 Shamus P. Smith
Shamus P. Smith Eugene Nalivaiko
Eugene Nalivaiko Sam Owen3
Sam Owen3 Didier Depireux
Didier Depireux Mark Flynn
Mark Flynn
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 23 January 2025
Sec. Technologies for VR
Volume 5 - 2024 | https://doi.org/10.3389/frvir.2024.1478106
Introduction: There is increasing use of head-worn displays to support immersive virtual reality (VR) experiences. However, users of such technology often encounter motion sickness-like effects, commonly termed cybersickness. The unpleasant effects of cybersickness can limit the duration of VR technology usage and deter return use after only one bad experience. One explanation of cybersickness is that it is a physiological responses to perceived differences between the visual and vestibular stimulation provided via VR technology and the user’s current body positioning and movement, i.e., a mismatch between visual and vestibular senses.
Methods: An exploratory user study is described that investigates the use of technology to influence vestibular cues and change experiences of cybersickness. A vestibular stimulation device using bone conduction was applied to users experiencing cybersickness induced by a VR roller-coaster in a head-worn display. Three conditions were tested: a control group without the device and two groups with the device configured to different vibration force levels.
Results: Results showed that users with the stronger vibration level, when compared to a control group, had different virtual environment experiences with longer ride durations and lower reported nausea scores.
Discussion: Although limited by participant numbers, the results are promising for applying vestibular stimulation to positively influence cybersickness experiences in head-worn displays. Given the spreading application of VR technologies and the need to mitigate cybersickness, there is a need to further evaluate the efficacy of such devices.
The widespread availability of affordable head-worn displays (HWD), also commonly referred to as head-mounted displays or VR headsets, has significantly increased general engagement with virtual reality (VR) (Smith and Burd, 2019; Weech et al., 2018). This has led to increased opportunities for people to have virtual reality experiences and for the VR industry to both increase commercial output of hardware, i.e., head-worn displays and associated accessories, and software products, most notably VR games and educational products. Although each generation of HWD hardware has typically improved technical specifications, the immersive experiences provided in VR are not suited for all users.
Users of virtual reality technology often encounter motion sickness-like effects commonly termed cybersickness (Nesbitt and Nalivaiko, 2024; Rebenitsch and Owen, 2016; Stanney et al., 2020)1, with feelings of nausea, dizziness and sweatiness (Mittelstaedt et al., 2018). Cybersickness as a result of HWD use has been an ongoing research topic [reviews on cybersickness include (Botha and De Wet, 2024; Davis et al., 2014; Rebenitsch and Owen, 2016; Tian et al., 2022)]. Experiencing cybersickness can be a significant barrier to using virtual reality systems (Woo et al., 2023). Stanney and Kennedy (2009) note that 80%–95% of individuals using HWDs report some type of side effect and up to 50% of users experienced symptoms severe enough to end participation. Also approximately 50% of those that ended their VR experience did so in the first 20 min and nearly 75% did so by 30 min (Stanney and Kennedy, 2009).
Although repeated use of virtual reality has been shown to increase resistance to motion sickness (Mouloua et al., 2004) and cybersickness (Clemes and Howarth, 2003; Howarth and Hodder, 2008), the unpleasant effects of cybersickness can limit the duration of virtual reality technology usage and deter return use after only one bad experience. As there is increasing demand for the use of virtual reality applications in industry, defence, education and consumer markets, new approaches for reducing cybersickness are needed (Weech et al., 2018).
There are three main theories on the causes of cybersickness including (i) the sensory conflict theory, (ii) the poison theory and (iii) the postural instability theory [see (LaViola, 2000; Stanney et al., 2020) for overviews of each theory]. In the work described here, we focuses on the sensory conflict theory (LaViola, 2000; Reason and Brand, 1975) and how it can explain cybersickness as a mismatch between the visual and vestibular senses (Keshavarz et al., 2015; McCauley and Sharkey, 1992). Specifically, that the causes of cybersickness are grounded in physiological responses to perceived differences between the visual and vestibular stimulation provided via VR technology and the user’s current body positioning and movement.
VR applications often attempt to reduce sensory conflict by (i) providing a sympathetic VR use environment, for example, having users stand and move naturally in a small space so their movements mimic the VR presented visuals (Clifton and Palmisano, 2020; Farmani and Teather, 2020), (ii) providing specialised interface-based refinements to block cybersickness inducing visuals, for example, reducing the field-of-view when users engage in real-time lateral movement (Fernandes and Feiner, 2016) or (iii) adding additional feedback to reduce sensory misalignment, for example, providing airflow (Harrington et al., 2019) or proprioceptive (Gardé et al., 2018; Sra et al., 2019) feedback. These approaches limit VR application use due to the need for physical space/movement restrictions, customised user interface design and/or specialised hardware.
We have investigated a more general solution via a core physical determinant of cybersickness, namely the vestibular sense. A prototype vestibular stimulation technology has been developed (Otolith Labs, Washington DC, United States) and shown to reduce motion sickness-like symptoms, for example, decrease nausea in automated vehicles (Salter et al., 2020). Here, we have explored how this technology can interfere with the user’s natural physiological vestibular reaction to virtual reality experiences by adding additional vestibular stimulation.
Vestibular stimulation has been shown to improve measures of balance (Stefani et al., 2020) and reduce motor and non-motor symptoms associated with Parkinson’s disease (Wilkinson, 2021). Studies have also revealed a modulating effect of vestibular stimulation on mood state, emotional control, and anxiety level (Pasquier et al., 2019). Device induced vestibular stimulation has the advantage of being a non-pharmaceutical method and has been effective as a treatment for seasickness (Gutkovich et al., 2022).
In the current exploratory study, we have investigated the efficiency of vestibular stimulation to influence cybersickness experiences using a portable device equipped with a non-invasive bone conduction transducer that is worn by a user while using a head-worn display. To achieve reliable onset of cybersickness, we used an intentionally highly provocative virtual reality experience, in this case a virtual roller-coaster ride (Nalivaiko et al., 2015; Nesbitt et al., 2017; Sra et al., 2019). We used a verbal protocol to collect in situ experiences of nausea. Participant’s exit time from the roller-coaster ride was collected in addition to a pre-survey on previous motion sickness experiences and a post-survey on nausea during the current virtual reality experience.
An exploratory user study was conducted on 30 healthy individuals, 9 female and 21 male with an age range of 19–37 years (mean age = 25.80 years, std.dev = 4.77). Participants received either university course credit or a AUD$30 gift voucher for their time. The study protocol was approved by the Human Research Ethics Committee of the University of Newcastle, Australia (H-2019-0245).
An overview of the experimental approach can be seen in Figure 1. After arrival to an air-conditioned room (kept at
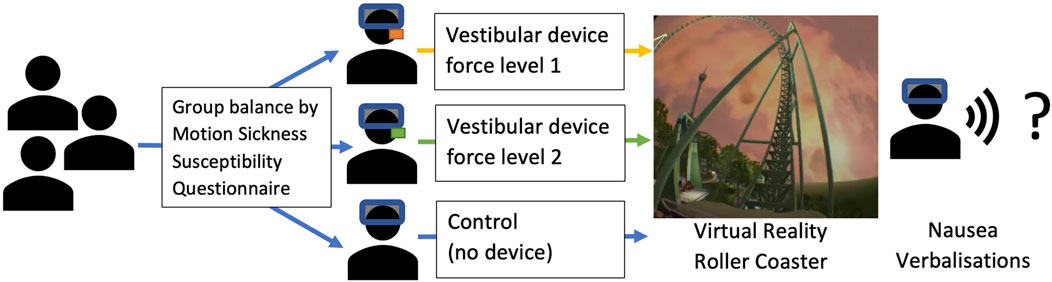
Figure 1. Summary of the vestibular stimulation experiment.
Based on the MSSQ-Short norms determined by (Lamb and Kwok, 2015) with a combined (weighted for gender bias) MSSQ-Short mean of 16.75 (stdev = 11.8), participants were allocated across four clusters with low to very high labels based on MSSQ-Short mean plus/minus 1 standard deviation. Final participant allocation is shown in Table 1.

Table 1. Final participant group allocation by MSSQ-Short score.
All participants successfully completed a stereo vision and depth perception test [the Frisby Stereotest (Frisby, 1983)]. After completing the test and confirming stereo vision, participants were fitted with a head-worn virtual display (Oculus Rift CV12, Facebook Reality Labs, United States). The interpupilary eye distance (IPD) setting on the CV1 was not adjusted between participants and set at the middle IPS setting of 65 mm. A vestibular stimulation device, provided by Otolith Labs (Otolith Labs, Washington DC, United States), was fitted to each participant in a device group, on the mastoid behind the right ear (see Figure 2). The Otolith device uses bone conduction and has four vibration force level settings, where setting 1 had the lowest vibration force and setting 4 had the strongest vibration force. In the experiment described here, the lowest vibration force level setting (1 on the device) is labelled as Device 1 and a medium setting (3 on the device) is labelled as Device 2. The experiment staff were not made aware of any expected benefits or differences from either vibration force level settings, only that setting 1 on the device had less vibration force than setting 3.

Figure 2. Otolith vestibular stimulation device placement.
While participants were seated in a stationary office chair, the VR roller-coaster simulation ride (Helix, Archivision, NL) was activated (see Figure 3) and continued for a maximum of 15 min or whenever participants decided to terminate the ride. Participants were asked to verbally report their current nausea level every minute during the exposure on a scale from zero (no effect) to 10 (severe nausea—just about to vomit). The ride was also terminated by the experiment staff if the participant verbalised a nausea score of 8.
Figure 3. Example stereo view of the Helix VR roller-coaster ride.
Directly after the ride, participants completed a Motion Sickness Assessment Questionnaire (MSAQ) (Gianaros et al., 2001). Participants were asked to complete the questionnaire thinking about the very end of the ride, i.e., just before they or the experiment staff terminated the ride. In the MSAQ, post-session symptoms are categorised into four clusters: gastrointestinal (nausea, feeling sick in the stomach, feeling queasy, about to vomit), central (faint-like, light headiness, disoriented, dizzy and spinning), peripheral (sweaty, hot, clammy, cold sweat, temperature discomfort) and sopite (annoyed, drowsy, tired, uneasy). When answering each question of the MSAQ, the participant assigns a value from a range of 1 (not at all) to 9 (severe). These ratings are then summed for each group of related questions and used to generate an overall MSAQ score.
Virtual roller-coasters can be very unpleasant, particularly when they are selected to induce cybersickness. This can impact participant recruitment and therefore data analysis. This is particularly the case for within-subjects designs, as participants’ dropout and fail to return for additional roller-coaster sessions. For this exploratory study we used a between-subjects design to avoid participant dropout.
Our focus is on exploring whether the vestibular device, with its different vibration levels, indicate any differences when compared to a control group. Thus our analysis is matched to our smaller sized participant group, and specifically looking for differences in correlations between relevant metrics, rather than group wide significance. As an exploratory study with a new technology, we are looking for indicative evidence of difference on the participants’ virtual reality experiences to motivate further studies with larger numbers of participants. Without evidence of usefulness there are ethical implications for exposing large participants groups to unpleasant experiences such as virtual roller-coasters.
In evaluating the vestibular device, we were interested in four primary measures, (i) the previous history of motion sickness (MSSQ), (ii) the in situ virtual roller-coaster experience (the verbal reports of nausea), (iii) the duration of the roller-coaster ride and (iv) the reports of experience, collected post-session (MSAQ).
Our expectation is that participants with a previous history of motion sickness will experience more cybersickness (Jang et al., 2022) and that this will limit their ride duration (Nalivaiko et al., 2015; Nesbitt et al., 2017). Also, these participants will report higher scores in the post session reports of cybersickness effects. We expect that the control group (with no vestibular stimulation) will have similar cybersickness experiences to those reported in previous research (Nalivaiko et al., 2015; Nesbitt et al., 2017). We have formed the following hypothesis to determine whether the device groups have produced evidence of different experiences, i.e., from the additional vestibular stimulation.
H1: Participants with previous experiences of motion sickness will feel similar negative cybersickness effects in the roller-coaster simulation. We expect that reported history of previous motion sickness (MSSQ) will:
• H1a: positively correlate to verbal reports of nausea (i.e., the in situ nausea measure).
• H1b: negatively correlate to ride duration (time in seconds), i.e., as participants’ exit the virtual environment early.
• H1c: positively correlate to post-session recall of motion sickness-like symptoms (via the MSAQ) that are indicative of cybersickness.
H2: Reported nausea by participants will influence the time spent in the virtual roller-coaster and that this experience will be reported post-session. We expect that the verbal nausea rating will:
• H2a: negatively correlate to ride duration (time in seconds), i.e., more in situ feelings of nausea should shorten ride duration.
• H2b: positively correlate to post-session recall of motion sickness-like symptoms (via the MSAQ) that are indicative of cybersickness, i.e., more actual feelings of nausea should mean higher scores recalled in the post-session questionnaire.
H3: The time that participants spend in the roller-coaster will effect the participants’ experience reported post-session. We expect that ride duration (time in seconds) will negatively correlate to the post-session MSAQ scores, i.e., shorter ride time implies more motion sickness-like symptoms that are indicative of cybersickness.
The reported nausea ratings were only collected while participants were in the virtual roller-coaster. Thus if participants’ exited early, this would impact any rating average to create a standard nausea score [as in (Nesbitt et al., 2017)]. Therefore we have padded the nausea ratings up to 15 min with the highest rating, i.e., “10,” to indicate significant cybersickness that stopped the roller-coaster experience. Thus a participant who exited the roller-coaster after 3 min would have “10” added to ratings for 4–15 min before an average nausea score for their experience was generated.
Statistical analyses were performed using IBM SPSS Statistics (v29). Shapiro-Wilk tests determined that the data was not normally distributed and thus, the non-parametric Spearman’s rho was used to generate correlations. Statistical significance was set to
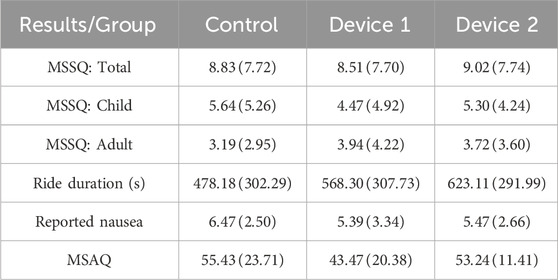
Table 2. Participant results, as mean and standard deviation (SD), across groups.
There was a strong, positive correlation between previous motion sickness (MSSQ) and reported nausea, which was statistically significant
There was a strong, negative correlation between reported nausea and ride duration, which was statistically significant
There was a moderate, negative correlation between ride duration and ride experience reported post-session (MSAQ), which was statistically significant
There was a weak, positive correlation between previous motion sickness (MSSQ) and reported nausea, which was not statistically significant
There was a strong, negative correlation between reported nausea and ride duration, which was statistically significant
There was a strong, negative correlation between ride duration and ride experience reported post-session (MSAQ), which was statistically significant
There was a weak, positive correlation between previous motion sickness (MSSQ) and reported nausea, which was not statistically significant
There was a strong, negative correlation between reported nausea and ride duration, which was statistically significant
There was a moderate, negative correlation between ride duration and ride experience reported post-session (MSAQ), which was not statistically significant
Table 3 provides a summary of the results of the correlation tests. Similar to other studies with virtual roller-coasters, the Control group exhibited the expected behaviour with previous higher motion sickness being predictive of cybersickness, resulting in higher nausea ratings and shorter ride duration. This provides a baseline for the other two groups where vestibular stimulation had been applied. In both the device groups, there were no statistically significant trends for previous motion sickness and negative cybersickness effects. This indicates the vibration from the device was having some influence on the experience, i.e., interfering with the baseline experiences.

Table 3. Summary of correlation results. Statistically significant results supporting hypotheses are bolded.
Participants across all the groups had a negative correlation of nausea rating versus ride duration. This is expected with provocative stimuli, like virtual roller-coasters, that was intentionally selected to induce cybersickness. What is more interesting is that participants in Device group 2 (moderate vibration) did not have a significant correlation between their reported nausea or ride duration versus their post-session experience questionnaire. Unlike the Control and Device 1 (low vibration) groups, this indicates a different experience for these participants.
Overall, the vestibular stimulation device with a medium vibration force level (Device group 2) induced a different in situ experience in the virtual reality roller-coaster with participants’ having fewer significant correlations to the metrics collected. After data collection and analysis were completed, Otolith Labs indicated that the device vibration force on setting 3 was calibrated to 96 dB (re:1 dyne3) and 50 Hz4. Thus the results are indicative of a positive influence of vestibular stimulation technology with a calibrated vibration force setting of 96 dB (re:1 dyne) and 50 Hz in a cybersickness provocative virtual environment.
In contrast to other research on the use of bone-conducted vibration (Weech et al., 2018), our experiment (i) used a commercial grade HWD, the Oculus CV1 compared to the Oculus Development Kit (version 0.8.0), (ii) applied constant vibration stimulation to the participants rather than brief random bursts of stimulation or stimulation bursts linked to angular acceleration thresholds within the virtual environment, (iii) used a commercial virtual environment in contrast to building a custom environment in a game engine, for example, Unity3D and (iv) included in situ participant’s verbal rating of current nausea rather than relying on post-session participant feedback. The aim was to differentiate our work from (Weech et al., 2018), specifically with the use of constant vestibular stimulation and capture a more ecological valid (McMahan et al., 2011) use of virtual reality technology with commercial off-the-shelf software and hardware.
However, the study was likely impacted by self selection bias, i.e., participants who know they have significant motion sickness or previous poor VR experiences are unlikely to volunteer for a VR roller-coaster study. These participants are likely to be those whom would get the most benefit from using vestibular device, i.e., more likely to have more cybersickness (Jang et al., 2022). One alternative approach would be for all participants to encounter all conditions, i.e., move from a between-subject to a within-subject design. Unfortunately, when using provocative stimuli, like a roller-coaster, participants with poor experiences are likely to opt out of future sessions, thus impacting recruitment. Also repeated VR experiences are known to have habituation effects (Clemes and Howarth, 2003; Howarth and Hodder, 2008), although this can be managed by extending the time between VR exposure sessions.
The study was also limited by the small participant pool. This suited the exploratory nature of investigating the new vestibular device but restricted the use of rigorous inferential testing. However, virtual roller-coasters can be an unpleasant experience and recruitment is thus difficult and, as noted above, potentially biased. However, we have balanced the smaller participant size with appropriate statistical measures and note that the results are only indicative of the changed VR experience for the participants with the stronger level of vibration. This motivates the need for further research in the use of such technologies. Based on the findings here, there is scope for further studies, with a larger number of participants, specifically focused on VR users with high MSSQ-Short scores.
The VR environment used in the research reported here was intentionally provocative, i.e., a VR roller-coaster, in order to elicit cybersickness within a short duration. This environment is not representative of many VR experiences. However, even with newer HWDs, users do report cybersickness after short durations of use. With the positive correlations found here between previous motion sickness and nausea ratings, participants with a history of motion sickness may get more benefit from the use of vestibular stimulation technology.
The impact of when to introduce vestibular stimulation (in the work described here, the stimulation was started before the VR experience), the appropriate duration of the stimulation (i.e., constant versus intermittent vibration) and the best level of vibration for an individual are all open research questions. Dynamic vestibular stimulation, both in duration and intensity, triggered by activity in the virtual environment and/or physiological changes of the user may also be useful areas of research. In our current work, we are exploring a more ecological valid (McMahan et al., 2011) VR environment and will repeat our approach to measure the influence of vestibular stimulation with a commercial off-the-shelf VR video game that supports active user interaction including VR walking and object selection/manipulation, rather than the seated, more passive, experience as in the VR roller-coaster used here.
The widespread availability of affordable HWDs and easy access to VR applications and games has significantly increased the use of VR technologies by the general public. Explicit negative effects of HWD use, such as cybersickness, often leads to self-selection opt out as users who experience negative effects stop using or avoid the technology (Stanney et al., 2020; Woo et al., 2023). However, opportunities to self-select away from VR use may be increasingly limited if VR technology is integrated into mainstream usage, e.g., training, general education and telepresence activities.
The work presented here has explored the use of vestibular stimulation to influence cybersickness experiences using a portable device equipped with a non-invasive bone conduction transducer that is worn by a user while using a head-worn display. Participants experienced a VR roller-coaster, to induce cybersickness. Data on participants’ experiences was captured via qualitative verbalisations in-session and a post-session survey. Three condition groups were investigated, namely control (no device) and two vestibular device groups with different vibration force settings.
Results indicated positive influence of a vestibular stimulation device, compared to a control group baseline, with a calibrated vibration force level on participants using a head-worn display. However, this was only an exploratory study and with a limited participant pool. Use of such vestibular technologies may be useful to support VR use if bone conductor technology could be built into HWDs or offered as an accessory. However, more research is needed in this area to map out individual user requirements. Future work will explore more typical VR environments, i.e., VR video games, and look for a larger participant pool to consolidate the results reported here.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Human Research Ethics Committee of the University of Newcastle, Australia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Validation, Visualization, Writing–original draft, Writing–review and editing. EN: Conceptualization, Funding acquisition, Methodology, Resources, Writing–review and editing. SO: Conceptualization, Funding acquisition, Methodology, Resources, Writing–review and editing. DD: Conceptualization, Funding acquisition, Methodology, Resources, Writing–review and editing. MF: Conceptualization, Funding acquisition, Methodology, Writing–review and editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported in part by an Australian Academy of Technology and Engineering: Global Connections Fund—Bridging Grant (#512035161).
The authors would like to thank the participants for their perseverance when experiencing the VR roller-coaster and Alireza Mazloumi Gavgani for his help during data collection.
Otolith Labs provided the prototype vestibular stimulation device but formed no part of the results analysis or conclusions on the device’s efficacy as reported here.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1Nesbitt and Nalivaiko (2024) note that “cybersickness and simulator sickness share similar symptoms with motion sickness although the conditions are caused by exposure to slightly different situations” where “motion sickness can be brought on by travelling in any type of moving vehicle including cars, buses, trains, aircraft, boats, and submarines and may also be induced on an amusement ride, a spinning chair or simply by using a swing at a playground” and “cybersickness is typically experienced by stationary users that perceive that they are moving in a virtual scene.” In the work presented here, we are interested in the latter, with the use of a virtual environment to induce cybersickness. In our experiment method we do use motion sickness surveys as these elicit the user experiences of motion sickness-like symptoms that happen with cybersickness. Exploring the differences/similarities between motion sickness and cybersickness is outside the scope of the work reported here [see (Gavgani et al., 2018; Palmisano et al., 2020)].
2The Oculus Rift CV1 has the following specifications: Resolution (1,080 × 1,200 per-eye), Refresh Rate (90 Hz), Display Type (2 x AMOLED binocular), IPD Range (58–72 mm hardware manual adjustable), Visible FoV (87° horizontal; 88° vertical), Rendered FoV (87.95° horizontal; 89.66° vertical; 98.07° diagonal), Binocular Overlap (71.15°).
3A unit of force in the centimeter-gram-second system equal to the force that would give a free mass of 1 g an acceleration of 1 cm per second per second (Merriam-Webster, 2024).
4Force level was measured using a Artificial Mastoid Type 4930 (Brüel and Kjær, Denmark). The Artificial Mastoid supports the calibration of bone-conduction devices by simulating the mechanical impedance of the human mastoid. The 96 dB force level is in reference to 1 dyne. This is not a sound pressure level. It is a force level with respect to 1 dyne.
Botha, B. S., and De Wet, L. (2024). CyPVICS: A framework to prevent or minimise cybersickness in immersive virtual clinical simulation. Heliyon 10, e29595. doi:10.1016/j.heliyon.2024.e29595
Clemes, S. A., and Howarth, P. A. (2003). “Habituation to virtual simulation sickness when volunteers are tested at weekly intervals,” in Human factors in the age of virtual reality, Editors D. de Waard, K. A. Brookhuis, S. M. Sommer, and W. B. Verwey(Maastricht, Netherlands: Shaker), 61–72.
Clifton, J., and Palmisano, S. (2020). Effects of steering locomotion and teleporting on cybersickness and presence in HMD-based virtual reality. Virtual Real. 24, 453–468. doi:10.1007/s10055-019-00407-8
Davis, S., Nesbitt, K., and Nalivaiko, E. (2014). “A systematic review of cybersickness,” in Proceedings of the 2014 Conference on Interactive Entertainment (IE2014), New York, NY (Newcastle, NSW: ACM), 8, 1–9. doi:10.1145/2677758.2677780
Farmani, Y., and Teather, R. J. (2020). Evaluating discrete viewpoint control to reduce cybersickness in virtual reality. Virtual Real. 24, 645–664. doi:10.1007/s10055-020-00425-x
Fernandes, A. S., and Feiner, S. K. (2016). “Combating VR sickness through subtle dynamic field-of-view modification,”in 2016 IEEE Symposium on 3D User Interfaces (3DUI). Greenville, SC, March 19–20, 2016 (IEEE), 201–210. doi:10.1109/3DUI.2016.7460053
Frisby, J. (1983). Frisby stereotest. Available at: https://www.frisbystereotest.co.uk/ (Accessed October 30, 2024).
Gardé, A., Léger, P.-M., Sénécal, S., Fredette, M., Labonté-Lemoyne, E., Courtemanche, F., et al. (2018). “The effects of a vibro-kinetic multi-sensory experience in passive seated vehicular movement in a virtual reality context,” in Extended Abstracts of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, QC (New York, NY: Association for Computing Machinery), 1–6. doi:10.1145/3170427.3188638
Gavgani, A. M., Walker, F. R., Hodgson, D. M., and Nalivaiko, E. (2018). A comparative study of cybersickness during exposure to virtual reality and “classic” motion sickness: are they different? J. Appl. Physiol. 10, 1670–1680. doi:10.1152/japplphysiol.00338.2018
Gianaros, P. J., Muth, E. R., Mordkoff, J. T., Levine, M. E., and Stern, R. M. (2001). A questionnaire for the assessment of the multiple dimensions of motion sickness. Aviat. Space Environ. Med. 72, 115–119.
Golding, J. F. (2006). Predicting individual differences in motion sickness susceptibility by questionnaire. Personality Individ. Differ. 41, 237–248. doi:10.1016/j.paid.2006.01.012
Gutkovich, Y. E., Lagami, D., Jamison, A., Fonar, Y., and Tal, D. (2022). Galvanic vestibular stimulation as a novel treatment for seasickness. Exp. Brain Res. 240, 429–437. doi:10.1007/s00221-021-06263-w
Harrington, J., Williams, B., and Headleand, C. (2019). “A somatic approach to combating cybersickness utilising airflow feedback,” in Computer graphics and visual computing (CGVC). Editors F. P. Vidal, G. K. L. Tam, and J. C. Roberts (Eindhoven, The Netherlands: The Eurographics Association). doi:10.2312/cgvc.20191256
Howarth, P. A., and Hodder, S. G. (2008). Characteristics of habituation to motion in a virtual environment. Displays 29, 117–123. doi:10.1016/j.displa.2007.09.009
Jang, K.-M., Kwon, M., Nam, S. G., Kim, D., and Lim, H. K. (2022). Estimating objective (eeg) and subjective (ssq) cybersickness in people with susceptibility to motion sickness. Appl. Ergon. 102, 103731. doi:10.1016/j.apergo.2022.103731
Keshavarz, B., Riecke, B. E., Hettinger, L. J., and Campos, J. L. (2015). Vection and visually induced motion sickness: how are they related? Front. Psychol. 6, 472. doi:10.3389/fpsyg.2015.00472
Lamb, S., and Kwok, K. C. (2015). MSSQ-short norms may underestimate highly susceptible individuals: updating the MSSQ-short norms. Hum. factors 57, 622–633. doi:10.1177/0018720814555862
LaViola, J. J. (2000). A discussion of cybersickness in virtual environments. SIGCHI Bull. 32, 47–56. doi:10.1145/333329.333344
McCauley, M. E., and Sharkey, T. J. (1992). Cybersickness: perception of self-motion in virtual environments. Presence Teleoper. Virtual Environ. 1, 311–318. doi:10.1162/pres.1992.1.3.311
McMahan, R. P., Ragan, E. D., Leal, A., Beaton, R. J., and Bowman, D. A. (2011). Considerations for the use of commercial video games in controlled experiments. Entertain. Comput. 2, 3–9. doi:10.1016/j.entcom.2011.03.002
Merriam-Webster (2024). Dyne: merriam-webster.com dictionary. Available at: https://www.merriam-webster.com/dictionary/dyne (Accessed October 30, 2024).
Mittelstaedt, J., Wacker, J., and Stelling, D. (2018). Effects of display type and motion control on cybersickness in a virtual bike simulator. Displays 51, 43–50. doi:10.1016/j.displa.2018.01.002
Mouloua, M., Smither, J., Kennedy, R. C., Kenned, R. S., Compton, D., and Drexler, J. (2004). Visually-induced motion sickness: an experimental investigation. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 48, 2623–2626. doi:10.1177/154193120404802304
Nalivaiko, E., Davis, S. L., Blackmore, K. L., Vakulin, A., and Nesbitt, K. V. (2015). Cybersickness provoked by head-mounted display affects cutaneous vascular tone, heart rate and reaction time. Physiology and Behav. 151, 583–590. doi:10.1016/j.physbeh.2015.08.043
Nesbitt, K., Davis, S., Blackmore, K., and Nalivaiko, E. (2017). Correlating reaction time and nausea measures with traditional measures of cybersickness. Displays 48, 1–8. doi:10.1016/j.displa.2017.01.002
Nesbitt, K., and Nalivaiko, E. (2024). “Cybersickness,” in Encyclopedia of Computer Graphics and Games. Editor N. Lee (Los Angeles, CA: Springer). doi:10.1007/978-3-031-23161-2_252
Palmisano, S., Allison, R. S., and Kim, J. (2020). Cybersickness in head-mounted displays is caused by differences in the user’s virtual and physical head pose. Front. Virtual Real. 1. doi:10.3389/frvir.2020.587698
Pasquier, F., Denise, P., Gauthier, A., Bessot, N., and Quarck, G. (2019). Impact of galvanic vestibular stimulation on anxiety level in young adults. Front. Syst. Neurosci. 13, 14. doi:10.3389/fnsys.2019.00014
Rebenitsch, L., and Owen, C. (2016). Review on cybersickness in applications and visual displays. Virtual Real. 20, 101–125. doi:10.1007/s10055-016-0285-9
Salter, S., Diels, C., Kanarachos, S., Thake, D., Herriotts, P., and Depireux, D. A. (2020). Increased bone conducted vibration reduces motion sickness in automated vehicles. Int. J. Hum. Factors Ergonomics 6, 299–318. doi:10.1504/IJHFE.2019.105358
Smith, S. P., and Burd, E. L. (2019). Response activation and inhibition after exposure to virtual reality. Array 3-4, 100010. doi:10.1016/j.array.2019.100010
Sra, M., Jain, A., and Maes, P. (2019). “Adding proprioceptive feedback to virtual reality experiences using galvanic vestibular stimulation,” in Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems (New York, NY: Association for Computing Machinery), 1–14. doi:10.1145/3290605.3300905
Stanney, K., Lawson, B. D., Rokers, B., Dennison, M., Fidopiastis, C., Stoffregen, T., et al. (2020). Identifying causes of and solutions for cybersickness in immersivetechnology: reformulation of a research and development agenda. Int. J. Human-Computer Interact. 36, 1783–1803. doi:10.1080/10447318.2020.1828535
Stanney, K. M., and Kennedy, R. S. (2009). “Simulation sickness,” in Human factors in simulation and training. Editors P. A. Hancock, D. A. Vincenzi, J. A. Wise, and M. Mouloua (Boca Raton, FL: CRC Press), 117–127.
Stefani, S. P., Serrador, J. M., Breen, P. P., and Camp, A. J. (2020). Impact of galvanic vestibular stimulation-induced stochastic resonance on the output of the vestibular system: a systematic review. Brain Stimul. 13, 533–535. doi:10.1016/j.brs.2020.01.006
Tian, N., Lopes, P., and Boulic, R. (2022). A review of cybersickness in head-mounted displays: raising attention to individual susceptibility. Virtual Real. 26, 1409–1441. doi:10.1007/s10055-022-00638-2
Weech, S., Moon, J., and Troje, N. F. (2018). Influence of bone-conducted vibration on simulator sickness in virtual reality. PLOS ONE 13 (3), e0194137. doi:10.1371/journal.pone.0194137
Wilkinson, D. (2021). Caloric and galvanic vestibular stimulation for the treatment of Parkinson’s disease: rationale and prospects. Expert Rev. Med. Devices 18, 649–655. doi:10.1080/17434440.2021.1935874
Keywords: head-worn display, cybersickness, virtual reality, vestibular stimulation, head-mounted display, VR headset
Citation: Smith SP, Nalivaiko E, Owen S, Depireux D and Flynn M (2025) Exploring vestibular stimulation to reduce the influence of cybersickness on virtual reality experiences. Front. Virtual Real. 5:1478106. doi: 10.3389/frvir.2024.1478106
Received: 09 August 2024; Accepted: 23 December 2024;
Published: 23 January 2025.
Edited by:
Doug A. Bowman, Virginia Tech, United StatesReviewed by:
Thomas A. Stoffregen, University of Minnesota Twin Cities, United StatesCopyright © 2025 Smith, Nalivaiko, Owen, Depireux and Flynn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shamus P. Smith, c2hhbXVzLnNtaXRoQGdyaWZmaXRoLmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.