 Adriana Bastardas-Albero
Adriana Bastardas-Albero Berta Vall
Berta Vall Carles Pérez-Testor
Carles Pérez-Testor Josep-Maria Losilla
Josep-Maria Losilla- 1Faculty of Psychology, Educational and Sports Sciences-Blanquerna (FPCEE), Ramon Llull University, Barcelona, Spain
- 2Department of Psychobiology and Methodology of Health Sciences, Universitat Autònoma de Barcelona, Barcelona, Spain
Purpose: Prevention and rehabilitation of intimate partner violence (IPV) is a very important topic due to its high prevalence, visibility, and potential to generate negative consequences in survivor’s physical and mental health. Previous interventions have used traditional, explicit approaches giving mixed results for both prevention and rehabilitation. However, the number of implicit interventions using technological innovations, specifically virtual reality (VR), is limited in this field. In this review, we aim to find the existing literature on immersive VR targeting prevention or rehabilitation of IPV.
Method: The search used several databases: PsycINFO by EBSCOHost, and Medline by PubMed, specifically set to find IPV intervention articles, published after 2010, that included VR in their intervention.
Results: 11 studies met all of the eligibility criteria and were included in the review.
Conclusion: VR has overall proven useful to tackle the prevention and rehabilitation of intimate partner violence, as it offers the unique possibility of experiencing a variety of situations from a different perspective, in a safe and controlled environment. Therefore, it is a tool which has great potential for transformation, as it allows for experiential and implicit learning.
1 Introduction
The main goal of this study is to find out whether virtual reality (VR) could be a good tool to reduce intimate partner violence (IPV). Specifically, we aim to answer the following questions: a) Is VR an effective tool to prevent IPV?, b) Is VR a good tool to intervene in IPV, both in perpetrators and survivors? c) Is VR a good tool to improve bystander behavior in IPV situations? In order to do so, we have performed a systematic review to find the current state of VR treatment for IPV.
1.1 VR interventions in mental health and forensic settings
VR has been used for several mental health interventions. The underlying idea is that someone can stand and move in a computer-generated world, and feel immersed (Rothbaum et al., 2006; Botella et al., 2007; Fox et al., 2009; Baños et al., 2011; Bordnick et al., 2011; Repetto et al., 2013). That is, feel that they are in the real world while being somewhere else. VR treatment has been applied to tackle different psychiatric disorders, such as anxiety disorders, specific phobias, Post Traumatic Stress Disorder (PTSD), schizophrenia, Obsessive-Compulsive Disorder (OCD), eating disorders and autism, and has shown promising results (Turner and Casey, 2014; Valmaggia et al., 2016; Maples-Keller et al., 2017). VR as a treatment in mental healthcare settings has the ability to include dynamic yet controlled multisensory interactive situations, as well as register and analyze users’ behavioral responses. It therefore offers realistic situations, makes the treatment very personal through the adaptability of the VR-environment, motivates patients because it provides them with something new and different, and is a good tool for patients who have trouble with imagining or visualization (Riva, 2009; Maples-Keller et al., 2017). VR has the added benefit of facilitating learning, changing attitudes, and modifying behavior indirectly, as opposed to explicit interventions, where participants are directly given information and are aware of what is that they are learning. Thus, in this review we view VR interventions as implicit interventions.
VR has also been used in forensic settings. Forensic settings are defined, for the purpose of this paper, as correctional settings for people who have been accused of an offense. The characteristics of forensic mental healthcare patients (i.e., limited insight in their own health and diseases, not compliant to their treatment, heterogenous psychopathology and offending behavior, low levels of literacy, and low motivation for treatment) (Kip et al., 2020), make VR a potentially useful tool. Interactive, non-immersive, computerized case simulations have previously been explored in these settings and research has cautiously indicated that such programs may be beneficial (Arborelius et al., 2013; Kip et al., 2018; Sygel and Wallinius, 2021). However, immersive VR simulations can be an even bigger step forward for correctional rehabilitation (Ticknor, 2019). VR may facilitate treatment and reintegration of offenders into society through treatment of psychiatric disorders (e.g., using VR cognitive behavioral therapy), teaching necessary skills, providing feedback, and making virtual treatment groups possible (Sygel and Wallinius, 2021). Our aim with this paper is to see whether VR can also be an effective tool both in the prevention and treatment of IPV, within the perpetrators and the survivors. We want to find out whether the special benefits of VR produce a stronger effect than other types of interventions.
In the following pages we will review what has been done in terms of prevention and intervention of IPV in general. Regarding prevention, we will first review general interventions, followed by bystander interventions, and then delve into recent technological innovations in prevention. Shifting our focus to rehabilitation, we will explore interventions designed for both perpetrators and survivors separately, and end that section discussing technological advances in the treatment of IPV.
1.2 Prevention
1.2.1 General interventions for the prevention of IPV
Interventions for Intimate Partner Violence (IPV) have grown over the past 2 decades. In countries around the world, interventions for IPV have been developed and delivered with the goal of preventing or at least reducing the prevalence of this form of violence.
Existing robust programs address the acceptability of violence and simultaneously tackle the root causes of violence, which include societal norms related to gender dynamics, the acceptance of violence, and women’s financial reliance on men. These programs, like “Stepping Stones”, additionally teach participants a new set of skills, ranging from recognizing healthy relationships and employing conflict resolution techniques, to enhancing empathy, managing anger, making decisions, asserting oneself, improving communication skills, providing education about dating violence, and implementing strategies for emotional regulation (Arango et al., 2014; Ellsberg et al., 2018; Gibbs et al., 2020). These activities are mainly carried out in classrooms and hospitals, are either face-to-face and/or by computer, and include both individual and group formats It is clear that programs involving multiple stakeholders have been proven to be the most effective ones. Other approaches focusing on changing norms have involved awareness-raising campaigns and small group workshops, often accompanied by community engagement activities, such as street theatre, posters, and behavior change and communication strategies (Heise, 2011).
Included within the prevention of IPV we find bystander interventions. The bystander approach suggests that individuals can intervene in public settings when observing situations involving interpersonal violence or sexual violence (Banyard et al., 2004; McMahon et al., 2011). Evaluations of bystander intervention programs in the literature largely focus on the issue of sexual violence but offer a foundation for the development of effective IPV-focused bystander programs, which have seen an increase in recent years (Park and Kim, 2023). Existing multiple programs have demonstrated long-term changes in men’s attitudes and behavior, including decreases in rape myth acceptance and likelihood of raping, increases in empathy towards rape victims, increases in willingness to curtail sexist comments, and increases in the disposition to offer support to rape victims (Foubert, 2000; Banyard et al., 2007), as well as more willingness to intervene (Katz and Moore, 2013; McMahon et al., 2014).
1.2.2 Technological interventions for the prevention of IPV
With technological interventions being a focus on today’s scientific climate, one wonders whether these kinds of interventions could also be used to target IPV. The term “mHealth”, or mobile health, refers to the utilization of mobile phones or other wireless technology in providing medical care. Some programs using phone applications have been developed, which have shown a reduction in psychological and physical dating violence among college students (Glass et al., 2015). However, evidence for efficacy compared to conventional IPV prevention approaches is limited (Martinez and Rey, 2014; Anderson et al., 2021).
Recent intervention programs have included non-immersive video simulations for IPV prevention, which have shown to be effective in improving relationship quality, reducing odds of perpetration, increasing bystander behavior, and recognizing signs of violence in non-violent population (Kleinsasser et al., 2015; Kearney, 2018; Peskin et al., 2019; Doss et al., 2020). A recent computerized program, designed for couples who had experienced violence, was delivered through the Web called WISER (Writing to Improve Selfin-Relations), which included videos of violent relationships and the writing of a story about the participants’ own relationship. The intervention demonstrated to be feasible, decreased psychological and physical dating violence, increased constructive communication, and improved relationship satisfaction in men (Draucker et al., 2019).
These kinds of interventions tend to use a more active approach (i.e., those that engage the user), which some researchers have concluded are more effective than passive psychoeducation strategies (i.e., merely listening and receiving information) (Albarracin et al., 2005).
1.3 Rehabilitation
1.3.1 General interventions for the treatment of IPV—perpetrators
To address the issue of repeated intimate partner violence (IPV) by perpetrators, it is common for individuals who have been arrested for IPV to be mandated by the court to engage in batterer intervention programs (Stuart et al.,, 2007). The prevailing intervention model for IPV perpetrators in the USA is the “Duluth Model,” which aims to modify patriarchal and sexist beliefs that are believed to contribute to IPV perpetration (Pence and Paymar, 1993; Gondolf, 2007). Other interventions, including Cognitive Behavioral Therapy (CBT) groups have also been used to treat IPV perpetrators. In practice, most programs incorporate parts of both the Duluth Model and CBT programs (Babcock et al., 2004).
Moreover, it is thought that differentiating perpetrators by certain typology could help with the effectiveness of these programs. These programs usually focus on understanding gender roles, being more emotionally engaging, being less conflictual in friendships and intimate relationships and improving their economic position (Ellsberg et al., 2015). Research findings suggest that some subtypes, characterized by high levels of personality traits like borderline, avoidant, and antisocial tendencies, have poor outcomes in standard batterer interventions. Different subtypes exhibit varying success in completing treatment and avoiding further violence, with some being more likely to drop out of treatment and experience rearrest following treatment (Holtzworth-Munroe and Meehan, 2000; Cantos et al., 2015). The findings emphasize the need to tailor interventions based on the specific subtype of batterer to improve treatment effectiveness. For example, Saunders (1996) analyzed data comparing cognitive-behavioral-feminist treatment with a new process-psychodynamic treatment. It was observed that batterers with high antisocial scores benefited more from structured cognitive-behavioral interventions, whereas those with high dependency scores showed better progress with the new intervention approach (Saunders, 1996). A more recent study suggested a shift in approach emphasizing individualized interventions based on factors like demographics, perpetrator types, readiness to change, and co-occurring problems such as substance abuse and mental health issues. This personalized approach is crucial to enhance treatment efficacy and prevent further victimization (Butters et al., 2021).
To date, intervention programs developed to address IPV have been evaluated with mixed results. A meta-analytic review of domestic violence treatment by Babcock et al. (2004) found that current interventions, including those based on the Duluth model have minimal impact on reducing recidivism. The authors argued that these interventions should not simply be abandoned but suggested that, as no one treatment method was proven superior to the others, further research should be conducted and components should be added to the existing interventions, which could also be individualized for specific patients (Babcock et al., 2004).
1.3.2 General interventions for treatment of IPV experience—survivors
When talking about treatment of IPV, we do not only focus on reducing perpetrators’ violent behavior, but also on helping survivors deal with the consequences of an abusive relationship and reducing their risk of suffering violence again. Previous research has indicated that both empowerment-based advocacy and cognitively focused clinical interventions demonstrate positive physical and mental health changes. Specifically, the interventions for survivors include improving problem-solving strategies, decision-making, and changing the survivor´s distorted self-thinking and self-perception (Trabold et al., 2018).
1.3.3 Technological interventions for treatment of IPV
Realistic computer simulations not only have potential for the prevention of IPV as previously mentioned, but also for the rehabilitation of IPV offenders, as it can help activate, motivate, and emotionally engage users. This contributes to the possibility of building knowledge, better understanding of the simulated experience, better confidence in one’s own ability to solve problems, and better memory (Courteille et al., 2008; Botezatu et al., 2010; Pantziaras et al., 2012). A study in 2014 used computerized case simulation for the treatment of men convicted of IPV, and found beneficial results (Sygel et al., 2014) for the rehabilitation of offenders. Simulations also have the amazing ability of creating potential for instruction, by creating a realistic world in which the user can be exposed to different contextual factors and practice behaviors which would be too dangerous or rare to practice in real life (Bell et al., 2008).
There is currently limited evidence regarding VR or immersive computerized simulation interventions for either the prevention or rehabilitation of IPV. However, some studies do exist. The goal of this review is to shed light on those studies and see whether they could be a strong option for tackling the current IPV issue. VR interventions have the benefit of being able to adapt to specific people, therefore providing a much-needed cost-effective individualized treatment, Moreover, VR has the added value of embodiment (i.e., feeling like you are part of a different body) through an avatar, which can induce different emotions, and could thus have a greater impact on the user (Slater and Sanchez-Vives, 2016).
2 Materials and methods
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses, PRISMA guidelines.
2.1 Search strategy
In order to evaluate which effective VR interventions exist for the prevention and rehabilitation of IPV, we established the search terms with the highest number of possible synonyms. The general search expression was (“Intimate partner violence (MeSH)” OR “Dating violence (MeSH)” OR “Spouse abuse (MeSH)” OR “Intimate partner abuse (MeSH)” OR “Domestic violence” OR “gender violence” OR “IPV”) AND (“Virtual Reality (MeSH)” OR “Virtual Reality, Educational (MeSH)” OR “Educational Virtual Realities (MeSH)” OR “Educational Virtual Reality (MeSH)” OR “Virtual Reality Immersion Therapy (MeSH)” OR “Virtual Reality Therapy (MeSH)” OR “Reality Therapies, Virtual (MeSH)” OR “Reality Therapy, Virtual (MeSH)” OR “Therapies, Virtual Reality (MeSH)” OR “Therapy, Virtual Reality (MeSH)” OR “Virtual Reality Therapies (MeSH)” OR “Virtual reality intervention” OR “VR intervention” OR “360 video”).
The search used several databases: PsycINFO by EBSCOHost, and Medline by PubMed. The specific syntaxes for the databases are in Supplementary Appendix S1.
Lastly, we reviewed the references in the selected studies in order to identify potential studies of interest that were missed during the database search, but no new ones were found.
2.2 Inclusion criteria and selection process of the studies
Inclusion criteria for the current review were the following a) Participants must be over 14 years old; b) The study must be published in English, Spanish or Catalan; c) The study must have an experimental or quasi-experimental design d) The study must evaluate the effectiveness of VR interventions for the prevention or rehabilitation of IPV; e) The study must have been published after 2010, and f) the study must have used VR. Exclusion criteria included studies with participants under 14 years old, reviews, observations, single case studies, and studies with non-immersive videos. Location or sample size were not part of the exclusion criteria.
The selection process was carried out by the author of the review, doing a first selection based on the title and abstract of the studies and the final selection based on the full text of some studies and of those that did not give enough information in their title or abstract.
2.3 Data extraction
A data extraction protocol was designed for the selected studies. The registered information was the following: authors, publication year, research design, demographic characteristics of the target population (forensic or community, gender, age, and sexual orientation when available), number of participants, type of outcome, instruments that were used to analyze the main study variables, type of intervention (prevention, early intervention, or rehabilitation), conclusions, length of treatment with VR, length of control group intervention, and type of control group (waitlist, active, or delayed). Data extraction was carried out by the author.
2.4 Bias risk assessment
The risk of bias of the included articles in the review was evaluated by the author of the review applying the checklists recommended by The Joanna Briggs Institute (JBI) for Randomized Controlled Trials (RCT) and Quasi-Experiments (Table 1 and Table 2).

TABLE 1. Bias risk assessment for RCTs.
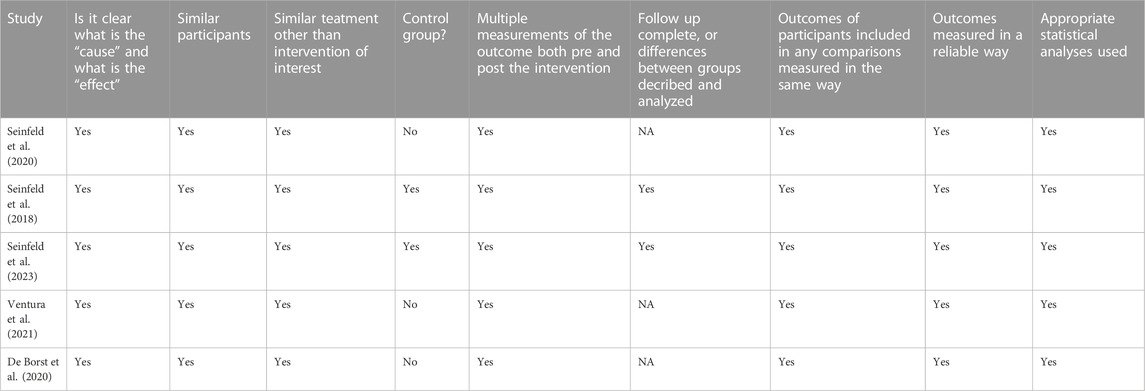
TABLE 2. Bias risk assessment for quasi-experiments.
2.5 Data analysis strategy
A narrative summary of the results was carried out of the studies regarding the effectiveness of VR or other interactive interventions for the prevention and rehabilitation of IPV. The main effectiveness results and conclusions were shown in a table, and future research opportunities were discussed.
3 Results
Figure 1 summarizes the complete search and selection process of the current review.
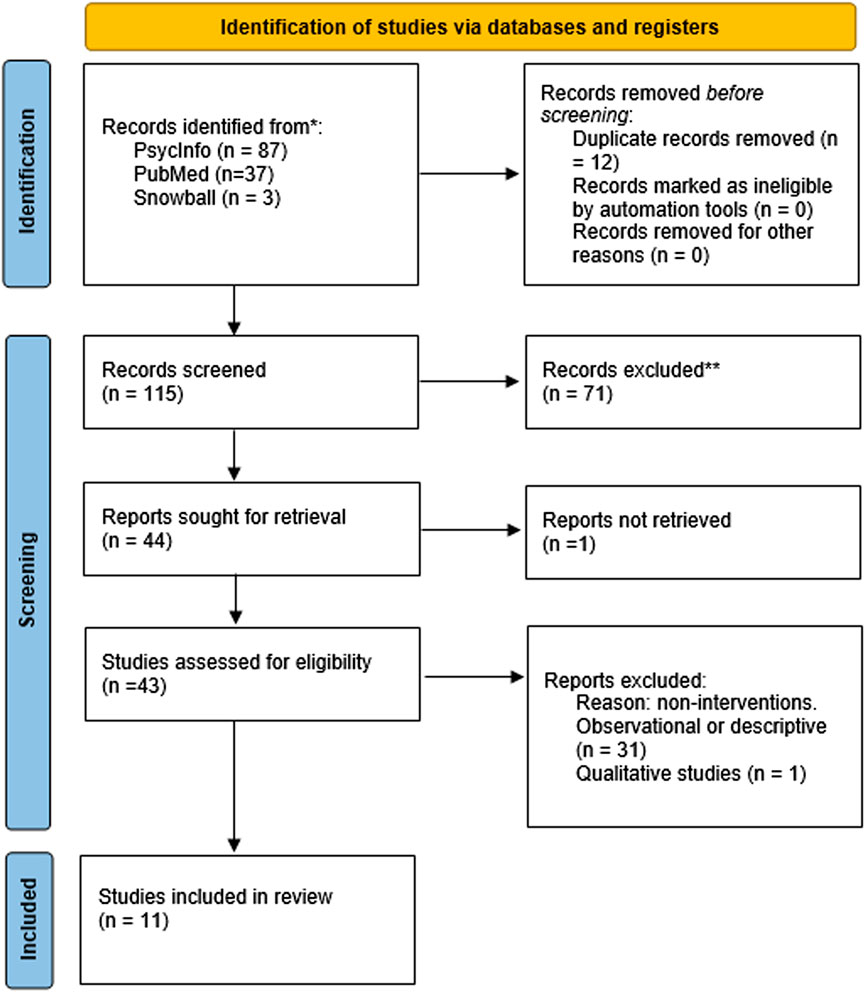
FIGURE 1. PRISMA flow diagram of the process of identifying and selecting and studies for the review. Reproduced from Page et al. (2021), licensed under CC-BY 4.0.
Starting with the 126 studies initially located with the search engines, 12 were removed for being duplicated, and therefore 114 studies were left. After a quick view, 71 studies were removed for various reasons (mainly due to lack of relevance to the study topic). Careful reading of the remaining 43 studies was carried out. Out of these 43 studies left, 31 were excluded because they were not intervention studies, and 1 because it was a qualitative study, therefore not meeting an inclusion criterion. Instead, they were observations of the issue or reviews. Lastly, 1 study had to be excluded because we could not find the full article (Wu and Chen, 2022), and therefore could not include it in the review. Finally, 11 studies met all of the eligibility criteria and were included in the review.
Results are represented in three different tables. In Table 3, relevant information of the review is represented (i.e., Study’s research design, Type of study population—forensic or community, Number of participants, Age range of participants, Gender of participants, Type of outcome, Measures/Instruments used, Conclusions, Type of intervention, Length of treatment with VR, Length of control group intervention, Type of control group). Overall, studies represent 539 participants of a wide range of ages (i.e., university students, high school students, students, and participants in community ranging from 14 to 63 years old). 8 of the 11 studies recruited participants from the community, while 3 focused on offenders. Moreover, none of the studies directly stated or asked for participants’ sexual orientation, although heterosexuality can be assumed by having male participants watch female victim avatars. In regards to gender, six studies recruited only male participants, two studies only female participants, and two studies recruited both males and females. One study did not specify the gender of the participants, but they did state they were recruiting offenders from a forensic center (Klein Tuente et al., 2020).
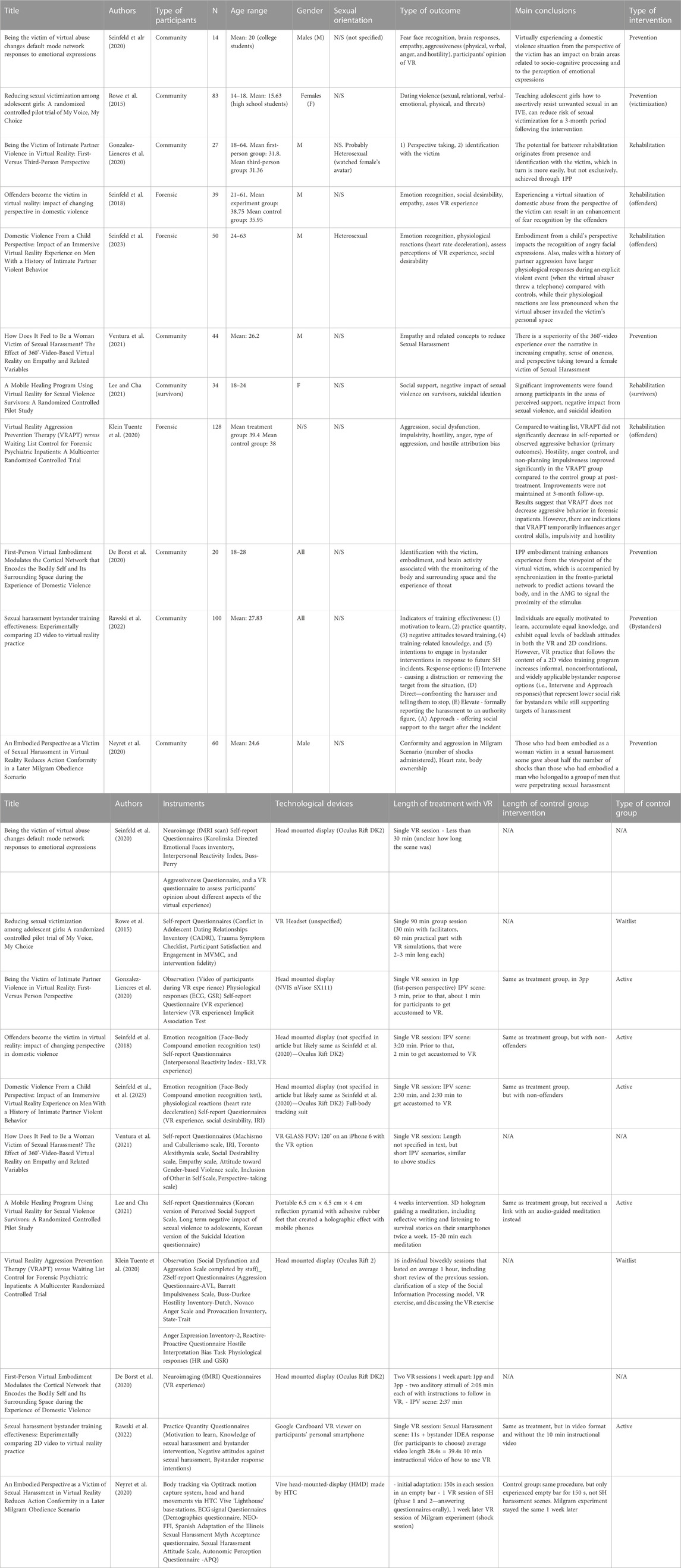
TABLE 3. Main results.
In terms of gender effects on outcome, working with male patients/female patients (i.e., previous experience with IPV) cannot be compared, since for the studies recruiting forensic participants, only men were recruited as offenders, not women. Women “patients” (i.e., having experienced IPV) were recruited for studies with survivors, which did not include any men.
Regarding male or female non-clinical participants (i.e., community, no previous experience in IPV), gender differences were not analyzed in either of the studies (De Borst et al., 2020; Rawski et al., 2022). However, in De Borst et al. (2020), it is stated that it could be interesting to investigate whether for female participants it is easier to place themselves in the victims’ shoes than for the male participants.
In terms of the measures being used, three studies included a measure of intimate partner violence (both physical or psychological) or aggression (Rowe et al., 2015; Klein Tuente et al., 2020; Seinfeld et al., 2020). It is important to note that all three studies had a slightly different focus. The first two studies focused specifically on the prevention of dating violence targeted towards community participants. However, the interventions used VR differently. While Seinfeld et al. (2020) focused on exploring the brain responses, aggressive behaviors and attitudes of male college students with low sensitivity to recognize female fearful faces, Rowe et al. (2015) focused on increasing assertive behaviors from teenage girls. Lastly, Klein Tuente et al. (2020) focused on the rehabilitation of offenders directly targeting aggressive behavior. While the reduction of aggressive behavior is a common goal in all IPV rehabilitation (i.e., treatment) studies, some assessed it using more indirect measures. VR offers the opportunity to literally feel like you are in someone else’s shoes, so these latter studies targeted empathy, perspective taking, and emotion recognition, a common practice within IPV, since these constructs are indirectly linked to aggressive behavior. Three rehabilitation studies (Seinfeld et al., 2018; Gonzalez-Liencres et al., 2020; Seinfeld et al., 2023) and three prevention studies (De Borst et al., 2020; Seinfeld et al., 2020; Ventura et al., 2021) have included these measures through interventions using embodiment of a female victim. Lastly et al., 2020 used VR in order to measure if prior embodiment with the victim of a sexual harassment situation could modify conformity when administering shocks to a woman. According to the authors, this could suggest that body ownership over a virtual body introduces another level of psychological proximity which contributes to the concept of shared identity (Neyret et al., 2020). The more we relate to someone, the more willing we are to help them (Levine et al., 2005; Slater et al., 2013).
In terms of the type of intervention, seven studies focused on prevention, and five studies focused on rehabilitation. While most prevention studies focused on increasing assertiveness skills and empathy to prevent being the victim or the offender of IPV or sexual harassment (Ventura et al., 2021; Rowe et al., 2015; De Borst et al., 2020), one study sought to help reduce sexual harassment by training bystanders (Rawski et al., 2022), and another one focused on trying to explore group aggression and bystander behavior through embodiment with a victim of sexual harassment (Neyret et al., 2020). Regarding rehabilitation studies, most were done with the purpose of reducing offenders’ risk of IPV or aggressive behavior (Seinfeld et al., 2018; Gonzalez-Liencres et al., 2020; Klein Tuente et al., 2020; Seinfeld et al., 2023), while one study focused on the rehabilitation of sexual violence survivors (Lee and Cha, 2021).
Regarding types of participants, the studies could be divided into either community (i.e., with no prior history of perpetuating IPV) (eight studies) or forensic (i.e., participants with history of perpetuating IPV—offenders) (three studies). Among those who had recruited participants from the community, one study specifically recruited women who had been survivors of IPV (“Community (survivors)” on the table). Among those who had recruited offenders, one study specifically recruited men who were inpatients at the time of the study, while the other two recruited men who were convicted and sentenced to attend a domestic violence intervention program. Regarding VR treatment length, most studies included a single VR session, where participants embodied an avatar for a few minutes and experiencing an IPV scene as a victim through the eyes of the avatar (Seinfeld et al., 2020; Gonzalez-Liencres et al., 2020; Seinfeld et al., 2018; Seinfeld et al., 2023; Ventura et al., 2021, De Borst et al., 2020). In Rawski et al., 2022 one short training session was also used, but participants watched the situation as a bystander. Additionally, in Neyret et al., 2020, participants encountered a different VR scenario in two different days, one in which they were either a woman victim of sexual harassment, or part of a group of men who were perpetrating the harassment, and the other virtual environment where they had to decide whether to obey the virtual experimenter’s orders of shocking a woman for getting answers wrong. On the other hand, in Klein Tuente et al., 2020, participants had several sessions and VR was used as a way for them to learn new social skills. The environment and interactions were controlled by the therapist, so treatment was more personalized than in other studies. Similarly, in Lee and Cha, 2021, VR was used as a way of delivering meditation exercises also during several weeks.
4 Discussion and conclusion
Focusing on the question at hand (i.e., which effective VR interventions exist for the prevention and rehabilitation of IPV), we can extract several conclusions from the analyzed studies.
4.1 VR and empathy
First, virtually experiencing a domestic violence situation from the perspective of the victim can result in an enhancement of fear recognition in female faces, both in forensic and in community population (Seinfeld et al., 2018; Seinfeld et al., 2020). Moreover, this type of experience is able to physically change brain areas that are related to socio-cognitive processing and to the perception of emotional expressions (Seinfeld et al., 2018; Seinfeld et al., 2020; De Borst et al., 2020). Thus, VR could be a useful tool to increase empathy in those who might have it underdeveloped, and therefore reduce intimate partner violence. Moreover, the effect of perspective taking and identification with the victim is more easily achieved if the participant directly embodies the victim from first-person perspective than if they are merely observing the scene as a third-person (Gonzalez-Liencres et al., 2020). However, third-person perspective can still have an effect as well, especially if participants are indirectly affected by the violence even if it is not directly targeted at them. In fact, when participants embody a child that is put in a situation of abuse and violence from the father avatar to the mother avatar, where they are standing next to the mother, there is an increase in emotion recognition of angry faces and physiological reactions (Seinfeld et al., 2023). Emotion recognition outcomes are important as they can increase the ability to empathize with the victim and therefore decrease perpetration. The effect that VR has on the increasing empathy and perspective taking is higher than simply reading about a situation and imagining it is happening to them (Ventura et al., 2021). VR has also been used to attempt to change implicit gender bias, with participants embodying a gender different than their own and experiencing sexual harassment, and has shown promising results (Wu and Chen, 2022).
4.2 VR and aggressive behavior
While the positive effect of VR in perspective taking, emotion recognition and identification with the victim is clear, evidence is mixed regarding a decrease on actual aggressive behavior. A study by Klein Tuente et al. showed that self-reported or observed aggressive behavior did not significantly decrease with VR compared to a control group. Moreover, while VR does seem to decrease hostility, anger control, and non-planning impulsiveness, these effects are not maintained in time (Klein Tuente et al., 2020; Neyret et al., 2020) suggested that by allowing participants to take part in being a woman victim of sexual harassment by a group of men, and then being asked by a group of men to harm another woman, they could psychologically identify with the woman, become aware of the illegitimacy of the behavior of the perpetrators of sexual harassment, and thus avoid doing such behavior.
4.3 VR and assertiveness
VR is a useful tool to train individuals to act more assertively in situations of sexual violence, reducing the risk of sexual victimization, psychological victimization, and psychological distress (Rowe et al., 2015). However, no significant reduction of risk was observed for physical violence or threats. Future studies could expand this finding and apply VR to reduce other kinds of violence.
4.4 VR and bystander behavior
Regarding the effect of VR in bystander behavior, participants in the VR group were more likely than the video group to report intentions to engage in indirect, non-confrontational interventions, such as “intervening” (i.e., causing a distraction or removing the target from the situation), or “approaching” (i.e., offering social support to the target after the incident) (Rawski et al., 2022). In fact, a recent review by Park and Kim (2023) concluded that traditional offline methods, VR, and web-based methods significantly improved bystander outcomes (i.e., awareness, definition, responsibility, bystander efficacy, gender norms/attitudes, intention to intervene, and action to intervene), while videos did not.
4.5 Implications and future directions
There are several implications to this review.
First, studies that focused on rehabilitation interventions in the forensic context have shown that VR could be a potential tool to reduce recidivism by increasing empathy within the forensic population (Seinfeld et al., 2018; Gonzalez-Liencres et al., 2020; Seinfeld et al., 2018; Seinfeld et al., 2023; Ventura et al., 2021; De Borst et al., 2020). However, we would need future longitudinal studies following the forensic population to see whether these interventions directly have an effect on recidivism. Furthermore, it is important to mention the difficulty of running interventions within rehabilitation programs within the forensic setting, which is one explanation for the short number of articles found. Participants in most rehabilitation interventions included in this review are forensic population, that are usually in prison and difficult to be motivated to do the intervention voluntarily. Therefore, those participants typically want to be part of the rehabilitation program in general, and more specifically do the VR intervention, to show an improvement in their behavior and rehabilitation and thus, to obtain prison benefits (e.g., permission to go out). As such, this population tends to rate high on social desirability, reducing the reliability of the studies. In treating this kind of population, indirect interventions such as the VR we have seen in this review, become even more advantageous (Sanz Fernández et al., 2018; Seinfeld et al., 2018; Johnston, 2021). Future research should include more VR interventions in the context of rehabilitation programs in the community setting to be able to compare its impact in the community vs. in a forensic setting.
Second, in this review we have seen how different usages of VR can be advantageous for specific population groups. Specifically, using VR as a prevention tool has proven to be effective with young adults (Rowe et al., 2015; Neyret et al., 2020; Seinfeld et al., 2020; Lee and Cha, 2021; Rawski et al., 2022). Institutions could benefit from using VR in educational settings in order to reduce psychological violence (increasing empathy), prevent victimization (assertiveness training), decrease sexual harassment, and increase bystander behavior.
Third, studies mentioned in this review have shown that VR can change implicit gender bias (Wu and Chen, 2022). This is a crucial result to design interventions that would tackle gender stereotypes and promote gender equality. More studies are needed that use VR to change implicit gender bias. It is important that those studies include both genders in order to be able to detect the impact of the intervention and possible gender differences. Similarly, only men were recruited as offenders when applying the intervention with forensic participants, and only women for studies with survivors. Future research should attempt to recruit both genders for studies with offenders and with survivors in order to assess any gender differences.
Fourth, and along the same lines, studies should aim at being more diverse, especially in terms of sexual orientation. Future research should take sexual orientation into account, include participants who are homosexual and bisexual, and study the impact of the intervention and possible sexual orientation differences.
Fifth, while quantitative studies inform us of the results in a general sense, future research should also include qualitative studies to be able to specifically see the impact of VR on an individual level, and thus have a more comprehensive idea of the effect of VR on IPV. Along the same lines, it is crucial to include behavioral changes measures to assess reduction in violent behavior (in terms of both aggression and victimization).
Lastly, both the context and the duration of the VR intervention are important factors to consider, as they might have an impact on the final results. In regards to the context, we would need to see whether the intervention mainly only uses VR, or if it is included in a longer/more comprehensive intervention in the context of a rehabilitation or prevention program. In terms of the duration of the VR intervention, we have to consider whether it is a one-off intervention lasting a few hours or whether it is a longer intervention, spanning multiple days. Future research should include longer interventions to obtain a higher effect, as well as tailor them to specific target groups, according to the results found in Klein Tuente et al. (2020).
A similar narrative review by Johnston et al. (2023) was recently published about this topic, focusing on the effectiveness of embodiment and perspective taking in general, and more specifically in IPV. Johnston et al. (2023) concluded that the integration of validated VR embodiment technology inspired by neuroscience could positively contribute to IPV rehabilitation processes. Our present study has built on the result of Johnston et al. (2023) by conducting a systematic review to analyze the studies that have used VR in the context of IPV. Both Johnston et al. (2023)’s study and the present study give a comprehensive understanding of the use of VR in contexts of IPV.
4.6 Conclusion
Overall, there are few interventions using VR to tackle the prevention or rehabilitation of IPV, and many still use more traditional approaches. The specific strategies and content used to reduce IPV is different in VR compared with more traditional IPV interventions. As mentioned previously, in most VR interventions the main focus was more on indirectly changing attitudes and enhancing emotional recognition by experiencing being a victim themselves, or part of an abusive scene, through embodiment (i.e., implicit interventions) (Seinfeld et al., 2018; Gonzalez-Liencres et al., 2020; Neyret et al., 2020; Seinfeld et al., 2023; Ventura et al., 2021; De Borst et al., 2020).
In contrast, as mentioned in the introduction, most of the traditional interventions or online programs, were focused on directly training participants on the identification of healthy relationships, and on the development of techniques of conflict resolution, empathy, anger management, making decisions, assertiveness, communication skills, psychoeducation about dating violence and emotion regulation strategies (i.e., explicit interventions) (Arango et al., 2014; Sygel et al., 2014; Levesque et al., 2016; Ellsberg et al., 2018; Kearney, 2018; Draucker et al., 2019; Peskin et al., 2019; Doss et al., 2020; Gibbs et al., 2020). Specifically, some of these studies that do not use VR are still using technology, showing several videos (mostly as part of a broader online or computer program) in order to model behavior, train perspective taking, or educate participants in what should not be done (Sygel et al., 2014; Levesque et al., 2016; Kearney, 2018; Draucker et al., 2019; Peskin et al., 2019; Doss et al., 2020). These technological interventions have overall proven more useful to tackle intimate partner violence than traditional non-technological educational interventions, although the effects have mostly been seen as a reduction of psychological violence, and not physical violence (Sygel et al., 2014; Levesque et al., 2016; Kearney, 2018; Draucker et al., 2019; Peskin et al., 2019; Doss et al., 2020).
However, although these programs have effect sizes similar to VR interventions (Sygel et al., 2014; Rowe et al., 2015; Levesque et al., 2016; Kearney, 2018; Seinfeld et al., 2018; Draucker et al., 2019; Peskin et al., 2019; Doss et al., 2020; Gonzalez-Liencres et al., 2020; Klein Tuente et al., 2020; De Borst et al., 2020; Seinfeld et al., 2020; Lee and Cha, 2021; Ventura et al., 2021; Rawski et al., 2022; Seinfeld et al., 2023), future research should evaluate whether the immersive aspect of VR, and more specifically the increased outcomes of perspective taking achieved with embodiment, has a significant added value in reducing aggressive behavior compared to those more traditional non-immersive video programs by comparing them in equal conditions.
Author contributions
AB-A: Conceptualization, Investigation, Writing–original draft, Writing–review and editing. BV: Conceptualization, Methodology, Writing–review and editing. CP-T: Writing–review and editing. J-ML: Writing–review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Pre-doctoral grant FI: 2022 FI_B1 00192. This work was supported by Grant PID2022-141403NB-I00 funded by MCIN/AEI/10.13039/501100011033/FEDER, UE.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2023.1263545/full#supplementary-material
References
Albarracín, D., Gillette, J. C., Earl, A. N., Glasman, L. R., Durantini, M. R., and Ho, M. H. (2005). A test of major assumptions about behavior change: a comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychol. Bull. 131 (6), 856–897. doi:10.1037/0033-2909.131.6.856
Anderson, E. J., Krause, K. C., Meyer Krause, C., Welter, A., McClelland, D. J., Garcia, D. O., et al. (2021). Web-based and mHealth interventions for intimate partner violence victimization prevention: a systematic review. Trauma, violence and abuse 22 (4), 870–884. doi:10.1177/1524838019888889
Arango, D., Morton, M., Gennari, F., Kiplesund, S., Contreras, M., and Ellsberg, M. (2014). Interventions to reduce or prevent violence against women and girls: a systematic review of reviews. Washington, DC: Women’s Voice, Agency and Participation Research Series, World Bank. doi:10.13140/RG.2.1.2545.6168
Arborelius, L., Fors, U., Svensson, A.-K., Sygel, K., and Kristiansson, M. (2013). A new interactive computer simulation system for violence risk assessment of mentally disordered violent offenders. Crim. Behav. Ment. Health 23 (1), 30–40. doi:10.1002/cbm.1849
Babcock, J. C., Green, C. E., and Robie, C. (2004). Does batterers' treatment work? A meta-analytic review of domestic violence treatment. Clin. Psychol. Rev. 23 (8), 1023–1053. doi:10.1016/j.cpr.2002.07.001
Baños, R. M., Guillen, V., Quero, S., Garcia-Palacios, A., Alcañiz, M., and Botella, C. (2011). A virtual reality system for the treatment of stress-related disorders: a preliminary analysis of efficacy compared to a standard cognitive behavioral program. Int. J. Hum. Comput. Stud. 69, 602–613. doi:10.1016/j.ijhcs.2011.06.002
Banyard, V., Plante, E., and Moynihan, M. (2004). Bystander education: bringing a broader community perspective to sexual violence prevention. J. Community Psychol. 32, 61–79. doi:10.1002/jcop.10078
Banyard, V. L., Moynihan, M. M., and Plante, E. G. (2007). Sexual violence prevention through bystander education: an experimental evaluation. J. Community Psychol. 35 (4), 463–481. doi:10.1002/jcop.20159
Bell, B., Kanar, A., and Kozlowski, S. (2008). Current issues and future directions in simulation-based training in North America. Int. J. Hum. Resour. Manag. 19, 1416–1434. doi:10.1080/09585190802200173
Bordnick, P. S., Carter, B. L., and Traylor, A. C. (2011). What virtual reality research in addictions can tell us about the future of obesity assessment and treatment. J. Diabetes Sci. Technol. 5 (2), 265–271. doi:10.1177/193229681100500210
Botella, C., Garcia-Palacios, A., Baños, R., and Quero, S. (2007). ISSN 1695-4238, No. 82, 2007 (ejemplar dedicado a: psicoterapia y nuevas tecnologías. Parte II). Real. virtual Trat. psicológicos. Cuad. Med. Psicosomática Psiquiatr. Enlace 17-31, 82.
Botezatu, M., Hult, H., Tessma, M. K., and Fors, U. (2010). Virtual patient simulation: knowledge gain or knowledge loss? Med. Teach. 32 (7), 562–568. doi:10.3109/01421590903514630
Butters, R. P., Droubay, B. A., Seawright, J. L., Tollefson, D. R., Lundahl, B., and Whitaker, L. (2021). Intimate partner violence perpetrator treatment: tailoring interventions to individual needs. Clin. Soc. Work J. 49, 391–404. doi:10.1007/s10615-020-00763-y
Cantos, A., Goldstein, D., Brenner, L., O’Leary, K., and Verborg, R. (2015). Correlates and program completion of family only and generally violent perpetrators of intimate partner violence. Behav. Psychology/Psicologia Conduct. 23 (3), 549–569.
Courteille, O., Bergin, R., Stockeld, D., Ponzer, S., Fors, U., et al. (2008). The use of a virtual patient case in an OSCE-based exam--a pilot study. Med. Teach. 30 (3), e66–e76. doi:10.1080/01421590801910216
Doss, B., Knopp, K., Roddy, M., Rothman, K., Hatch, G., and Rhoades, G. (2020). Online programs improve relationship functioning for distressed low-income couples: results from a nationwide randomized controlled trial. J. Consult. Clin. Psychol. 88, 283–294. doi:10.1037/ccp0000479
De Borst, A. W., Sanchez-Vives, M. V., Slater, M., and Gelder, B. de. (2020). First-person virtual embodiment modulates the cortical network that encodes the bodily self and its surrounding space during the experience of domestic violence. eNeuro 7 (3). doi:10.1523/ENEURO.0263-19.2019
Draucker, C. B., Martsolf, D. S., Crane, S., McCord, A. L., Romero, L., and Al-Khattab, H. A. (2019). A feasibility test of an online intervention to prevention dating violence in emerging adults. Archives Psychiatric Nurs. 33 (1), 37–45. doi:10.1016/j.apnu.2018.09.002
Ellsberg, M., Arango, D. J., Morton, M., Gennari, F., Kiplesund, S., Contreras, M., et al. (2015). Prevention of violence against women and girls: what does the evidence say? Lancet (London, Engl. 385 (9977), 1555–1566. doi:10.1016/S0140-6736(14)61703-7
Ellsberg, M., Ullman, C., Blackwell, A., Hill, A., and Contreras, M. (2018). “What works to prevent adolescent intimate partner and sexual violence? A global review of best practices,” in Adolescent dating violence: theory, research, and prevention. Editors D. A. Wolfe, and J. R. Temple (Elsevier Academic Press), 381–414. doi:10.1016/B978-0-12-811797-2.00016-5
Foubert, J. D. (2000). The longitudinal effects of a rape-prevention program on fraternity men's attitudes, behavioral intent, and behavior. J. Am. Coll. health J ACH 48 (4), 158–163. doi:10.1080/07448480009595691
Fox, J., Arena, D., and Bailenson, J. N. (2009). Virtual reality: a survival guide for the social scientist. J. Media Psychol. Theor. Methods, Appl. 21 (3), 95–113. doi:10.1027/1864-1105.21.3.95
Gibbs, A., Washington, L., Abdelatif, N., Chirwa, E., Willan, S., Shai, N., et al. (2020). Stepping Stones and creating futures intervention to prevent intimate partner violence among young people: cluster randomized controlled trial. J. Adolesc. health official Publ. Soc. Adolesc. Med. 66 (3), 323–335. doi:10.1016/j.jadohealth.2019.10.004
Glass, N., Clough, A., Case, J., Hanson, G., Barnes-Hoyt, J., Waterbury, A., et al. (2015). A safety app to respond to dating violence for college women and their friends: the MyPlan study randomized controlled trial protocol. BMC Public Health 15 (1), 871. doi:10.1186/s12889-015-2191-6
Gondolf, E. W. (2007). Theoretical and research support for the Duluth model: a reply to dutton and corvo. Aggress. Violent Behav. 12 (6), 644–657. doi:10.1016/j.avb.2007.03.001
Gonzalez-Liencres, C., Zapata, L. E., Iruretagoyena, G., Seinfeld, S., Perez-Mendez, L., Arroyo-Palacios, J., et al. (2020). Being the victim of intimate partner violence in virtual reality: first- versus third-person perspective. Front. Psychol. 11, 820. doi:10.3389/fpsyg.2020.00820
Heise, L. (2011). What works to prevent partner violence? An evidence overview. London, England: Department for International Development.
Holtzworth-Munroe, A., and Meehan, J. C. (2004). Typologies of men who are maritally violent. J. Interpers. Violence 19 (12), 1369–1389. doi:10.1177/0886260504269693
Johnston, T. (2021). Assessment, prevention and rehabilitation of intimate partner violence through immersion in virtual reality. Modifying Cognitions, Emotions and Behaviours through Embodied Perspective Taking. Doctoral dissertation. Spain: University of Barcelona.
Johnston, T., Seinfeld, S., Gonzalez-Liencres, C., Barnes, N., Slater, M., and Sanchez-Vives, M. V. (2023). Virtual reality for the rehabilitation and prevention of intimate partner violence - from brain to behavior: a narrative review. Front. Psychol. 13, 788608. doi:10.3389/fpsyg.2022.788608
Katz, J., and Moore, J. (2013). Bystander education training for campus sexual assault prevention: an initial meta-analysis. Violence Vict. 28 (6), 1054–1067. doi:10.1891/0886-6708.vv-d-12-00113
Kearney, M. S. (2018). Educating men to recognize warning signs of dating violence. doi:10.13016/6bps-hqqbAppealing to masculinity or empathy?
Kip, H., Bouman, Y. H. A., Kelders, S. M., and van Gemert-Pijnen, L. J. E. W. C. (2018). eHealth in treatment of offenders in forensic mental health: a review of the current state. Front. Psychiatry 9, 42. doi:10.3389/fpsyt.2018.00042
Kip, H., Oberschmidt, K., and Bierbooms, J. (2020). eHealth technology in forensic mental healthcare: recommendations for achieving benefits and overcoming barriers. Int. J. Forensic Ment. Health 20, 31–47. doi:10.1080/14999013.2020.1808914
Kleinsasser, A., Jouriles, E. N., McDonald, R., and Rosenfield, D. (2015). An online bystander intervention program for the prevention of sexual violence. Psychol. Violence 5 (3), 227–235. doi:10.1037/a0037393
Klein Tuente, S., Bogaerts, S., Bulten, E., Keulen-de Vos, M., Vos, M., Bokern, H., et al. (2020). Virtual reality aggression prevention therapy (VRAPT) versus waiting list control for forensic psychiatric inpatients: a multicenter randomized controlled trial. J. Clin. Med. 9 (7), 2258. doi:10.3390/jcm9072258
Lee, M. R., and Cha, C. (2021). A mobile healing program using virtual reality for sexual violence survivors: a randomized controlled pilot study. Worldviews evidence-based Nurs. 18 (1), 50–59. doi:10.1111/wvn.12478
Levesque, D. A., Johnson, J. L., Welch, C. A., Prochaska, J. M., and Paiva, A. L. (2016). Teen dating violence prevention: cluster-randomized trial of teen choices, an online, stage-based program for healthy, nonviolent relationships. Psychol. Violence 6 (3), 421–432. doi:10.1037/vio0000049
Levine, M., Prosser, A., Evans, D., and Reicher, S. (2005). Identity and emergency intervention: how social group membership and inclusiveness of group boundaries shape helping behavior. Personal. Soc. Psychol. Bull. 31, 443–453. doi:10.1177/0146167204271651
Maples-Keller, J. L., Bunnell, B. E., Kim, S. J., and Rothbaum, B. O. (2017). The use of virtual reality technology in the treatment of anxiety and other psychiatric disorders. Harv. Rev. psychiatry 25 (3), 103–113. doi:10.1097/HRP.0000000000000138
Martínez, J. A., and Rey, C. A. (2014). Prevención de violencia en el noviazgo: una revisión de programas publicados entre 1990 y 2012. Pensam. Psicológico 12 (1), 117–132. doi:10.11144/Javerianacali.PPSI12-1.pvnr
McMahon, S., Postmus, J. L., and Koenick, R. A. (2011). Conceptualizing the engaging bystander approach to sexual violence prevention on college campuses. J. Coll. Student Dev. 52 (1), 115–130. doi:10.1353/csd.2011.0002
McMahon, S., Postmus, J. L., Warrener, C., and Koenick, R. A. (2014). Utilizing peer education theater for the primary prevention of sexual violence on college campuses. J. Coll. Student Dev. 55 (1), 78–85. doi:10.1353/csd.2014.0001
Neyret, S., Navarro, X., Beacco, A., Oliva, R., Bourdin, P., Valenzuela, J., et al. (2020). An embodied perspective as a victim of sexual harassment in virtual reality reduces action conformity in a later Milgram obedience scenario. Sci. Rep. 10, 6207. doi:10.1038/s41598-020-62932-w
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I, Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Pantziaras, I., Courteille, O., Mollica, R., Fors, U., and Ekblad, S. (2012). A pilot study of user acceptance and educational potentials of virtual patients in transcultural psychiatry. Int. J. Med. Educ. 3, 132–140. doi:10.5116/ijme.5004.7c78
Park, S., and Kim, S.-H. (2023). A systematic review and meta-analysis of bystander intervention programs for intimate partner violence and sexual assault. Psychol. Violence 13 (2), 93–106. doi:10.1037/vio0000456
Pence, E., and Paymar, M. (1993). Education groups for men who batter: the Duluth model. Springer Publishing Company. doi:10.1891/9780826179913
Peskin, M. F., Markham, C. M., Shegog, R., Baumler, E. R., Addy, R. C., Temple, J. R., et al. (2019). Adolescent dating violence prevention program for early adolescents: the me and you randomized controlled trial, 2014–2015. Am. J. Public Health 109 (10), 1419–1428. doi:10.2105/AJPH.2019.305218
Rawski, S. L., Foster, J. R., and Bailenson, J. (2022). Sexual harassment bystander training effectiveness: experimentally comparing 2D video to virtual reality practice. Technol. Mind, Behav. 3 (2). Summer 2022). doi:10.1037/tmb0000074
Repetto, C., Gaggioli, A., Pallavicini, F., Cipresso, P., Raspelli, S., and Riva, G. (2013). Virtual reality and mobile phones in the treatment of generalized anxiety disorders: a phase-2 clinical trial. Personal Ubiquitous Comput. 17, 253–260. doi:10.1007/s00779-011-0467-0
Riva, G. (2009). Is presence a technology issue? Some insights from cognitive sciences. Virtual Real. 13, 159–169. doi:10.1007/s10055-009-0121-6
Rothbaum, B. O., Anderson, P., Zimand, E., Hodges, L., Lang, D., and Wilson, J. (2006). Virtual reality exposure therapy and standard (in vivo) exposure therapy in the treatment of fear of flying. Behav. Ther. 37 (1), 80–90. doi:10.1016/j.beth.2005.04.004
Rowe, L. S., Jouriles, E. N., and McDonald, R. (2015). Reducing sexual victimization among adolescent girls: a randomized controlled pilot trial of my voice, my choice. Behav. Ther. 46 (3), 315–327. doi:10.1016/j.beth.2014.11.003
Sanz Fernández, J., Navarro Montes, R., Fausor de Castro, R., Altungy, P., Gesteira Santos, C., Morán Rodríguez, N., et al. (2018). La escala de deseabilidad social de Marlowe-Crowne como instrumento para la medida de la deseabilidad social, la sinceridad y otros constructos relacionados en psicología legal y forense. Piscopatología Clínica Leg. Forense 18, 112–133.
Saunders, D. G. (1996). Feminist-cognitive-behavioral and process-psychodynamic treatments for men who batter. Violence Vict. 4, 393–414. doi:10.1891/0886-6708.11.4.393
Seinfeld, S., Arroyo-Palacios, J., Iruretagoyena, G., Hortensius, R., Zapata, L. E., Borland, D., et al. (2018). Offenders become the victim in virtual reality: impact of changing perspective in domestic violence. Sci. Rep. 8 (1), 2692. doi:10.1038/s41598-018-19987-7
Seinfeld, S., Hortensius, R., Arroyo-Palacios, J., Iruretagoyena, G., Zapata, L. E., de Gelder, B., et al. (2023). Domestic violence from a child perspective: impact of an immersive virtual reality experience on men with a history of intimate partner violent behavior. J. Interpers. violence 38 (3-4), 2654–2682. doi:10.1177/08862605221106130
Seinfeld, S., Zhan, M., Poyo-Solanas, M., Barsuola, G., Vaessen, M., Slater, M., et al. (2020). Being the victim of virtual abuse changes default mode network responses to emotional expressions. Cortex 135, 268–284. doi:10.1016/j.cortex.2020.11.018
Slater, M., Rovira, A., Southern, R., Swapp, D., Zhang, J. J., Campbell, C., et al. (2013). Bystander responses to a violent incident in an immersive virtual environment. PLOS ONE 8 (1), e52766. doi:10.1371/journal.pone.0052766
Slater, M., and Sanchez-Vives, M. V. (2016). Enhancing our lives with immersive virtual reality. Front. Robot. AI 3, 74. doi:10.3389/frobt.2016.00074
Stuart, G. L., Temple, J. R., and Moore, T. M. (2007). Improving batterer intervention programs through theory-based research. JAMA 298 (5), 560–562. doi:10.1001/jama.298.5.560
Sygel, K., Kristiansson, M., Furberg, R., and Fors, U. (2014). Reactions on display/intimate partner violence (RoD/IPV)—a study of a new interactive computer simulation program for the treatment of men convicted of intimate partner violence. Int. J. Forensic Ment. Health 13, 369–380. doi:10.1080/14999013.2014.951104
Sygel, K., and Wallinius, M. (2021). Immersive virtual reality simulation in forensic psychiatry and adjacent clinical fields: a review of current assessment and treatment methods for practitioners. Front. Psychiatry 12, 673089. doi:10.3389/fpsyt.2021.673089
Ticknor, B. (2019). Virtual reality and correctional rehabilitation: a game changer. Crim. Justice Behav. 46 (9), 1319–1336. doi:10.1177/0093854819842588
Trabold, M. M., Alsobrooks, W., Mittal, H., and Mittal, M. (2018). A systematic review of intimate partner violence interventions: state of the field and implications for practitioners. Trauma, Violence, and Abuse 21, 311–325. doi:10.1177/1524838018767934
Turner, W. A., and Casey, L. M. (2014). Outcomes associated with virtual reality in psychological interventions: where are we now? Clin. Psychol. Rev. 34 (8), 634–644. doi:10.1016/j.cpr.2014.10.003
Valmaggia, L. R., Latif, L., Kempton, M. J., and Rus-Calafell, M. (2016). Virtual reality in the psychological treatment for mental health problems: an systematic review of recent evidence. Psychiatry Res. 236, 189–195. doi:10.1016/j.psychres.2016.01.015
Ventura, S., Cardenas, G., Miragall, M., Riva, G., and Baños, R. (2021). How does it feel to Be a woman victim of sexual harassment? The effect of 360°-video-based virtual reality on empathy and related variables. Cyberpsychology, Behav. Soc. Netw. 24 (4), 258–266. doi:10.1089/cyber.2020.0209
Keywords: virtual reality, intimate partner violence, prevention, rehabilitation, immersive, domestic violence
Citation: Bastardas-Albero A, Vall B, Pérez-Testor C and Losilla J-M (2023) Which effective virtual reality (VR) interventions exist for the prevention and rehabilitation of intimate partner violence (IPV)?. Front. Virtual Real. 4:1263545. doi: 10.3389/frvir.2023.1263545
Received: 19 July 2023; Accepted: 09 November 2023;
Published: 21 December 2023.
Edited by:
Sofia Seinfeld, Open University of Catalonia, SpainReviewed by:
Peter Eachus, University of Salford, United KingdomFilippo Aschieri, Catholic University of the Sacred Heart, Italy
Copyright © 2023 Bastardas-Albero, Vall, Pérez-Testor and Losilla. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana Bastardas-Albero, YWRyaWFuYWJhQGJsYW5xdWVybmEudXJsLmVkdQ==