Original Research
25 May 2016
Sadegh Massarrat
, 4 more and
Saman Khalili-Samani



Gastric cancer can be classified as cardia and non-cardia subtypes according to the anatomic site. Although the gastric cancer incidence has decreased steadily in several countries over the past 50 years, the incidence of cardia cancers and esophageal adenocarcinoma (EAC) continue to increase. The etiological factors involved in the development of both cardia cancers and EACs are associated with high animal fat intake, which causes severe obesity. Central obesity plays roles in cardiac-type mucosa lengthening and partial hiatus hernia development. There are two distinct etiologies of cardia cancer subtypes: one associated with gastroesophageal reflux (GER), which predominantly occurs in patients without Helicobacter pylori (H. pylori) infection and resembles EAC, and the other associated with H. pylori atrophic gastritis, which resembles non-cardia cancer. The former can be developed in the environment of high volume duodenal content reflux, including bile acids and a higher acid production in H. pylori–negative patients. N-nitroso compounds, which are generated from the refluxate that includes a large volume of bile acids and are stabilized in the stomach (which has high levels of gastric acid), play a pivotal role in this carcinogenesis. The latter can be associated with the changing colonization of H. pylori from the distal to the proximal stomach with atrophic gastritis because a high concentration of soluble bile acids in an environment of low acid production is likely to act as a bactericide or chemorepellent for H. pylori in the distal stomach. The manuscript introduces new insights in causative factors of adenocarcinoma of the cardia about the role of bile acids in gastro-esophageal refluxate based upon robust evidences supporting interactions among pH, H. pylori, and bile acids.
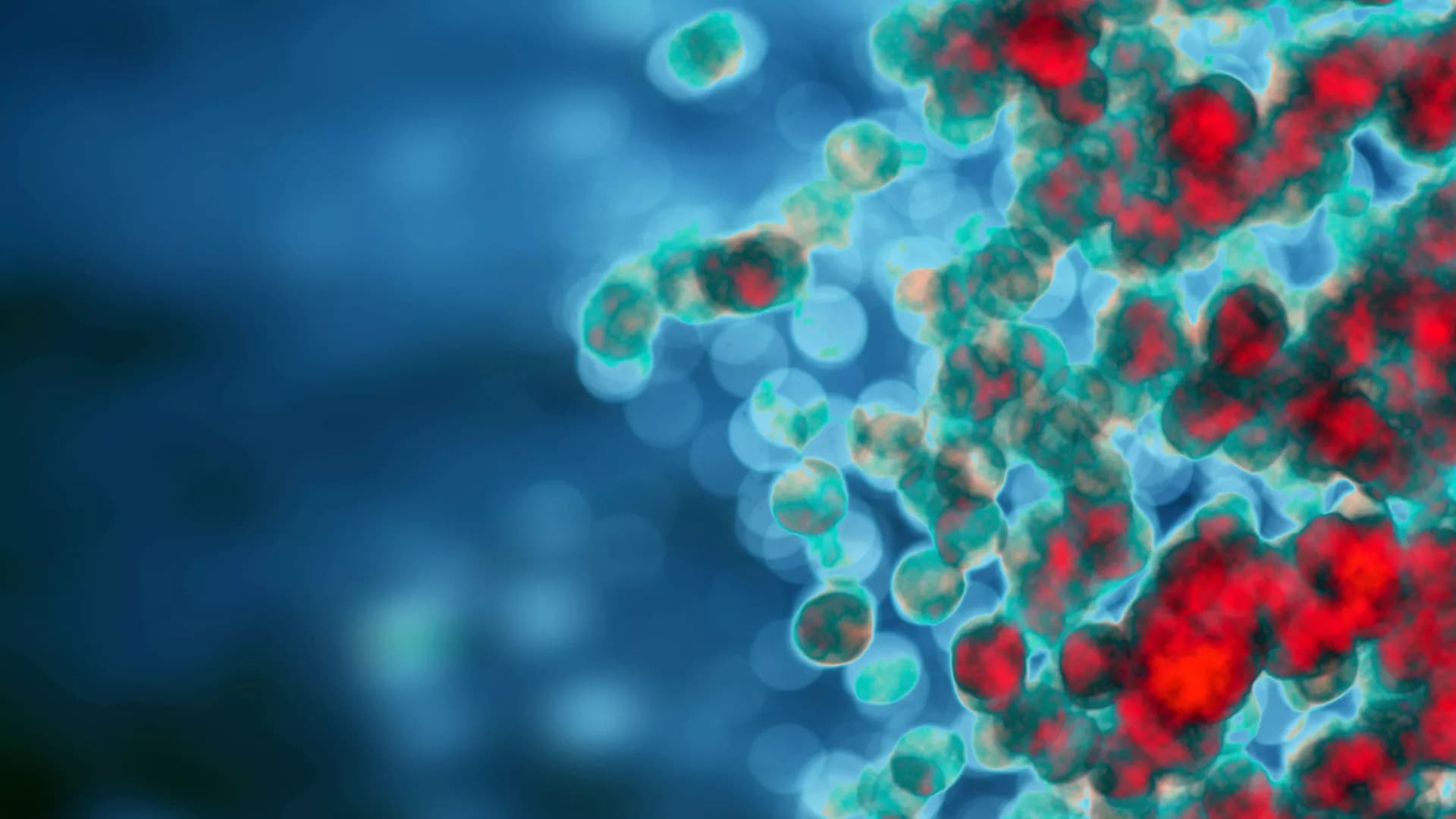
![Proliferation of splenocytes in response to stimulation by MOG35-55 peptide. Mice were infected with H. pylori (Hp/EAE), or given a placebo dose (Broth/EAE). After 3 weeks, EAE induction treatment with MOG35-55 peptide was administered. Splenocytes were isolated from mice after a further 3 weeks. Splenocytes were stimulated with MOG35-55 peptide and incorporation of [3H]thymidine was used to measure the proliferative response in counts per minute (CPM). The median CPMs following stimulation with anti-CD3/28 antibodies were 118946 and 57633 for the Broth/EAE and Hp/EAE groups, respectively. Bars depict the mean CPM for mice in each group; error bars represent SD. p-values were calculated using Mann–Whitney U-tests.](https://www.frontiersin.org/_rtmag/_next/image?url=https%3A%2F%2Fwww.frontiersin.org%2Ffiles%2FArticles%2F123776%2Ffmicb-06-00052-HTML%2Fimage_m%2Ffmicb-06-00052-g002.jpg&w=3840&q=75)
Recent research has demonstrated that infection with the bacterial pathogen Helicobacter pylori is less common amongst patients with multiple sclerosis (MS), an inflammatory demyelinating disease of the central nervous system (CNS). We aimed to compare the prevalence of H. pylori amongst MS patients and healthy controls, and also investigated the impact of this infection on an animal model for MS, experimental autoimmune encephalomyelitis (EAE). The H. pylori status of 71 MS patients and 42 healthy controls was determined by serology. Groups of C57BL/6 mice were infected with H. pylori, or given diluent alone as a placebo, prior to inducing EAE. Clinical scores were assessed for all mice, and spleens and spinal cord tissue were harvested. CD4+ T cell subsets were quantified by flow cytometry, and T cell proliferation assays were performed. In MS patients the seroprevalence of H. pylori was half that of healthy controls (p = 0.018). Over three independent experiments, prior H. pylori infection had a moderate effect in reducing the severity of EAE (p = 0.012). In line with this, the antigen-specific T cell proliferative responses of infected animals were significantly reduced (p = 0.001), and there was a fourfold reduction in the number of CD4+ cells in the CNS. CD4+ populations in both the CNS and the spleens of infected mice also contained greatly reduced proportions of IFNγ+, IL-17+, T-bet+, and RORγt+ cells, but the proportions of Foxp3+ cells were equivalent. There were no differences in the frequency of splenic CD4+cells expressing markers of apoptosis between infected and uninfected animals. H. pylori was less prevalent amongst MS patients. In mice, the infection exerted some protection against EAE, inhibiting both Th1 and Th17 responses. This could not be explained by the presence of increased numbers of Foxp3+ regulatory T cells, or T cell apoptosis. This is the first direct experimental evidence showing that H. pylori may provide protection against inflammatory demyelination in the CNS.