
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Virtual Real., 13 March 2025
Sec. Virtual Reality in Medicine
Volume 6 - 2025 | https://doi.org/10.3389/frvir.2025.1552370
 Lillian Hung1,2*
Lillian Hung1,2* Carol Hok Ka Ma3Chih Yun Huang4
Carol Hok Ka Ma3Chih Yun Huang4 Joey Wong1,2
Joey Wong1,2 Karen Lok Yi Wong2
Karen Lok Yi Wong2 Keng Hao Chew5Ying Cheng Chao4Ali Hussein2Katrina Yuen2Lily Haopu Ren2
Keng Hao Chew5Ying Cheng Chao4Ali Hussein2Katrina Yuen2Lily Haopu Ren2 Yong Zhao2
Yong Zhao2Background: The increasing ageing population highlights the urgent need for enhanced dementia care training among formal caregivers. Virtual reality technology has emerged as an innovative tool to address this challenge, offering potential improvements in training outcomes. This scoping review focuses on identifying the barriers, facilitators, and impacts of implementing fully immersive VR training programs for dementia care among staff in long-term care facilities.
Method: The Consolidated Framework for Implementation Research informed our searching strategies and data analysis. Following the Joanna Briggs Institute methodology and PRISMA-ScR guidelines, this review included both published and unpublished studies. A systematic search of CINAHL, MEDLINE, Embase, Scopus, Web of Science, and ProQuest databases yielded 469 publications, with nine articles meeting the inclusion criteria. These studies, published in English between 2015 and 2024, involved 362 formal caregivers with a mean age ranging from 44.7 to 65 years. VR interventions were found to foster empathy (through first-person perspectives) and to help participants recognize triggers of responsive behaviors and apply solutions (via second-person and third-person perspectives).
Results: Most barriers and facilitators were associated with the innovation domain. The primary barriers included simulation sickness, uncomfortable headsets, and limited immersive, interactive, and embodied experiences. Key facilitators were technical advantages, highly immersive, interactive, and embodied experiences, a safe training environment, individual attributes, and the provision of orientation and support during training. The VR training programs demonstrated the potential to impact caregiving at multiple levels, including initial reactions, learning (knowledge, skills, and attitudes), behavioral changes, and broader systemic outcomes.
Conclusion: This scoping review maps out the current landscape of VR training for healthcare professionals. Future research should continuously improve the VR training experience by investigating the impact of VR training on dementia care outcomes, such as caregiver-resident interactions. By addressing the barriers and leveraging the facilitators, VR training can be successfully implemented to enhance the quality of care and wellbeing of residents living with dementia in long-term care homes.
Due to population aging, the prevalence of dementia in long-term care (LTC) has increased (Falzarano et al., 2022). In Canadian LTC homes, almost 70% of residents live with dementia, according to the latest statistics in 2015–2016 (Canadian Institute for Health Information, 2024), and in Asian countries such as Taiwan, the prevalence of residents with dementia is about 87% in LTC settings (Kao et al., 2022), There is a growing need for staff training on providing care for residents with dementia in LTC. People living with dementia (PLWD) may have challenges to communicate their needs. Unmet needs may trigger responsive behaviors by these individuals (Cohen-Mansfield et al., 2015). 50% of residents with dementia in Canadian LTC homes had responsive behaviors (Canadian Institute for Health Information, 2024). In addition to addressing responsive behaviors, staff face physical and emotional inquiries and moral distress, causing burnout and turnover (Woodhead et al., 2016; Shrestha et al., 2021). Therefore, to ensure the quality of care for residents and the safety and wellbeing of residents and staff, training staff on effective ways to work and communicate with residents is crucial (Zimmerman et al., 2005).
With the rapid development of technology, some literature has explored how virtual reality (VR) may support the provision of training on dementia care and the benefits of using VR in dementia care training (Hirt and Beer, 2020). First, VR increases healthcare providers’ access to dementia training and provides them with a safe and controlled environment to build competence working with PLWD, such as enhancing their skills, confidence, dementia symptom awareness, and empathy towards PLWD (Adefila et al., 2016; Muirhead et al., 2021; Plotzky et al., 2021; Mäkinen et al., 2022). Also, VR dementia care training can be provided at different times, places and training resources and is not expensive (Slater et al., 2019; Muirhead et al., 2021; Plotzky et al., 2021; Brown et al., 2023).
Although a review study on VR training for caregiving (Wang et al., 2023) exists, it focused only on informal caregivers, leaving formal caregiving contexts underexplored. Other studies on VR training for students and staff (Barros Una et al., 2023; Bauce et al., 2023; Tay et al., 2023) did not address dementia care, a critical area for improving competency for quality of care. With the advancement of using VR technologies in healthcare (Plotzky et al., 2021; Mäkinen et al., 2022), a significant knowledge gap remains regarding the application of fully immersive head-mounted device (HMD) VR technology in dementia care training among formal caregivers. Addressing this gap is essential to leveraging VR’s potential for enhancing caregiving practices and outcomes in LTC settings.
With the ongoing challenges in delivering competent and quality care for PLWD in the LTC settings, where the environment can be stressful and unfamiliar for PLWD, the potential of immersive HMD VR technology in staff training remains largely unexplored. Understanding the influential factors (barriers and facilitators) for implementing this innovative training method is crucial to support staff with the knowledge and skills to do their work. This scoping review aims to bridge the knowledge gap by investigating the facilitators, barriers and impacts of fully immersive VR training programs for frontline formal caregivers in LTC settings. The study is particularly important for addressing staff retention in LTC, as improving training programs can enhance staff competence, confidence, and job satisfaction, which are critical factors in reducing turnover. This review is guided by the following research questions:
1. What are the barriers and facilitators to introducing a VR training programme for dementia care among formal caregivers in LTC settings?
2. What impacts does a VR training programme for dementia care have on the staff competence and wellbeing of residents in LTC settings?
This scoping review was conducted using the JBI methodology (Peters et al., 2024), selected for its comprehensive framework that systematically incorporates diverse study designs and emphasizes practical evidence for healthcare practice and policy development. This methodology ensures a thorough and transparent synthesis of the available literature. The protocol for this study was published in May 2024 (Hung et al., 2024). Additionally, the review adheres to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews) checklist (Supplementary Table S1), ensuring methodological rigor and clarity in reporting (Tricco et al., 2018).
This scoping review included studies that focus on VR training programs for dementia care aimed at formal caregivers (paid employees) in LTC homes. Formal caregivers are defined as trained professionals who deliver medical and health services, including nurses, physicians, therapists, and other frontline healthcare workers employed in LTC homes. We excluded studies related to informal caregivers, such as family and friends, or medical and nursing students without professional experience.
This scoping review included studies utilizing fully immersive VR technology for dementia care training programs, specifically those employing HMD systems. Research indicates that immersive virtual environments, particularly VR HMD environments, enhance avatar perception and visual realism (Lee and Ji, 2024), positively impacting user experience (Gonçalves et al., 2023). Studies focusing on non-immersive or semi-immersive VR technology, such as 2D simulations or virtual environment-based programs, were excluded. The selected studies had to address barriers and facilitators to implementing VR training programs or their impacts on formal caregivers’ competencies and residents’ wellbeing.
Due to a high portion of residents in LTC homes (69%) being people living with dementia and the significant impact this has on frontline formal caregivers, we exclusively focus on studies conducted in LTC settings (Canadian Institute for Health Information, 2024). We adopted the Canadian Institute for Health Information’s definition of LTC homes: “also called nursing homes, continuing care facilities, and residential care homes, which provide a wide range of health and personal care services for Canadians with medical and physical needs who require access to 24-h nursing care, personal care, and other therapeutic and support services” (Canadian Institute for Health Information, 2021). Other care contexts, such as assisted living facilities, community settings, and private homes, were excluded from this review to maintain a focused scope.
This scoping review includes quantitative, qualitative, and mixed-method research designs. It considers experimental and quasi-experimental study designs, along with analytical observational studies such as prospective and retrospective cohort studies, case-control studies, and cross-sectional studies. Descriptive observational study designs, including case series, individual case reports, and descriptive cross-sectional studies, are also included. Additionally, qualitative study designs such as phenomenology, grounded theory, ethnography, qualitative description, action research, and feminist research are considered. Systematic reviews, as well as test and opinion papers, are also included.
The research team consists of student trainees, interdisciplinary academic scholars from the fields of nursing and computer science, and patient and family partners. Our members come from three different countries: Taiwan, Singapore, and Canada. This diverse composition has enriched our understanding of the topic and highlighted the importance of incorporating perspectives from lived experiences. All team members have actively participated in discussions and analyses of data from the selected studies during research meetings and the writing of the paper.
We employed a three-step search strategy following the JBI methodology (Peters et al., 2024) to identify both published and unpublished studies. Initially, we conducted a preliminary search in the CINAHL and MEDLINE databases to locate relevant articles. This was followed by analyzing the text words in the titles and abstracts, as well as the index terms of the retrieved papers, with input from a librarian. These terms were then used to create a comprehensive search strategy tailored to English-based search engines, incorporating logical expressions and database-specific search tips such as auto-stemming, wildcards, truncations, and quotations. The search terms used included: Title/Abstract/Keywords/Subject Headings ((virtual reality OR VR) AND (Alzheimer OR cognitive impairment OR dementia OR memory loss) AND (care aid OR caregivers OR healthcare worker OR nurses) AND (course OR curriculum OR education OR program OR teach OR train)). In the second step, we searched the following electronic databases using the identified keywords and index terms: CINAHL (via EBSCOhost, 1982 to 31/December/2023); MEDLINE (via Ovid, 1946 to 31/December/2023); Scopus (1788–31/December/2023); EMBASE (via Ovid, 1974 to 31/December/2023); Conference Proceedings Citation Index–Science (via Web of Science, 1990 to 31/December/2023); Conference Proceedings Citation Index–Social Science & Humanities (via Web of Science, 1990 to 31/December/2023); Emerging Sources Citation Index (via Web of Science, 2015 to 31/December/2023); ProQuest Dissertations and Theses Global (via ProQuest, 1861 to 31/December/2023). The search strategies applied keywords and subject headings to harvest relevant literature on VR program development for caregivers of PLWD. The following websites were searched: AgeWell (https://agewell-nce.ca/31/December/2023). We also contacted original authors for further literature retrieval, obtaining two articles, and screened the reference lists of all included articles for additional studies. Detailed electronic search strategies are provided in Supplementary Table S2.
Collaboration with a medical librarian helped refine the search strategy to ensure comprehensive coverage of relevant articles. As a scoping review, we aimed to include all potential articles. The inclusion criteria were broad, encompassing studies in any language with English abstracts, with a cut-off date of December 2023. However, only full-text articles in English and Chinese were included for full-text screening due to our team’s language proficiency, ensuring accurate interpretation and analysis. Unpublished studies and conference abstracts were used to establish contact with corresponding authors to potentially access full-text studies.
The identified articles were collated and uploaded into Covidence, a bibliographic reference management tool, to ensure systematic management of references and articles. Duplicate articles were automatically removed by Covidence and manually at a later stage. The review process consisted of two steps. First, two researchers independently reviewed titles and abstracts for relevance, with a third reviewer resolving any conflicts. Second, relevant articles underwent a full-text review against the following inclusion criteria: (a) formal caregivers in LTC facilities, (b) fully immersive VR (with at least an HMD headset), (c) VR training on dementia care, and (d) content related to barriers, facilitators, or impacts of VR program implementation. We included studies published in English and Chinese, with no time limit on the publication date. Various study designs were considered, including qualitative, quantitative, mixed designs, and systematic reviews. Articles were excluded if they: (a) addressed only informal caregivers (families) or medical and nursing students, (b) conducted the VR program in settings other than LTC facilities, (c) did not mention VR (e.g., video games, exergames, or other augmented reality technologies), (d) included only non-immersive or semi-immersive VR (without HMD equipment), (e) did not relate to dementia care, or (f) lacked content on barriers, facilitators, or impacts of VR program implementation.
The initial database search yielded 469 publications. After removing duplicates, 343 articles were screened by title and abstract, resulting in 48 potentially relevant articles. During the full-text screening, 39 articles were excluded for the following reasons: wrong study design (scoping review protocol; n = 1), wrong context (hospital; n = 1), wrong intervention (non-immersive or semi-immersive VR; n = 9), wrong participants (family caregivers or students; n = 24), and poster presentations without full text (n = 4). After discussing the eligibility of the articles with participants and family partners, nine publications were included in the final review. See Figure 1 for the PRISMA flow diagram detailing the review process (Page et al., 2021).
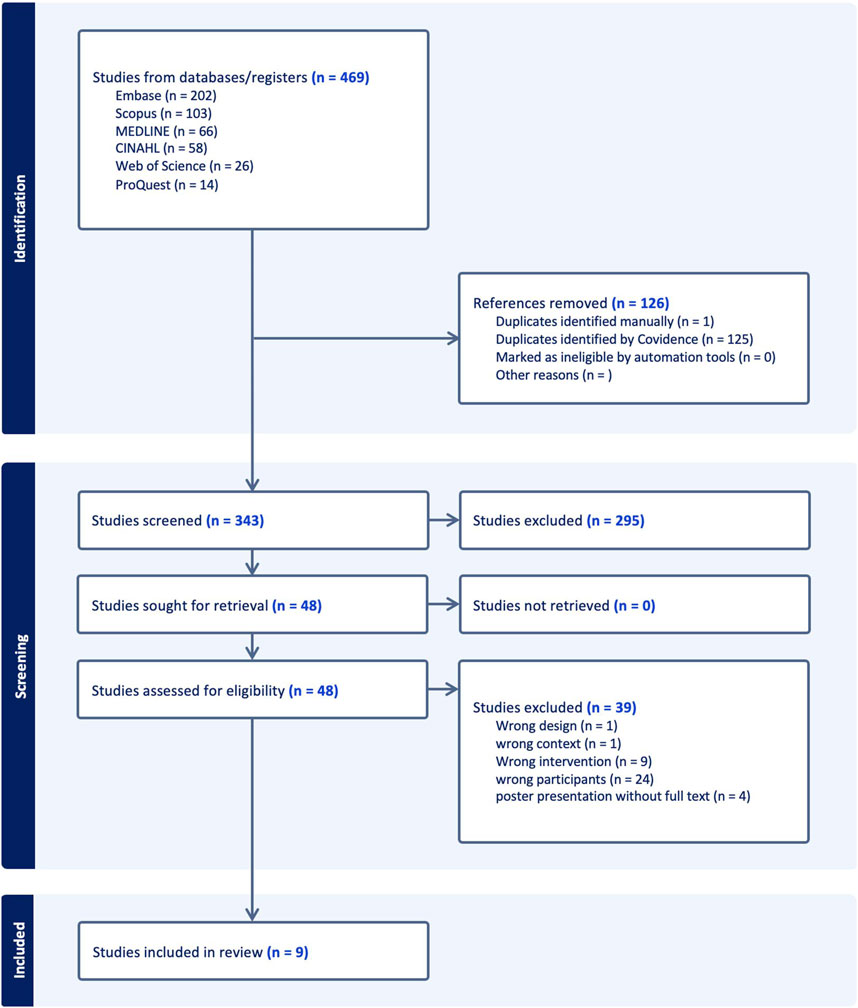
Figure 1. PRISMA flow diagram.
We compiled the chosen articles into a spreadsheet, which provides a summary of the articles by author, publication year, country, research design, participants, sample size, interventions, VR contents, barriers, facilitators, and impacts.
We employed a narrative synthesis method to accommodate the diverse designs and reporting styles of the studies. Data synthesis through narrative summary linked the findings to the study objectives and research questions.
Barriers and facilitators were evaluated using the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., 2022), which examines factors influencing implementation success across five domains: innovation (VR training program), inner setting (LTC settings), outer setting (society and policy), individuals involved (formal caregivers), and the process of implementation (education and training). This framework aids in understanding the complexities of adopting and integrating interventions within organizations.
The impact on staff competencies and resident wellbeing was assessed using the Kirkpatrick Four-Level Training Evaluation Model (Barros Una et al., 2023), a widely used framework for evaluating training program effectiveness. The model encompasses four levels: reaction, learning, behavior, and results, with a specific focus on caregiver competence and resident wellbeing.
Extracted data were assessed and categorized to develop themes. Data extraction was conducted independently by two researchers, followed by collaborative discussions and synthesis involving the entire research group. This approach ensured a rigorous and comprehensive analysis, incorporating multiple perspectives to enhance the validity and reliability of the findings.
This scoping review did not require research ethics approval or consent to participate because the methodology only consisted of data from articles in the public domain.
Table 1 summarizes the characteristics of nine eligible studies. Of these, three were conducted in the UK (Ball et al., 2015; Lee, 2019; Hicks et al., 2023), two in Canada (Holmes et al., 2023; Garcia et al., 2024), two in Taiwan (Sung et al., 2022; Tsai et al., 2023), one in Australia (Stargatt et al., 2021), and one in Korea (Kim, 2021). The study designs included two quantitative studies (RCTs) (Stargatt et al., 2021; Sung et al., 2022), two qualitative studies (Kim, 2021; Hicks et al., 2023), four mixed-methods studies (Ball et al., 2015; Holmes et al., 2023; Tsai et al., 2023; Garcia et al., 2024), and one review (Lee, 2019). A total of 362 formal caregivers participated, with a mean age range of 44.7–65 years and a maximum age of 82. The percentage of female participants ranged from 87.1% to 100%. Three studies did not report participants’ ages (Ball et al., 2015; Hicks et al., 2023; Holmes et al., 2023).
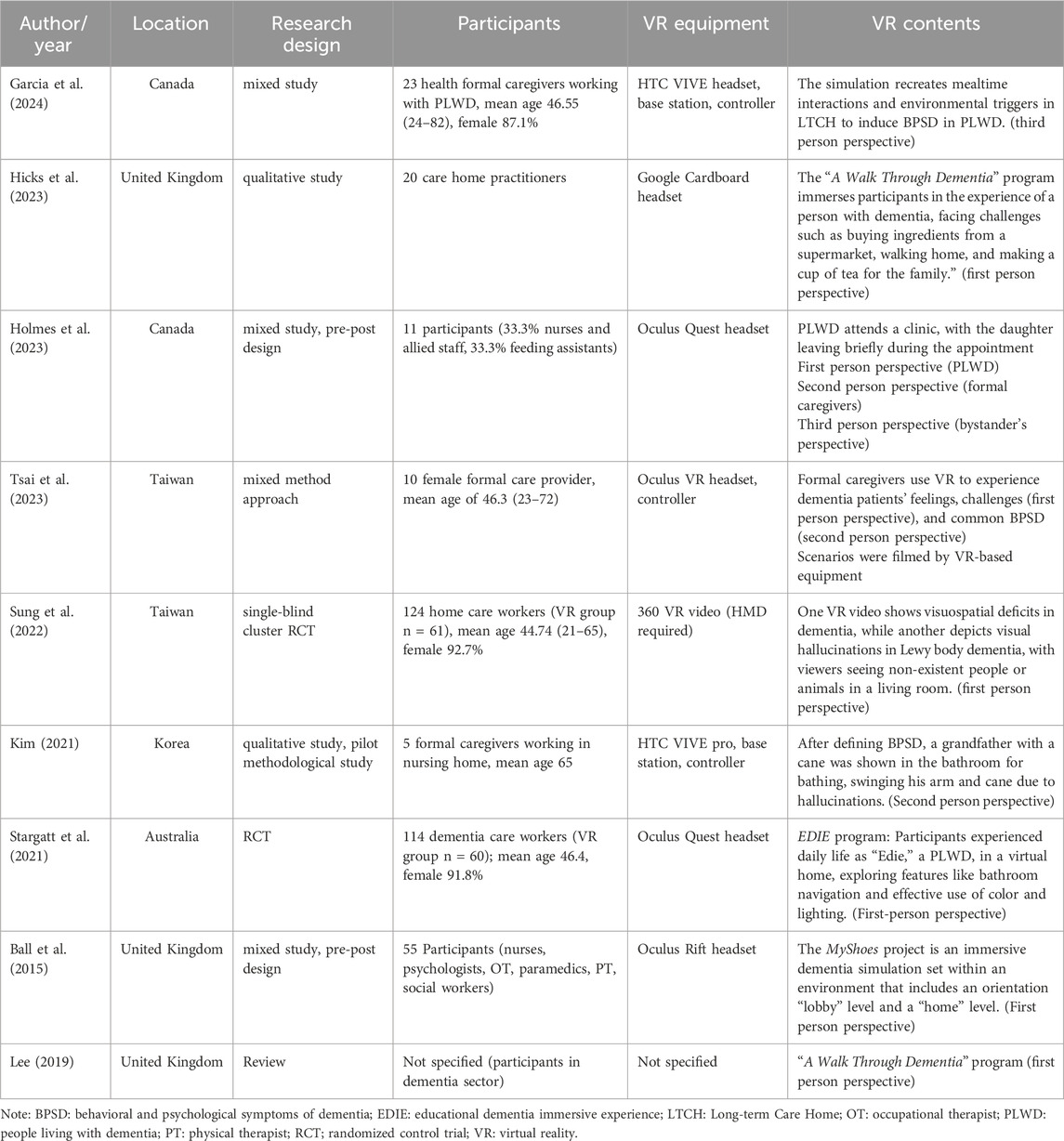
Table 1. Summary of studies on VR training for formal caregivers.
Regarding VR equipment, four studies used Oculus VR headsets (Ball et al., 2015; Stargatt et al., 2021; Holmes et al., 2023; Tsai et al., 2023), two used HTC VIVE (Kim, 2021; Garcia et al., 2024), and one used Google Cardboard (Hicks et al., 2023). One study did not specify the headset used (Sung et al., 2022).
In terms of VR content perspectives, five studies used a first-person perspective (Ball et al., 2015; Lee, 2019; Stargatt et al., 2021; Sung et al., 2022; Hicks et al., 2023), one used a second-person perspective (Kim, 2021), one used a third-person perspective (Garcia et al., 2024), one used both first and second-person perspective (Tsai et al., 2023), and one employed all three perspectives, representing PLWD, formal caregivers, and observers (Holmes et al., 2023). Scenarios consist of mealtime (Garcia et al., 2024), bathing (Kim, 2021), shopping (Lee, 2019; Hicks et al., 2023), walking home (Lee, 2019; Hicks et al., 2023), making tea (Lee, 2019; Hicks et al., 2023), visiting clinic (Holmes et al., 2023), lobby or room navigation (Ball et al., 2015; Stargatt et al., 2021). Two studies focus on visual impairment (Sung et al., 2022) and BPSD (Tsai et al., 2023), with unspecified scenarios.
The CFIR framework contributed to the analysis of barriers and facilitators, as shown in Table 2.
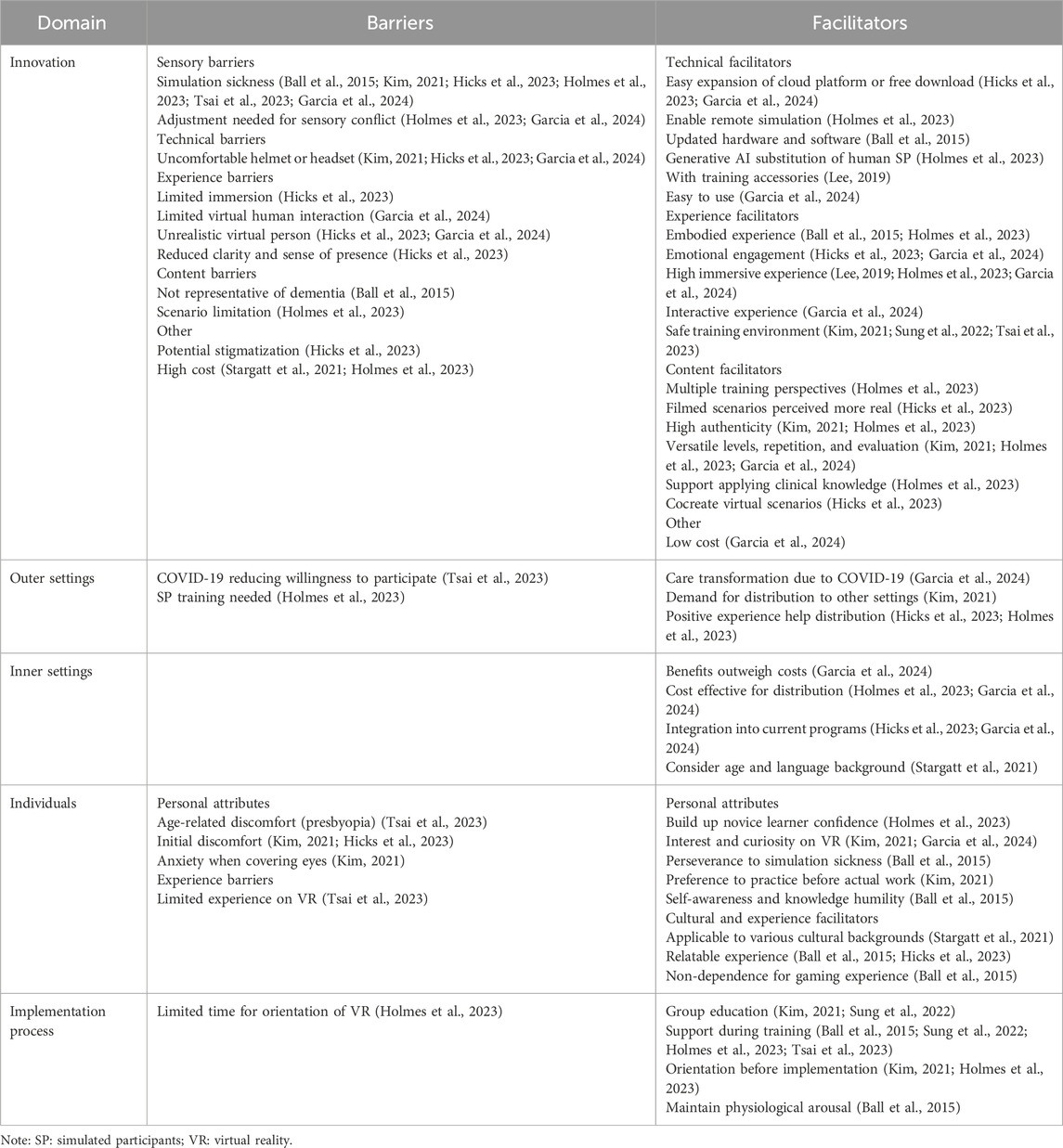
Table 2. Barriers and facilitators of implementation of VR training for formal caregivers.
Most barriers reported were in the innovation domain of the CFIR framework, which can be categorized into sensory, technical, content, experience, and other barriers. Among these, simulation sickness was the most commonly reported barrier (6/9), followed by uncomfortable headsets (3/9). Other issues included limited immersion, interaction, realism, and clarity, as well as content-related concerns such as the lack of dementia representation and insufficient scenario variety. Additionally, high costs and potential stigmatization were noted as barriers.
In the individual domain, various LTC staff participant groups reported challenges, including dizziness due to aging and presbyopia, as well as limited VR experience, which hindered usability (Tsai et al., 2023). Other reported issues included embarrassment and anxiety, particularly for first-time users or those experiencing eye coverage (Kim, 2021).
The outer settings domain presented both challenges and opportunities. While the COVID-19 pandemic reduced willingness to participate in research (Tsai et al., 2023), there is also an increased demand for innovations to improve care (Garcia et al., 2024). Holmes et al. (2023) used simulated participants (SP) in VR training and noted higher costs and increased effort. Stargatt et al. (2021) found VR workshops to be slightly more expensive than in-person workshops. For implementation, Holmes et al. (2023) suggested that more time should be allocated to orientation to help participants learn about the virtual space, headset, and hand controls before entering the VR environment.
Most facilitators reported that they were also in the innovation domain and were categorized into technical, content, experience, and other facilitators. VR and accompanying technologies, such as cloud platforms and free apps, facilitate the expansion and participation in training programs (Hicks et al., 2023; Holmes et al., 2023; Garcia et al., 2024). Updated hardware and software help reduce simulation sickness (Ball et al., 2015), while generative AI can replace SPs and offer more complex behavioral scenarios (Holmes et al., 2023). Combining VR with traditional dementia suits also enhances the empathy experience (Lee, 2019).
High immersion, interactivity, and embodied experiences improve participant engagement (Ball et al., 2015; Lee, 2019; Holmes et al., 2023; Garcia et al., 2024). Audio and visuals, such as narration of the protagonist’s thoughts, rapid heartbeat, and screen blurring, evoke emotional engagement (Hicks et al., 2023; Garcia et al., 2024). VR, combined with group meetings, can create a safer, more comfortable learning environment (Kim, 2021; Sung et al., 2022; Tsai et al., 2023). In terms of content, participants prefer switching between different perspectives (Holmes et al., 2023), with filmed scenarios being perceived as more realistic than digital ones, contributing to higher authenticity (Kim, 2021; Hicks et al., 2023; Holmes et al., 2023). Additionally, participants expressed a need for more versatile scenarios, repetition, and evaluation (Kim, 2021; Holmes et al., 2023; Garcia et al., 2024). Co-creating virtual scenarios with PLWD and ensuring scenarios allow for the application of clinical knowledge are also facilitators (Hicks et al., 2023; Holmes et al., 2023).
In the outer settings domain, Kim and Hicks highlighted the demand for distribution, with positive experiences leading participants to recommend VR training to colleagues. In the individual domain, personal attributes such as interest, curiosity, confidence, perseverance through sickness, preference for practice, and knowledge humility motivate participants to join VR training (Ball et al., 2015; Kim, 2021; Holmes et al., 2023; Garcia et al., 2024). The VR training program also suits individuals from various cultural backgrounds and those without gaming experience, while it resonates with those who have experience working with PLWD (Ball et al., 2015; Stargatt et al., 2021). In the inner settings domain, cost-effectiveness and integration into current programs can encourage institutional acceptance of VR training (Hicks et al., 2023; Holmes et al., 2023; Garcia et al., 2024). For the implementation domain, support from facilitators and peers, orientation ahead of time, and maintaining physiological arousal can facilitate the success of VR training programs (Ball et al., 2015; Kim, 2021; Sung et al., 2022; Holmes et al., 2023; Tsai et al., 2023).
The Kirkpatrick model was used to evaluate the effectiveness of this VR training program for formal caregivers, as shown in Table 3. The VR training program demonstrated the potential to influence caregiving at multiple levels, from initial reactions and learning to behavioral changes and broader systemic impacts.

Table 3. Impacts of implementation of VR training for formal caregivers.
VR presentation method provides immersive experiences and simulates real-life scenes (Ball et al., 2015; Hicks et al., 2023; Tsai et al., 2023; Garcia et al., 2024). Most participants saw the VR experience as a fantastic tool and were interested in such new teaching methods (Kim, 2021). However, participants mentioned that the sound in the lesson plan was blurred, and their eyesight deteriorated, making them feel lonely, helpless, and afraid at the same time during the process (Hicks et al., 2023). After the VR experience, most participants expressed that the frustration they felt during the experience would make them more empathetic and better able to understand the situations that dementia patients encounter in their daily lives (Ball et al., 2015). Such learning experiences provide participants with ‘next-level’ dementia-awareness training through touch and vision (Hicks et al., 2023).
Overall, the literature demonstrates that experiential learning in VR is highly effective at increasing knowledge. VR training helps formal caregivers understand the dementia care environment and BPSD, bridge gaps between theory and practice and connect knowledge with personal experience (Ball et al., 2015; Stargatt et al., 2021; Sung et al., 2022; Hicks et al., 2023; Holmes et al., 2023; Tsai et al., 2023; Garcia et al., 2024). The VR experience integrates theoretical knowledge related to dementia, as highlighted by two articles using the Dementia Knowledge Assessment Scale (DKAS) to measure understanding (Stargatt et al., 2021; Sung et al., 2022). The DKAS consists of 25 questions across four aspects, with a total score of 50 points; higher scores indicate greater dementia knowledge (Annear et al., 2017). One study reported that the DKAS scores of formal caregivers increased from 30.34 to 37.54 1 month after completing 3 months of VR training. In contrast, another study did not observe a significant increase in DKAS scores but reported improvements in Understanding of Dementia Care Environments (UDCE) scores, particularly among non-English-speaking and younger participants (younger than median age 46). Enhancing basic dementia theories through VR has numerous clinical care benefits, such as reducing falls and chest infections (Slater et al., 2019). Kim (2021) emphasized that beyond basic clinical knowledge, it is crucial to understand the formal caregivers of people with dementia and how patients manage their lives. The study also addressed issues like dementia behavior, communication between patients and carers, and maintaining patience (Kim, 2021).
VR training programs can help formal caregivers improve communication skills, identify BPSD triggers, suggest solutions, and deliver safe, compassionate, and responsive care (Holmes et al., 2023; Tsai et al., 2023; Garcia et al., 2024). Compared to traditional learning, VR lesson plans offer real-time interactivity and the ability to practice complex scenarios. To enhance skills in managing dementia, the literature suggests caregiving skills, interaction with dementia patients, communication skills, and self-training lives for dementia patients (Kim, 2021). All the research primarily assessed the impact, effectiveness, or usability of VR training course immediately after the training, with no studies addressing the long-term retention of dementia care skills, highlighting an important gap for future research.
VR training programs can help build up empathy in formal caregivers in caring for PLWD (Ball et al., 2015; Lee, 2019; Stargatt et al., 2021; Sung et al., 2022; Tsai et al., 2023). In terms of the lesson plan itself, participants noted that the realistic scenarios and repeated practice provided by VR training significantly increased their confidence in caring for patients with dementia (Kim, 2021; Sung et al., 2022; Holmes et al., 2023). They become more patient and caring and regard themselves as a potential environmental trigger to BPSD (Ball et al., 2015; Garcia et al., 2024), with one second-year physiotherapist reflecting, “OK, that was scary. I now know what it must feel like, and I need to be much more patient and understanding. It must be so scary.” They were also impressed by this experience, finding learning from the first-person perspective helpful (Holmes et al., 2023).
Regarding attitudes toward dementia patients, measured by the Dementia Attitudes Scale (DAS), higher scores indicate more positive attitudes toward dementia (O’Connor and McFadden, 2010). Participants showed slightly higher positive scores (87.02 vs 82.93) after the post-test (Stargatt et al., 2021).
After the virtual training intervention, participants demonstrated improved knowledge and confidence regarding the needs of people with dementia. For example, in the study by Garcia et al., one learner reported, “Mr. Smith seemed to be affected by all the simultaneous noises and information that were co-occurring at the scene.” This enabled them to modify their interactions and interpersonal approaches with PLWD, as well as adopt a more empathetic perspective. They were also able to effectively apply new techniques to responsive behaviors, such as responding more patiently and promptly to patient needs (Holmes et al., 2023; Tsai et al., 2023).
VR training programs benefit PLWD by helping address challenges within LTC facilities and enabling trainees to apply their newfound knowledge in everyday situations. For example, trainees paused and gave more time to individuals struggling with tasks, such as finding their change in a busy supermarket (Hicks et al., 2023; Tsai et al., 2023). Additionally, VR can challenge younger learners to confront and reduce the stigma associated with aging and dementia (Hicks et al., 2023).
This review underscores the increasing adoption of VR-based training for formal caregivers in dementia care. The studies examined span diverse geographical regions, methodologies, and participant demographics, offering a comprehensive understanding of the barriers, facilitators, and impacts associated with implementing immersive VR training programs for formal caregivers. The nine literature reviewed were published from 2015 to 2024. The primary findings of this study indicate that the VR training program offers a positive learning experience, significantly enhances participants’ knowledge, skills, and attitudes toward dementia, fosters empathy by evoking negative emotions, and enables formal caregivers to apply their learning in practice to effectively address patient challenges.
To ensure the successful implementation of VR training for formal caregivers, careful consideration should be given to the main barriers and facilitators within the innovation domain. Key barriers include sensory issues such as simulation sickness, discomfort from headsets, limited immersion, unrealistic virtual interactions, and scenarios not fully representative of dementia care. These challenges can impact user experience and reduce the effectiveness of training. Conversely, facilitators within this domain emphasize the importance of high-quality VR content and advanced technologies. Factors such as improved hardware and software to minimize simulation sickness, the integration of generative AI to create more complex scenarios, and the use of immersive and interactive elements enhance the learning experience. Additionally, co-creating scenarios with formal caregivers and PLWD, and incorporating diverse perspectives and relatable experiences, contribute to higher engagement and relevance. By addressing these barriers and leveraging these facilitators, organizations can enhance the usability, effectiveness, and adoption of VR training programs among formal caregivers.
Simulation has long been a foundational tool in nursing education, effectively training both novice and expert learners in clinical skills, competencies, and professional attitudes. Traditional simulation techniques, such as mannequin-based scenarios or standardized patient interactions, have demonstrated their value in replicating clinical environments and building learner confidence (So et al., 2019). VR takes this a step further by enhancing simulation fidelity, providing immersive and interactive experiences that engage learners on cognitive, emotional, and sensory levels (Tsai et al., 2023). The diverse learning outcomes from VR training programs highlight its potential for addressing varied educational needs. Stargatt’s findings underscore a distinction between the impacts on older and younger participants (Stargatt et al., 2021). Older learners were better able to relate to dementia and enhance their empathy, likely due to personal connections or life experiences that resonated with the scenarios. Younger participants, on the other hand, demonstrated greater gains in acquiring dementia care knowledge and practical skills, benefiting from the interactive and detailed training design. This dual impact highlights VR’s versatility, offering both emotional engagement and technical skill development tailored to learners’ age and experience levels. Moreover, VR training programs show particular value in deepening learners’ understanding of the lived experiences of PLWD. Hicks et al. (2023) noted that even participants who were already knowledgeable about dementia care challenges gained a deeper appreciation for the psychological toll of these barriers through the immersive qualities of VR. Ball et al. (2015) emphasized that VR resonates strongly with those who have prior experience working with PLWD, such as through placements or personal caregiving stories. This connection facilitates a richer and more meaningful learning experience. In summary, while VR initially strengthens empathy through emotional immersion, a more profound empathy can be cultivated as learners advance to mastering dementia care knowledge and skills, suggesting a two-step approach to comprehensive dementia care training.
Scenarios in the reviewed studies include mealtime, bathing, shopping, walking home, making tea, visiting a clinic, and navigating lobbies or rooms (Ball et al., 2015; Lee, 2019; Kim, 2021; Stargatt et al., 2021; Hicks et al., 2023; Holmes et al., 2023; Garcia et al., 2024). VR content can be broadly categorized based on training objectives: first-person perspectives aim to help learners experience the emotions of PLWD and foster empathy (Ball et al., 2015; Lee, 2019; Stargatt et al., 2021; Sung et al., 2022; Hicks et al., 2023), while second- and third-person perspectives focus on training learners to recognize BPSD triggers and practice responses to these situations (Kim, 2021; Holmes et al., 2023; Tsai et al., 2023; Garcia et al., 2024).
Simulation sickness emerged as one of the most significant barriers in implementing VR training, causing notable user discomfort (Ball et al., 2015; Kim, 2021; Hicks et al., 2023; Holmes et al., 2023; Tsai et al., 2023; Garcia et al., 2024). This discomfort, including blurred vision, dizziness, and general physical unease, not only affected participants’ comfort but also hindered their ability to sustain attention and fully engage in VR scenarios. Tsai et al. (2023) highlighted older participants, particularly those with presbyopia or limited VR experience, were more susceptible to such symptoms, underscoring the need for VR training programs tailored to accommodate age-related visual impairments.
While simulation sickness was commonly reported qualitatively in studies, one study quantitatively assessed it using the Simulator Sickness Questionnaire (SSQ) (Garcia et al., 2024). Garcia et al. (2024) found that simulation sickness was mild overall (mean SSQ score: 3.27), explaining why it was generally tolerable in another dementia care VR training study and did not lead to participant dropouts (Ball et al., 2015). Garcia et al. (2024) also analysed the correlation between SSQ and immersive tendencies questionnaire (ITQ), reporting weak correlations between sickness and immersion (r = 0.23) but moderate to strong correlations with immersive tendencies during gameplay (r = 0.64) and emotional arousal (r = 0.77). These findings suggest that simulation sickness in dementia care VR training is often triggered by the negative emotions evoked during virtual interactions, making it distinct from other VR applications.
Several strategies have been proposed to mitigate simulation sickness. Keeping participants seated during sessions (Tsai et al., 2023; Garcia et al., 2024) and upgrading hardware and software—such as maintaining high frame rates, reducing mouse sensitivity, creating world-based interactions, and removing vertical motion—are effective measures (Ball et al., 2015). Conflicting evidence exists regarding VR exposure duration: while Kim (2021) found longer sessions exacerbated sickness, Hicks et al. (2023) noted reduced symptoms among participants with greater exposure to VR over time. Furthermore, Kennedy et al. (2000) identified that exposure duration positively correlated with simulation sickness, whereas repeated exposure reduced overall symptoms. Both Ball et al. (2015) and Holmes et al. (2023) emphasized the role of high-quality VR technology in reducing discomfort, offering hope that advancements in VR equipment could further mitigate these challenges.
To minimize motion sickness and physical strain, VR experiences are suggested to prioritize ergonomic design, such as adjustable focus and interpupillary distance. Gradual acclimatization to VR environments could also help participants adapt and enhance the immersive experience. As VR technology continues to evolve, addressing these barriers will be critical to ensuring widespread adoption and effectiveness of VR training in dementia care.
Immersion, interaction, embodiment, and authenticity are regarded as the core characteristics that enhance the sense of realism in VR, which positively impacts user experience during VR training (Gonçalves et al., 2023). Failure to achieve these elements can act as barriers, while successfully fulfilling them can serve as facilitators. Garcia et al. (2024) reported that participants generally positioned VR between training videos and real-world situations, with VR being perceived as closer to the real world in terms of immersion. Garcia et al. (2024) also noted that some participants found multisensory inputs helped make non-human virtual environments (such as rooms and objects) feel more realistic, although the movements and physical characteristics of virtual people lacked realism. Hicks et al. (2023) highlighted that scenarios perceived as unrealistic detracted from practitioners’ otherwise positive experiences, with two participants even refusing to wear headsets due to their feelings of unreality. Hicks et al. (2023) also found that film-based scenarios were perceived as more realistic and preferred over digital ones. These findings suggest that human elements in VR are more difficult to render realistically than non-human objects or that participants have higher expectations for the realism of virtual humans compared to the virtual environment. This insight points toward a potential direction for the development of VR training content, focusing on improving the realism of virtual humans.
Two studies highlighted the role of interest and curiosity in enhancing VR training programs (Kim, 2021; Garcia et al., 2024). Participants expressed frustration when limited to an observer role, unable to interact with virtual characters (Garcia et al., 2024). They preferred shifting between perspectives—residents, caregivers, and observers—to enhance their learning experience (Holmes et al., 2023). This indicates that VR’s ability to engage curiosity and interest is key to facilitating deeper learning. The increased engagement from VR training can be seen in studies that improved learners’ understanding of dementia care. VR programs can stimulate pre-intervention willingness to learn and boost satisfaction and learning outcomes afterward. Inoue et al. (2024) found that VR programs, particularly those featuring immersive dementia videos, enhanced community members’ understanding of dementia. This highlights how VR not only fosters interest and curiosity but also improves training outcomes, benefiting both caregivers and those they care for.
Cost is a critical factor influencing the adoption of VR training in certain institutions. The high initial investment for VR hardware and ongoing expenses for software updates and maintenance can be prohibitive for many educational institutions (Holmes et al., 2023; Wang et al., 2023). Additionally, Holmes et al. (2023) highlighted that the use of human SPs also incurs significant costs, which could limit the scalability of VR training in nursing practice. However, the effectiveness of SP-based simulations reinforces their central role in healthcare training. Holmes further emphasized the importance of training with human SPs to address some limitations of current VR equipment, such as the inability to simulate transitions between sitting and standing. Garcia et al. (2024) suggested that VR training could serve as a viable alternative to high-cost in-person training with simulated patients, with long-term benefits outweighing the significant upfront costs. Therefore, cost-effectiveness analysis is crucial for institutions to make informed decisions regarding VR adoption.
When evaluating the impact of VR training on dementia care using Kirkpatrick’s Model, it becomes evident that VR training possesses unique characteristics that set it apart from other training methods. Typically, Level 1 of Kirkpatrick’s Model focuses on learner satisfaction, assessing participant reactions such as engagement, enjoyment, and the relevance of the content to their needs (Muirhead et al., 2021). However, in the context of VR training for dementia care, this level extends beyond positive feedback to include negative emotions such as frustration, anxiety, or discomfort. These emotions provide a valuable opportunity for learners to experience the feelings often encountered by PLWD. Ball et al. (2015) noted that when first-person perspectives were applied, learners reported feelings of fear, depression, frustration, and isolation. Similarly, Holmes et al. observed that when all three perspectives—first-person, second-person, and third-person—were utilized, learners experienced frustration and anxiety. These emotions mirror the challenges faced by both PLWD and their caregivers, providing critical insights into the emotional dynamics of dementia care. Furthermore, the ability of VR to evoke such emotions highlights its role in preparing learners for the psychological complexities of real-world caregiving. It also underscores the importance of providing a safe and controlled learning environment, which VR can uniquely deliver. Beyond replicating realistic scenarios, VR training has the potential to escalate the complexity of scenarios, exposing learners to increasingly tricky and nuanced situations (Ball et al., 2015; Garcia et al., 2024). This feature in VR enables presenting a wide spectrum of challenges in dementia care, preparing frontline staff with different levels of experience to manage these challenges. By immersing learners in emotionally charged and high-stakes scenarios within a safe environment, VR equips them with the emotional resilience and problem-solving skills necessary for effective caregiving, reinforcing its critical role in enhancing dementia care training. However, the lack of research on the long-term retention of dementia care skills following VR training suggests a critical gap in understanding the sustained impact of such interventions. Future studies should explore how well caregivers retain and apply these skills over time, as well as identify factors that support long-term competency. Addressing this gap could enhance training programs by incorporating reinforcement strategies to ensure lasting benefits in dementia care.
For VR dementia care education to achieve equity and robust impact across diverse care settings, including rural areas, it must be accessible, inclusive, and adaptable. This involves incorporating culturally relevant content, multiple language options, and ensuring compatibility with varying levels of digital infrastructure to bridge disparities in training access. In rural settings, where access to specialized dementia education may be limited, VR can serve as a scalable solution, providing high-quality training without the need for frequent travel. Additionally, cost-effective implementation strategies are needed to integrate VR into different care environments, from home care to long-term care facilities. By prioritizing accessibility and sustainability, VR training can provide continuous skill reinforcement, leading to lasting improvements in dementia care practices and better outcomes for individuals living with dementia.
This scoping review made threefold key contributions to current literature: (1) it provides a comprehensive overview of the current status and potential impacts of VR training for frontline formal caregivers on dementia care in LTC settings; (2) it advanced knowledge in barriers and facilitators to implementing VR training for frontline formal caregivers; and (3) it offers insights into future research and practice in VR training for staff for a better dementia care in the focused setting.
Our study ensured scientific rigor by adhering to the JBI guidelines. We also included studies with various research design (e.g., qualitative, quantitative, mix-methods), different types of studies (e.g., published and unpublished articles; conference proceedings) and two languages (English and Chinese). We encompassed articles published within a wide range of time. The credibility of our review is further enhanced by involving an interdisciplinary team of members from diverse countries and cultural backgrounds, ensuring relevance and inclusivity.
One limitation of this review is the exclusion of studies published in languages other than English and Chinese, which may result in the omission of valuable research from other linguistic and cultural contexts and introduce potential language bias. Further, our study result is limited by databases we searched and is potentially biased by the biases embedded in the original articles. For example, some authors may be more inclined to report facilitators than barriers in implementing VR training programs to staff.
Future research and nursing practice are recommended to leverage barriers and facilitators reported in this scoping review to explore the acceptance and effectiveness of future VR training programs in LTC settings, especially at the systemic level (health authority level; provincial and federal government level).
Future research should focus on addressing key barriers within the innovation domain, particularly sensory and technical challenges, such as simulation sickness, headset discomfort, and limited virtual interactions. Studies should investigate optimal hardware and software configurations, including frame rate adjustments and interaction design, to reduce simulation sickness and enhance immersion. Additionally, research can explore the integration of generative AI into VR program development to create authentic and dynamic scenarios that address the diverse needs of formal caregivers.
Content development is another critical area for research. Creating scenarios that are representative of dementia care and allow for versatile levels, repetition, and evaluation can improve the applicability of VR training. Co-creation with caregivers and PLWD should be prioritized to ensure relevance and authenticity. Research should also examine the cost-effectiveness of VR programs, particularly for widespread adoption and integration into existing training curricula.
Researchers are also recommended to investigate novel approaches to assess the long-term effect of VR training programs for staff in their dementia care delivery. For example, researchers can focus on behavioral changes in caregiver-patient interactions reflected by adopting measurements (e.g., quality of care provided by staff to residents). Researchers can also evaluate broader outcomes such as stigma reduction and patient problem-solving.
Lastly, it is essential for researchers to explore VR training programs that considered cultural and demographic adaptability for staff, residents and LTC homes. Future studies can explore VR training programs tailored to staff from various cultural and professional backgrounds, as well as individual preferences, while minimizing barriers such as age-related discomfort or anxiety to help improve accessibility and inclusivity.
In practice, nursing educators should focus on enhancing the usability and accessibility of VR training programs. Addressing barriers like simulation sickness and discomfort from headsets can be achieved through proper orientation, ergonomic improvements, and gradual acclimatization. Providing group education sessions with adequate facilitator support can ensure a safer and more engaging learning environment. Similarly, dementia education programs for future staff educators and trainers are suggested to centre on factors that enable or hinder frontline staff in learning dementia care delivery through VR within local contexts. VR training should aim to improve caregiver’s knowledge of dementia care environment, BPSD, and communication skills while fostering empathy, confidence, and patience. The training content should prioritize clinical relevance by incorporating scenarios that help formal caregivers recognize and respond to BPSD. These scenarios should also allow learners to apply theoretical knowledge to practice, fostering skills in empathy, communication, and problem-solving. Encouraging feedback from participants can guide scenario updates and improve training outcomes.
VR training programs should be integrated into existing educational frameworks with a focus on cost-effectiveness and scalability. Leveraging cloud platforms, free downloadable applications, and remote simulation can expand access. Emphasizing the positive learning experiences and practical benefits of VR can motivate adoption among formal caregivers and institutions, ultimately transforming dementia care practices.
Finally, training can drive meaningful changes in care provider interactions with PLWD, enabling them to provide more responsive, patient-centered care. By addressing stigma and equipping formal caregivers with problem-solving skills, VR training can have a lasting impact both inside and outside the workplace.
In conclusion, this scoping review provides a comprehensive overview of the emerging literature on VR training for supporting dementia care frontline formal caregivers. The results indicate that barriers such as simulation sickness, uncomfortable headsets, and limited immersive experiences can hinder the effectiveness of VR programs, while facilitators like technical advantages, immersive and interactive experiences, and proper orientation and support enhance their impact. VR training can positively affect caregiving at multiple levels, including initial reactions, learning (knowledge, skills, and attitudes), behavioral changes, and broader systemic outcomes. Overall, VR has the potential to revolutionize healthcare education and training, particularly in the field of dementia care. By providing a safe and effective learning environment and equipping healthcare professionals with knowledge, practical skills and empathy, VR can improve the quality of care for individuals with dementia and enhance the overall resident wellbeing.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
LH: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing–review and editing. CM: Formal Analysis, Writing–review and editing. CH: Formal Analysis, Writing–original draft. JW: Formal Analysis, Writing–original draft. KW: Formal Analysis, Writing–original draft. KC: Formal Analysis, Writing–original draft. YC: Formal Analysis, Writing–original draft. AH: Formal Analysis, Writing–original draft. KY: Formal Analysis, Writing–original draft. LR: Formal Analysis, Writing–original draft. YZ: Formal Analysis, Methodology, Project administration, Writing–original draft.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was funded by the Canada Research Chair in Senior Care, grant number GR021222.
We acknowledge the invaluable support from UBC librarian Katherine Miller for guiding and supervising the entire search process. We extend our gratitude to Mona Upreti for her valuable contributions to the literature screening process. We also extend our gratitude to Professor Linda Garcia from University of Ottawa and professor Jordan Holmes from the Michener Institute of Education at UHN, University of Toronto, for kindly providing us pre-publication copies and access links of identified papers in response to our email requests. Their outstanding research contributions have significantly enhanced the validity of this scoping review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2025.1552370/full#supplementary-material
Adefila, A., Graham, S., Clouder, L., Bluteau, P., and Ball, S. (2016). myShoes – the future of experiential dementia training? J. Ment. Health Train. Educ. Pract. 11, 91–101. doi:10.1108/JMHTEP-10-2015-0048
Annear, M. J., Toye, C., Elliott, K.-E. J., McInerney, F., Eccleston, C., and Robinson, A. (2017). Dementia knowledge assessment scale (DKAS): confirmatory factor analysis and comparative subscale scores among an international cohort. BMC Geriatr. 17, 168. doi:10.1186/s12877-017-0552-y
Ball, S., Bluteau, P., Clouder, L. C., Adefila, A., and Graham, S. (2015). MyShoes: an immersive simulation of dementia, in International conference on e-learning, Academic Conferences International Limited, 16. Available online at: https://books.google.ca/books?hl=en&lr=&id=ZfNrCwAAQBAJ&oi=fnd&pg=PA16&dq=MyShoes:+an+immersive+simulation+of+dementia&ots=DIDro8S7f8&sig=zK9CKTIBRZMDIfGwA_SAj_K3kQ4#v=onepage&q=MyShoes%3A%20an%20immersive%20simulation%20of%20dementia&f=false (Accessed December 11, 2024).
Barros Una, L., Brangman, S., Indelicato, A., Krueger, A., Ludwig, A., Slutzky, A. R., et al. (2023). Using second life to teach health professions students about Alzheimer’s Disease: a comprehensive review. Gerontol. Geriatr. Educ. 44, 243–253. doi:10.1080/02701960.2021.2022660
Bauce, K., Kaylor, M. B., Staysniak, G., and Etcher, L. (2023). Use of theory to guide integration of virtual reality technology in nursing education: a scoping study. J. Prof. Nurs. 44, 1–7. doi:10.1016/j.profnurs.2022.10.003
Brown, K. M., Swoboda, S. M., Gilbert, G. E., Horvath, C., and Sullivan, N. (2023). Curricular integration of virtual reality in nursing education. J. Nurs. Educ. 62, 364–373. doi:10.3928/01484834-20230110-01
Canadian Institute for Health Information (2021). Long-term care homes in Canada: how many and who owns them? Available online at: https://www.cihi.ca/en/long-term-care-homes-in-canada-how-many-and-who-owns-them (Accessed December 11, 2024).
Canadian Institute for Health Information (2024). Dementia in long-term care. Available online at: https://www.cihi.ca/en/dementia-in-canada/dementia-care-across-the-health-system/dementia-in-long-term-care (Accessed December 11, 2024).
Cohen-Mansfield, J., Dakheel-Ali, M., Marx, M. S., Thein, K., and Regier, N. G. (2015). Which unmet needs contribute to behavior problems in persons with advanced dementia? Psychiatry Res. 228, 59–64. doi:10.1016/j.psychres.2015.03.043
Damschroder, L. J., Reardon, C. M., Widerquist, M. A. O., and Lowery, J. (2022). The updated Consolidated Framework for Implementation Research based on user feedback. Implement. Sci. 17, 75. doi:10.1186/s13012-022-01245-0
Falzarano, F., Cimarolli, V. R., Minahan, J., and Horowitz, A. (2022). Long-distance caregivers: what are their experiences with formal care providers? Clin. Gerontol. 45, 1273–1284. doi:10.1080/07317115.2020.1783043
Garcia, L., Robitaille, A., Bouchard, S., Rivard, M.-C., and McCleary, L. (2024). The usability of virtual reality to train individuals in responding to behaviors related to dementia. Front. Dementia 2 2, 1237127. doi:10.3389/frdem.2023.1237127
Gonçalves, G., Coelho, H., Monteiro, P., Melo, M., and Bessa, M. (2023). Systematic review of comparative studies of the impact of realism in immersive virtual experiences. ACM Comput. Surv. 55, 1–36. doi:10.1145/3533377
Hicks, B., Konovalova, I., Myers, K., Falconer, L., and Board, M. (2023). Taking ‘A walk through dementia’: exploring care home practitioners’ experiences of using a virtual reality tool to support dementia awareness. Ageing Soc. 43, 1042–1067. doi:10.1017/S0144686X21000994
Hirt, J., and Beer, T. (2020). Use and impact of virtual reality simulation in dementia care education: a scoping review. Nurse Educ. Today 84, 104207. doi:10.1016/j.nedt.2019.104207
Holmes, J., Sokoloff, L., McNaughton, N., Gardner, S., Truong, L., Nemethy, K., et al. (2023). VR-based simulation training for de-escalation of responsive behaviours in persons with dementia: efficacy and feasibility. Int. J. Healthc. Simul. doi:10.54531/bfqc7623
Hung, L., Zhao, Y., Lam, M., Ren, H., and Wong, K. L. Y. (2024). Facilitators, barriers and impacts to implementing dementia care training for staff in long-term care settings by using fully immersive virtual reality: a scoping review protocol. BMJ Open 14, e083724. doi:10.1136/bmjopen-2023-083724
Inoue, K., Iizuka, H., Kamio, H., Yao, D. P., Yatsu, C., Sasaki, C., et al. (2024). A pilot study on the use of virtual reality to educate community members about dementia. Phys. Occup. Ther. Geriatr. 42, 170–185. doi:10.1080/02703181.2023.2291361
Kao, Y.-H., Hsu, C.-C., and Yang, Y.-H. (2022). A nationwide survey of dementia prevalence in long-term care facilities in taiwan. J. Clin. Med. 11, 1554. doi:10.3390/jcm11061554
Kennedy, R. S., Stanney, K. M., and Dunlap, W. P. (2000). Duration and exposure to virtual environments: sickness curves during and across sessions. Presence Teleoperators Virtual Environ. 9, 463–472. doi:10.1162/105474600566952
Kim, D. (2021). Development and effect of virtual reality practice program for improving practical competency of caregivers specializing in dementia. Healthcare 9, 1390. doi:10.3390/healthcare9101390
Lee, S. (2019). A showcase of medical, therapeutic and pastime uses of virtual reality (VR) and how (VR) is impacting the dementia sector. Adv. Exp. Med. Biol. 1156, 135–141. doi:10.1007/978-3-030-19385-0_10
Lee, Y. J., and Ji, Y. G. (2024). Effects of visual realism on avatar perception in immersive and non-immersive virtual environments. Int. J. Hum. Comput. Interact., 1–14. doi:10.1080/10447318.2024.2351713
Mäkinen, H., Haavisto, E., Havola, S., and Koivisto, J.-M. (2022). User experiences of virtual reality technologies for healthcare in learning: an integrative review. Behav. and Inf. Technol. 41, 1–17. doi:10.1080/0144929X.2020.1788162
Muirhead, K., Macaden, L., Smyth, K., Chandler, C., Clarke, C., Polson, R., et al. (2021). Establishing the effectiveness of technology-enabled dementia education for health and social care practitioners: a systematic review. Syst. Rev. 10, 252. doi:10.1186/s13643-021-01781-8
O’Connor, M. L., and McFadden, S. H. (2010). Development and psychometric validation of the dementia attitudes scale. Int. J. Alzheimers Dis. 2010, 1–10. doi:10.4061/2010/454218
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ n71, n71. doi:10.1136/bmj.n71
Peters, M. D., Godfrey, C., McInerney, P., Munn, Z., Tricco, A. C., and Khalil, H. (2024). “Scoping reviews,”. Adelaide, SA: JBI Manual for Evidence Synthesis. (JBI). doi:10.46658/JBIMES-24-09
Plotzky, C., Lindwedel, U., Sorber, M., Loessl, B., König, P., Kunze, C., et al. (2021). Virtual reality simulations in nurse education: a systematic mapping review. Nurse Educ. Today 101, 104868. doi:10.1016/j.nedt.2021.104868
Shrestha, S., Alharbi, R. J. M., While, C., Ellis, J., Rahman, M. A., and Wells, Y. (2021). Self-efficacy of direct care workers providing care to older people in residential aged care settings: a scoping review protocol. Syst. Rev. 10, 105. doi:10.1186/s13643-021-01655-z
Slater, P., Hasson, F., Gillen, P., Gallen, A., and Parlour, R. (2019). Virtual simulation training: imaged experience of dementia. Int. J. Older People Nurs. 14, e12243. doi:10.1111/opn.12243
So, H. Y., Chen, P. P., Wong, G. K. C., and Chan, T. T. N. (2019). Simulation in medical education. J. R. Coll. Physicians Edinb. 49, 52–57. doi:10.4997/jrcpe.2019.112
Stargatt, J., Bhar, S., Petrovich, T., Bhowmik, J., Sykes, D., and Burns, K. (2021). The effects of virtual reality-based education on empathy and understanding of the physical environment for dementia care workers in Australia: a controlled study. J. Alzheimer’s Dis. 84, 1247–1257. doi:10.3233/JAD-210723
Sung, H., Su, H., Lee, W., Yamakawa, M., and Wang, H. (2022). Effects of a dementia virtual reality-based training with peer support for home care workers: a cluster randomized controlled trial. Int. J. Geriatr. Psychiatry 37. doi:10.1002/gps.5799
Tay, J. L., Xie, H., and Sim, K. (2023). Effectiveness of augmented and virtual reality-based interventions in improving knowledge, attitudes, empathy and stigma regarding people with mental illnesses—a scoping review. J. Pers. Med. 13, 112. doi:10.3390/jpm13010112
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern Med. 169, 467–473. doi:10.7326/M18-0850
Tsai, C.-M., Hsu, T.-C., and Hsieh, C.-J. (2023). A virtual reality intervention to improve formal caregivers’ understanding of community-dwelling people with dementia: a pilot study. Contemp. Nurse 59, 334–343. doi:10.1080/10376178.2023.2259495
Wang, J., Li, Q., Cui, J., Tu, S., Deng, Z., Yang, R., et al. (2023). Effectiveness of virtual reality on the caregiving competence and empathy of caregivers for elderly with chronic diseases: a systematic review and meta-analysis. J. Nurs. Manag. 2023, 1–15. doi:10.1155/2023/5449955
Woodhead, E. L., Northrop, L., and Edelstein, B. (2016). Stress, social support, and burnout among long-term care nursing staff. J. Appl. Gerontology 35, 84–105. doi:10.1177/0733464814542465
Keywords: virtual reality, formal caregivers, dementia care, caregiver training, barriers and facilitators, impacts
Citation: Hung L, Ma CHK, Huang CY, Wong J, Wong KLY, Chew KH, Chao YC, Hussein A, Yuen K, Ren LH and Zhao Y (2025) Facilitators, barriers, and impacts to implementing dementia care training for staff in long-term care settings by using fully immersive virtual reality: a scoping review. Front. Virtual Real. 6:1552370. doi: 10.3389/frvir.2025.1552370
Received: 27 December 2024; Accepted: 27 February 2025;
Published: 13 March 2025.
Edited by:
Maryalice Jordan-Marsh, University of Southern California, United StatesReviewed by:
Ciro Gaona, Alzheimer’s Foundation of Venezuela, VenezuelaCopyright © 2025 Hung, Ma, Huang, Wong, Wong, Chew, Chao, Hussein, Yuen, Ren and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lillian Hung, bGlsbGlhbi5odW5nQHViYy5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.