
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 02 October 2023
Sec. Technologies for VR
Volume 4 - 2023 | https://doi.org/10.3389/frvir.2023.1261093
This article is part of the Research TopicBeyond audiovisual: novel multisensory stimulation techniques and their applicationsView all 11 articles
 Belmir Jose De Jesus Junior1*
Belmir Jose De Jesus Junior1* Léa Perreault1,2
Léa Perreault1,2 Marilia K. S. Lopes1
Marilia K. S. Lopes1 Marie-Claude Roberge2
Marie-Claude Roberge2 Alcyr A. Oliveira3
Alcyr A. Oliveira3 Tiago H. Falk1*
Tiago H. Falk1*Introduction: Immersive virtual reality (VR) applications are burgeoning within healthcare as they promote high levels of engagement. Notwithstanding, existing solutions only stimulate two of our five senses (audio and visual), thus may not be optimal in the sense of promoting immersion and of “being present”. In this paper, we explore the benefits of an immersive multisensory experience as a therapeutic modality for participants suffering from post-traumatic stress disorder (PTSD).
Methods: In addition to 360-degree videos and corresponding natural sounds, nature smells are also presented by means of a portable ION 2 scent diffusion device attached to an Oculus Quest 2 VR head-mounted display. A 3-week 12-sessions protocol was applied to a sample of 20 participants diagnosed with PTSD.
Results and discussion: We report the outcomes seen from a battery of qualitative metrics, including cognitive functioning tests, psychological symptoms, severity of PTSD, and several self-reported questionnaires and heart rate variability (HRV) metrics. Results are compared not only between pre-and post intervention, but also after a 3-month follow-up period. Results suggest a decrease in the severity of PTSD, as well as improvements in processing speed and sustained attention post-intervention, but also sustained decrease in the severity of PTSD and in dissociative tendencies at the 3-month follow-up. Overall, participants rated the experience as highly immersive and produced very mild to no symptoms of cybersickness, thus corroborating the feasibility and usefulness of the proposed multisensory immersive VR tool for reducing PTSD symptoms.
Post-traumatic stress disorder (PTSD) is a mental health condition that results from experiencing or witnessing a traumatic life event. People suffering from PTSD may experience psychological symptoms such as intrusive thoughts, nightmares, flashbacks, hypervigilance, and severe anxiety. Cognitive functions might also be impaired, leading to attention and memory deficits. Furthermore, PTSD can lead to diminished physical health, debilitated social and daily functioning, decline in work performance and increase in demand for healthcare and mental health resources. Therefore, PTSD impacts not only the individual, but also their family, their community, and society in general (Shalev et al., 2017).
Even though extensive research has been conducted to reduce PTSD symptoms, its complexity and individual variations make the elaboration of treatments challenging. Exposure therapy, for example, has been regarded as a useful method to treat PTSD (Rauch et al., 2012). However, it still entails high dropout rates and insufficient accessibility to many patients. Some clinicians opt for other treatment methods, as exposing the patient to their trauma can be a distressing experience (Bomyea and Lang, 2012). Less invasive therapies also exist, such as relaxation training or eye movement desensitization and reprocessing (EMDR). However, the treatments have been found to be less efficacious than exposure therapy (Taylor et al., 2003). Therefore, the need for new therapeutic modalities that increase patient’s motivation and are clinically effective in diminishing PTSD symptoms is more present than ever. In response, modern technology has earned scientific interest in the past few years for its unique advantages and promising results.
Technological advances in computer graphics hardware, communications, and immersive media software have brought an ascension in computer-simulated environments, commonly referred to as virtual reality (VR). Today, applications of VR go beyond entertainment, and many treatment pathways are emerging in healthcare (Halbig et al., 2022). Within mental health research, VR has been used to treat phobias, addictions, attention deficit and hyperactivity disorder, autism spectrum disorder, and post-traumatic stress disorder (Freeman et al., 2017; Kothgassner et al., 2019; Emmelkamp and Meyerbröker, 2021). VR allows different stimuli to be invoked in immersive virtual worlds, which would often be hard or impossible to accomplish in a usual real-life treatment scenario (Rizzo and Shilling, 2017). A recent systematic review has shown that treatment delivered in an intense format, for example, with multiple or continuous sessions over 1 week, is effective and reduces the amount of time required to obtain its benefits, which in turn diminishes dropout rates (Ragsdale et al., 2020). The use of VR in the clinic and at home could allow for such intense sessions to be conducted and could be a good adjuvant to regular therapy, thus increasing the frequency of services for patients in need.
The use of VR immersive content to promote relaxation has also been investigated recently, not only among people suffering from mental health problems, but also among healthy individuals. For relaxation, most of the applications consist of exposing the subject to a relaxing environment, usually featuring nature content, or even using the content to induce a meditative state (Noronha and Campos, 2021; Lopes et al., 2022; Riches et al., 2023). In addition, nature immersion delivered by head-mounted displays (HMDs) has been self-reported as more relaxing than when they are delivered on a PC screen (Knaust et al., 2022). Recently, Mistry et al. (2020) reported that promoting relaxation through VR for PTSD patients increased positive affect. Although more positive affect was obtained from meditating with VR than in the non-VR condition, the authors emphasize the need for further exploration of VR to promote greater relaxation states. VR applications are known to induce a strong sense of presence in the user while immersed in the virtual environment, making them a useful tool for medical interventions, as they are more engaging and can increase participant’s motivation. One main limitation of existing VR systems is that they only stimulate two of our five senses and, thus, may be considered sub-optimal for immersion. Introducing smells into the VR content has been revealed to improve the sense of realism, presence, immersion and emotion in users (De Jesus Jr et al., 2022). Additionally, Lopes et al. (2022) showed the potential of multisensorial VR applications to promote greater relaxation states in healthy individuals. Furthermore, Aiken and Berry (2015) stated the possibility of translating the benefits of olfaction therapy to patients suffering from PTSD symptoms with the utilization of VR exposure therapy.
In this paper, we explore the use of multisensory nature immersion, where VR audio-visual nature scenes are combined with nature smells, as a new therapeutic modality for PTSD patients. In particular, we explore the benefits of multisensory VR on psychological, cognitive, and physiological symptoms of PTSD.
Data were collected from July 2022 to May 2023 at a clinic specializing in PTSD assessment and treatment located in Sept-Îles, QC, Canada. The Ethics Committee of Research with Human Beings (CER-22-669) from INRS (University of Québec) approved the study. The trial was registered under the ISRCTN registry identifier: ISRCTN68760993. Twenty-four subjects with a diagnosis of PTSD recognized by their family doctor were initially recruited. Twenty completed the protocol, as four participants withdrew from the study due to personal reasons. The remaining participants had an average age of 42.2 ± 11.35 years old. Most of the participants were male (65%), married (35%), with at least one child (65%), and holding a bachelor’s degree or higher education (40%). Sixty percent of the participants were not working due to disability. Table 1 displays a summary of the demographic characteristics of the participants. All participants were native French speakers or had an acceptable understanding of French. The nature of traumatic events in the sample included transportation accident (3), work accident (2), physical (5) or sexual aggression (5), war (2), witness of the death of another (1) and having or witnessing an injury or a sickness (2). Fifteen percent of participants declared only one traumatic event, whereas 25% identified two, 20% identified three, 5% identified four and 35% identified five or more. Eighty percent of participants followed psychotherapy during the intervention, and all participants had access to psychological support on their demand if they experienced mental distress due to the modality.
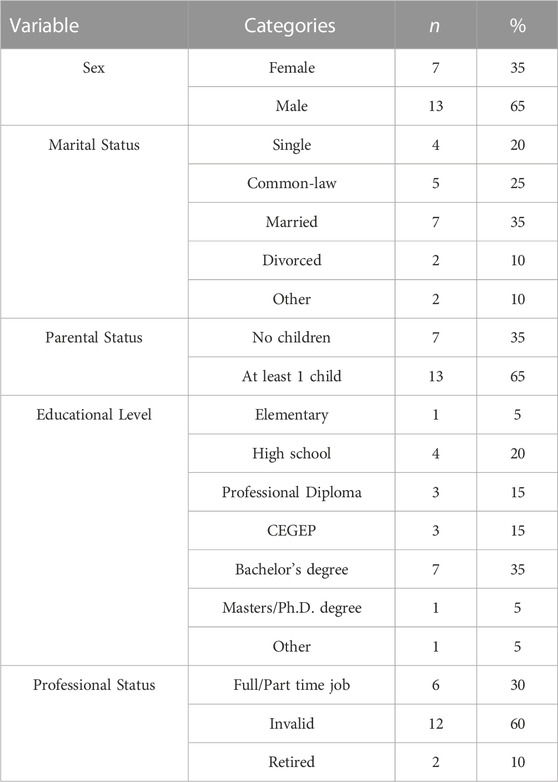
TABLE 1. Demographics of study participants. CEGEPs are exclusive to the Québec provincial education system and correspond to a vocational college.
Participants had to be over 18 years old, understand French, and have a PTSD diagnosis recognized by their doctors. They could not have a severe addiction, uncontrolled epilepsy or trauma linked with nature to participate. They provided their written and informed consent to take part in the experiment. Figure 1 depicts the protocol followed. At week 1 of the protocol, they were exposed to a short VR environment with olfactory stimuli to assess the presence of symptoms of so-called cybersickness (i.e., motion sickness caused by immersion in VR content) or any other impediment that could cause the exclusion of the participant from the experiment. Participants who could continue the protocol then proceeded to the first pretest phase, which was composed of a 30–45 min neurocognitive assessment (CNS Vital Signs, United States), a demographic questionnaire, four questionnaires measuring psychological symptoms and subjective distress, and a semi-structured interview administered by a trained psychologist to determine the symptoms and severity of PTSD (see Section 2.5). At the beginning and at the end of pretest 1, participants’ heart rate variability was assessed to measure the activation level of the autonomic nervous system with a one-minute heart rate variability test using the EmWave Pro Plus software (HeartMath, United States) (see Section 2.6).
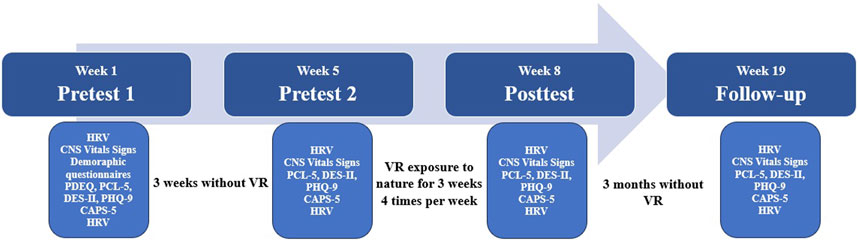
FIGURE 1. Protocol of VR nature immersion for each participant.
Next, a three-week period free of VR immersion was prescribed for every participant (those who followed psychotherapy continued as usual) to monitor changes in variables unrelated to the experiment. Then, 1 day before starting immersion in the multisensory VR environments, each subject completed a second pretest that included all the measures from the first pretest, except for the demographic questionnaire and the PDEQ questionnaire. The protocol itself was comprised of 12 sessions, distributed across 3 weeks, four times per week. Each session lasted 15 min and was comprised of three different virtual reality environments, each with a duration of 5 minutes (more details below). The order in which the participants viewed the environments was randomized per participant and per session to avoid possible biases. Once the participants finished all 12 sessions, they completed a posttest identical to the second pretest, as well as a three-month follow-up to evaluate the long-term effects of the protocol. At the end of each VR exposition session, participants also reported their sense of presence, immersion, and cybersickness using standard questionnaires (see Section 2.7).
A VR headset (Oculus Quest 2, Meta, United States) with 1832 × 1920 resolution, up to 120 Hz display refresh rate, and 90° field-of-view was used in our studies. The HMD was instrumented with electroencephalography (EEG), electrocardiography (ECG), facial electromyography (EMG), and electro-oculography (EOG) sensors following advice from Cassani et al. (2018, 2020). More specifically, the VR headset was instrumented with 16 ExG sensors connected to a wireless bioamplifier (OpenBCI Cyton/Daisy) operating at a sample rate of 125 Hz. EEG data were obtained from 12 channels where sensors were embedded in the foam and straps of the headset (i.e., Fp1, Fpz, Fp2, F3, F4, FCz, C3, C4, O1, O2, P3, and P4), four EOG electrodes were strategically placed on the foam of the headset (two pairs of horizontal and vertical electrodes to track eye activity), heart rate was obtained through PPG via a sensor that was placed on the left upper side of the visual foam, and two electrodes were placed on mastoids as a reference. In this work, we will focus only on experiment outcomes and leave the analyses of these biosignals for future exploration. Lastly, the olfactory stimulation was provided by an OVR ION2 scent diffuser device (OVR Technologies, United States) attached to the instrumented headset. The ION 2 device was calibrated to disperse up to nine different nature scents, out of which five were mainly used (flowers, earth dirt, forest, ocean breeze, and grass).
As mentioned above, each of the 12 sessions was comprised of three nature scenes chosen to promote relaxation. The first scene brought the participant to the shore of an in-mountain lake (Figure 2—first row). This scenario acted as a baseline for the nature immersion, as no other stimulus (guided meditation, relaxing music or breathing exercise) was added to the existing natural sounds and odours associated with the scenario. The second scenario depicted a local beach in Sept-Îles (QC, Canada), in which the participant was placed near the water. In this scenario, a cardiac coherence exercise was added to observe its effects on the level of relaxation in the natural environment. At every moment, the participant could synchronize their breathing with a sphere moving up and down at 5 seconds intervals (Figure 2—middle row). The third scenario also depicted a local rocky seaside location in Sept-Îles, surrounded by forest. The participant was guided by an audio-guided meditation female voice instructing them to focus on their breathing and relaxation (Figure 2—third row).

FIGURE 2. Captures from environment one (first row), two (second row), and three (third row). Environment one: Cabin Near Misty Lake, by Eric Fassbender. Licensed by Atmosphaeres. Environment two and three: Reproduced with permission from Martin Demassieux.
The French version of the Peritraumatic Dissociative Experiences Questionnaire (PDEQ) (Marmar et al., 2004) was used to assess if a dissociative episode occurred during and/or after the traumatic event that led to PTSD. Participants rate 10-items on a scale of 1 (1 = not at all true) to 5 (5 = extremely true) the presence of symptoms such as depersonalization, derealization, and amnesia that might have occurred during and/or after the event. A total score above 15 indicates significant dissociation. This instrument has shown satisfactory convergent validity [Pearson’s correlation (r) of 0.39–0.54] with other measures of PTSD, including PTSD diagnosis supported by CAPS-5 interview (Bomyea and Lang, 2012).
The French version of the Post-traumatic Stress Disorder Checklist (PCL-5) (Weathers et al., 1993); validated in French by Ashbaugh et al. (2016) was used to assess PTSD symptoms severity as perceived by the participants. The instrument consists of a 20-items questionnaire associated with each PTSD symptom as they appear in their respective clusters (intrusions, avoidance, changes in cognition and mood, and changes in reactivity). Patients rate each item on a scale from 0 (Not at all) to 4 (Extremely). The subjective endorsement of the necessary DSM-5 criterion for PTSD indicates a provisional diagnosis of PTSD, which usually sums up to a total score of 33 or higher. PCL-5 has shown average to strong internal consistency (Cohen’s alpha (α) of 0.94) and test-retest reliability (α = 0.89), as well as moderate to strong validity of construct and criterion, as shown by its correlation with the CAPS-5 (r = 0.90) and other measures of PTSD. It was also used in other studies to measure the subjective perception of changes in PTSD symptoms pre- and post-experiment (Forkus et al., 2022; Ashbaugh et al., 2016).
The French version of the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) (Weathers et al., 2018); validated in French by Rivest-Beauregard et al. (2022) was used to objectively assess PTSD symptoms severity based on the DSM-5 criteria. It is a semi-structured interview in which the clinician evaluates the presence, frequency, and intensity of each symptom of PTSD on a scale from 0 (0 = absent) to 4 (4 = extreme/incapacitating). A rating of 2 (moderate) represents the threshold to qualify a symptom as clinically significant. Following this scale, a mean score of the first 20 questions (criteria B, C, D and E) indicates the presence and severity of PTSD (0 to 1 = Absent to mild PTSD; 1 to 2 = Moderate PTSD; 2 to 3 = Severe PTSD; 3 to 4 = Extreme PTSD). The CAPS-5 has been validated and used in many studies involving PTSD patients with great internal consistency (α = 0.90), test-retest reliability (Cohen’s Kappa = 100) over a 1-month period and convergent validity with the PCL-5 (r = 0.30) (Rivest-Beauregard et al., 2022).
The French version of the Dissociative Experiences Scale (DES-II) (translated by Saintonge, 1999) was used to assess dissociation, amnesia and absorption symptoms. This self-assessment is composed of 28-items depicting day-to-day situations of dissociative symptoms. Patients rate on a scale of 0–100 the percentage of time that they spend in each dissociative state described. The total score is obtained by calculating the mean of all 28 items, and a score above 30 indicates significant dissociation in day-to-day life. DES-II was found to have high test-retest reliability (0.79
The French version of the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001) was used to assess symptoms of depression. The measure consists of a self-assessment based on a 9-items questionnaire associated with cognitive, affective, and somatic symptoms of depression. Patients must rate the frequency to which they presented each symptom in the last 2 weeks on a scale from 0 (Never) to 3 (Almost every day). The cut-offs are of 4 and under for no depression, 5 to 9 for minor depression, 10 to 14 for moderate depression, 15 to 19 for moderate to severe depression and 20 and above for severe depression. PHQ-9 presents great construct validity for depression and anxiety, has been found sensible to changes pre- and post-treatment and has a good internal consistency (α = 0.87) (Beard et al., 2016).
The CNS Vitals Signs was used to assess cognitive functions. It is a computerized battery containing seven tests (verbal and visual memory, finger tapping, symbol digit coding, Stroop Test, shifting attention and continuous performance). The test picks from a bank of words, numbers, and drawings for each testing session to avoid memorization, and is sensible to invalid responses. Standard scores of verbal and visual memory, complex attention, processing speed, working memory, and sustained attention were analyzed according to the test’s normative categories (Above average =
Literature has shown that PTSD patients have increased heart rate (Pole, 2007) and decreased heart rate variability (Schneider and Schwerdtfeger, 2020) when compared to controls. Therefore, the EmWave Ear sensor from HeartMath was used to assess heart rate variability before and after each pretest, posttest, and follow-up for a duration of 1 minute. Lo et al. (2017) showed that the Emwave Pro sensor, attached to the earlobe, is not obtrusive to participants and provides data with comparable validity to other heart rate variability devices. Metrics such as heart rate (HR), inter-beat interval (IBI), maximal heart rate reserve (MHRR), standard deviation of NN intervals (SDNN), and root mean square of successive differences (RMSSD) were extracted from the segments.
After each VR session, the french-Canadian versions of the Immersive Tendencies Questionnaire (QPI), the Presence Questionnaire (QÉP) (Witmer and Singer, 1998) and Simulator Sickness Questionnaire (QC) (Kennedy et al., 1993) were used. All questionnaires were validated in French by the Laboratory of Cyberpsychology of the University of Quebec in Outaouais (UQO) with Cronbach alpha’s of 0.86 for the QC (Bouchard et al., 2011), 0.78 for the QPI, and 0.84 for the QÉP (Robillard et al., 2002). The QC contains 16 items covering different symptoms of cybersickness rated on a scale from 0 (Not at all) to 3 (Severely). QPI contains 18 items rated on a scale from 1 (Never or Not at all) to 7 (Often or A lot). QÉP contains 24 items in total, but only the basic scale of 19 items was used and rated on a scale from 1 (Not at all, Very Artificial, Not reactive) to 7 (Completely, Very reactive, Completely natural). The total score of all three questionnaires is equal to the sum of the rating of each item, with the inversion of items 14, 17 and 18 in the QÉP. Therefore, a higher score represents the higher intensity of the concept. QPI was only distributed at the first session, as it is considered a trait rather than a state.
The protocol used is a single-centre longitudinal pretest-posttest study that aims to examine whether virtual nature immersion has an impact on HRV, cognitive functions and affective symptoms in participants with PTSD. Therefore, a non-parametric option to the one-way repeated measures analyses of variance (ANOVA) was conducted (Cleophas et al., 2016). Friedman’s test was chosen for the analysis since the Shapiro-Wilk test’s null hypothesis for normality was rejected for some groups of measurements. Non-parametric post hoc analyses were performed by the Nemenyi post hoc test for the significant results of Friedman’s test to verify which pairwise groups had a significant difference. If participants had a missing value for any of the tests, they were excluded from that specific analysis.
Table 2 outlines the Pearson correlation coefficients measured among the psychological measurements taken. As expected, scores of PDEQ, CAPS-5, PHQ-9, and PCL-5 were positively and significantly correlated with each other at pretest 1. From pretest 1 to pretest 2, no significant change was found in psychological symptoms. In general, PCL-5 was significantly and strongly correlated with CAPS-5 in all four measurements, since both tests are used to measure PTSD symptom severity. Additionally, there was a significant correlation between PHQ-9 scores and PTSD severity measurements, implying that the severity of PTSD and depression symptoms are correlated. Therefore, participants with higher scores of depression and dissociative tendencies presented higher severity of PSTD on the CAPS-5 interview. DES-II scores were not significantly correlated with other psychological variables.
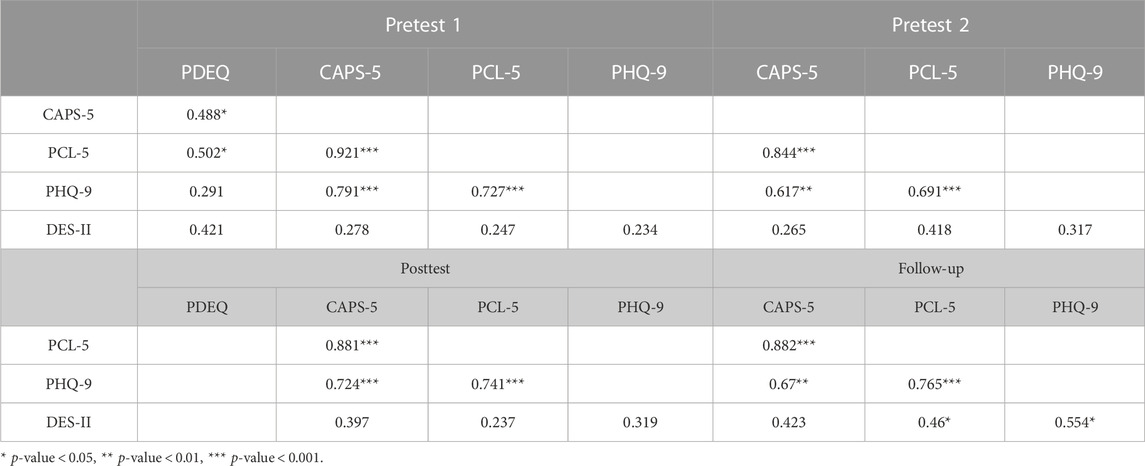
TABLE 2. Psychological tests correlations.
Figure 3 depicts the distribution of the psychological test variables collected throughout the experiment. Overall, a declining trend in the median of all psychological variables from pretests to posttest measurements can be observed. Furthermore, this decrease is still observable for CAPS-5 and DES-II during the three-month follow-up measurements, suggesting the experiment’s lasting efficacy at least 3 months after its termination on PTSD severity and dissociative tendencies. Even though the declining trend does not continue for PCL-5 and PHQ-9 in the follow-up measurements, their lower quartile levels are decreased in comparison to the pretest 2 lower quartiles. The fact that a decrease in CAPS-5 scores is observable at follow-up but not in PCL-5 scores may be linked to the self-reported nature of the second instrument. It would seem that subjectively, participants did not perceive their decrease in PTSD severity as lasting, but a more objective, exterior measure of the disorder’s severity did. This finding is coherent with Lee et al. (2022) results, which also observed lower self-reported improvement in PTSD symptoms at posttest compared to clinician-administered CAPS-5 interview.
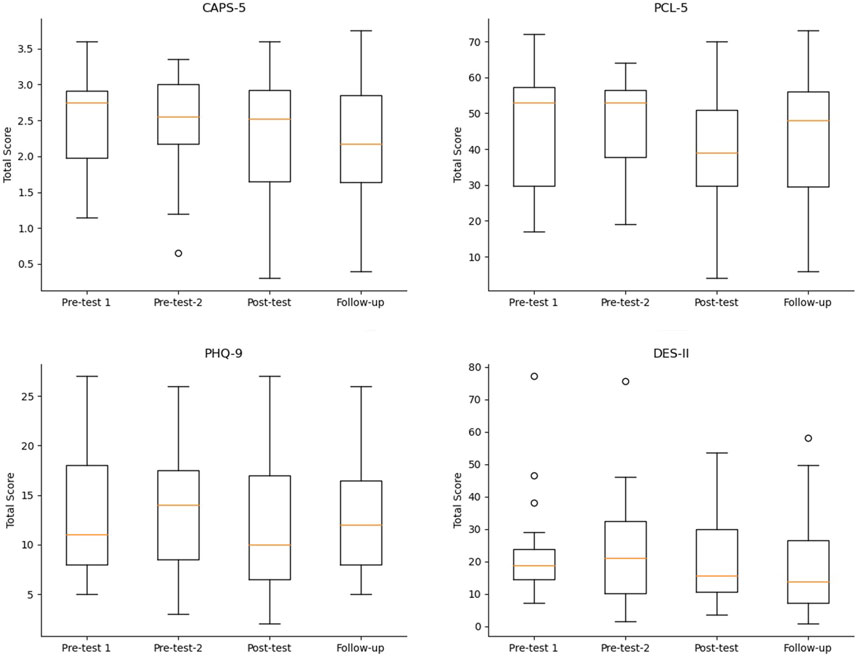
FIGURE 3. Boxplot showing the distributions from the psychological measurements.
Figure 4 displays the CAPS-5 and PCL-5 for each participant for pretest 2, posttest, and follow-up. On both pretests, a total of 16 participants presented PCL-5 above 30 and 15 participants exhibited a CAPS-5 above two, which indicates clinical significance of the disorder at pretest. At follow-up, 15 participants had CAPS-5 scores lower than in pretest 2 (represented by a blue dot in Figure 4). From the remaining 5 subjects that did not decrease in CAPS-5 score at follow-up, three presented a decline from pretest 2 to posttest. In the case of PCL-5, 13 participants resulted in a lower measurement in the follow-up compared to pretest 2. Four participants declined from pretest 2 to posttest but increased from posttest to follow-up. A possible explanation for this is that punctual events happening in the 3 months gap between follow-up and posttest can trigger the rise of symptoms from a subjective point of view. Nonetheless, the VR protocol decreased PSTD severity from a subjective as well as an objective point of view, from pretests to posttest, for most participants. This suggests that this therapeutic modality might be clinically more useful to reduce high peaks of PTSD symptoms in a short period of time, for example, when patients face temporary stressors.
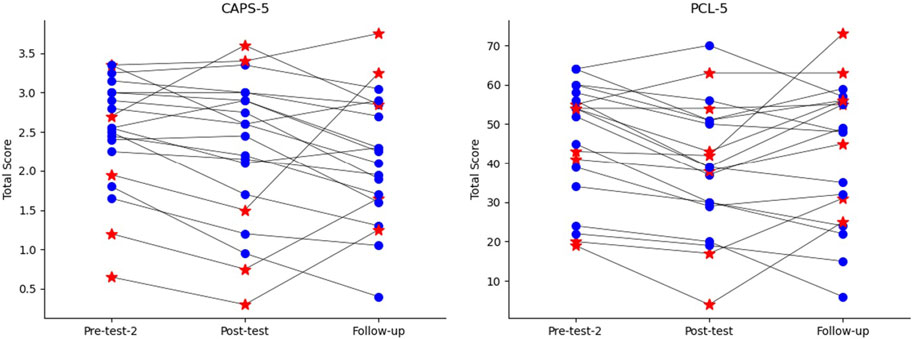
FIGURE 4. CAPS-5 and PCL-5 plots per subject.
Figure 5 displays the progression in standardized cognitive scores from pretest 1 to follow-up. It is possible to notice a rising trend between pretest 2 and posttest for processing speed and sustained attention variables, but the trend does not maintain on the follow-up measurements. Furthermore, from the curves of working memory and complex attention, a decrease in the standard deviation for the posttest analysis compared to the pretests can be observed. Therefore, a tendency to regroup around higher scores can be observed throughout the sample as the protocol progresses, even though no significant improvement occurred on these cognitive variables. Overall, a slight improvement in the cognitive faculties evaluated by the CNS Vitals Signs neurocognitive assessment was observed between pretest 1 and pretest 2, possibly as a result of the practice effect. However, Littleton et al. (2015) also observed this phenomenon in their validation study of the CNS Vitals Signs, and no additional improvement was observed in participants without training following the second testing session. These findings increase confidence in the results indicating improvement in cognitive function due to the VR immersion from pretest 2 to posttest.
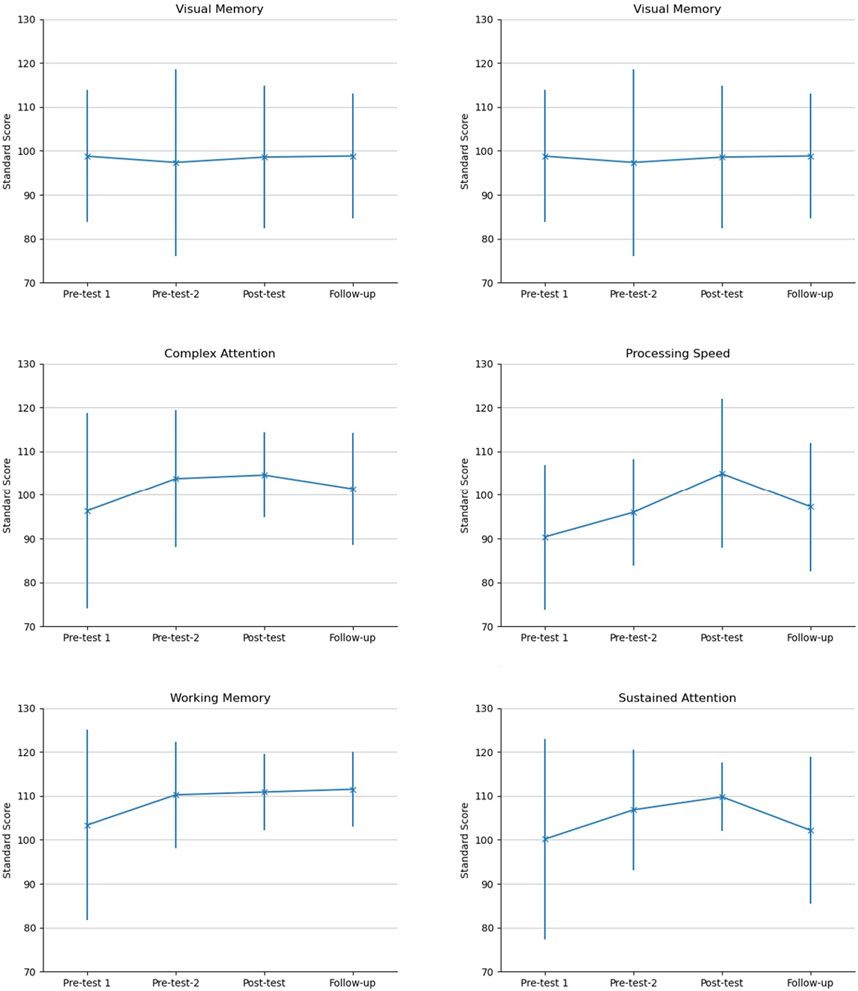
FIGURE 5. Mean and standard deviation of standard scores of cognitive variables.
Table 3 demonstrates the mean, standard deviation, and the result of the Friedman statistical test for the psychological variables and cognitive variables. All the psychological variables resulted in a statistical difference among the groups of measurements, while only two variables showed differences among the cognitive factors (i.e., processing speed, sustained attention). The following scores exhibit differences according to the post hoc analysis: PCL-5 (pretest 1 and posttest, p
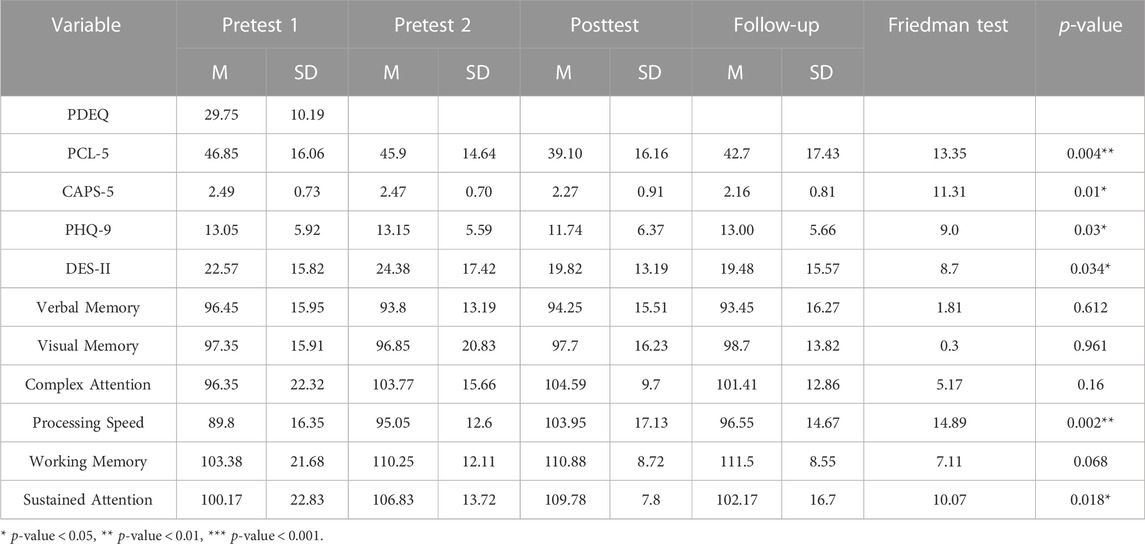
TABLE 3. Psychological and Cognitive tests mean (M) and standard deviation (SD).
Upon further analysis of the difference between groups of participants according to cut-off scores of psychological measures, no significant difference in cognitive variables was found linked to higher or lower scores of PHQ-9, CAPS-5, DES-II, or to the presence of psychotherapy during the intervention. Non-depressed people (PHQ-9 score below 10) tended to start at pretest 1 with higher overall cognitive scores on all variables, but improvement between pretest 1 and posttest stayed similar and exclusive to processing speed and sustained attention for both depressed and non-depressed participants. Improvement of cognitive functions following a relaxation immersion in VR is yet to be observed elsewhere in the scientific literature, which is why these findings deserve further consideration with a greater sample. Furthermore, it would seem that cognitive improvement took place regardless of other conditions. Multiple studies have found that cognitive functioning is impaired in people with PTSD (Qureshi et al., 2011). If VR relaxation in nature proves to be efficient in this population to improve this particular problem, and thus even in the presence of comorbidity of depression, dissociative tendencies or a severe case of PSTD, it would be an addition to the clinical arsenal of therapeutic modalities for PTSD symptoms that impair daily functioning.
Figure 6 displays the HR and RMSSD distributions of the measures taken prior to and posterior to the tests. Table 4 complements the information displaying the mean and standard variation of the variables collected from HR and HRV. The mean values and standard deviation of heart rate are lower in the posttest and follow-up than during pretest two, showing a reverse tendency as expected for patients with PTSD that have higher heart rate than controls (Pole, 2007). In addition, it is possible to notice that heart rate data below the middle quartile measured before the subjects have done the tests gets lower towards the posttest when compared to the pretests. PTSD patients also show decreased HRV when compared to controls (Schneider and Schwerdtfeger, 2020). However, HVR scores above the middle quartile for the RMSSD variable increase towards the posttest in comparison to the after-test HVR scores on pretests 1 and 2 as displayed in Figure 6. Additional analysis of HR and HRV will be further explored from the biosignals collected from the participants during each section of immersion.
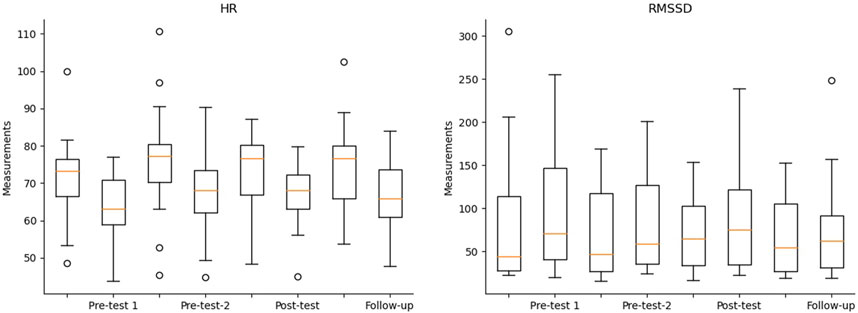
FIGURE 6. Boxplot showing the distributions of HR and HRV measurements.
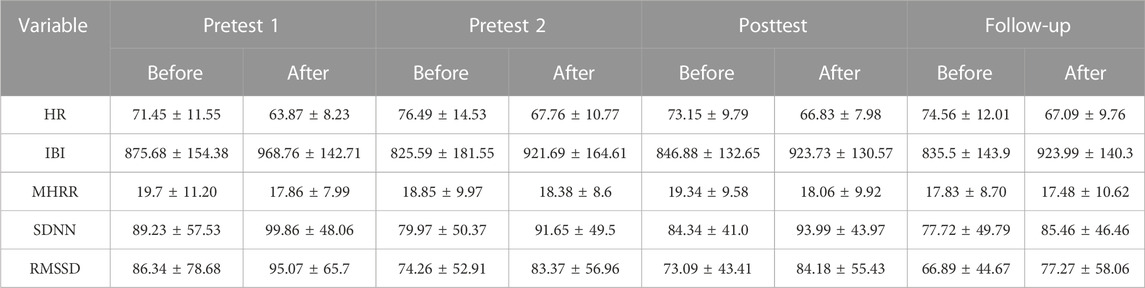
TABLE 4. HR and HRV mean ± standard deviation.
Figure 7 depicts the average and standard deviation results of the sense of presence and cybersickness for each session of the treatment. The results showed that the participants graded their sense of presence highly and almost no symptoms of cybersickness. These results and the rate of participants that finished the entire intervention reinforce the utilization of VR as a high motivator and safe tool.
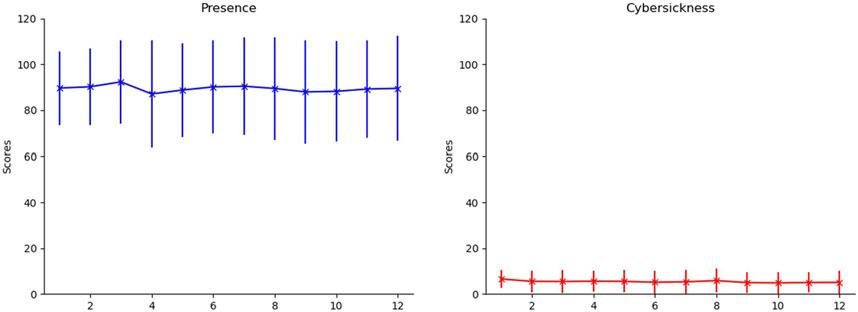
FIGURE 7. Mean and standard deviation of the scores for presence (blue) and cybersickness (red) for each section.
This study examined the feasibility and clinical outcomes of a multisensory VR nature immersion in participants suffering from PTSD symptoms. Preliminary results suggest that the procedure may be efficacious in promoting a statistically significant decline in patients’ self-reported PTSD symptoms (PCL-5) and clinician-examined severity of PTSD (CAPS-5). Additionally, depressive symptoms declined from pretest to posttest, as well as dissociative symptoms. Decline in PTSD severity assessed by CAPS-5 interview and dissociative tendencies were maintained at the 3-month follow-up. Considering the analyzed cognitive variables, only two presented a statistically significant improvement in processing speed and sustained attention showing the benefits of the procedure on the cognitive aspects of the participants. Although we could not observe a statistically significant improvement, the variables of working memory and complex attention also present an increased average up to the posttest analysis. In addition, visual and verbal memory results stayed consistent across the period of VR immersion. These results show that improvement in cognition is not attributable to learning from repeated testing. These results display a reverse tendency between PTSD severity and processing speed as well as sustained attention, suggesting that a decrease in PTSD symptoms could have improved these cognitive functions in our participants. This interesting trend should be further explored with a greater sample size. Moreover, according to the questionnaires evaluating the experience, most of the participants graded the experience as highly immersive and free of considerable symptoms of cybersickness. All the outcomes give us an early indication that the treatment is feasible and safe. Notwithstanding the not-very-conclusive results from heart rate analysis, we will be analyzing the EEG and PPG signals collected from each of the 12 sessions of VR nature immersion in order to investigate their behaviours across the duration of the protocol.
Limitations of this study include the small sample size of 20 participants and a lack of a control group. A larger study with a greater number of participants would enable the determination of a control group and would benefit the analysis of the efficacy of the intervention by the comparison of both groups. Furthermore, a group having the intervention with the olfactory stimulation compared with a group without the olfactory stimulation would provide an analysis of the separated contribution of smells to the intervention. Another limitation consisted of some participants rating the smells of the scenarios as not very realistic, mainly for the scenarios representing the hometown locations. Future studies will investigate the possibility of improvements by using different smells, such as multisensory pods, which provide a more realistic experience (Lopes et al., 2022). Lastly, while this paper has focused on the qualitative outcomes of the multisensory intervention, ongoing work includes analysis of the biosignals collected and potential quantitative outcomes on neural and bio-markers.
Although many virtual reality applications have been explored recently, most still rely on the stimulation of only hearing and vision senses. The work presented in this paper investigated the feasibility of a multisensory relaxing natural virtual reality application as a therapeutic modality for PTSD patients. Significant decreases in the severity of PTSD symptoms were seen as a result of the intervention. Ratings from CAPS-5, PCL-5, PHQ-9, and DES-II’s scores significantly dropped after the intervention, and scores of CAPS-5 and DES-II also maintained a significant decrease three-month post-protocol. After the VR nature immersion, participants showed to have significantly improved their cognitive function levels of sustained attention and processing speed. However, the cognitive improvements did not persist up to the three-month follow-up measurements. The virtual reality experience was rated by participants as inducing a high level of presence with little to no negative effects of cybersickness, reinforcing its safety to use in a clinical setting.
The datasets presented in this article are not yet readily available because they are being processed. The questionnaire data and the collected biosignals will be made available to the research community via the authors’ website: https://musaelab.ca/resources. Requests to access the datasets should be directed to TF, dGlhZ28uZmFsa0BpbnJzLmNh.
The studies involving humans were approved by the Ethics Committee of Research with Human Beings (CER-22-669) from INRS (University of Quebec). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
BD: Formal Analysis, Investigation, Visualization, Writing–original draft, Writing–review and editing. LP: Data curation, Writing–original draft, Writing–review and editing. ML: Writing–review and editing. M-CR: Conceptualization, Data curation, Writing–original draft, Writing–review and editing. AO: Writing–review and editing. TF: Conceptualization, Writing–original draft, Writing–review and editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded partly by an NSERC Discovery grant to TF (RGPIN-2021-03246).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aiken, M. P., and Berry, M. J. (2015). Posttraumatic stress disorder: possibilities for olfaction and virtual reality exposure therapy. Virtual Real. 19, 95–109. doi:10.1007/s10055-015-0260-x
Ashbaugh, A. R., Houle-Johnson, S., Herbert, C., El-Hage, W., and Brunet, A. (2016). Psychometric validation of the English and French versions of the posttraumatic stress disorder checklist for dsm-5 (pcl-5). PloS one 11, e0161645. doi:10.1371/journal.pone.0161645
Beard, C., Hsu, K., Rifkin, L., Busch, A., and Björgvinsson, T. (2016). Validation of the phq-9 in a psychiatric sample. J. Affect. Disord. 193, 267–273. doi:10.1016/j.jad.2015.12.075
Bomyea, J., and Lang, A. J. (2012). Emerging interventions for ptsd: future directions for clinical care and research. Neuropharmacology 62, 607–616. doi:10.1016/j.neuropharm.2011.05.028
Bouchard, S., Robillard, G., Renaud, P., and Bernier, F. (2011). Exploring new dimensions in the assessment of virtual reality induced side effects. J. Comput. Inf. Technol. 1, 20–32.
Carlson, E. B., and Putnam, F. W. (1993). An update on the dissociative experiences scale. Dissociation Prog. dissociative Disord. 6, 1, 16-27.
Cassani, R., Moinnereau, M.-A., and Falk, T. H. (2018). “A neurophysiological sensor-equipped head-mounted display for instrumental qoe assessment of immersive multimedia,” in 2018 Tenth international conference on quality of multimedia experience (QoMEX) (IEEE), May 2018, Cagliari, Italy, 1–6.
Cassani, R., Moinnereau, M.-A., Ivanescu, L., Rosanne, O., and Falk, T. H. (2020). Neural interface instrumented virtual reality headsets: toward next-generation immersive applications. IEEE Syst. Man, Cybern. Mag. 6, 20–28. doi:10.1109/msmc.2019.2953627
Cleophas, T. J., Zwinderman, A. H., Cleophas, T. J., and Zwinderman, A. H. (2016). Non-parametric tests for three or more samples (friedman and kruskal-wallis). Clinical data analysis on a pocket calculator: understanding the scientific methods of statistical reasoning and hypothesis testing, Springer, Berlin, Germany, 193–197.
De Jesus, B., Lopes, M., Moinnereau, M.-A., Gougeh, R. A., Rosanne, O. M., Schubert, W., et al. (2022). “Quantifying multisensory immersive experiences using wearables: is (stimulating) more (senses) always merrier?,” in Proceedings of the 2nd Workshop on Multisensory Experiences-SensoryX’22 (SBC). June 2022, Aveiro, Portugal, .
Emmelkamp, P. M., and Meyerbröker, K. (2021). Virtual reality therapy in mental health. Annu. Rev. Clin. Psychol. 17, 495–519. doi:10.1146/annurev-clinpsy-081219-115923
Forkus, S. R., Raudales, A. M., Rafiuddin, H. S., Weiss, N. H., Messman, B. A., and Contractor, A. A. (2022). The posttraumatic stress disorder (ptsd) checklist for dsm–5: A systematic review of existing psychometric evidence. Clin. Psychol. Sci. Pract. 30, 110–121. doi:10.1037/cps0000111
Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., et al. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47, 2393–2400. doi:10.1017/s003329171700040x
Gualtieri, C. T., and Johnson, L. G. (2006). Reliability and validity of a computerized neurocognitive test battery, cns vital signs. Archives Clin. Neuropsychology 21, 623–643. doi:10.1016/j.acn.2006.05.007
Halbig, A., Babu, S. K., Gatter, S., Latoschik, M. E., Brukamp, K., and von Mammen, S. (2022). Opportunities and challenges of virtual reality in healthcare–a domain experts inquiry. Front. Virtual Real. 3, 14. doi:10.3389/frvir.2022.837616
Kennedy, R. S., Lane, N. E., Berbaum, K. S., and Lilienthal, M. G. (1993). Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3, 203–220. doi:10.1207/s15327108ijap0303_3
Knaust, T., Felnhofer, A., Kothgassner, O. D., Höllmer, H., Gorzka, R.-J., and Schulz, H. (2022). Exposure to virtual nature: the impact of different immersion levels on skin conductance level, heart rate, and perceived relaxation. Virtual Real. 26, 925–938. doi:10.1007/s10055-021-00595-2
Kothgassner, O. D., Goreis, A., Kafka, J. X., Van Eickels, R. L., Plener, P. L., and Felnhofer, A. (2019). Virtual reality exposure therapy for posttraumatic stress disorder (ptsd): A meta-analysis. Eur. J. psychotraumatology 10, 1654782. doi:10.1080/20008198.2019.1654782
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The phq-9: validity of a brief depression severity measure. J. general Intern. Med. 16, 606–613. doi:10.1046/j.1525-1497.2001.016009606.x
Lee, D. J., Weathers, F. W., Thompson-Hollands, J., Sloan, D. M., and Marx, B. P. (2022). Concordance in ptsd symptom change between dsm-5 versions of the clinician-administered ptsd scale (caps-5) and ptsd checklist (pcl-5). Psychol. Assess. 34, 604–609. doi:10.1037/pas0001130
Littleton, A. C., Register-Mihalik, J. K., and Guskiewicz, K. M. (2015). Test-retest reliability of a computerized concussion test: cns vital signs. Sports health 7, 443–447. doi:10.1177/1941738115586997
Lo, J. C., Sehic, E., and Meijer, S. A. (2017). Measuring mental workload with low-cost and wearable sensors: insights into the accuracy, obtrusiveness, and research usability of three instruments. J. cognitive Eng. Decis. Mak. 11, 323–336. doi:10.1177/1555343417716040
Lopes, M. K., de Jesus, B. J., Moinnereau, M.-A., Gougeh, R. A., Rosanne, O. M., Schubert, W., et al. (2022). “Nat (ur) e: quantifying the relaxation potential of ultra-reality multisensory nature walk experiences,” in 2022 IEEE International Conference on Metrology for Extended Reality, Artificial Intelligence and Neural Engineering (MetroXRAINE) (IEEE), October 2022, Rome, Italy, 459–464.
Marmar, C. R., Metzler, T. J., and Otte, C. (2004). The peritraumatic dissociative experiences questionnaire. New York, NY, USA, The Guilford Press.
Mistry, D., Zhu, J., Tremblay, P., Wekerle, C., Lanius, R., Jetly, R., et al. (2020). Meditating in virtual reality: proof-of-concept intervention for posttraumatic stress. Psychol. Trauma Theory, Res. Pract. Policy 12, 847–858. doi:10.1037/tra0000959
Noronha, H., and Campos, P. (2021). Harnessing virtual reality nature to promote well-being. Interact. Comput. 33, 353–366. doi:10.1093/iwc/iwac004
Pole, N. (2007). The psychophysiology of posttraumatic stress disorder: A meta-analysis. Psychol. Bull. 133, 725–746. doi:10.1037/0033-2909.133.5.725
Qureshi, S. U., Long, M. E., Bradshaw, M. R., Pyne, J. M., Magruder, K. M., Kimbrell, T., et al. (2011). Does ptsd impair cognition beyond the effect of trauma? J. neuropsychiatry Clin. Neurosci. 23, 16–28. doi:10.1176/appi.neuropsych.23.1.16
Ragsdale, K. A., Watkins, L. E., Sherrill, A. M., Zwiebach, L., and Rothbaum, B. O. (2020). Advances in ptsd treatment delivery: evidence base and future directions for intensive outpatient programs. Curr. Treat. Options Psychiatry 7, 291–300. doi:10.1007/s40501-020-00219-7
Rauch, S. A., Eftekhari, A., and Ruzek, J. I. (2012). Review of exposure therapy: A gold standard for ptsd treatment. J. Rehabil. Res. Dev. 49, 679–687. doi:10.1682/jrrd.2011.08.0152
Riches, S., Jeyarajaguru, P., Taylor, L., Fialho, C., Little, J., Ahmed, L., et al. (2023). Virtual reality relaxation for people with mental health conditions: A systematic review. Soc. Psychiatry Psychiatric Epidemiol. 58, 989–1007. doi:10.1007/s00127-022-02417-5
Rivest-Beauregard, M., Brunet, A., Gaston, L., Al Joboory, S., Trousselard, M., Simson, J.-P., et al. (2022). The clinician-administered ptsd scale for dsm-5 (caps-5) structured interview for ptsd: A French language validation study. Psychol. Assess. 34, e26–e31. doi:10.1037/pas0001099
Rizzo, A. S., and Shilling, R. (2017). Clinical virtual reality tools to advance the prevention, assessment, and treatment of ptsd. Eur. J. psychotraumatology 8, 1414560. doi:10.1080/20008198.2017.1414560
Robillard, G., Bouchard, S., Renaud, P., and Cournoyer, L. (2002). “Validation canadienne-française de deux mesures importantes en réalité virtuelle: l’immersive tendencies questionnaire et le presence questionnaire,” in Poster presented at the 25e congrès annuel de la Société Québécoise pour la Recherche en Psychologie (SQRP), November 2002, Trois-Riviéres, Canada.
Schneider, M., and Schwerdtfeger, A. (2020). Autonomic dysfunction in posttraumatic stress disorder indexed by heart rate variability: A meta-analysis. Psychol. Med. 50, 1937–1948. doi:10.1017/s003329172000207x
Shalev, A., Liberzon, I., and Marmar, C. (2017). Post-traumatic stress disorder. N. Engl. J. Med. 376, 2459–2469. doi:10.1056/nejmra1612499
Taylor, S., Thordarson, D. S., Maxfield, L., Fedoroff, I. C., Lovell, K., and Ogrodniczuk, J. (2003). Comparative efficacy, speed, and adverse effects of three ptsd treatments: exposure therapy, emdr, and relaxation training. J. Consult. Clin. Psychol. 71, 330–338. doi:10.1037/0022-006x.71.2.330
Weathers, F. W., Bovin, M. J., Lee, D. J., Sloan, D. M., Schnurr, P. P., Kaloupek, D. G., et al. (2018). The clinician-administered ptsd scale for dsm–5 (caps-5): development and initial psychometric evaluation in military veterans. Psychol. Assess. 30, 383–395. doi:10.1037/pas0000486
Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A., Keane, T. M., et al. (1993). “The ptsd checklist (pcl): reliability, validity, and diagnostic utility,” in Annual convention of the international society for traumatic stress studies, 462, San Antonio, TX, USA. October 1993.
Keywords: virtual reality, relaxation training, olfactory, multisensory, mental health
Citation: De Jesus Junior BJ, Perreault L, Lopes MKS, Roberge M-C, Oliveira AA and Falk TH (2023) Using multisensory virtual reality nature immersion as a therapeutic modality for improving HRV and cognitive functions in post-traumatic stress disorder: a pilot-study. Front. Virtual Real. 4:1261093. doi: 10.3389/frvir.2023.1261093
Received: 18 July 2023; Accepted: 15 September 2023;
Published: 02 October 2023.
Edited by:
Hai-Ning Liang, Xi’an Jiaotong-Liverpool University, ChinaReviewed by:
Diego Vilela Monteiro, ESIEA University, FranceCopyright © 2023 De Jesus Junior, Perreault, Lopes, Roberge, Oliveira and Falk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Belmir Jose De Jesus Junior, YmVsbWlyLmplc3VzQGlucnMuY2E=; Tiago H. Falk, dGlhZ28uZmFsa0BpbnJzLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.