 Meron Asmamaw Alemayehu*
Meron Asmamaw Alemayehu* Muluken Chanie Agimas
Muluken Chanie Agimas Daniel Alayu Shewaye
Daniel Alayu Shewaye Nebiyu Mekonnen Derseh
Nebiyu Mekonnen Derseh Fantu Mamo Aragaw
Fantu Mamo Aragaw- Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Introduction: Safe and easily accessible drinking water service generates substantial benefits for public health and the economy. Approximately 10% of the global burden of disease worldwide could be prevented with improved access to drinking water. The death of ~ 30% of children younger than 5 years in developing countries is attributable to inadequate access to improved drinking water. Despite the presence of abundant water sources in Ethiopia, uneven distribution and waste pollution coupled with unprecedented population growth, rapid urbanization, and climate change are hindering the country's ability to maintain the balance between the demand and supply of accessible and improved drinking water services. The importance of up-to-date evidence for actions regarding the distribution of access to improved drinking water services is indicated by the Ethiopian Ministry of Water and Energy. Therefore, this study aimed to explore the spatial distribution and determinants of limited access to improved drinking water service among households in Ethiopia.
Methods: This study used the 2019 Ethiopian Mini Demographic and Health Survey (EMDHS). The data were weighted using sampling weight to restore the representativeness and to obtain valid statistical estimates. After excluding ineligible households, a total weighted sample of 5,760 households was included in the final analysis. The analysis was performed using STATA version 14.2, ArcGIS Pro, and SaTScan version 10.1 software. To find significant determinants with limited access to improved drinking water service, we used a multilevel logistic regression model. A P-value of <0.05 was used to declare statistical significance.
Results: This study found that in Ethiopia, 16.1% (95% CI: 15.2, 17.1) of households have limited access to improved drinking water services. The spatial distribution of households with limited access was identified to be clustered across a few regions of the country (Moran's I = 0.17, p-value < 0.01). The most likely significant primary clusters with highly limited access were seen in the Somali region (RR = 4.16, LLR = 162.8), the border between Amhara and Afar region (RR = 4.74, LLR = 41.6), the border between Oromia and Afar region (RR = 5.21, LLR = 13.23), and the northeastern Tigray region (RR = 2.52, LLR = 9.87). The wealth index, the age of household head, residence, and region were significantly associated with limited access to improved drinking water service. A high rate of limited access to improved drinking water service is predicted in the southwestern part of Gambella, the northeastern part of Oromia, the southwestern part of South Nation Nationalities and Peoples' region, and part of the Oromia region that surrounds Addis Ababa.
Conclusion: Limited access to improved drinking water service in Ethiopia varies across regions, and inequality in the service provision exists in the country. Prioritization and extra level of efforts should be made by concerned government and non-government organizations as well as other stakeholders for those underprivileged areas and groups of the population as they are found in the study.
Introduction
Safe and easily accessible drinking water service generates substantial benefits for public health, the economy, and the environment. The United Nations General Assembly acknowledged access to clean drinking water is even further essential to the realization of all human rights as well (United Nations Department of Economic Social Affairs, 2010). Limited access to improved drinking water service (LAIDWS) is defined as drinking water where the estimated collection time is more than 30 min for a round trip. According to the World Health Organization, improved water sources include piped water, boreholes or tube wells, protected dug wells, protected springs, and packaged or delivered water (WHO/UNICEF, 2021).
In 2020, ~ 282 million people worldwide had limited access to improved drinking water services (LAIDWS). In the same year, this problem contributed to 829,000 deaths among children younger than 5 years, which accounts for 60% of total diarrheal deaths. The deaths of 35.8% of those children could have been avoided if access to improved drinking water was facilitated (World Health Organization United Nations Children's Fund, 2020, 2021). Similarly, ~ 10% of the global burden of disease worldwide could be prevented with improved access to drinking water, sanitation, and hygiene. The burden of water-related diseases is extremely higher among developing countries and particularly among children younger than 5 years, with ~ 30% of deaths of these children attributable to inadequate access to improved drinking water (Patrick et al., 2023).
Distance is an important determinant of the quantity of water brought to the household, which, in turn, has an impact on infectious diseases and other health problems associated with water carriage (Muluken Azage and Nigatu, 2020). People living in rural Africa must walk an average of 6 km to collect drinking water. A systematic review and meta-analysis revealed that people living far away from an improved water source have a significant increase in illness risk, such as diarrheal diseases (Wang and Hunter, 2010), musculoskeletal disorders, perinatal and mental health problems, and violence against vulnerable people (Patrick et al., 2023). The public health benefit of easily accessible drinking water not only is linked with a reduction in the incidence of various diseases and health-related problems (Andualem et al., 2021) but also has extensive economic benefits that essentially stem from the time gained by not having to walk long distances to fetch water or queue at the source (Abraha et al., 2022).
The Sustainable Development Goal (SDG) 6.1 calls for universal and equitable access to safe and affordable drinking water. This target is tracked with the indicator of “safely managed drinking water services,” i.e., drinking water from an improved water source located on-premises, available when needed, and free from fecal and chemical contamination (World Health Organization United Nations Children's Fund, 2020). Despite the presence of abundant water resources in Ethiopia, improved drinking water service is not accessible to all people equitably. Although there are undeniable signs of progress in the provision of the service, the country still is nowhere closer to achieving SDG number 6.1. There still is room for more advancements in overcoming the problem (World Health Organization United Nations Children's Fund, 2020). One existing reason for this problem is the fact that water resources in the country are either unevenly distributed or are being polluted by industrial, agricultural, and domestic wastes (Falk et al., 2022). On the other hand, a study conducted in 2022 reported that the most important emerging reason is unprecedented population growth and rapid urbanization along with climate change in the country. According to the report, these combinations are hindering the country's ability to keep the balance between the demand and supply of accessible and improved drinking water services (Abraha et al., 2022).
The 2023 report of the Ethiopian Ministry of Water and Energy stated that the current efforts to provide accessible drinking water service among regions in Ethiopia require up-to-date evidence about the distribution of drinking water services in the country. According to the report, the ministry would use this information to operate fair allocation of water resources among cities and regions, to address the existing gaps, and to facilitate the provision of accessible and sustainable water supply (Federal Democratic Republic of Ethiopia, 2023). As a result, identifying a cluster of households with limited access to drinking water service and their determinants can inform such governmental and non-governmental organizations as well as relevant health actors that are working on this area where to give the most emphasis. Therefore, this study aimed to assess the spatial distribution and determinants of limited access to improved drinking water service among households in Ethiopia.
Methodology
Study area
The study was conducted in Ethiopia. Ethiopia is strategically located in the Horn of Africa, 3′ and 14.8″ latitude 33′ and 48′ longitude bordering Somalia, Sudan, Djibouti, Kenya, and Eritrea with a total border length of 5,311 km. It is the 10th largest country in Africa and the second most populous country in Africa with a population of over 115 million. Currently, Ethiopia has 10 regional states which are subdivided into zonal administration and two city administrations (Embassy of Ethiopia in Washington, 2022).
Study design, data sources, and sampling
A secondary analysis of the 2019 EMDHS was conducted in this study. The data collection of the 2019 EMDHS was carried out from 21 March 2019 28 to June 2019. During that time, there were nine regions and two administrative cities. The survey sample was intended to reveal an estimate of key indicators for rural and urban areas of the whole country. The sampling frame of the EMDHS was taken from the 2019 Ethiopia Population and Housing Census (EPHC) that was conducted by the Central Statistical Agency (CSA) of the country. The EPHC created and used a complete list of the 149,093 EAs where, on average, one EA contains 131 households (Ethiopian Public Health Institute, 2021).
The overall sampling procedure of the 2019 EMDHS was a two-stage stratified sampling technique. In the first stage, each of the nine regions including the two city administrations was stratified into urban and rural areas. This revealed a total of 21 sampling strata. In the second stage, samples of EAs were selected from each stratum in two stages. In the first stage of selecting EAs, 305 EAs were selected with the probability sampling technique from a total of 149,093 EAs. Of those EAs, 93 were from urban strata while 212 were from rural strata. Then, the list of households in all selected EAs was recorded. Household listing in large EAs (more than 300 households) was carried out after segmenting the EA and selecting only one segment for the survey so that the task of listing will be minimized. This makes the cluster in the 2019 EMDHS to be either an EA (where the EA is not too large) or a segment of EA (where the EA is larger than 300 households). In the second stage of selecting EAs, 30 households from each cluster were selected with systematic random sampling techniques. Here, the list of households recorded in each selected EA or segment of EA was used as a sampling frame to select the pre-fixed number of 30 households. The interview was conducted among all women who are either permanent residents or visitors who spend at least a night in the selected household and were aged between 15 and 49 years (Croft et al., 2018; Ethiopian Public Health Institute, 2021).
In the 2019 EMDHS, a total of 8,663 households were studied. However, eligible households for this study were those with improved drinking water sources and those who reported the roundtrip time that it takes them to collect the water from that improved source. In this regard, we have excluded 2,892 households that do not have an improved drinking water source and 11 households with an improved water source but did not report the roundtrip time that it takes to fetch the water. As a result, a total weighted sample of 5,760 households was included in the final analysis.
Study variables
The household questionnaire was one of the five questionnaires used for the 2019 EMDHS which we used for the current study. It was based on the DHS program's standard questionnaire and was adapted to reflect the population and households of Ethiopia. It had questions about the list of all the usual members and visitors of the selected households with basic demographic information including age, sex, education, and relationship with the head of the household. It was also designed to collect information on characteristics of the household's dwelling unit, such as the source of water, roundtrip water collection time, type of toilet facilities, materials used for the floor of the dwelling unit, and ownership of various durable goods. The outcome variable of the study was limited access to improved drinking water services. It was coded as a dichotomous variable with possible values of “1” if the household has limited access to improved drinking water service and “0” if the household has basic access to improved drinking water service.
The possible predictor variables were further classified as individual-level and cluster-level variables. Age, sex, wealth index, media exposure, educational status, and source of water were individual-level independent variables included in this study, while the region and place of residence were cluster variables included in the study. Media exposure status was created from the frequency of watching TV and listening to the radio, and if a woman has at least one yes, she was considered to have media exposure. The wealth index was calculated by the “DHS program” using the Gini coefficient, and we only regrouped the original categories into three as follows: poorest and poorer as poor, middle as middle and richest, and richer as rich.
Operational definitions
Limited Access to Improved Drinking Water Service (LAIDWS) is defined as drinking water from an improved source, where the estimated collection time is more than 30 min for a round trip, including queuing (WHO/UNICEF, 2021).
Basic access to improved drinking water service is drinking water from an improved source, provided collection time is <30 min for a round trip, including queuing (WHO/UNICEF, 2021).
Improved drinking water sources are defined as those that are likely to be protected from outside contamination and fecal matter in particular. It includes household connections/premises, public standpipes, boreholes, protected dug wells, protected springs, and rainwater collection (World Health Organization United Nations Children's Fund, 2020).
Data source and extraction
After permission was obtained through a formal online request, the data were retrieved from the DHS program's official website and database (https://www.dhsprogram.com/data). The data of the 2019 EMDHS are open to all DHS-registered researchers. After downloading the data, we extracted the response variable (limited access to improved drinking water service) and potential predictor variables.
Data management and analysis
Before any statistical analysis was conducted, data cleaning, recoding, and weighting were undertaken. Data were weighted, and the survey was declared using the sample weight, primary sampling unit (PSU), and sampling strata to make the survey representative and to identify the survey design characteristics. A detailed explanation of the sample weighting procedure is presented in the 2019 EMDHS final report (Ethiopian Public Health Institute, 2021). Descriptive and summary statistics such as frequency tables and cross-tabulations were generated using STATA version 14.2 (Stata Corp. Statistical Software). ArcGIS Pro and SaTScan version 10.1 were used for the spatial analysis.
Spatial autocorrelation analysis
The distribution of limited access to improved drinking water service among households in Ethiopia was examined using spatial autocorrelation (Global Moran's I) statistics to identify whether it is clustered, dispersed, or random. Moran's I is a statistic that produces a single output number between −1 and +1. A Global Moran's I-value approaching +1 suggests that LAIDWS is spatially clustered. A Global Moran's I-value approaching −1 indicates a dispersed spatial distribution of LAIDWS, while a Global Moran's I-value of 0 indicates a dispersed spatial distribution of LAIDWS. The presence of a significant spatial autocorrelation (p-value < 0.05) is confirmed by a statistically significant Global Moran's' I-test.
Hotspot Analysis of limited access to improved drinking water service
The spatial variability of the limited access to improved drinking water service among households in Ethiopia was calculated using Getis-Ord Gi* statistics in a hot spot analysis. The statistical significance of clustering was confirmed using the Z-score with a 95% confidence interval and a p-value of < 0.05. Statistical output with a high Gi* shows LAIDWS hotspots, while a low Gi* indicates basic drinking water cold spots. The proportion of LAIDWS among households in each cluster was taken as input for this hot spot analysis.
Spatial scan statistical analysis
Purely spatial scan statistics were employed to test the occurrence of statistically significant spatial clusters of areas with low and high limited access to improved drinking water service distribution using a Bernoulli -based model by SaTScan version 10.1 software. SaTScan uses a scanning window that moves across the study area to identify statistically significant clustering of areas with the same LAIDWS coverage. We used the default maximum spatial cluster size of 50% of the population as an upper limit, which allowed both small and large clusters to be detected and ignored clusters that contained more than the maximum limit with the circular shape of a window. For this Bernoulli model, households with LAIDWS were taken as cases and those households with basic drinking water service were taken as controls. Most likely clusters were identified using high log-likelihood ratio tests and significant p-value based on Monte Carlo replication.
Spatial interpolation
The percentage of limited access to improved drinking water service for unsampled areas in the country was predicted based on sampled EAs using the spatial interpolation technique. The ordinal kriging method of Gaussian distribution was used to make the prediction.
Factors associated with limited access to improved drinking water service
Multilevel logistic regression models were used to identify significant predictor variables of limited access to improved drinking water service by considering the hierarchical nature of the DHS data. Variance inflation factor (VIF) was used to test multicollinearity and rule out the presence of a significant correlation between variables. All variables have VIF < 5 and a tolerance >0.01, indicating that there was no multicollinearity. Variation between clusters was measured by computing the intra-cluster correlation coefficient (ICC) and likelihood ratio (LR) tests. The ICC quantifies the proportion of the total observed variation in LAIDWS coverage attributed to between-cluster variation. The median odds ratio (MOR) was also used to estimate the measure of variation or random effects. MOR is defined as the median value of the odds ratio of LAIDWS between the area at the highest risk and the area at the lowest risk when two clusters are randomly picked. MOR = e0.95√VA where VA is the area level variance (Merlo et al., 2005).
For multivariable multilevel logistic regression analysis, four models were constructed using the STATA command melogit. The first model (a multilevel random intercept-only logistic regression model without covariates) was used as a null model to examine the extent of cluster variation in limited access to drinking water services. Individual-level factors were used to adjust the second model (a multilevel model with level one independent variables). The third model (a multilevel model with level two variables) was adjusted for community-level variables. Finally, the fourth model was fitted with individual and community-level variables simultaneously. Then, the models were compared using the log-likelihood ratio (LLR) and deviance. Consequently, the model with the highest LLR and lowest deviance value was selected as the best-fitted model. Adjusted odds ratio (AOR) with 95% CI and p-value of < 0.05 were utilized to declare significantly associated factors with limited access to drinking water service.
Ethics approval and consent to participate
Ethical clearance and permission were obtained from the DHS program through a formal online request to their official website and database accessed through (https://www.dhsprogram.com/data). The data used in this study are publicly available, and aggregated secondary data that do not have any personal identifying information can be linked to study households. The confidentiality of data was maintained anonymously.
Results
A total of 5,760 households were included in the final analysis. The largest percentage of households was taken from the three relatively largest regions, namely, Amhara 634 (11%), Oromia 654 (11.3%), and SNNP 678 (11.7%). In contrast, the smallest number of households was taken from the Somali region 213 (3.7%) and Afar region 302 (5.2%). Approximately 3,612 (62.7%) households were sampled from rural residences. A total of 35% of household heads were in the age group between 15 and 30 years while 840 (14.5%) were between the age group of 61 and 95 years. The percentage of households with a woman being the head of the household was 1,630 (28.3%) and 2,487 (43.1%), and household heads were not educated at all. Above half the percentage of household heads, 3,098 (53%) did not have any media exposure and 1,698 (29.4%) of the households belonged to a poor wealth index category (Table 1).
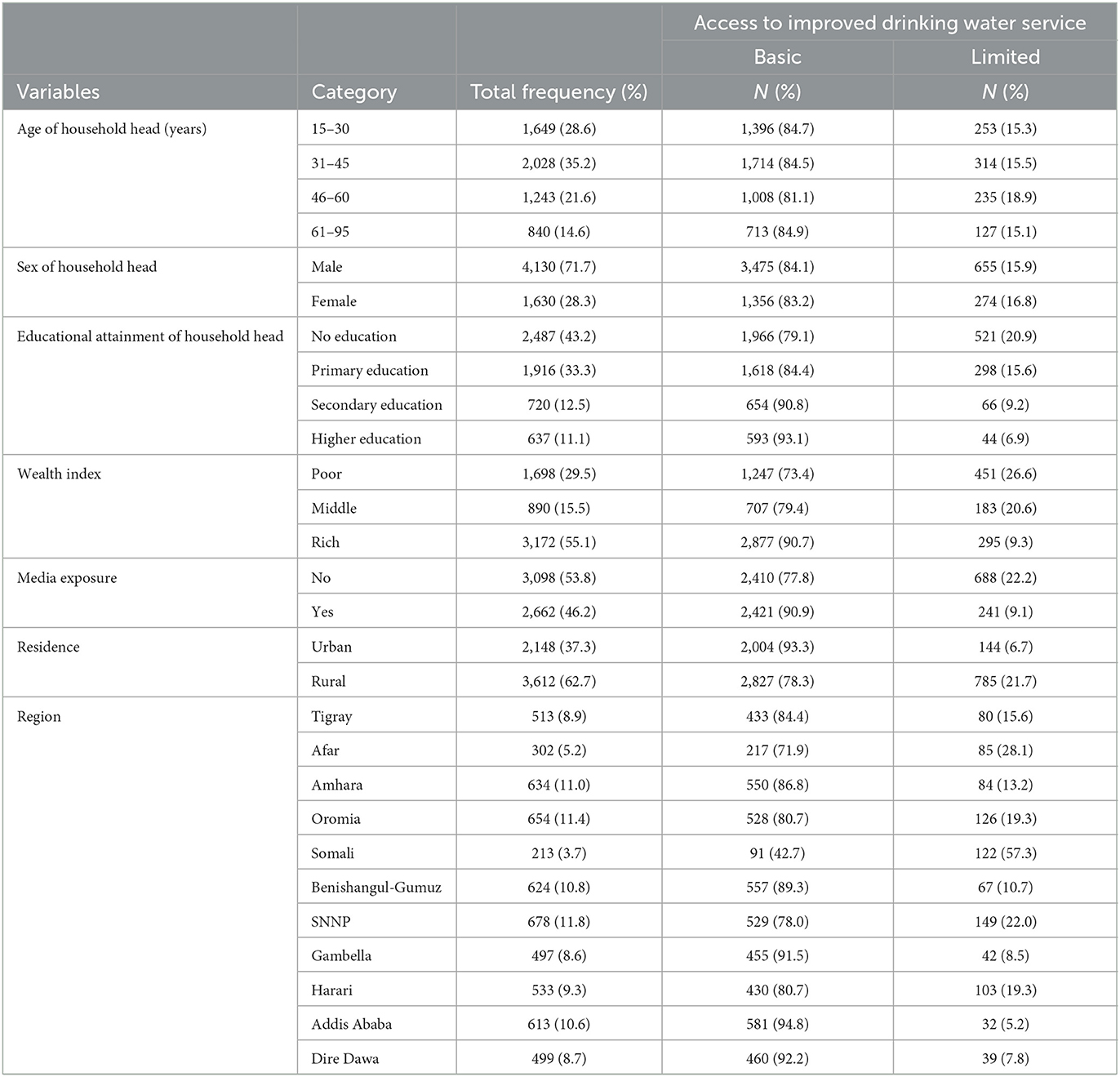
Table 1. Background characteristics of study populations and limited access to improved drinking water service coverage by various background characteristics among households in Ethiopia, the 2019 EMDHS.
Limited access to improved drinking water service in Ethiopia
The prevalence of limited access to improved drinking water services in Ethiopia was 16.1% (95% CI: 15.2, 17.1). At the regional level, the highest prevalence of limited access to improved drinking water was found in the Somali region (57.3%) and Afar (28.1%). Limited access to improved drinking water service varied highly according to the wealth index, ranging from 26.6% among households with a poor wealth index to 9.3% in households with a rich wealth index. People living in rural residents that have LAIDWS were ~ 21.7% while for those who reside in urban areas, it was only 6.7% (Table 1).
Spatial autocorrelation of the limited access to improved drinking water service
The spatial distribution of limited access to drinking water service in Ethiopia was clustered (Moran's I = 0.17, p-value < 0.01). The result shows that the observed Moran's Index value (0.17) was greater than the expected index (−0.0062), and the p-value was <0.01, which is statistically significant. Given the Z-score of 4.796359, there is a <1% likelihood that this clustered pattern could be the result of random chance (Figure 1).
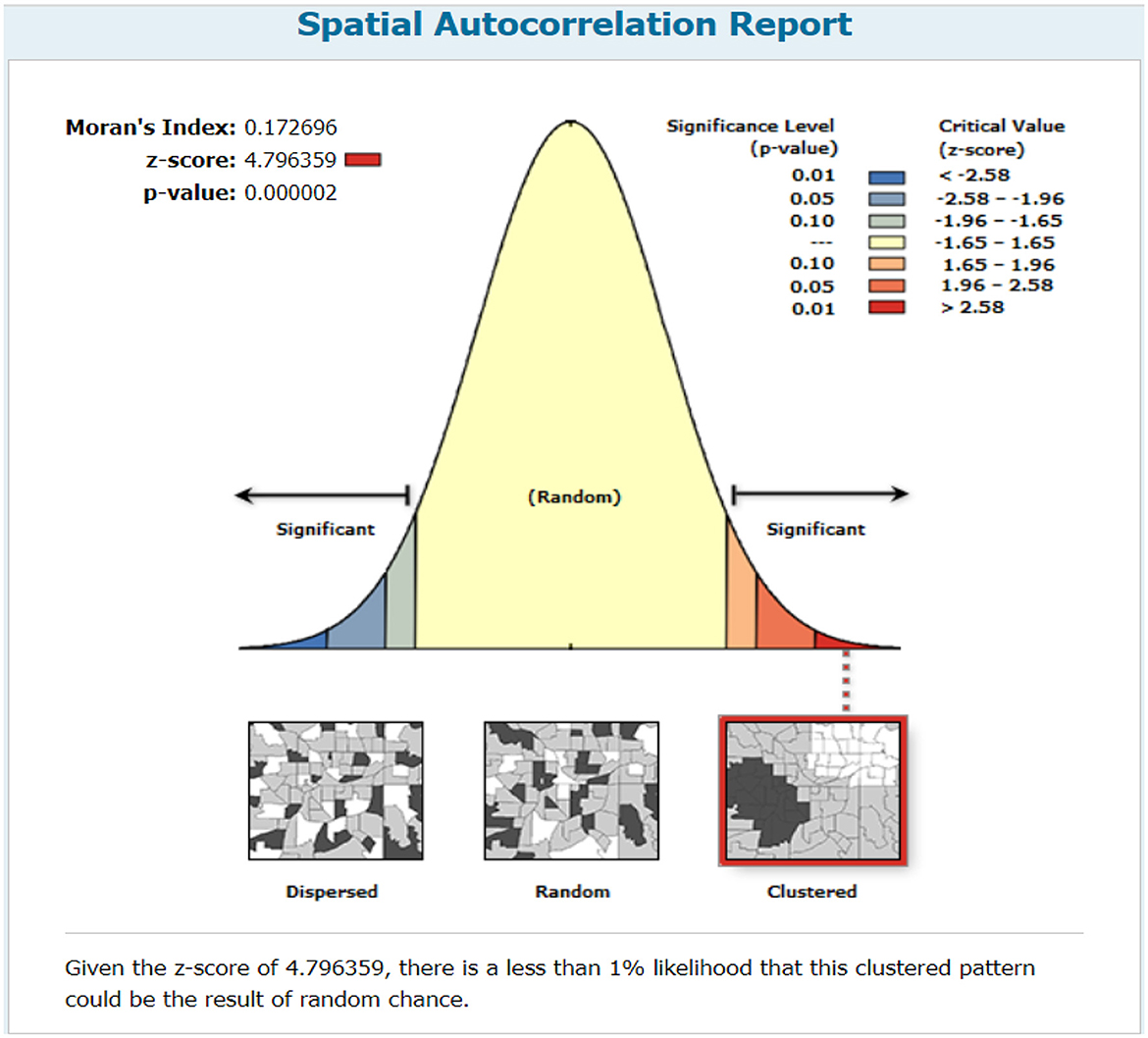
Figure 1. Spatial autocorrelation of limited access to improved drinking water service among households in regions of Ethiopia, 2019 EMDHS.
Incremental spatial autocorrelation by distance
To determine spatial clustering for limited access to improved drinking water service, global spatial statistics were estimated using Moran's I-value. As shown in Figure 2, statistically significant Z-scores indicate at 111 km distances where spatial processes promoting clustering are most pronounced. The incremental spatial autocorrelation indicates that a total of 10 distance bands were detected with a beginning distance of 30,000 m. The spatial distribution of LAIDWS among households in Ethiopia was found to be non-random with a Global Moran's I of 0.17 and a p-value of 0.0001. With a Z-score of 4.79, there is a <1% likelihood that this high-clustered pattern could be the result of random chance (Figure 2).
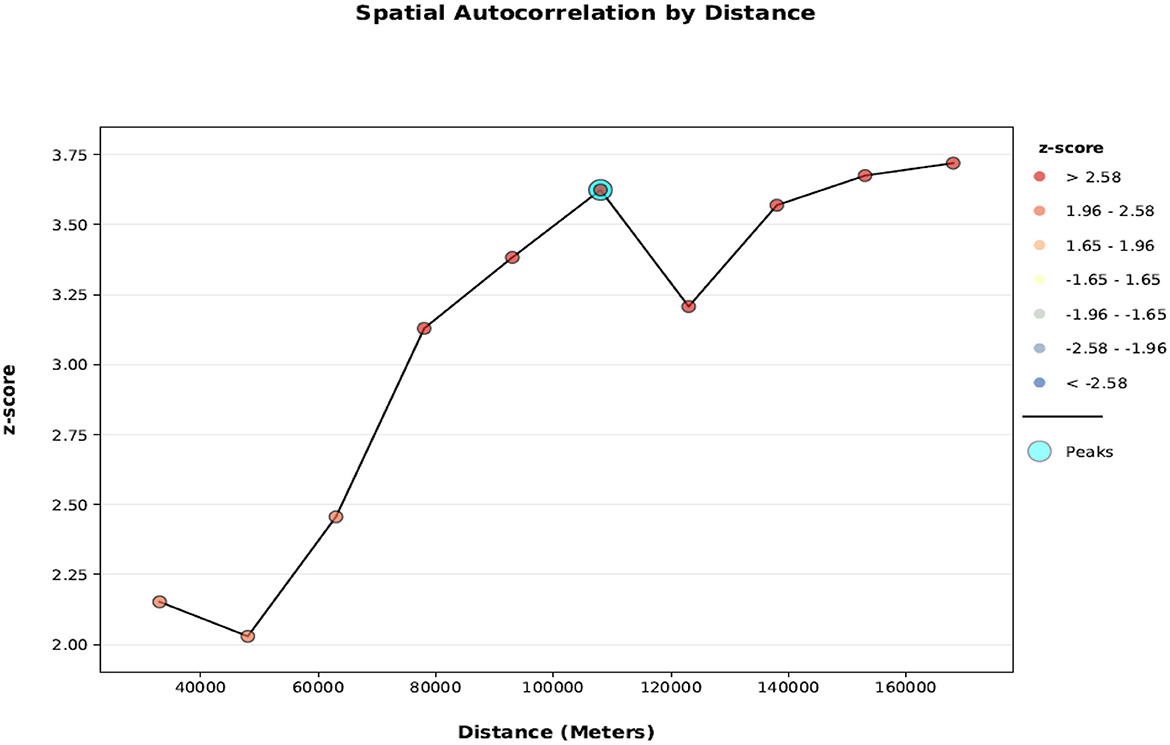
Figure 2. Incremental spatial autocorrelation by the distance of limited access to improved drinking water service among households in regions of Ethiopia, the 2019 EMDHS.
Hotspot analysis of the limited access to improved drinking water service
The Getis-Ord GI* statistical analysis was performed to identify the hotspot and cold spot areas of the limited access to improved drinking water service. The dark and light green color points indicate the significant cold spot areas of clusters with low coverage of LAIDWS that are observed in central Gambella, southwest and central Amhara region, and Western Oromia region. On the contrary, Northern and Western Somali, Southeast Amhara region (where the region borders with the Afar region), central and southwest Afar (where the region borders with the Amhara region), southeast Oromia region, and northeast part of the South Nation Nationalities and Peoples' region are indicated to have significant hotspot locations. This group is denoted by light and dark red color points and is clustered with high frequencies of LAIDWS (Figure 3).

Figure 3. Spatial patterns of hot spots and cold spots of drinking water service across regions in Ethiopia, 2019 EMDHS.
Spatial scan statistical analysis
A total of 11 most likely significant clusters with limited access to improved drinking water service were detected in the spatial scan statistical analysis, which means that the proportion of LAIDWS is higher among households inside the spatial scan circular window than in households outside the circular window. Of these, nine clusters of areas were the primary most likely significant clusters and were found in the Somali region centered at 6.639662 N, 44.465850 E with 390 km radius (RR = 4.16, LLR = 162.8, with p-value < 0.01). The northeastern Tigray region centered at 14.379220 N, 39.606690 E with a 52.05 km radius (RR = 2.52, LLR = 9.87, with p-value < 0.01); the border between Afar and Oromia regions centered at 9.391181 N, 40.923110 E with 75.86 km radius (RR = 5.21, LLR = 13.23, with p-value < 0.01); and the border between Amhara and Afar regions centered at 10.886150 N, 40.296920 E with 54.09 km radius (RR = 4.74, LLR = 41.6, with p-value < 0.01; Table 2 and Figure 4).

Table 2. SaTScan analysis of limited access to improved drinking water service among households in Ethiopia, the 2019 EMDHS.
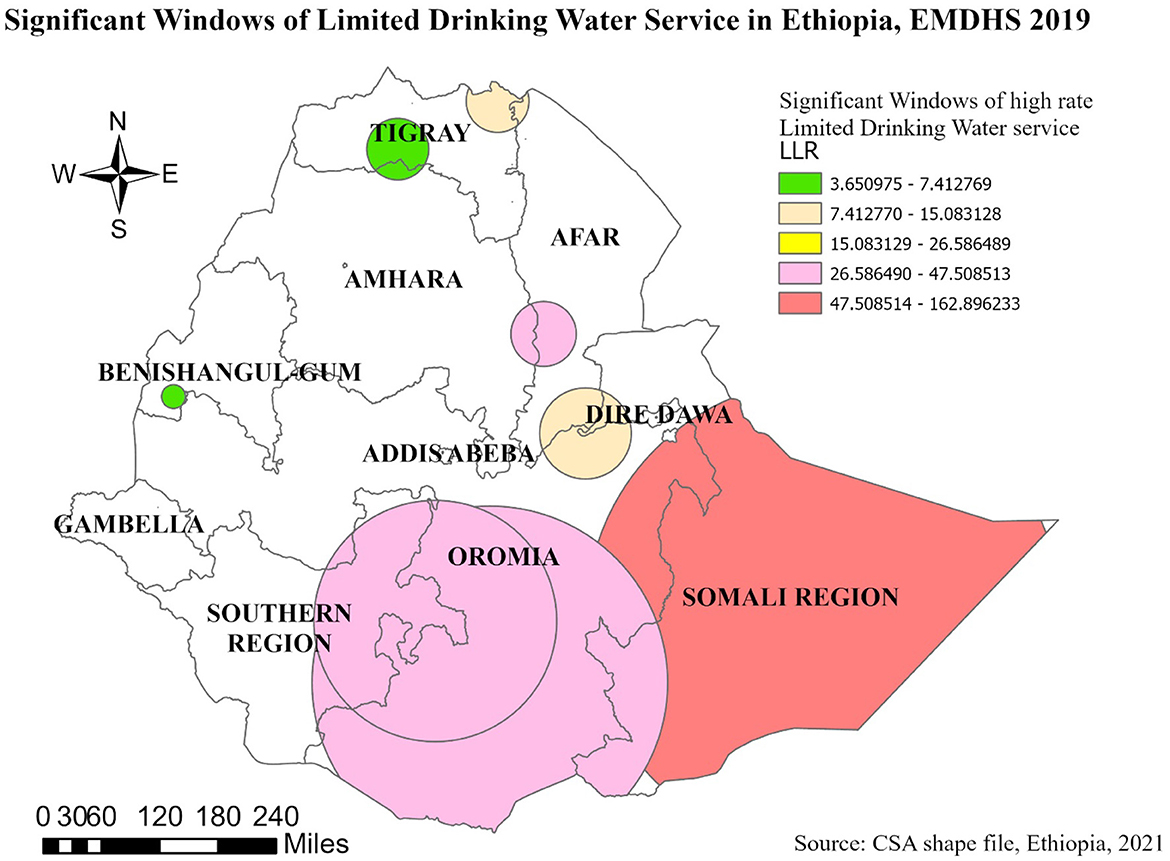
Figure 4. Significant primary and secondary windows of limited access to improved drinking water service among households in Ethiopia, the 2019 EMDHS.
Moreover, the two most likely significant secondary clusters were observed in the SNNP region centered at 6.583480 N, 38.656880 E with 201.10 km radius (RR = 2.02, LLR = 42.27, with a p-value of < 0.01) and Oromia region centered at 5.658143 N, 39.474260 E with 294.35 km radius (RR = 2.11, LLR = 47.50, with a p-value of < 0.01; Table 2 and Figure 4).
Spatial interpolation
The output of kriging interpolation prediction for unsampled areas ranged from light white color, which indicates low-risk areas, to dark brown color, which indicates high-risk areas. The rate of high-risk areas of LAIDWS was predicted, and the rate ranges from 19.5 to 29.2 and located in the southwestern part of Gambella, the northeastern part of Oromia, the southwestern part of the South Nation Nationalities and Peoples' region, as well as part of the Oromia region that surrounds Addis Ababa. Whereas, the lower rate predicted areas were seen in Tigray, Afar, and Amhara regions and ranged from 0.84 to 5.51 (Figure 5).
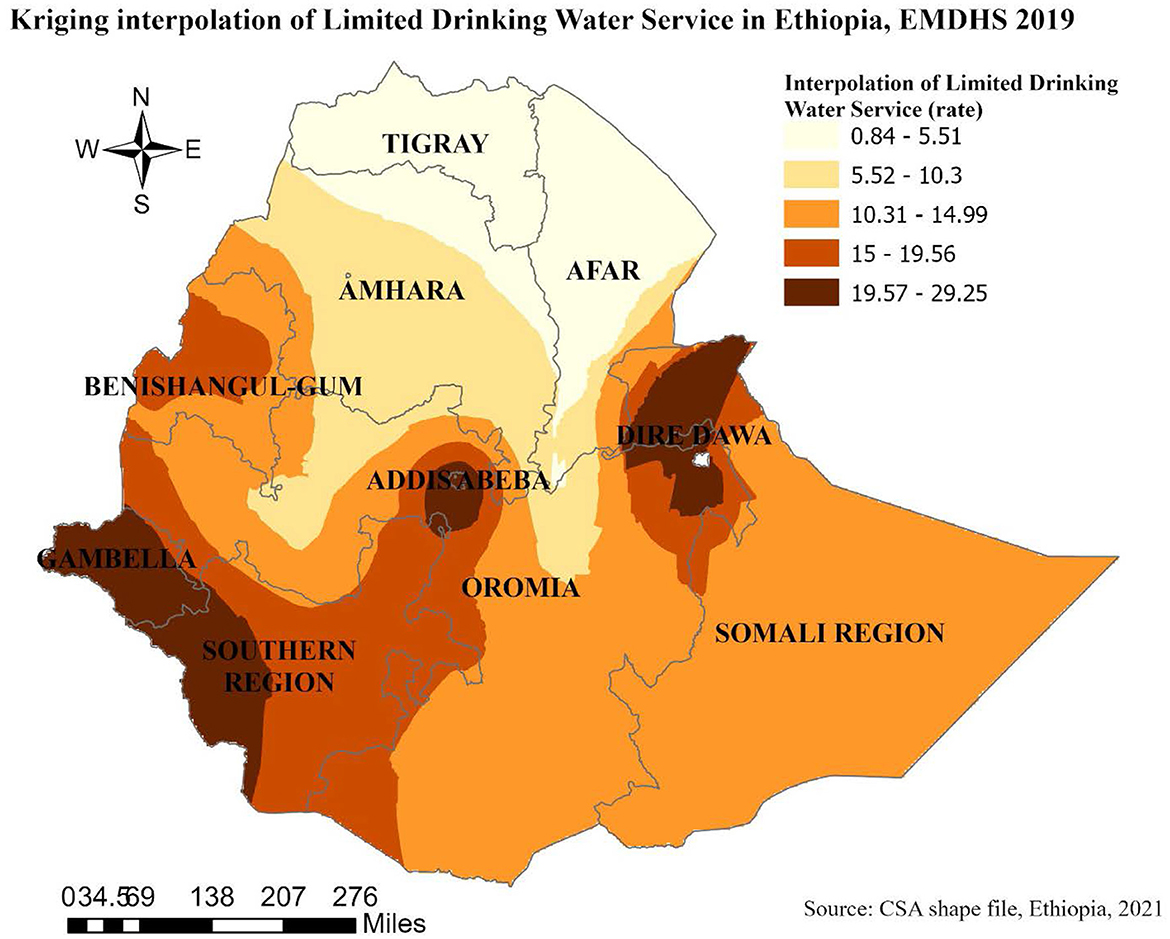
Figure 5. Kriging interpolation of limited access to improved drinking water service among households in Ethiopia, the 2019 EMDHS.
Random effect analyses and model comparison
The random effect analyses showed significant clustering of limited access to improved drinking water service among households (OR of variance = 3.18, 95% CI: 2.31 to 4.36). As shown in Table 3, the ICC value in model I (the null model) indicated that cluster/EA variability accounted for 59.4% of the overall LAIDWS distribution variability, while individual differences accounted for the remaining 40.6% of the variability. The variation in limited access to improved drinking water distribution remained significant after accounting for individual- and community-level factors. Across the communities, 49.1% of the chances of variations in limited access to improved drinking water service coverage were detected in the full model. Deviance and Log-likelihood were used to assess model fitness. Finally, the model with the lowest deviance and the highest Log-likelihood (model four) was chosen as the best-fitted model (Table 3).
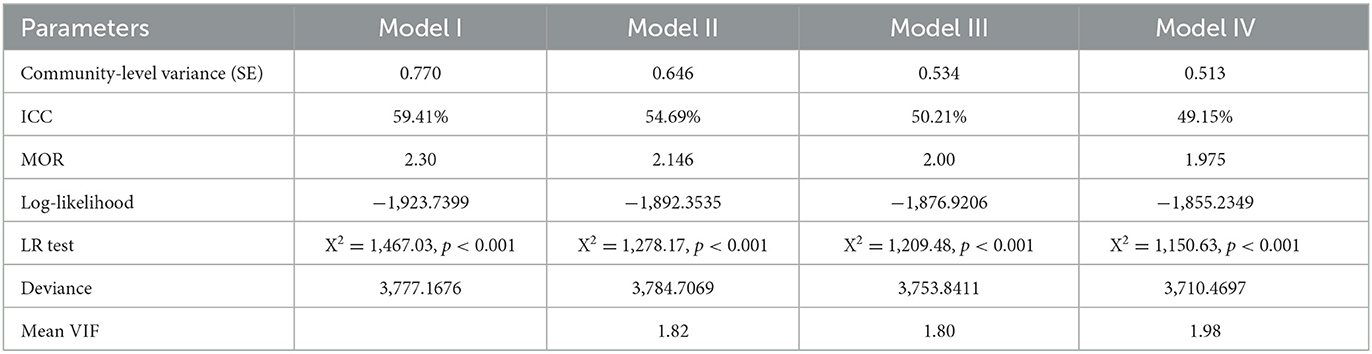
Table 3. Model comparison and random effect analysis for multilevel regression analysis.
Factors associated with limited access to improved drinking water service
Individual-level and community-level variables were included in the multivariable multilevel logistic regression analyses. Age (one category) and wealth index were the individual-level factors that were significantly associated with limited access to improved drinking water service, while residence and region (one category) were the significantly associated community-level variable.
According to our secondary analysis, when the age of the household head is between 46 and 60 years, the odds of having limited access to improved drinking water service was 1.37 [AOR = 1.37, 95% CI:1.01, 1.81] than the age group of 15–30 years. Households with poor wealth index category were 63% more likely to have LAIDWS while those with middle wealth index category were 35% more likely to have LAIDWS than households with rich wealth index [AOR = 1.63, 95% 365 CI:1.23, 2.17] and [AOR = 1.35, 95% CI:1.03, 1.76] respectively.
Among community-level factors, households in rural areas were 4.8 times more likely to have LAIDWS than households in urban areas [AOR = 1.80, 95% CI:2.17, 10.59]. Furthermore, households in the Somali region were 55.8 times more likely to have LAIDWS than households in the Dire Dawa region (AOR = 55.8, 95% CI: 6.91, 441.9; Table 4).
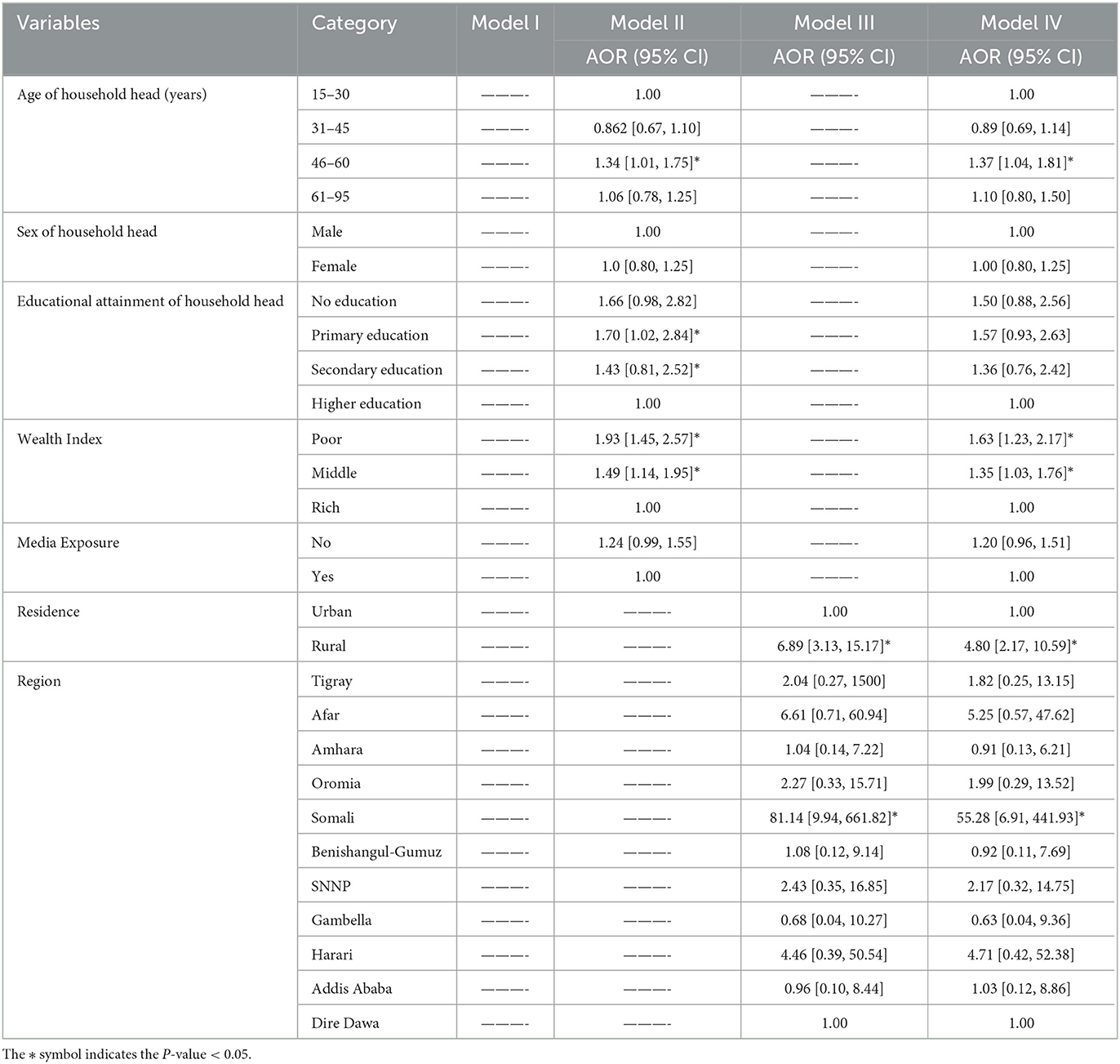
Table 4. Multilevel analysis of factors associated with limited access to improved drinking water service among households in Ethiopia, the 2019 EMDHS.
Discussion
This study reveals that 16.1% of households in Ethiopia have limited access to improved drinking water service, including 6.7% of urban households and 21.7% of rural households. The finding shows that households with a high percentage of LAIDWS are highly clustered in the Somali region 57.3%, Afar region 28.1%, and Southern Nation Nationalities and Peoples' region 22%.
It is proven that people with LAIDWS have a significantly increased risk of various communicable diseases and other health-related problems such as musculoskeletal disorders, perinatal and mental health problems, and violence against vulnerable people. With that being known, Ethiopia is still struggling to achieve and maintain a sustainable provision of improved and accessible drinking water service. The proportion of limited access to improved drinking water service in this study (16.1%) was in line with studies conducted in low- and middle-income countries (Gomez et al., 2019; Hasan and Alam, 2020) but less than a study conducted in Ghana (Tetteh et al., 2022). The possible explanation for the observed discrepancy might be due to the diverseness of countries regarding population growth and distribution, the socioeconomic status of the countries, and geographical variation (Adams, 2018; Falk et al., 2022).
To assess the spatial distribution of limited access to improved drinking water service, analysis techniques such as spatial autocorrelation, hot spot, kriging interpolation, and spatial scan analysis were executed. The spatial autocorrelation statistics confirmed that the distribution of LAIDWS was clustered in a few geographical areas (Moran's I = 0.17, p-value of < 0.01). The hot spot analysis identified areas with a low and high distribution of LAIDWS. Kriging interpolation predicted the rate of high-risk areas of LAIDWS among unsampled areas, whereas the spatial scan statistical analysis identified the most likely significant clusters, which had high LAIDWS coverage.
The SaTScan analysis identified nine primary and two secondary most likely significant clusters across the study area, implying that the proportion of limited access to improved drinking water service is higher among households inside the spatial scan circular window than in households outside the circular window. The most likely significant primary clusters with a high proportion of LAIDWS were found in the rural zones of the Somali region, the border between Afar and Oromia regions, the border between Amhara and Afar regions, as well as the northeastern Tigray region. The second most significant clusters were observed in the Oromia region and South Nation Nationalities and Peoples' region. This clustering of LAIDWS in these locations could first be because areas like this are populated by nomadic pastoral populations who essentially do not have a permanent living area, which makes the construction of basic drinking water services ineffective. The second reason, however, might be related to the negligence of the organizations and private contractors who won the rural water projects that were tendered and opened for bidding by the federal government in Ethiopia. Even if those private contractors are paid in stages and receive up to 90% of payment only after the completion of the project, they usually do not emphasize the quality of the work. Instead, they rush to finish the project as fast as possible and move on. On the other hand, the concerned government organizations also do not usually appoint engineers who play the crucial role in determining the water source location and type of water source that best fits the location in that particular rural community. They are also expected to collaborate with community leaders to create a sense of ownership and rapport. Any form of failure to do this puts the sustainability of the water service in question and might even initiate careless and misuse of the service which prevents other non-government organizations from commencing their project in such areas (Zablon Adane and Yohannes, 2021).
In the multilevel analysis, the age of the household head, household wealth index, region, and residence were significantly associated with household LAIDWS. Households with poor and middle wealth index categories had higher odds of having LAIDWS than households with rich wealth index. This finding concurs well with studies conducted in Ethiopia (Andualem et al., 2021), Kenya (Koskei et al., 2013), Nigeria (Lukman et al., 2016; Abubakar, 2019), and Malaysia (Kong et al., 2020). The first compelling justification for this consistency might be that people with low financial ability and stability have so many other pressing issues to invest their money on than installing a private water pipeline for their family. They are also more likely to reside in towns and villages found in the country-sides where the living expenditure is relatively lower, and hence, essential infrastructures such as water, sanitary, and road facilities are not well-built or not built at all (Afifah et al., 2018; Gomez et al., 2019).
A statistically significant association was seen between the place of residence and limited access to improved drinking water service. This was in line with studies conducted in low- and middle-income countries (Gomez et al., 2019; Falk et al., 2022), Ethiopia (Andualem et al., 2021), Nepal (He et al., 2018), and Uganda (Hirai et al., 2016), which revealed that households found in rural areas have greater odds of having LAIDWS than households found in urban areas. This association was also seen among regions within the country. Households found in the Somali region were more likely to have LAIDWS than households in Dire Dawa. The alternative explanation for this regional inequality could be a completely different living style that people in these regions follow. People who live in the Somali region, particularly in the east and southeast, are pastoral and semi-pastoral. Pastoral communities often live an entirely nomadic or semi-nomadic life, and they are often rudimentary and easily movable. Thus, it is difficult for the concerned actors to provide a single permanent drinking water facility within the recommended distance. On the other hand, people who live in bigger cities such as Dire Dawa and Addis Ababa have a well-settled life and convenient provision of sustainable access to an improved drinking water service (Desta, 2010; Hasan and Alam, 2020). Furthermore, there exists unequal commitment and effectiveness of governmental and non-governmental organizations that work toward the provision of basic water supplementation (Falk et al., 2022).
The first notable strength of this study is that it was conducted based on the latest up-to-date national and sub-national representative DHS data. A multilevel analysis was used, and the data were weighted to obtain a reliable estimate and standard error by considering the hierarchical nature of the DHS data. In contrast, one of the major limitations of this study was that a few important variables such as marital status and the person who fetches the water were not included in this study because no data were collected for those variables in the 2019 EMDHS. In addition, since it was a cross-sectional study, it also shares the limitations of cross-sectional studies.
Conclusion
Limited access to drinking water service in Ethiopia has improved in the 3 years but still varies across regions, and there exists within-country inequality in the service. The spatial analysis confirmed a total of 11 most likely significant clusters and the highest number of limited access were found among rural households of Somali, Tigray, border between Amhara and Afar, SNNP, and the border between Oromia and Afar regions. Wealth index, age of household head, residence, and region were the significantly associated factors. Accordingly, this study recommends:
• Both government and non-government bodies should set out objectives for joint action and be able to efficiently address the underprivileged communities with poor economic status and rural residents as they are found in the study.
• The concerned government bodies should put an extra level of effort and dedication into monitoring the progress and sustainability of water projects in difficult-to-reach rural areas.
• Researchers should conduct further and continuous studies with the latest EDHS dataset as it grasps the potential to inform concerned actors to evaluate the impact of their actions on the progress of household access to improved drinking water service.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: https://www.dhsprogram.com/data.
Ethics statement
This study was done based on secondary data analysis, and permission was obtained from the MEASURE DHS program to download and use the data for our study purpose. Hence, ethical approval and participants' consent do not apply to this particular study. The dataset is publicly available in the official database of the MEASURE DHS program with no information for the identification of households.
Author contributions
MAA contributed to writing the manuscript draft. All authors made a substantial contribution to the study's conception, design, methodology, data analysis, read and revised it critically for important intellectual content, and gave the final approval of the manuscript.
Acknowledgments
We would like to thank the MEASURE DHS Program for providing us with the data for further analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
CSA, Central Statistical Agency; DHS, Demographic and Health Survey; EA, Enumeration Areas; EMDHS, Ethiopian Mini Demographic and Health Survey; EPHC, Ethiopian Population and Housing Census; LAIDWS, Limited Access to Improved Drinking Water Service; MOR, Median Odds ratio; SNNPR, South Nation Nationalities and Peoples Region; VA, Variance; WHO, World Health Organization.
References
Abraha, T., Tibebu, A., and Ephrem, G. (2022). Rapid urbanization and the growing water risk challenges in Ethiopia: The need for water sensitive thinking. Front. Water 4, 890229. doi: 10.3389/frwa.2022.890229
Abubakar, I. (2019). Factors influencing household access to drinking water in Nigeria. Utilit. Pol. 58, 40–51. doi: 10.1016/j.jup.2019.03.005
Adams, E. A. (2018). Thirsty slums in African cities: household water insecurity in urban informal settlements of Lilongwe, Malawi. Int. J. Water Resour. Dev. 34, 869–887. doi: 10.1080/07900627.2017.1322941
Afifah, T., Nuryetty, M. T., Cahyorini, A., Musadad, D. A., Schlotheuber, A., Bergen, N., et al. (2018). Subnational regional inequality in access to improved drinking water and sanitation in Indonesia: Results from the 2015 Indonesian National Socioeconomic Survey (SUSENAS). Glob. Health Action 11(Supp.1), 31–40. doi: 10.1080/16549716.2018.1496972
Andualem, Z., Dagne, H., Azene, Z. N., Taddese, A. A., Dagnew, B., Fisseha, R., et al. (2021). Households access to improved drinking water sources and toilet facilities in Ethiopia: A multilevel analysis based on 2016 Ethiopian Demographic and Health Survey. Br. Med. J. Open 11, e042071. doi: 10.1136/bmjopen-2020-042071
Croft, T. N., Marshall, A. M. J., and Allen, C. K. (2018). Guide to DHS Statistics. Rockville, MD. ICF.
Desta, S. (2010). Pastoralism and Development in Ethiopia. Available online at: https://media.africaportal.org/documents/Economic_Focus__Vol_9_No_3_0.pdf (accessed November 10, 2021).
Embassy of Ethiopia in Washington DC. (2022). Overview About Ethiopia. Available online at: https://ethiopianembassy.org/overview-about-ethiopia/ (accessed April 3, 2023).
Ethiopian Public Health Institute and ICF. (2021). Ethiopia Mini Demographic and Health Survey 2019: Final Report. Rockville, MD: EPHI and ICF.
Falk, J., Globisch, B., Angelmahr, M., Schade, W., and Schenk-Mathes, H. (2022). Drinking water supply in rural africa based on a mini-grid energy system—A socio-economic case study for rural development. Sustainability 14, 159458. doi: 10.3390/su14159458
Federal Democratic Republic of Ethiopia Ministry of Water Energy. (2023). Ethiopia's Climate-Resilient Green Economy! Climate Resilience Strategy: Water and Energy. Available online at: https://mowe.gov.et/en/resource_types/water-resource-management-documents-pdf (accessed April 5, 2023).
Gomez, M., Perdiguero, J., and Sanz, A. J. W. (2019). Socioeconomic factors affecting water access in rural areas of low and middle-income countries. Water 11, 202. doi: 10.3390/w11020202
Hasan, M. M., and Alam, K. (2020). Inequality in access to improved drinking water sources and childhood diarrhea in low-and middle-income countries. Indian J. Econ. 226:113493. doi: 10.1016/j.ijheh.2020.113493
He, W.-J., Lai, Y.-S., Karmacharya, B. M., Dai, B.-F., Hao, Y.-T., and Xu, D. (2018). Geographical heterogeneity and inequality of access to improved drinking water supply and sanitation in Nepal. Int. J. Equity Health 17, 1–14. doi: 10.1186/s12939-018-0754-8
Hirai, M., Roess, A., Huang, C., and Graham, J. (2016). Exploring geographic distributions of high-risk water, sanitation, and hygiene practices and their association with child diarrhea in Uganda. Glob. Health Action 9, 32833. doi: 10.3402/gha.v9.32833
Kong, Y.-L., Anis-Syakira, J., Fun, W. H., Balqis-Ali, N. Z., Shakirah, M., Sararaks, S., et al. (2020). Socio-economic factors related to drinking water source and sanitation in Malaysia. Int. J. Environ. Res. Public Health 17, 7933. doi: 10.3390/ijerph17217933
Koskei, E. C., Koskei, R., Koske, M., and Koech, H. (2013). Effect of socio-economic factors on access to improved water sources and basic sanitation in Bomet Municipality, Kenya. Res. J. Environ. Earth Sci. 5, 714–719. doi: 10.19026/rjees.5.5727
Lukman, S., Ismail, A., Asani, M., Bolorunduro, K., Foghi, P., and Oke, I. (2016). Effect of selected factors on water supply and access to safe water in Nigeria. Ife J. Sci. 18, 623–639.
Merlo, J., Chaix, B., Yang, M., Lynch, J., and Råstam, L. (2005). A brief conceptual tutorial of multilevel analysis in social epidemiology: Linking the statistical concept of clustering to the idea of contextual phenomenon. J. Epidemiol. Community Health 59, 443–449. doi: 10.1136/jech.2004.023473
Muluken Azage, A. M., and Nigatu, D. (2020). Exploring geographical variations and inequalities in access to improved water and sanitation in Ethiopia: Mapping and spatial analysis. Heliyon 6, e03828. doi: 10.1016/j.heliyon.2020.e03828
Patrick, M., Hennink, M., Dasmohapatra, M., Rout, M., Clasen, T., and Caruso, B. A. (2023). Influences on water source selection and use among women in rural Odisha, India. Front. Water 5, 1040981. doi: 10.3389/frwa.2023.1040981
Tetteh, J. D., Templeton, M. R., Cavanaugh, A., Bixby, H., Owusu, G., Yidana, S. M., et al. (2022). Spatial heterogeneity in drinking water sources in the Greater Accra Metropolitan Area (GAMA), Ghana. Popul. Environ. 44, 46–76. doi: 10.1007/s11111-022-00407-y
United Nations Department of Economic Social Affairs (2010). Resolution 64/292. The Human Right to Water and Sanitation. Available online at: https://www.un.org/waterforlifedecade/human_right_to_water.shtml
Wang, X., and Hunter, P. R. (2010). A systematic review and meta-analysis of the association between self-reported diarrheal disease and distance from home to water source. Am. J. Trop. Med. Hyg. 83, 582–584. doi: 10.4269/ajtmh.2010.10-0215
WHO/UNICEF. (2021). Joint Monitoring Programme (JMP) for Water Supply, Sanitation, and Hygiene: The World Bank. Available online at: https://washdata.org (accessed April 3, 2023).
World Health Organization and United Nations Children's Fund (2020). Licence: CC BY-NC-SA 3.0 IGO. Progress on Household Drinking Water, Sanitation, and Hygiene 2000–2020: Five Years Into the SDGs2021. Geneva: World Health Organization (WHO) and the United Nations Children's Fund (UNICEF).
World Health Organization and United Nations Children's Fund (2021). Progress on Household Drinking Water, Sanitation, and Hygiene 2000–2020: Five Years Into the SDGs [PDF – 164 Pages]. Geneva: World Health Organization (WHO) and the United Nations Children's Fund (UNICEF).
Keywords: EDHS 2019, households, determinants, spatial analyses, multilevel analyses, Ethiopia, limited access, improved drinking water
Citation: Alemayehu MA, Agimas MC, Shewaye DA, Derseh NM and Aragaw FM (2023) Spatial distribution and determinants of limited access to improved drinking water service among households in Ethiopia based on the 2019 Ethiopian Mini Demographic and Health Survey: spatial and multilevel analyses. Front. Water 5:1166733. doi: 10.3389/frwa.2023.1166733
Received: 16 February 2023; Accepted: 13 April 2023;
Published: 16 May 2023.
Edited by:
Fadl A. Essa, Kafrelsheikh University, EgyptReviewed by:
Zakaria Omara, Kafrelsheikh University, EgyptHitesh Panchal, Government Engineering College, Patan, India
Copyright © 2023 Alemayehu, Agimas, Shewaye, Derseh and Aragaw. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meron Asmamaw Alemayehu, bWVycnlhbGVtMTAxQGdtYWlsLmNvbQ==