 Nadine Elisa van der Waal
Nadine Elisa van der Waal Julie A. W. van Bokhorst
Julie A. W. van Bokhorst Laura Nynke van der Laan
Laura Nynke van der Laan- Department of Communication and Cognition, Tilburg School of Humanities and Digital Sciences, Tilburg University, Tilburg, Netherlands
Virtual reality technologies can be used to alter one’s body image by inducing ownership of an overweight virtual body. This illusion can possibly lead to both negative affective responses toward the virtual body as well as perceptual changes of one’s own body size, which are both scarcely examined with regard to the embodiment of an overweight avatar. This study’s fundamental aim is to investigate, among healthy weight participants, whether negative affect toward a virtual body and changes in body-size perception can be evoked when embodying an overweight virtual avatar. Additionally, the study investigates whether applying visuotactile stimulation (which has been identified as a proxy for virtual body ownership by previous studies) and drive for thinness influence the strength of these effects. A 2 (healthy weight vs. overweight virtual body) × 2 (congruent vs. incongruent visuotactile stimulation) between-subjects design was employed, with participants’ drive for thinness measured to test its potential moderating effect. ANOVAs revealed that participants (N = 114) experienced significantly more negative affect toward the virtual body when embodying one that was overweight compared to a healthy weight virtual body. Visuotactile stimulation did not moderate this effect, even though the manipulation of visuotactile stimulation worked as intended (i.e., the experience of ownership over the virtual body was significantly higher in the congruent compared to incongruent visuotactile stimulation condition). Additionally, participants with a high drive for thinness did not experience significantly more negative affect than participants with a low drive for thinness. Embodiment of an overweight avatar did not affect body-size perceptions, nor did visuotactile stimulation or the drive for thinness moderate this effect. Knowing that embodiment of an overweight avatar results in negative affective responses toward it, future studies could deepen our understanding of the role of negative affect in the transfer of emotions to one’s own body, and the interplay between negative affect toward a virtual body and body-size perceptions.
1 Introduction
Negative affect toward the body arises when the mental image one holds of their own body—referred to as “body image”—is not in agreement with their desired body—for instance, one that is slimmer (Boldero et al., 2005). Recent advances in virtual reality (VR) technologies allow users to alter their bodily self-representation by generating an illusion of owning a body dissimilar in size to their own (Piryankova et al., 2014). Knowing that strong negative affect can deregulate cognition and behavior (Levinson et al., 2020), combined with the development of an increasing number of virtual environments in which virtual bodies are becoming important features (i.e., VRchat, Metaverse), there is a need to identify how users respond to those altered bodies, both emotionally and cognitively. In addition, when designing VR interventions that incorporate altered virtual body sizes, it is crucial to understand the extent to which these virtual experiences affect humans emotionally. Negative affect in the current study refers to negative emotional responses and negative states that are induced by and experienced during the embodiment of an (dissimilar) overweight virtual body (e.g., disgust, fear, tension).
Two previous studies have examined how the embodiment of a larger-sized virtual avatar could negatively influence subsequent experienced affect, demonstrating increased levels of body anxiety, fear of weight gain (Ferrer-Garcia et al., 2017; Porras Garcia et al., 2019), and body dissatisfaction (Porras Garcia et al., 2019) toward one’s own body. The present study contributes to emotion research in VR as the first to examine affective responses toward the virtual body rather than focusing on the affective responses toward one’s own. Hypothetically, the effects of embodying an overweight virtual avatar on negative affect could occur through two pathways: changes in body-size perception of one’s own body, which in turn facilitate negative affect toward one’s body, or changes in negative affect toward the virtual body, which in turn transfer to negative affect toward one’s own body. The initial affective responses to the virtual body could facilitate our understanding of subsequent cognitive, affective, and behavioral effects. Measuring affective responses toward a virtual body is a first step in understanding whether and how emotion transfer manifests after embodying an overweight avatar.
This study will also focus on perceptual responses to the full body illusion, as studies examining body-size perceptions after the embodiment of an overweight avatar, compared to a healthy weight avatar, are limited (Piryankova et al., 2014). Previous studies have focused on the perceptual effects of embodying a healthy weight avatar among anorexia nervosa patients and found that the overestimation of body size decreased after the virtual experience (Keizer et al., 2016). Furthermore, studies that employed a skinny avatar showed a significant decrease in participants’ perceived body size (for hips only: 7; 8). The second aim of this study is to examine whether body-size perceptions of healthy weight participants can be altered after embodying an overweight virtual avatar.
The third novel contribution of this study is to assess whether visuotactile stimulation (VTS) could be induced to strengthen negative affect toward an overweight virtual body. When applying VTS, the simultaneous stroking of the real body and perception of touch on the virtual body leads to a misattribution of the virtual body as being one’s own (Petkova et al., 2011). It is known that VTS can influence the strength of virtual body ownership (VBO), which is defined as the psychological illusion of temporarily experiencing a (dissimilar) virtual body to one’s own (Slater et al., 2009). It is likely that the stronger the illusion of perceiving the virtual body as one’s own, the stronger will be the perceptual and affective responses toward the virtual body. Indeed, one study found that, when embodying an overweight avatar (compared to a virtual body of one’s own size), those receiving synchronous VTS reported stronger body anxiety than those receiving asynchronous VTS (Porras Garcia et al., 2019). Previous studies have not yet examined whether VTS could also influence affective responses to the virtual body, which is the second aim of this study. Additionally, the role of VTS in perceptual responses will be examined, even though most studies retrieved null findings (Piryankova et al., 2014; Serino et al., 2016; Porras Garcia et al., 2019).
The extent to which one experiences negative affect toward one’s body depends on individual trait variables, which can accurately predict body dissatisfaction and eating disorder predispositions (Cuesta-Zamora et al., 2018). “Drive for thinness” (DT) can be conceived as the extent to which one is concerned about one’s body shape and change (Ferrer-Garcia et al., 2017). As high levels of body shape concern are associated with increased body-related negative affect and stronger emotions during exposure to one’s own body in a mirror (Vocks et al., 2008), DT will be included in this study to assess its influence on the experience of emotions toward an overweight virtual body. Previous studies have already shown that participants with higher levels of DT experience more body anxiety toward their own body after embodying a virtual dissimilar overweight body than participants with low levels of DT (Ferrer-Garcia et al., 2017). Whether these responses are also stronger toward the virtual body is still unknown, but are equally relevant to understanding the cognitive processes that manifest after embodying an overweight avatar, and especially whether these processes depend on one’s psychological characteristics. Regarding body-size perceptions, most studies using the full body illusion are conducted among eating-disorder patients, while initial evidence shows that body sizes are also perceived differently among healthy subjects (Piryankova et al., 2014; Keizer et al., 2016). However, healthy subjects can still vary in the degree to which they are preoccupied with their body size and weight; therefore, the fourth aim of the study is to investigate whether these psychological traits precede body-size perceptions.
In sum, the following research questions will be addressed:
1) To what extent is negative affect experienced toward a virtual body when embodying an overweight virtual avatar (compared to a healthy weight virtual avatar) and is this effect moderated by VTS and DT?
2) To what extent does embodying an overweight virtual avatar (compared to a healthy weight virtual avatar) lead to perceptual changes of one’s own body size, and is this effect moderated by VTS and DT?
2 Theoretical framework
In our assessment of our bodies, a mental model of our subjective perception of the body is created—"body image” (Gleeson et al., 2006). Such mental representation not only involves our physical appearance but also includes our emotions, attitudes, behaviors, and beliefs about the self (Cash et al., 2004). According to Higgins’ self-discrepancy theory, three concepts of the self can be distinguished: the actual self, the ideal self, and the ought self (Higgins, 1989). The actual self refers to the subjective representation of the self in the mind (i.e., body image) rather than its objective representation (i.e., the body as it is, not biased by the mind). The ideal self can be described as the self that one would like to be or the physical features that one would like to possess. Finally, the ought self reflects how one thinks he or she must be or look like. A discrepancy between our own body image and how we desire or ought to be can evoke emotional responses and negative affect (Boldero et al., 2005). Negative affect can be described as “…a general dimension of subjective distress and unpleasurable engagement including aversive mood states [such] as guilt, disgust and fear” (15, p. 2). In the present study, “negative affect” will be defined as the negative emotional states/responses toward the virtual body that are evoked by the embodiment of an overweight virtual body.
Recent developments in VR have allowed researchers to alter the perception of one’s body by inducing ownership of a differently sized virtual avatar—in other words, the experience of a dissimilar virtual body as if it were one’s own body (Ferrer-García and Gutiérrez-Maldonado, 2012; Keizer et al., 2016). The strength of the illusion of VBO on perceptions of the bodily self has been demonstrated by studies in which a shift in the perceptual component of body image (i.e., body-size estimation) was established (Normand et al., 2011; Serino et al., 2016), which transferred onto one’s own body and persisted for at least 3 hours (Keizer et al., 2016). Slater et al. (2009) showed that owning a virtual body may trigger the same perceptual and emotional processes as our physical body. Hence, it can be speculated that the illusion of ownership of a body discrepant with one’s desired body can affect actual/ideal/ought discrepancies and elicit negative emotions if these discrepancies are increased.
Few studies have investigated how full-body illusions could affect negative affect toward one’s body. Preston and Ehrsson (2014) attempted to alter body satisfaction by eliciting ownership of a smaller (85%) and larger (115%) virtual body compared to one’s actual body size. In this study, body satisfaction was found to increase with a thinner virtual body size but not to decrease with a larger virtual body. In later research, Ferrer-Garcia et al. (2017) examined the influence of VBO over a larger-sized virtual body on subsequent affective responses toward one’s own body. In a study among healthy college students, ownership of three different virtual avatars was induced: one similar in size, one 20%, and one 40% larger in size. Large effects toward the subjects’ own bodies were found after the embodiment of the largest virtual avatar compared to the real-sized one. Porras Garcia et al. (2019) confirmed the results and also found increased body dissatisfaction and body-size perception (i.e., the discrepancy between one’s own perceived body size, which was selected on a figural drawing scale, and actual body size) after the embodiment of the larger-sized avatar compared to before the experiment. These results indicate how VR can establish a shift in body-size perceptions and affective responses toward one’s body.
As the perceptual component of body image has been shown to be tightly linked with the affective component of body image (Ferrer-García and Gutiérrez-Maldonado, 2012; Preston and Ehrsson, 2014), a discrepancy between the perceived and ideal body is expected to give rise to negative emotional responses not only toward one’s own body but already toward the virtual body. The following hypotheses are formulated:
H1:. Participants embodying an overweight virtual avatar will report stronger negative affect than participants embodying a healthy weight virtual avatar.
H2:. Participants embodying an overweight virtual avatar will report a larger body-size discrepancy (i.e., the difference between actual body size and perceived body size) compared to participants embodying a healthy weight virtual avatar.
2.1 The moderating role of visuotactile stimulation
Visuotactile stimulation (VTS) is an important facilitator of VBO, as shown by multiple studies, whereby multisensory stimulation is applied to both the real and the virtual body (Maselli and Slater, 2013). When VTS is applied to one’s real body and this touch is simultaneously perceived on an embodied larger-sized virtual avatar, the simultaneous integration of the incoming tactile and visual information in the brain results in a misattribution of ownership of the larger-sized virtual body (Tsakiris et al., 2006; Petkova et al., 2011). Consensus has been reached on the fact that synchronous VTS (i.e., synchronizing visual input in VR with tactile sensations in real life) leads to higher feelings of VBO than asynchronous simulation (i.e., a temporal mismatch between visual input in VR and tactile sensations in real life) in setups where the virtual body is merely a static object (Maselli and Slater, 2013). However, some argue that the extent to which VTS affects VBO depends on other factors that contribute to the experience of a full-body illusion (Maselli and Slater, 2013). Examples of these factors are congruent visual perspective (first vs. third person), appearance similarity, and synchronous visuomotor movements between the virtual and real body (Kokkinara and Slater, 2014). A high correspondence between features of one’s own body and features of the avatar’s body could dispel the negative influence of asynchronous VTS on VBO (Kokkinara et al., 2016). In this study, VTS is included to examine its influence on the strength of affective responses on the embodied virtual avatar, whereby the movements of the avatar and its user are synchronized. It should be noted that previous studies that retrieved significant findings, which are discussed below, all used a static virtual body.
Previous research has already shown that VTS indeed plays a role in affective responses in VR, in contexts other than virtual body size. At a more general level, a study showed that, when participants were shown pictures in VR while receiving synchronous or asynchronous VTS on their virtual hand, the affective responses (e.g., arousal) to these pictures were stronger when synchronous VTS was applied than when asynchronous VTS was applied (Gall et al., 2021). This demonstrates that information processing can fundamentally be changed by the experience of VBO. Additionally, a study has shown that the embodiment of an invisible virtual body (whereby VTS was applied to the real body and to an empty space in VR at the same distance as where the body was supposed to be) led to lower social anxiety (i.e., anxiety for groups and crowds) in the virtual environment, and that this effect was stronger when synchronous VTS was applied (Guterstam et al., 2015). Even though these studies did not measure response toward the virtual body, they do show that VTS moderates affect in VR.
In studies that examined body-related affect (i.e., body dissatisfaction and body anxiety), most used synchronous multisensory stimulation to induce VBO over differently sized avatars but did not include an asynchronous control condition (visuomotor synchrony: 5; VTS: 19). Until now, only one study has investigated the influence of synchronous versus asynchronous VTS on VBO and investigated body image disturbance and body-related affect (i.e., body dissatisfaction and body anxiety: 6). VBO was induced over a similar and larger-sized virtual avatar. Higher self-reported VBO was found in the synchronous conditions compared to the asynchronous conditions in both avatar body-size conditions. Most interestingly, an interaction effect between avatar body size and VTS condition was found. Post hoc analyses revealed that, within the larger body-size condition, anxiety significantly increased when synchronous compared to asynchronous VTS was applied; this indicates that stronger feelings of VBO facilitate affective responses toward one’s own body.
Combining these findings with findings regarding other stimulus types in VR and the role of VTS, it is expected that:
H3:. The effect of avatar body size on negative affect (as hypothesized in H1) is moderated by VTS, such that the difference in negative affect between the healthy and overweight condition is larger when congruent VTS is applied than when incongruent VTS is applied.The role of VTS on perceptual responses has been demonstrated in different contexts. For example, overestimation of object sizes after a small-body illusion and underestimation of object sizes after a large-body illusion were stronger after synchronous VTS compared to asynchronous VTS (van der Hoort et al., 2011). Some scholars have investigated the effect that VTS could have on body-size perceptions but the results varied. For example, participants embodying a skinny avatar perceived their own hips to be smaller, compared to participants embodying a healthy weight avatar (Scarpina et al., 2019) but only after synchronous and not asynchronous VTS. However, this finding did not hold for the size estimation of other body parts (i.e., shoulders, abdomen). Other scholars, however, did not find that VTS moderated body-size estimations after the experience of a different virtual body size (Keizer et al., 2016; Serino et al., 2016). Nevertheless, it is expected that:
H4:. The effect of avatar body size on body-size discrepancy (as hypothesized in H2) is moderated by VTS, such that the difference in body-size discrepancy between the over- and healthy weight conditions is larger when congruent VTS is applied, compared to when incongruent VTS is applied.
2.2 The moderating role of drive for thinness
The extent to which one experiences negative affect toward one’s body depends on individual trait variables (Cuesta-Zamora et al., 2018). Previous studies have shown that the extent to which owning a differently sized body influenced subsequent body dissatisfaction depended on one’s susceptibility to eating disorders (Preston and Ehrsson, 2014; Ferrer-Garcia et al., 2017). Individuals with a high DT are easily concerned about their body weight and shape, are often afraid of gaining weight, and are therefore easily dissatisfied with their bodies (Wiederman and Pryor, 2000). As body dissatisfaction is tightly coupled with strong reactions to weight-related cues (DelRosario et al., 1984), this is expected to transfer into stronger emotional responses toward undesired body change (Preston and Ehrsson, 2014).
Ferrer-Garcia et al. (2017) investigated the impact of DT on the elicitation of body anxiety after an embodied VR experience. Interaction effects between DT and virtual body size were found, where only participants with high DT (compared to low DT) experienced significantly more body anxiety after the embodiment of a 40% larger avatar than after the embodiment of a similar-sized avatar. Even though Cardoso et al. (2020) did not investigate affective responses toward the virtual body, their findings do indicate that there is an increased sensitivity of VR body image change amongst high DT individuals. Additionally, Preston and Ehrsson (2018) found that individuals with higher non-clinical eating disorder characteristics experienced increased negative affect toward their own bodies. Hence, it is expected that the extent to which one will be emotionally affected by owning an overweight virtual body is influenced by one’s degree of DT.
H5:. The effect of avatar body size on negative affect (as hypothesized in H1) is moderated by DT, such that the difference in negative affect between the over- and healthy weight condition is greater among those with high DT compared to those with low DT.Combining the evidence that the effects of virtual body size on negative affect are found in individuals with higher non-clinical eating disorder characteristics (Piryankova et al., 2014; Preston and Ehrsson, 2018) and that the perceptions of one’s own body size can affect one’s emotional state (Preston and Ehrsson, 2014; Preston and Ehrsson, 2018), it is arguable that, among a healthy sample, DT could strengthen perceptual effects. For example, research that exposed healthy participants to pictures of attractive people has shown that those with a high DT have an attentional bias (i.e., looking longer and more often) toward pictures of hips, waists, legs, and arms (Hewig et al., 2008), which supports the notion that they perceive bodies differently. It is expected that these individuals are more prone to the experience of negative alterations to the body since they are more weight-focused:
H6:. The effect of avatar body size on body-size discrepancy (as hypothesized in H2) is moderated by DT, such that the difference in body-size discrepancy between the over- and healthy weight condition is higher among those with high DT compared to those with low DT.
3 Materials and methods
3.1 Design
A 2 (avatar body size: healthy weight vs. overweight) × 2 (visuotactile stimulation: congruent vs. incongruent) experiment between subjects-design was conducted. Negative affect toward the virtual body and body-size discrepancy were the dependent variables. Drive for thinness (DT) was measured and used as a moderator.
Participants were randomly assigned to one of the four experimental conditions: healthy weight avatar, incongruent VTS (n = 27); healthy weight avatar, congruent VTS (n = 26); overweight avatar, incongruent VTS (n = 29); overweight avatar, congruent VTS (n = 32). Data collection took place from April to October 2021 in the Media Design Lab of Tilburg University. The protocol for the experiment was approved by the Research Ethics and Data Management Committee of the Tilburg School of Humanities and Digital Science.
3.2 Participants and recruitment
Participants were recruited through the researchers’ personal networks, on campus, and via the university’s participant pool. Hence, the sample predominantly contained university students. All participants participated voluntarily and were rewarded with either 10 euros or one course credit. Several exclusion criteria were applied. Participants were excluded when a history of or a present eating disorder was reported, due to the likeliness of discomfort they would experience in response to the embodied experience in VR. Individuals with a BMI lower than 18.5 or higher than 25 were excluded from the study to assure observable (dis)similarity between the participants’ and virtual body size. This cut-off score was chosen following the definition of an underweight and overweight BMI (Voedingscentrum. | Voedingscentrum, 2020). Participants who had participated in related studies before—that is, in a study on body size and food choices in a virtual supermarket—were also excluded.
After removing two cases due to technical flaws (e.g., rendering issues), the final sample consisted of 114 Dutch-speaking participants: the majority were female (64%), 75% were studying or had finished study at university (bachelor's or master's), and 24% were studying or had finished study at higher vocational education. The participants had an average BMI of 21.86, ranging from 18.50 to 24.88 (SD = 1.66).
3.3 Materials and manipulations
3.3.1 Hardware
The virtual experience was established using an HTC Vive Head-Mounted Display (HMD). Two trackers were attached to the feet and two controllers were held by the participant. These were synchronized with four base stations to demarcate the virtual arena and render the participants’ movements in the virtual space.
3.3.2 Virtual environment and avatar
The virtual living room to which participants were transported had been used in a previous study (van der Waal et al., 2021). Participants could view their virtual body from the first-person perspective and through a virtual mirror placed in the virtual living room (Figure 1). The virtual face was covered by the HMD to reduce the influence of facial dissimilarities and facial expressions on the VR experience (Jun et al., 2018). The clothes worn by the virtual avatar and skin tone were equal across all conditions, and the avatar’s gender was adapted to the participant’s gender. Visuomotor synchrony was enabled in all conditions, providing participants with agency over the virtual body (Kokkinara and Slater, 2014). Additionally, in all conditions, participants were to do a movement task with the goal of enhancing the feeling of agency over the virtual body.
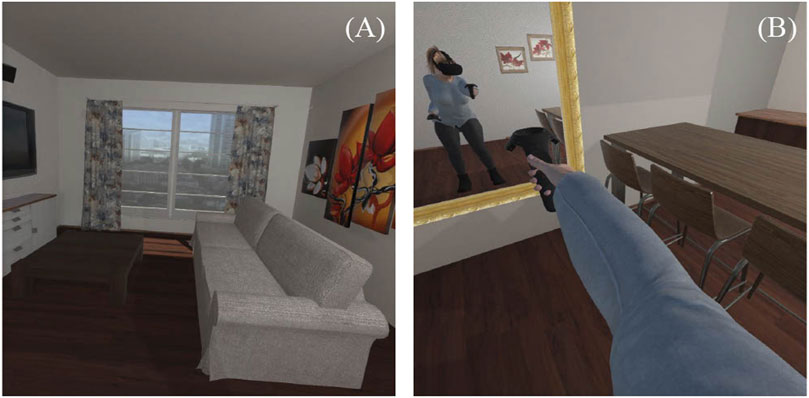
FIGURE 1. Depiction of the virtual environment from the participant’s perspective. Note. (A) Virtual environment on participant’s left, (B) Participant’s point of view when looking at one’s virtual arm.
3.3.3 Manipulation of avatar body size
Four pre-designed avatars were created using Reallusion Character Creator software (Figure 2). This software enabled changes to the degree of “body fat” on a scale of 0–100, rather than by means of BMI. Hence, an online pre-test was conducted to determine body size for the healthy weight and for the overweight avatar. In the pre-test, participants were presented with six differently sized avatars matched to their gender (see the Supplementary Material) and asked to what extent the avatar resembled their own body size and whether they considered the avatar overweight.
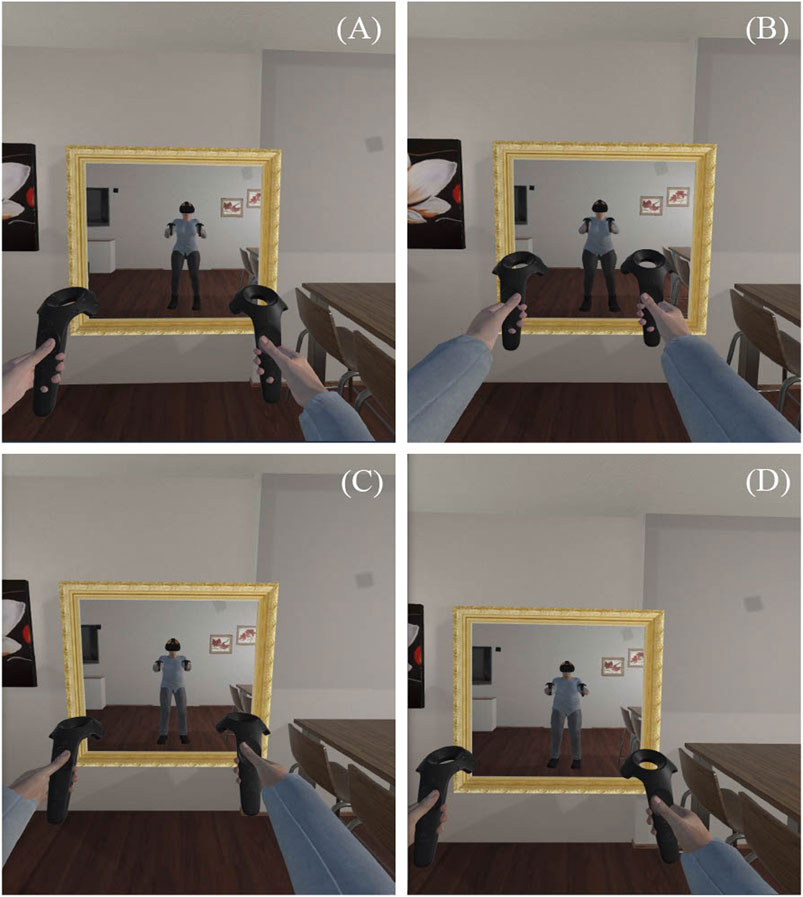
FIGURE 2. Healthy weight and overweight male and female avatar, presented from the participant’s perspective. Note. (A) Female healthy weight avatar, (B) Female overweight avatar, (C) Male healthy weight avatar, (D) Male overweight avatar.
To determine the size of the healthy weight avatar, participants were grouped based on their BMI (18.5–25): low BMI < 22.87 > high BMI. The low BMI group perceived the thinnest avatar (0) as significantly more similar to their own body than the high BMI group. The avatar with a body size of 15 was not perceived as significantly different to their own body in either of the two groups (low or high BMI). Hence, the body size for the healthy weight avatar was set at 15.
For the overweight avatar, the extent to which it was perceived as overweight differed significantly between participants; no inferences could be made based on this data. Hence, the avatar was set at 45, to keep the body size somewhat realistic and to take into consideration future studies with overweight participants.
Depending on the condition, participants embodied the healthy weight or overweight virtual avatar, in which a change in body weight could primarily be noticed in the size of the abdomen.
3.3.4 Manipulation of visuotactile stimulation
Either congruent or incongruent visuotactile stimulation (VTS) was applied, depending on the experimental condition. For the VTS procedure, participants stretched their arms in front of their body so that the experimenter could stroke their arm with a controller (Figures 3A,B). In both conditions, VTS was applied for 45 s on each arm. After 45 s, the controllers switched arms and the procedure was repeated. The experimenter wore earphones in which the time and pace of the VTS application were dictated via a metronome.

FIGURE 3. Depiction of the VTS procedure. Note. (A) Congruent VTS condition, controller touches arm, (B) Incongruent VTS condition, left controller touches arm, right controller does not touch the arm (from the experimenter’s perspective), (C) Participant’s viewpoint during the VTS procedure in both conditions, seeing a controller stroking the virtual arm.
In the congruent VTS condition, participants saw a controller stroking the VR arm and they felt this stroking on their real arm on the same side. This enabled the illusion that the virtual arm was being stroked. An extra controller was turned on in order to be visible in the virtual environment that was used to create this illusion. The experimenter consecutively stroked the participant’s real arm (Kokkinara and Slater, 2014) for 3 s while moving down the arm to the wrist. Some space was left between the controller and the arm when the controller went back up (in one second). To illustrate, Figure 3A shows the experimental setup in the congruent VTS condition and Figure 3C shows the participant’s viewpoint.
In the incongruent VTS condition, participants saw their arm being stroked in VR but they felt this stroking on their other arm, creating a mismatch of perceived touch and location of the touch. This was applied by the use of two controllers, one being turned off and one being turned on. The activated controller did not touch but moved along the real arm whilst, in VR, the illusion was created that the controller did touch the arm (see Figure 3C). Simultaneously, the experimenter stroked the participant’s other arm with the controller which was not visible in VR. In this way, the controller was felt on one arm and perceived on the other arm in VR, establishing a mismatch of location (Perez-Marcos et al., 2018). Figure 3B illustrates the setup for the incongruent VTS procedure.
3.4 Measurements
3.4.1 Drive for thinness
A Dutch translation of the subscale “Drive for Thinness” (DT) from The Eating Disorder Inventory 2 (EDI-2) was used to measure body weight and shape importance. The “Drive for Thinness” scale is one of the EDI-2 subscales that measures Eating Disorder Risk Symptoms (Van Strien, 2002). The scale comprises seven items measuring a.o., “fear to gain weight,” “importance of weight,” and “desire to be thin.” Answers to statements such as “I am afraid of gaining weight” were reported on a six-point Likert scale (1 = never, 6 = always). The reliability of the subscale was good (α = 0.88) and was also previously found to be a sensible measure for DT for non-eating disordered individuals (Van Strien and Ouwens, 2003).
Since previous research has shown that males and females differ significantly with regard to their scores on this scale (Smith et al., 2017), the DT scale was categorized differently for males and females. That is, the DT scale was split at the 33rd percentile and at the 67th percentile for males and females separately. The male and female categories were then merged into one variable. For the male subgroups, all values below 1.89 were considered “low DT” (n = 14), values between 1.89 and 2.86 were considered “moderate DT” (n = 15), and values greater than 2.86 were considered “high DT” (n = 12). For females, values below 2.43 were considered “low DT” (n = 25), values between 2.43 and 3.61 were considered “moderate DT” (n = 24), and values greater than 2.61 were considered “high DT” (n = 24).
3.4.2 Body-size discrepancy
As with Porras Garcia et al. (2019), a figural drawing scale was used to measure the subjects’ own estimated body size after the virtual experience. This scale consisted of 17 female or male contour-line drawings, representing adults with a weight ranging from 60% below the average BMI to 140% above it (Gardner and Brown, 2010). A difference in each figural drawing represented a 5% change in body weight, ranging from 16.92 to 39.48 for women, and 16.68 to 38.92 for men.
Participants were presented with the figural drawing scale and had to indicate which drawing best matched their own body size by means of a slider. Participants were not presented with the percentages belonging to the scale.
The percentages were converted to BMI for each participant. To calculate the discrepancy between one’s real body size and one’s estimated own body size after the experiment, the estimated BMI was subtracted from the actual BMI. The final measure ranged from −9.55 (estimating one’s own body to be larger than the actual BMI) to 6.84 (estimating one’s own body size to be smaller than the actual BMI), with a mean of −2.04 (SD = 3.11).
3.4.3 Negative affect
Negative affect toward the virtual body was measured by an Emotion Rating Scale (ERS), which is a measurement of affect that addresses specific emotions by rating them individually on their prevalence in a specific context. This type of measurement has been used before in the assessment of emotions in body exposure therapy (Vocks et al., 2007; Trentowska et al., 2013) but, until now, has not been applied in the context of VR. The ERS provided the participants with 11 distinct body-related emotions (e.g., guilt, distress, fear). Participants were asked to think about the experience of owning the virtual body in retrospect and report their feelings by means of the following question “To what extent did you feel < Emotion (e.g., shame) > toward the virtual body during the virtual experience?” on a six-point Likert scale (1 = not at all, 6 = extreme). Mean sum scores were calculated per participant. The ERS can be used for time frames ranging from “during the last year” to “right now” and is therefore considered an appropriate measure to study retrospective emotion evaluation. The ERS was taken in retrospect rather than during the virtual experience due to technological constraints and to prevent the ERS from influencing the cover story and measurements used for other studies.
Based on previous studies that investigated emotional responses toward the body in real life, 11 negative emotions were included in this study. In previous studies, sadness, tension, fear, uneasiness, frustration, distress, reduced self-confidence, and disgust were displayed by individuals experiencing negative affect toward their body (Tuschen-Caffier et al., 2003; Vocks et al., 2007; Trentowska et al., 2013). Other studies showed that the self-conscious body-related emotions of shame and guilt are often associated with perceived self-discrepancies (Castonguay et al., 2012) and are the emotions underlying “fear of fatness and weight gain” (Levinson et al., 2020). Therefore, guilt and shame were included in the negative affect subscale. Last, “shocked” was added to the negative affect scale. The latter emotion is not predominantly experienced in real-life as weight gain occurs gradually; however, “feeling shocked” can potentially arise when a sudden discrepancy between the perceived and ideal/ought body arises in VR. The order of the items was randomized for each individual. The scale demonstrated sound psychometric properties, reporting a good internal consistency for the complete scale (α = 0.92; M = 1.97, SD = 0.91).
3.4.4 Manipulation checks
To assess whether the experimental manipulations worked as intended, manipulation checks were included for avatar body size and VTS. For the manipulation check of avatar body size, four items that assessed judgments about the body weight of the virtual avatar (in comparison to one’s own body weight) were merged into one scale (i.e., “The avatar had a higher body weight than myself,” “The avatar in the virtual environment was overweight,” “The body weight of my avatar was approximately the same as my own body weight,” and “It felt as if my body size was different from my own body size in the virtual environment”). Responses were rated on a seven-point Likert scale from 1 (totally disagree) to 7 (totally agree), and one item was reverse-coded. The internal consistency of this scale was sufficient (α = 0.70, M = 5.47, SD = 1.19).
A manipulation check was included for visuotactile stimulation (VTS) to check whether congruent and incongruent VTS were accurately perceived across conditions by asking the following question “It felt like the controller that moved through the virtual space caused the touch on my arm” (M = 4.44, SD = 2.29). Responses were rated on a seven-point Likert scale of 1 (totally disagree) to 7 (totally agree).
3.4.5 Procedure
The study was part of a larger study (van der Waal, Janssen, Antheunis, Otte, Van der Laan). Tasks outside the scope of the current study will be briefly mentioned but not accounted for in the analysis and discussion. All lab procedures conformed to the COVID-19 health guidelines that applied at that time.
Participants received information about the study and its procedures, partly by means of a cover story. They were told they were about to participate in three different and unrelated studies (Boldero et al., 2005): body proportions and motor movements in VR (Piryankova et al., 2014), personality traits and satisfaction with the self, and (Levinson et al., 2020) taste perception and the evaluation of house vs. premium branded food products. They were also instructed to complete an inclusion questionnaire, either online or on campus. When all inclusion criteria were met, participants were invited to the lab where any remaining questions could be asked and informed consent signed.
Upon arrival in the lab, participants were provided with instructions. They were told they were about to see a virtual representation of the self and that the avatar’s body measurements could differ from their own measurements (e.g., longer arms), in order to boost the cover story. They were instructed to perform several movements in the virtual environment which were first demonstrated by the experimenter. The experimenter emphasized that the participant could not touch his or her own physical body. They were also instructed that they would be touched with a controller, which was part of the VTS procedure. Participants were then transported to the virtual living room, where they were asked to slowly execute the movements as practiced before. Lastly, either congruent or incongruent VTS was applied to the participant’s arms for 2 × 45 s by the experimenter.
After the virtual experience, participants were seated in a separate room and asked to complete a questionnaire that was said to correspond to “Study 1: body proportions and motor movements in VR.” In fact, VBO and negative affect were measured in this questionnaire. Subsequently, participants continued with the supposed second study in which drive for thinness, body-size perceptions, and manipulation checks were measured via a questionnaire. Several other questions were asked, which were only relevant for other studies. After completion of this questionnaire, the experimenter prepared the “third” experiment. Here, participants executed a bogus taste task. As this is not relevant to the present study, it will not be discussed any further. When the experimental procedure was completed, the participants were debriefed, thanked, and instructed to not discuss the procedure of the study with others. Respecting COVID-19 measures, all rooms and materials were disinfected after each participant.
3.5 Assumption testing and data analysis strategy
Statistical analyses were performed using R. An ANOVA was run to analyze the data. Before analysis, all responses were checked for completeness, data were cleaned, and assumptions were tested. Not all participants completely filled out the negative affect scale (four missing values amongst four participants) but these participants were kept for analysis as a mean score still could be calculated for the outcome variable.
Skewness and kurtosis were inspected and the Shapiro Wilk test was run to determine whether the data were normally distributed in the combinations of conditions for which the effects were expected—avatar body-size * VTS and avatar body-size * DT. Inspection of the data led to the conclusion that the data were positively skewed on the negative affect variable, which was confirmed by the Shapiro-Wilk test. The assumption of homogeneity of variance between the groups was assessed with Levene’s test and not met either. For the dependent variable body-size estimation, both the assumption of normality and the assumption of homogeneity of variances were met.
Data were log-transformed to reduce the skewness of the distribution. However, it was still decided to run an ANOVA on the non-transformed data because 1) outcomes of data analysis on the transformed data hardly differed from analysis of the raw data, 2) an ANOVA has shown to be a fairly robust measure even in the case of deviation from normality (Schmider et al., 2010), and 3) transforming the data would lead to interpretation issues.
4 Results
4.1 Randomization checks
ANOVAs and chi-square tests revealed that participants were equally distributed across the four conditions regarding DT [F (3, 110) = 2.19, p = 0.094], BMI [F (3, 110) = 1.37, p = 0.256], age [F (3, 110) = 0.72, p = 0.542], gender [χ2 (Levinson et al., 2020) = 6.20, p = 0.102], and educational level [χ2 (Levinson et al., 2020) = 12.92, p = 0.167].
4.2 Manipulation checks
To assess whether participants perceived the avatar body size as (dis)similar to their own body, an independent t-test was performed, including the manipulation check variable as dependent (i.e., four items merged into one scale variable) and avatar body size as an independent variable. There was a significant difference found in terms of the assessment of the avatar’s weight between the overweight condition (M = 6.25, SD = 0.64) and the healthy weight condition (M = 4.57, SD = 1.03), t (84.82) = −10.35, p < 0.001, 95% CI [−2.01, −1.36], d = 2.00, concluding that the manipulation was successful.
To assess whether the VTS manipulation was successful, an independent t-test was conducted, showing that participants in the congruent VTS condition (M = 5.47, SD = 1.82) agreed more with the statement that “The object in the virtual environment caused the feelings of touch on my arm” than participants in the incongruent VTS condition (M = 3.38, SD = 2.26), t(105.46) = −5.43, p < 0.001, 95% CI [−2.85, −1.33], d = 1.02. It can be concluded that the VTS manipulation was successful, with mean scores showing that the perception of the controller producing the touch in the congruent condition was higher and more absent than in the incongruent condition.
4.3 Hypotheses testing
Four ANOVAs were conducted to investigate the effects of avatar body size, and the moderating roles of VTS and DT, on experienced negative affect toward the virtual body and on body-size discrepancies. All results were interpreted at the 95% confidence interval. Means and standard deviations of negative affect for each experimental condition are specified in Tables 1, 2.
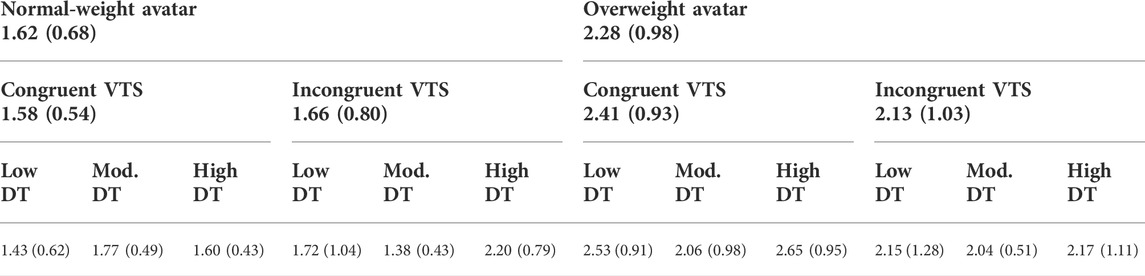
TABLE 1. Means (SD)s of negative affect per experimental condition.
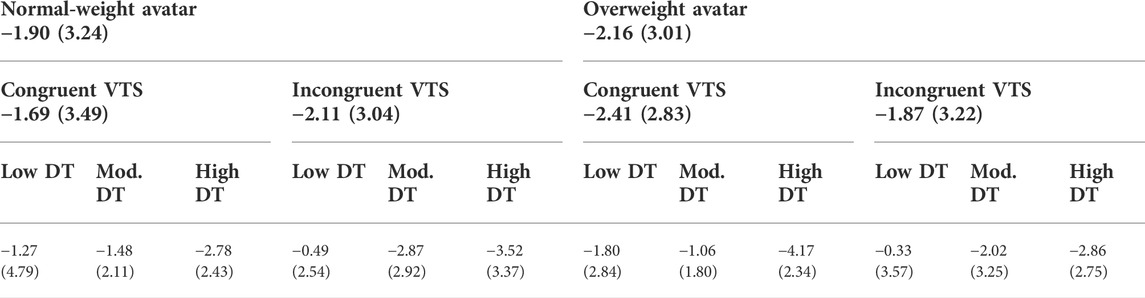
TABLE 2. Means (SD)s of body-size discrepancy per experimental condition.
4.3.1 Negative affect
The ANOVA including VTS as moderator and negative affect as a dependent variable revealed a significant main effect for avatar body size—F (1, 110) = 16.82, p < 0.001, ηp2 = 0.13, where participants in the overweight condition (M = 2.28, SD = 0.98) experienced more negative affect than participants in the healthy weight condition (M = 1.62, SD = 0.68). Hence, H1, in which it was hypothesized that participants in the overweight condition would experience more negative affect toward their virtual avatar than participants in the healthy weight condition, was supported. The interaction between avatar body size and VTS was not significant—F (1, 110) = 1.21, p = 0.275, ηp2 = 0.01. Thus, H3, in which it was hypothesized that VTS moderated the effect of avatar body size on negative affect, was not supported.
The second ANOVA, including DT as moderator, did not show a significant interaction between avatar body size and DT—F (1, 110) = 0.16, p = 0.691, ηp2 = 0.12. Thus, no support was found for H5, which hypothesized that those with a high DT would experience stronger negative affect toward the overweight avatar compared to the healthy weight avatar than those with a low DT.
4.3.2 Body-size discrepancy
Another ANOVA was conducted in which VTS was included as a moderator and body-size discrepancy as the dependent variable. In H2, the main effect of avatar body size on body-size discrepancy was hypothesized, such that those in the overweight condition would have a larger discrepancy between estimated BMI and real BMI than those in the healthy weight condition. However, this effect was not significant—F (1, 110) = 0.18, p = 0.671, ηp2 = 0.002. Thus, H2 was not supported. Additionally, there was no interaction effect of VTS on the effect of avatar body size on body-size discrepancy, as predicted in H4—F (1, 110) = 0.66, p = 0.418, ηp2 = 0.01—which led to rejection of H4.
The ANOVA including DT also led to null findings with regard to the moderation effect—F (1, 110) = 0.02, p = 0.897, ηp2 = 0.00. This led to the rejection of H6, which hypothesized that the main effect of avatar body size on body-size discrepancy would be stronger with a high DT than with a low DT.
5 Discussion
In the present study, the affective and perceptual responses toward an embodied overweight virtual body were assessed among healthy weight participants. While previous studies examined whether the embodiment of an overweight virtual body leads to affective responses toward one’s own body, this is the first study to investigate affective responses toward the virtual body. To build further on previous studies that solely investigated perceptual changes as an outcome measure, the current study also included this. Lastly, we aimed to identify conditions under which this negative emotion elicitation occurs more strongly, and hence included a moderator operating at the procedure level (VTS) and one at the user level (DT).
5.1 The effect of avatar body size on negative affect
In line with the first hypothesis, we found that the embodiment of an overweight virtual body elicited stronger negative affect toward the virtual body compared to the embodiment of a healthy weight virtual body. This study adds to previous studies in the domain of full-body illusions, which have shown that embodying an overweight avatar leads to an increase in body anxiety and body dissatisfaction toward one’s own body (Ferrer-Garcia et al., 2017; Preston and Ehrsson, 2018; Porras Garcia et al., 2019). Knowing from the current study that embodying an overweight avatar influences affective responses toward the virtual body, it would be interesting to combine in one study measurements of negative affect toward the virtual body during, and negative affect toward the own body after, the illusion. Such a study could examine whether a causal relationship exists between the experience of negative affect toward the virtual body and toward one’s own body. This could be hypothesized based on the excitation transfer theory, which posits that an individual who experiences any negative or positive affect misattributes any residual affect to a subsequent situation (Zillmann, 1971). For example, a study showed that being in a virtual environment with either anxious, relaxing, or neutral cues led to the experience of the same emotions after the virtual experience (Riva et al., 2007). In the realm of VR advertising, it has been demonstrated that brands in VR games elicit a positive emotional response (i.e., arousal and valence), and these emotional responses in VR transfer to a more positive brand attitude and higher purchase intention (Van Berlo et al., 2021). Whether negative affect elicited through the embodiment of a virtual avatar, as found in the current study, also transfers to the real body should be further investigated.
Putting this result in a broader context, anti-fat prejudices and stigmatization of obese people have been prevalent in Western society for many years, paired with a negative evaluation of overweight people (Battan and Stearns, 1998). This negative affect is seen as a result of beliefs that being overweight violates health standards, moral values, and (social) responsibility (Biefeld and Brown, 2022). For example, an emotion like disgust has been found to be an important factor in the evaluation of obese people (Vartanian, 2010). The current study shows that negative affective responses are also elicited toward a virtual body when having the illusion of owning this body.
5.2 The effect of avatar body size on body-size perceptions
The current study did not find support for the second hypothesis that owning an overweight virtual body could lead to a shift in body-size perceptions in line with the overweight body, even though participants perceived the overweight avatar as indeed heavier than the healthy weight avatar. It is difficult to establish which factors enabled this shift in previous studies, as various experimental designs, samples, and outcome measures are used to study this relationship, impeding a proper comparison of the studies.
To our knowledge, only one study included avatar body size as a between-subjects factor (while other studies employed a within-subjects design or exposed all participants to the same avatar) and found an effect of embodying an overweight avatar on body-size estimations of the experienced body (i.e., the body that the participant feels she has at that moment) rather than on the physical body (Piryankova et al., 2014). This could indicate that participants still have some knowledge stored about their physical body size, which ensures that estimations regarding their actual body are still accurate, although the body is not experienced in that way at that moment. These results indicate that the distinction between one’s physical body and experienced body size might be important to make. Related to this are two studies that measured body-size estimations in the virtual environment and retrieved significant effects (Normand et al., 2011; Piryankova et al., 2014). In these studies, participants were not exposed to their own body when estimating their body size, which might have resulted in the fact that participants paid more attention to the virtual body because their own body was not visible during the experience.
Nevertheless, another study found an effect of body-size estimation using a figural drawing scale (as in the current study) after the virtual experience, without distinguishing between an experienced and physical body (Ferrer-Garcia et al., 2017). This study, however, employed a within-subjects design, whereby participants might have been able to compare the avatar’s body sizes in the different conditions, possibly leading to contrast effects. As these abovementioned studies are the only ones that included an overweight avatar, replication studies are necessary to understand whether methodological factors underlie the significant findings retrieved in these studies.
Other scholars used a skinny virtual avatar in combination with a pre- and post-estimation of body size, and found effects on body-size estimations among obese participants (Scarpina et al., 2019) and healthy weight participants (Serino et al., 2016; Scarpina et al., 2019). In these studies, body-size estimation was operationalized as the distance between two adhesive markers on a blackboard for participants to indicate their body size. It should also be noted that Scarpina et al. (2019) only found this effect for estimated hip size and not for other body parts. Lastly, a study using a healthy weight avatar included anorexia patients and healthy controls, whereby body-size estimations were measured at two time points (Keizer et al., 2016). They also found significant changes in body-size estimation, however, among both anorexia nervosa patients and healthy subjects. In all these studies, body-size estimations of healthy weight participants were affected by embodying a skinny or healthy weight avatar. This provides evidence for the malleability of body-size perceptions among healthy weight individuals, even though the current study does not provide support for this after embodying an overweight avatar. An alternative explanation could be that body-size perceptions are more easily adjusted in the direction of a skinny or healthy weight avatar and less in the direction of an overweight avatar. It would be interesting for future studies to include three avatars in the experimental design (i.e., skinny, normal, and overweight) to be able to identify how shifts in perceptions occur with regard to these three body sizes.
Based on previous studies, it is difficult to identify explanations for when effects on perceptions do and do not occur. Future research should place more focus on methodology—for instance, on what is the most accurate way to measure these body-size perceptions, and the boundary conditions under which these effects occur.
5.3 Possible pathways for affective responses to occur
A remaining question is the mechanisms by which negative affect toward the own body is elicited, as found by previous studies (Ferrer-Garcia et al., 2017; Preston and Ehrsson, 2018; Porras Garcia et al., 2019). This is a fundamental question, as negative affect experienced toward the virtual body could be a driver for effects occurring with regard to the real body—for example, emotions toward one’s own body or altered body-size perceptions. Two pathways are thus considered plausible: 1) an effect of avatar body size on negative affect toward the virtual body, which facilitates negative affect toward one’s own body (i.e., via emotion transfer as explained above); 2) an effect of avatar body size on body-size perceptions which facilitates negative affect toward one’s own body. While previous studies have argued that the full-body illusion can modify the affective experience of one’s body through a perception shift, it is also arguable, based on the current study’s findings, that an emotion transfer takes place, as proposed in Pathway 1. Future studies should include measurements of negative affect toward one’s own body, to examine the mediating roles of the variables included in the current study.
5.4 The moderating role of VTS
The effects of avatar body size on negative affect toward the virtual body (H3) and body-size perceptions (H4) were not moderated by VTS, which contradicted expectations. Previous studies argued that, in order to change perceptions toward one’s own body, VBO must be induced (Preston and Ehrsson, 2014), which can be established in various ways. In setups where avatars are static objects, it is known that VTS is an important facilitator of VBO (e.g., 20). Nevertheless, the results of the current study indicate that VTS is of less importance in the current setup, which is characterized by synchronized movements between the avatar and its user. This is in line with a previous study that demonstrated that visuomotor synchrony is a stronger predictor of VBO and that asynchronous VTS can be discounted when movements are synchronized (Kokkinara and Slater, 2014). The null effects that were retrieved regarding VTS could be explained by the notion that VBO was already high due to the advanced VR setup used in this study, and that the addition of VTS could not increase VBO further (i.e., ceiling effects). Consequently, negative affect and body-size perceptions were not influenced by VTS. This finding also leads to the discussion of whether VBO is something that affects certain outcome measures linearly (e.g., higher VBO leads to stronger affective responses) or whether VBO is an experience that you simply have or do not have.
VTS’s strengthening of affective responses to virtual stimuli in other studies using static avatars (Guterstam et al., 2015; Gall et al., 2021) supports this explanation. Only one study that measured the affective component of body image, by measuring body anxiety toward the own body, also included an asynchronous control condition for VTS (Porras Garcia et al., 2019). They found that it was only in the overweight virtual body condition that synchronous VTS led to stronger body anxiety levels compared to asynchronous VTS. In the present study, congruent VTS did not amplify the experience of negative affect toward the virtual body in the overweight condition, although significantly higher feelings of VBO were reported in the congruent condition (van der Waal, Janssen, Antheunis, Otte, Van der Laan). It is possible that VTS is of more importance when assessing effects on one’s own body, as this procedure establishes the integration of one’s body with the virtual body. The emotion elicited toward the virtual body might already be established when viewing a virtual body from a first-person perspective, thus requiring less powerful methods to establish the illusion.
However, this alternative explanation does not corroborate our finding that the effect on body-size perceptions, which is an effect regarding one’s own body, is not moderated by VTS. Interestingly, the majority of studies investigating virtual body sizes did not find significant effects of VTS as a moderator on body-size perceptions (Piryankova et al., 2014; Keizer et al., 2016; Serino et al., 2016; Porras Garcia et al., 2019); some found (partial) support for VTS as a moderator (Normand et al., 2011; Scarpina et al., 2019). Again, it is difficult to compare these and the current study’s findings, as VTS is applied in distinct ways (e.g., self-administered: 18; administered by the experimenter: 2, 4, 6, 17) for durations varying from 90 s (e.g., 4) to 4 min (e.g., 18) and on various body parts—for example, on the abdomen (e.g., 4, 6, 17) or on the arms and legs (e.g., 2). In the current study, VTS was applied by the experimenter for 90 s on the arms. The location where this is applied might be of importance here, as the increase of the abdomen of the virtual body compared to the subject’s own abdomen is probably larger than the increase in the arms of the virtual body compared to the subject’s own arms, which could lead to a stronger perceptual shift regarding that specific body part. A more detailed investigation into the stimulation of, and perception change of, different body parts will facilitate our understanding of how these changes in perception occur.
5.5 The moderating role of drive for thinness
Contrary to what was expected, participants’ degree of DT did not significantly influence the level of experienced negative affect, as hypothesized in H5, nor body-size perceptions, as hypothesized in H6. Ferrer-Garcia et al. (2017) found a significant increment in negative affect toward one’s own body (i.e., body anxiety and fear to gain weight) solely amongst high DT individuals after the embodiment of a larger-sized avatar. Similarly, Preston and Ehrsson (2018) found that the experience of negative affect toward one’s own body after embodying an overweight avatar was dependent on eating disorder traits, even in a non-clinical sample. This could mean that DT only affects the relationship when emotions are transferred toward one’s own body and not when assessing a virtual body. Alternatively, the current sample might have been too homogeneous to detect effects, as it mainly comprised (university) students, all without (prior) diagnoses of an eating disorder. Future studies could aim to study healthy subjects with different levels of body shape and weight concerns. Gender should also be taken as a control variable, as women have shown more proneness to being affected by body-size change than men (Preston and Ehrsson, 2018).
5.6 Implications
Emotions often precede thoughts and behavior; thus, when investigating the potential of full-body illusions as an intervention tool to establish perceptual changes or behavior changes, it is important to understand the effects of embodied experiences on perception and affect toward the virtual and the biological, knowing that negative affect is elicited with the embodiment of an overweight avatar. Furthermore, since virtual avatars are becoming increasingly prevalent in society (i.e., MetaVerse, VRchat), there is a need to understand how these could affect their users and whether certain psychological traits make users more vulnerable to being emotionally affected.
6 Conclusion
The current study aimed to investigate whether affective and perceptual responses occur in response to embodying an overweight avatar in virtual reality, and whether visuotactile stimulation (VTS) and drive for thinness (DT) moderated the effects. This is the first study to demonstrate that emotions are elicited toward the virtual body, irrespective of VTS or DT. This finding provides new research directions, as it is likely that this emotion elicitation is a driving force behind any effects that could occur in response to an overweight virtual body, including negative affect toward one’s own body and changes in body perception. This study also indicates that, among healthy subjects, body-size perceptions were not altered after the embodiment of an overweight avatar and that VTS and DT did not play a role in this relationship. Hence, body-size perceptions might not be vulnerable to change among healthy individuals, opposing conclusions of previous studies. VTS might have been of less importance in this setup than in other studies, as movements between the avatar and the user were synchronized in the current study, which might have already sufficiently facilitated the experience of having a virtual body. Future research is needed to gather more support for this finding.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Research Ethics and Data Management Committee of the Tilburg School of Humanities and Digital Science. The patients/participants provided their written informed consent to participate in this study.
Author contributions
NvdW: conceptualization, data curation, formal analysis, resources, project administration, writing (original draft), supervision. JvB: conceptualization, data collection, formal analysis, writing (original draft). NvdL: writing (review and editing), supervision.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2022.989676/full#supplementary-material
References
Battan, J. F., and Stearns, P. N. (1998). Fat history: Bodies and beauty in the modern west. J. Am. Hist. 85 (1), 194. doi:10.2307/2568446
Biefeld, S. D., and Brown, C. S. (2022). Fat, sexy, and human? Perceptions of plus-size sexualized women and dehumanization. Body Image 42, 84–97. doi:10.1016/j.bodyim.2022.05.002
Boldero, J. M., Moretti, M. M., Bell, R. C., and Francis, J. J. (2005). Self-discrepancies and negative affect: A primer on when to look for specificity, and how to find it. Aust. J. Psychol. 57, 139–147. doi:10.1080/00049530500048730
Cardoso, A., Oliveira, S., and Ferreira, C. (2020). Negative and positive affect and disordered eating: The adaptive role of intuitive eating and body image flexibility. Clin. Psychol. Aust. Psychol. Soc. 24 (2), 176–185. doi:10.1111/cp.12224
Cash, T. F., Phillips, K. A., Santos, M. T., and Hrabosky, J. I. (2004). Measuring “negative body image”: Validation of the body image disturbance questionnaire in a nonclinical population. Body Image 1 (4), 363–372. doi:10.1016/j.bodyim.2004.10.001
Castonguay, A. L., Brunet, J., Ferguson, L., and Sabiston, C. M. (2012). Weight-related actual and ideal self-states, discrepancies, and shame, guilt, and pride: Examining associations within the process model of self-conscious emotions. Body Image 9 (4), 488–494. doi:10.1016/j.bodyim.2012.07.003
Cuesta-Zamora, C., González-Martí, I., and García-López, L. M. (2018). The role of trait emotional intelligence in body dissatisfaction and eating disorder symptoms in preadolescents and adolescents. Pers. Individ. Dif. 126, 1–6. doi:10.1016/j.paid.2017.12.021
DelRosario, M. W., Brines, J. L., and Coleman, W. R. (1984). Emotional response patterns to body weight-related cues. Pers. Soc. Psychol. Bull. 10 (3), 369–375. doi:10.1177/0146167284103004
Ferrer-García, M., and Gutiérrez-Maldonado, J. (2012). The use of virtual reality in the study, assessment, and treatment of body image in eating disorders and nonclinical samples: A review of the literature. Body Image 9, 1–11. doi:10.1016/j.bodyim.2011.10.001
Ferrer-Garcia, M., Porras-Garcia, B., Gonzalez-Ibanez, C., Gracia-Blanes, M., Vilalta-Abella, F., Pla-Sanjuanelo, J., et al. (2017). Does owning a “fatter” virtual body increase body anxiety in college students? Annu. Rev. CyberTherapy Telemed. 15, 147–153.
Gall, D., Roth, D., Stauffert, J. P., Zarges, J., and Latoschik, M. E. (2021). Embodiment in virtual reality intensifies emotional responses to virtual stimuli. Front. Psychol. 12, 674179. doi:10.3389/fpsyg.2021.674179
Gardner, R. M., and Brown, D. L. (2010). Body image assessment: A review of figural drawing scales. Personality Individ. Differ. 48, 107–111. doi:10.1016/j.paid.2009.08.017
Gleeson, K., Frith, H., and De), (2006). (De)constructing body image. J. Health Psychol. 11, 79–90. doi:10.1177/1359105306058851
Guterstam, A., Abdulkarim, Z., and Ehrsson, H. H. (2015). Illusory ownership of an invisible body reduces autonomic and subjective social anxiety responses. Sci. Rep. 5 (1), 9831–9838. doi:10.1038/srep09831
Hewig, J., Cooper, S., Trippe, R. H., Hecht, H., Straube, T., and Miltner, W. H. R. (2008). Drive for thinness and attention toward specific body parts in a nonclinical sample. Psychosom. Med. 70 (6), 729–736. doi:10.1097/psy.0b013e31817e41d3
Higgins, E. T. (1989). Self-discrepancy theory: What patterns of self-beliefs cause people to suffer? Adv. Exp. Soc. Psychol. 22 (C), 93–136.
Jun, J., Jung, M., Kim, S. Y., and Kim, K. (2018). “Full-body ownership illusion can change our emotion,” in Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, Canada (Association for Computing Machinery), 1–11. [Internet] Available at: https://dl.acm.org/doi/abs/10.1145/3173574.3174175?casa_token=hwCEe3JqrBkAAAAA:wU93Kb-KToeFGOsaVRmPjtT5y7iuzmkX7t-eMT_DWA8vpzbWUnbJwE1Ek8ie WGxVgkZCFHUzRtiiRQ.
Keizer, A., Van Elburg, A., Helms, R., and Dijkerman, H. C. (2016). A virtual reality full body illusion improves body image disturbance in anorexia nervosa. PLoS One 11 (10), e0163921. doi:10.1371/journal.pone.0163921
Kokkinara, E., Kilteni, K., Blom, K. J., and Slater, M. (2016). First person perspective of seated participants over a walking virtual body leads to illusory agency over the walking. Sci. Rep. 6, 1–11. doi:10.1038/srep28879
Kokkinara, E., and Slater, M. (2014). Measuring the effects through time of the influence of visuomotor and visuotactile synchronous stimulation on a virtual body ownership illusion. Perception 43 (1), 43–58. doi:10.1068/p7545
Levinson, C. A., Williams, B. M., and Christian, C. (2020). What are the emotions underlying feeling fat and fear of weight gain? J. Affect. Disord. 277, 146–152. doi:10.1016/j.jad.2020.08.012
Maselli, A., and Slater, M. (2013). The building blocks of the full body ownership illusion. Front. Hum. Neurosci. 7 (83), 83–15. doi:10.3389/fnhum.2013.00083
Normand, J. M., Giannopoulos, E., Spanlang, B., and Slater, M. (2011). Multisensory stimulation can induce an illusion of larger belly size in immersive virtual reality. PLoS One 6 (1), e16128. doi:10.1371/journal.pone.0016128
Perez-Marcos, D., Martini, M., Fuentes, C. T., Bellido Rivas, A. I., Haggard, P., and Sanchez-Vives, M. V. (2018). Selective distortion of body image by asynchronous visuotactile stimulation. Body Image 24, 55–61. doi:10.1016/j.bodyim.2017.11.002
Petkova, V. I., Khoshnevis, M., and Ehrsson, H. H. (2011). The perspective matters! Multisensory integration in egocentric reference frames determines full-body ownership. Front. Psychol. 2, 35. doi:10.3389/fpsyg.2011.00035
Piryankova, I. V., Wong, H. Y., Linkenauger, S. A., Stinson, C., Longo, M. R., Bülthoff, H. H., et al. (2014). Owning an overweight or underweight body: Distinguishing the physical, experienced and virtual body. PLoS One 9 (8). doi:10.1371/journal.pone.0103428
Porras Garcia, B., Ferrer Garcia, M., Olszewska, A., Yilmaz, L., González Ibañez, C., Gracia Blanes, M., et al. (2019). Is this my own body? Changing the perceptual and affective body image experience among college students using a new virtual reality embodiment-based technique. J. Clin. Med. 8 (7), 925. doi:10.3390/jcm8070925
Preston, C., and Ehrsson, H. H. (2014). Illusory changes in body size modulate body satisfaction in a way that is related to non-clinical eating disorder psychopathology. PLoS One 9 (1), e85773. doi:10.1371/journal.pone.0085773
Preston, C., and Ehrsson, H. H. (2018). Implicit and explicit changes in body satisfaction evoked by body size illusions: Implications for eating disorder vulnerability in women. PLoS One 13 (6), e0199426. doi:10.1371/journal.pone.0199426
Riva, G., Mantovani, F., Capideville, C. S., Preziosa, A., Morganti, F., Villani, D., et al. (2007). Affective interactions using virtual reality: The link between presence and emotions. Cyberpsychol. Behav. 10 (1), 45–56. doi:10.1089/cpb.2006.9993
Scarpina, F., Serino, S., Keizer, A., Chirico, A., Scacchi, M., Castelnuovo, G., et al. (2019). The effect of a virtual-reality full-body illusion on body representation in obesity. J. Clin. Med. 8 (9), 1330. doi:10.3390/jcm8091330
Schmider, E., Ziegler, M., Danay, E., Beyer, L., and Bühner, M. (2010). Is it Really Robust?: Reinvestigating the robustness of ANOVA against violations of the normal distribution assumption. Methodology 6 (4), 147–151. doi:10.1027/1614-2241/a000016
Serino, S., Pedroli, E., Keizer, A., Triberti, S., Dakanalis, A., Pallavicini, F., et al. (2016). Virtual reality body swapping: A tool for modifying the allocentric memory of the body. Cyberpsychol. Behav. Soc. Netw. 19 (2), 127–133. doi:10.1089/cyber.2015.0229
Slater, M., Perez-Marcos, D., Ehrsson, H. H., and Sanchez-Vives, M. V. (2009). Inducing illusory ownership of a virtual body. Front. Neurosci. 3, 214–220. doi:10.3389/neuro.01.029.2009
Smith, K. E. R., Mason, T. B., Murray, S. B., Griffiths, S., Leonard, R. C., Wetterneck, C. T., et al. (2017). Male clinical norms and sex differences on the eating disorder inventory (EDI) and eating disorder examination questionnaire (EDE-Q). Int. J. Eat. Disord. 50 (7), 769–775. doi:10.1002/eat.22716
Trentowska, M., Bender, C., and Tuschen-Caffier, B. (2013). Mirror exposure in women with bulimic symptoms: How do thoughts and emotions change in body image treatment? Behav. Res. Ther. 51 (1), 1–6. doi:10.1016/j.brat.2012.03.012
Tsakiris, M., Prabhu, G., and Haggard, P. (2006). Having a body versus moving your body: How agency structures body-ownership. Conscious. Cogn. 15 (2), 423–432. doi:10.1016/j.concog.2005.09.004
Tuschen-Caffier, B., Vögele, C., Bracht, S., and Hilbert, A. (2003). Psychological responses to body shape exposure in patients with bulimia nervosa. Behav. Res. Ther. 41 (5), 573–586. doi:10.1016/s0005-7967(02)00030-x
Van Berlo, Z. M. C., Van Reijmersdal, E. A., Smit, E. G., and Van der Laan, L. N. (2021). Brands in virtual reality games: Affective processes within computer-mediated consumer experiences. J. Bus. Res. 122, 458–465. doi:10.1016/j.jbusres.2020.09.006
van der Hoort, B., Guterstam, A., and Ehrsson, H. H. (2011). Being barbie: The size of one’s own body determines the perceived size of the world. PLoS One 6 (5), e20195. doi:10.1371/journal.pone.0020195
van der Waal, N. E., Janssen, L., Antheunis, M., Culleton, E., and van der Laan, L. N. (2021). The appeal of virtual chocolate: A systematic comparison of psychological and physiological food cue responses to virtual and real food. Food Qual. prefer. 90, 104167. doi:10.1016/j.foodqual.2020.104167
van der Waal, N. E., Janssen, L., Antheunis, M., Otte, M., and Van der Laan, L. N. Effects of embodying an overweight avatar on eating intentions and behavior: The moderating role of visuotactile stimulation. Prep.
Van Strien, T., and Ouwens, M. (2003). Validation of the Dutch EDI-2 in one clinical and two nonclinical Populations1. Eur. J. Psychol. Assess. 19 (1), 66–84. doi:10.1027//1015-5759.19.1.66
Van Strien, T. (2002). Eating disorder inventory-II, nederlandse versie. Amsterdam, Netherlands: Swets Test Publishers.
Vartanian, L. R. (2010). Disgust and perceived control in attitudes toward obese people. Int. J. Obes. (Lond). 34 (8), 1302–1307. doi:10.1038/ijo.2010.45
Vocks, S., Legenbauer, T., Wächter, A., Wucherer, M., and Kosfelder, J. (2007). What happens in the course of body exposure? Emotional, cognitive, and physiological reactions to mirror confrontation in eating disorders. J. Psychosom. Res. 62 (2), 231–239. doi:10.1016/j.jpsychores.2006.08.007
Vocks, S., Wächter, A., Wucherer, M., and Kosfelder, J. (2008). Look at yourself: Can body image therapy affect the cognitive and emotional response to seeing oneself in the mirror in eating disorders? Eur. Eat. Disord. Rev. 16 (2), 147–154. doi:10.1002/erv.825
Voedingscentrum. | Voedingscentrum (2020). Overgewicht: Voedingscentrum. Available at: https://www.voedingscentrum.nl/encyclopedie/overgewicht.aspx Jun 30, 2022).
Wiederman, M. W., and Pryor, T. L. (2000). Body dissatisfaction, bulimia, and depression among women: The mediating role of drive for thinness. Int. J. Eat. Disord. 27 (1), 90–95. doi:10.1002/(sici)1098-108x(200001)27:1<90::aid-eat10>3.0.co;2-0
Keywords: negative affect, body-size perception, visuotactile stimulation, drive for thinness, virtual body ownership
Citation: van der Waal NE, van Bokhorst JAW and van der Laan LN (2022) Identifying emotions toward an overweight avatar in Virtual Reality: The moderating effects of visuotactile stimulation and drive for thinness. Front. Virtual Real. 3:989676. doi: 10.3389/frvir.2022.989676
Received: 08 July 2022; Accepted: 20 September 2022;
Published: 13 October 2022.
Edited by:
Dimitra Anastasiadou, Universitat Autònoma de Barcelona, SpainReviewed by:
Pierre Bourdin, Open University of Catalonia, SpainFilip Škola, CYENS Centre of Excellence, Cyprus
Copyright © 2022 van der Waal, van Bokhorst and van der Laan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nadine Elisa van der Waal, bi5lLnZkd2FhbEB0aWxidXJndW5pdmVyc2l0eS5lZHU=