the early death of a parent (see also McLaughlin et al., 2012). During adolescence, a maturation of cognitive structures and functions occurs, leading to the acquisition of concepts such as the irreversibility and causality of events connected with the concept of death (Corr, 1995; Cerniglia et al., 2015) and involving a re-elaboration of past traumas, such as the death of a parent (Blos, 1962). In fact, empirical research has widely confirmed that childhood parental loss is a crucial risk factor for adolescent onset and maintenance of both internalized and externalized psychopathological difficulties (Kaplow et al., 2010; Stikkelbroek et al., 2012), such as depression (Melhem et al., 2008; Jacobs and Bovasso, 2009; Babore et al., 2016; Feigelman et al., 2017), suicidality (Serafini et al., 2015), and an increased tendency to risky behaviors, including substance abuse (von Sydow et al., 2002; Cerniglia et al., 2017b). Moreover, there is evidence that early parental death is significantly associated with eating disorder symptoms (Beam et al., 2004; Nickerson et al., 2013; Cerniglia et al., 2017a) and dissociative symptoms (Cerniglia et al., 2014), which may represent maladaptive strategies used by adolescents to cope with negative emotions related to loss (Cimino et al., 2012a).
In adolescence, the impact of early parental death also seems to affect other domains associated with the specific evolutionary tasks of this phase. In particular, adolescence is described as a transitional period of consolidation and integration of identity transformations (Blos, 1977). Studies have shown that in this developmental period, the early death of a parent is also associated with difficulties in interpersonal and intimate bonds (Maier and Lachman, 2000), lower grades or school dropout (Cas et al., 2013; Berg et al., 2014), and lower employment rates (Ellis et al., 2013). Furthermore, a growing body of research has evidenced that besides the impact of this early adverse experience on individual emotional-behavioral functioning, early parental death also plays a crucial predictive role for negative physical health outcomes in adolescence (McEwen and Lasley, 2002; Luecken, 2008; van de Pavert et al., 2017), such as chronic illness (Raposa et al., 2014), cortisol dysregulation (Biank and Werner-Lin, 2011), and premature death (Li et al., 2014; Smith et al., 2014). In particular, epidemiological studies on the effects of adverse childhood experiences (ACEs) on an individual’s health throughout the lifespan development have reported an increased risk of developing a wide spectrum of physical illnesses (Felitti et al., 1998; Felitti and Anda, 2003; Anda et al., 2006; Felitti, 2009). With specific regard to early parental loss, more contemporary ACE-related studies have shown that this experience was prospectively associated with adolescent obesity, unhealthy weight control behaviors (Isohookana et al., 2016), heart disease, asthma (Scott et al., 2011), and painful medical conditions, including arthritis or rheumatism, chronic back and neck problems, severe migraines or headaches, and other forms of chronic pain (Sachs-Ericsson et al., 2017). Overall, these findings are hypothesized to result from altered stress responses over a lifetime that could increase the risk for physical difficulties, including hypertension, asthma, and heart disease (Wright, 2011; Cassel, 2017). Raposa et al. (2014) found that early stress conditions are related to the presence of depression during adolescence, which could have a negative impact on physical health in early adulthood.
Recent studies have suggested that the main mechanisms responsible for increased vulnerability to psychological and physical illnesses after parental death in childhood arise from the impact of this event on the system of response to physiological stress (Pendry and Adam, 2007). In accordance with transitional events theory (Felner et al., 1988), variability in children’s adjustment after the loss of a parent is influenced by the chain of stressful life events that follow the death, children’s protective resources, and the dynamic relationships between these variables. More specifically, early parental death represents a stressful experience that may overwhelm a child’s ability to cope with this event (Goodman, 2002), initiating a cascade of negative life events that affect the development of emotional and self-regulatory abilities to respond to daily stressors over time (Luecken and Lemery, 2004; Tottenham et al., 2011). At a neurobiological level, it may induce important biological changes that impact nervous, endocrine, and immune systems (Danese and McEwen, 2012), which causes their effects to persist throughout the lifespan (Rutter, 1996; Adejuwon, 2010), increasing children’s vulnerability to both psychopathological and physical illness (Luecken et al., 2009; Flaherty et al., 2013; Serafini et al., 2015).
In this regard, among the primary resources that could help a child to adapt positively to his/her parental loss are the quality of the relationship with the surviving parent (Compas et al., 2001; Eisenberg et al., 2001) and the ability to cope with future stressful life events (Kwok et al., 2005; Haine et al., 2006; Pendry and Adam, 2007). Furthermore, the quality of the relationship with the surviving parent may be impaired by the maladaptive psychopathological functioning of the caregiver, representing a significant risk factor for the bereaved offspring’s later psychological and physical health (Wolchik et al., 2008). Several studies have shown that the presence of parental psychopathological symptoms is prospectively associated with the development of psychopathological difficulties in offspring over time (van der Pol et al., 2016; Hannigan et al., 2017; Plass-Christl et al., 2017). A parent with psychological problems may provide a family environment that does not promote children’s emotional regulation, leading children to develop ineffective emotional regulation strategies (Luecken et al., 2005), resulting in excessive emotional and physiological reactivity to later stress in adolescence (Luecken et al., 2009; Tafà et al., 2017).
On the basis of the present literature, the aims of this 6-year longitudinal study were to (1) assess the possible predictive values of offsprings’ and parents’ psychopathological symptoms for the occurrence of physical problems in adolescents and (2) determine the sex differences in the predictive value of psychopathological symptoms for the occurrence of physical problems in adolescents.
Materials and Methods
Participants
The subjects recruited for this study were part of a larger sample (N = 3548 children) and were recruited in the first grade of elementary schools in central Italy in March 2010. All students from four randomly selected classes in each school were invited to contribute to the study. The research group was composed of five psychologists who explained the goals and procedure of the study to the students and teachers in their classrooms and to their parents in two information sessions. In addition, the children’s pediatricians collaborated in the study, providing information on the state of the children’s physical health at different stages of the research.
In accordance with the Declaration of Helsinki, the study was approved before its start by the Ethical Committee of the Faculty of Psychology at Uninettuno University (n. 2/2010), and written informed consent was obtained from the parents before assessment.
From the larger sample, we selected for the aims of this study adolescents who had lost a parent in their first 3 years of life (N = 418 adolescents, 53% boys).
The assessments were carried out in four steps over 6 years. The mean (SD) age of the children at Time 1 was 6.31 (0.42) years; Time 2 was at 8 years of age; Time 3 was at 10 years of age; and Time 4 was at 12 years of age. The surviving parents’ mean age at Time 1 was 43.55 (2.3) years. At Time 2, the surviving parents’ mean age was 45.85 (1.9) years; at Time 3, it was 47.91 (2.4) years; and at Time 4, it was 50.01 (1.4) years. Sixty-two percent of surviving parents were mothers. All the children were of homogeneous nationality and were their parents’ biological children. Most families were of middle socioeconomic status (94%) (SES; Bornstein and Bradley, 2003).
Measures
Physical Health
Physical health assessment was measured by pediatricians at all sessions through a modified questionnaire derived from Health Appraisal Questionnaire of the Centers for Disease Control and Prevention. The questions concerned gastrointestinal diseases (irritable bowel symptoms, duodenal, or gastric ulcer), cardiovascular diseases (hypertension, angina pectoris), and respiratory symptoms and diseases (asthma, chronic bronchitis, shortness of breath). A detailed description of this measure and its characteristics can be found in Felitti et al.’s (1998) work.
Children’s psychopathological symptoms were assessed at all session through the CBCL 6-18 (CBCL; Achenbach and Rescorla, 2001; Italian validation – Frigerio et al., 2004), which is a report-form measure filled out by parents (in this study, it was filled out by the surviving parent) that assesses children’s emotional-behavioral functioning. It contains 113 items that are rated as Not True (0), Somewhat or Sometimes True (1), or Very True or Often True (2). Validity and reliability are excellent, and extensive normative data are available for children ranging from 6 to 18 years (Frigerio et al., 2004). In this tool, Anxious/Depressed, Withdrawn/Depressed, and Somatic Complaints are grouped into the subscale of Internalizing Problems; Rule-Breaking Behavior and Aggressive Behavior are grouped into the subscale of Externalizing Problems; in addition, Social Problems, Thought Problems, and Attention Problems (not grouped into any subscale) are also considered. For the aims of this study, we used DSM-oriented scales (oriented to the DSM-IV-TR, since the study began before the publication of the fifth version): affective problems, anxiety problems, somatic problems, attention deficit/hyperactivity problems, oppositional defiant problems, and conduct problems. We used the clinical cut-offs for the DSM-oriented scales and thus regarded these variables as categorical.
Dissociation
The Child Dissociative Checklist (Putnam et al., 1993) is a 20-item observer-report checklist with a 3-point scale (0 = not true, 1 = sometimes true, 2 = frequently true). The Child Dissociative Checklist is a clinical screening instrument that assesses dissociation on the basis of ratings given by caregivers or adults in close contact with the child. A score of 12 or higher on the Child Dissociative Checklist is evidence of pathological dissociation. The Child Dissociative Checklist shows good 1-year test–retest stability (r = 0.65) and internal consistency (Cronbach’s alpha = 0.86) (Putnam et al., 1993). Good convergent and discriminant validity have been indicated (Putnam et al., 1993).
Parental Psychopathological Risk
The Symptom Check-List (SCL-90-R) is a 90-item self-report symptom inventory aimed at measuring psychological symptoms and psychological distress (Derogatis, 1994). Its main symptom dimensions are Somatization, Obsessive-Compulsivity, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. The SCL-90-R has been shown previously to have good internal coherence (α coefficient = 0.70–0.96) in adolescents and adults (Italian validated version: Prunas et al., 2012). Besides these nine primary scales, the questionnaire provides a Global Severity Index (GSI). The GSI is obtained from the average severity score of all the symptoms indicated by the subjects, making it possible to determine severity and degree of psychological distress. The clinical cut-off for this index is 1 (Prunas et al., 2012). In this study, we chose to use the GSI as a global index of psychopathology, following the suggestion of Bergly et al. (2013) who pointed out a high collinearity between the nine syndromic subscales.
Procedure and Statistical Analysis
The parents of the recruited subjects completed the assessments for demographic information, offspring emotional-behavioral functioning, and their dissociation symptoms at their home, while the pediatricians filled out the measure to assess physical health at schools. Parents also filled out the measure for the screening of their own psychopathological risk (at home). Parents and pediatricians were asked to fill out the measures at 6, 8, 10, and 12 years of the child. To determine the risk factors for physical problems, data from participants who were classified as healthy in the initial assessment were selected for statistical analysis. Statistical analyses were performed using the Statistical Package for the Social Sciences, SPSS software (IBM corp, 2013). A univariate Cox proportional hazard regression analysis with time-dependent variables was used to examine the predictive values of baseline psychopathological symptoms (assessed through the CBCL/6-18 and SCL-90-R), dissociation, and demographic characteristics (sex and age) for the occurrence of physical problems during the 6-year period of follow-up. The formula of the Hazard Function was H(t) = H0(t) x exp(b1X1 + b2X2 + b3X3 +... bkXk, where X1... Xk are a collection of predictor variables and H0(t) is the baseline hazard at time t, representing the hazard for a person with the value 0 for all the predictor variables.
The outcome variable (survival time) in the Cox proportional hazard regression was defined as the period between the initial assessment and the detection of occurrence of physical problems during follow-up. If a participant showed a relevant physical problem in a follow-up assessment, an event was recorded and that case’s data were not censored. On the other hand, if no relevant physical problem was detected by the pediatrician in any follow-up assessment, no event was recorded and the participant’s data were censored. Thus, censored individuals were those who either had no physical problem by the end of the study or were lost to follow-up during the course of the study before the physical problem had been identified. We examined the predictive values of sex and age for the occurrence of physical problems using the univariate Cox proportional hazard regression, and then we evaluated the predictive values of the psychopathological symptoms on the basis of those indicated by Peduzzi et al. (1995). All significant psychopathological predictors found in the univariate analysis were then further used in a forward stepwise multivariate Cox proportional hazard regression to determine which psychopathological symptom was the most significant predictor of physical problems among all, male, and female participants. A p-value lower than 0.05 was considered significant.
Results
A total of 418 mourning families completed the protocol, and all children were assessed by pediatricians in the course of their development toward adolescence. Of these, 12% (N = 50) were classified as having a physical problem at Time 1 (52% females). Three-hundred and sixty-eight children (51% females) showed no relevant physical problem at the first assessment at 6 years of age.
To examine the predictive values of offsprings’ and parents’ psychopathological symptoms and offsprings’ dissociation and demographic characteristics (sex and age) for the occurrence of physical problems during the 6-year period, we carried out a univariate Cox proportional hazard regression analysis with time-dependent variables. In particular, we examined the predictive values of sex and age for the occurrence of physical problems using a univariate Cox proportional hazard regression and then we evaluated the predictive values of the psychopathological symptoms.
The results of the univariate Cox proportional hazard regression analysis are shown in Tables 1, 2 and indicate that, irrespective to sex, offsprings’ affective problems and dissociation and surviving parents’ GSI were risk factors for the occurrence of a relevant physical problem (Table 1).
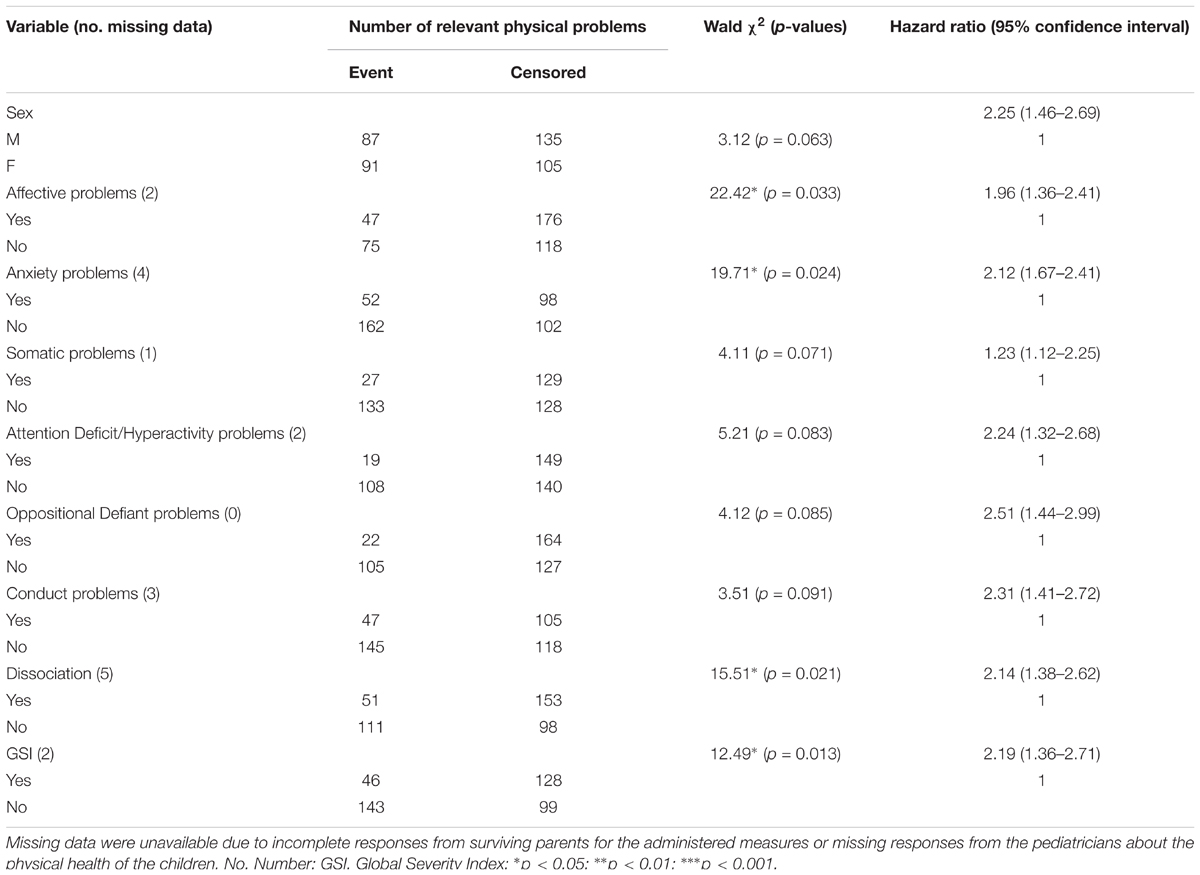
TABLE 1A. Predictive value of sex and psychopathological problems for the occurrence of a relevant physical problem in the univariate Cox proportional hazard regression.
Moreover, as can be seen in the procedure section, the children’s and parents’ psychopathological symptoms were input into a forward stepwise multivariate Cox proportional hazard regression (see Table 2) to establish which symptomatic manifestation showed the highest predictive value for the occurrence of a physical problem. The results indicated that offspring dissociation was the most significant predictor for the occurrence of relevant physical problems after controlling for sex and age. The most prevalent physical problem was respiratory symptoms (54%), followed by gastrointestinal diseases (35%) and cardiovascular diseases (11%).

TABLE 1B. Number of cases with relevant physical problems at each follow-up assessment point.
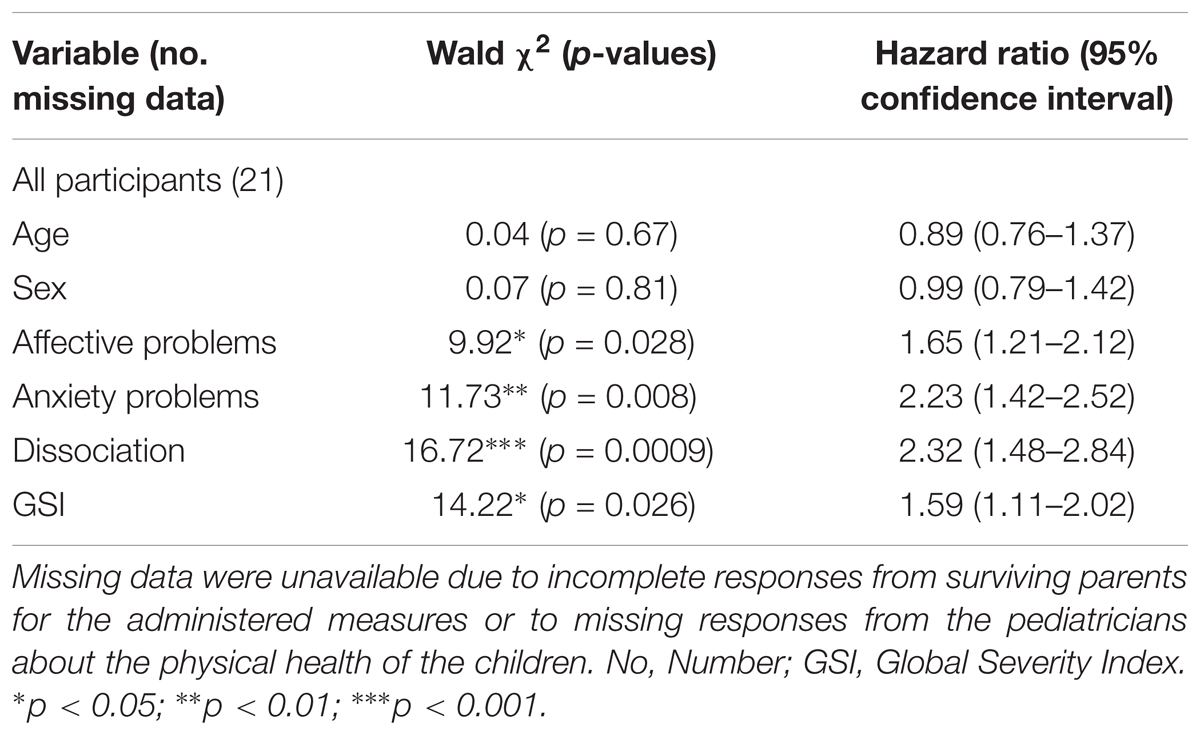
TABLE 2. Predictive value of age, sex, and psychopathological symptoms for the occurrence of a relevant physical problem: Multivariate Cox proportional hazard (forward) regression.
Discussion
The loss of a parent in childhood is one of the most significant painful events for a child’s emotional development. Several studies have highlighted that individuals who have lost a parent in early childhood have a greater risk of developing depressive symptoms in adolescence (Melhem et al., 2007, 2008) and that this loss also affects physical health (Abdelnoor and Hollins, 2004). However, there are few studies interested in the possible mechanisms underlying the associations between parental loss and subsequent mental and physical health (Luecken et al., 2009; Sachs-Ericsson et al., 2017) or evidencing the central role of ongoing stress exposure (Raposa et al., 2014). The current longitudinal study aims to understand better the link between parental death during childhood and physical illness during adolescence, considering the role played by the psychological profiles of surviving parents and offspring. In particular, this study aims to assess the possible predictive values of children’s and parental psychopathological symptoms for the occurrence of physical problems in adolescents.
To examine the predictive values of offspring’s and parents’ psychopathological symptoms, dissociation, and demographic characteristics (sex and age) for the occurrence of physical problems during a 6-year period, we carried out a univariate Cox proportional hazard regression analysis with time-dependent variables. Results showed that, regardless of sex, offspring’s affective problems and dissociation and parents’ GSI were risk factors for the occurrence of relevant physical problems.
With regard to the surviving parent’s psychopathological risk, the international literature has underlined that a relationship characterized by warmth, emotional support, and acceptance (i.e., positive or effective parenting) is associated with lower psychopathological difficulties in bereaved children and adolescents (Hagan et al., 2011, 2012). By contrast, a surviving parent who is struggling emotionally herself/himself over the loss of his/her partner may be less sensitive and supportive to grief-related emotions in their children (Werner-Lin and Biank, 2013). The ways in which the surviving parent faces the loss of their own partner influence how their children handle mourning (Kirwin and Hamrin, 2005) and their adaptation to life (Saldinger et al., 2004). Furthermore, a parent with a psychological problem may provide a family environment that does not promote their children’s emotional regulation, leading children to develop ineffective emotional regulation strategies (Luecken et al., 2005), resulting in excessive emotional and physiological reactivity to later stress in adolescence (Luecken et al., 2009). In addiction, interestingly, several studies have found that parental roles and couple dynamics are associated with children’s healthy behaviors and adherence to medical regimes, which are critical elements of cardiovascular rehabilitation (Martire and Helgeson, 2017; Smith and Baucom, 2017).
Our findings would seem to confirm the influence of parental psychological difficulties and the emotional problems of children on their physical health. In order to understand the predictive value of these variables better and to determine which psychopathological symptom was the most significant predictor of physical problems, we used all significant psychopathological predictors found in the univariate analysis in a forward stepwise multivariate Cox proportional hazard regression. Results showed that offspring dissociation was the most significant predictor for the occurrence of relevant physical problems after controlling for sex and age.
According to our study, both the psychopathological parental risk and the youth dissociation contribute to physical problems, although the main predictor of these is dissociation. We can assume that the traumaticity of the event involves not only the loss of the parent but also the consequent change in the relationship with the surviving parent. In addition, Schimmenti and Caretti (2016) have suggested that dissociation is a key variable in understanding clinical disorders that have their roots in relationally traumatic experiences during childhood. The authors, focusing on emotionally traumatic experiences during childhood, emphasized how dissociation could, paradoxically, protect the child through multiple disconnections in the self, which occur at both a mental and bodily level. Furthermore, Schimmenti (2017) has argued that excessive activation of dissociative processes following interpersonal trauma during childhood can hinder cognitive and affective treatment of information and the integration of mental, behavioral, and somatic states, including at the neurobiological level (Frewen et al., 2008). This may result in an increased risk of emotional dysregulation and exposure to further traumatic experiences, resulting in maladaptive developments. Putnam (1997) stressed how these alterations in consciousness reflect an inability to integrate or combine information and experiences in a normally predictable way. Therefore, thoughts and emotions are disconnected, somatic sensations are outside conscious awareness, and behavioral repetitions occur without deliberate choice, planning, or self-consciousness (Cook et al., 2017).
It is important to note that, in our sample, it appears that dissociating symptoms predict physical diseases in the specific period of puberty. Adolescence makes its debut with puberty. In this period, there are two changes that are fundamental to the psychophysical development of the individual: pubertal development and the consolidation of logical-formal thinking that makes it possible to organize the contents of the experience. Boys and girls go through a rapid and often unexpected bodily maturation, with the consequent modification of the relationship with themselves that is often perceived as outside their control. In addition, during adolescence, the maturation of cognitive structures and functions allows the acquisition of concepts, such as irreversibility and causality of events, connected with the concept of death (Corr, 1995), allowing a re-elaboration and control of childhood traumas.
On the basis of our results and Bucci’s (2003) multiple code theory, we hypothesized that the dissociative defense used by a child during childhood manifests itself in adolescence with a greater difficulty in understanding her/his emotions, which can manifest itself in physical symptoms. In this respect, further research should also take into account the alexithymic difficulties in adolescents who have lost a parent in childhood.
The present study has some limitations. First, the gender of the missing parent was not considered. Weller et al. (1991) found that children who lost their father figure had more symptoms of depression than did children who lost their mother. However, the scientific literature contains conflicting data. Some studies found that higher adolescent psychopathological risk was associated with the early death of the mother rather than the father (Brown et al., 1977; Kunugi et al., 1995), while other studies highlighted that losing the same-sex parent in childhood had a greater negative impact (Takeuchi et al., 2003). These conflicting results may be linked to the second limitation of this study: The cause of parent’s death was not considered, and it is possible that different causes of death lead to very different living environments for the child. As Dowdney (2000) points out, it is important to investigate how the parent’s death occurred, such as whether there was murder, suicide, or death after a long illness. Third, our research did not take into account the social network that could have been of support to adolescents during their development; a good relationship with the extended family and/or peers could be important protection factors.
On the other hand, this study has several strengths. In particular, this is a longitudinal study, which takes into consideration a large sample of children who have lost a parent in early childhood, following them with assessments until early adolescence. Numerous studies have in fact underlined the importance of this delicate passage (Blos, 1977), with the consequent modifications linked to puberty. Furthermore, in these assessments, we evaluated both the psychopathological symptoms of parents and children, as well as the offsprings’ physical symptoms, taking into consideration various channels of symptomatic manifestation, in a period of development in which the body becomes a central element in the manifestation of individual suffering. These results can be relevant and add to the previous literature in the field of prevention and intervention practices in samples of adolescents who lost a parent in their early childhood, orientating clinical work.
Author Contributions
MT designed the study and wrote the draft of the introduction section. LC wrote the introduction and the methods sections. SC wrote the discussion section and the draft of the introduction section. GB and EM performed statistical analyses. RT supervised the study and approved the final draft.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Abdelnoor, A., and Hollins, S. (2004). The effect of childhood bereavement on secondary school performance. Educ. Psychol. Pract. 20, 43–54. doi: 10.1080/0266736042000180401
Abraham, K. (1924). A Short Study of the Development of the Libido, Viewed in the Light of Mental Disorders. Selected Papers on Psychoanalysis, (New York, NY: Basic Books), 418–479.
Achenbach, T. M., and Rescorla, L. A. (2001). Manual for the ASEBA School–Age Forms & Profiles. Burlington, VT: University of Vermont.
Adejuwon, G. A. (2010). Consequences of childhood adversity on health concerns in adulthood. IFE Psychol. 18, 55–73. doi: 10.4314/ifep.v18i1.51652
Ahern, N. R., Ark, P., and Byers, J. (2008). Resilience and coping strategies in adolescents additional content. J. Ped. Nur. 20, 51–58.
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., et al. (2006). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 256, 174–186. doi: 10.1007/s00406-005-0624-4
Babore, A., Trumello, C., Candelori, C., Paciello, M., and Cerniglia, L. (2016). Depressive symptoms, self-esteem and perceived parent–child relationship in early adolescence. Front. Psychol. 7:982. doi: 10.3389/fpsyg.2016.00982
Beam, M. R., Servaty-Seib, H. L., and Mathwes, L. (2004). Parental loss and eating-related cognitions and behaviors in college-age women. J. Loss Trauma 9, 247–255. doi: 10.1080/15325020490458336
Berg, L., Rostila, M., Saarela, J., and Hjern, A. (2014). Parental death during childhood and subsequent school performance. Pediatrics 133, 682–689. doi: 10.1542/peds.2013-2771
Bergly, T. H., Nordfjærn, T., and Hagen, R. (2013). The dimensional structure of SCL-90-R in a sample of patients with substance use disorder. J. Subst. Use 19, 257–261. doi: 10.3109/14659891.2013.790494
Biank, N. M., and Werner-Lin, A. (2011). Growing up with grief: revisiting the death of a parent over the life course. Omega 63, 271–290. doi: 10.2190/OM.63.3.e
Bifulco, A. T., Brown, G. W., and Harris, T. O. (1987). Childhood loss of parent, lack of adequate parental care and adult depression: a replication. J. Affect. Disord. 12, 115–128. doi: 10.1016/0165-0327(87)90003-6
Blos, P. (1977). When and how does adolescence end: Structural criteria for adolescent closure. Adolesc. Psychiatry 5, 5–17.
Bornstein, M. H., and Bradley, R. H. (2003). Socioeconomic Status, Parenting, and Child Development. Mahwah, NJ: Routledge.
Bowlby, J. (1960). “Grief and mourning in infancy and early childhood,” in The Psychoanalytic Study of the Child, Vol. 15, eds R. Eissler, S. Freud, H. Hartmann, and E. Krk (New York, NY: International University Press), 9–52.
Bowlby, J. (1980). Attachment and Loss: Loss, sadness and Depression, Vol. 3. New York, NY: Basic Books.
Breier, A., Kelsoe, J. R., Kirwin, P. D., Beller, S. A., Wolkowitz, O. M., and Pickar, D. (1988). Early parental loss and the development of adult psychopathology. Arch. Gen. Psychiatry 45, 987–993. doi: 10.1001/archpsyc.1988.01800350021003
Brent, D. A., Melhem, N. M., Masten, A. S., Porta, G., and Payne, M. W. (2012). Longitudinal effects of parental bereavement on adolescent developmental competence. J. Clin. Child Adolesc. Psychol. 41, 778–791. doi: 10.1080/15374416.2012.717871
Brown, F. (1966). Childhood bereavement and subsequent psychiatric disorder. Br. J. Psychiatry 112, 1043–1048. doi: 10.1192/bjp.112.491.1043
Brown, G. W., and Harris, T. (1978). Social origins of depression: a reply. Psychol. Med. 8, 577–588. doi: 10.1017/S0033291700018791
Brown, G. W., Harris, T., and Copeland, J. R. (1977). Depression and loss. Br. J. Psychiatry 130, 1–18. doi: 10.1192/bjp.130.1.1
Bucci, W. (2003). Varieties of dissociative experiences: a multiple code account and a discussion of Bromberg’s case of”. William”. Psychoanal. Psychol. 20, 542–557. doi: 10.1037/0736-9735.20.3.542
Bylund-Grenklo, T., Fürst, C. J., Nyberg, T., Steineck, G., and Kreicbergs, U. (2016). Unresolved grief and its consequences. A nationwide follow-up of teenage loss of a parent to cancer 6–9 years earlier. Support. Care Cancer 24, 3095–3103. doi: 10.1007/s00520-016-3118-1
Cas, G. A., Frankenberg, E., Suriastini, W., and Thomas, D. (2013). The Problems of Parental Death on Child Well-being: Evidence from the Indian Ocean Tsunami. Washington, DC: World Bank.
Cassel, J. (2017). “Physical illness in response to stress,” in Reason and Controversy in the Arts, ed. M. R. Kadish (Cleveland, OH: The Press of Case Western Reserve University), 189–209.
Cerniglia, L., Cimino, S., Ballarotto, G., Casini, E., Ferrari, A., Carbone, P., et al. (2015). Motor vehicle accidents and adolescents: an empirical study on their emotional and behavioral profiles, defense strategies and parental support. Transp. Res. Part F Traffic Psychol. Behav. 35, 28–36. doi: 10.1016/j.trf.2015.09.002
Cerniglia, L., Cimino, S., Ballarotto, G., and Monniello, G. (2014). Parental loss during childhood and outcomes on adolescents’ psychological profiles: a longitudinal study. Curr. Psychol. 33, 545–556. doi: 10.1007/s12144-014-9228-3
Cerniglia, L., Cimino, S., Tafà, M., Marzilli, E., Ballarotto, G., and Bracaglia, F. (2017a). Family profiles in eating disorders: family functioning and psychopathology. Psychol. Res. Behav. Manag. 10, 305–312. doi: 10.2147/PRBM.S145463
Cerniglia, L., Zoratto, F., Cimino, S., Laviola, G., Ammaniti, M., and Adriani, W. (2017b). Internet addiction in adolescence: neurobiological, psychosocial and clinical issues. Neurosci. Biobehav. Rev. 76, 174–184. doi: 10.1016/j.neubiorev.2016.12.024
Cimino, S., Cerniglia, L., Paciello, M., and Sinesi, S. (2012a). A six-year prospective study on children of mothers with eating disorders: the role of paternal psychological profiles. Eur. Eat. Disord. Rev. 21, 238–246. doi: 10.1002/erv.2218
Cimino, S., Monniello, G., and Sinesi, S. (2012b). La perdita di un genitore nell’infanzia: uno studio empirico su un campione di pre-adolescenti. Psichiatr. Infanz. Adolesc. 79, 398–410.
Cipriano, D. J., and Cipriano, M. R. (2017). Factors underlying the relationship between parent and child grief. Omega. doi: 10.1177/0030222817726935 [Epub ahead of print]
Compas, B. E., Connor-Smith, J. K., Saltzman, H., Thomsen, A. H., and Wadsworth, M. E. (2001). Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research. Psychol. Bull. 127, 87–127. doi: 10.1037//0033-2909.127.1.87
Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., Cloitre, M., et al. (2017). Complex trauma in children and adolescents. Psychiatr. Ann. 35, 390–398. doi: 10.3928/00485713-20050501-05
Corr, C. A. (1995). “Entering into adolescent understandings of death,” in Bereaved Children and Teens: A Support Guide for Parents and Professionals, ed. E. A. Grollman (Boston, MA: Beacon), 21–35.
Danese, A., and McEwen, B. S. (2012). Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiol. Behav. 106, 29–39. doi: 10.1016/j.physbeh.2011.08.019
Derogatis, L. R. (1994). Symptom Checklist 90-R: Administration, Scoring and Procedures Manual. Minneapolis, MN: National Computer Systems.
Dowdney, L. (2000). Annotation: childhood bereavement following parental death. J. Child Psychol. Psychiatry. 41, 819–830. doi: 10.1111/1469-7610.00670
Eisenberg, N., Cumberland, A., Spinrad, T. L., Fabes, R. A., Shepard, S. A., Reiser, M., et al. (2001). The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Dev. 72, 1112–1134. doi: 10.1111/1467-8624.00337
Ellis, J., Dowrick, C., and Lloyd-Williams, M. (2013). The long-term impact of early parental death: lessons from a narrative study. J. R. Soc. Med. 106, 57–67. doi: 10.1177/0141076812472623
Faravelli, C., Webb, T., Ambonetti, A., Fonnesu, F., and Sessarego, A. (1985). Prevalence of traumatic early life in 31 agoraphobic patients with panic attack. Am. J. Psychiatry 142, 1493–1494. doi: 10.1176/ajp.142.12.1493
Feigelman, W., Rosen, Z., Joiner, T., Silva, C., and Mueller, A. S. (2017). Examining longer-term effects of parental death in adolescents and young adults: evidence from the National Longitudinal Survey of Adolescent to Adult Health. Death Stud. 41, 133–143. doi: 10.1080/07481187.2016.1226990
Felitti, V. J. (2009). Adverse childhood experiences and adult health. Acad. Pediatr. 9, 131–132. doi: 10.1016/j.acap.2009.03.001
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Valerie, E., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) Study. Am. J. Prev. Med. 14, 245–258. doi: 10.1016/S0749-3797(98)00017-8
Felner, R. D., Terre, L., and Rowlison, R. T. (1988). “A life transition framework for understanding marital dissolution and family reorganization,” in Children of Divorce: Empirical Perspectives on Adjustment, eds S. A. Wolchik and P. Kauroly (New York, NY: Gardner Press), 35–65.
Flaherty, E. G., Thompson, R., Dubowitz, H., Harvey, E. M., English, D. J., Proctor, L. J., et al. (2013). Adverse childhood experiences and child health in early adolescence. JAMA Pediatr. 167, 622–629. doi: 10.1001/jamapediatrics.2013.22
Frewen, P. A., Lanius, R. A., Dozois, D. J., Neufeld, R. W., Pain, C., Hopper, J. W., et al. (2008). Clinical and neural correlates of alexithymia in posttraumatic stress disorder. J. Abnorm. Psychol. 117, 171–181. doi: 10.1037/0021-843X.117.1.171
Frigerio, A., Cattaneo, C., Cataldo, M., Schiatti, A., Molteni, M., and Battaglia, M. (2004). Behavioral and emotional problems among Italian children and adolescents aged 4 to 18 years as reported by parents and teachers. Eur. J. Psychol. Assess. 20, 124–133. doi: 10.1027/1015-5759.20.2.124
Goodman, S. (2002). “Depression and early adverse experiences,” in Handbook of Depression, eds I. Gotlib and C. Hammen (New York, NY: Guilford Press), 245–267.
Hagan, M. J., Roubinov, D. S., Gress-Smith, J., Luecken, L. J., Sandler, I. N., and Wolchik, S. (2011). Positive parenting during childhood moderates the impact of recent negative events on cortisol activity in parentally bereaved youth. Psychopharmacology 214, 231–238. doi: 10.1007/s00213-010-1889-5
Hagan, M. J., Tein, J. Y., Sandler, I. N., Wolchik, S. A., Ayers, T. S., and Luecken, L. J. (2012). Strengthening effective parenting practices over the long term: effects of a preventive intervention for parentally bereaved families. J. Clin. Child Adolesc. Psychol. 41, 177–188. doi: 10.1080/15374416.2012.651996
Haine, R. A., Ayers, T. S., Sandler, I. N., and Wolchik, S. A. (2008). Evidence-based practices for parentally bereaved children and their families. Prof. Psychol. Res. Pr. 39, 113–121. doi: 10.1037/0735-7028.39.2.113
Haine, R. A., Wolchik, S. A., Sandler, I. N., Millsap, R. E., and Ayers, T. S. (2006). Positive parenting as a protective resource for parentally bereaved children. Death Stud. 30, 1–28. doi: 10.1080/07481180500348639
Hannigan, L. J., Walaker, N., Waszczuk, M. A., McAdams, T. A., and Eley, T. C. (2017). Aetiological influences on stability and change in emotional and behavioural problems across development: a systematic review. Psychopathol. Rev. 4, 52–108. doi: 10.5127/pr.038315
Harris, T., Brown, G. W., and Bifulco, A. (1986). Loss of parent in childhood and adult psychiatric disorder: the role of lack of adequate parental care. Psychol. Med. 16, 641–659. doi: 10.1017/S0033291700010394
Isohookana, R., Marttunen, M., Hakko, H., Riipinen, P., and Riala, K. (2016). The impact of adverse childhood experiences on obesity and unhealthy weight control behaviors among adolescents. Compr. Psychiatry 71, 17–24. doi: 10.1016/j.comppsych.2016.08.002
Jacobs, J. R., and Bovasso, G. B. (2009). Re-examining the long-term effects of experiencing parental death in childhood on adult psychopathology. J. Nerv. Ment. Dis. 197, 24–27. doi: 10.1097/NMD.0b013e3181927723
Kaplow, J. B., Saunders, J., Angold, A., and Costello, E. J. (2010). Psychiatric symptoms in bereaved versus nonbereaved youth and young adults: a longitudinal epidemiological study. J. Am. Acad. Child Adolesc. Psychiatry 49, 1145–1154. doi: 10.1016/j.jaac.2010.08.004
Kendler, K. S., Neale, M. C., Kessler, R. C., Heath, A. C., and Eaves, L. J. (1992). Childhood parental loss and adult psychopathology in women. A twin study perspective. Arch. Gen. Psychiatry 49, 109–116. doi: 10.1001/archpsyc.1992.01820020029004
Kirwin, K. M., and Hamrin, V. (2005). Decreasing the risk of complicated bereavement and future psychiatric disorders in children. J. Child Adolesc. Psychiatr. Nurs. 18, 62–78. doi: 10.1111/j.1744-6171.2005.00002.x
Kunugi, H., Sugawara, N., Aoki, H., Nanko, S., Hirose, T., and Kazamatsuri, H. (1995). Early parental loss and depressive disorder in Japan. Eur. Arch. Psychiatry. Clin. Neurosci. 245, 109–113. doi: 10.1007/BF0219073
Kwok, O. M., Haine, R. A., Sandler, I. N., Ayers, T. S., Wolchik, S. A., and Tein, J. Y. (2005). Positive parenting as a mediator of the relations between parental psychological distress and mental health problems of parentally bereaved children. J. Clin. Child. Adolesc. Psychol. 34, 260–271. doi: 10.1207/s15374424jccp3402_5
Li, J., Vestergaard, M., Cnattingius, S., Gissler, M., Bech, B. H., Obel, C., et al. (2014). Mortality after parental death in childhood: a nationwide cohort study in three Nordic countries. PLoS Med. 11:e1001679. doi: 10.1371/journal.pmed.1001679
Lin, K. K., Sandler, I. N., Ayers, T. S., Wolchik, S. A., and Luecken, L. J. (2004). Resilience in parentally bereaved children and adolescents seeking preventive services. J. Clin. Child. Adolesc. Psychol. 33, 673–683. doi: 10.1207/s15374424jccp3304_3
Luecken, L. J. (2008). “Long-term consequences of parental death in childhood: psychological and physiological manifestations,” in Handbook of Bereavement Research and Practice: Advances in Theory and Intervention, eds M. S. Stroebe, R. O. Hansson, H. Schut, and W. Stroebe (Washington, DC: American Psychological Association), 397–416.
Luecken, L. J., Kraft, A., Appelhans, B. M., and Enders, C. (2009). Emotional and cardiovascular sensitization to daily stress following childhood parental loss. Dev. Psychol. 45, 296–302. doi: 10.1037/a0013888
Luecken, L. J., and Lemery, K. S. (2004). Early caregiving and physiological stress responses. Clin. Psychol. Rev. 24, 171–191. doi: 10.1016/j.cpr.2004.01.003
Luecken, L. J., Rodriquez, A., and Appelhans, B. M. (2005). Cardiovascular stress responses in young adulthood associated with family-of-origin relationships. Psychosom. Med. 67, 514–521. doi: 10.1097/01.psy.0000160466.10397.18
Luecken, L. J., and Roubinov, D. S. (2012). Pathways to lifespan health following childhood parental death. Soc. Personal. Psychol. 6, 243–257. doi: 10.1111/j.1751-9004.2011.00422.x
Maier, E. H., and Lachman, M. E. (2000). Consequences of early parental loss and separation for health and well-being in midlife. Int. J. Behav. Dev. 24, 183–189. doi: 10.1080/016502500383304
Martire, L. M., and Helgeson, V. S. (2017). Close relationships and the management of chronic illness: associations and interventions. Am. Psychol. 72, 601–612. doi: 10.1037/amp0000066
McEwen, B. S., and Lasley, E. N. (2002). The End of Stress as We Know it. Washington, DC: Joseph Henry Press.
McLaughlin, K. A., Green, J. G., Gruber, M., Sampson, N., Zaslavsky, A. K., and Kessler, R. C. (2012). Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents. Arch. Gen. Psychiatry 69, 1151–1160. doi: 10.1001/archgenpsychiatry.2011.2277
Melhem, N. M., Moritz, G., Walker, M., Shear, M. K., and Brent, D. (2007). Phenomenology and correlates of complicated grief in children and adolescents. J. Am. Acad. Child Adolesc. Psychiatry 46, 493–499. doi: 10.1097/chi.0b013e31803062a9-
Melhem, N. M., Walker, M., Moritz, G., and Brent, D. A. (2008). Antecedents and sequelae of sudden parental death in offspring and surviving caregivers. Arch. Pediatr. Adolesc. Med. 162, 403–410. doi: 10.1001/archpedi.162.5.403
Nickerson, A., Bryant, R. A., Aderka, I. M., Hinton, D. E., and Hofmann, S. G. (2013). The impacts of parental loss and adverse parenting on mental health: findings from the National Comorbidity Survey-Replication. Psychol. Trauma 5, 119–127. doi: 10.1037/a0025695
Peduzzi, P., Concato, J., Feinstein, A. R., and Holford, T. R. (1995). Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J. Clin. Epidemiol. 48, 1503–1510. doi: 10.1016/0895-4356(95)00048-8
Pendry, P., and Adam, E. K. (2007). Associations between parents’ marital functioning, maternal parenting quality, maternal emotion and child cortisol levels. Int. J. Behav. Dev. 31, 218–231. doi: 10.1177/0165025407074634
Plass-Christl, A., Haller, A. C., Otto, C., Barkmann, C., Wiegand-Grefe, S., Hölling, H., et al. (2017). Parents with mental health problems and their children in a German population based sample: results of the BELLA study. PLoS One 12:e0180410. doi: 10.1371/journal.pone.0180410
Prunas, A., Sarno, I., Preti, E., Madeddu, F., and Perugini, M. (2012). Psychometric properties of the Italian version of the SCL-90-R: a study on a large community sample. Eur. Psychiatry 27, 591–597. doi: 10.1016/j.eurpsy.2010.12.006
Putnam, F. W. (1997). Dissociation in Children and Adolescents: A Developmental Perspective. New York, NY: The Guilford Press.
Putnam, F. W., Helmers, K., and Trickett, P. K. (1993). Development, reliability, and validity of a child dissociation scale. Child Abuse Negl. 17, 731–741. doi: 10.1016/S0145-2134(08)80004-X
Raposa, E. B., Hammen, C. L., Brennan, P. A., O’callaghan, F., and Najman, J. M. (2014). Early adversity and health outcomes in young adulthood: the role of ongoing stress. Health Psychol. 33, 410–418. doi: 10.1037/a0032752
Rostila, M., and Saarela, J. M. (2011). Time does not heal all wounds: mortality following the death of a parent. J. Marriage Fam. 73, 236–249. doi: 10.1111/j.1741-3737.2010.00801.x
Rutter, M. (1996). Transitions and turning points in developmental psychopathology: as applied to the age span between childhood and mid-adulthood. Int. J. Behav. Dev. 19, 603–626. doi: 10.1177/016502549601900309
Sachs-Ericsson, N. J., Sheffler, J. L., Stanley, I. H., Piazza, J. R., and Preacher, K. J. (2017). When emotional pain becomes physical: adverse childhood experiences, pain, and the role of mood and anxiety disorders. J. Clin. Psychol. 73, 1403–1428. doi: 10.1002/jclp.22444
Saldinger, A., Porterfield, K., and Cain, A. C. (2004). Meeting the needs of parentally bereaved children: a framework for child–centered parenting. Psychiatry 67, 331–352. doi: 10.1521/psyc.67.4.331.56562
Schimmenti, A. (2017). The trauma factor: examining the relationships among different types of trauma, dissociation, and psychopathology. J. Trauma Dissociation 11, 1–20. doi: 10.1080/15299732.2017.1402400
Schimmenti, A., and Caretti, V. (2016). Linking the overwhelming with the unbearable: developmental trauma, dissociation, and the disconnected self. Psychoanal. Psychol. 33, 106–128. doi: 10.1037/a0038019
Schoenfelder, E. N., Sandler, I. N., Wolchik, S., and MacKinnon, D. (2011). Quality of social relationships and the development of depression in parentally-bereaved youth. J. Youth Adolesc. 40, 85–96. doi: 10.1007/s10964-009-9503-z
Scott, K. M., Von Korff, M., Angermeyer, M. C., Benjet, C., Bruffaerts, R., De Girolamo, G., et al. (2011). Association of childhood adversities and early-onset mental disorders with adult-onset chronic physical conditions. Arch. Gen. Psychiatry 68, 838–844. doi: 10.1001/archgenpsychiatry.2011.77
Serafini, G., Muzio, C., Piccinini, G., Flouri, E., Ferrigno, G., Pompili, M., et al. (2015). Life adversities and suicidal behavior in young individuals: a systematic review. Eur. Child Adolesc. Psychiatry 24, 1423–1446. doi: 10.1007/s00787-015-0760-y
Smith, K. R., Hanson, H. A., Norton, M. C., Hollingshaus, M. S., and Mineau, G. P. (2014). Survival of offspring who experience early parental death: early life conditions and later-life mortality. Soc. Sci. Med. 119, 180–190. doi: 10.1016/j.socscimed.2013.11.054
Smith, T. W., and Baucom, B. R. (2017). Intimate relationships, individual adjustment, and coronary heart disease: implications of overlapping associations in psychosocial risk. Am. Psychol. 72, 578–589. doi: 10.1037/amp0000123
Spitz, R. A. (1945). “Hospitalism,” in The Psychoanalytic Study of the Child, eds R. S. Eissler, A. Freud, H. Hartmann, and E. Kris (New York, NY: International University Press), 52–74.
Spitz, R. A., and Wolf, K. M. (1946). “Anaclitic depression: an inquiry into the genesis of psychiatric conditions in early childhood,” in The Psychoanalytic Study of the Child, Vol. 2, eds R. S. Eissler, A. Freud, H. Hartamann, and E. Kris (New York, NY: International University Press), 313–341. doi: 10.1080/00797308.1946.11823551
Stikkelbroek, Y., Prinzie, P., de Graaf, R., ten Have, M., and Cuijpers, P. (2012). Parental death during childhood and psychopathology in adulthood. Psychiatry Res. 198, 516–520. doi: 10.1016/j.psychres.2011.10.024
Tafà, M., Cimino, S., Ballarotto, G., Bracaglia, F., Bottone, C., and Cerniglia, L. (2017). Female adolescents with eating disorders, parental psychopathological risk and family functioning. J. Child Fam. Stud. 26, 28–39. doi: 10.1007/s10826-016-0531-5
Takeuchi, H., Hiroe, T., Kanai, T., Morinobu, S., Kitamura, T., Takahashi, K., et al. (2003). Childhood parental separation experiences and depressive symptomatology in acute major depression. Psychiatry Clin. Neurosci. 57, 215–219. doi: 10.1046/j.1440-1819.2003.01103.x
Tottenham, N., Hare, T. A., Millner, A., Gilhooly, T., Zevin, J. D., and Casey, B. J. (2011). Elevated amygdala response to faces following early deprivation. Dev. Sci. 14, 190–204. doi: 10.1111/j.1467-7687.2010.00971.x
van de Pavert, I., Sunderland, M., Luijten, M., Slade, T., and Teesson, M. (2017). The general relationship between internalizing psychopathology and chronic physical health conditions: a population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 52, 1257–1265. doi: 10.1007/s00127-017-1422-9
van der Pol, L. D., Groeneveld, M. G., Endendijk, J. J., van Berkel, S. R., Hallers-Haalboom, E. T., Bakermans-Kranenburg, M. J., et al. (2016). Associations between fathers’ and mothers’ psychopathology symptoms, parental emotion socialization, and preschoolers’ social-emotional development. J. Child Fam. Stud. 25, 3367–3380. doi: 10.1007/s10826-016-0490-x
von Sydow, K., Lieb, R., Pfister, H., Höfler, M., and Wittchen, H. U. (2002). What predicts incident use of cannabis and progression to abuse and dependence?: A 4-year prospective examination of risk factors in a community sample of adolescents and young adults. Drug Alcohol Depend. 68, 49–64. doi: 10.1016/j.drugalcdep.2011.10.013
Weller, R. A., Weller, E. B., Fristad, M. A., and Bowes, J. M. (1991). Depression in recently bereaved prepubertal children. Am. J. Psychiatry 148, 1536–1540. doi: 10.1176/ajp.148.11.1536
Werner-Lin, A., and Biank, N. M. (2013). Holding parents so they can hold their children: grief work with surviving spouses to support parentally bereaved children. OMEGA 66, 1–16. doi: 10.1017/S1478951508000060
Williams, L. D., and Aber, J. L. (2016). Testing for plausibly causal links between parental bereavement and child socio-emotional and academic outcomes: a propensity-score matching model. J. Abnorm. Child Psychol. 44, 705–718. doi: 10.1007/s10802-015-0069-9
Wolchik, S. A., Ma, Y., Tein, J. Y., Sandler, I. N., and Ayers, T. S. (2008). Parentally bereaved children’s grief: self-system beliefs as mediators of the relations between grief and stressors and caregiver–child relationship quality. Death Stud. 32, 597–620. doi: 10.1080/07481180802215551
Keywords: parental loss, psychopathological risk, physical illness, hazard regression analysis, adolescence
Citation: Tafà M, Cerniglia L, Cimino S, Ballarotto G, Marzilli E and Tambelli R (2018) Predictive Values of Early Parental Loss and Psychopathological Risk for Physical Problems in Early Adolescents. Front. Psychol. 9:922. doi: 10.3389/fpsyg.2018.00922
Received: 28 February 2018; Accepted: 18 May 2018;
Published: 06 June 2018.
Edited by:
Raffaella Calati, Centre Hospitalier Universitaire de Montpellier, FranceReviewed by:
Adriano Schimmenti, Kore University of Enna, ItalyCarmen María Galvez-Sánchez, Universidad de Jaén, Spain
Copyright © 2018 Tafà, Cerniglia, Cimino, Ballarotto, Marzilli and Tambelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Cerniglia, bC5jZXJuaWdsaWFAdW5pbmV0dHVub3VuaXZlcnNpdHkubmV0