 Yijun Qian
Yijun Qian Luoying Lin2
Luoying Lin2 Yaning Li
Yaning Li
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 14 April 2025
Sec. Virtual Reality and Human Behaviour
Volume 6 - 2025 | https://doi.org/10.3389/frvir.2025.1557903
This article is part of the Research TopicUnlocking the potential of XR: Shaping a pro-social metaverseView all articles
Fear of Intimacy (FOI) affects approximately 2.5% of the population, posing diagnostic and treatment challenges relying on time-consuming psychotherapy, self-reported scales, and clinical interviews. This study addresses these clinical hurdles by exploring Virtual Reality’s (VR) potential in assessing FOI. Through simulating intimate scenarios and gathering context-based data, we investigate whether participants’ VR behaviors correlate with FOI and attachment insecurities, specifically avoidance and anxiety. Our findings reveal significant correlations between in-game behaviors and Fear of Intimacy Scale (FIS) scores, notably in avoidance tendencies following exposure to couple-conflict audio. Gender-specific effects are evident, with females exhibiting closeness-anxiety correlations and males displaying distinct fear responses. These results hold significant relevance for understanding FOI assessment challenges. Furthermore, our study underscores the potential of VR to predict avoidance tendencies based on in-game behaviors, while informing the design of gender-specific VR experiences for enhanced clinical assessment outcomes and patient experiences.
Fear of Intimacy (FOI) is a disorder in which patients experience difficulties in building and maintaining close physical and emotional relationships with an intimate partner despite desiring an intimate connection. FOI is characterized by purposeful avoidance of intimacy without realizing it (Descutner and Thelen, 1991). Despite the difficulty in diagnosing this sub-clinical disorder, FOI is found to affect at least 2.5% of the population in Western cultures (Lange and Pauli, 2019). Individuals affected by FOI are typically afflicted by low self-esteem, emotional suppression, and lack of social support (Henderson, 1992), which is associated with high risks for depression (Henderson, 1992), chronic pain (Roy, 2011), physical illness (Roy, 2011), breast cancer (Roy, 2011), alcoholism (Schilit and Gomberg, 1987) and job failure (Sparrevohn and Rapee, 2009).
Fear of Intimacy lacks clinical designation in the Diagnostic and Statistical Manual of Mental Disorders (DSM), making it difficult to distinguish from other conditions, such as social anxiety disorder and avoidant personality disorder, negatively impacting intervention outcomes for patients. A clinical interview encourages self-disclosure and provides more descriptive evidence for subsequent intervention (Letamendi et al., 2010), but its successful application in practice takes multiple sessions due to the difficulty of building trusting relationships with patients that may have FOI (Grossmann et al., 1985). Moreover, clinicians evaluate patients’ FOI levels based on their subjective judgment due to the lack of DSM diagnosis guidance. This makes it difficult to evaluate an individual’s FOI level to the same standards. Although the Fear of Intimacy Scale (FIS) (Doi and Thelen, 1993) and Adult Attachment Scale (AAS) (Collins and Read, 1990) are validated by behavioral psychology, they lack a self-representation aspect, such as self-disclosure measures. Thus, the FIS is rarely used in clinical settings (see Table 1). Furthermore, the clinical interview has to depend on the visitor’s one-sided description and memory recall, which can be different from what actually happened, or missing key information (Hyman and Loftus, 1998). Thus, these clinical FOI assessment challenges can make delivering quality patient care seem more demanding.
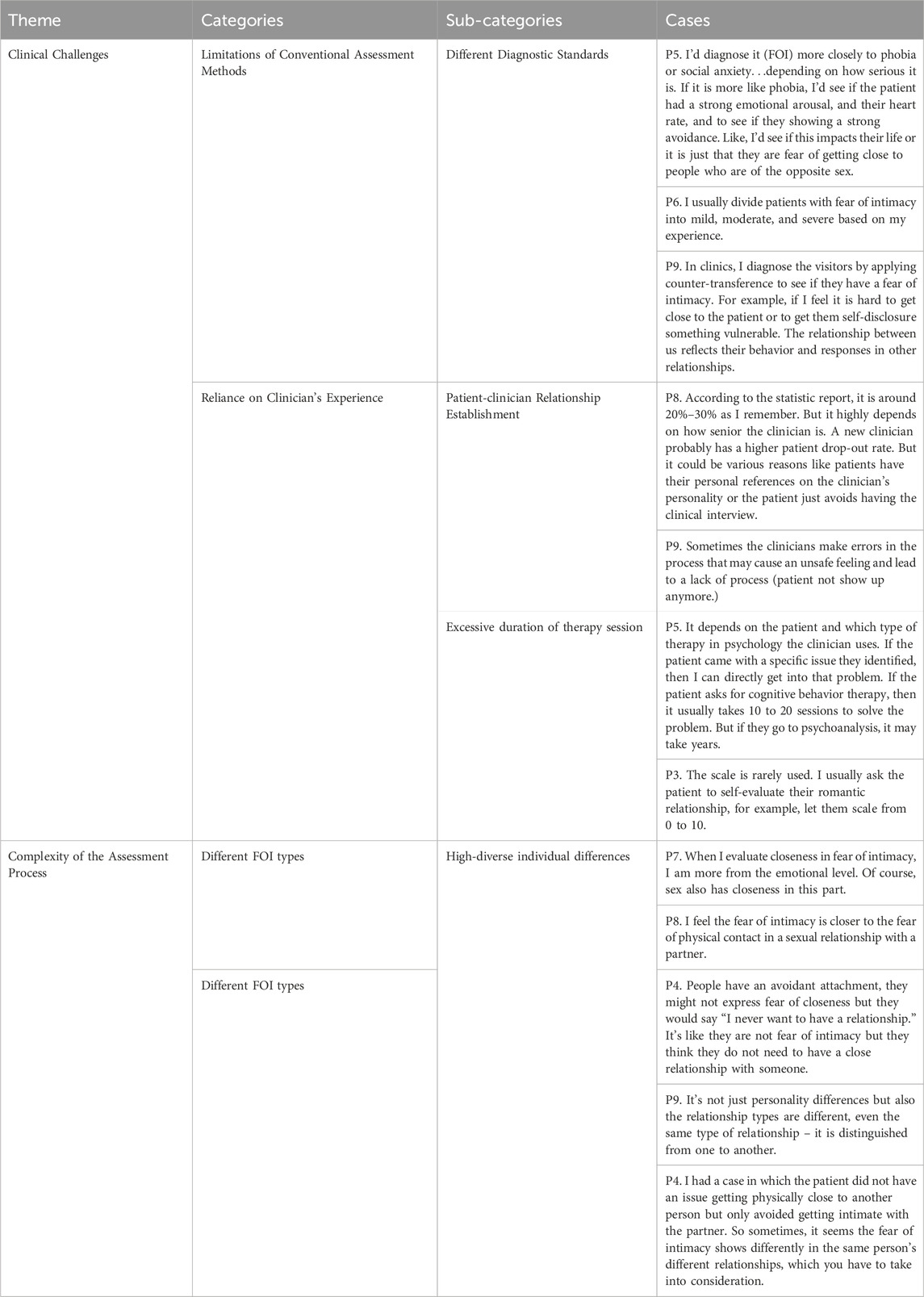
Table 1. This table shows the FOI diagnostic challenges from the focus group interview. The cases are representations that are summarized in the clinicians’ discussion and translated into English. We removed pauses and filler sounds, such as ‘Uh’ and ‘Mm’ during the translation, and kept the original meaning from the clinicians’ speaking.
The Adult Attachment Scale (AAS) (Collins and Read, 1990) is commonly used to assess the attachment insecurities (attachment avoidance and anxiety) of FOI patients prior to FOI intervention with a clinical interview together. In the context of FOI, individuals with attachment insecurities, specifically high levels of attachment avoidance and anxiety, are more likely to struggle with intimacy (Brassard et al., 2009). Identifying these behavioral markers is crucial for assessing FOI. However, the behavioral markers are often hard to access for clinicians due to the nature of the intimate issue, sometimes only being presented in certain scenarios (e.g., couple fights). The diagnostic interviews, such as semi-structured and structured clinical interviews, assist with differential diagnosis and evaluation of comorbid elements critical for comprehensive FOI assessments. However, these interviews involve social contact and self-disclosure, which produces significant anxiety for patients. A part of the challenge was building up a relationship with patients and disclosing their past intimate experiences. Thus, any approach offering additional FOI context-based information and easing the patients’ anxiety in the diagnostic process would substantially improve.
Virtual Reality (VR) can simulate much of the complexity of experiences of the real world in a controllable manner and mimic fear exposure in anxious individuals. Studies found that the in-game behavioral data, such as distance and gazing towards stressors, is different between low- and highly-anxious participants (Mühlberger et al., 2008; Diemer et al., 2015). Some studies explored how social anxiety impacts individuals’ social interactions in VR and the potential of using VR as a diagnostic tool for anxiety disorder (Wieser et al., 2010; Dechant et al., 2017). Other expected benefits of using a virtual agent in FOI assessment include its potential to reduce anxious individuals’ anxiety levels so they can reveal more information and greater intimacy about themselves (Kang et al., 2008; Sykownik and Masuch, 2020).
With the potential of applying VR in FOI assessment, we employed a human-centered design approach to understand the clinical challenges and then investigated using VR for FOI assessment to gather context-rich behavioral data (Figure 1). Additionally, we introduced Approach-Avoidance Tasks (AATs) as an assessment method to gauge individuals’ avoidant behaviors within a simulated virtual environment. Subsequently, we assessed participants’ in-game behavioral responses, including their inclination to approach the virtual partner, and their choices in conflict resolution.

Figure 1. Summary of Virtual Assessment. The left side shows a participant experiencing the VR environment for assessing Fear of Intimacy (FOI). The middle image shows the mapping of the in-game behaviors to indicators of FOI. The right side shows a game environment in which the participant is asked to verbalize their feeling based on the current situation.
Our goal is to explore the questions:
• RQ1. What are the clinical challenges of assessing FOI?
• RQ2. Are avoidant behaviors in a simulated intimacy VR environment associated with FIS score?
• RQ3. Are avoidant behaviors in a simulated intimacy VR environment associated with certain AAS-Attachment insecurities (e.g., Anxiety and Dependence)?
To understand RQ1, we consulted with nine clinicians in a focus group to verify the challenges as a part of our human-centered design. Then we designed a VR application to examine the potential of using VR for FOI assessment. The creation of a three-stage VR assessment is rooted in Attachment Theory, which is often used as a framework to understand the root cause of FOI. The theory suggests that early childhood experiences with primary caregivers influence an individual’s attachment style in adulthood (Bowlby, 1982).
To understand RQ2 and RQ3, we conducted an experiment involving 38 participants who experienced our VR scenarios and provided scores in the Fear of Intimacy Scale (FIS) (Descutner and Thelen, 1991) and Adult Attachment Scale (AAS) (Collins and Read, 1990) by questionnaire. We then analyzed the correlations between participants’ behavioral responses in VR scenarios and their FIS and AAS scores.
Our findings reveal the simulated intimacy VR environment has its effects on capturing participants’ anxiety and fear following exposure to the couple-conflict audio. Additionally, our results highlight gender-specific effects on psychological distance and interaction choices as explanatory factors for anxiety levels, as assessed by FIS and AAS scores. Specifically, female participants exhibited a pronounced alignment between their feelings of closeness to virtual partners and their levels of anxiety. Furthermore, we observed a noteworthy difference in fear levels among male participants and their responses to virtual partners’ attempts at relationship reconciliation.
These findings align with attachment theory, highlighting how attachment-related constructs, such as attachment anxiety and avoidance, manifest in VR settings when examining intimacy-related behaviors. These insights expand our understanding of how individuals navigate intimacy in virtual environments and have implications for developing VR-based interventions for individuals dealing with attachment-related issues or anxiety. Moreover, our results underscore the potential of this novel VR Fear of Intimacy (FOI) paradigm to predict avoidance tendencies based on in-game behavior. We believe this study takes VR application from the traditional realm of exposure therapy to explore the potential of using VR for FOI assessment. This offers clinicians and researchers a more accessible and context-specific data source for assessment and intervention strategies and has the potential to create a new healthcare experience.
A previous review shows that FOI is associated with attachment insecurity (assessed as levels of attachment anxiety and avoidance), which also impacts relationship dissatisfaction (Candel and Turliuc, 2019). As attachment is used here, it refers to an abiding emotional bond between particular individuals (Bartholomew, 1990). Attachment theory has been used as the framework to explore the questions, such as how to conceptualize the avoidance of closeness, the different existing forms of avoidance, and the relationships between defensiveness and avoidant behaviors (Richardson et al., 2023). One study shows that both men’s and women’s anxious and avoidant styles were associated with more frequent negative emotions in relationships (Mikulincer and Shaver, 2005).
Studies in attachment theory proposed that adult avoidance of intimacy has its roots in early childhood experiences with the primary care provider. The Strange Situation scenario (Ainsworth, 1969), involving moving infants from their caregivers to a novel environment, is a standard procedure to observe attachment security in children within the context of caregiver relationships. Upon reunion, children typically display strong physical avoidance and a lack of recognition of the attachment figure. According to the Strange Situation Experiment result (Ainsworth, 1969), the study summarized three typical attachment styles in infants, including secure attachment, anxious attachment, and anxious attachment. The findings are later extended to adults. For example, researchers found a similar pattern in men who are in unhappy marriages practicing different levels of emotional withdrawal to avoid interpersonal conflict (Carstensen et al., 1995).
The attachment behavioral system (Bowlby, 1982) is triggered by distressful conflicts between couples (Simpson et al., 1996). The research shows the involvement of cognitive processes in insecure attachment. Attachment system activation has both psychological (e.g., mental representations triggered in response to threatening cues) and physiological (e.g., neural responses triggered in response to threatening cues) responses, especially in anxious and avoidant attached individuals (Zayas et al., 2009).
In couple therapy, therapists are responsible for identifying attachment-related strategies in distressed couples (Johnson, 2003; Seedall and Wampler, 2013) and understanding couple conflict and attachment insecurity contributes to better relationship satisfaction (Feeney and Karantzas, 2017). In intimate relationship therapy (i.e., emotionally focused couples therapy), explaining the core issues in couples’ conflict is essential for early stage assessment (Johnson et al., 1999). Thus, it is crucial for therapists to identify and shape attached-related strategies in distressed couples (Taylor et al., 2018).
The clinical assessment methods (Goldstein and Hersen, 2000) in FOI include self-report questionnaires, diagnostic interviews, clinician-administered instruments, and behavioral assessment (Antony, 1997; Turk, 1999; Letamendi et al., 2010). The Fear of Intimacy Scale (FIS) is a self-report measure (Nowak and Rauh, 2005) used widely to determine an individual’s level of fear of intimacy. Studies have shown the FIS to be a reliable resource to assess anxiety and fear in close relationships (Descutner and Thelen, 1991; Doi and Thelen, 1993; Greenfield and Thelen, 1997; Sherman and Thelen, 1996). The FIS can assess intimacy in a broad cross-section of participants because it can be applied regardless of the participant’s current relationship status. Nevertheless, indirect evidence shows that questions asking for reflections on actual behaviors are better predictors than those involving imagined scenarios (Ingersoll et al., 2008).
Diagnostic interviews, such as semi-structured and structured clinical interviews, assist with differential diagnosis and evaluation of comorbid elements critical for comprehensive assessments. However, these interviews involve social contact and self-disclosure, which produces significant anxiety for patients. A part of the challenge was building up a relationship with patients and disclosing their past intimate experiences.
Behavioral assessment strategies are increasingly used in clinical practice. A review of Behavioral Assessment Tests (BATs) (McNeil et al., 1995) describes the direct evaluation of body movements and behaviors like role-play, avoidance, and physiological measures for clinical assessment. In particular, the measurement of physiological processes is critical for behavioral assessment of social anxiety and subtypes of social phobias, such as FOI (McNeil et al., 1995). However, most research has focused on mimicking social challenges in the laboratory, with little attention paid to psychophysiological assessment in the natural environment. This may be due to the difficulty of capturing data in patients’ daily workflow. More work needs to be done to bring physiological assessment and BAT strategies into mainstream clinical practice (McNeil et al., 1995).
Interactive virtual environments have been studied as therapeutic approaches for psycho-social related behaviors (Serrano et al., 2019). Applications have employed VR for mental health interventions like psychiatric care (Jl et al., 2017), phobias (Wiederhold et al., 1998), panic disorder (Seol et al., 2017), post-traumatic stress (Difede and Cukor, 2007), and social anxiety (Chesham et al., 2018). In one application, that of speech therapy, VR practice encouraged public speaking in college students (McNeil et al., 1995), who performed significantly better after VR exposure than visualization exposure alone (Prince et al., 2007). VR training for stage fright (Sherman and Thelen, 1996) and performance anxiety (Doi and Thelen, 1993) suggest that training in VR can reduce stress symptoms compared to controls. Speaking to imaginary audiences in VR was rated as more stressful than speaking in an empty room in VR, showing that VR environments can model the audience expectation that drives speech anxiety (Charmaz, 2014). In addition, a study using virtual humans for evaluating man’s social anxiety has shown that males with higher social anxieties showed more stress during a conversation with a female virtual avatar compared to a more confident male (Pan et al., 2012)s.
Earlier studies showed that people felt greater co-presence when the people whom they interacted with were represented visually (Kang et al., 2008; Nowak and Rauh, 2005). Hence, virtual characters have been suggested for use with patients to enhance engagement and self-disclosure, which are critical for relationships with clinicians in psychotherapy. A study demonstrated that socially anxious people revealed more information and greater intimacy about themselves when interacting with a virtual agent (Kang et al., 2008). One study shows how the realism of the avatar impacts how players feel about their body ownership and immersion (Latoschik et al., 2017).
One study found that a two-user VR scenario can induce meaningful interactions, and affect emotional expression based on interpersonal touch intimacy (Sykownik and Masuch, 2020) without haptic feedback. Users experience a similar range of emotional states in VR compared to face-to-face social groups (Moustafa and Steed, 2018).
Recently, several VR works have validated the Approach-Avoidance Tasks (AATs), an assessment tool that measures implicit approach- and avoidance tendencies (Asnaani et al., 2014; Wieser et al., 2010; Lange and Pauli, 2019). One study observed the gaze and head movements of individuals with high anxiety when a virtual agent approaches. Results show that high social anxiety led to a complex pattern of avoidance behavior (Wieser et al., 2010). High FOI individuals desire intimacy, but their fear of rejection keeps them from developing and maintaining close relationships (Sherman and Thelen, 1996). AATs are ideal strategies for detecting people’s fear of closeness, but few studies have explored the efficiency of using AATs in VR to assess fear levels. AATs measure unconscious behavioral tendencies using reaction times for pull and push movements in response to social-anxiety-related stimuli like dating, initiating conversation, and facial responses. For clinicians, measuring a patient’s avoidance behavior might lead to more reliable information on an individual’s social anxiety and avoidance in daily life by circumventing recall bias (Rinck et al., 2010).
VR studies mentioned above have collected players’ in-game quantitative data, such as distance between the virtual agent, gaze, and head movement, to predict anxiety levels (Wieser et al., 2010), but only in a general social context rather than specifically romantic relationships. Instead, our research collects multidimensional player-generated data, including in-game interactions, choices taken, and player-agent distance. Another novel design is that players in our assessment system are placed in a simulated romantic relationship environment without the requirements of completing specific tasks. This allows clinicians to observe patients’ behaviors in a more natural environment.
Our design is guided by the challenges we observed from clinical literature and focus group interviews. The structured clinical interview is a generally accepted methodology in psychiatric diagnosis for DSM (SCID), but due to the complexity, it requires lengthy rapport-building with the patient and professional training (FIRST et al., 1995; First, 2014). The challenges also include the difficulty in in-the-moment access to patients’ internal processes (Laurent and Powers, 2007; Mumtaz et al., 2023) when relationship threats (conflicts) occur; patients lack the feeling of safety due to having to divulge personal stories, leading to stagnation in the interaction. When people interacted visually with agents anonymously, they had better communication due to greater co-presence (Kang et al., 2008; Nowak and Rauh, 2005; Lee et al., 2021; Shih et al., 2023). We used a Human-Centered design approach to verify the clinical challenges by conducting a focus group interview with nine clinicians, the details are described in the Method and Result sections. To sum up, the challenges we observed from both literature and focus group interviews were:
(1) Patients not say something because they are afraid of the probing attitude taken by the clinician (Moutier, 1999; Lian et al., 2022).
(2) Patients not say something meaningful because the conversations are too casual as opposed to probing (Table 1).
(3) Lack of feeling of safety due to having to divulge personal stories, leading to stagnation in the interaction. When people interacted visually with agents anonymously, they had better communication due to greater co-presence (Kang et al., 2008; Nowak and Rauh, 2005; Lee et al., 2021; Shih et al., 2023).
(4) Difficulty in in-the-moment access to patients’ internal processes (Laurent and Powers, 2007; Åhlin et al., 2022) when relationship threats (conflicts) occur.
We used Unity 2020.3.4f1 and Oculus Quest 2 for the VR application development and hope the VR application can address some of the observed challenges to improve patient experience which may enhance the assessment process. There are three scenes (Figure 2) in this VR environment, each of them with a specific goal, including initiating intimacy in the living room with a virtual partner (Intimacy Initiating Room), activating attachment behavioral system (Bowlby, 1982) through couple conflict audio (Attachment Activation Room), and assessing avoidant behaviors after the conflict in the bedroom with the virtual partner (Assessment Room). The concepts of building three scenes are based on the three aspects of FOI (Nowak and Rauh, 2005): highly valuing others, strong emotional arousal, and sharing of personal feelings.
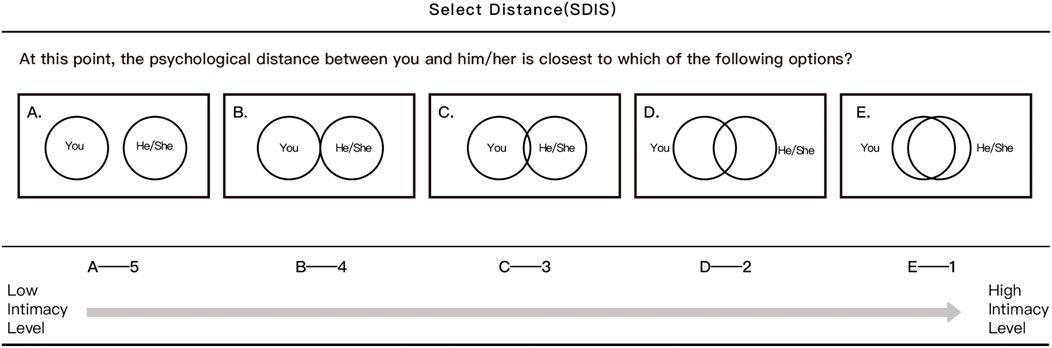
Figure 2. Distance measurements in Virtual Diagnostics. The content of the pop-up asking for the psychological distance between the participant and the virtual partner is shown. ‘1’ represents high intimacy and ‘5’ represents low intimacy Aron et al. (1992).
As mentioned earlier, Attachment Theory is often used as a framework to understand the root cause of FOI, more anxious and avoidant attached individuals typically experience negative emotions in response to relationship-relevant events (Campbell et al., 2005; Cassidy et al., 2013) (Figure 2). Research has shown that enhanced processing gains of emotional cues (visual and sound cues) can help individuals quickly initiate adequate approach or avoidance behaviors (Lang et al., 1997; Zimmer et al., 2022). One study found that changing specific visual and auditory features can effectively create different emotional versions of the same experience and increase the level of fear aroused in users (Chittaro et al., 2014). Taking inspiration from this, we used a couple-conflict scenario to observe participant avoidance tendency, and designed in-game interaction choices based on the level of attachment insecurities and emotional valence.
The Intimacy Initiating Room is developed to test how much participants value their virtual partners; the Attachment Activation Room assesses the level of emotional arousal in a conflict situation; the Assessment Room is built to evaluate participants’ willingness to share personal feelings and observe avoidance levels in their in-game behaviors. The player and the romantic virtual partner are separated after the conflict scene. In this scenario, even if there are no specific tasks for participants, their choices within the game will push the story forward in different directions.
It is worth mentioning that, these three VR scenes are displayed in a fixed order as the story moves forward. A scene transition effect will appear, bringing participants into the next scene after they make the behavioral responses in the last scene. The ending of the story can either be a relationship recovery or deterioration. We decided to duplicate the core module in Strange Situation (Ainsworth and Bell, 1970; Bérubé et al., 2020), a standard procedure to observe attachment security in children within the context of caregiver relationships by separating them from loved ones (Ainsworth, 1969; O’Reilly et al., 2023; Gemignani et al., 2024). We aim to observe participants’ attachment insecurities (e.g., anxiety and avoidance) under the simulated scenario since previous studies found the same pattern in adults in a committed relationship (Carstensen et al., 1995; Babcock and Banks, 2019).
This scene serves the dual purpose of gauging players’ perception of the virtual relationship and eliciting emotional responses, aligning with the three primary perspectives of Fear of Intimacy (FOI). When players initially enter the VR game, they find themselves in a real-world scaled living room, alongside their virtual partner. The scene unfolds in two phases:
• VR Familiarization: Initially, players are given time to familiarize themselves with VR operations, allowing them to self-navigate within the VR environment using controllers.
• Romantic Role Assignment: Subsequently, players assume the role of being in a romantic relationship. Upon entering the living room, a voiced narrator instructs players to imagine themselves in a romantic relationship with their virtual partner. A pop-up interface with options (as depicted in Figure 3) appears in front of the player. Participants are then required to select a distance that symbolizes the level of closeness they perceive in their interpersonal communication with the virtual partner.
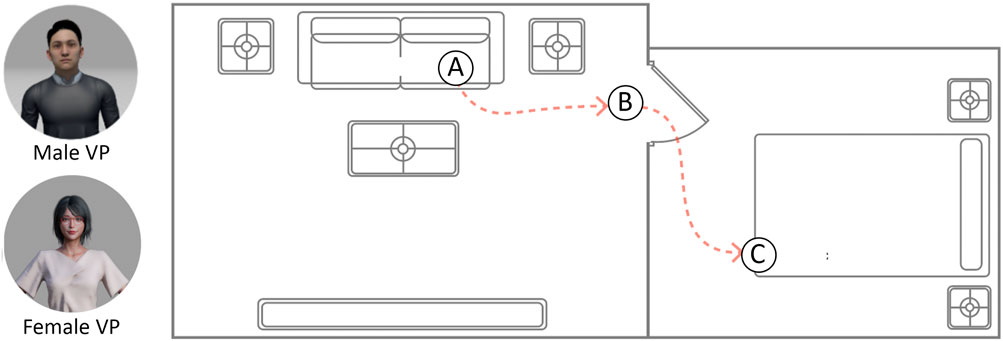
Figure 3. Overview of the environment. Left, are two Virtual Partner Models, a female version and a male version. Right, the overview of the virtual environment. The virtual partner will move from the living room to the bedroom.
This scene effectively captures players’ perceptions of the relationship and their emotional responses, contributing valuable data to our FOI analysis.
The primary objective of this scene is to activate the player’s attachment behavioral system, setting the stage for the assessment of their avoidance behaviors in the subsequent scene. In the realm of intimate relationship therapy, the early stages of assessment involve elucidating core issues within couples’ conflicts and how couples address these issues (Johnson et al., 1999) (Figure 3). Therefore, it is imperative for clinicians to identify and influence attachment-related strategies in couples undergoing distress (Taylor et al., 2018). In this scene, the player is immersed in a dimly lit environment and exposed to an audio-only couple conflict. The audio content comprises a heated argument between a couple, followed by the sound of a door closing, marking the conclusion of the conflict. Subsequently, a user interface appears (Figure 4), prompting players to share their personal reactions and emotional state following the exposure to the couple’s conflict.
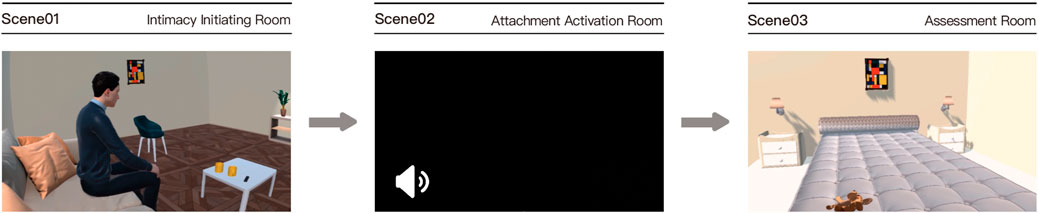
Figure 4. Three scenes for Virtual Diagnostics. The figure shows three game scenes we designed. The left image shows a man sitting on the couch in the living room; the middle image is a black scene with an audio icon; the right image is a real-world scale bedroom.
In this scene, our aim is to observe player behavior and verbal responses after the virtual partner initiates dialogue. The player is situated in a real-world scaled bedroom and hears a door-knocking sound. We recorded the following interactions:
• When the virtual partner knocks on the door, the player can choose to open it by interacting with the handle or refrain from acting, marked as “OpenDoor.”
• Following the door opening, the virtual partner starts a conversation. The player’s choice of interaction, reflecting their real-world reaction, is labeled as “VPDA.” (Figure 4)
• After the player’s selection, the virtual partner approaches and engages in conversation while seated on the bed.
• An in-game notification encourages the player to share thoughts and responses with the virtual partner. The player can choose to communicate or not. Verbal responses, if given, are recorded. (The data on verbal self-disclosure is not presented in the current study).
• Towards the conclusion, the virtual partner may seek relationship reconciliation, noted as “PAU.”
We employed a freely available 3D character model and incorporated animations using Adobe Mixamo, drawing inspiration from prior studies utilizing virtual humans to investigate participant engagement and self-disclosure (Kang et al., 2008; Nowak and Rauh, 2005).
We created two romantic virtual partners (Figure 5), one male and one female, leveraging previous studies that used virtual humans to explore participants’ engagement and self-disclosure. Previous studies also show that those with social anxiety revealed more intimate information when interacting with a virtual agent (Kang et al., 2008). Furthermore, Participants can choose the gender of their virtual partners based on their sexual orientation. One study shows how the realism of the avatar impacts how players feel about their body ownership and immersion (Latoschik et al., 2017). Thus we created virtual partners that simulated the appearance, height, and behavior of realistic people to enhance participants’ sense of immersion and realism.

Figure 5. In-game Behavioral Selections in each scene.
In our study, the appearance of the virtual partner is not customized based on participants’ preferences or mirrors their real partner (Figure 5). The appearance of the virtual partner is the same for people with the same sexual orientation.
Participants’ movement in the real world is reflected in VR, and they are allowed to walk freely in the current VR scene. To choose the interactive or behavioral choices (Figure 6), they have to use a VR controller to make the selection. To incorporate a critical FOI assessment metric, avoidance level, into our game, we offer players carefully designed behavioral choices. These options span a range of avoidance levels, from low to high (Figure 5). Their content was developed in consultation with a local clinician during the design phase. For example, when the virtual partner knocks on the door, the player can choose to either take no action or open the door by physically reaching for the handle (VPDA). In the bedroom scene, as the virtual partner invites the player to sit, the player can opt to remain standing, move closer, or stay put. We promote self-disclosure by having the virtual partner inquire, “Do you have anything to say?” Players can engage in free-form spoken responses. In the VR environment, players can navigate using controllers or by physically moving within the room-scale space (Figure 6). User interfaces present questions as the storyline progresses, allowing players to select their choices and advance the narrative.
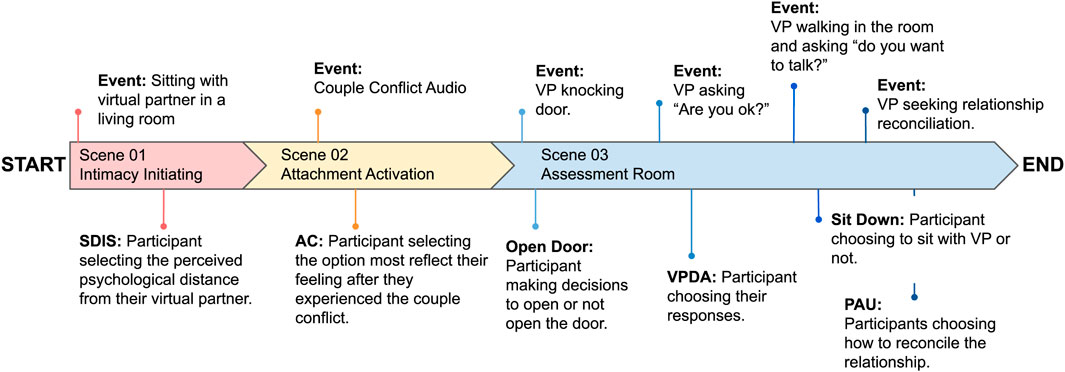
Figure 6. This figure shows the chronological order of occurrence of time when the events happen in simulated intimacy VR environment.
The goal of the focus group was to explore and verify the challenges in FOI assessment to inform the design decisions. We recruited a total of nine clinical psychologists (N = 9) through social media and online platforms. All psychologists must have the National (China)-certificated class-2 psychological counselor certification with at least 1 year of clinical practice and a minimum of 100 h of clinical practice. Three of them worked within the hospital system, another three worked primarily for schools and communities, and the remaining three worked as independent psychologists offering consultation services to individuals. The whole session lasted 90 min and was delivered in Chinese, and the questions used are listed below:
• Q1. How do you see Fear of Intimacy (FOI)?
• Q2. How is FOI generally assessed clinically?
• Q2-1. Do you use any scales to assess the patient’s level of Fear of Intimacy?
• Q2-2. If so, how do you interpret the results, and how do you use this in intervention?
• Q3. What are the difficulties you encounter in the clinical assessment phase?
• Q3-1. Can you share some examples?
• Q3-2. What is the usual reason for patient withdrawal?
Nine clinicians joined the conference call via Voov Meeting. Focus groups began with by moderator introducing the topic of FOI in romantic relationships and ground rules for discussion. Participants were told not to introduce themselves in terms of their years of working experience and detailed professional background, but rather, were asked about their experiences in assessing clients with FOI, the process of assessment, and the difficulties they are facing in patient-clinician relationships.
The session was recorded then transcribed, and verified by two research team members. Thematic analysis was applied in this analysis Clarke and Braun (2017). Two researchers used Nvivo12 to independently code the transcripts into themes first. Then they met for a discussion to unify the themes to create a codebook and coded the transcripts using the codebook while updating it as new themes emerged. The research team then refined the high-level themes through comparisons and memos.
The goal of conducting this user case is to investigate attachment insecurities in the context of VR-based assessment to verify the VR application we designed. Thirty-eight college students aged from 19 to 37 years old (Mean = 23.1, SD = 3.17, 26 female, 12 male) were recruited through posters, social media, campus online groups. After potential participants filled out the research interest form, a researcher would schedule a lab visit with them via text message or call. Consent form was delivered before participants completed a demographic pre-survey, including age, gender identification, and sexual orientation. Individuals with vision impairments, substance abuse issues, or neurological conditions (e.g., migraine, dementia, stroke, Parkinson’s disease) were excluded. After the eligibility screening, the FOI of individual was evaluated when they came to the lab before the VR experience. All participants had normal or corrected vision, no major health or trauma history, and no mobility issues. Compensation, 35 Chinese Yuan cash, was provided for participation after the visit. Ethical approval was obtained from the Institutional Review Board of City University of Hong Kong (IRB No. H002761).
We used the Fear of Intimacy Scale (FIS) Doi and Thelen (1993) and the Adult Attachment Scale (AAS) (Collins and Read, 1990) in this study to investigate the effectiveness of the tool since both scales are widely used in clinical FOI diagnosis. The FIS was used to assess the participants’ level of intimacy anxiety. The FIS has no subscales and has only one dimension. The internal consistency reliability of the scale was 0.93, and the retest reliability was 0.89. The AAS is used to measure adult attachment, particularly for the assessment of adult intimacy and partner relationships. It consists of 18 questions and is divided into two dimensions: Close and Depend (AAS-CD) and Anxiety (AAS-A). Participants were asked to complete the FIS during the recruitment phase and subsequently complete the informed consent form and AAS once they were in the laboratory.
Interaction responses are defined as the interaction selection of the participants after a certain event in each scene. The interaction selections were carefully designed that reflect high to low avoidance and participants’ selections were recorded during the VR after being interviewed by a local clinician. The order of these selections was randomized to present to participants. A detailed description of the event and selection are described below, some of the selections are shown in Figure 5:
• SDIS: Participants’ selection of psychological distance with the virtual partner after the initial interaction (Scene 1. Intimacy initiating room)
• AC: Participants’ selection of their feelings after the couple-conflict event (Scene 2. Attachment Activation Room)
• VPDA: Participants’ behavioral selection after the couple-conflict event and the virtual partner apologizes and the virtual partner asks “Do you feel better now?” (Scene 3. Assessment Room)
• Open Door Event: Participants’ behavioral selection of opening or not opening the door for their virtual partner after the conflict and the virtual partner asks “Can we have a talk?” (Scene 3. Assessment Room). The options include A. ok, let’s talk. and B. No, I do not want to talk.
• Sit Down Event: Participants’ behavioral selection of sitting or not sitting down with their virtual partner to have a conversation after the conflict and the virtual partner asks “Do you want to sit?” (Scene 3. Assessment Room)
• PAU: Participants’ behavioral selection of whether to accept the relationship reconciliation request from their virtual partner after the conflict (Scene 3. Assessment Room)
The maximum, minimum, and average distances between individuals and virtual partners, were also collected. We analyzed the correlation coefficient to explore the relationship between player-NPC distance and FIS and between player-NPC distance and AAS (AAS-CD and AAS-A.) Spearman’s rho was conducted on FIS and distance variables, and the Pearson correlation test was used on AAS and distance variables.
To analyze the association of the OpenDoor and SitDown (Yes/No) events to FIS, we used the Mann-Whitney U test since FIS is not normally distributed (Shapiro-Wil< 0.05). We applied the T-test on Open Door Event and Sit Down Event on AAS-A and AAS-CD because the two measurements were normally distributed (Shapiro-Wilk).
We scaled the participants’ responses from 1 to 7 (AC), or 1 to 5 (SDIS, VPDA, PAU), which indicates different levels of avoidant tendencies from low to high. For FIS, the Kruskal-Wallis Test was conducted because of the non-normal distribution. We use One-way ANOVA analysis to investigate the differences between individuals’ anxieties (AAS-A), and close dependence levels (AAS-CD) since both AAS-CD and AAS-A are normally distributed. Multiple comparisons are assessed (Tukey) if significance was found in the ANOVA.
Participants completed the FIS during the recruitment phase and subsequently completed the informed consent form and AAS once they were in the laboratory. The researcher then explained the operations of VR controllers and Oculus Quest 2 to the participants after their arrival. After adjusting the tightness of the headset and ensuring that the field of vision of the participant was clear and free from blur, participants were asked to get comfortable and walk around in the default Oculus VR home. After the participants got ready, they informed the researcher to start the experimental VR scenes until they finished all selections and interactions. The entire VR experience is approximately 10 min, and the program was delivered in Chinese. Once the experiment finished, they were asked to fill out again the FIS measurements and VR Presence Questionnaire to evaluate the immersive level of the VR application. The compensation was given immediately after the experiment session was over.
We recorded in-game behavioral data which were used to examine the correlations between participants’ behavior choices and avoidance tendencies. Our in-game data collection was divided into interaction responses after each scene and the in-game virtual distance between the player and the virtual partner.
The focus group discussion with clinicians (N = 9) was coded and analyzed in Table 1. The clinical challenges of diagnosing FOI are divided into two categories: The limitations of conventional assessment methods and the complexity of the assessment process. The limitations of the current assessment method include problems such as different diagnostic standards, reliance on clinicians’ experience, patient-clinician relationship establishment, the infrequency of using scales in clinics, and excessive duration of intervention sections. The complexity of the assessment process reflects on the individual differences and the types of FOI (e.g., avoiding physical contact or avoiding emotional closeness).
Our data (N = 38) shows that the maximum and minimum distance between the participant and the virtual partner is not associated with the FIS score and behavioral choices (Table 2) that participants indicated after hearing the couple conflict audio (AC). We observed a trend toward significance between participants’ FIS score and participants’ response on VPDA (p = 0.06585); a similar trend was found between participants’ FIS score and their behavioral response on how to fix the relationship with their virtual partner (PAU) (p = 0.07488). Where the attachment types show different distributions on the female and male participants (Figure 7), we broke down the results by gender and conducted the correlation analysis on the subgroups (Figures 8a, b).

Table 2. Analysis on FIS, AAS, and in-game behaviors.
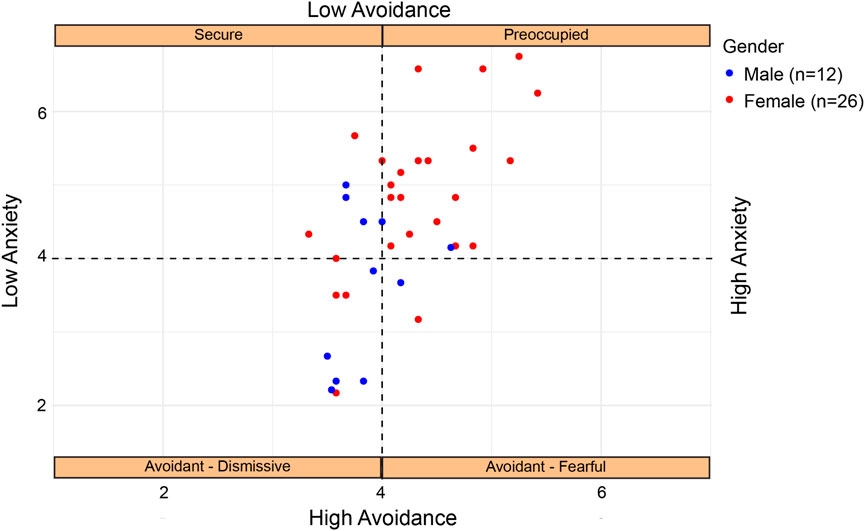
Figure 7. The figure shows the categorization of different attachment styles based on AAS measurements.
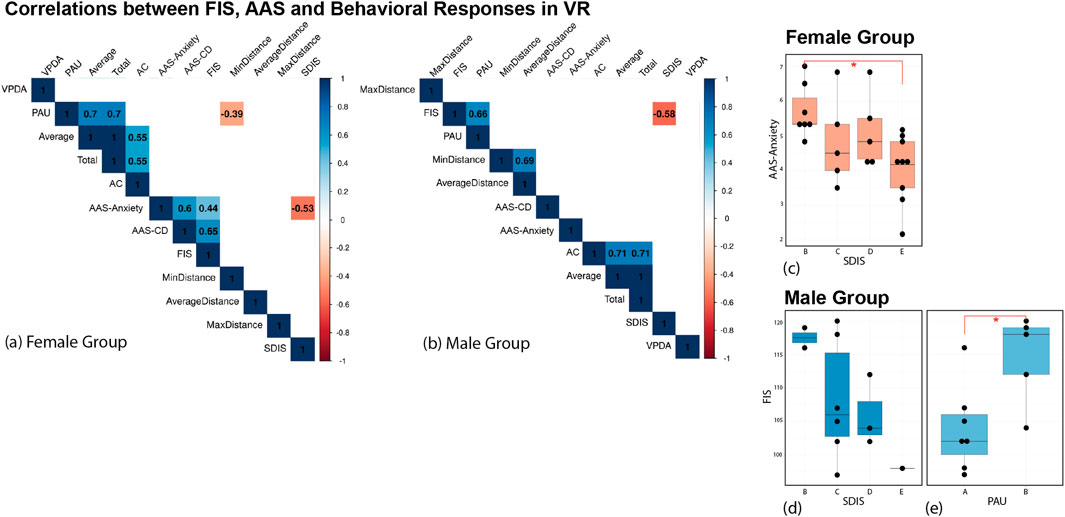
Figure 8. Subgroup Analysis: Correlations between FIS, AAS, and Behavioral Responses in VR. The square with color shows a strong correlation (p ≤ 0.05), (a) Correlation analysis in the female group, (b) Correlation analysis in the male group, (c) Post-hoc test on AAS-Anxiety and SDIS in the female group, (d) Post-hoc test on FIS and SDIS in the male group, (e) Post-hoc test on FIS and PAU in the male group.
We found that there are correlations between FIS and SDIS, and FIS and PAU in the male group. After conducting a two-way ANOVA, we found that in the male group, after the virtual partner asked for relationship reconciliation, the participant had to select an option that represented how they would fix the relationship or not (PAU). Out of five choices (Figure 5), 58.3% males chose “agree to reconcile,” while the rest of them chose “Hug and agree to reconcile.” None of them selected the choices to not reconcile the relationship, which is “Let’s calm down for a little bit,” “Keep Silent,” and “Don’t want to reconcile.” A significant observation was also made regarding the correlation between male participants’ approaches in choosing “agree to reconcile” and “hug and agree to reconcile” to relationship reconciliation with their virtual partner (PAU) and participant’s FIS score (chi-sq = 4.8235, df = 1, p = 0.02807*) (Figures 7, 8e). There are no significant differences between male participants’ selection on SDIS and their FIS scores (Figure 8d). No significant correlation between FIS and behavioral responses in VR is found in the female group (Figure 8a).
Participants were asked to select an option (Figure 5) that best represented their feelings from the interface after they heard the conflict audio (AC). The selections were scaled and coded from 1 to 7 on the basis of the degree of avoidant tendency. No significant difference between participants’ degree of avoidant tendency after hearing the couple-conflict audio (AC) and their closeness and dependency score (AAS-CD). However, there is close to a statistically significant difference between participants’ degree of avoidant tendency (AC) and their anxiety score (AAS-A) (p = 0.0597) after the couple conflict audio.
In the scenario of female players sitting with virtual partners, we asked the participants to select the closeness that they felt with their virtual partner (Figure 2). There is a relationship between their feeling of closeness with their virtual partner and their anxiety score (AAS-A) (p = 0.00528**, F value = 9.412, df = 1). Additionally, by conducting the Tukey HSD post hoc test, we found a significant difference in anxiety levels between females who feel “very close” and females who feel “neither close nor distant” (p = 0.01781*, diff-1.6561) (Figure 8c). This means that in females, anxiety scores can be predicted by psychological distance, as higher measures of SDIS in the game correlated with higher anxiety in general. Whereas in males, the way they responded to reacting to conflict with their partner can explain their FOI level.
We investigated the Fear of Intimacy (FOI) assessment challenges in clinics through the focus group with nine clinicians. The lack of DSM diagnostic guidelines for FOI as a standard clinical counseling problem has led to inconsistent assessment criteria used by clinical counselors in assessing FOI. In addition, we found that the Fear of Intimacy Scale (FIS) only stays in the laboratory and is used rarely in clinics. Thus the assessment of FOI appears to be based on Adult Attachment Scale (AAS) assessment and clinical interviews. This may be due to the limitations of the existing FOI scale in lacking context-based patient information to support patient-centered assessments.
However, clinical interviews also have limitations in terms of relying on the experience and communication skills of the clinical psychologists. Clinical work also relies on unreliable patient self-reporting and a lengthy treatment duration. An effective assessment and intervention not only depends on the clinician’s experience but also depends on the patient’s willingness to be able to self-disclose and establish a healthy patient-clinician relationship with the psychologist. Despite this, many patients with intimacy fear are often triggered by insecurity when the relationship is established too closely, leading to avoidance or drop-out, and we believe based on the qualitative findings that approaches that can help clinicians address the problem can focus on (1) constructing a more private and safe environment to guide patients to self-report, and (2) developing multiple sources of information for intimacy fear assessment.
We created a VR paradigm that uses clinically relevant scenarios to assess avoidance behavior in intimate situations. The interactions in each scene were based on clinically studied measures of self-perception, tendency of avoidance, and degrees of self-disclosure. We explored the potential of capturing FOI in VR by collecting multidimensional participant-generated data, and comparing them with FIS scores provided by each participant to examine the correlation between the avoidance behavioral choices, FIS, and close-dependence and anxiety scores measured by AAS.
Different from previous studies finding that in-game distance is associated with anxiety levels in people with social anxiety to non-player characters (NPCs), there is no significant association found between high-anxious individuals and the distance between them and their virtual partners in our study. One explanation is that FOI is a distinct psychological construct that may not share a strong relationship with in-game distance to NPCs. Social anxiety, on the other hand, is more broadly related to social interactions. It is possible that fear of intimacy has unique characteristics or triggers that are not closely tied to the proximity of virtual characters in a game.
Although no significance is found between participants’ in-game behavior and their FIS and AAS scores, we found that the capture of fear and anxiety levels differed by gender depending on the scene, and this may be related to the different tendencies of males and females in different types of fear of intimacy. In the results divided into subgroups according to gender, we found a significant difference in the fear scores of male in-game behavior when the virtual partner asked for relationship reconciliation. There is a difference in FIS score in the male group of those who chose to reconcile with physical contact (hug and agree to reconcile) and those who chose to reconcile (agree to reconcile) without physical contact. This significant difference in FIS scores could be due to the physical behavior components (Hug or no hug) in the behavioral response. This can also explained by different types of fear of intimacy, and males with FOI typically more commonly share physical fear rather than psychological fear of a romantic relationship. Also, males in our study all chose the options with positive tendencies in reconciling the relationship. For male participants who are “secure” attachment style, this can be explained by the adult attachment style theory that secured individuals with low-avoidance behavior in intimate relationships are more likely to fix the relationship. However, it is hard to use this to explain the male participants who are in avoidant-dissmissive attachment style. Where we did not find the same pattern in the female group, this could be interpreted as a tendency for males to avoid conflict and withdraw from the situation (Christensen and Walczynski, 1997). Indeed, one previous study found that, upon reunion, males in unhappy marriages tend to have emotional withdrawal to avoid interpersonal conflict (Carstensen et al., 1995). This result highlights the difference between genders in relationship conflict resolution (Dunbar and Machin, 2014), suggesting that parameters of this resolution strategy may be differentially expressed in suspected FOI patients who are male vs. female. The relationship between FOI forms and behavioral responses with or without physical contact gives us hints for addressing the avoidance of disclosure and physical fear of partners in FOI.
Another finding is that female participants’ choice of psychological distance in intimate settings in sitting with a virtual partner reflects their anxiety levels. In particular, the difference between female participants who felt they were “generally intimate” and “very intimate” with the virtual partner was significant which aligns with the attachment theory explanation that individuals with higher attachment anxiety tend to seek greater closeness and reassurance in relationships due to their fear of abandonment or rejection. The finding was that female participants who felt “very intimate” with the virtual partner exhibited higher anxiety levels, which can be seen as a manifestation of their attachment anxiety. However, this pattern is not found in the male group and this may be related to the sensitivity of females in interpersonal relationships in an initiated environment (Reis and Grenyer, 2004). This finding highlights the adaptability of attachment theory to virtual contexts and underscores the importance of understanding how individuals navigate intimacy within digital spaces.
The gender differences observed in participants’ responses are also noteworthy. For example, SDIS seems an interesting marker in virtual reality, which captured anxiety in the female group and fear in the male group, the same environment that captured different attachment insecurities might be due to the distribution of the attachment type and the nature of attachment insecurities tends to be different in gender. The gender-specific nature of these findings suggests that gender may play a role in how individuals approach and experience intimacy in virtual environments, which can inform the design of VR experiences tailored to specific gender-related dynamics. These findings shed light on the conflict resolution strategies employed by individuals in virtual environments. Understanding these strategies can be useful not only for psychological research but also for industries such as gaming and virtual dating platforms, where interpersonal interactions are central.
The lack of demographic diversity is a limitation of our experiment. Our study tested only a single group of college students in a Chinese cultural context. It does not include analyses in different cultural contexts, and across age groups and relationship statuses. Chinese populations may bias our sample to non-sexual forms of expression of FOI, giving priority to components like commitment over components like passion (Ingersoll et al., 2008). In particular, higher individualism in the East predicts FOI, showing that the cultural context of East and West differ in terms of prediction of FOI, although the structures of the validated scales for East and West cultures do not differ (Ingersoll et al., 2008). There may be contextual differences in interpersonal relationships between East and West, thus a bigger study with the Western demographic is needed to validate the VR assessment approach for Western populations. In addition to cultural differences, we also suggest that future studies should focus on the clinical population to validate the findings.
In terms of gender differences, our sample size for males (N = 12) is relatively small compared to the female group (N = 26). In a study of gender differences in FOI, females were found to have lower FIS correlations of desired intimacy compared to actual intimacy (Thelen et al., 2000), which indicates that our over-dependence on female samples may be over-stating the correlations with physical intimacy in the study. It is worth noting that individuals in our sample generally had high levels of FIS and anxiety, so differences between those with low levels of intimacy and those with high FIS may not have been distinguished.
We have a limited representative distribution of attachment styles (only “avoidant-dismissive”, “Secure” and “Preoccupied”.) The type of “avoidant-fear” individuals are not presented because of the limitation of the recruitment method. Thus, the findings may not fully capture the complexity of attachment-related responses. A further recruitment method should be updated to include the diversity of attachment styles in this study.
In addition, due to the immense time requirements already allotted for the full testing, our prototype lacked an exit interview to explore the immersive experience and presence in more depth. Although the scenarios were designed to be consistent with what was asked in the clinic, our design did not validate the participants’ level of situational arousal on the biological level, and future directions could consider incorporating physiological data probes to test actual levels of emotional arousal in different scenarios. Additionally, the extent to which they genuinely perceive the virtual agent as an intimate relationship partner and their level of immersion might be limited.
Finally, our system only simulated environments that present romantic relationships, and it may exclude the assessment of people who do not have such intimate experiences but still desire such relationships. Within the VR environment, only emotional intimacy can be assessed, but in fact, fear of intimate physical behavior is included in the FIS questionnaire. It is a challenge to stimulate a haptically plausible physically intimate environment in a believable way that will not trigger people’s trauma or ethical concerns. Future work may explore the suggestibility of virtual elements to measure FOI physical contact. An advantage of our VR intervention is its potential to probe FOI without needing to establish clinical rapport, and this might let us bypass establishing rapport with some groups who are uncomfortable with communicating and self-disclosing to strangers and clinicians (He, 2021). Based on our summary of the challenges of clinically assessing FOI, we suggest future studies explore other behavioral or biometric measurements that is not included in this study, such as gazing behavior for predictive avoidance behavior (Guerrero, 1996) and electrodermal activity for emotional responses.
Participants in VR studies are provided informed consent that includes a clear understanding of the study’s objectives, procedures, and potential emotional or psychological impact. Given the intimate nature of the scenarios, the researcher ensures that participants are fully aware of what they will experience and how their data will be used. Data was analyzed anonymously and separately.
We investigated a novel VR framework aimed at identifying Fear of Intimacy (FOI) avoidant behaviors. Utilizing a role-playing VR setting, we gathered participant data via the Fear of Intimacy Scale (FIS) and attachment style questionnaires (AAS) and employed in-game behaviors to forecast FOI levels. Several metrics successfully predicted variations in FIS and anxiety levels. These findings align with attachment theory and contribute to the field by demonstrating how attachment-related constructs, such as attachment anxiety and avoidance, can be observed within VR settings when examining intimacy-related behaviors. These findings expand our understanding of how individuals navigate intimacy in virtual environments and provide insights that can inform the development of VR-based interventions and therapies for individuals with attachment-related issues or anxiety. Additionally, the gender-specific nature of these findings emphasizes the importance of considering gender dynamics in future research and applications of VR technology in the realm of intimacy and attachment.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Institutional Review Board of City University of Hong Kong. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
YQ: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review and editing. LL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review and editing. YL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review and editing. ZW: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Writing – original draft. ML: Project administration, Software, Supervision, Validation, Writing – review and editing. XT: Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. RL: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
The author(s) declare that no financial support was received for the research and/or publication of this article.
The authors would like to gratefully acknowledge the invaluable suggestions from the reviewers.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Åhlin, P., Almström, P., and Wänström, C. (2022). When patients get stuck: a systematic literature review on throughput barriers in hospital-wide patient processes. Health Policy 126, 87–98. doi:10.1016/j.healthpol.2021.12.002
Ainsworth, M. D. S. (1969). Individual differences in strange-situational behaviour of one-year-olds. London: Academie Press.
Ainsworth, M. D. S., and Bell, S. M. V. (1970). Attachment, exploration, and separation: illustrated by the behavior of one-year-olds in a strange situation. Child. Dev. 41 (1), 49–67. doi:10.2307/1127388
Antony, M. M. (1997). Assessment and treatment of social phobia. Can. J. Psychiatry 42, 826–834. doi:10.1177/070674379704200804
Aron, A., Aron, E. N., and Smollan, D. (1992). Inclusion of other in the self scale and the structure of interpersonal closeness. J. Personality Soc. Psychol. 63, 596–612. doi:10.1037/0022-3514.63.4.596
Asnaani, A., Rinck, M., Becker, E., and Hofmann, S. G. (2014). The effects of approach–avoidance modification on social anxiety disorder: a pilot study. Cognitive Ther. Res. 38, 226–238. doi:10.1007/s10608-013-9580-x
Babcock, J. C., and Banks, J. C. (2019). Interobserver agreement and the effects of ethnicity on observational coding of affect. J. Soc. Personal Relat. 36, 2842–2856. doi:10.1177/0265407518803474
Bérubé, A., Blais, C., Fournier, A., Turgeon, J., Forget, H., Coutu, S., et al. (2020). Childhood maltreatment moderates the relationship between emotion recognition and maternal sensitive behaviors. Child abuse and Negl. 102, 104432. doi:10.1016/j.chiabu.2020.104432
Bowlby, J. (1982). Attachment and loss: retrospect and prospect. Am. J. orthopsychiatry 52, 664–678. doi:10.1111/j.1939-0025.1982.tb01456.x
Brassard, A., Lussier, Y., and Shaver, P. R. (2009). Attachment, perceived conflict, and couple satisfaction: test of a mediational dyadic model. Fam. Relat. 58, 634–646. doi:10.1111/j.1741-3729.2009.00580.x
Campbell, L., Simpson, J. A., Boldry, J., and Kashy, D. A. (2005). Perceptions of conflict and support in romantic relationships: the role of attachment anxiety. J. Personality Soc. Psychol. 88, 510–531. doi:10.1037/0022-3514.88.3.510
Carstensen, L. L., Gottman, J. M., and Levenson, R. W. (1995). Emotional behavior in long-term marriage. Psychol. Aging 10, 140–149. doi:10.1037/0882-7974.10.1.140
Cassidy, J., Jones, J. D., and Shaver, P. R. (2013). Contributions of attachment theory and research: a framework for future research, translation, and policy. Dev. Psychopathol. 25, 1415–1434. doi:10.1017/S0954579413000692
Charmaz, K. (2014). “Constructing grounded theory,” in Introducing qualitative methods series (London, England: SAGE Publications).
Chesham, R. K., Malouff, J. M., and Schutte, N. S. (2018). Meta-analysis of the efficacy of virtual reality exposure therapy for social anxiety. Behav. Change 35, 152–166. doi:10.1017/bec.2018.15
Chittaro, L., Buttussi, F., and Zangrando, N. (2014). “Desktop virtual reality for emergency preparedness: user evaluation of an aircraft ditching experience under different fear arousal conditions,” in Proceedings of the 20th ACM symposium on virtual reality software and technology - vrst ’14 (Edinburgh, Scotland: ACM Press), 141–150.
Christensen, A., and Walczynski, P. T. (1997). “Conflict and satisfaction in couples,” in Satisfaction in close relationships (New York, NY, US: The Guilford Press), 249–274.
Clarke, V., and Braun, V. (2017). Thematic analysis. J. Posit. Psychol. 12, 297–298. doi:10.1080/17439760.2016.1262613
Collins, N. L., and Read, S. J. (1990). Adult attachment, working models, and relationship quality in dating couples. J. Personality Soc. Psychol. 58, 644–663. doi:10.1037/0022-3514.58.4.644
Dechant, M., Trimpl, S., Wolff, C., Mühlberger, A., and Shiban, Y. (2017). Potential of virtual reality as a diagnostic tool for social anxiety: a pilot study. Comput. Hum. Behav. 76, 128–134. doi:10.1016/j.chb.2017.07.005
Descutner, C. J., and Thelen, M. H. (1991). Development and validation of a fear-of-intimacy scale. Psychol. Assess. A J. Consult. Clin. Psychol. 3, 218–225. doi:10.1037/1040-3590.3.2.218
Diemer, J., Alpers, G. W., Peperkorn, H. M., Shiban, Y., and Mühlberger, A. (2015). The impact of perception and presence on emotional reactions: a review of research in virtual reality. Front. Psychol. 6, 26. doi:10.3389/fpsyg.2015.00026
Difede, J., and Cukor, J. (2007). Virtual reality exposure therapy for the treatment of posttraumatic stress disorder following september 11, 2001. J. Clin. Psychiatry 68, 1682–1689. doi:10.4088/JCP.v68n1102
Doi, S. C., and Thelen, M. H. (1993). The fear-of-intimacy scale: replication and extension. Psychol. Assess. 5, 377–383. doi:10.1037/1040-3590.5.3.377
Dunbar, R., and Machin, A. (2014). Sex differences in relationship conflict and reconciliation. J. Evol. Psychol. 12, 109–133. doi:10.1556/jep-d-13-00024
Feeney, J. A., and Karantzas, G. C. (2017). Couple conflict: insights from an attachment perspective. Curr. Opin. Psychol. 13, 60–64. doi:10.1016/j.copsyc.2016.04.017
First, M. B. (2014). Structured clinical interview for the dsm (scid). Encycl. Clin. Psychol. 1–6. doi:10.1002/9781118625392.wbecp351
First, M., Spitzer, R., Gibbon, M., and Williams, J. (1995). The structured clinical interview for dsm-iii-r personality disorders (scid-ii). Part i: description. J. personality Disord. 9, 83–91. doi:10.1521/pedi.1995.9.2.83
Gemignani, M., Giannotti, M., Rigo, P., and De Falco, S. (2024). Attentional bias to infant faces might be associated with previous care experiences and involvement in childcare in same-sex mothers. Int. J. Clin. health Psychol. 24, 100419. doi:10.1016/j.ijchp.2023.100419
Greenfield, S., and Thelen, M. (1997). Validation of the fear of intimacy scale with a lesbian and gay male population. J. Soc. Personal Relat. 14, 707–716. doi:10.1177/0265407597145007
Grossmann, K., Grossmann, K. E., Spangler, G., Suess, G., and Unzner, L. (1985). Maternal sensitivity and newborns’ orientation responses as related to quality of attachment in northern Germany. Monogr. Soc. Res. Child Dev. 50, 233–256. doi:10.2307/3333836
Guerrero, L. K. (1996). Attachment-style differences in intimacy and involvement: a test of the four-category model. Commun. Monogr. 63, 269–292. doi:10.1080/03637759609376395
Henderson, A. S. (1992). “Social support and depression,” in The meaning and measurement of social support (Washington, DC, US: Hemisphere Publishing Corp), 85–92.
Hyman, I. E., and Loftus, E. F. (1998). Errors in autobiographical memory. Clin. Psychol. Sci. Pract. 18, 933–947. doi:10.1016/s0272-7358(98)00041-5
Ingersoll, T. S., Norvilitis, J. M., Zhang, J., Jia, S., and Tetewsky, S. (2008). Reliability and validity of the fear of intimacy scale in China. J. Personality Assess. 90, 270–279. doi:10.1080/00223890701885019
Jl, M.-K., Be, B., Sj, K., and Bo, R. (2017). The use of virtual reality technology in the treatment of anxiety and other psychiatric disorders. Harv. Rev. psychiatry 25, 103–113. doi:10.1097/HRP.0000000000000138
Johnson, S. M. (2003). Attachment theory: a guide for couple therapy. Attachment Process. couple Fam. Ther., 103–123.
Johnson, S. M., Hunsley, J., Greenberg, L., and Schindler, D. (1999). Emotionally focused couples therapy: status and challenges. Clin. Psychol. Sci. Pract. 6 (1). 67–79. doi:10.1093/clipsy.6.1.67
Kang, S.-H., Watt, J. H., and Ala, S. K. (2008). “Social copresence in anonymous social interactions using a mobile video telephone,” in Proceeding of the twenty-sixth annual CHI conference on Human factors in computing systems - CHI ’08 (Florence, Italy: ACM Press), 1535.
Lang, P. J., Bradley, M. M., and Cuthbert, B. N. (1997). “Motivated attention: affect, activation, and action,” in Attention and orienting: sensory and motivational processes (Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers), 97–135.
Lange, B., and Pauli, P. (2019). Social anxiety changes the way we move—a social approach-avoidance task in a virtual reality CAVE system. PLOS ONE 14, e0226805. doi:10.1371/journal.pone.0226805
Latoschik, M. E., Roth, D., Gall, D., Achenbach, J., Waltemate, T., and Botsch, M. (2017). “enThe effect of avatar realism in immersive social virtual realities,” in Proceedings of the 23rd ACM symposium on virtual reality software and technology (Gothenburg Sweden: ACM), 1–10.
Laurent, H., and Powers, S. (2007). Emotion regulation in emerging adult couples: temperament, attachment, and HPA response to conflict. Biol. Psychol. 76, 61–71. doi:10.1016/j.biopsycho.2007.06.002
Lee, Y., Chung, J. J. Y., Song, J. Y., Chang, M., and Kim, J. (2021). “Personalizing ambience and illusionary presence: how people use “study with me” videos to create effective studying environments,” in Proceedings of the 2021 CHI conference on human factors in computing systems (New York, NY, USA: Association for Computing Machinery).
Letamendi, A. M., Chavira, D. A., and Stein, M. B. (2010). Issues in the assessment of social phobia. A Rev. 15.
Lian, O. S., Nettleton, S., Grange, H., and Dowrick, C. (2022). “i’m not the doctor; i’m just the patient”: patient agency and shared decision-making in naturally occurring primary care consultations. Patient Educ. Couns. 105, 1996–2004. doi:10.1016/j.pec.2021.10.031
McNeil, D. W., Ries, B. J., and Turk, C. L. (1995). “Behavioral assessment: self-report, physiology, and overt behavior,” in Social phobia: diagnosis, assessment, and treatment (New York, NY, US: The Guilford Press), 202–231.
Moustafa, F., and Steed, A. (2018). “A longitudinal study of small group interaction in social virtual reality,” in Proceedings of the 24th ACM symposium on virtual reality software and technology (tokyo Japan: acm), 1–10.
Moutier, S., and Stein, M. B. (1999). The history, epidemiology, and differential diagnosis of social anxiety disorder. J. Clin. Psychiatry 60 (5), 4–8.
Mühlberger, A., Neumann, R., Wieser, M. J., and Pauli, P. (2008). The impact of changes in spatial distance on emotional responses. Emotion 8, 192–198. doi:10.1037/1528-3542.8.2.192
Mumtaz, H., Riaz, M. H., Wajid, H., Saqib, M., Zeeshan, M. H., Khan, S. E., et al. (2023). Current challenges and potential solutions to the use of digital health technologies in evidence generation: a narrative review. Front. Digital Health 5, 1203945. doi:10.3389/fdgth.2023.1203945
Nowak, K. L., and Rauh, C. (2005). The influence of the avatar on online perceptions of anthropomorphism, androgyny, credibility, homophily, and attraction. J. Computer-Mediated Commun. 11, 153–178. doi:10.1111/j.1083-6101.2006.tb00308.x
O’Reilly, G., Cheung, P. S., and McCaffrey, T. (2023). A pilot study of maternal songwriting to support bonding during pregnancy:“i could feel her rise and fall with my breath while singing”. J. midwifery and women’s health 68, 205–209. doi:10.1111/jmwh.13463
Pan, X., Gillies, M. F. P., Barker, C., Clark, D. M., and Slater, M. (2012). Socially anxious and confident men interact with a forward virtual woman: an experimental study. PLoS ONE 7, e32931. doi:10.1371/journal.pone.0032931
Prince, M., Patel, V., Saxena, S., Maj, M., Maselko, J., Phillips, M. R., et al. (2007). No health without mental health. Lancet 370, 859–877. doi:10.1016/S0140-6736(07)61238-0
Reis, S., and Grenyer, B. F. S. (2004). Fear of intimacy in women: relationship between attachment styles and depressive symptoms. Psychopathology 37, 299–303. doi:10.1159/000082268
Rinck, M., Rörtgen, T., Lange, W.-G., Dotsch, R., Wigboldus, D. H. J., and Becker, E. S. (2010). Social anxiety predicts avoidance behaviour in virtual encounters. Cognition Emot. 24, 1269–1276. doi:10.1080/02699930903309268
Roy, R. (2011). Social support, health, and illness: a complicated relationship. Toronto: University of Toronto Press.
Schilit, R., and Gomberg, E. L. (1987). Social support structures of women in treatment for alcoholism. Health and Soc. Work 12, 187–195. doi:10.1093/hsw/12.3.187
Seedall, R. B., and Wampler, K. S. (2013). An attachment primer for couple therapists: research and clinical implications. J. Marital Fam. Ther. 39, 427–440. doi:10.1111/jmft.12024
Seol, E., Min, S., Seo, S., Jung, S., Lee, Y., Lee, J., et al. (2017). “Drop the beat: virtual reality based mindfulness and cognitive behavioral therapy for panic disorder — a pilot study,” in Proceedings of the 23rd ACM symposium on virtual reality software and technology (Gothenburg Sweden: ACM), 1–3.
Serrano, B., Botella, C., Wiederhold, B. K., and Baños, R. M. (2019). Virtual reality and anxiety disorders treatment: evolution and future perspectives. Virtual Real. Psychol. Neurocognitive Interventions, 47–84. doi:10.1007/978-1-4939-9482-3_3
Sherman, M. D., and Thelen, M. H. (1996). Fear of intimacy scale: validation and extension with adolescents. J. Soc. Personal Relat. 13, 507–521. doi:10.1177/0265407596134002
Shih, M. T., Lee, Y.-C., Huang, C.-M., and Chan, L. (2023). A feeling of déjà vu: the effects of avatar appearance-similarity on persuasiveness in social virtual reality. Proc. ACM Hum.-Comput. Interact. 7, 1–31. doi:10.1145/3610167
Simpson, J. A., Rholes, W. S., and Phillips, D. (1996). Conflict in close relationships: an attachment perspective. J. Personality Soc. Psychol. 71, 899–914. doi:10.1037/0022-3514.71.5.899
Sparrevohn, R. M., and Rapee, R. M. (2009). Self-disclosure, emotional expression and intimacy within romantic relationships of people with social phobia. Behav. Res. Ther. 47, 1074–1078. doi:10.1016/j.brat.2009.07.016
Sykownik, P., and Masuch, M. (2020). “The experience of social touch in multi-user virtual reality,” in 26th ACM symposium on virtual reality software and technology (New York, NY, USA: Association for Computing Machinery), VRST ’20. doi:10.1145/3385956.3418944
Taylor, N. C., Seedall, R. B., Robinson, W. D., and Bradford, K. (2018). The systemic interaction of attachment on psychophysiological arousal in couple conflict. J. Marital Fam. Ther. 44, 46–60. doi:10.1111/jmft.12239
Thelen, M. H., Vander Wal, J. S., Thomas, A. M., and Harmon, R. (2000). Fear of intimacy among dating couples. Behav. Modif. 24, 223–240. doi:10.1177/0145445500242004
Wiederhold, B. K., Gevirta, R., and Wiederhold, M. D. (1998). Fear of flying: a case report using virtual reality therapy with physiological monitoring. CyberPsychology and Behav. 1, 97–103. doi:10.1089/cpb.1998.1.97
Wieser, M. J., Pauli, P., Grosseibl, M., Molzow, I., and Mühlberger, A. (2010). Virtual social interactions in social anxiety—the impact of sex, gaze, and interpersonal distance. Cyberpsychology, Behav. Soc. Netw. 13, 547–554. doi:10.1089/cyber.2009.0432
Zayas, V., Shoda, Y., Mischel, W., Osterhout, L., and Takahashi, M. (2009). Neural responses to partner rejection cues. Psychol. Sci. 20, 813–821. doi:10.1111/j.1467-9280.2009.02373.x
Keywords: virtual reality, human-computer interaction, game, fear of intimacy, psychological assessment
Citation: Qian Y, Lin L, Li Y, Wang Z, Li M, Tong X and LC R (2025) Virtual assessment: using in-game behaviors during immersive role-play for contextually relevant assessment of fear of intimacy. Front. Virtual Real. 6:1557903. doi: 10.3389/frvir.2025.1557903
Received: 09 January 2025; Accepted: 14 March 2025;
Published: 14 April 2025.
Edited by:
Ren Xu, g.tec medical engineering GmbH, AustriaReviewed by:
Triton Ong, Doxy.me Inc., United StatesCopyright © 2025 Qian, Lin, Li, Wang, Li, Tong and LC. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: RAY LC, bGNAcmF5bGMub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.