 Mathias Torp Ernst
Mathias Torp Ernst Jakob Hyldig Nielsen1†‡
Jakob Hyldig Nielsen1†‡ Eik Runge
Eik Runge Stéphane Bouchard
Stéphane Bouchard- 1Center for Digital Psychiatry, Mental Health Services in the Region of Southern Denmark, Odense, Denmark
- 2Department of Clinical Research, University of Southern Denmark, Odense, Denmark
- 3Department of Psychology, University of Southern Denmark, Odense, Denmark
- 4Department of Psychoeducation and Psychology, University du Québec en Outaouais, Gatineau, QC, Canada
- 5Research Center, Integrated Services Center of Health and Social Services of Outaouais, Gatineau, QC, Canada
- 6Copenhagen Research Centre on Mental Health (CORE), Copenhagen University Hospital, Copenhagen, Denmark
- 7Child and Adolescent Mental Health Centre, Mental Health Services – Capital Region of Denmark, Copenhagen, Denmark
Background: A large proportion of individuals with anxiety-related disorders refrain from seeking treatment. This may be because traditional exposure treatments induce anxiety. However, advances in exposure using virtual reality technology may encourage more individuals to seek treatment. Furthermore, using biomarkers with VR-based exposure may enable clinicians to assess anxiety levels objectively and collect data in a naturalistic setting.
Methods:: Here, we conduct a systematic review of the literature on the use of biomarkers in VR-based exposure treatment for anxiety. Twenty-seven studies were included, with a total of 1046 participants.
Results: We found that heart rate was the only biomarker that tentatively could identify changes within (75% of instances) and between sessions (60% of instances). The levels of synchrony between the findings for overall biomarkers and the results from questionnaires showed inconclusive results. Regarding the levels of synchrony between the findings for particular biomarkers and the results from questionnaires, only skin conductance level was highly synchronous for differences between groups (87% of instances).
Conclusion: Based on the present review, biomarkers cannot yet be used reliably to distinguish differences in self-reported symptoms of anxiety in VR-based exposure treatments.
Highlights
- Heart rate and skin conductance level are the most frequently used biomarkers.
- Virtual reality-based exposure with biomarkers is mostly used to treat specific phobias.
- Based on synergy with questionnaires, heart rate can be used to identify changes in anxiety within and between sessions, with moderate success.
- Based on synergy with questionnaires, skin conductance level can be used to identify differences between groups with high success.
- Biomarkers cannot yet be used reliably to distinguish differences in symptoms of anxiety in virtual reality-based exposure treatments.
1 Introduction
1.1 Psychological treatment of anxiety
The gold standard treatment for anxiety is cognitive-behavioral therapy (CBT). Central to CBT is the behavioral component called exposure. Exposure in vivo, facing the fear in a real-life situation, has proved effective (Rodebaugh et al., 2004); however, this may be costly, time-consuming, and could involve situational elements that are difficult to control (Bouchard, 2007; Bouchard et al., 2014). Few individuals with anxiety-related disorders seek treatment or only do so after a long delay (Wang et al., 2005; Stein and Stein, 2008; Bandelow and Michaelis, 2015; Kampmann et al., 2016). Additionally, whereas CBT has a success rate of approximately 70% in research trials (van Dis et al., 2019), the actual success rate is lower because exposure is not used in 70%–80% of cases treated in routine care settings, due to barriers such as practicability and logistical challenges, negative beliefs about exposure and therapist distress (Pittig et al., 2019). To overcome these difficulties, as described thoroughly below, researchers and clinicians have combined exposure with virtual reality (VR) (Bouchard, 2007; Bouchard et al., 2014). Using biomarkers with VR-based exposure may enable clinicians to assess anxiety levels objectively and regulate interventions in real-time (Lindner et al., 2017). This review investigates using biomarkers in VR-based exposure to treat anxiety disorders.
1.2 Virtual reality
VR is defined as the use of computer and behavioral interfaces to simulate the behavior of three-dimensional (3D) entities that interact in real-time with each other and with a user immersed via sensorimotor channels (Fuch et al., 2011). VR content is generally created using 3D computer graphics or 360° videos (Gregg and Tarrier, 2007; Flores-Arredondo and Assad-Kottner, 2015; Stupar-Rutenfrans et al., 2017). Some studies refer to setups displayed on a monitor as VR (Costa et al., 2018). However, such simulations are not included in this review, as they do not include an immersive experience.
VR has been used for clinical assessments (Emmelkamp et al., 2020) and to treat anxiety disorders. Studies have shown that VR may be effective in treating various phobias (e.g., agoraphobia and fear of flying) (Gregg and Tarrier, 2007) and anxiety disorders (Parsons and Rizzo, 2008; Powers and Emmelkamp, 2008; Opris et al., 2012; Morina et al., 2015; Kampmann et al., 2016; Chesham et al., 2018; Carl et al., 2019). A study by Garcia-Palacios et al. (2007) on patients with various anxiety disorders (including specific phobias, claustrophobia, and social anxiety disorder [SAD]) showed that 76% of participants preferred to receive exposure via VR, rather than in vivo (Garcia-Palacios et al., 2007). In addition, exposure via VR has several advantages compared with traditional exposure methods. For example, although VR-based exposure scenarios can be felt as very realistic (Gutierrez-Maldonado et al., 2015), situational factors can be controlled and regulated (Levin et al., 2015). Furthermore, VR-based exposure can occur in the privacy and safety of the psychotherapist’s office (Gutierrez-Maldonado et al., 2015). Additionally, although they know the VR experiences are not real, patients’ minds and bodies respond to the VR experiences as they would to authentic experiences (Freeman et al., 2017). Hence, patients can face challenging situations more easily in VR and may find it easier to adapt their behavior. Furthermore, VR sessions are less expensive, less time-consuming, and can be planned more flexibly than in vivo sessions (Bouchard et al., 2017). However, VR has disadvantages; these include determining costs, hardware dependency, and VR-induced side effects such as cybersickness (Martirosov and Kopecek, 2017).
Some researchers have sought to add biomarkers to augment VR-based exposure treatments. Using biomarkers with VR-based exposure may enable researchers to assess anxiety levels objectively, regulate interventions in real-time, and collect valuable data (Lindner et al., 2017).
1.3 Biomarkers
Anxiety disorders are associated with heightened physiological arousal (Bond et al., 1974; Hoehn-Saric and McLeod, 1988), expressed as elevated muscle tension (Barlow and Ellard, 2018), respiration rate (Wilhelm et al., 2001), skin conductance level (SCL) (Globisch et al., 1999), and heart rate (HR) (Cuthbert et al., 2003), as well as decreased heart rate variability (HRV) (Bandelow et al., 2017). These physiological measures are similar to preferred stress measurements, as they are indicators of the larger response of the Hypothalmic Pituitary Adrenal (HPA) axis and Autonomic Nervous System (ANS) (Dammen et al., 2022) Such biological measures can be referred to as biomarkers. A biomarker is a measurable indicator of a biological state or condition. In a psychiatric context, biomarkers can be used to detect, assess, or predict the development of psychiatric disorders, personality traits, or behavioral characteristics and to evaluate emotional or cognitive capacities (Perez et al., 2014). Furthermore, biomarkers may be used to inform treatment decisions (Perez et al., 2014). Biomarkers that are analyzed at different time points to monitor the status of a disease or medical condition and to provide feedback on the response to an intervention are called monitoring biomarkers (Group, 2016; Garcia-Gutierrez et al., 2020). Behavioral markers may also be considered biomarkers. Examples of behavioral markers include information from trackers attached to the feet, information provided by motion capture technology, body movements that are associated with depression (Alessi and Huang, 2001), changes in tone of voice (Place et al., 2017), and eye-tracking data (Shic, 2016). However, these behavioral markers are not considered biomarkers in this review because they are not direct measures of a biological state or condition.
Biomarkers may also be used to provide biofeedback. Biofeedback is a noninvasive procedure with the operating principle of conscious registration of otherwise unconscious bodily procedures (Gaume et al., 2016). The patient’s physiological outputs (i.e., biomarkers) are detected, monitored, and processed electronically and then returned as feedback in different forms (e.g., visual and auditory) to the same individual (Gaume et al., 2016; Fernández-Álvarez et al., 2020). Thus, positive physiological outcomes (e.g., reduced physiological arousal) may be generated by constant positive feedback (Frank et al., 2010).
Biofeedback has been used for stress reduction (Dillon et al., 2016), facilitating relaxation (Poleszak et al., 2019), and conditioning (Duits et al., 2016), and it has been effective in the treatment of an array of medical and psychological conditions. Anxiety disorders are among the most frequently treated psychiatric conditions (Schoenberg and David, 2014), and HRV biofeedback has proved effective in treating anxiety (Goessl et al., 2017; Fernández-Álvarez et al., 2020). Biofeedback is frequently used for exposure-based therapy. By convention, exposure-based treatment and biofeedback-based interventions take different approaches. Exposure-based treatment focuses on learning principles that range from habituation to inhibitory learning (Craske et al., 2008; Craske et al., 2014) and on achieving extinction of the fear response by facing situations that induce anxiety. Biofeedback-based interventions focus on practicing anxiety regulation skills informed by physiological information concerning the arousal response (Lin et al., 2019). While the term “habituation” often refers to changes in underlying psychological, neurophysiological, and social processes, in this review “habituation” is considered an indicator that fear extinction learning is taking place (Craske et al., 2008).
Although biofeedback has been effective in treating anxiety disorders, some means may be more relevant to VR-based exposure than others, such as those more closely associated with autonomous nervous system activity (Tolin et al., 2020). Clinicians must identify the best methods for combining targeted physiological processes and VR-based exposure (Repetto et al., 2013; Zotev et al., 2013).
1.4 Biomarkers in virtual reality
Combining biomarkers with VR allows researchers to collect data in a controlled setting, facilitates objective anxiety assessments, and means that interventions can be regulated (Lindner et al., 2017). Fernández-Álvarez (2020) noted that VR enables physiological processes to be represented by virtual stimuli. These stimuli are transmitted using biosensors, strengthening user engagement and potentially augmenting the effectiveness of the interventions (Fernández-Álvarez et al., 2020). A range of studies has demonstrated the effectiveness of this approach in healthy and clinical populations (Repetto et al., 2013; Zotev et al., 2013). For example, in a study by Repetto et al. (2013), patients with generalized anxiety disorder (GAD) were treated with VR relaxation simulations in which the environment (a campfire, beach, waterfall, or gazebo) was adapted in real-time by therapists based on HR biofeedback: a reduction in HR reduced the intensity of the stressful stimuli (e.g., fire intensity, wave movement, or stressful image/video).
Combining real-time biofeedback and real-time adaptable VR may facilitate learning relaxation techniques (Repetto et al., 2013; Bossenbroek et al., 2020). For example, in the VR biofeedback game DEEP, players wear a stretch sensor that measures the expansion of the diaphragm associated with breathing: the slower and deeper players breathe, the better they can move around in a VR underwater world (Bossenbroek et al., 2020).
A recent systematic review of randomized controlled trials (RCTs) investigating biofeedback for anxiety disorders found 21 articles eligible of inclusion (Tolin et al., 2020). However, only one of these articles combined VR with biofeedback (Repetto et al., 2013). Few studies have investigated using biofeedback to regulate interventions for anxiety-related disorders (Repetto et al., 2013; Lin et al., 2019). However, more studies have investigated using biomarkers with VR for other purposes, such as assessing treatment effects (Peperkorn et al., 2014; Gujjar et al., 2018; Kaussner et al., 2020).
Results from studies using biomarkers have frequently been compared with results from questionnaires to asses symptom reduction (Tolin et al., 2020). The terms synchrony and desynchrony (Hodgson and Rachman, 1974; Rachman and Hodgson, 1974) refer to the consistency in changes over time between physiological and subjective measures. Findings indicate that questionnaires and biomarkers are not always in synchrony (Craske and Craig, 1984). This inconsistency may be due to psychological factors, such as expectations and attention to bodily sensations, leading to distortions in perceived anxiety (Hoehn-Saric and McLeod, 2000). Furthermore, biomarkers such as HR and respiratory rate often peak and return to their resting state faster than subjective self-report measures (Lande, 1982). Interestingly, increased arousal is associated with greater consistency between questionnaire and biomarker data (Gerew et al., 1989), and greater consistency may also be observed for phobic anxiety (Schaefer et al., 2014).
Combining VR and biomarkers has intriguing and promising potential, allowing for clinical advantages during exposure, such as real-time monitoring and adaption. However, no systematic review has investigated using biomarkers with VR-based exposure to treat anxiety. Here, we investigate synchrony and desynchrony between biomarkers and self-report questionnaires in completed trials.
1.4.1 Objectives
The main objective of this study was to conduct a systematic review of the existing literature addressing the use of biomarkers (not including behavioral markers) in VR-based exposure used to treat anxiety in adults.
To attain this goal, we defined the following secondary aims.
1. Which biomarkers are used in VR-based exposure?
2. For which anxiety-related diagnoses are biomarkers used in VR-based exposure?
3. What function(s) can biomarkers have in VR-based exposure?
4. Can biomarkers identify expected:
a) Differences between groups
b) Changes within sessions
c) Changes between sessions
5. Are findings obtained from biomarkers synchronous with findings obtained from questionnaires in terms of identification of:
a) Differences between groups
b) Changes within sessions
c) Changes between sessions
The report was written in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Moher et al., 2009).
2 Methods
The protocol for this systematic review was registered at The International Prospective Register of Systematic Reviews (PROSPERO registration number: CRD42020186826).
2.1 Search strategies
Journal articles were identified using searches in the scientific databases PubMed PMC, PsychInfo (Ovid), and the Cochrane Library. Potential cross-references were sought; however, this yielded no additional studies for screening. Search criteria included all publications from the Diagnostic and Statistical Manual of Mental Disorders-IV released in 1994 until 2 October 2023. The search strategy was the same for each database and involved searching for the following keywords in the title and abstract: “virtual reality” AND (“galvanic skin response” OR “heart rate” OR “biofeedback” OR “biometric*" OR “biomarker*" OR “EEG” OR “eye tracking” OR “physiological”) AND “exposure” AND (“anxiety” OR "*phobia” OR “posttraumatic stress disorder” OR “ptsd” OR “obsessive compulsive disorder” OR “ocd”) AND “adult".
2.2 Study selection
Studies published in peer-reviewed journals were included if the following criteria were met: 1) written in English, 2) only included participants aged 18 years or older, 3) included participants diagnosed with an anxiety-related disorder, based on DSM-IV (American Psychiatric Association, 1994) or DSM-V criteria (American Psychiatric Association, 2013), 4) included exposure to anxiety by using VR in at least one arm of the study, 5) included therapy with the intention of reducing symptoms of anxiety, 6) included at least one biomarker, and 7) included immersive VR equipment (e.g., HMDs) with immersive properties. Meta-analyses, reviews, single-case studies, and study protocols were excluded.
The initial search of titles and abstracts yielded 2,292 results in Pubmed PMC, 39 results in PsychInfo (OVID), and 78 results in the Cochrane Library, totaling 2,409 studies. Next, 12 duplicates were identified and removed, leaving 2,397 abstracts for screening. Reference manager (Thomson Reuters, Toronto, ON, Canada), Mendeley (London, UK), and Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) were all used to identify duplicates and review the articles. Titles and abstracts were independently reviewed by two authors (MTE and ER) and coded as to whether they met the inclusion criteria. Disagreements were resolved by discussion until a consensus was reached or were decided by the senior author. After the initial screening of abstracts, 53 studies remained. Full-text articles were obtained for these abstracts, and all were independently reviewed by two authors (MTE and ER). Of the 53 articles selected for full-text review, 27 articles (Gujjar et al., 2019; Shiban et al., 2017; Shiban et al., 2015; Diemer et al., 2013; Malbos E et al., 2013; Donahue et al., 2009; Norrholm et al., 2016; Levy et al., 2016; de Quervain et al., 2011; Cote and Bouchard, 2005; Wiederhold et al., 2002; Tardif et al., 2019; Hur et al., 2021; Kaussner et al., 2020; Loucks et al., 2019; Mühlberger et al., 2001; Borghese et al., 2022; Diemer et al., 2023; Gramlich et al., 2021; Hong et al., 2017; Premkumar et al., 2021; van ’t Wout-Frank et al., 2019; Wechsler et al., 2021; McGlade et al., 2023; McInerney et al., 2021; Price et al., 2015; Reitmaier et al., 2022), representing 1046 participants, were retained for final inclusion (Figure 1).
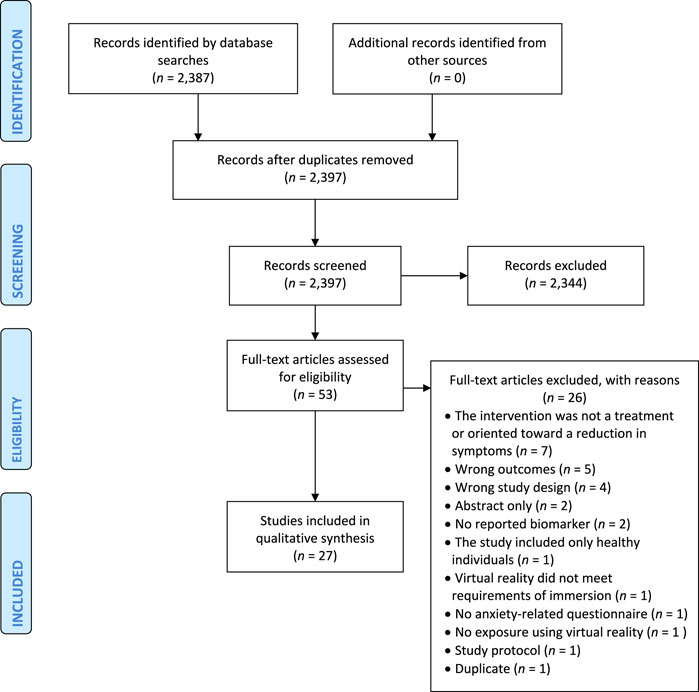
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
2.3 Risk of bias
Two assessment tools were utilized to evaluate Risk of Bias (RoB). For RCTs, the Cochrane tool for RoB in RCTs (Higgins et al., 2011), which categorizes RoB into three groups (High, Low, and Unclear), was used. For cohort studies, the Newcastle–Ottawa Assessment Scale (Stang, 2010), which categorizes each study into one of three groups (Good quality, Fair quality, or Poor quality), was used. The RoB assessment was carried out by three authors (MTE, JHN, and ER), and any disagreement was resolved by the senior author (LC). The scoring groups for the cohort studies and the RCTs were combined in an overall RoB assessment. RoB for each study is shown in Figure 2 and Table 1.
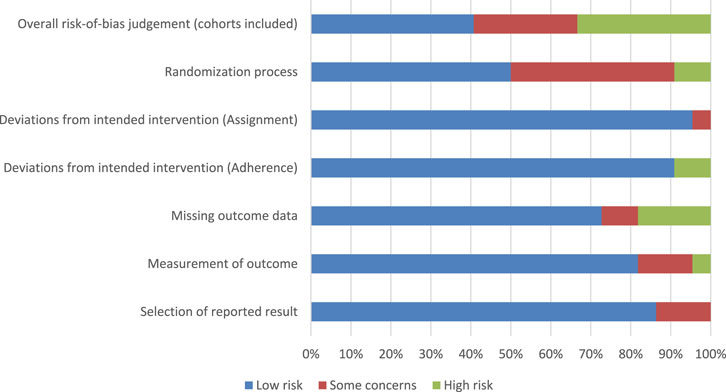
Figure 2. Risk of bias summary.
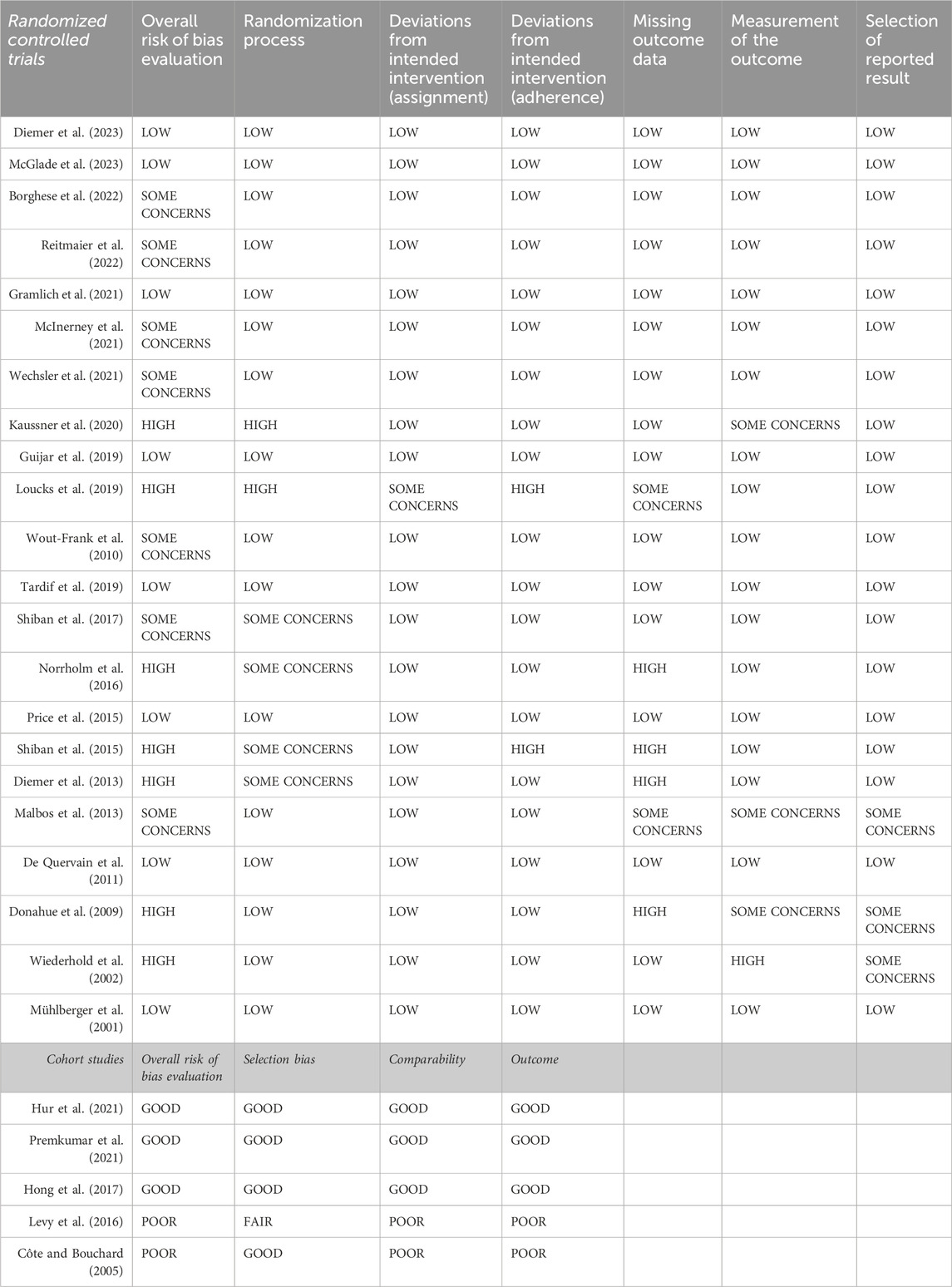
Table 1. “Risk of bias”.
2.4 Data extraction and items
The following data were retrieved from the included studies: authors, publication year, number of participants, gender distribution, age, anxiety-related diagnosis, study design, biomarkers, time of biomarker measurement, anxiety-related questionnaires, and function of biomarkers. In this review, “over time” includes data collected for a single session as well as data collected at several time points within a single session.
Data on identification of group differences and changes within and between sessions were retrieved for both biomarkers and questionnaires. Group differences were defined as differences in score at a particular point in time, if these data were available, and reported as significant or non-significant. Changes within or between sessions were categorized as significant increases, significant decreases, or not significant.
Furthermore, synchrony between biomarkers and questionnaires was assessed. Findings were considered synchronous if both biomarkers and questionnaires showed a significant increase, a significant decrease, or no significant change. The findings were considered synchronous if a particular biomarker and at least one questionnaire exhibited similar results. When summarizing the synchrony over several studies, “levels of synchrony” is descriptively used as instances of positive biomarker detection as a percentage of the total number of instances. The authors agreed upon the following definition of synchrony levels: Low levels of synchrony were categorized as <30%, moderate levels of synchrony as 30%–80%, and high levels of synchrony as >80%.
Data were extracted independently by three authors (MTE, JHN, and ER) using a predefined information sheet. Any discrepancies were resolved by discussion and consultation with the senior author until a consensus was reached.
3 Results
Table 1 and Figure 2 show that the overall RoB in the studies was high because nine studies were scored “High” and seven studies were scored “Some concerns.” These ratings were mainly due to randomization processes and missing outcome data.
3.1 Characteristics of studies
The 27 studies included a total of 1046 participants with a mean sample size of 38.7 (range, 6–116). Differences in sample sizes across studies were not considered; thus, each study was given equal weight. The majority of participants were female (59.1%), ranging from 0% to 96% (based on 26 studies), and the (weighted) mean age was 32.9 years (range of mean age, 20.6–44.5 years).
Six studies were on social anxiety disorder (SAD), five on post-traumatic stress disorder (PTSD), five on arachnophobia, five on acrophobia, three on aviophobia, one on dental phobia, one on agoraphobia, and one study was on driving phobia. Twenty-three of the studies were RCTs, and five were cohort studies. Sixteen studies had follow-up assessments, and the follow-up periods ranged from 0.5 to 12 months (Table 2).

Table 2. Characteristics of studies.
Table 3 shows that all 27 studies used biomarkers as outcome measures. Thirteen of the studies (Gujjar et al., 2019; Shiban et al., 2017; Shiban et al., 2015; Diemer et al., 2013; Malbos E et al., 2013; Donahue et al., 2009; Kaussner et al., 2020; McGlade et al., 2023; Borghese et al., 2022; Reitmaier et al., 2022; Gramlich et al., 2021; Premkumar et al., 2021; van ’t Wout-Frank et al., 2019) also used biomarkers as measures of inter-session or intra-session habituation. These thirteen studies measured physiological responses at the beginning and/or during the exposure and/or at the end of each exposure session, or they measured changes in physiological responses between specific scenarios during the exposure. The changes were compared with subjective measurements to determine whether anxiety levels had decreased and habituation had occurred. Only two studies provided participants with visual feedback, based on physiological responses, during the exposure in VR (Wiederhold et al., 2002; Hong et al., 2017). None of the studies used biomarkers to automatically and/or dynamically adapt VR-based exposure via computer algorithms.
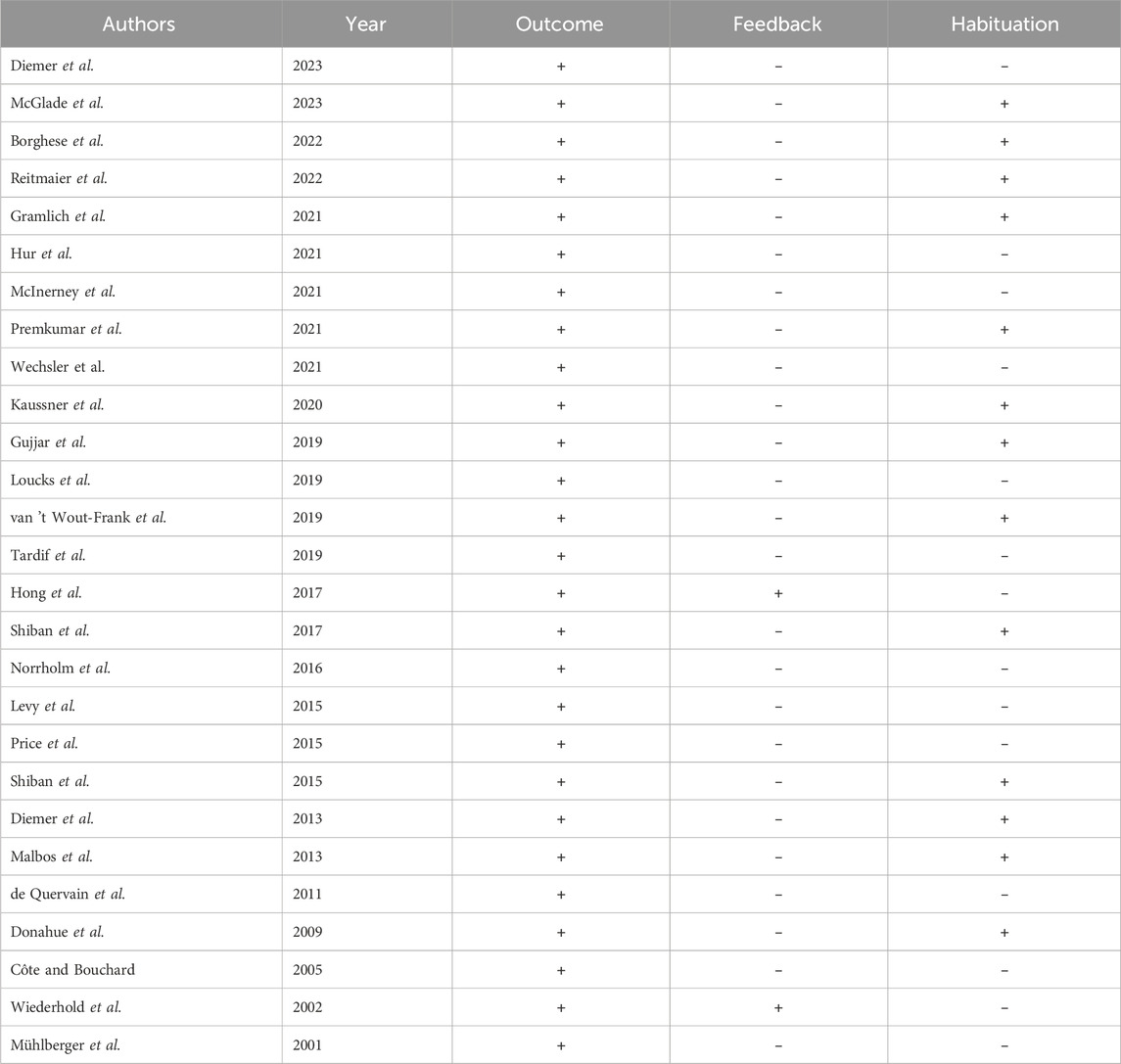
Table 3. Function of the biomarkers.
Biomarkers were applied in a total of 94 instances across all the studies (Table 4). These included 40 instances of HR, 33 instances of SCL, four instances of HRV, four instances of startle response, three instances of systolic blood pressure (SBP), three instances of diastolic blood pressure (DBP), three instances of peripheral skin temperature (SKT), two instances of functional magnetic resonance imaging (fMRI), and two instances of cortisol levels. In this review, the term “instance” refers to an occasion on which a measurement was used; for example, in the study by Donahue et al. (2009), HR data were collected for group differences, as well as within sessions and between sessions, totaling three instances of HR use.
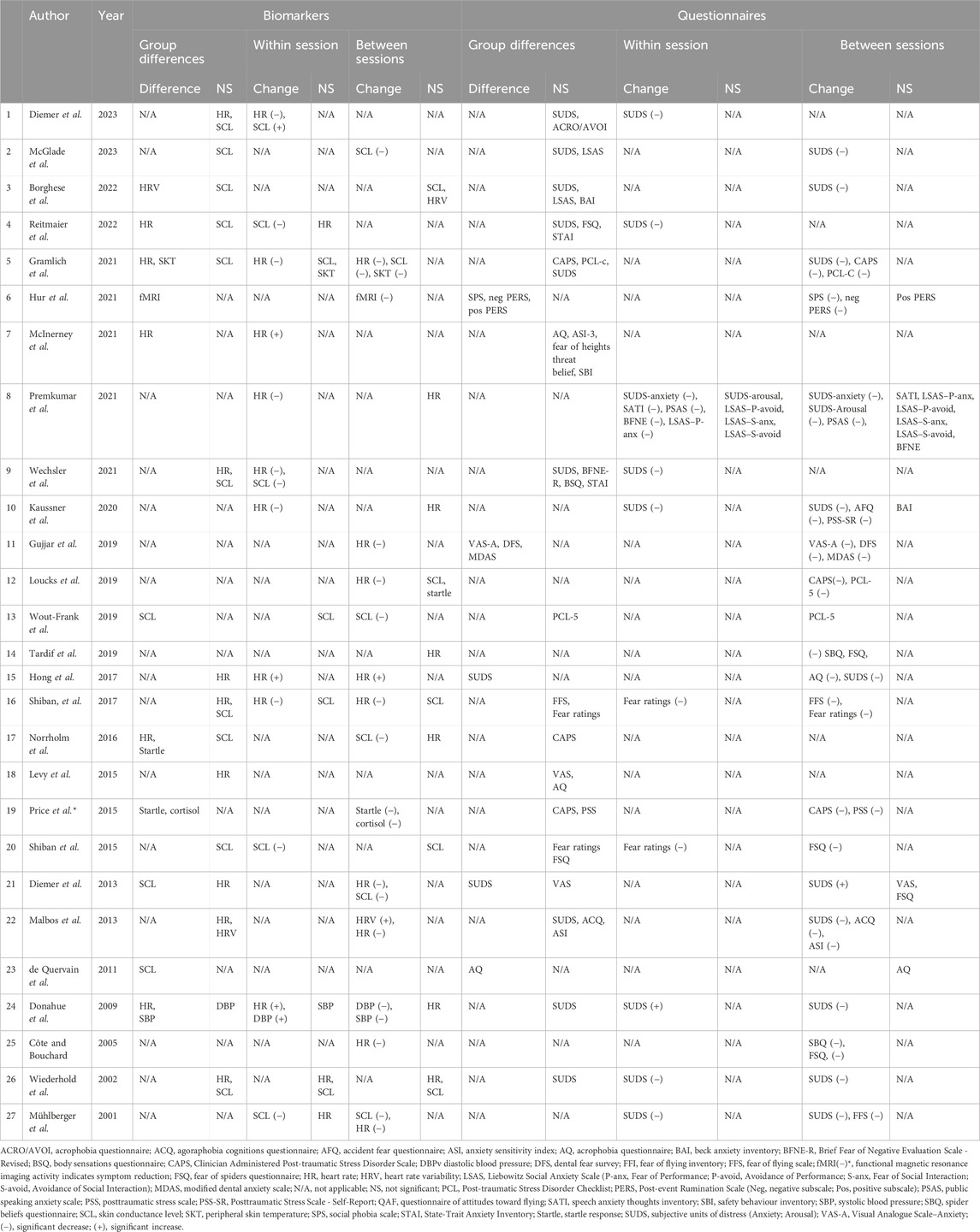
Table 4. Detection of differences between groups and changes within and between sessions by biomarkers and questionnaires.
Table 4 shows that HR was the most frequently used biomarker, and HR was reported in 20 of the 27 studies. The next most frequently used biomarker was SCL, which was reported in 15 studies. Only two studies did not use HR or SCL. Eight studies used other biomarkers. Two studies used HRV, two used the startle response, one used SBP and DBP, one used fMRI, one used peripheral skin temperature, and one used cortisol levels. Several studies measured more than one biomarker, and there were a total of 94 instances of biomarker investigation across the 27 studies (Table 4).
Biomarkers identified 15 significant differences among 35 instances that investigated group differences. Biomarkers identified 15 changes within sessions from a total of 24 instances investigated and 24 instances of changes between sessions from a total of 35 instances investigated. Biomarkers were used in 21 studies to investigate changes between sessions. Of these, 15 studies reported significant differences for at least one biomarker.
Regarding specific biomarkers, HR identified group differences in 5 of 13 instances investigated (38%), and SCL identified group differences in 3 of 13 instances investigated (23%). Moreover, HR identified changes within sessions in 9 of 12 instances investigated (75%), and SCL identified changes within sessions in 5 of 9 instances investigated (56%). Finally, HR identified changes between sessions in 9 of 15 instances investigated (60%), and SCL identified changes between sessions in 6 of 11 instances investigated (55%; Table 5).
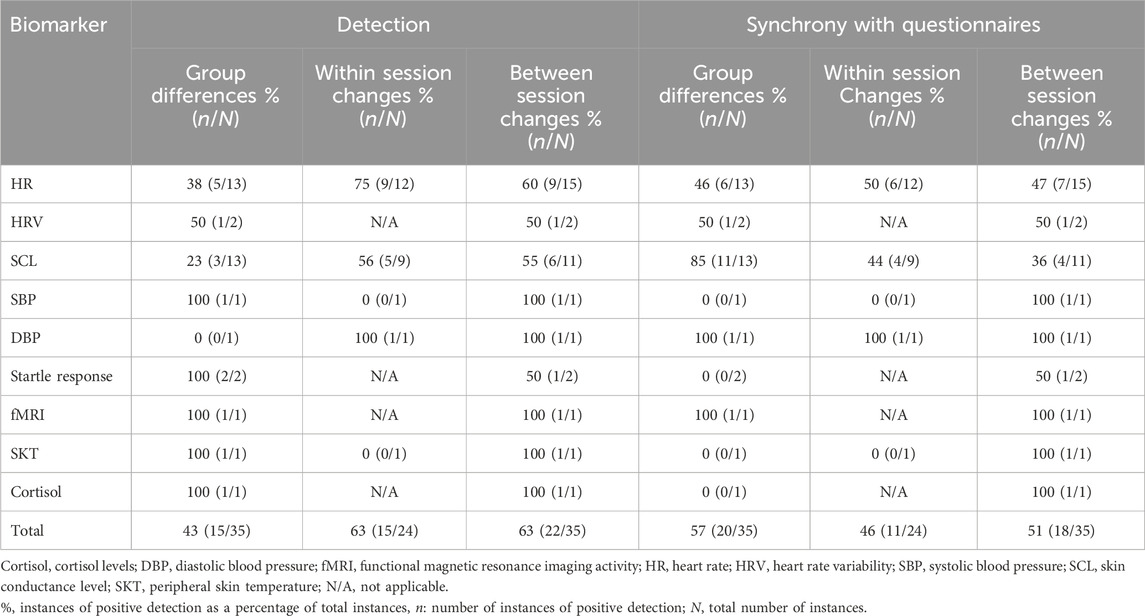
Table 5. Positive detection with biomarkers and synchrony between the findings for biomarkers and the results from questionnaires.
Table 5 shows that the findings for biomarkers were synchronous with the results from questionnaires in 20 of 35 instances for group differences (57%), 11 of 24 instances for changes within sessions (46%), and 18 of 35 instances for changes between sessions (51%). For group differences, the findings for HR were synchronous with the results from questionnaires in 6 of 13 instances (46%), and the findings for SCL were synchronous with the results from questionnaires in 11 of 13 instances (85%). For changes within sessions, the findings for HR were synchronous with the results from questionnaires in 6 of 12 instances (50%), and the findings for SCL were synchronous with the results from questionnaires in 4 of 9 instances (44%). For changes between sessions, the findings for HR were synchronous with the results from questionnaires in 7 of 15 instances (47%), and the findings for SCL were synchronous with the results from questionnaires in 4 of 11 instances (36%).
4 Discussion
This systematic review analyzed the literature on the use of biomarkers in VR-based exposure treatment for anxiety in adults. As a means of investigating this, five secondary aims were defined. In the following discussion, findings regarding the secondary aims are discussed.
The first secondary aim concerned the biomarkers that were used. We identified a limited number of biomarkers used in VR-based exposure treatments, with a total of 94 instances across the 27 studies. HR was the most frequently used biomarker (40 instances), and SCL was the next most frequently used biomarker (33 instances). The other much less frequently used biomarkers included HRV, SBP, DBP, startle response, fMRI, SKT and cortisol levels. Elevated HR and SCL are among anxiety disorders’ most common physiological symptoms (Tolin et al., 2020), which could explain the frequent use of these biomarkers in VR-based exposure. Furthermore, HR is a sensitive measure of anxiety (Wilhelm and Roth, 1998; Alpers et al., 2005), and both HR and SCL are noninvasive biomarkers that are easy to use and do not interfere with VR-based exposure.
The second secondary aim concerned the diagnoses investigated. We found that biomarkers were most commonly used in studies that investigated specific phobias (15 of 27). This domain consisted of five studies on arachnophobia and acrophobia respectively, three studies on aviophobia, one on dental phobia, and one on driving phobia. Additionally, there were six studies on social anxiety disorder, five on PTSD and one on agoraphobia. Specific phobias were frequently addressed in these VR-based exposure studies, possibly due to the particular situations that induce fear in these cases. Such fear stimuli may be easier to simulate in VR than disorders such as GAD or illness anxiety disorder, which rely on abstract anxiety-related stimuli. Furthermore, biomarkers may be relatively easy to use with specific phobias because perceptual, especially visual, cues are processed rapidly and with high specificity and result in characteristic activation patterns in the sympathetic nervous system (Peperkorn et al., 2014). HR and SCL are also among the most frequently used biomarkers for measuring sympathetic nervous system activity (Tolin et al., 2020). Finally, biomarkers show little response to peripheral threats unrelated to the specific phobia (e.g., laboratory settings). This makes it easier to isolate biomarker activity (Hoehn-Saric and McLeod, 1988).
The third secondary aim concerned the function of biomarkers. All of the included studies used the biomarkers as outcome measures, but few studies used these biomarkers to measure primary outcomes. The use of these biomarkers as outcome measures in VR is probably analogous to their use in monitoring similar responses in non-VR settings. Biomarkers are more likely to be used in novel settings if they have been validated as reliable measures of the outcome of interest. In total, 13 of the 27 studies also used biomarkers to measure habituation, either within or between sessions. Habituation is an important goal of exposure in CBT (Benito and Walther, 2015) and is strongly associated with autonomic nervous system activation (Craske et al., 2008), which is linked to HR and SCL (Pohjavaara et al., 2003). Finally, one study provided participants with biofeedback and found that the group receiving visual biofeedback was more capable of decreasing their arousal and anxiety compared to the group that received no visual biofeedback (Wiederhold et al., 2002). Although no unequivocal conclusions can be drawn from a single study, this observation is consistent with non-VR studies that indicate biofeedback may be used to improve treatment outcomes by training patients to reduce physiological reactivity (e.g., SCL or HRV), thereby decreasing autonomic arousal and anxiety (Goessl et al., 2017; Tolin et al., 2020).
The lack of studies investigating the use of biomarkers to automatically adapt the VR experience may be due to the difficulty of adapting exposure based on feedback from biomarkers. First, some biomarkers may not reflect the subjective experience of anxiety within sessions for every patient, as shown in this review. Second, the response by the VR environment may not align with each patient’s idiosyncrasies regarding their specific disorder. For example, a patient with SAD may or may not feel a decrease in anxiety as the VR environment adapts to reduce the amount of social interaction required. Furthermore, the patient may or may not experience decreased anxiety when virtual agents are removed or added. Finally, not all investigators may be interested in decreasing physiological arousal, but rather, in building tolerance towards negative emotional states, and thus, would not benefit from an adaptive experience.
The fourth secondary aim was to determine if biomarkers could identify differences between groups and changes within and between sessions. Differences between groups were found in less than half of the instances across all biomarkers. This may be due to differences in design and expected outcomes. Indeed, some studies did not expect differences in biomarker activity between groups, e.g., Malbos E et al. (2013), whereas others intentionally aimed to initiate different biomarker activity between groups, e.g., McInerney et al. (2021). Regarding within session and between session changes, overall biomarkers were able to detect changes for almost two-thirds of the instances.
The two most frequently used biomarkers (HR and SCL) showed comparable ability to detect changes between sessions–however, while SCL was able to detect within session changes in approximately half of the instances, HR was able to do so in the majority of instances (75%).
A challenge for SCL anxiety detection may be partly due to its’ sensitivity to novel inputs (Shiban et al., 2017). Thus, for SCL to change significantly between sessions, the degree of novelty in exposure may have to be low. For example, in a study that involved exposure trials for aviophobia, researchers found no significant change in SCL between sessions (Shiban et al., 2017). The researchers hypothesized that the repeated use of novel stimuli (e.g., acceleration, deceleration, and initial turbulence) may have impeded habituation; thus, SCL remained constant. However, by the third trial, SCL no longer responded to turbulence, indicating desensitization to this stimulus. Further, the same argument may be applied in lack of within session habituation in single-session exposure studies–such as the included paper by Diemer et al. (2023) on acrophobia, where patients were gradually exposed to increasingly difficult novel situations, where only reduction in SUDS and HR was found, but not in SCL.
In general, these findings indicate that biomarkers may be used with moderate success to identify differences between groups, within sessions, and between sessions.
The fifth secondary aim concerned the synchrony between the findings for biomarkers and the results from questionnaires to validate the biomarkers used.
Both high and low levels of synchrony were found between the findings for biomarkers and the results from questionnaires. In cases of low levels of synchrony, these may reflect the inadequacy of biomarkers as accurate measures of anxiety. Alternatively, this may be due to differences that are not entirely understood between responses on questionnaires and responses by biomarkers. Factors influencing the synchrony between physiological responses associated with anxiety and the results from questionnaires remain poorly understood (Hoehn-Saric and McLeod, 2000). The timing of measurements may also influence whether the findings for biomarkers and the results from questionnaires are synchronous. HR reaches a peak and returns to its resting state more rapidly than the subjective measurements that are self-reported on a questionnaire (Schaefer et al., 2014). In addition, there is greater synchrony between the findings for biomarkers and the results from questionnaires when physiological arousal is increased (Gerew et al., 1989). Furthermore, higher levels of synchrony may be associated with specific phobias (Schaefer et al., 2014). Finally, differences in self-report measurements may be due to demand characteristics rather than actual effects. The lack of significant changes in biomarker levels may be the actual result of VR-based exposure therapy.
4.1 Strengths and limitations
This review has several strengths. The literature search was exhaustive; therefore, our conclusions are based on a comprehensive assessment of the work published within this research field. In addition, the majority of the studies that were included were RCTs. The rating process was thorough, with several researchers providing independent ratings before reaching a consensus. The studies were homogeneous regarding VR content (render-based content) and publication year, with all studies being published within the last 23 years.
However, the review also has limitations. While studies were homogenous in terms of VR content, the quality of included content may vary significantly between studies due to content development design choices and resources, and technology development throughout the years. Indeed, HMD and computing capabilities have increased since the earliest included studies, however, even the earliest included studies were able to detect differences in biomarkers and subjective measurements. Changes in biomarker levels were not the primary outcomes of most of these studies, and the findings described in this review were not always reported in a suitable format by the authors of the studies that were included, resulting in variations in the quality and quantity of data that could be used to address our secondary aims. This is particularly true for the findings for biomarkers that were used to assess changes within sessions, which are based on a total of only 24 of 94 instances. Furthermore, because there is no consensus on standard practice for collecting SCL data, the included studies applied different approaches, which may have influenced our analyses. Additionally, few of the included studies focused on comparing the findings for biomarkers with the results from questionnaires, and many of the studies did not report concurrent measures for biomarkers and questionnaires. Except for HR and SCL, few biomarkers were comprehensively assessed; therefore, conclusions regarding other biomarkers are relatively weak. We did not differentiate between experimental tasks, which may vary widely based on diagnosis and scope. Tasks including a higher degree of movement may have affected biomarker outcomes, as these are commonly sensitive to movement.
Using the results from questionnaires to validate findings for biomarkers has limitations. As described above, previous studies (Craske and Craig, 1984) have reported low levels of synchrony between the findings for biomarkers and the results from questionnaires. Furthermore, using more than one questionnaire may generate conflicting results, with only some results agreeing with the findings for biomarkers. Although all questionnaires assessed anxiety levels, some focused on the subjective symptoms of anxiety rather than the physiological symptoms of anxiety that are most closely linked to biomarkers.
A majority of the participants were female (59.1%). However, this observation is consistent with the lifetime prevalence of anxiety among the general population, which is also higher among females (33%) than among males (22%) (McLean et al., 2011). The mean age range was narrow (approximately 21–44 years), perhaps reflecting the recruitment strategies used. Thirteen studies reported their recruitment procedures (Wiederhold et al., 2002; Cote and Bouchard, 2005; Donahue et al., 2009; de Quervain et al., 2011; Diemer et al., 2013; Shiban et al., 2015; Hong et al., 2017; Shiban et al., 2017; McInerney et al., 2021; Premkumar et al., 2021; Wechsler et al., 2021; Borghese et al., 2022; Diemer et al., 2023). These studies mainly used public advertisements for recruitment, and seven of the 13 used advertisements at universities, schools, and colleges, which might explain the narrow mean age range. Younger adults may exhibit more technological literacy than older adults, which may result in younger adults being more likely to participate in relevant research, including research involving VR. Therefore, we may find it more difficult to obtain data on older adults’ psychological reactions to VR-based exposure. One non-VR study found that older adults reacted more calmly than younger adults when anxiety was induced unless a physical threat was involved (Teachman and Gordon, 2009). However, whether older adults react more calmly than younger adults to VR-based exposure is not known.
Finally, our risk of bias assessment showed a “high risk” tendency in one-third of the studies, mainly due to missing outcome data. This could compromise our findings because it is unclear whether the missing data are linked to particular anxiety levels or perhaps to publication bias. Thus, it is uncertain whether particular findings are valid or are influenced by the quality of studies or other confounding variables.
4.2 Implications and future research
Based on the findings of this review, we cannot provide strong recommendations regarding the use of monitoring biomarkers in clinical practice. However, we can present recommendations for further research based on theoretical and logical considerations and implications.
In this review, we did not differentiate among diagnoses. Therefore, our findings provide valuable information across diagnoses. However, there may be diagnostic differences in the physiological reactions to exposure, or there may be particular diagnoses for which the physiological reactions are particularly sensitive to treatment. Variations in the response of particular biomarkers may be associated with particular anxiety disorders. For example, individuals with phobic anxiety exhibit an increased HR in response to phobic imagery compared with control imagery; this response is greatest for simple phobias, intermediate for SAD, and smallest for agoraphobia (Cook et al., 1988; Hoehn-Saric and McLeod, 2000). Furthermore, baseline differences in HRV have been reported for panic disorder, GAD, and SAD (Pittig et al., 2013). Finally, whereas individuals with anxiety show decreased HRV, no significant decrease in HRV is observed among individuals with obsessive-compulsive disorder (Chalmers et al., 2014). Thus, important physiological differences exist among diagnoses. In the future, VR will be used more widely, and biometric data will be available for more diagnoses. Therefore, understanding the data associated with different diagnoses may enable clinicians to provide the most appropriate treatments.
Frequently used biomarkers, such as HR and SCL, may provide valuable information concerning anxiety levels experienced by patients. However, they do not provide the critical information necessary to decide how to proceed during exposure. Indeed, arousal plays a small role in assessing the optimal rate of progression for exposure. Arousal is essentially an indicator that emotional processing and inhibitory learning are occurring, but it is a poor predictor of outcomes (Craske et al., 2014). Therefore, clinicians should consider collecting data from other biomarkers, such as electroencephalography (EEG) and body temperature, as well as subtle behavioral markers such as voice tone or pitch, facial muscle contractions, and behavioral avoidance patterns. Information from several biomarkers may be needed to draw meaningful conclusions. Whereas individual biomarkers may show low levels of synchrony with questionnaires, combining several biomarkers may increase levels of synchrony. Biomarkers have different characteristics. For example, SCL is particularly sensitive to novel inputs and is associated with the sympathetic nervous system, whereas HR may be used as a biomarker for diverse diagnoses (Craske et al., 2014). Combining several biomarkers may provide a better indication of the anxiety levels actually experienced by sampling diverse patterns of sympathetic nervous system activity. Furthermore, different individuals may react differently across modalities: some may react primarily by exhibiting changes in SCL, whereas others may exhibit changes in cardiovascular activity. Additionally, some individuals may exhibit low SCL when faced with severe anxiety. Therefore, using several modalities can avoid the pitfall of relying on unsuitable markers. Future studies should identify information that most accurately reflects anxiety states and changes and how to use this information most effectively.
Our review suggests that procedures that involve real-time monitoring of biomarkers are associated with low validity in VR-based exposure therapy. However, real-time application of biomarkers during therapy may provide clinicians with insight and inform decision-making, or it may be used as a tool for post-exposure functional analyses. Indeed, one novel approach has involved using biomarkers during therapy sessions to inform therapists and provide a basis for developing artificial intelligence systems that can automate treatment and replace human therapists (Rizzo and Bouchard, 2019; Šalkevicius et al., 2019). This research has the potential to improve therapy by providing detailed guidance for therapists, as well as by enhancing patient interoception and self-regulation. Information may be provided by personalized virtual or conversational agents. Personalized conversational agents (i.e., a virtual character that patients can modify and engage with in verbal conversations) can increase motivation and commitment to psychotherapy (Briskilal.J et al., 2020). These agents may be adjusted by real-time biomarker data and artificial intelligence technology to improve the effectiveness of guidance and therapy, providing valuable information to patients and clinicians. Moreover, such agents may eventually be implemented in everyday practice to bridge the gap between innovative research and the practitioner’s office.
5 Conclusions
The objective of this study was to comprehensively review the literature on the use of biomarkers in VR-based exposure treatment of anxiety disorders. We included 27 studies with a total of 1046 participants. HR and SCL were the most frequently used biomarkers. Over half of the studies included on anxiety-related diagnoses focused on specific phobias. This may be because VR is particularly suitable for simulating stimuli that induce fear compared with abstract stimuli. All of the studies used biomarkers as outcome measures, although these were generally secondary outcomes. In total, thirteen of the 27 studies used biomarkers to measure habituation. Only two studies used biomarkers to provide participants with biofeedback.
HR measurements may be used tentatively to identify changes in anxiety within and between sessions. SCL may be able to identify differences between groups. In conclusion, biomarkers cannot yet be used reliably to distinguish differences in symptoms of anxiety in VR-based exposure treatments.
Author contributions
ME: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Writing–original draft, Writing–review and editing, Investigation. JH: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing–original draft, Writing–review and editing. ER: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing–original draft, Writing–review and editing. SB: Conceptualization, Methodology, Supervision, Visualization, Writing–original draft. LC: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Visualization, Writing–original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank Pia Veldt Larsen for statistical advice.
Conflict of interest
SB is president and owner of Clinique et Development In Virtuo, a spin-off company from his university that distributes virtual environments. The terms and arrangements for this spin-off have been reviewed and approved by the Université du Québec en Outaouais in accordance with its Conflict of Interest policies. He also receives honoraria from conferences, workshops and books.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alessi, N. E., and Huang, M. P. (2001). Digital motion phenomenology of depression. Stud. Health Technol. Inf. 81, 30–37. doi:10.3233/978-1-60750-925-7-30
Alpers, G. W., Wilhelm, F. H., and Roth, W. T. (2005). Psychophysiological assessment during exposure in driving phobic patients. J. Abnorm Psychol. 114, 126–139. doi:10.1037/0021-843X.114.1.126
AMERICAN PSYCHIATRIC ASSOCIATION (1994) Diagnostic and statistical manual of mental disorders: dsm-IV. Washington, DC: American psychiatric association.
AMERICAN PSYCHIATRIC ASSOCIATION (2013) Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American psychiatric association.
Bandelow, B., Baldwin, D., Abelli, M., Bolea-Alamanac, B., Bourin, M., Chamberlain, S. R., et al. (2017). Biological markers for anxiety disorders, OCD and PTSD: a consensus statement. Part II: neurochemistry, neurophysiology and neurocognition. World J. Biol. Psychiatry 18, 162–214. doi:10.1080/15622975.2016.1190867
Bandelow, B., and Michaelis, S. (2015). Epidemiology of anxiety disorders in the 21st century. Dialogues Clin. Neurosci. 17, 327–335. doi:10.31887/dcns.2015.17.3/bbandelow
Benito, K. G., and Walther, M. (2015). Therapeutic process during exposure: habituation model. J. Obsessive Compuls. Relat. Disord. 6, 147–157. doi:10.1016/j.jocrd.2015.01.006
Bond, A. J., James, D. C., and Lader, M. H. (1974). Physiological and psychological measures in anxious patients. Psychol. Med. 4, 364–373. doi:10.1017/s0033291700045803
Borghese, F., Henckaerts, P., Guy, F., Mayo, C., Delplanque, S., Schwartz, S., et al. (2022). Targeted Memory Reactivation during REM sleep: implications in the treatment of social anxiety disorder. Sleep. Med. 100, S39–S40. doi:10.1016/j.sleep.2022.05.120
Bossenbroek, R., Wols, A., Weerdmeester, J., Lichtwarck-Aschoff, A., Granic, I., and Van Rooij, M. (2020). Efficacy of a virtual reality biofeedback game (DEEP) to reduce anxiety and disruptive classroom behavior: single-case study. JMIR Ment. Health 7, e16066. doi:10.2196/16066
Bouchard, S., Côté, S., and Richard, D. C. (2007). “Virtual reality applications for exposure,” in Handbook of exposure therapies.
Bouchard, S., Dumoulin, S., Robillard, G., Guitard, T., Klinger, E., Forget, H., et al. (2017). Virtual reality compared with in vivo exposure in the treatment of social anxiety disorder: a three-arm randomised controlled trial. Br. J. Psychiatry 210, 276–283. doi:10.1192/bjp.bp.116.184234
Bouchard, S., Wiederhold, B. K., and Bossé, J. (2014) Advances in virtual reality and anxiety disorders.
Briskilal, J., Ashwin, SINGH, and Ojha, D. (2020). My therapist: a cognitive approach towards natural language processing. Int. J. Adv. Sci. Technol. 29, 12.
Carl, E., Stein, A. T., Levihn-Coon, A., Pogue, J. R., Rothbaum, B., Emmelkamp, P., et al. (2019). Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J. Anxiety Disord. 61, 27–36. doi:10.1016/j.janxdis.2018.08.003
Chalmers, J. A., Quintana, D. S., Abbott, M. J., and Kemp, A. H. (2014). Anxiety disorders are associated with reduced heart rate variability: a meta-analysis. Front. Psychiatry 5, 80. doi:10.3389/fpsyt.2014.00080
Chesham, R. K., Malouff, J. M., and Schutte, N. S. (2018). Meta-Analysis of the efficacy of virtual reality exposure therapy for social anxiety. Behav. Change 1. doi:10.1017/bec.2018.15
Cook, E. W., Melamed, B. G., Cuthbert, B. N., Mcneil, D. W., and Lang, P. J. (1988). Emotional imagery and the differential diagnosis of anxiety. J. Consult Clin. Psychol. 56, 734–740. doi:10.1037//0022-006x.56.5.734
Costa, R. T. D., Carvalho, M. R., Ribeiro, P., and Nardi, A. E. (2018). Virtual reality exposure therapy for fear of driving: analysis of clinical characteristics, physiological response, and sense of presence. Braz J. Psychiatry 40, 192–199. doi:10.1590/1516-4446-2017-2270
Cote, S., and Bouchard, S. (2005). Documenting the efficacy of virtual reality exposure with psychophysiological and information processing measures. Appl. Psychophysiol. Biofeedback 30, 217–232. doi:10.1007/s10484-005-6379-x
Craske, M. G., and Craig, K. D. (1984). Musical performance anxiety: the three-systems model and selfefficacy theory. Behav. Res. Ther. 22, 267–280. doi:10.1016/0005-7967(84)90007-x
Craske, M. G., Kircanski, K., Zelikowsky, M., Mystkowski, J., Chowdhury, N., and Baker, A. (2008). Optimizing inhibitory learning during exposure therapy. Behav. Res. Ther. 46, 5–27. doi:10.1016/j.brat.2007.10.003
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., and Vervliet, B. (2014). Maximizing exposure therapy: an inhibitory learning approach. Behav. Res. Ther. 58, 10–23. doi:10.1016/j.brat.2014.04.006
Cuthbert, B. N., Lang, P. J., Strauss, C., Drobes, D., Patrick, C. J., and Bradley, M. M. (2003). The psychophysiology of anxiety disorder: fear memory imagery. Psychophysiology 40, 407–422. doi:10.1111/1469-8986.00043
Dammen, L. V., Finseth, T. T., Mccurdy, B. H., Barnett, N. P., Conrady, R. A., Leach, A. G., et al. (2022). Evoking stress reactivity in virtual reality: a systematic review and meta-analysis. Neurosci. Biobehav Rev. 138, 104709. doi:10.1016/j.neubiorev.2022.104709
De Quervain, D. J., Bentz, D., Michael, T., Bolt, O. C., Wiederhold, B. K., Margraf, J., et al. (2011). Glucocorticoids enhance extinction-based psychotherapy. Proc. Natl. Acad. Sci. U. S. A. 108, 6621–6625. doi:10.1073/pnas.1018214108
Diemer, J., Domschke, K., Muhlberger, A., Winter, B., Zavorotnyy, M., Notzon, S., et al. (2013). Acute anxiolytic effects of quetiapine during virtual reality exposure--a double-blind placebo-controlled trial in patients with specific phobia. Eur. Neuropsychopharmacol. 23, 1551–1560. doi:10.1016/j.euroneuro.2013.01.001
Diemer, J., Muhlberger, A., Yassouridis, A., and Zwanzger, P. (2023). Distraction versus focusing during VR exposure therapy for acrophobia: a randomized controlled trial. J. Behav. Ther. Exp. Psychiatry 81, 101860. doi:10.1016/j.jbtep.2023.101860
Dillon, A., Kelly, M., Robertson, I. H., and Robertson, D. A. (2016). Smartphone applications utilizing biofeedback can aid stress reduction. Front. Psychol. 7, 832. doi:10.3389/fpsyg.2016.00832
Donahue, C. B., Kushner, M. G., Thuras, P. D., Murphy, T. G., Van Demark, J. B., and Adson, D. E. (2009). Effect of quetiapine vs. placebo on response to two virtual public speaking exposures in individuals with social phobia. J. Anxiety Disord. 23, 362–368. doi:10.1016/j.janxdis.2008.12.004
Duits, P., Cath, D. C., Heitland, I., and Baas, J. M. (2016). High current anxiety symptoms, but not a past anxiety disorder diagnosis, are associated with impaired fear extinction. Front. Psychol. 7, 252. doi:10.3389/fpsyg.2016.00252
Emmelkamp, P. M. G., Meyerbroker, K., and Morina, N. (2020). Virtual reality therapy in social anxiety disorder. Curr. Psychiatry Rep. 22, 32. doi:10.1007/s11920-020-01156-1
Fernández-Álvarez, J., Di Lernia, D., and Riva, G. (2020). “Virtual reality for anxiety disorders: rethinking a field in expansion,” in Anxiety disorders (Singapore: Springer).
Flores-Arredondo, J. H., and Assad-Kottner, C. (2015). Virtual reality: a look into the past to fuel the future. Bull. R. Coll. Surg. Engl. 97, 424–426. doi:10.1308/rcsbull.2015.424
Frank, D. L., Khorshid, L., Kiffer, J. F., Moravec, C. S., and Mckee, M. G. (2010). Biofeedback in medicine: who, when, why and how? Ment. Health Fam. Med. 7, 85–91.
Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., et al. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47, 2393–2400. doi:10.1017/S003329171700040X
Fuch, P., and Moreau, G. P. G. (2011) Virtual reality: concepts and technologies. New York: CRC Press.
Garcia-Gutierrez, M. S., Navarrete, F., Sala, F., Gasparyan, A., Austrich-Olivares, A., and Manzanares, J. (2020). Biomarkers in psychiatry: concept, definition, types and relevance to the clinical reality. Front. Psychiatry 11, 432. doi:10.3389/fpsyt.2020.00432
Garcia-Palacios, A., Botella, C., Hoffman, H., and Fabregat, S. (2007). Comparing acceptance and refusal rates of virtual reality exposure vs. in vivo exposure by patients with specific phobias. Cyberpsychol Behav. 10, 722–724. doi:10.1089/cpb.2007.9962
Gaume, A., Vialatte, A., Mora-Sanchez, A., Ramdani, C., and Vialatte, F. B. (2016). A psychoengineering paradigm for the neurocognitive mechanisms of biofeedback and neurofeedback. Neurosci. Biobehav Rev. 68, 891–910. doi:10.1016/j.neubiorev.2016.06.012
Gerew, A. B., Romney, D. M., and Leboeuf, A. (1989). Synchrony and desynchrony in high and low arousal subjects undergoing therapeutic exposure. J. Behav. Ther. Exp. Psychiatry 20, 41–48. doi:10.1016/0005-7916(89)90006-2
Globisch, J., Hamm, A. O., Esteves, F., and Ohman, A. (1999). Fear appears fast: temporal course of startle reflex potentiation in animal fearful subjects. Psychophysiology 36, 66–75. doi:10.1017/s0048577299970634
Goessl, V. C., Curtiss, J. E., and Hofmann, S. G. (2017). The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. Psychol. Med. 47, 2578–2586. doi:10.1017/S0033291717001003
Gramlich, M. A., Smolenski, D. J., Norr, A. M., Rothbaum, B. O., Rizzo, A. A., Andrasik, F., et al. (2021). Psychophysiology during exposure to trauma memories: comparative effects of virtual reality and imaginal exposure for posttraumatic stress disorder. Depress. anxiety 38, 626–638. doi:10.1002/da.23141
Gregg, L., and Tarrier, N. (2007). Virtual reality in mental health: a review of the literature. Soc. Psychiatry Psychiatr. Epidemiol. 42, 343–354. doi:10.1007/s00127-007-0173-4
Gujjar, K. R., Van Wijk, A., Kumar, R., and De Jongh, A. (2019). Efficacy of virtual reality exposure therapy for the treatment of dental phobia in adults: a randomized controlled trial. J. Anxiety Disord. 62, 100–108. doi:10.1016/j.janxdis.2018.12.001
Gujjar, K. R., Van Wijk, A., Sharma, R., and De Jongh, A. (2018). Virtual reality exposure therapy for the treatment of dental phobia: a controlled feasibility study. Behav. Cogn. Psychother. 46, 367–373. doi:10.1017/S1352465817000534
Gutierrez-Maldonado, J., Wiederhold, B. K., and Riva, G. (2015). Future directions: how virtual reality can further improve the assessment and treatment of eating disorders and obesity. Cyberpsychol Behav. Soc. Netw. 19, 148–153. doi:10.1089/cyber.2015.0412
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Hodgson, R., and Rachman, S. (1974). II. Desynchrony in measures of fear. Behav. Res. Ther. 12, 319–326. doi:10.1016/0005-7967(74)90006-0
Hoehn-Saric, R., and Mcleod, D. R. (1988). The peripheral sympathetic nervous system. Psychiatr. Clin. North Am. 11, 375–386. doi:10.1016/s0193-953x(18)30504-5
Hoehn-Saric, R., and Mcleod, D. R. (2000). Anxiety and arousal: physiological changes and their perception. J. Affect Disord. 61, 217–224. doi:10.1016/s0165-0327(00)00339-6
Hong, Y.-J., Kim, H. E., Jung, Y. H., Kyeong, S., Kim, J.-J., American Psychiatric Association, A. P. L. P. M. E. S. M. B. C. J. A. B. B. F. A. B. C. O. J. G.-P., et al. (2017). Usefulness of the mobile virtual reality self-training for overcoming a fear of heights. Cyberpsychology, Behav. Soc. Netw. 20, 753–761. doi:10.1089/cyber.2017.0085
Hur, J.-W., Shin, H., Jung, D., Lee, H.-J., Lee, S., Kim, G. J., et al. (2021). Virtual reality–based psychotherapy in social anxiety disorder: fMRI study using a self-referential task. JMIR Ment. Health 8, e25731. doi:10.2196/25731
Kampmann, I. L., Emmelkamp, P. M., and Morina, N. (2016). Meta-analysis of technology-assisted interventions for social anxiety disorder. J. Anxiety Disord. 42, 71–84. doi:10.1016/j.janxdis.2016.06.007
Kaussner, Y., Kuraszkiewicz, A. M., Schoch, S., Markel, P., Hoffmann, S., Baur-Streubel, R., et al. (2020). Treating patients with driving phobia by virtual reality exposure therapy - a pilot study. PLoS One 15, e0226937. doi:10.1371/journal.pone.0226937
Lande, S. D. (1982). Physiological and subjective measures of anxiety during flooding. Behav. Res. Ther. 20, 81–88. doi:10.1016/0005-7967(82)90011-0
Levin, M. F., Weiss, P. L., and Keshner, E. A. (2015). Emergence of virtual reality as a tool for upper limb rehabilitation: incorporation of motor control and motor learning principles. Phys. Ther. 95, 415–425. doi:10.2522/ptj.20130579
Levy, F., Leboucher, P., Rautureau, G., and Jouvent, R. (2016). E-virtual reality exposure therapy in acrophobia: a pilot study. J. Telemed. Telecare 22, 215–220. doi:10.1177/1357633X15598243
Lin, X. B., Lee, T. S., Cheung, Y. B., Ling, J., Poon, S. H., Lim, L., et al. (2019). Exposure therapy with personalized real-time arousal detection and feedback to alleviate social anxiety symptoms in an analogue adult sample: pilot proof-of-concept randomized controlled trial. JMIR Ment. Health 6, e13869. doi:10.2196/13869
Lindner, P., Miloff, A., Hamilton, W., Reuterskiöld, L., Andersson, G., Powers, M. B., et al. (2017). Creating state of the art, next-generation Virtual Reality exposure therapies for anxiety disorders using consumer hardware platforms: design considerations and future directions. Cogn. Behav. Ther. 46, 404–420. doi:10.1080/16506073.2017.1280843
Loucks, L., Yasinski, C., Norrholm, S. D., Maples-Keller, J., Post, L., Zwiebach, L., et al. (2019). You can do that?!: feasibility of virtual reality exposure therapy in the treatment of PTSD due to military sexual trauma. J. anxiety Disord. 61, 55–63. doi:10.1016/j.janxdis.2018.06.004
Malbos, E., Rapee, R. M. M. K., and Kavakli, M. (2013). A controlled study of agoraphobia and the independent effect of virtual reality exposure therapy. Aust. N. Z. J. Psychiatry 47, 160–168. doi:10.1177/0004867412453626
Martirosov, S., and Kopecek, P. (2017). CYBER SICKNESS IN VIRTUAL REALITY - LITERATURE REVIEW. Ann. DAAAM Proc. 28, 0718–0726. doi:10.2507/28th.daaam.proceedings.101
Mcglade, A. L., Treanor, M., Kim, R., and Craske, M. G. (2023). Does fear reduction predict treatment response to exposure for social anxiety disorder? J. Behav. Ther. Exp. psychiatry 79, 101833. doi:10.1016/j.jbtep.2022.101833
Mcinerney, J., Brown, P., Bird, J. C., Nickless, A., Brown, G., and Freeman, D. (2021). Does raising heart rate prior to a behavioural test enhance learning in cognitive therapy for anxiety? An experimental test for the treatment of fear of heights using virtual reality. Behav. Res. Ther. 144, 103928. doi:10.1016/j.brat.2021.103928
Mclean, C. P., Asnaani, A., Litz, B. T., and Hofmann, S. G. (2011). Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J. Psychiatr. Res. 45, 1027–1035. doi:10.1016/j.jpsychires.2011.03.006
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., and Group, P. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J. Clin. Epidemiol. 62, 1006–1012. doi:10.1016/j.jclinepi.2009.06.005
Morina, N., Ijntema, H., Meyerbroker, K., and Emmelkamp, P. M. (2015). Can virtual reality exposure therapy gains be generalized to real-life? A meta-analysis of studies applying behavioral assessments. Behav. Res. Ther. 74, 18–24. doi:10.1016/j.brat.2015.08.010
Mühlberger, A., Herrmann, M. J., Wiedemann, G., Ellgring, H., and Pauli, P. (2001). Repeated exposure of flight phobics to flights in virtual reality. Behav. Res. Ther. 39, 1033–1050. doi:10.1016/s0005-7967(00)00076-0
Norrholm, S. D., Jovanovic, T., Gerardi, M., Breazeale, K. G., Price, M., Davis, M., et al. (2016). Baseline psychophysiological and cortisol reactivity as a predictor of PTSD treatment outcome in virtual reality exposure therapy. Behav. Res. Ther. 82, 28–37. doi:10.1016/j.brat.2016.05.002
Opris, D., Pintea, S., Garcia-Palacios, A., Botella, C., Szamoskozi, S., and David, D. (2012). Virtual reality exposure therapy in anxiety disorders: a quantitative meta-analysis. Depress Anxiety 29, 85–93. doi:10.1002/da.20910
Parsons, T. D., and Rizzo, A. A. (2008). Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: a meta-analysis. J. Behav. Ther. Exp. Psychiatry 39, 250–261. doi:10.1016/j.jbtep.2007.07.007
Peperkorn, H. M., Alpers, G. W., and Muhlberger, A. (2014). Triggers of fear: perceptual cues versus conceptual information in spider phobia. J. Clin. Psychol. 70, 704–714. doi:10.1002/jclp.22057
Perez, V. B., Swerdlow, N. R., Braff, D. L., Naatanen, R., and Light, G. A. (2014). Using biomarkers to inform diagnosis, guide treatments and track response to interventions in psychotic illnesses. Biomark. Med. 8, 9–14. doi:10.2217/bmm.13.133
Pittig, A., Arch, J. J., Lam, C. W., and Craske, M. G. (2013). Heart rate and heart rate variability in panic, social anxiety, obsessive-compulsive, and generalized anxiety disorders at baseline and in response to relaxation and hyperventilation. Int. J. Psychophysiol. 87, 19–27. doi:10.1016/j.ijpsycho.2012.10.012
Pittig, A., Kotter, R., and Hoyer, J. (2019). The struggle of behavioral therapists with exposure: self-reported practicability, negative beliefs, and therapist distress about exposure-based interventions. Behav. Ther. 50, 353–366. doi:10.1016/j.beth.2018.07.003
Place, S., Blanch-Hartigan, D., Rubin, C., Gorrostieta, C., Mead, C., Kane, J., et al. (2017). Behavioral indicators on a mobile sensing platform predict clinically validated psychiatric symptoms of mood and anxiety disorders. J. Med. Internet Res. 19, e75. doi:10.2196/jmir.6678
Pohjavaara, P., Telaranta, T., and Vaisanen, E. (2003). The role of the sympathetic nervous system in anxiety: is it possible to relieve anxiety with endoscopic sympathetic block? Nord. J. Psychiatry 57, 55–60. doi:10.1080/08039480310000266
Poleszak, J., Szabat, P., Szabat, M., Boreński, G., Wójcik, M., and Milanowska, J. (2019). Biofeedback in psychiatric and psychological clinical practice. J. Educ. Health Sport 9, 8. doi:10.5281/zenodo.3228936
Powers, M. B., and Emmelkamp, P. M. (2008). Virtual reality exposure therapy for anxiety disorders: a meta-analysis. J. Anxiety Disord. 22, 561–569. doi:10.1016/j.janxdis.2007.04.006
Premkumar, P., Heym, N., Brown, D. J., Battersby, S., Sumich, A., Huntington, B., et al. (2021). The effectiveness of self-guided virtual-reality exposure therapy for public-speaking anxiety. Front. Psychiatry 12, 694610. doi:10.3389/fpsyt.2021.694610
Price, M., Maples, J. L., Jovanovic, T., Norrholm, S. D., Heekin, M., and Rothbaum, B. O. (2015). An investigation of outcome expectancies as a predictor of treatment response for combat veterans with PTSD: comparison of clinician, self-report, and biological measures. Depress Anxiety 32, 392–399. doi:10.1002/da.22354
Rachman, S., and Hodgson, R. (1974). I. Synchrony and desynchrony in fear and avoidance. Behav. Res. Ther. 12, 311–318. doi:10.1016/0005-7967(74)90005-9
Reitmaier, J., Schiller, A., Mühlberger, A., Pfaller, M., Meyer, M., and Shiban, Y. (2022). Effects of rhythmic eye movements during a virtual reality exposure paradigm for spider-phobic patients. Psychol. psychotherapy 95, 57–78. doi:10.1111/papt.12363
Repetto, C., Gaggioli, A., Pallavicini, F., Cipresso, P., Raspelli, S., and Riva, G. (2013). Virtual reality and mobile phones in the treatment of generalized anxiety disorders: a phase-2 clinical trial. Personal Ubiquitous Comput. 17, 253–260. doi:10.1007/s00779-011-0467-0
Rizzo, A. S., and Bouchard, S. (2019) Virtual reality for psychological and neurocognitive interventions. Springer-Verlag.
Rodebaugh, T. L., Holaway, R. M., and Heimberg, R. G. (2004). The treatment of social anxiety disorder. Clin. Psychol. Rev. 24, 883–908. doi:10.1016/j.cpr.2004.07.007
Šalkevicius, J., Damaševičius, R., Maskeliunas, R., and Laukienė, I. (2019). Anxiety level recognition for virtual reality therapy system using physiological signals. Electronics 8, 1039. doi:10.3390/electronics8091039
Schaefer, H. S., Larson, C. L., Davidson, R. J., and Coan, J. A. (2014). Brain, body, and cognition: neural, physiological and self-report correlates of phobic and normative fear. Biol. Psychol. 98, 59–69. doi:10.1016/j.biopsycho.2013.12.011
Schoenberg, P. L., and David, A. S. (2014). Biofeedback for psychiatric disorders: a systematic review. Appl. Psychophysiol. Biofeedback 39, 109–135. doi:10.1007/s10484-014-9246-9
Shiban, Y., Brutting, J., Pauli, P., and Muhlberger, A. (2015). Fear reactivation prior to exposure therapy: does it facilitate the effects of VR exposure in a randomized clinical sample? J. Behav. Ther. Exp. Psychiatry 46, 133–140. doi:10.1016/j.jbtep.2014.09.009
Shiban, Y., Diemer, J., Muller, J., Brutting-Schick, J., Pauli, P., and Muhlberger, A. (2017). Diaphragmatic breathing during virtual reality exposure therapy for aviophobia: functional coping strategy or avoidance behavior? a pilot study. BMC Psychiatry 17, 29. doi:10.1186/s12888-016-1181-2
Shic, F. (2016). Eye tracking as a behavioral biomarker for psychiatric conditions: the road ahead. J. Am. Acad. Child. Adolesc. Psychiatry 55, 267–268. doi:10.1016/j.jaac.2016.02.002
Stang, A. (2010). Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25, 603–605. doi:10.1007/s10654-010-9491-z
Stein, M. B., and Stein, D. J. (2008). Social anxiety disorder. Lancet 371, 1115–1125. doi:10.1016/S0140-6736(08)60488-2
Stupar-Rutenfrans, S., Ketelaars, L. E. H., and Van Gisbergen, M. S. (2017). Beat the fear of public speaking: mobile 360° video virtual reality exposure training in home environment reduces public speaking anxiety. Cyberpsychol Behav. Soc. Netw. 20, 624–633. doi:10.1089/cyber.2017.0174
Tardif, N., Therrien, C.-É., and Bouchard, S. (2019). Re-examining psychological mechanisms underlying virtual reality-based exposure for spider phobia. Cyberpsychology, Behav. Soc. Netw. 22, 39–45. doi:10.1089/cyber.2017.0711
Teachman, B. A., and Gordon, T. (2009). Age differences in anxious responding: older and calmer, unless the trigger is physical. Psychol. Aging 24, 703–714. doi:10.1037/a0016813
Tolin, D. F., Davies, C. D., Moskow, D. M., and Hofmann, S. G. (2020). Biofeedback and neurofeedback for anxiety disorders: a quantitative and qualitative systematic review. Adv. Exp. Med. Biol. 1191, 265–289. doi:10.1007/978-981-32-9705-0_16
Van Dis, E. A. M., Van Veen, S. C., Hagenaars, M. A., Batelaan, N. M., Bockting, C. L. H., Van Den Heuvel, R. M., et al. (2019). Long-term outcomes of cognitive behavioral therapy for anxiety-related disorders: a systematic review and meta-analysis. JAMA Psychiatry 77, 265. doi:10.1001/jamapsychiatry.2019.3986
Van ‘T Wout-Frank, M., Shea, M. T., Larson, V. C., Greenberg, B. D., and Philip, N. S. (2019). Combined transcranial direct current stimulation with virtual reality exposure for posttraumatic stress disorder: feasibility and pilot results. Brain Stimul. 12, 41–43. doi:10.1016/j.brs.2018.09.011
Wang, P. S., Berglund, P., Olfson, M., Pincus, H. A., Wells, K. B., and Kessler, R. C. (2005). Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62, 603–613. doi:10.1001/archpsyc.62.6.603
Wechsler, T. F., Pfaller, M., Eickels, R. E. V., Schulz, L. H., and Muhlberger, A. (2021). Look at the audience? A randomized controlled study of shifting attention from self-focus to nonsocial vs social external stimuli during virtual reality exposure to public speaking in social anxiety. Front. psychiatry 12, 751272. doi:10.3389/fpsyt.2021.751272
Wiederhold, B. K., Jang, D. P., Gevirtz, R. G., Kim, S. I., Kim, I. Y., and Wiederhold, M. D. (2002). The treatment of fear of flying: a controlled study of imaginal and virtual reality graded exposure therapy. IEEE Trans. Inf. Technol. Biomed. 6, 218–223. doi:10.1109/titb.2002.802378
Wilhelm, F. H., Gevirtz, R., and Roth, W. T. (2001). Respiratory dysregulation in anxiety, functional cardiac, and pain disorders. Assessment, phenomenology, and treatment. Behav. Modif. 25, 513–545. doi:10.1177/0145445501254003
Wilhelm, F. H., and Roth, W. T. (1998). Taking the laboratory to the skies: ambulatory assessment of self-report, autonomic, and respiratory responses in flying phobia. Psychophysiology 35, 596–606. doi:10.1017/s0048577298970196
Keywords: biomarkers, exposure therapy, virtual reality, anxiety, systematic review
Citation: Ernst MT, Hyldig Nielsen J, Runge E, Bouchard S and Clemmensen L (2024) Biomarkers in exposure-based treatment of anxiety in virtual reality: a systematic review. Front. Virtual Real. 5:1355082. doi: 10.3389/frvir.2024.1355082
Received: 13 December 2023; Accepted: 16 May 2024;
Published: 13 June 2024.
Edited by:
Clint Bowers, University of Central Florida, United StatesReviewed by:
Cristin D. Runfola, Stanford University, United StatesYamin Wang, Capital Normal University, China
Copyright © 2024 Ernst, Hyldig Nielsen, Runge, Bouchard and Clemmensen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mathias Torp Ernst, bXRvcnBlcm5zdEBoZWFsdGguc2R1LmRr, bWF0aGlhcy50b3JwLmVybnN0QHJzeWQuZGs=
†ORCID: Mathias Torp Ernst, orcid.org/0000-0003-3630-6960; Jakob Hyldig Nielsen, orcid.org/0000-0002-5902-5144; Eik Runge, orcid.org/0000-0002-7397-6114; Stéphane Bouchard, orcid.org/0000-0002-5995-340X; Lars Clemmensen, orcid.org/0000-0002-1750-4649
‡These authors share first authorship