 Joakim Ingrell
Joakim Ingrell Caroline Mellgren
Caroline Mellgren
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 03 March 2025
Sec. Virtual Reality and Human Behaviour
Volume 6 - 2025 | https://doi.org/10.3389/frvir.2025.1547752
Simulator sickness (SS) poses significant challenges in the widespread adoption of driving simulators for traffic research, training, and other applications. This study investigates the effects of gender, age, driving environment, and gaming experience on SS in a desktop driving simulator, using a sample of 363 Swedish police trainees. Participants completed the Simulator Sickness Questionnaire (SSQ) after simulator sessions involving either city traffic or country road scenarios. Results revealed that females experienced significantly higher SS emerging as the most influential predictor in a multiple regression model. Age also positively correlated with SS, with older participants reporting more severe symptoms. Rural driving scenarios induced higher SS than city traffic. Although prior gaming experience reduced SS symptoms in univariate analyses, it was not a significant predictor in the regression model. These findings emphasize the need for personalized simulator design and tailored scenario optimization to reduce simulator sickness, promoting an inclusive and accessible educational experience. This aligns with broader goals of equity and excellence in professional training programs. Future research should expand these findings by exploring a broader age range and different simulator types.
Driving simulators are widely used in fields like traffic research, driver training, vehicle design, and entertainment due to their ability to recreate real-world driving scenarios in a controlled environment (Alonso et al., 2023). However, a major drawback is simulator sickness (SS), which could be explained by sensory conflicts between the visual, vestibular, and proprioceptive systems and presents symptoms such as nausea, dizziness, and disorientation, like motion sickness (Kennedy et al., 2010). In driving simulators, users remain physically static while perceiving movement in the virtual environment, causing a sensory mismatch. This issue is often exacerbated by latency between real-world actions and their virtual representation (Stanney et al., 1997). While motion-based simulators, which provide physical movement cues, can help alleviate some conflicts, they do not fully eliminate SS (Bles et al., 1998). SS can hinder performance and reduce user experience, posing challenges to the broader adoption of simulators in areas like police driver training. Another explanation for SS could be found in the postural instability theory (Riccio and Stoffregen, 1991) suggesting that motion sickness (or simulator sickness) arises from instability in the control of the body. The key prediction of this theory is that movement patterns should differ between individuals who experience motion sickness and those who do not, with these differences appearing even before any subjective symptoms arise. This prediction has been supported in different studies (e.g., Stoffregen et al., 2017).
Universities use driving simulators in police training programs for several practical and pedagogical reasons. For example, in a Swedish university, driving simulators are used to train police students in low-speed maneuvering with promising results (Ingrell et al., 2022). Driving simulators offer an environmentally sustainable alternative to traditional in-vehicle training, reducing fuel consumption and emissions. They are resource-efficient and cost-effective, enabling institutions to train many students without the logistical challenges of maintaining a large fleet of vehicles. As universities in Sweden are required to accommodate increasing numbers of police students, simulators provide a scalable solution for offering critical skills training. Moreover, driving simulators allow for repetitive practice in controlled and customizable scenarios, ensuring that students can master complex driving situations safely. This is particularly important for police training, where officers must develop quick decision-making skills in high-stakes environments.
Understanding and mitigating simulator sickness is crucial to maximizing the effectiveness of this technology. If not addressed, simulator sickness can limit participation and learning, creating barriers for some students. Studies frequently report participant dropout due to the severity of SS symptoms in virtual environments (Balk et al., 2013; Brooks et al., 2010). However, research indicates that familiarization or adaptation can reduce SS. Hoffmann et al. (2003) showed that adaptation to simulators can diminish SS, enhancing training outcomes and reducing dropout rates.
The increasing use of driving simulators, especially in fields like police driver training, highlights the need to understand how simulator design and adaptation strategies can reduce SS. The severity of SS is influenced by factors like gender, age, type of driving environment, gaming experience, and different types of simulators (Kennedy et al., 2010). Despite these insights, gaps remain in understanding how these factors interact and how SS can be mitigated across different user groups. This study aims to explore these factors when driving a desktop driving simulator. By studying prevalence and causes of SS work can be done towards ensuring that driving simulator training is accessible to all students, fostering an inclusive educational environment in higher education. This aligns with broader goals of equity and excellence in professional training programs.
Research consistently shows that females are more prone to SS, with higher levels of nausea, dizziness, and discomfort in driving simulators (Almallah et al., 2021; Garcia et al., 2010; Matas et al., 2015; Mourant and Thattacherry, 2000). Chaumillon et al. (2017) and Stanney et al. (2020) linked this susceptibility to vestibular and hormonal differences, suggesting females are disproportionately affected by visual-vestibular conflicts in VR. Pohlmann et al. (2021) noted that gaming experience may help mitigate these symptoms in women. Physiological factors, including vestibular sensitivity and hormonal fluctuations, contribute to the higher SS prevalence among females, particularly in HMD-based simulations (Stanney et al., 2020). Kennedy et al. (2010) and Rangelova et al. (2020) [17] highlighted women’s heightened sensitivity to sensory conflicts, exacerbating nausea and disorientation. However, some studies, such as Kolasinski and Gilson (1998), argue that SS differences are driven more by individual traits and simulation design than by gender.
Simulator sickness (SS) varies significantly across age groups, with distinct patterns observed among older adults, younger adults, and children. Understanding these differences is essential for designing effective interventions and improving user experiences in simulations. Research consistently shows that older adults are more susceptible to SS than younger individuals (Brooks et al., 2010). This increased vulnerability is due to age-related sensory processing changes, such as diminished vestibular function and slower visual and motor responses (Diels and Howarth, 2013). Keshavarz et al. (2018) found that older adults experienced more severe symptoms during simulated driving tasks, especially under visual-only conditions where recovery times were longer. Additionally, older adults often drop out of studies due to severe symptoms, limiting generalizability and introducing selection bias (Trick and Caird, 2011). In contrast, younger adults generally experience less severe SS, though symptoms can still vary by gender and individual sensitivity. Keshavarz et al. (2018) noted that younger adults reported fewer symptoms of nausea, dizziness, and disorientation, but females within this group were more prone to SS. Prior experience with virtual environments, such as gaming, helps mitigate symptoms, highlighting the role of habituation in reducing SS. However, younger adults without prior exposure may still face challenges, especially in settings with pronounced motion-induced symptoms. Children and adolescents appear to be more sensitive to SS than both younger and older adults. Wang et al. (2023) found that children and adolescents experienced more severe symptoms due to developmental differences in sensory and cognitive processing. However, not all virtual environments provoke the same level of sickness in children. Godfrey et al. (2024) found minimal symptoms of cybersickness in children aged 8 to 12 during VR exergaming, suggesting that engaging and interactive environments may reduce symptoms. Nevertheless, children may need additional support when using complex visual environments (Wang et al., 2023).
Different driving environments influence SS in different ways. Although more predictable, with fewer directional changes and smoother motion, lower traffic density and simpler driving tasks, Mourant and Thattacherry (2000) found that participants driving in highway or rural road environments exhibited more symptoms of simulator sickness compared to those driving in a city environment. This suggests that vehicle velocity may play a role in simulator sickness, as participants drove at speeds of 60 mph in the highway and rural road scenarios but only 25 mph in the city environment. Furthermore, specific driving maneuvers also play a role, with Mourant et al. (2007) noting increased symptoms during curves and turns. Keshavarz and Hecht (2011) also noted that high-speed turns and rapid visual changes create stronger sensory conflicts, leading to more nausea. This is attributed to heightened optic flow—the perceived motion of objects relative to the driver—which causes mismatches between visual and vestibular cues. Urban driving environments are also influencing SS, as they require drivers to navigate dense traffic, frequent stops, and dynamic interactions. Pawar et al. (2023) found that urban driving, especially under time pressure, significantly increases mental workload and SS due to the higher cognitive demands. Regardless of driving environments, the design and realism of the simulation could play a critical role. Almallah et al. (2021) found that a strong sense of presence—when users feel fully immersed in the virtual environment—can help reduce SS by aligning user expectations with visual experience. However, overly complex simulations may worsen SS by overwhelming the senses, while simplified environments can mitigate conflicts but may reduce immersion.
Individuals with gaming experience tend to show lower susceptibility to SS compared to non-gamers, as documented across multiple studies. Gamers generally experience fewer symptoms, such as nausea, dizziness, and disorientation, in virtual environments (Grassini et al., 2021; Himmels et al., 2022; Pohlmann et al., 2021). This reduction in SS symptoms is attributed to their familiarity with virtual environments, which require frequent visual-motor coordination and adaptation to virtual motion. Pohlmann et al. (2021) found that gamers report significantly fewer symptoms of virtual reality sickness, especially in scenarios involving illusory motion, where visual cues suggest movement without physical motion. Gamers’ exposure to such environments allows them to anticipate and process sensory conflicts more effectively, reducing their likelihood of experiencing SS. Similarly, Grassini et al. (2021) observed that gamers reported a stronger sense of presence in virtual reality (VR), which correlates with fewer SS symptoms, suggesting that their familiarity with dynamic environments helps them manage sensory inputs better. In addition to familiarity, enhanced cognitive flexibility and visual-motor coordination are key factors. Himmels et al. (2022) found that gamers performed better in managing optic flow, reducing SS symptoms in a driving simulator. This skill, developed through gaming, helps them handle rapid visual changes and maintain control and orientation in fast-moving simulations, further reducing SS incidence. Frequent gaming exposure allows users to adapt to rapid visual changes and virtual motion, which are common SS triggers. Dennison et al. (2016) and Kennedy et al. (2010) noted that gaming improves visual-motor skills and spatial awareness, helping users navigate virtual environments without experiencing sensory conflicts.
The type of simulator—whether desktop-based or motion-based—significantly influences the likelihood of experiencing SS, with each having distinct effects on sensory conflict and user discomfort. Studies have shown that the degree of sensory immersion and the synchronization between visual and physical cues are key factors affecting the severity of simulator sickness. Desktop-based simulators, which typically involve stationary monitors or VR headsets, are more likely to induce simulator sickness due to the absence of physical motion cues. Dennison and D'Zmura (2017) pointed out that this lack of congruent vestibular input—where the visual system detects motion but the body does not feel it—results in a sensory mismatch that contributes to feelings of nausea and disorientation. The deep immersion provided by VR headsets can further aggravate this issue, as the visual stimuli immerse users without corresponding physical feedback, amplifying the sensory conflict. Weidner et al. (2017) compared different display setups and found that virtual reality (VR) head-mounted displays (HMDs) led to significantly higher levels of simulator sickness than stereoscopic 3D or traditional 2D screens. The heightened sensory immersion of VR HMDs tends to induce sensory conflicts between visual cues and physical sensations, particularly when the visual system perceives motion that the vestibular system does not register. This mismatch between what is seen and what is felt often results in nausea, dizziness, and disorientation. Motion-based simulators are generally more effective at reducing simulator sickness because they provide congruent motion cues, which help synchronize visual and vestibular inputs. Lucas et al. (2020) found that incorporating specific vibration configurations in motion-based simulators could reduce the severity of simulator sickness. These vibrations replicate tactile sensations associated with real-world driving, such as road texture and vehicle movement, helping to create a more cohesive sensory experience. However, Bles et al. (1998) cautioned that the effectiveness of motion-based simulators in mitigating sickness relies on the accuracy and timing of motion cues. Delayed or exaggerated motion cues can exacerbate sensory conflicts, intensifying simulator sickness instead of reducing it. Despite the advantages of motion-based simulators, they are less accessible due to their high cost and technical complexity, limiting their widespread use. Stanney et al. (2020) emphasized the need for cost-effective solutions for desktop-based simulators to minimize simulator sickness without relying on expensive motion platforms.
Simulator sickness continues to pose a significant challenge in the use of driving simulators across various sectors. While individual factors such as gender, age, and gaming experience play a crucial role in determining susceptibility to SS, there are still substantial research gaps in understanding how these factors relate with the type of driving task and simulator platform used. Addressing these gaps will not only improve the design of simulators but also enhance the user experience, making these tools more effective and accessible for a broader range of applications. In the present study we investigated the prevalence of simulator sickness and the effects of gender, age, type of driving environment, and previous experience of gaming on the degree of simulator sickness when driving a desktop driving simulator. Furthermore, an attempt is made to predict which of the factors; age, gender, type of driving environment, and previous experience of gaming best predict simulator sickness when driving a desktop driving simulator.
A total of 363 Swedish police students (Mage = 29.1, SD = 7.88) participated in the study between December 2022 to August 2024. More specifically, 203 males (Mage = 28.5, SD = 7.72) and 160 females (Mage = 29.8, SD = 8.04. At this university’s police education program, students participate in simulation-based lessons as part of their training. Specifically, they have a low-speed maneuvering and city traffic lesson during their first semester and a country road driving lesson during their fourth semester. Based on the timing of data collection, no student completed the questionnaire for both lessons. Each driving simulator featured a QR code for participants interested in joining the study. After their session, they scanned the code to access a questionnaire that included background questions (e.g., informed consent, age, gender, simulator driving type, gaming experience) and the Simulator Sickness Questionnaire (SSQ) (Bimberg et al., 2020; Kennedy et al., 1993).
The simulator room, where students practice driving, is equipped with six desktop-based simulation stations (Figure 1). Each station is powered by a PC featuring an Intel i7 10700k processor (3.80 GHz), an NVIDIA RTX 3070 GPU (8 GB), and 64 GB of DDR4 RAM at 2,933 MHz. The visual display comprises three 31.5-inch curved monitors (1500R curvature) with a native resolution of 2560 × 1440 and a refresh rate of 60 Hz. These monitors provide a front view and two side views, offering a visual field of approximately 135° for the driver. The simulation setup includes Logitech TrueForce C923 steering wheel and pedals, along with a Logitech Driving Force Shifter for gear changes, delivering realistic tactile feedback. Audio output is provided via Jabra headphones. The simulations run on Skillster software operated on Windows 11 Education (version 23H2). The maximum speed within the simulation environment is approximately 180 km/h.

Figure 1. Three-monitor simulator configuration with steering wheel and pedals.
Each lesson is scheduled for 1 hour and 45 min, with six students attending each session, one per simulator. On average, students drive for approximately 60 min, as the lesson also includes theoretical components and breaks. During low-speed maneuvering, various exercises are used where students practice driving in tight spaces, both forward and backward, in urban environments (see Figure 2).

Figure 2. Shown is the simulation exercise where students practiced maneuvering in tight urban situations.
Additionally, a more advanced exercise was included where students trained on a simulated track that was an exact replica of the track used on the actual driving yard (see Figure 3). To create this simulated track, drone footage and video clips, along with measurements of the total length and width of the driving yard, obstacles, and distances between them, were sent to Skillster so they could replicate the exercise in the simulator. This exercise is therefore a simulated copy of the driving yard setup that all students are tested on using real vehicles.

Figure 3. Shown is the simulation exercise where students practiced in advanced maneuvering paths similar to the real driving yard.
For rural road driving, students practiced various exercises in the simulator (see Figure 4). Here, students trained to apply safe police tactical driving in traffic environments, which required them to explain and, on a basic level, drive according to the principles of vehicle positioning. Students also had to identify the need to adapt their driving and speed to changing conditions to ensure safety was not compromised.

Figure 4. Simulation exercise where the students practiced rural road driving.
In this study, the Simulator Sickness Questionnaire (SSQ), developed by Kennedy et al. (1993), was used to assess participants’ symptoms of simulator sickness after exposure to the driving simulator. This tool was chosen for its reliability and widespread use in studies involving simulated environments and virtual reality.
The SSQ, a 16-item self-report scale, evaluates symptoms across three dimensions: nausea, oculomotor disturbance, and disorientation. Each symptom is rated on a scale from 0 to 3, with scores then weighted (see Bimberg et al., 2020; Kennedy et al., 1993) to calculate an overall SSQ score.
Statistical analysis was performed using IBM SPSS Statistics (version 29). We began with a descriptive analysis of the participants, age, gender, gaming experience, type of driving in the simulator, and perceived simulator sickness. In the next step we compared the outcome, namely, the perceived simulator sickness, between the groups. One-way ANOVA was used to compare means in perceived simulator sickness. If there was a statistically significant difference between groups a post-hoc Tukey’s HSD test was used to follow up the analysis.
Furthermore, a multiple linear regression analysis was conducted to examine the relationship between the overall simulator sickness score (TotalSimSick) and age, gender, gaming experience, and type of driving (base model). We then ran another model which included interaction terms between the independent variables.
The descriptive overview (see Table 1) of the study’s participants based on key variables, means and standard deviations, showed that, regarding gaming experience, 135 males and 25 females reported having prior gaming experience, while 68 males and 135 females indicated no such experience. This highlights a notable gender disparity in gaming background, with a significantly higher proportion of male participants having gaming experience.
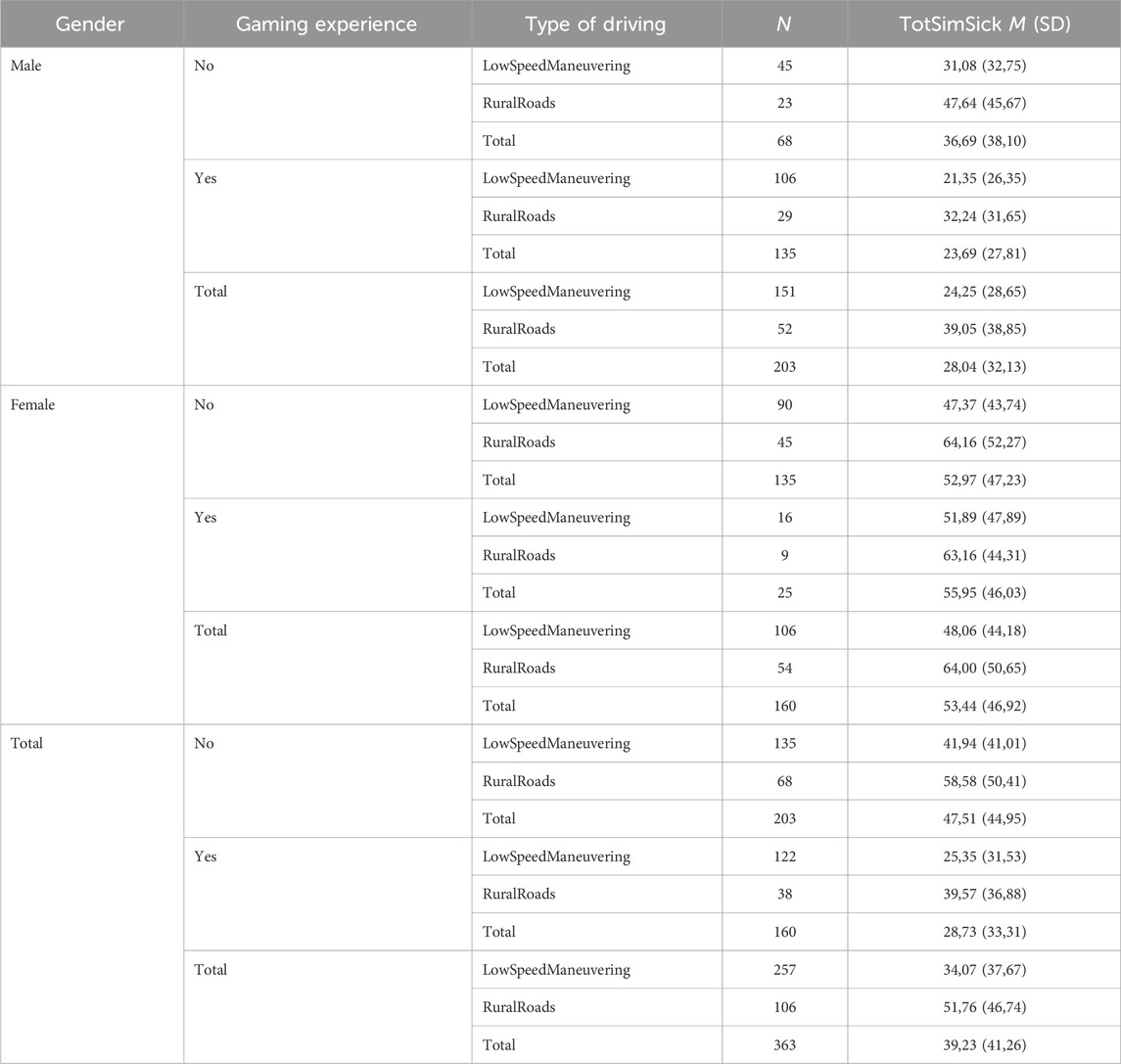
Table 1. Summary of means and standard deviation for all variables.
The type of driving environment was categorized into low-speed maneuvering and rural roads. For low-speed maneuvering, 151 males and 106 females were included, while for rural roads, 52 males and 54 females participated. These distributions show relatively balanced representation between genders across the different driving scenarios, allowing for a comparative analysis of simulator sickness symptoms under varying conditions.
A one-way analysis of variance (ANOVA) was conducted to examine the effect of gender on total simulator sickness score. Effect sizes were calculated using eta squared (η2) to measure the strength of the associations (Cohen, 1988). The total simulator sickness score was significantly different between males and for females, F (1,361) = 37.30, p < 0.001, with a small-to-medium effect size (η2 = 0.094). To further explore these differences, a post-hoc analysis using Tukey’s Honest Significant Difference (HSD) test was performed. The post-hoc Tukey’s HSD test revealed that females showed significantly higher scores compared to males, with a mean difference of 25.39 (95% CI [17.22, 33.57], p < 0.001). These findings indicate that females experienced significantly greater simulator sickness symptoms than males.
Another one-way ANOVA was conducted to evaluate the effect of game experience on total simulator sickness score. The ANOVA for total simulator sickness demonstrated a significant effect of game experience, F (1,361) = 19.50, p < 0.001, with a small effect size (η2 = 0.051). The post-hoc Tukey’s HSD test showed a significant difference, with gamers reporting a mean decrease of −18.79 (95% CI: [-27.15, −10.42], p < 0.0001). These results highlight that individuals without game experience tend to experience more severe symptoms of simulator sickness.
Finally, a one-way ANOVA was conducted to evaluate the effect of type of driving in the simulator on total simulator sickness score. The total simulator sickness score was significantly higher in country road driving scenarios compared to city traffic, F (1,361) = 14.31, p < 0.001, with a small-to-moderate effect size (η2 = 0.038). The post-hoc Tukey’s HSD test, for total simulator sickness, revealed that those driving on country roads reported significantly higher sickness scores, with a mean difference of 17.69 (95% CI [8.49, 26.89], p < 0.001). These results confirm that participants in the country road scenario experienced more severe simulator sickness symptoms compared to those in the city traffic scenario.
A multiple linear regression analysis was conducted to examine the relationship between simulator sickness (measured by the TotalSimSick score) and four independent variables: gender (0 = male, 1 = female), age (continuous), game experience (0 = no, 1 = yes), and type of driving (0 = city traffic, 1 = country road). The goal was to determine the extent to which these factors predict the severity of simulator sickness. Variance Inflation Factor (VIF) values were calculated to check for multicollinearity among the predictor variables. All VIF values (Gender 1.36, Age 1.08, Game experience 1.43, and Type of driving 1.03) were below 2, indicating no multicollinearity concerns (Hair et al., 2010).
The overall regression model was statistically significant, F (4,358) = 14.95, p < 0.001, indicating that the independent variables together explain a significant portion of the variance in simulator sickness. The model had an R2 of 0.143, meaning that approximately 14.3% of the variability in TotalSimSick was accounted for by the predictor variables. The adjusted R2 was 0.134, reflecting a slight adjustment for the number of predictors. The regression coefficients and their statistical significance are presented in Table 2.
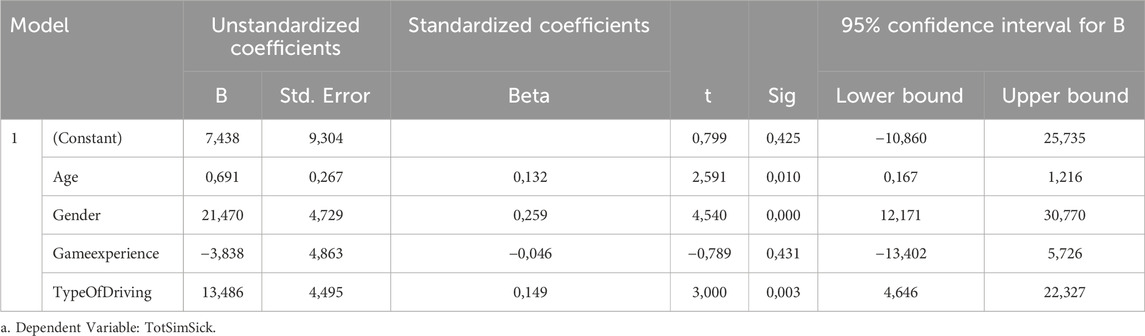
Table 2. Multiple linear regression results for simulator sickness (TotalSimSick.
The multiple linear regression model explained 14.3% of the variance in simulator sickness scores (R2 = 0.143). Gender was the most influential predictor, with a standardized beta coefficient (β = 0.259) indicating that females significantly higher simulator sickness scores compared to males, with an increase of 21.47 points on the TotalSimSick scale (p < 0.001).
There was a positive relationship between age and simulator sickness, with a 0.69-point increase (β = 0.132) in TotalSimSick for each additional year of age (p = 0.010). Participants who experienced country road driving reported significantly higher simulator sickness scores compared to those who drove in city traffic, with a 13.49-point increase (β = 0.149, p = 0.003). Game experience was not a significant predictor of simulator sickness (β = − 0.046, p = 0.431).
The regression model with interaction terms showed that, collectively, age, gender, game experience, type of driving, and their interactions accounted for 15.1% of the variance in simulator sickness scores, R2 = 0.151, F (10,352) = 6.28, p < 0.001. However, none of the individual predictors or interaction terms (Gender × Age, Gender × Type of Driving, Age × Type of Driving, Gender × Game experience, Age × Game experience, Type of driving × Game experience) reached statistical significance, suggesting that the inclusion of interactions does not meaningfully enhance the model’s explanatory power over the main effects alone. The base model, without interaction terms, is more interpretable and achieves nearly the same explanatory power. Interaction effects between gender, age, and type of driving do not meaningfully impact simulator sickness scores. Therefore, the base model is preferable for interpreting the main effects of each variable.
The findings of this study contribute to the growing body of literature on simulator sickness (SS) in general, highlighting the significant influence of gender, age, driving environment, and gaming experience on SS in the context of a desktop driving simulator. More specifically, using a relatively large sample of police trainees, this research not only confirms several established patterns in SS susceptibility but also provides new insights into the complex interplay between individual differences and simulator design.
The results strongly support that females experience higher levels of SS. This aligns with numerous studies emphasizing gender as a critical determinant of SS. Mourant and Thattacherry (2000) and Stanney et al. (2020) reported that women tend to experience greater symptoms due to physiological differences, particularly in vestibular sensitivity and hormonal fluctuations. Another explanation could be sex differences in postural stability (Riccio & Stoffregen, (1991). For example, a study by Munafo et al. (2017) confirmed that sex differences in postural control precede and contribute to variations in motion sickness susceptibility. Their findings showed that motion sickness was more common in women than in men, potentially due to physiological differences between the sexes. In this study, females consistently reported higher SS scores, with significant mean differences confirmed by both ANOVA and post-hoc analyses. The regression analysis identified gender as the most significant predictor of SS, with females scoring 21.47 points higher on the Total Simulator Sickness scale than males. This finding underscores the persistent gender disparity in SS, which has been described by some researchers (e.g.; Munafo et al., 2017; Stanney et al., 2020) as a form of “technological sexism.” This suggests that simulator developers must prioritize gender-sensitive design features, such as reducing optic flow intensity or incorporating pre-adaptation protocols to mitigate SS among female users.
Age emerged as another significant predictor of SS, with older participants reporting more severe symptoms. For every additional year of age, SS scores increased by 0.69 points, a finding consistent with research by Diels and Howarth (2013) and Keshavarz et al. (2018). These studies highlight the age-related decline in sensory processing, which compromises the ability to resolve sensory conflicts effectively. Despite the relatively narrow age range in this study (M = 29.1, SD = 7.88), even small differences in age significantly influenced SS outcomes. Notably, older participants in this sample were still relatively young (with most under 40), suggesting that the observed age effects might be more pronounced in older populations. Trick and Caird (2011) emphasized that older adults often exhibit severe SS symptoms, leading to higher dropout rates in simulator studies. This underscores the importance of designing simulators that accommodate age-related sensory changes, particularly for applications involving older users.
This study also found that country road scenarios resulted in significantly higher sickness scores than city traffic scenarios. This finding is consistent with prior research by Mourant and Thattacherry (2000) and Keshavarz and Hecht (2011), who reported that high-speed environments and scenarios with heightened optic flow (e.g., rural roads with curves) amplify sensory conflicts. Similar findings have been reported in studies using driving simulation in VR (e.g., Venkatakrishnan et al., 2020) where participants had increased SS-symptoms based on the workload (i.e., higher levels of optic flow). Participants driving in rural environments experienced increased disorientation and oculomotor strain, likely due to the combination of rapid visual changes and prolonged exposure to consistent motion cues. In contrast, city traffic scenarios, characterized by frequent stops and lower speeds, produced milder symptoms. These results support Brooks et al. (2010), who noted that predictability in driving tasks, such as in urban environments, can help reduce SS by minimizing unexpected sensory mismatches. The regression analysis further confirmed that driving on country roads increased Total Simulator Sickness scores by 13.49 points compared to city driving, highlighting the need to adapt driving scenarios to reduce optic flow and visual demands in rural settings.
Previous research has often highlighted gaming experience as a protective factor against SS (Grassini et al., 2021; Pohlmann et al., 2021). However, in this study, while ANOVA results showed that non-gamers reported significantly higher SS scores, gaming experience did not emerge as a significant predictor in the regression model. This discrepancy suggests that gaming’s influence on SS may be context-dependent, offering limited benefits in desktop-based simulators with specific design characteristics. The findings imply that while gaming may help users adapt to virtual environments, its mitigating effects on SS are overshadowed by stronger predictors like gender and driving environment. It is also possible that gaming experience has a more pronounced impact in highly immersive setups, such as those using head-mounted displays (HMDs), as noted by Grassini et al. (2021). Further research is needed to explore how different types of gaming exposure interact with various simulator configurations.
Interestingly, the inclusion of interaction terms in the regression model did not significantly enhance its explanatory power, suggesting that the main effects of gender, age, and driving environment are sufficient to account for most observed variability in SS. The final model explained 14.3% of the variance in Total Simulator Sickness scores, indicating that while these factors are important, additional unexplored variables (e.g., visual fidelity, motion cue alignment) might also contribute to SS. The absence of significant interaction effects, such as between gender and age or driving environment, reinforces the idea that these factors independently influence SS. This simplifies the interpretation of the results and supports the development of targeted interventions based on individual characteristics rather than their combinations.
The study’s findings have several practical implications for the design and application of driving simulators. First, given the significant impact of gender, developers and educators should consider implementing gender-sensitive features, such as adjustable visual flow rates or personalized acclimatization protocols. These adaptations could help mitigate the heightened SS susceptibility observed in females. Furthermore, the significant impact of age underscores the need for customized simulation designs. Older adults require tailored simulations to account for sensory decline and longer recovery times, while younger adults and children benefit from designs that consider gender differences and the potential for habituation through prior experience. Age- and gender-specific interventions are crucial as virtual environments become increasingly prevalent in higher education, ensuring that pedagogical and didactical approaches are adapted to meet the diverse needs of learners. By addressing the unique challenges faced by different demographic groups, educators can create equitable and inclusive learning experiences that enhance accessibility and foster equal opportunities for academic success across all genders and age groups.
Second, the strong influence of driving environment underscores the need for scenario-specific optimizations. For rural or high-speed environments, reducing optic flow intensity and incorporating predictive motion cues could alleviate SS symptoms. Conversely, urban scenarios may require less adjustment, given their lower associated SS severity.
Finally, while gaming experience may offer limited protective benefits in desktop simulators, it still holds potential as a training tool for non-gamers. Familiarizing users with virtual environments through controlled gaming exposure could enhance their tolerance to sensory conflicts, particularly in more immersive simulation setups.
This study’s analysis has several limitations related to variable types, sample size, and generalizability. First, the study includes both categorical and continuous predictors in the regression model, such as gender (categorical), age (continuous), and type of driving (categorical). While this approach allows for analysis across different types of variables, it assumes a linear relationship between continuous variables and simulator sickness. Non-linear relationships could potentially exist, especially with age, and may impact the accuracy of the model’s predictions. Furthermore, the reliance on self-reported data for categorical variables (e.g., game experience) could introduce recall or response bias, which may affect the accuracy of the findings. Future research should include objective measures of SS (e.g., physiological data on participants) and consider larger and more diverse samples, test for potential non-linear effects, and incorporate additional predictors (e.g., workload measures) to enhance the model’s generalizability and robustness.
Second, the sample size, though sufficient for detecting medium effect sizes, may limit the power to detect smaller but potentially meaningful effects, especially with several interaction terms. A larger sample size could provide more stable estimates and increase the sensitivity of the model to detect subtle effects. This is particularly relevant given the inclusion of game experience as an independent variable, which did not reach statistical significance and may have benefited from additional data to clarify its role. More research is needed to explore how different gaming types, such as first-person shooters or racing games, impact SS and how long-term gaming interacts with factors like gender and age. While females generally exhibit greater SS susceptibility, individual factors like gaming experience and virtual environment exposure play a role. Future research should focus on gender-sensitive solutions, such as pre-exposure training and adaptive simulator designs, to reduce SS. Understanding the interplay of physiological, psychological, and experiential factors remains key to mitigating SS in diverse user groups.
A third limitation involves potential confounding variables. While no student completed the questionnaire for both lessons, those who responded after the country road lesson had previously participated in a simulator session during their first semester. This prior experience could have led to familiarization or adaptation, possibly reducing simulation sickness (SS) in this group. However, this seems unlikely given the more than 1-year gap between sessions and the fact that SS was higher during the country road session. Another potential confounder is the difference in traffic conditions between the two environments. The urban environment may have involved less prolonged movement, which could reduce SS. Additionally, the study did not measure workload (e.g., visual-, auditory-, cognitive aspects of the different tasks in the simulator), a factor that could influence perceived SS across environments (Jasper et al., 2023; Sepich et al., 2022; Venkatakrishnan et al., 2023). Workload is also tied to the duration of simulator sessions; for example, low-speed maneuvering and city traffic exercises are shorter than country road driving sessions, potentially affecting SS. These factors were not controlled for in this study.
Furthermore, the sample, while large and diverse in terms of gender and type of driving in the simulator, predominantly consisted of young adults, limiting the generalizability of age-related findings. Future research should aim to include older populations to better understand how age interacts with SS.
Another thing is that the model’s R-squared value indicates that approximately 14.3% of the variance in simulator sickness scores is explained by the predictors, suggesting that other unmeasured factors may play a substantial role. While this study examined key predictors of SS, other variables such as visual display quality, latency, prior exposure to simulators, user expectations, motion sensitivity, and physiological factors were not considered. Investigating these factors could further enhance the predictive power of SS models and inform the design of more effective simulators.
Lastly, the study focused exclusively on a desktop simulator, which may produce different SS patterns compared to motion-based systems. Exploring how different simulator types influence the relationships between individual factors and SS would provide a more comprehensive understanding of these dynamics.
This study highlights the complex interplay between gender, age, driving environment, and gaming experience in predicting simulator sickness in a desktop driving simulator. Females and older participants consistently reported higher SS symptoms. Rural driving scenarios lead to increased sickness levels. Although gaming experience had a modest effect, it was overshadowed by stronger predictors. These findings emphasize the importance of personalized simulator design and scenario optimization to reduce SS and improve user experience and provide equal learning environments. Future research should expand on these insights by including more diverse populations and exploring additional factors that contribute to SS.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Swedish Ethical Review Authority (Dnr 2022-01641-01, 25 May 2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
JI: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing–original draft. CM: Conceptualization, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing–review and editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Almallah, M., Hussain, Q., Reinolsmann, N., and Alhajyaseen, W. K. M. (2021). Driving simulation sickness and the sense of presence: correlation and contributing factors. Transp. Res. Part F Traffic Psychol. Behav. 78, 180–193. doi:10.1016/j.trf.2021.02.005
Alonso, F., Faus, M., Riera, J. V., Fernandez-Marin, M., and Useche, S. A. (2023). Effectiveness of driving simulators for drivers’ training: a systematic review. Appl. Sci. 13 (9), 5266. doi:10.3390/app13095266
Balk, S. A., Bertola, D. B., and Inman, V. W. (2013). Simulator sickness questionnaire: twenty years later. Driv. Assess. Conf. 7. doi:10.17077/drivingassessment.1498
Bimberg, P., Weissker, T., and Kulik, A. (2020). “On the usage of the simulator sickness questionnaire for virtual reality research,” in 2020 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW). Atlanta, USA, 22–26 March 2020, (IEEE), 464–467. doi:10.1109/VRW50115.2020.00098
Bles, W., Bos, J. E., de Graaf, B., Groen, E. L., and Wertheim, A. H. (1998). Motion sickness: only one provocative conflict? Brain Res. Bull. 47 (5), 481–487. doi:10.1016/S0361-9230(98)00115-4
Brooks, J. O., Goodenough, R. R., Crisler, M. C., Klein, N. D., Alley, R. L., Koon, B. L., et al. (2010). Simulator sickness during driving simulation studies. Accid. Analysis and Prev. 42 (3), 788–796. doi:10.1016/j.aap.2009.04.013
Chaumillon, R., Romeas, T., Paillard, C., Faubert, J., Giraudet, G., Bouchard, J. F., et al. (2017). The use of transdermal scopolamine to solve methodological issues raised by gender differences in susceptibility to simulator sickness. Transp. Res. Part F Traffic Psychol. Behav. 47, 42–58. doi:10.1016/j.trf.2017.04.003
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates.
Dennison, M. S., and D'Zmura, M. (2017). Cybersickness without the wobble: experimental results speak against postural instability theory. Appl. Ergon. 58, 215–223. doi:10.1016/j.apergo.2016.06.014
Dennison, M. S., Wisti, A. Z., and D’Zmura, M. (2016). Use of physiological signals to predict cybersickness. Displays 44, 42–52. doi:10.1016/j.displa.2016.07.002
Diels, C., and Howarth, P. A. (2013). Frequency characteristics of visually induced motion sickness. Hum. Factors 55 (3), 595–604. doi:10.1177/0018720812469046
Garcia, A., Baldwin, C., and Dworsky, M. (2010). Gender differences in simulator sickness in fixed-versus rotating-base driving simulator. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 54 (19), 1551–1555. doi:10.1177/154193121005401941
Godfrey, C. A., Oody, J. F., Conger, S. A., and Steeves, J. A. (2024). Active virtual reality games: comparing energy expenditure, game experience, and cybersickness to traditional gaming and exercise in youth aged 8–12. Games Health J. 13 (1), 42–48. doi:10.1089/g4h.2024.0034
Grassini, S., Laumann, K., and Luzi, A. K. (2021). Association of individual factors with simulator sickness and sense of presence in virtual reality mediated by head-mounted displays (HMDs). Multimodal Technol. Interact. 5 (3), 7. doi:10.3390/mti5030007
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., and Tatham, R. L. (2010). Multivariate data analysis. 7th ed. New York: Pearson Prentice Hall.
Himmels, C., Czupala, A. R., Fahmüller, T., and Riener, A. (2022). “The influence of gaming experience and optic flow on simulator sickness: insights from a driving simulator study,” in Adjunct proceedings of the 14th international ACM conference on automotive user interfaces and interactive vehicular applications, 97–102. doi:10.1145/3544999.3552532
Hoffmann, S., Kruger, H. P., and Buld, S. (2003). Avoidance of simulator sickness by training the adaptation to the driving simulation. VDI Berichte 1745, 385–406.
Ingrell, J., Egerius, C., and Mellgren, C. (2022). Simulator-based driving training in low-speed maneuvering for Swedish police students. Nordic J. Stud. Polic. 1, 1–13. doi:10.18261/njsp.9.1.10
Jasper, A., Sepich, N. C., Gilbert, S. B., Kelly, J. W., and Dorneich, M. C. (2023). Predicting cybersickness using individual and task characteristics. Comput. Hum. Behav. 146, 107800–107812. doi:10.1016/j.chb.2023.107800
Kennedy, R. S., Drexler, J., and Kennedy, R. C. (2010). Research in visually induced motion sickness. Appl. Ergon. 41 (4), 494–503. doi:10.1016/j.apergo.2009.11.006
Kennedy, R. S., Lane, N. E., Berbaum, K. S., and Lilienthal, M. G. (1993). Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3 (3), 203–220. doi:10.1207/s15327108ijap0303_3
Keshavarz, B., and Hecht, H. (2011). Axis rotation and visually induced motion sickness: the role of combined roll, pitch, and yaw motion. Aviat. Space, Environ. Med. 82 (11), 1023–1029. doi:10.3357/ASEM.3078.2011
Keshavarz, B., Ramkhalawansingh, R., Haycock, B., and Campos, J. L. (2018). Comparing simulator sickness in younger and older adults during simulated driving under different multisensory conditions. Transp. Res. Part F Traffic Psychol. Behav. 54, 47–62. doi:10.1016/j.trf.2018.01.007
Kolasinski, E. M., and Gilson, R. D. (1998). Simulator sickness and related findings in a virtual environment. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 42 (21), 1511–1515. doi:10.1177/154193129804202110
Lucas, G., Kemeny, A., Paillot, D., and Colombet, F. (2020). A simulation sickness study on a driving simulator equipped with a vibration platform. Transp. Res. Part F Traffic Psychol. Behav. 72, 15–22. doi:10.1016/j.trf.2019.11.011
Matas, N. A., Nettelbeck, T., and Burns, N. R. (2015). Dropout during a driving simulator study: a survival analysis. J. Saf. Res. 55, 159–169. doi:10.1016/j.jsr.2015.08.004
Mourant, R. R., Rengarajan, P., Cox, D., Lin, Y., and Jaeger, B. K. (2007). The effect of driving environments on simulator sickness. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 51 (18), 1232–1236. doi:10.1177/154193120705101838
Mourant, R. R., and Thattacherry, T. R. (2000). Simulator sickness in a virtual environments driving simulator. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 44 (5), 534–537. doi:10.1177/154193120004400513
Munafo, J., Diedrick, M., and Stoffregen, T. A. (2017). The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp. Brain Res. 235 (3), 889–901. doi:10.1007/s00221-016-4846-7
Pawar, N. M., Yadav, A. K., and Velaga, N. R. (2023). A comparative assessment of subjective experience in simulator and on-road driving under normal and time pressure driving conditions. Int. J. Inj. Control Saf. Promot. 30 (1), 116–131. doi:10.1080/17457300.2022.2114091
Pohlmann, T., O'Hare, L., Focker, J., and Dickinson, P. (2021). “Is virtual reality sickness elicited by illusory motion affected by gender and prior video gaming experience?,” in Proceedings of the 2021 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops, Lisbon, Portugal, 27 March 2021–01 April 2021 (IEEE), 535–536. doi:10.1109/VRW52623.2021.00095
Rangelova, S., Rehm, K., Diefenbach, S., Motus, D., and André, E. (2020). “Gender differences in simulation sickness in static vs. moving platform VR automated driving simulation,” in HCI in mobility, transport, and automotive systems. Automated driving and in-vehicle experience design (Springer International Publishing), 146–165. doi:10.1007/978-3-030-50523-3_11
Riccio, G. E., and Stoffregen, T. A. (1991). An ecological theory of motion sickness and postural instability. Ecol. Psychol. 3 (3), 195–240. doi:10.1207/s15326969eco0303_2
Sepich, N. C., Jasper, A., Fieffer, S., Gilbert, S. B., Dorneich, M. C., and Kelly, J. W. (2022). The impact of task workload on cybersickness. Front. Virtual Real. 3, 1–19. doi:10.3389/frvir.2022.943409
Stanney, K. M., Fidopiastis, C., and Foster, L. (2020). Virtual reality is sexist: but it does not have to be. Front. Robotics AI 7, 4–10. doi:10.3389/frobt.2020.00004
Stanney, K. M., Kennedy, R. S., and Drexler, J. M. (1997). Cybersickness is not simulator sickness. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 41 (2), 1138–1142. doi:10.1177/107118139704100292
Stoffregen, T. A., Chang, C.-H., Chen, F.-C., and Zeng, W.-J. (2017). Effects of decades of physical driving on body movement and motion sickness during virtual driving physical driving on body movement and motion sickness during virtual driving. PLOS ONE, 12(11): e0187120. doi:10.1371/journal.pone.0187120
Trick, L. M., and Caird, J. K. (2011). “Methodological issues when conducting research on older drivers,” in Handbook of driving simulation for engineering, medicine, and psychology. Editor D. L. Fisher (Boca Raton: CRC Press), 24–32.
Venkatakrishnan, R., Venkatakrishnan, R., Anaraky, R. G., Volonte, M., Knijnenburg, B., and Babu, S. V. (2020). “A structural equation modeling approach to understand the relationship between control, cybersickness and presence in virtual reality,” in 2020 IEEE conference on virtual reality and 3D user interfaces (VR) (IEEE), 682–691. doi:10.1109/VR46266.2020.00091
Venkatakrishnan, R., Venkatakrishnan, R., Raveendranath, B., Sarno, D. M., Robb, A. C., Lin, W. C., et al. (2023). The effects of auditory, visual, and cognitive distractions on cybersickness in virtual reality. IEEE Trans. Vis. Comput. Graph. 30, 5350–5369. doi:10.1109/TVCG.2023.3293405
Wang, Q., Zhao, W.-X., and Zhang, L. (2023). Assessment of individual differences for aftereffect of viewing autostereoscopic 3D display. J. Soc. Inf. Disp. 31 (1), 689–699. doi:10.1002/jsid.1265
Keywords: age, driving simulator, gaming experience, gender, higher education, police, simulator sickness
Citation: Ingrell J and Mellgren C (2025) From pixels to patrol cars: exploring desktop-based simulator sickness in police driving training. Front. Virtual Real. 6:1547752. doi: 10.3389/frvir.2025.1547752
Received: 18 December 2024; Accepted: 18 February 2025;
Published: 03 March 2025.
Edited by:
Thomas A. Stoffregen, University of Minnesota Twin Cities, United StatesReviewed by:
Rohith Venkatakrishnan, University of Florida, United StatesCopyright © 2025 Ingrell and Mellgren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joakim Ingrell, am9ha2ltLmluZ3JlbGxAbWF1LnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.