Editorial
09 June 2022
Elisabeth M. W. Eekhoff
, Teun J. de Vries
, Ralph J. B. Sakkers
and
Wim Van Hul





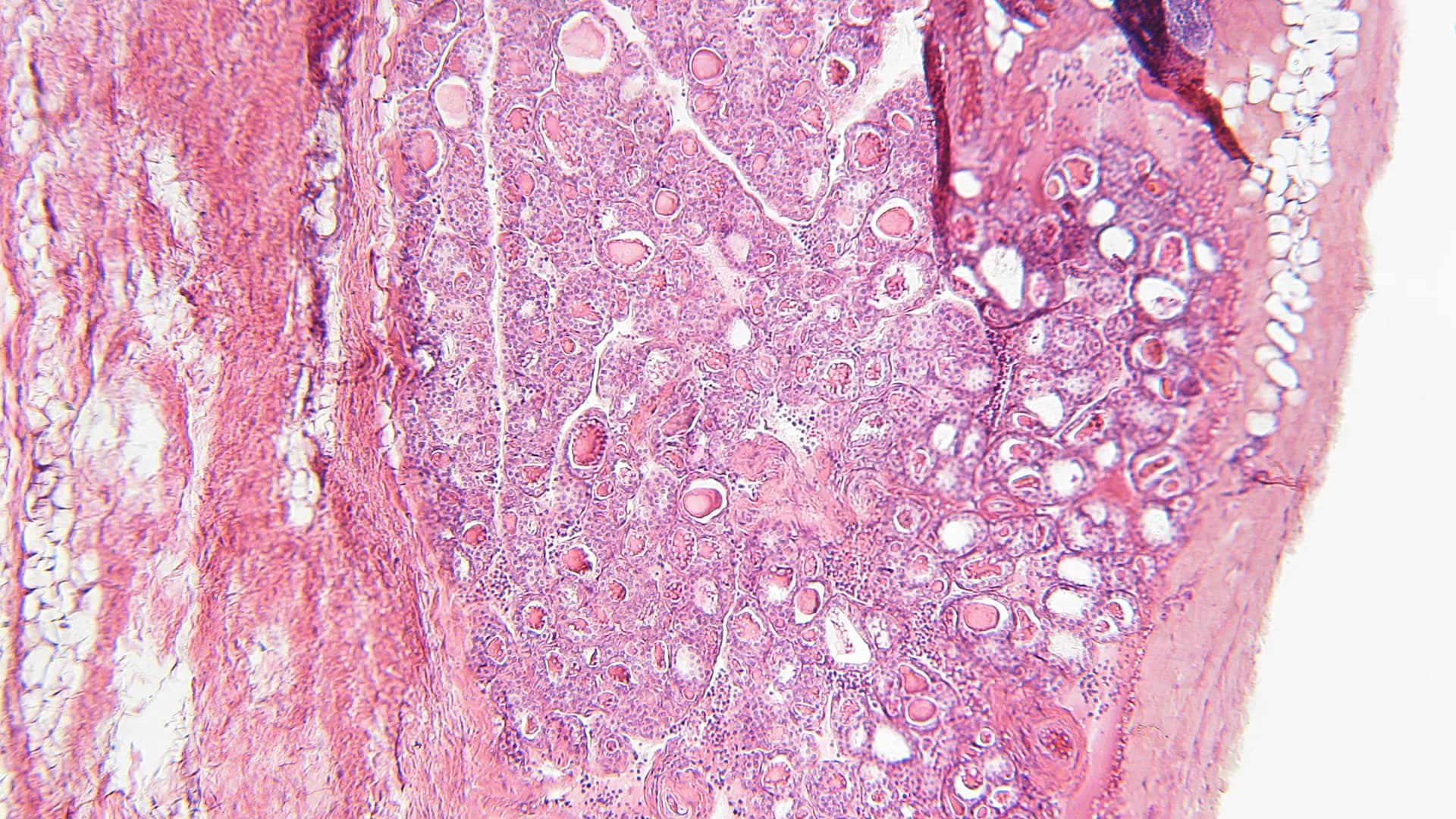
![Patient Care Rare Bone Disease ABC, Amsterdam UMC. FOP, fibrodysplasia ossificans progressiva; FD, fibrous dysplasia; OI, osteogenesis imperfecta; Her-OP, hereditary osteoporosis; ABC, Amsterdam bone Center; DXA, Dual X-ray absorptiometry; [18F] NaF PET/CT, 18F-Sodium Fluoride positron emission tomograph/-computed tomography; MRI, Magnetic resonance imaging; MDO, multidisciplinary consultation.](https://www.frontiersin.org/_rtmag/_next/image?url=https%3A%2F%2Fwww.frontiersin.org%2Ffiles%2FArticles%2F553977%2Ffendo-11-00481-HTML%2Fimage_m%2Ffendo-11-00481-g003.jpg&w=3840&q=75)


Osteogenesis imperfecta (OI) is the term used to describe a group of rare inherited skeletal disorders characterized by a greatly increased risk of fragility fractures (1). Mutations in several genes can cause OI but the condition is most commonly caused by mutations of COLIA1 or COL1A2 resulting in the production of collagen which is abnormal or present in reduced amounts. Fractures in OI are particularly common during childhood but the elevated fracture risk continues throughout life. Bone mineral density (BMD) can be reduced in OI but the magnitude of increase in fracture risk is far greater than can be accounted for by low BMD, highlighting that a key mechanism of bone fragility is reduced bone quality due to defects of bone matrix and mineralization. A multidisciplinary approach is needed to optimize management of OI, with input from physicians, orthopedic surgeons, physiotherapists, occupational therapists, and other allied health professionals. Orthopedic surgery plays a key role both in the fixation of fractures and in the correction of limb deformities. Bisphosphonates have been widely used in the treatment of children and adults with OI. Although there is good evidence that they increase BMD, it is uncertain to what extent they reduce fracture risk. Clinical trials of bone anabolic drugs such as teriparatide and inhibitors of sclerostin have also been studied; although they increase BMD, studies of these agents have not been powered to look at fracture endpoints. Various other treatment modalities including denosumab, and cell therapy have been explored but haven't gained acceptance in routine clinical practice. There have been huge advances in understanding the pathogenesis of OI but these have not been accompanied by advances in treatment. This signals need for well-designed clinical trials with fracture endpoints in OI, both with existing agents and with the newer therapeutic agents that are now starting to emerge.


A 24-year old man was referred to the Erasmus MC Bone Center because of an asymptomatic increasing skull defect of the left parietal bone. The defect was first noticed at the age of six, and gradually increased over the years. His medical history was unremarkable, without any known trauma and a negative family history for bone diseases. Laboratory tests showed a low vitamin D level without other abnormalities. Particularly, there was no increase in markers of inflammation or bone turnover. CT-scans of the skull showed an osteolytic region of the parietal skull bone, with a two-centimeter increase in diameter over 9 years. Contrast enhanced MRI showed lymphangiogenic invasion, which was compatible with our suspicion of Gorham-Stout disease. The patient was referred to the neurosurgeon for treatment with a bone graft while considering additional drug treatment. Gorham-Stout or vanishing bone disease is a rare entity characterized by progressive osteolysis with lymphangiogenic bone invasion. Although already reported in 1838, currently the diagnosis and treatment of Gorham-Stout disease is still challenging. The underlying pathophysiology is not clarified yet and several theories exist. The disease usually affects persons younger than 40 years and the majority present with bone disease of the maxillofacial region, the upper extremities or the torso. The clinical presentation includes most frequently pain, swelling, and functional impairment of the affected region, but the disease can also be asymptomatic. Laboratory investigations are usually normal, and diagnosis is based upon imaging and sometimes pathology examination of affected bone tissue. Treatment is experimental and there is no general consensus about the best option due to lack of randomized controlled trials. Case reports showed patients treated with bisphosphonates, interferon-alpha, anti-VEGF therapy, mTOR inhibitors, and radiotherapy. There are some reports of surgery with prosthetic or bone grafts but no long-term follow-up data exist. This paper describes a unique case of Gorham-Stout disease of the parietal skull bone and discusses the current state of knowledge about this rare bone disease.

The kyphosis angle of the thoracic spine tends to increase with aging. Hyperkyphosis is a kyphosis angle, exceeding the normal range. This narrative literature review aims to provide an overview of the current literature concerning kyphosis measurement methods, the etiology and adverse health effects of hyperkyphosis. As of yet, a well-defined threshold for hyperkyphosis is lacking. To attain more generalizability and to be able to compare study results in older adults, we propose to define age-related hyperkyphosis as a Cobb angle of 50° or more in standing position. Hyperkyphosis may be a potentially modifiable risk factor for adverse health outcomes, like fall risk and fractures. Additionally, hyperkyphosis may indicate the presence of osteoporosis, which is treatable. Prospective and intervention studies, using a Cobb angle of 50° as a clear and uniform definition of hyperkyphosis, are warranted to investigate the clinical relevance of hyperkyphosis.