Editorial
05 June 2018
Johannes W. Dietrich
, John E. M. Midgley
and
Rudolf Hoermann

In thyroid health, the pituitary hormone thyroid-stimulating hormone (TSH) raises glandular thyroid hormone production to a physiological level and enhances formation and conversion of T4 to the biologically more active T3. Overstimulation is limited by negative feedback control. In equilibrium defining the euthyroid state, the relationship between TSH and FT4 expresses clusters of genetically determined, interlocked TSH–FT4 pairs, which invalidates their statistical correlation within the euthyroid range. Appropriate reactions to internal or external challenges are defined by unique solutions and homeostatic equilibria. Permissible variations in an individual are much more closely constrained than over a population. Current diagnostic definitions of subclinical thyroid dysfunction are laboratory based, and do not concur with treatment recommendations. An appropriate TSH level is a homeostatic concept that cannot be reduced to a fixed range consideration. The control mode may shift from feedback to tracking where TSH becomes positively, rather than inversely related with FT4. This is obvious in pituitary disease and severe non-thyroid illness, but extends to other prevalent conditions including aging, obesity, and levothyroxine (LT4) treatment. Treatment targets must both be individualized and respect altered equilibria on LT4. To avoid amalgamation bias, clinically meaningful stratification is required in epidemiological studies. In conclusion, pituitary TSH cannot be readily interpreted as a sensitive mirror image of thyroid function because the negative TSH–FT4 correlation is frequently broken, even inverted, by common conditions. The interrelationships between TSH and thyroid hormones and the interlocking elements of the control system are individual, dynamic, and adaptive. This demands a paradigm shift of its diagnostic use.

The hypothalamus–pituitary–thyroid feedback control is a dynamic, adaptive system. In situations of illness and deprivation of energy representing type 1 allostasis, the stress response operates to alter both its set point and peripheral transfer parameters. In contrast, type 2 allostatic load, typically effective in psychosocial stress, pregnancy, metabolic syndrome, and adaptation to cold, produces a nearly opposite phenotype of predictive plasticity. The non-thyroidal illness syndrome (NTIS) or thyroid allostasis in critical illness, tumors, uremia, and starvation (TACITUS), commonly observed in hospitalized patients, displays a historically well-studied pattern of allostatic thyroid response. This is characterized by decreased total and free thyroid hormone concentrations and varying levels of thyroid-stimulating hormone (TSH) ranging from decreased (in severe cases) to normal or even elevated (mainly in the recovery phase) TSH concentrations. An acute versus chronic stage (wasting syndrome) of TACITUS can be discerned. The two types differ in molecular mechanisms and prognosis. The acute adaptation of thyroid hormone metabolism to critical illness may prove beneficial to the organism, whereas the far more complex molecular alterations associated with chronic illness frequently lead to allostatic overload. The latter is associated with poor outcome, independently of the underlying disease. Adaptive responses of thyroid homeostasis extend to alterations in thyroid hormone concentrations during fetal life, periods of weight gain or loss, thermoregulation, physical exercise, and psychiatric diseases. The various forms of thyroid allostasis pose serious problems in differential diagnosis of thyroid disease. This review article provides an overview of physiological mechanisms as well as major diagnostic and therapeutic implications of thyroid allostasis under a variety of developmental and straining conditions.


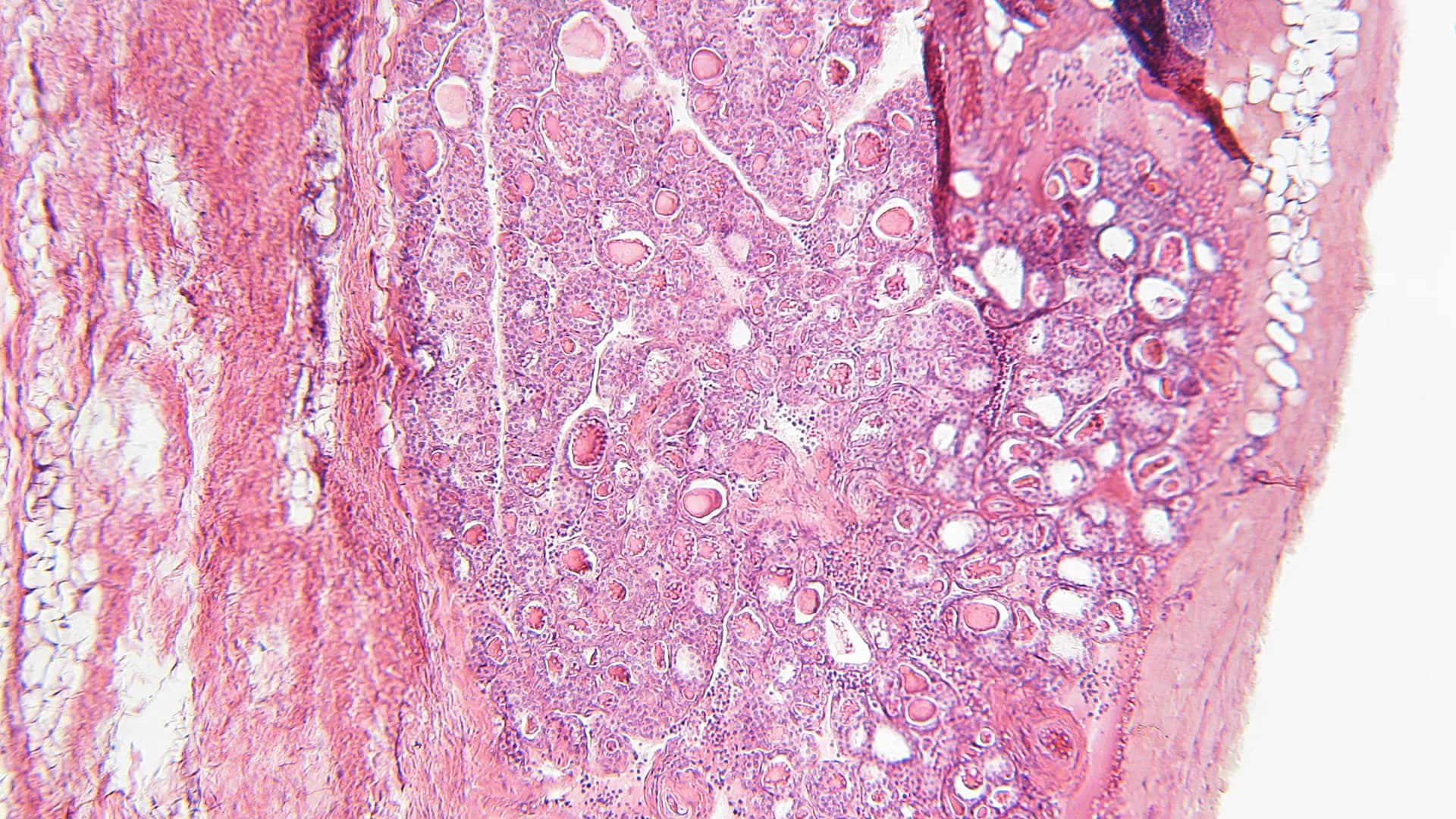
![Hysteresis model showing a clockwise loop formed by an ascending limb represented by the pink curve during recovery of severe thyrotoxicosis and a blue descending limb during recovery from severe hypothyroidism. The black curve represents the TSH response trajectory that can be followed with more gentle deviations of FT4 from the euthyroid set point indicated by the red diamond. [Figure adapted from Ref. (30)].](https://www.frontiersin.org/_rtmag/_next/image?url=https%3A%2F%2Fwww.frontiersin.org%2Ffiles%2FArticles%2F207897%2Ffendo-07-00064-HTML%2Fimage_m%2Ffendo-07-00064-g006.jpg&w=3840&q=75)

Although technical problems of thyroid testing have largely been resolved by modern assay technology, biological variation remains a challenge. This applies to subclinical thyroid disease, non-thyroidal illness syndrome, and those 10% of hypothyroid patients, who report impaired quality of life, despite normal thyrotropin (TSH) concentrations under levothyroxine (L-T4) replacement. Among multiple explanations for this condition, inadequate treatment dosage and monotherapy with L-T4 in subjects with impaired deiodination have received major attention. Translation to clinical practice is difficult, however, since univariate reference ranges for TSH and thyroid hormones fail to deliver robust decision algorithms for therapeutic interventions in patients with more subtle thyroid dysfunctions. Advances in mathematical and simulative modeling of pituitary–thyroid feedback control have improved our understanding of physiological mechanisms governing the homeostatic behavior. From multiple cybernetic models developed since 1956, four examples have also been translated to applications in medical decision-making and clinical trials. Structure parameters representing fundamental properties of the processing structure include the calculated secretory capacity of the thyroid gland (SPINA-GT), sum activity of peripheral deiodinases (SPINA-GD) and Jostel’s TSH index for assessment of thyrotropic pituitary function, supplemented by a recently published algorithm for reconstructing the personal set point of thyroid homeostasis. In addition, a family of integrated models (University of California-Los Angeles platform) provides advanced methods for bioequivalence studies. This perspective article delivers an overview of current clinical research on the basis of mathematical thyroid models. In addition to a summary of large clinical trials, it provides previously unpublished results of validation studies based on simulation and clinical samples.
The long-held concept of a proportional negative feedback control between the thyroid and pituitary glands requires reconsideration in the light of more recent studies. Homeostatic equilibria depend on dynamic inter-relationships between thyroid hormones and pituitary thyrotropin (TSH). They display a high degree of individuality, thyroid-state-related hierarchy, and adaptive conditionality. Molecular mechanisms involve multiple feedback loops on several levels of organization, different time scales, and varying conditions of their optimum operation, including a proposed feedforward motif. This supports the concept of a dampened response and multistep regulation, making the interactions between TSH, FT4, and FT3 situational and mathematically more complex. As a homeostatically integrated parameter, TSH becomes neither normatively fixed nor a precise marker of euthyroidism. This is exemplified by the therapeutic situation with l-thyroxine (l-T4) where TSH levels defined for optimum health may not apply equivalently during treatment. In particular, an FT3–FT4 dissociation, discernible FT3–TSH disjoint, and conversion inefficiency have been recognized in l-T4-treated athyreotic patients. In addition to regulating T4 production, TSH appears to play an essential role in maintaining T3 homeostasis by directly controlling deiodinase activity. While still allowing for tissue-specific variation, this questions the currently assumed independence of the local T3 supply. Rather it integrates peripheral and central elements into an overarching control system. On l-T4 treatment, altered equilibria have been shown to give rise to lower circulating FT3 concentrations in the presence of normal serum TSH. While data on T3 in tissues are largely lacking in humans, rodent models suggest that the disequilibria may reflect widespread T3 deficiencies at the tissue level in various organs. As a consequence, the use of TSH, valuable though it is in many situations, should be scaled back to a supporting role that is more representative of its conditional interplay with peripheral thyroid hormones. This reopens the debate on the measurement of free thyroid hormones and encourages the identification of suitable biomarkers. Homeostatic principles conjoin all thyroid parameters into an adaptive context, demanding a more flexible interpretation in the accurate diagnosis and treatment of thyroid dysfunction.