 Paul Best
Paul Best Alison McKenna1
Alison McKenna1 Paul Quinn
Paul Quinn Tom Van Daele
Tom Van Daele
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Virtual Real., 19 November 2020
Sec. Virtual Reality in Medicine
Volume 1 - 2020 | https://doi.org/10.3389/frvir.2020.563739
The evidence base for the use of immersive technologies, such as Virtual Reality (VR), for the treatment of Post-Traumatic Stress Disorder (PTSD) is compelling. Despite promising results wide spread use and adoption of this technology within routine clinical practice remains limited. A lack of detailed technical guidelines might be one of the reasons that hamper such uptake. To address this gap, the current review focuses on earlier design types, namely Clinical Case Reports in order to uncover additional detail in relation to clinical presentations and unique technical procedures. Systematic searches returned 419 results with 15 studies meeting inclusion criteria. This included 13 single subject case reports studies and 2 case series, totaling 27 participants. Results show the use of VR technology to treat PTSD is mainly exposure based. When using such interventions clinicians should conduct a thorough assessment of their clients' background, trauma memory, and triggers in order to tailor the VR experience. They should also plan some early orientation work to help clients acclimatize to the new virtual environment. Gathering self-reported data every 5 min throughout exposure will help with client monitoring, alongside physiological data. The use of olfactory or tactile stimuli may also be helpful during exposure, but is not a necessity. In conclusion, the costs of VR equipment have dropped significantly in the past years making this more accessible and affordable for healthcare providers. Nonetheless, a significant gap remains regarding the use of VR interventions for PTSD in clinical practice. The dearth of qualitative data available within the case report literature, might however help to bridge this gap.
The evidence base surrounding the use and potential use of digital technologies for the treatment of mental health conditions continues rapidly (Hollis et al., 2018). As a result, more and more traditional (face-to-face) therapeutic interventions are being tested in online formats with promising results (Cuijpers et al., 2008). This is particularly apparent when one examines the literature on online Cognitive Behavioral Therapy (CBT) (Dèttore et al., 2015; Rooksby et al., 2015; Jolstedt et al., 2018; Thew et al., 2019). Yet despite moderate to large effect sizes, lower costs, and little in the way of harmful side effects there isn't the uptake of digital technologies by CBT practitioners that one might expect. This is in spite of evidence showing that practitioners are generally receptive to the idea of “computerized” therapies (Stallard et al., 2010; Vigerland et al., 2014). Some have suggested that a lack of consideration regarding implementation issues may be a factor, such as set up costs and the time to up-skill staff (van Gemert-Pijnen et al., 2011; van der Vaart et al., 2014). It is also considered whether there is sufficient technical and treatment protocol information within academic publications, such as Randomized Controlled Trials (RCT) to give therapists the confidence to implement these new approaches within their current practice (Garrett et al., 2018).
This is no more apparent than when one examines the evidence regarding Virtual Reality (VR) technology for the treatment of Post-traumatic Stress Disorder (PTSD). PTSD is described as “a common reaction to traumatic events such as assault, disaster, or severe accidents. The symptoms include repeated and unwanted re-experiencing of the event, hyperarousal, emotional numbing, and avoidance of stimuli (including thoughts) which could serve as reminders for the event” (Ehlers and Clark, 2000, p. 319). Currently, there are a number of RCT studies showing medium effect sizes in relation to the use of VR technology to treat PTSD (Carl et al., 2019). Yet this hasn't led to wide spread adoption and uptake within the health care sector (Lindner et al., 2019). To help clinicians better understand how VR technology can be implemented within clinical practice, the current article synthesizes data from case reports involving the use of VR to treat PTSD. Case Reports are widely recognized as a useful source information for clinical decision making purposes and provide greater opportunity to discuss important clinical matters, such as symptoms, challenging diagnosis, and unique technical procedures (Garg et al., 2016).
Ehlers et al. (2005, p. 414) note that “several versions of cognitive behavioral treatment for post-traumatic stress disorder have been described in the literature” with most showing positive effect (van Etten and Taylor, 1998; Bisson et al., 2013). Currently there are three main Trauma Focused CBT (TF-CBT) models; Resick et al., cognitive processing Therapy (CPT) (2002; 2008; 2014), Foa et al.'s prolonged exposure model (PE) (1999; 2013) and, Ehlers and Clark's (2000) cognitive model of PTSD. All have shown positive outcomes when used to treat PTSD (Foa et al., 1999; Ehlers et al., 2005; Schulz et al., 2006; Duffy et al., 2007) and are recommended in clinical guidelines developed by American Psychological Association (2017).
To date, Foa et al. (1999) PE model has remained one of the most extensively researched treatments for PTSD and has generally shown positive outcomes (Marks et al., 1998; Foa et al., 1999, 2005, 2013). Largely influenced by Emotional Processing Theory (EPT) (Foa and Kozak, 1986) the model suggests that “a fear (emotional) structure is a program for escaping or avoiding danger that includes representations of feared stimuli, responses, and the meaning of stimuli and responses” (Foa, 2011, p. 1044). As such, when one is exposed to their fears in a safe and controlled manner they are able to “emotionally process” the information more accurately. Within PTSD treatment the “traumatic memory is conceived as a specific pathological fear structure.” PE acknowledges that clients have erroneous negative beliefs regarding the traumatic event, and this has led to a lack of cognitive (or emotional) processing of the trauma (Foa, 2011).
Ehlers and Clark (2000) suggest a more cognitively based approach to treatment of PTSD which prioritizes the following three areas—(1) characteristics of the trauma memory; (2) excessively negative appraisals of the trauma incident and; (3) the implementation of strategies to control the “threat.” While both PE and the cognitive model differ, there are some common elements, including exposure to the trauma memory (e.g., imaginal, writing a narrative and in-vivo) as well as some form of cognitive restructuring of the meaning of the trauma (Ehlers et al., 2005).
Resick et al.'s CPT (2002; 2008; 2014) has similarities to the Ehlers and Clark (2000) model but has a different protocol and some treatment components differ also. Similar techniques that are utilized in PE are provided within CPT and TF-CT models but for different purposes for example: imaginal reliving is not used to promote habituation to the painful memory, but to identify key hot spots in the trauma memory that could help to focus further therapy. Behavioral experiments also play an important role and a stronger emphasis is placed on problematic appraisals of trauma sequelae and the modification of maintaining strategies. CPT differs from TF-CT in that the protocol is manualized with each session content more prescribed whereas in TF-CT there is more flexibility in session content and sequencing and techniques applied depend on the case specific formulation derived from the model.
According to Freeman et al. (2017, p. 2393) “immersive virtual reality creates interactive computer generated worlds, which substitute real-world sensory perceptions with digitally generated ones.” Freeman et al. (2017) suggest that if “presence” is achieved within virtual environments then the technology has extraordinary potential for mental health therapy. Rizzo et al. (2004) first described the features inherent within VR technology that may prove useful for therapeutic interventions, such as the ability to provide real time feedback, introduce safe exposure settings, provide low cost environments, control exposure stimulus etc. (Riva et al., 2004). Moreover, Parsons and Rizzo (2008, p. 251) suggested that VR may enhance some current approaches by claiming that VR “produces better outcomes than imaginal exposure and is a pragmatically attractive alternative to in-vivo exposure.” Indeed, a recent systematic review has showed little difference in effect when comparing in-vivo to VR exposure therapy (Wechsler et al., 2019).
In regard to PTSD treatment specifically, a large number of studies have already been conducted in the field with the majority showing positive outcomes (Rothbaum et al., 2001; Rizzo et al., 2007, 2010; Reger and Gahm, 2008; McLay et al., 2011; Difede et al., 2014; Roy et al., 2014; Beidel et al., 2017). Yet as mentioned above, the adoption of VR technology within clinical settings remains low. In the past this has been attributed to the high cost of VR equipment and a somewhat imbalanced “expectation to delivery” ratio (Rizzo et al., 2019, p. 54) whereby headsets offered a limited field of view, the graphics were poor and the interfaces were not as user friendly. However, this is beginning to change with the introduction of both affordable, high end VR headsets as well as several lower cost models.
A final consideration is that the clinical detail required to fully implement and incorporate VR technology within clinical practice is often missing within published research trials (were the chief aim is to establish effectiveness). This has led to an imbalance between outcome data and process data. Garrett et al. (2018) notes the lack of technical standards available to practitioners as well as the high level of technical proficiency required to implement VR interventions. As such, the implementation of VR interventions for PTSD outside of the laboratory setting remains a challenge.
To review and synthesize data from clinical case reports and case series involving VR technology for the treatment of PTSD.
• To identify and assess differences in clinician assessed outcomes for interventions using VR technology to treat PTSD
• To identify implementation procedures and processes involved in the delivery of an intervention using VR technology to treat PTSD
• To explore the areas where VR technology adds value to existing approaches for PTSD treatment.
This study presents evidence from case reports informed by systematic narrative review methodologies (Popay et al., 2006; Best et al., 2014). Results are reported in line with PRISMA guidelines (Appendix A).
Murad et al. (2018, p. 60) state that “a case report is the description of the clinical course of one individual.” A case report is the smallest publishable unit in the literature, whereas case series report aggregates individual cases in one publication (Grimes and Schulz, 2002). According to Nissen and Wynn (2014) case reports are particularly useful for their educational value as well detecting novelties and facilitating in-depth understanding. Unlike other research designs, case reports provide opportunities for additional depth in relation to clinical presentations (e.g., diagnostic criteria, details of the traumatic event, coping strategies/behaviors, family history, risk history etc.) as well as important practical information regarding implementation and unique technical procedures (e.g., session by session overview, explanation of how the technology added value to the protocol, potential adverse events etc.) (Garg et al., 2016).
Systematic searches were conducted in August 2019 and took place across five different bibliographic databases including, (1) Scopus; (2) PsychInfo; (3) Social Science Citation Index; (4) Medline and (5) PILOTS (formerly PTSD Pubs). Within each database, three concept groups were used to create the search structure (a) Virtual Reality; (b) Post-traumatic Stress Disorder and (3) Case Reports. Table 1 shows a generic search string used as part of the systematic search process.
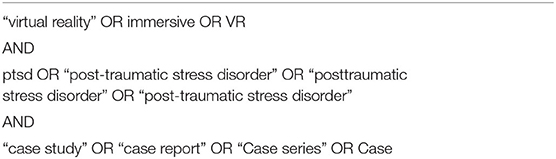
Table 1. Generic search string.
Titles and abstracts (n = 419) were reviewed by the lead author (PB) based on pre-defined inclusion criteria as agreed by the research team (see Figure 1). All included papers must have utilized virtual reality as part of the intervention (either fully or as an adjunct) and the primary condition under treatment must have been defined as a PTSD. Finally, a case report methodology or variant, such as a case series must have been clearly stated. Non English language and gray literature were excluded due to time constraints and no time limits were set.
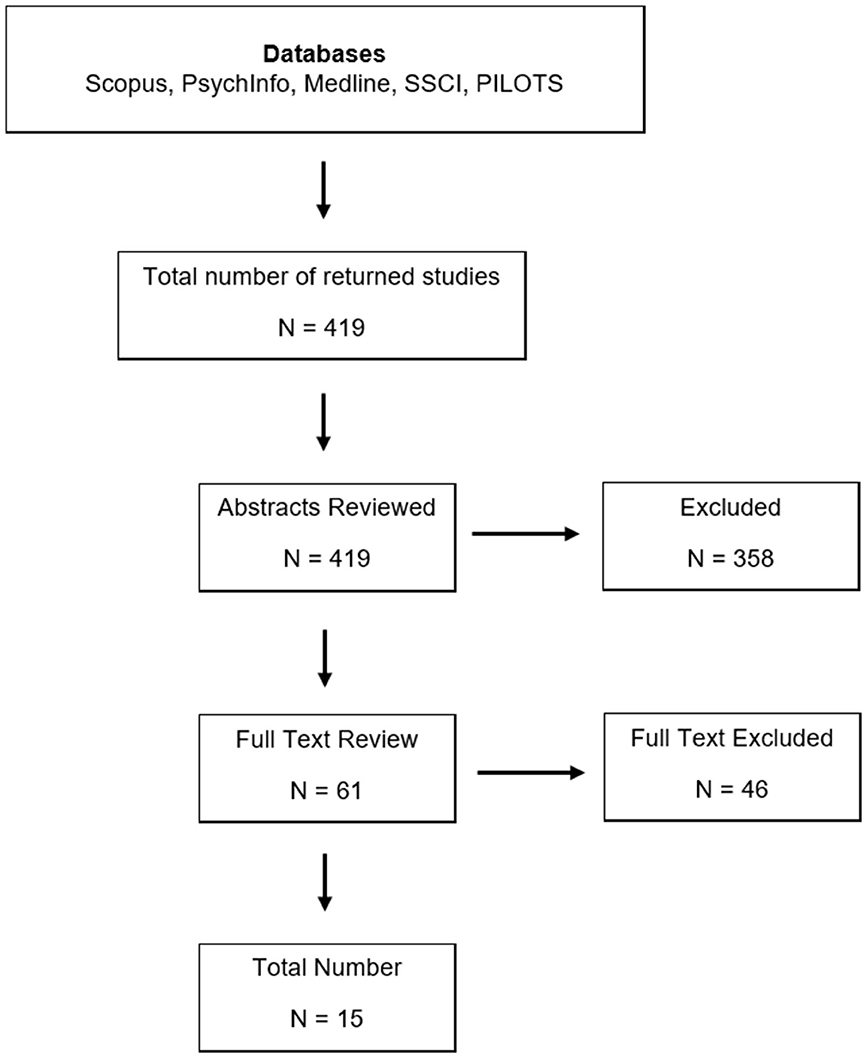
Figure 1. Overview of search strategy.
Each selected article was appraised using a modified version of the Garg et al. (2016) checklist for case reports (see Appendix B). This checklist was developed to assist academic peer reviewers and thus encourages the reader to examine the specific detail(s) contained within case reports rather than simply focus on more traditional appraisal areas, such as risk of bias (an unavoidable and inherent feature of Case Reports). The checklist instead focuses on areas, such as novelty, ethics, case description, importance to the field etc. Each article was given a score on a 1–10 scale to give an indication of study quality (although no cut-off points were used).
The aim of this review is to provide a synthesis of the multiple case report “narratives” surrounding the implementation of VR to treat PTSD. The synthesis framework is informed by the widely recognized CARE guidelines for case reports (Gagnier et al., 2013). These guidelines suggest that the narrative format of case reports should include information on the following—presenting concerns (e.g., client symptoms); diagnoses; intervention; clinical outcome(s); and adverse events (see Table 2). Further to this, the guidance produced by Popay et al. (2006) on approaches to narrative synthesis were also used to inform the early stages of analysis stage. Popay et al. (2006) suggest a non-linear, four step approach to the narrative synthesis that includes exploring the facilitators and barriers as well as understanding how these issues explain differences across studies. This strategy was viewed as the most appropriate given the overall aim of the study and the heterogeneity of data contained within case reports.
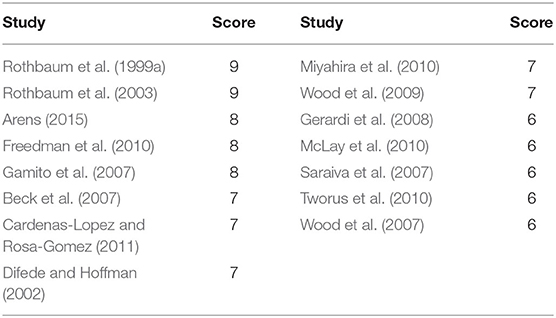
Table 2. Quality assessment scores.
Figure 1 shows the flowchart of bibliographic searching as well as title and abstracts screening. In total, 61 articles were identified for full text review and following the removal of duplicates, theoretical material, and expert commentaries (n = 46) this produced a final list of 15 articles. Of the included studies, 13 were described as a Case Report/Study with a further 2 articles described as Case Series. Data presented here is categorized under the following headings as informed by CARE guidelines—(1) Participant Profile and Diagnosis; (2) Intervention Models; (3) Technical Procedures; and (4) Clinical Outcomes and Adverse Events.
Scores using the modified version of the Garg et al. (2016) checklist, ranged from 6 (Saraiva et al., 2007; Wood et al., 2007; McLay et al., 2010; Tworus et al., 2010) to 9 (Rothbaum et al., 1999a, 2003) (Table 2). The mean score across all articles was 7.1 (SD = 1.1). It is however, worth noting that the checklist does not account for risk bias and therefore caution should be taken when interpreting the results.
There were 27 participants represented within the final 15 studies, 10 (37%) were female and 17 (63%) were male. The majority of female participants (n = 7) came from one case series study involving VR based treatment for PTSD following a road traffic accident (Beck et al., 2007). All 15 studies stated that participants had PTSD although the justification and evidenced provided differed. The most common justification was that participant(s) symptoms matched DSM-IV diagnostic criteria. The Clinician Administered PTSD Scale (CAPS) (Blake et al., 1995) was also used as a justification for PTSD diagnosis as well as being used as a final outcome measure in 10 (67%) studies (discussed below in more detail). Eight (53.%) of the 15 included studies gave additional detail regarding symptomology in order to support the PTSD diagnosis (see data extraction table—Appendix C). Single incident trauma cases were only reported in five (33%) of 15 studies and traumatic events were categorized as follows—(1) war/military; (2) terrorist attack; (3) road traffic accident (RTA); and (4) assault. Most of the military based studies reported participants as having complex PTSD (cPTSD) although it is believed they were simply referring to a “severe” form of PTSD given that cPTSD has only recently emerged as a separated diagnostic category (World Health Organization, 2018) and does not appear in the DSM IV or V (American Psychiatric Association, 2013).
All studies conceptualized and justified using VR technology based on exposure therapy and PE models (Rothbaum and Foa, 1999; Rothbaum et al., 2001). This mainly involved placing the participant within a specific (tailored) VR environment until they habituated. Habituation was determined largely through self-reported Subjective Units of Distress (SUDs) recorded every 5 min (Rothbaum et al., 1999a, 2003; Wood et al., 2007; Gerardi et al., 2008; Cardenas-Lopez and Rosa-Gomez, 2011). There were however, some differences in the application of exposure and PE techniques. For example, Arens (2015) tailored a virtual Iraq environment to the participant's specific sensory experiences (gunfire diesel exhaust smell, body odor etc.) and instructed them to remain there until their SUDs naturally dropped to 50%. Whereas, in Wood et al. (2009), when the participant reached their maximum arousal state (within a virtual Baghdad environment) they were instructed to actively use the relaxation and meditation techniques in order to reduce their anxiety and SUDs rating. It is important note here that some debate exists between whether (helpful) adaptive coping strategies seen in Wood et al. (2009) may develop into (unhelpful) safety seeking behavior over time. Thwaites and Freeston (2005, p. 178) suggest that “with repeated, excessive, or situationally inappropriate use, it is possible that the behavior shifts along a continuum from adaptive coping strategy to safety behavior, depending upon the intention, actual function and objective benefit to the individual.” Another interesting approach was taking by, Freedman et al. (2010) where they asked the participant to recall the traumatic memory while in the virtual environment (BusWorld) but did not recreate the traumatic event itself (terrorist attack). As a result, the fidelity of application differed across studies.
Although the majority of included studies used a PE based rationale, the use of other (more cognitively based) CBT approaches were also evident. While Arens (2015) conducted her study using behaviorist techniques, she firstly presented a detailed case conceptualization from a cognitive perspective which ultimately informed the VR scenario. Miyahira et al. (2010) delivered 10 treatment sessions using a combination of CBT and VR exposure and thus demonstrated how they can be used in tandem. Others, such as Freedman et al. (2010), introduced a CBT session (session five) as part of their overall course of treatment however this appeared in response to specific participant need rather than being standardized within the treatment protocol. Finally, Wood et al. (2007), used VR exposure therapy and group based CBT to treat combat related PTSD. However, the extent to which to two treatments models were combined is unclear. Other techniques described were “trauma management therapy,” psycho-education, meditation, attentional re-focusing, and attention control.
The computer equipment varied throughout. Earlier studies, such as Rothbaum et al. (1999a) used a PC with 233 MHz Intel Pentium Processor, 64 MB of RAM and Evans and Sutherland 3D Graphics Card with more recent studies (Cardenas-Lopez and Rosa-Gomez, 2011) using a DELL XPS with Intel Pentium III, 256 RAM and a AGP graphic board [the most recent study, Arens (2015) did not provide any details regarding computer specification]. Head mounted displays (e.g., VR Headsets) were utilized most often (n = 11, 73%) to experience the VR environment. Built-in microphones were available so that the therapist could communicate with the participant while in the VR environment. Other display equipment used were “translucid” screens (n = 2, 13%), a projector screen with 3D glasses (n = 1, 7%) and a computer screen (n = 1, 7%). In each case, the therapist was able to view what the participant was seeing through an external monitor. Joysticks were often used to control movement within the VR environment and in some cases, clients were seated on specially designed chairs with built in woofers to simulate the vibration from a moving vehicle etc. (Rothbaum et al., 1999a, 2003; Gerardi et al., 2008).
The number of sessions in which VR technology was used varied, this ranged from 3 (Gerardi et al., 2008) to 22 sessions (Tworus et al., 2010). For the most part, therapy took place once per week, but it was noted that not all of this time was spent in the VR environment. For example, in Wood et al. (2007) only 20 min of the 90 min session were spent in VR. At least one initial assessment session was conducted in each study in order to discuss the participants experiences of the trauma and, in some cases, enable some tailoring of the VR scenario. There was some variation in the application and use of VR technology but typically participants were encouraged to remain in the VR environment until they habituated by reporting SUDs throughout. This approach differed if the study was using a non-exposure based rationale. For example, Miyahira et al. (2010) appeared to use the VR technology within an existing CBT treatment framework and therefore habituation wasn't necessary. Nonetheless, there is some evidence to suggest that VR technology may be used as a standalone exposure based approach or as tool within a pre-existing CBT treatment model.
The highest number of studies included war/military environments for combat related PTSD (n = 10). As such, VR environments included “Virtual Iraq,” “Virtual Middle East,” and “Virtual Vietnam” etc. This was followed by two VR scenarios involving terrorist attacks (BusWorld and World Trade Center) and RTA's (VR World Highway and Virtual Driving Scenarios). The final VR environment was Virtual Mexico City, and this was used for a participant with PTSD following a physical assault.
Each of these virtual environments had some level of customization (imagery, auditory etc.) which was controlled by the therapist and used to match with the participants own experiences. For example, in their recreation of the World Trade Center attack, Difede and Hoffman (2002) had 11 different options to choose from in order to increase the level of exposure within the VR environment. This ranged from jets flying overhead with and without sound to images of the second tower collapsing. In Freedman et al. (2010) the authors used a graded approach within their virtual Jerusalem environment. This included four different “levels” which were designed to increase the intensity of exposure. The authors noted that this customizable option was particularly useful during a session when they observed the participant was disengaging (dissociating) and they were able to change the scenario intensity from level 1 to level 2.
For military or war based VR environments, there were a range of customizable options although the settings were exclusively in the Middle East and East Asia (Vietnam). Rothbaum et al. (2003) were to increase the number of gunshots and explosions within the virtual Vietnam environment in order to increase intensity of exposure whereas Gerardi et al. (2008) were able to introduce imagery of wounded civilians and combatants in virtual Iraq. For non-military environments, customization was shown by Saraiva et al. (2007) through a driving-based scenario for those with PTSD following an RTA: the authors were able to increase the volume of traffic on a virtual highway from 10 to 150 vehicles.
A number of studies also customized the audio and olfactory senses in the VR environments. This ranged from simply increasing the volume (Rothbaum et al., 2003) to introducing multiple sounds at once (Gerardi et al., 2008). Arens (2015) used a combination of image, sound and smell in order to tailor the VR environment based on client's experiences. This included introducing smells, such as diesel exhaust fumes and body odor. Gerardi et al. (2008: 210) also used olfactory stimuli “via a scent palette in an airtight chamber filled with compressed air” (burning rubber, weapons fire etc.) to tailor an experience during a virtual Iraq simulation. In addition to this, studies by Saraiva et al. (2007), Gerardi et al. (2008), and Rothbaum et al. (1999a, 2003) used tactile stimuli by placing participants in a chair with a built in woofer so as to simulate the vibration from sitting in helicopter or moving vehicle.
All 15 studies reported positive outcomes in relation to the use of VR technology for the reduction of PTSD symptoms (Appendix C) with Freedman et al. (2010) in particular showing a drop in CAPS score from 79 to 0. This was followed by Gerardi et al. (2008), Wood et al. (2009), McLay et al. (2010), Cardenas-Lopez and Rosa-Gomez (2011), and Arens (2015) who all reported a 50% or more reduction in pre and post treatment scores. There were no noticeable differences in outcomes in relation to gender, age, or other demographic variables.
The primary outcome measure used at baseline and post-treatment in nine (60%) of the 15 studies was the CAPS tool. This was followed by the PTSD Checklist for Military (PCL-M) (n = 2, 13%) (McLay et al., 2010 and Wood et al., 2007), the Impact of Events Scale (IES) (n = 2, 13%) (Gamito et al., 2007; Saraiva et al., 2007), and the Post-traumatic Stress Disorder Scale (PDS) (n = 1, 7%) (Difede and Hoffman, 2002) [Wood et al. (2009) used both CAPS and PCL-M]. Tworus et al. (2010) did not provide any quantitative data regarding outcomes although the authors did report a drop in PTSD intensity. Evaluation time points varied across all studies with only Rothbaum et al. (1999a, 2003), and Freedman et al. (2010) reporting post treatment data at 6 months. Wood et al. (2009) and Miyahira et al. (2010) reported outcome data at 3 months post treatment but the remaining studies tended to report outcomes immediately post-treatment which varied from study to study. Physiological data was also collected in a number of studies, such as heart rate, skin conductance, respiratory rate, temperature etc. (Gamito et al., 2007; Saraiva et al., 2007; Miyahira et al., 2010).
Qualitative comments were also positive with one participant stating that therapy “assisted in improving my skills with being in the moment and having better control over my combat thoughts, feelings, and being startled” (Wood et al., 2009, p. 1220). In Miyahira et al. (2010) the participant reported positive changes in how he now “felt” and “thought” about the traumatic events he experienced and that the headset “helped him to feel as if he was ‘there' in Iraq.” For others, such as Gerardi et al. (2008) it was noted that the VR intervention opened up “forgotten” memories. For Difede and Hoffman (2002), VR therapy was used after several (unsuccessful) attempts to engage the participant in traditional imaginal exposure exercises. Similarly, in Tworus et al. (2010) VR therapy was used after other treatments had failed to show any improvements in the participant's condition.
Adverse events were reported in two studies. Arens (2015) noted that participant noticed a slight increase in hallucinations as well as a brief relapse of alcohol use during the first week of treatment but this stopped at week 2. In Gamito et al. (2007) the participant withdrew after seven sessions due to a distressing flashback the evening after his therapy session which caused him to disengage from treatment.
Case Reports were chosen due their capacity to provide additional detail in relation to unique technical procedures (i.e., the implementation and use of VR technology to treat PTSD). This review included 15 original studies with results presented and categorized using the CARE guidelines for the reporting of clinical case reports.
The evidence presented demonstrates that using VR technology to support the treatment of those with PTSD can lead to positive outcomes. However, it is difficult to generalize these findings or make causal inferences given the inherent weaknesses of case report designs. There was evidence to suggest that VR technology is adaptable to a range of treatment models with no discernible differences in clinical outcomes for studies that reported using TF-CBT models and those that did not. However, it was also clear from the data presented that a large proportion of case report research in the area has relied heavily on behavioral approaches. These techniques have been shown to be inferior to cognitive based approaches for PTSD treatment, particularly for retention and maintaining long term benefits (Imel et al., 2013). Finally, while the CAPS tool is considered a gold standard of PTSD measurement, it does require significant time to complete and was developed using data from military populations. As such, it may not translate as easily into routine clinical practice.
There were no reported challenges regarding the implementation of VR technology within clinical settings however, it did appear that most studies had access to specialist facilities and equipment. While lack of equipment may be viewed as an implementation barrier there have been several recent reductions in the cost of VR equipment that should make this more accessible. Moreover, most of the mid-level workstations used today (i.e., intel i5 processor or AMD Ryzen 5 and above) will be able to display VR content with the addition of a dedicated Graphics Card. Nonetheless, the availability of VR equipment is an important implementation consideration.
In terms of process, most studies described an initial assessment session in which data was gathered to tailor the VR environment based on participant experiences. Introductions to the VR environment were gradual in most cases with participants given freedom to explore the virtual world using a joystick for navigation before the scenario began in earnest. Head mounted displays were the preferred choice (73%) and while specific details regarding make and model were not available for each study, there are a number of high end commercial options available today from Oculus (Rift, Quest, Go), Samsung (Gear), HTC (Vive and Vive Pro), and Valve (Index). There was no clear guidance on the amount of time one should spend within VR environments and this may vary depending on the traumatic event. Rothbaum et al. (1999b) whilst developing a VR experience for fear of flying suggested that a maximum of 30–45 min should be spent in the simulation to avoid potential VR sickness.
Olfactory and tactile stimulation were used successfully in some studies (Gerardi et al., 2008; Arens, 2015) but others have shown equally positive results without these additional sensory options. In fact, a successful outcome was reported by Freedman et al. (2010) who didn't include any imagery relating to the trauma memory (let alone olfactory or tactile sensory information). As Freedman et al. (2010, p. 100) noted “VR was used to provide a context, and imaginal exposure was used by the patients while they were in VR.” This is particularly important given that many of the more customizable VR experiences may not be available for routine practice or may not exist for that trauma type. It is also considered that the approach by Freedman et al. (2010) may be adapted for use within more cognitively based TF-CBT models (e.g., Ehlers and Clark, 2000).
VR technology was implemented successfully within studies using both TF-CBT and non TF-CBT treatment protocols. Prolonged Exposure has featured heavily with most studies using and encouraging a number of behavioral techniques and processes (habituation, attentional refocusing etc.). There was little evidence of the use of cognitive based techniques during treatment (e.g., challenging negative beliefs and meaning(s) associated with the trauma memory) although there were examples of when cognitive restructuring could have occurred and where other techniques could have been used, such as stimulus discrimination (Gerardi et al., 2008; Arens, 2015). Arens (2015) reported a number of cognitive distortions described by her participant (e.g., “the world is a dangerous place”), but failed to return to these in her post treatment analysis. Further to this, an apparent significant moment in the treatment of a young female with PTSD by Difede and Hoffman (2002) appeared to occur during VR exposure when the participant suddenly remembered (for the first time since the event) “believing that she would die.” Again however, no detail was given on how (or if) this belief was challenged. CBT was specifically referenced within four studies; however, its application was not consistent. In one study it was delivered in a group based format in parallel to a VR based intervention (Wood et al., 2007); in another it was a standalone session in response to emerging client need (Freedman et al., 2010). Miyahira et al. (2010) was the only study to report delivering both CBT and VR exposure therapy together.
Reflecting the lack of cognitive techniques used in reported studies to date, one could consider VR technology as particularly relevant for practitioners during imaginal reliving sessions, stimulus discrimination and preparation for site visits (Ehlers and Clark, 2000). For imaginal reliving, VR technology may encourage individuals to “open up” more easily and stay with the trauma memory for longer periods. There are less distractions within the virtual world and there was evidence to suggest in Freedman et al. (2010) that if a person begins to dissociate during the exposure, the scenario could be increased in intensity to re-engage them. Given the success of visual, audio, tactile, and olfactory stimuli, it is considered that VR technology may also enhance stimulus discrimination activities. VR technology could also be used in preparation for site visits or as an alternative if the area is difficult to access. It may even reduce the need for this component entirely. Interestingly, the cognitive model has recently been adapted as a comprehensive therapist-assisted web-based programme using video material and other forms of technology (Wild et al., 2016). As such, the use of VR technology could prove a logical next step for this form of therapy delivery.
More generally, it was also noted that many of the participants were reported to have complex PTSD and had received several other treatments before taking part in the VR intervention. Complex PTSD is defined as “a disorder that may develop following exposure to an event or series of events of an extremely threatening or horrific nature, most commonly prolonged or repetitive events from which escape is difficult or impossible” (ICD-11—World Health Organization, 2018). As such, VR technology may be useful for those with more complex presentations or whom (for whatever reason) are unable or reluctant to engage in traditional imaginal exposure exercises.
The strengths of this study are that it is the first review of clinical case report evidence in the field VR technology for the treatment of PTSD. It is also considered that the information provided here on technical procedures and clinical presentation(s) are not presented elsewhere in this detail. The data gathered here has also been presented in such a way as to be easily translated into clinical practice.
There are however a number of limitations that must be stated. Firstly, clinical case reports are inherently biased, namely in selection and publication bias (Nissen and Wynn, 2014). There is also a tendency to over-generalize case report evidence and no causal inferences can be made from this data. Moreover, the studies retrieved in this review are somewhat dated and as such, do not account for the recent advances in VR technology. There was little consideration within studies of the fact that participant's faces were “hidden” by the headset and important facial cues and non-verbal information could have been lost. Other potential risks, such as photosensitivity, motion sickness, and eye strain were not mentioned. Given that few recent studies could be retrieved, it is also important to note that the included case studies could not have relied on the most recent protocols available, which may limit the generalizability of findings to the current conceptualization of the different models. Finally, while the review has revealed more clinical information regarding treatment implementation, more qualitative data from participants is needed.
In conclusion, case report evidence suggests positive outcomes for the use of VR technology to treat PTSD. While the main therapeutic model that informs this area is PE, some attempts have been made to incorporate VR technologies using other treatment models. Nonetheless, major gaps remain when one considers the lack of available data on how VR technology can be incorporated within existing more cognitively based approaches. Consequently, there is an urgent need for further research into potential benefits of VR technology to support key clinical procedures, such as imaginal reliving, stimulus discrimination, and site visits.
For practitioners interested in using this technology, the costs of VR equipment have dropped significantly in recent years making this more accessible. An increasing number of clinical VR environments are also becoming available, often at limited costs. Complementary, also non-clinical (free of charge) VR environments might prove helpful. Although these might lack options to tailor an experience to the individual patient's needs, the VR environment can still add value by providing a better context for imaginary exposure. Data gathered on technical procedures suggests that practitioners should conduct a thorough assessment of their clients' background, trauma memory, and triggers in order to tailor the experience. They should also plan some early orientation work to help clients acclimatize to the new environment. Gathering self-reported data every 5 min will help with client monitoring, alongside potential physiological data. When a client is in the VR environment the use of olfactory or tactile stimuli may also be helpful but is not a necessity.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
PB undertook initial searches, article screening, and data extraction as well as preparing the first draft of the manuscript. AM also supported initial searches and screening tasks as well as contributing to the final manuscripts through edits within each section. PQ supported the early design and initial development of review questions. He also supported data extraction tasks and contributed to various drafts of the manuscripts. MD supported data synthesis and interpretation and has is internationally recognized for his clinical work on PTSD. TVD helped draft the discussion section and contributed and supported with initial data extraction. All authors contributed to the article and approved the submitted version.
This publication was developed as part of funding obtained from a Medical Research Council Proximity to Discovery Award (P2D). Open access publication funding was provided by Queen's University, Belfast.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2020.563739/full#supplementary-material
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn (DSM-V). Washington, DC: American Psychiatric Publishing.
American Psychological Association (2017). Guideline Development Panel for the Treatment of PTSD in Adults. Washington, DC: American Psychological Association.
Arens, A. M. (2015). Trauma management therapy for a veteran with co-occurring combat PTSD and hallucinations: a case study. Clin. Case Stud. 14, 115–128. doi: 10.1177/1534650114541324
Beck, J. G., Palyo, S. A., Winer, E. H., Schwagler, B. E., and Ang, E. J. (2007). Virtual reality exposure therapy for PTSD symptoms after a road accident: an uncontrolled case series. Behav. Ther. 38, 39–48. doi: 10.1016/j.beth.2006.04.001
Beidel, D. C., Frueh, B. C., Neer, S. M., and Lejuez, C. W. (2017). The efficacy of trauma management therapy: a controlled pilot investigation of a three-week intensive outpatient program for combat-related PTSD. J. Anxiety Disord. 50, 23–32. doi: 10.1016/j.janxdis.2017.05.001
Best, P., Taylor, B., Manktelow, R., and McQuilkin, J. (2014). Systematically retrieving research in the digital age: case study on the topic of social networking sites and young people's mental health. J. Inform. Sci. 40, 346–356. doi: 10.1177/0165551514521936
Bisson, J. I., Roberts, N. P., Andrew, M., Cooper, R., and Lewis, C. (2013). Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst. Rev. 12:CD003388. doi: 10.1002/14651858.CD003388.pub4
Blake, D. D., Weathers, F. W., Nagy, L. M., Kaloupek, D. G., Gusman, F. D., Charney, D. S., et al. (1995). The development of a clinician-administered PTSD scale. J. Traumatic Stress 8, 75–90. doi: 10.1002/jts.2490080106
Cardenas-Lopez, G., and Rosa-Gomez, A. D. L. (2011). Post-traumatic stress disorder treatment with virtual reality exposure for criminal violence: a case study in assault with violence post-traumatic stress disorder treatment with virtual reality exposure for criminal violence: a case study in assault with violence. Int. J. Disabil. Hum. Dev. 10, 379–383. doi: 10.1515/IJDHD.2011.061
Carl, E., Stein, A. T., Levihn-Coon, A., Pogue, J. R., Rothbaum, B., Emmelkamp, P. M. G., et al. (2019). Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J. Anxiety Disord. 61, 27–36. doi: 10.1016/j.janxdis.2018.08.003
Cuijpers, P., van Straten, A., and Andersson, G. (2008). Internet-administered cognitive behavior therapy for health problems: a systematic review. J. Behav. Med. 31, 169–177. doi: 10.1007/s10865-007-9144-1
Dèttore, D., Pozzam, A., and Andersson, G. (2015). Efficacy of technology-delivered cognitive behavioural therapy for OCD versus control conditions, and in comparison with therapist-administered CBT: meta-analysis of randomized controlled trials. Cogn. Behav. Ther. 44, 190–211. doi: 10.1080/16506073.2015.1005660
Difede, J., Cukor, J., Wyka, K., Olden, M., Hoffman, H., Lee, F. S., et al. (2014). D-cycloserine augmentation of exposure therapy for post-traumatic stress disorder: a pilot randomized clinical trial. Neuropsychopharmacology 39, 1052–1058. doi: 10.1038/npp.2013.317
Difede, J., and Hoffman, H. G. (2002). Virtual reality exposure therapy for world trade center post-traumatic stress disorder: a case report. Cyberpsychol. Behav. 5, 529–535. doi: 10.1089/109493102321018169
Duffy, M., Gillespie, K., and Clark, D. M. (2007). Posttraumatic stress disorder in the context of terrorism and other civil conflict in Northern Ireland: randomized controlled trial. Br. Med. J. 334, 147–150. doi: 10.1136/bmj.39021.846852.BE
Ehlers, A., and Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behav. Res. Ther. 38, 319–345. doi: 10.1016/S0005-7967(99)00123-0
Ehlers, A., Clark, D. M., Hackmann, A., McManus, F., and Fennell, M. (2005). Cognitive therapy for post-traumatic stress disorder: development and evaluation. Behav. Res. Ther. 43, 413–431. doi: 10.1016/j.brat.2004.03.006
Foa, E. B. (2011). Prolonged exposure therapy: past, present, and future. Depress. Anxiety 28, 1043–1047. doi: 10.1002/da.20907
Foa, E. B., Dancu, C. V., Hembree, E. A., Jaycox, L. H., Meadows, E. A., and Street, G. P. (1999). A comparison of exposure therapy, stress inoculation training, and their combination for reducing posttraumatic stress disorder in female assault victims. J. Consult. Clin. Psychol. 67, 194–200. doi: 10.1037/0022-006X.67.2.194
Foa, E. B., Gillihan, S. J., and Bryant, R. A. (2013). Challenges and successes in dissemination of evidence-based treatments for posttraumatic stress: Lessons learned from prolonged exposure therapy for PTSD. Psychol. Sci. Pub. Inter. 14, 65–111. doi: 10.1177/1529100612468841
Foa, E. B., Hembree, E. A., Cahill, S. P., Rauch, S. A. M., Riggs, D. S., Feeny, N. C., et al. (2005). Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics. J. Consult. Clin. Psychol. 73, 953–964. doi: 10.1037/0022-006X.73.5.953
Foa, E. B., and Kozak, M. J. (1986). Emotional processing of fear: exposure to corrective information. Psychol. Bull. 99, 20–35. doi: 10.1037/0033-2909.99.1.20
Freedman, S., Hoffman, H., Garcia-Palacios, A., Tamar Weiss, P., Avitzour, S., and Josman, N. (2010). Prolonged exposure and virtual reality-enhanced imaginal exposure for PTSD following a terrorist bulldozer attack: a case study. Cyberpsychol. Behav. Soc. Netw. 13, 95–101. doi: 10.1089/cyber.2009.0271
Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., et al. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47, 1–8. doi: 10.1017/S003329171700040X
Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H., and Riley, D. (2013). CARE group. The CARE guidelines: consensus-based clinical case reporting guideline development. Br. Med. J. Case Rep. 2, 38–43. doi: 10.7453/gahmj.2013.008
Gamito, P., Oliveira, J., Morais, D., Saraiva, T., Rosa, J., and Gamito, L. (2007). War PTSD: A VR pre-trial case study. Annu. Rev. CyberTher. Telemed. 5, 199–205.
Garg, R., Lakhan, S. E., and Dhanasekaran, A. K. (2016). How to review a case report. J. Med. Case Rep. 10:88. doi: 10.1186/s13256-016-0853-3
Garrett, B., Taverner, T., Gromala, D., Tao, G., Cordingley, E., and Sun, C. (2018). Virtual reality clinical research: promises and challenges. JMIR Ser. Games 6:e10839. doi: 10.2196/10839
Gerardi, M., Rothbaum, B. O., Ressler, K., Heekin, M., and Rizzo, A. A. (2008). Virtual reality exposure therapy using a virtual Iraq: case report. J. Traumatic Stress 21, 209–213. doi: 10.1002/jts.20331
Grimes, D. A., and Schulz, K. F. (2002). Descriptive studies: what they can and cannot do. Lancet 359, 145–149. doi: 10.1016/S0140-6736(02)07373-7
Hollis, C., Sampson, S., Simons, L., Davies, E. B., Churchill, R., Betton, V., et al. (2018). Identifying research priorities for digital technology in mental health care: results of the james lind alliance priority setting partnership. Lancet Psychiatry 5, 845–854. doi: 10.1016/S2215-0366(18)30296-7
Imel, Z. E., Laska, K., Jakupcak, M., and Simpson, T. L. (2013). Meta-analysis of dropout in treatments for posttraumatic stress disorder. J. Consult. Clin. Psychol. 81, 394–404. doi: 10.1037/a0031474
Jolstedt, M., Ljótsson, B., Fredlander, S., Tedgård, T., Hallberg, A., Ekeljung, A., et al. (2018). Implementation of internet-delivered CBT for children with anxiety disorders in a rural area: a feasibility trial. Internet Interv. 12, 121–129. doi: 10.1016/j.invent.2017.11.003
Lindner, P., Miloff, A., Zetterlund, E., Reuterskiöld, L., Andersson, G., and Carlbring, P. (2019). Attitudes toward and familiarity with virtual reality therapy among practicing cognitive behavior therapists: a cross-sectional survey study in the era of consumer VR platforms. Front. Psychol. 10:176. doi: 10.3389/fpsyg.2019.00176
Marks, I., Lovell, K., Noshirvani, H., Livanou, M., and Thrasher, S. (1998). Treatment of posttraumatic stress disorder by exposure and/or cognitive restructuring: a controlled study. Arch. Gen. Psychiatry 55, 317–325. doi: 10.1001/archpsyc.55.4.317
McLay, R. N., McBrien, C., Wiederhold, M. D., and Wiederhold, B. K. (2010). Exposure therapy with and without virtual reality to treat PTSD while in the combat theater: a parallel case series. Cyberpsychol. Behav. Soc. Netw. 13, 37–42. doi: 10.1089/cyber.2009.0346
McLay, R. N., Wood, D. P., Webb-Murphy, J. A., Spira, J. L., Wiederhold, M. D., Pyne, J. M., et al. (2011). A randomized, controlled trial of virtual reality exposure therapy for post-traumatic stress disorder in active duty service members with combat- related post-traumatic stress disorder. Cyberpsychol. Behav. Soc. Netw. 14, 223–229. doi: 10.1089/cyber.2011.0003
Miyahira, S. D., Folen, R. A., Hoffman, H. G., Garcia-Palacios, A., and Schaper, K. M. (2010). Effectiveness of brief VR treatment for PTSD in war-fighters: a case study. Stud. Health Technol. Inform. 154, 214–221. doi: 10.3233/978-1-60750-561-7-214
Murad, M. H., Sultan, S., Haffar, S., and Bazerbachi, F. (2018). Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 23, 60–63. doi: 10.1136/bmjebm-2017-110853
Nissen, T., and Wynn, R. (2014). The clinical case report: a review of its merits and limitations. BMC Res. Notes 7:264. doi: 10.1186/1756-0500-7-264
Parsons, T. D., and Rizzo, A. A. (2008). Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: a meta-analysis. J. Behav. Ther. Exp. Psychiatry 39, 250–261. doi: 10.1016/j.jbtep.2007.07.007
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rogers, M., et al. (2006). Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. ESRC Methods Programme: University of Lancaster, UK.
Reger, G., and Gahm, G. (2008). Virtual reality exposure therapy for active duty soldiers. J. Clin. Psychol. 64, 940–946. doi: 10.1002/jclp.20512
Resick, P. A., Galovski, T. E., Uhlmansiek, M. O., Scher, C. D., Clum, G. A., and Young-Xu, Y. (2008). A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. J. Consult. Clin. Psychol. 76, 243–258. doi: 10.1037/0022-006X.76.2.243
Resick, P. A., Monson, C. M., and Chard, K. M. (2014). Cognitive Processing Therapy: Veteran/Military Version: Therapist's Manual. Washington, DC: Department of Veterans Affairs.
Resick, P. A., Nishith, P., Weaver, T. L., Astin, M. C., and Feuer, C. A. (2002). A comparison of cognitive processing therapy with prolonged exposure and a waiting condition for the treatment of chronic posttraumatic stress disorder in female rape victims. J. Consult. Clin. Psychol. 70, 867–879. doi: 10.1037/0022-006X.70.4.867
Riva, G., Mantovani, F., and Gaggioli, A. (2004). Presence and rehabilitation: toward second-generation virtual reality applications in neuropsychology. J. Neuroeng. Rehabil. 1:9. doi: 10.1186/1743-0003-1-9
Rizzo, A., Koenig, S. T., and Talbot, T. B. (2019). Clinical results using virtual reality. J. Technol. Hum. Serv. 37, 51–74, doi: 10.1080/15228835.2019.1604292
Rizzo, A. A., Graap, K., Mclay, R. N., Perlman, K., Rothbaum, B., Reger, G., et al. (2007). “Virtual Iraq: initial case reports from a VR exposure therapy application for combat-related post traumatic stress disorder,” in IEEE XPlore Virtual Rehabilitation International Conference (Venice: IEEE), 124–130.
Rizzo, A. A., Schultheis, M. T., Kerns, K., and Mateer, C. (2004). Analysis of assets for virtual reality applications in neuropsychology. Neuropsychol. Rehabil. 14, 207–239. doi: 10.1080/09602010343000183
Rizzo, A. S., Difede, J., Rothbaum, B. O., Reger, G., Spitalnick, J., Cukor, J., et al. (2010). Virtual iraq/afghanistan: development and early evaluation of a virtual reality exposure therapy system for combat-related PTSD. Ann. N. Y. Acad. Sci. 1208, 114–125. doi: 10.1111/j.1749-6632.2010.05755.x
Rooksby, M., Elouafkaoui, P., Humphris, G., Clarkson, J., and Freeman, R. (2015). Internet-assisted delivery of cognitive behavioural therapy (CBT) for childhood anxiety: systematic review and meta-analysis. J. Anxiety Disord. 29, 83–92. doi: 10.1016/j.janxdis.2014.11.006
Rothbaum, B. O., Hodges, L., Alarcon, R., Ready, D., Shahar, F., Graap, K., et al. (1999a). Virtual reality exposure therapy for PTSD vietnam veterans: a case study. J. Traumatic Stress 12, 263–271. doi: 10.1023/A:1024772308758
Rothbaum, B. O., Hodges, L., Ready, D., Graap, K., and Alarcon, R. (2001). Virtual reality exposure therapy for vietnam veterans with posttraumatic stress disorder. J. Clin Psychiatry 62, 617–622. doi: 10.4088/JCP.v62n0808
Rothbaum, B. O., Hodges, L. F., and Smith, S. (1999b). Virtual reality exposure therapy abbreviated treatment manual: fear of flying application. Cogn. Behav. Pract. 6, 234–244. doi: 10.1016/S1077-7229(99)80081-9
Rothbaum, B. O., Ruef, A. M., Litz, B. T., Han, H., and Hodges, L. (2003). Virtual reality exposure therapy of combat-related PTSD: a case study using psychophysiological indicators of outcome. J. Cogn. Psychother. 17, 163–177. doi: 10.1891/jcop.17.2.163.57438
Roy, M. J., Costanzo, M. E., Blair, J. R., and Rizzo, A. A. (2014). Compelling evidence that exposure therapy for PTSD normalizes brain function. Stud. Health Technol. Inform. 199, 61–65. doi: 10.3233/978-1-61499-401-5-61
Saraiva, T., Gamito, P., Oliveira, J., Morais, D., Pombal, M., Gamito, L., et al. (2007). The use of VR exposure in the treatment of motor vehicle PTSD: a case report. Annu. Rev. CyberTher. Telemed. 5, 199–205.
Schulz, P. M., Resick, P. A., Huber, L. C., and Griffin, M. G. (2006). The effectiveness of cognitive processing therapy for PTSD with refugees in a community setting. Cogn. Behav. Pract. 13, 322–331. doi: 10.1016/j.cbpra.2006.04.011
Stallard, P., Richardson, T., and Velleman, S. (2010). Clinicians' attitudes towards the use of computerized cognitive behaviour therapy (cCBT) with children and adolescents. Behav. Cogn. Psychother. 38, 545–560. doi: 10.1017/S1352465810000421
Thew, G. R., Powell, C. L., Kwok, A. P., Lissillour-Chan, M. H., Wild, J., Warnock-Parkes, E., et al. (2019). Internet-based cognitive therapy for social anxiety disorder in hong kong: therapist training and dissemination case series. J. Med. Internet Res. 3:e13446. doi: 10.2196/13446
Thwaites, R., and Freeston, M. H. (2005). Safety-seeking behaviours : fact or function? How can we clinically differentiate between safety behaviours and adaptive coping strategies across anxiety disorders. Behav. Cogn. Psychother. 33, 177–188. doi: 10.1017/S1352465804001985
Tworus, R., Szymanska, S., and Ilnicki, S. (2010). A soldier suffering from PTSD, treated by controlled stress exposition using virtual reality and behavioral training. Cyberpsychol. Behav. Soc. Netw. 13, 103–107. doi: 10.1089/cyber.2009.0329
van der Vaart, R., Witting, M., Riper, H., Kooistra, L., Bohlmeijer, E. T., and van Gemert-Pijnen, L. J. (2014). Blending online therapy into regular face-to-face therapy for depression: content, ratio and preconditions according to patients and therapists using a Delphi study. BMC Psychiatry 14:355. doi: 10.1186/s12888-014-0355-z
van Etten, M. L., and Taylor, S. (1998). Comparative efficacy of treatments for post-traumatic stress disorder: a metaanalysis. Clin. Psychol. Psychother. 5, 126–144. doi: 10.1002/(SICI)1099-0879(199809)5:3<126::AID-CPP153>3.0.CO;2-H
van Gemert-Pijnen, J. E. W. C., Nijland, N., van Limburg, M., Ossebaard, H. C., Kelders, S. M., Eysenbach, G., et al. (2011). A holistic framework to improve the uptake and impact of eHealth technologies. J. Med. Internet Res. 13:e111. doi: 10.2196/jmir.1672
Vigerland, S., Ljótsson, B., Gustafsson, F., Hagert, S., Thulin, U., and Andersson, G. (2014). Attitudes towards the use of computerized cognitive behavior therapy (cCBT) with children and adolescents: a survey among Swedish mental health professionals. Internet Interv. 1, 111–117. doi: 10.1016/j.invent.2014.06.002
Wechsler, T. F., Kümpers, F., and Mühlberger, A. (2019). Inferiority or even superiority of virtual reality exposure therapy in phobias?—A systematic review and quantitative meta-analysis on randomized controlled trials specifically comparing the efficacy of virtual reality exposure to gold standard in vivo exposure in agoraphobia, specific phobia, and social phobia. Front. Psychol. 10:1758. doi: 10.3389/fpsyg.2019.01758
Wild, J., Warnock-Parkes, E., Grey, N., Stott, R., Wiedemann, M., Canvin, L., et al. (2016). Internet-delivered cognitive therapy for PTSD: a development pilot series. Eur. J. Psychotraumatol. 7:31019. doi: 10.3402/ejpt.v7.31019
Wood, D. P., Murphy, J., Lay, R. M. C., and Reeves, D. (2007). Combat-related post-traumatic stress disorder: a case report using virtual reality exposure therapy with physiological monitoring. Cyberpsychol. Behav. 10, 309–315. doi: 10.1089/cpb.2006.9951
Wood, D. P., Webb-Murphy, J., Center, K., McLay, R., Koffman, R., Johnston, S., et al. (2009). Combat-related post-traumatic stress disorder: a case report using virtual reality graded exposure therapy with physiological monitoring with a female Seabee. Milit. Med. 174, 1215–1222. doi: 10.7205/MILMED-D-03-4408
World Health Organization (2018). International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision) (ICD-11). Available online at: https://icd.who.int/browse11/l-m/en
Keywords: virtual reality, post-traumatic stress disorder (PSTD), case reports, clinical settings, implementation
Citation: Best P, McKenna A, Quinn P, Duffy M and Van Daele T (2020) Can Virtual Reality Ever Be Implemented in Routine Clinical Settings? A Systematic Narrative Review of Clinical Procedures Contained Within Case Reports for the Treatment of PTSD. Front. Virtual Real. 1:563739. doi: 10.3389/frvir.2020.563739
Received: 19 May 2020; Accepted: 25 September 2020;
Published: 19 November 2020.
Edited by:
Georgina Cardenas-Lopez, National Autonomous University of Mexico, MexicoReviewed by:
Pedro Gamito, Universidade Lusófona, PortugalCopyright © 2020 Best, McKenna, Quinn, Duffy and Van Daele. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paul Best, cC5iZXN0QHF1Yi5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.