 Moufid Mhamadi1,2*
Moufid Mhamadi1,2* Ousseynou Sene1
Ousseynou Sene1 Arfang Diamanka3Moundhir Mhamadi4Marie Pedapa Mendy1Andy Mahine Diouf1Mignane Ndiaye1Mamadou Aliou Barry5Samba Niang Sagne5Mahfouz Cissé Traoré1
Arfang Diamanka3Moundhir Mhamadi4Marie Pedapa Mendy1Andy Mahine Diouf1Mignane Ndiaye1Mamadou Aliou Barry5Samba Niang Sagne5Mahfouz Cissé Traoré1 Amadou Alpha Sall1Gamou Fall1Ndongo Dia1
Amadou Alpha Sall1Gamou Fall1Ndongo Dia1 Oumar Faye1
Oumar Faye1- 1Virology Department, Institut Pasteur de Dakar, Dakar, Senegal
- 2Vaccine Research Center, Institut Pasteur de Dakar, Dakar, Senegal
- 3Department of Animal Biology, Université Cheikh Anta Diop de Dakar, Dakar, Senegal
- 4Diatropix, Institut Pasteur de Dakar, Dakar, Senegal
- 5Epidemiology, Clinical Research and Data Science Department, Institut Pasteur de Dakar, Dakar, Senegal
A fatal case of Crimean-Congo hemorrhagic fever virus (CCHFV) was detected in Dakar, Senegal, West Africa, in April 2023. To elucidate the mechanisms involved in this outcome, the kinetics of viral load, immunoglobulins, and cytokines were assessed using RT-qPCR and ELISA. A high IL-6 titer, low IL-10 titer, and delayed IgG response were associated with disease severity. These biomarkers may serve as predictors of disease severity, potentially aiding in early intervention and treatment strategies.
1 Introduction
Crimean Congo hemorrhagic fever virus (CCHFV) is a WHO blueprint pathogen that can cause human disease. Human CCHFV cases have been reported in Africa, Asia, and Europe (1). Clinical reports and epidemic data showed that less than 5% of cases were severe with a mortality rate of 40% among these hospitalized patients (1). However, few studies have analyzed the role of host immunity and viral load in severe outcomes and fatality (2–7) but no data are available in Senegal about the biological mechanisms involved in fatal outcomes. In Senegal, the circulation of CCHFV has been reported since 1967 (8). Recent studies suggest that the CCHFV could be present in the whole Senegalese territory (Dakar = 2.7%, Diourbel = 4.6%, Fatick = 14.4%, Kaffrine = 14.5%, Kaolack = 4%, Louga = 12,1%, Matam = 5.2%, Sedhiou = 10.1%, Thies = 6.1%, Saint-Louis = 38.4%, Kolda = 28.3%, Tambacounda = 22.2%, Kedougou = 20.9%, and Ziguinchor = 14.8%) (9) and sporadic cases have been reported every year since the implementation of the Sentinel Syndromic Surveillance Network in Senegal (4S) in 2011 (10). Human febrile samples (swab, urine, feces, blood, and cerebrospinal fluid) collected at the 4S healthcare centers are sent weekly to the Institut Pasteur de Dakar (IPD) for molecular and serological diagnosis of arbovirus, viral hemorrhagic fevers (VHFs), respiratory viruses [influenza A/B/C, rubella, measles, rhinovirus, para influenza 1-4, bocavirus, coronavirus (SARS-CoV 1/2, MERS-CoV, HCoV 229E, OC43, NL63, HKU1), respiratory syncytial virus, paraechovirus, adenovirus, and metapneumovirus], enterovirus, poliovirus, and rabies virus.
This sentinel surveillance allows the Senegalese stakeholders to take appropriate measures in case management to prevent or contain epidemic outbreaks.
In this study, we detected and tested a fatal case of CCHFV through the 4S network. Our objective was to analyze the role of certain immune markers [immunoglobulin M (IgM), immunoglobulin G (IgG), interleukin 6 (IL-6), interleukin 10 (IL-10), tumor necrosis factor-alpha 1 (TNF-α1), and interferon-gamma 1 (IFN-γ1)] (2–7) that have been associated with fatal outcomes in studies conducted in other countries to better understand the mechanisms involved in the fatal progression observed in our patient.
2 Case study
On 18 April 2023, a 35-year-old male butcher from Parcelles Assainies (Dakar, western Senegal) presented at the Dalal Jam National Hospital Center (Dakar) with febrile syndrome. Symptoms started on 10 April 2023 and included a flu-like syndrome (headaches, muscle pain, and joint pain) and meningoencephalitis signs (confusion, hallucination, disorientation, seizures, neck stiffness, and coma). These signs were confirmed by a clinical examination conducted by a doctor. As the patient was negative for malaria, he was hospitalized for treatment (rehydration through an intravenous saline solution and symptomatic treatment for the various signs and symptoms of the patient), and blood samples were taken for further analysis in the hospital such as blood glucose test, sedimentation rate, coagulation factors, and complete blood count. The administration of care and treatment were provided throughout the entire duration of his hospitalization. All the interventions were well tolerated by the patient. This tolerance and adherence were evaluated visually by healthcare staff by monitoring the appearance of any side effects or allergies and no adverse events were detected. On 20 April, hemorrhage signs were detected and another blood sample was taken and sent to IPD for laboratory diagnosis. At IPD, the sample was tested by IgM ELISA and RT-qPCR to test for a diagnosis of several arboviruses and VHF. The sample tested positive for CCHFV on both the RT-qPCR and the IgM ELISA. Unfortunately, the patient died on 22 April 2023 due to his illness. A retrospective study was undertaken with the blood samples collected from this patient between 18 and 22 April 2023 to understand the biological mechanisms involved in this fatal outcome.
For this case report, the kinetics of viral load and several immunological markers, including IgM, IgG, IL-6, IL-10, TNF-α1, and IFN-γ1, were determined by RT-qPCR (11) and ELISA (in-house test for immunoglobulins and Invitrogen kits for cytokines) respectively, as many studies show that variations in the concentrations of these markers are involved in the outcome of patients affected by CCHFV (2–7). Each experiment was repeated three times.
A low average number of platelets of 7000/µL was measured during the patient’s hospitalization (reference range 150,000–450,000/μL) as has already been reported (5). This low number of platelets could explain the hemorrhagic syndrome developed by the patient. It is commonly known that platelets are essential for hemostasis and a lack of proper platelet function leads to excessive bleeding.
The RT-PCR testing revealed that the viral load decreased from the day of hospital admission (5 x 105/mL) to the day of death (3 x 103/mL) (Figure 1). Our results differ from previous findings where fatal cases of CCHFV had viral loads of 108–107 (5, 12). For this reason, we explored the immune response pathway to understand the cause of this fatal progression better. This decrease could be associated with an increase in humoral IgM and IgG immunity as previously shown (13). Our analysis showed that IgM was detected on 19 April and the highest signal was observed on 22 April (Figure 2). However, an IgG signal was only detected on the day of death (Figure 2) as has been already reported in another study (7), which did not detect anti-CCHFV IgG in fatal cases 11 days after the symptom onset. Previous studies showed that IgG concentration is inversely correlated with viral loads (2, 5). This means that a late IgG secretion could be correlated to this fatality.
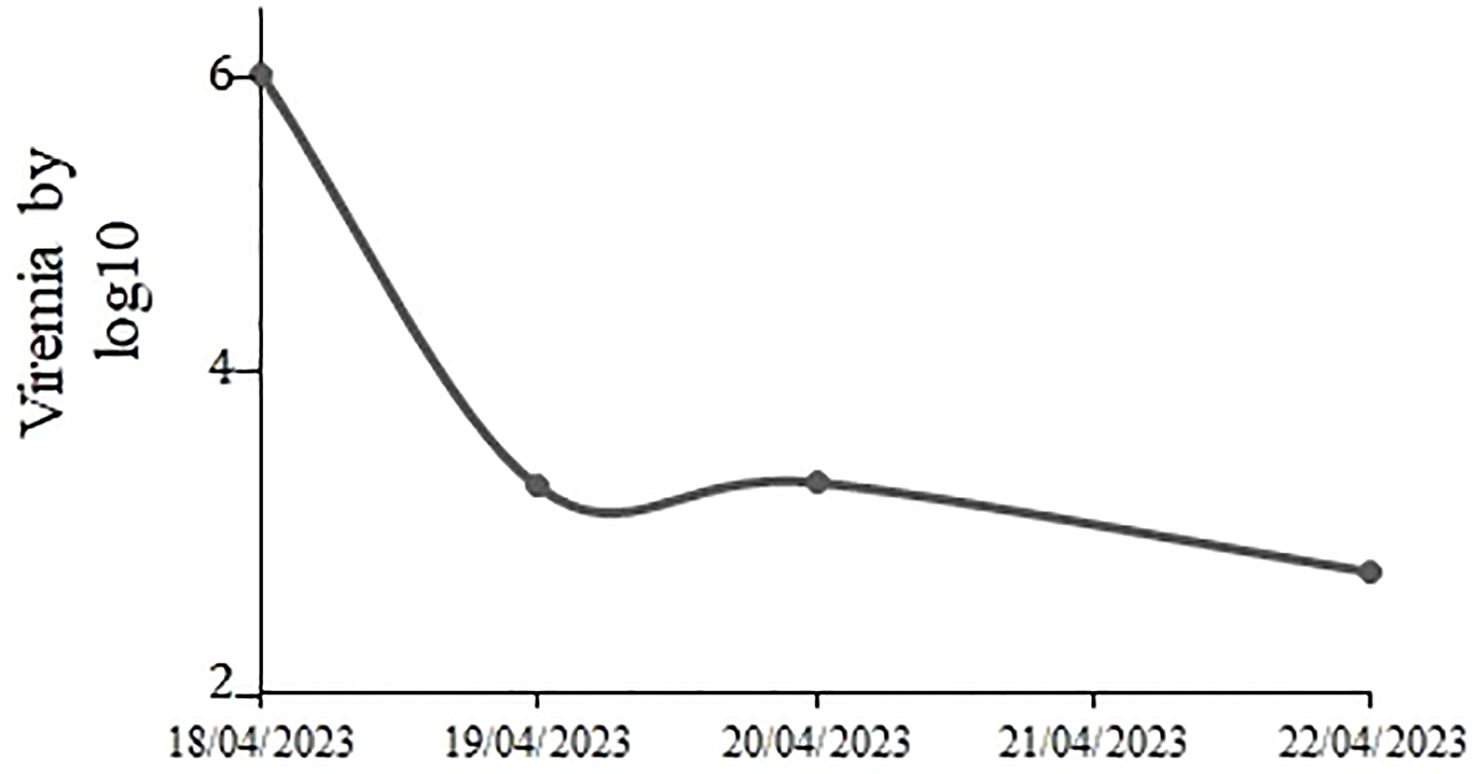
Figure 1. Viral load during the hospitalization. Viral load per mL was determined by RT-qPCR and decreased between 5 log 10 to 3 log 10.
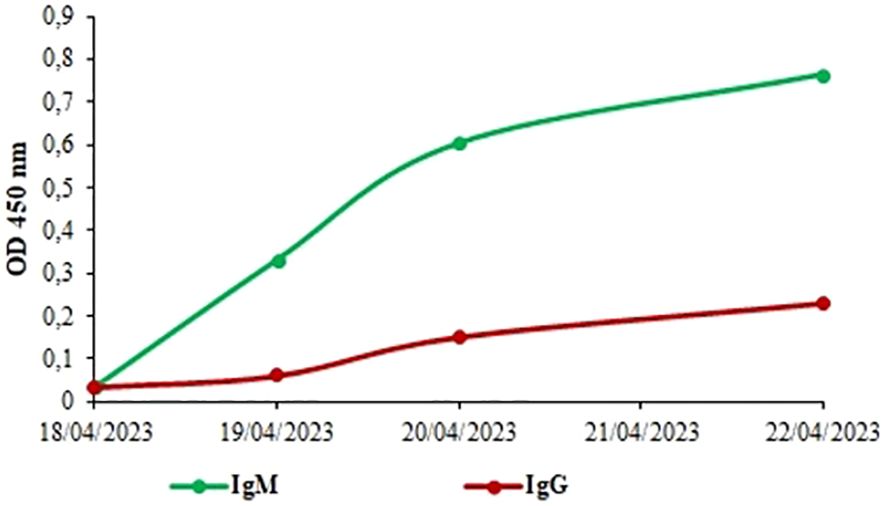
Figure 2. The kenetics of immunoglobulins M and G in the fatal case where evaluated by ELISA. A high IgM titer (green curve) and lower IgG (red curve) were detected during this hospitalization.
Interestingly, the titers of IL-6 increased continuously from the day of admission (Figure 3) and the highest titer was reached on the day of death (404.16 pg/mL). This high titer of IL-6 could be correlated to the severity of the disease (3–5, 7). Many studies have shown a significant role of IL-6 in cytokine storms, a severe immune reaction in some patients, leading to widespread inflammation, organ damage, and potentially death (5).
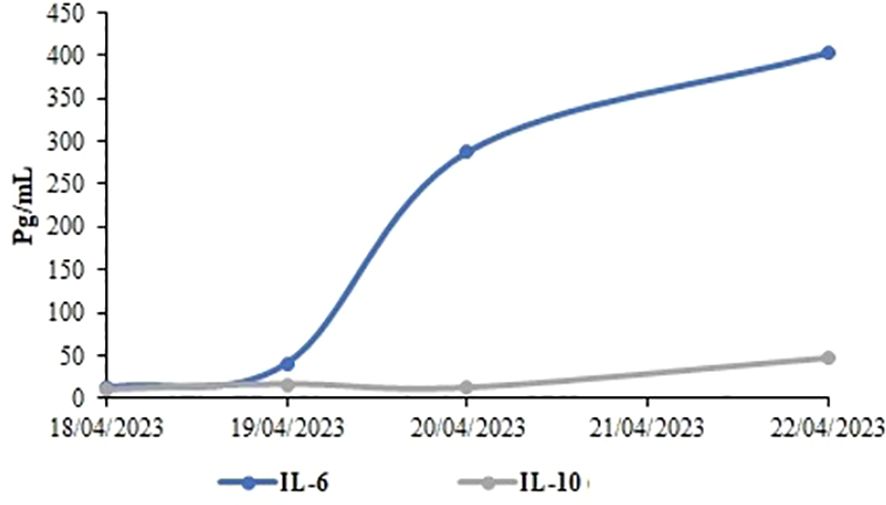
Figure 3. Sequential of interleukins 6 and 10 during hospitalization. The average IL-10 titer was lower (21.56 pg/ml, grey curve) than the average IL-6 titer (186.53 pg/mL, blue curve).
Additionally, a subsequent increase in IL-10 was detected during the hospitalization (Figure 3) but lower titers were found (10.16 - 46.96 pg/mL). The lower rate of IL-10 in fatal cases has already been documented (6, 7). This could be because IL-10 is a potent inflammatory mediator of vascular injury (14) and a low IL-10 concentration leads to coagulation disturbance which can explain the severity of the disease.
Furthermore, TNF-α1 was not detected during the hospitalization as has been already reported (7). TNF-α1 production contributes to macrophage activation with resulting hemophagocytosis, stimulates vasodilatation by acting on the endothelium, and has an antifibrinolytic action (6). Given this, a progression towards a fatal outcome might have occurred in the absence of TNF-α1.
IFN-γ1 was not detected during the hospitalization as has already been described (5). IFN-γ is secreted by activated T cells and natural killer (NK) cells. This cytokine is responsible for the inflammatory response and viral immunity via macrophage activation (14). An absence of this immune mediator could be related to the fatal outcome.
3 Conclusion
Our analysis provides some explanations for the fatal outcome in this human CCHFV case. Based on our findings, we suggest that the fatality could be associated with a high IL-6 titer, a low IL-10 titer, an absence of TNF-α1 and IFN-γ1, and a late anti-CCHFV IgG response.
As this study is the first in Senegal to demonstrate the feasibility and utility of measuring immune markers to predict the outcome of CCHFV, it has certain limitations. Notably, control samples are absent for severe cases and for survivors. Furthermore, we plan to measure additional immune markers such as IL-1β, IL-2, IL-7, IL-8, IL-12, IL-13, IL-17A, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), monocyte chemoattractant protein-1 (MCP-1), and macrophage inflammatory protein-1β (MIP-1β).
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Comité National d’Ethique pour la Recherche en Santé (CNERS) (N°000243/MSAS/DPRS/CNERS). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
MoufM: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. OS: Formal analysis, Investigation, Methodology, Writing – review & editing. AD: Data curation, Formal analysis, Supervision, Writing – review & editing. MounM: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. MPM: Formal analysis, Investigation, Methodology, Writing – review & editing. AMD: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. MN: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. MB: Formal analysis, Investigation, Supervision, Writing – review & editing. SN: Formal analysis, Investigation, Software, Writing – review & editing. MT: Formal analysis, Resources, Software, Writing – review & editing. AS: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – review & editing. GF: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Visualization, Writing – review & editing. ND: Conceptualization, Funding acquisition, Resources, Supervision, Validation, Visualization, Writing – review & editing. OF: Resources, Supervision, Validation, Visualization, Writing – review & editing, Conceptualization, Funding acquisition.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The IPD’s proper funds supported this work. This research was also funded supported by the International Development Research Center (grant 109075-001), the Canadian Department of Global Affairs (grant BIO-2019-005).
Acknowledgments
We extend our sincere gratitude to the Ministry of Health and Social Action for their support, as well as to all healthcare workers at the sentinel sites. We are pleased to thank all the virology department members and the Dalal Jam National Hospital Center urgent care unit members for their helpful contribution to this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bente DA, Forrester NL, Watts DM, McAuley AJ, Whitehouse CA, Bray M. Crimean-Congo hemorrhagic fever: history, epidemiology, pathogenesis, clinical syndrome and genetic diversity. Antiviral Res. (2013) 100:159−89.
2. Duh D, Saksida A, Petrovec M, Ahmeti S, Dedushaj I, Panning M, et al. Viral load as predictor of crimean-congo hemorrhagic fever outcome. Emerging Infect Dis J. (2007) 13.
3. Ergonul O, Tuncbilek S, Baykam N, Celikbas A, Dokuzoguz B. Evaluation of serum levels of interleukin (IL)-6, IL-10, and tumor necrosis factor-alpha in patients with Crimean-Congo hemorrhagic fever. J Infect Dis. (2006) 193:941−4.
4. Ergönül Ö, Şeref C, Eren Ş, Çelikbaş A, Baykam N, Dokuzoğuz B, et al. Cytokine response in crimean-congo hemorrhagic fever virus infection. J Med Virol. (2017) 89:1707−13.
5. Kaya S, Elaldi N, Kubar A, Gursoy N, Yilmaz M, Karakus G, et al. Sequential determination of serum viral titers, virus-specific IgG antibodies, and TNF-α, IL-6, IL-10, and IFN-γ levels in patients with Crimean-Congo hemorrhagic fever. BMC Infect Dis. (2014) 14:416.
6. Papa A, Bino S, Velo E, Harxhi A, Kota M, Antoniadis A. Cytokine levels in Crimean-Congo hemorrhagic fever. J Clin Virol. (2006) 36:272−6.
7. Sahay RR, Shete AM, Yadav PD, Patil S, Majumdar T, Jain R, et al. Sequential determination of viral load, humoral responses and phylogenetic analysis in fatal and non-fatal cases of Crimean-Congo hemorrhagic fever patients from Gujarat, India, 2019. PloS Negl Trop Dis. (2021) 15:e0009718.
8. Chunikhin SP, Chumakov MP, Butenko AM, Smirnova SE, Taufflieb R, Camicas JL, et al. Results from investigating human and domestic and wild animal blood sera in the Sénégal Republic (western Africa) for antibodies to Crimean hemorrhagic fever virus Vol. 2. Moscow: Mater16 NauchnSessInstPolioVirusEntsefalitov (1969). p. 158−60.
9. Gahn MCB, Diouf G, Cissé N, Ciss M, Bordier M, Ndiaye M, et al. Large-scale serological survey of crimean-congo hemorrhagic fever virus and rift valley fever virus in small ruminants in Senegal. Pathogens. 15 août. (2024) 13:689.
10. Niang MN, Dosseh A, Ndiaye K, Sagna M, Gregory V, Goudiaby D, et al. Sentinel surveillance for influenza in Senegal, 1996-2009. J Infect Dis 15 déc. (2012) 206 Suppl 1:S129–135.
11. Weidmann M, Faye O, Faye O, Abd El Wahed A, Patel P, Batejat C, et al. Development of mobile laboratory for viral hemorrhagic fever detection in africa. J Infect Dis. (2018) 218:1622−30.
12. Yapar M, Aydogan H, Pahsa A, Besirbellioglu BA, Bodur H, Basustaoglu AC, et al. Rapid and quantitative detection of Crimean-Congo hemorrhagic fever virus by one-step real-time reverse transcriptase-PCR. Jpn J Infect Dis. (2005) 58:358−62.
13. Tezer H, Polat M. Diagnosis of Crimean-Congo hemorrhagic fever. Expert Rev Anti-infective Ther. (2015) 13:555−66.
Keywords: CCHFV, biomarkers, viremia, immunoglobulins, cytokines, severity
Citation: Mhamadi M, Sene O, Diamanka A, Mhamadi M, Mendy MP, Diouf AM, Ndiaye M, Barry MA, Niang Sagne S, Traoré MC, Sall AA, Fall G, Dia N and Faye O (2025) Case report: Kinetics of viral load, immunoglobulins, and cytokines in a fatal case of Crimean-Congo hemorrhagic fever virus. Front. Virol. 4:1498672. doi: 10.3389/fviro.2024.1498672
Received: 19 September 2024; Accepted: 09 December 2024;
Published: 07 January 2025.
Edited by:
Emanuela Marcenaro, University of Genoa, ItalyReviewed by:
Ling Ding, University of Pittsburgh Medical Center, United StatesSthita Pragnya Behera, Indian Council of Medical Research (ICMR), India
Copyright © 2025 Mhamadi, Sene, Diamanka, Mhamadi, Mendy, Diouf, Ndiaye, Barry, Niang Sagne, Traoré, Sall, Fall, Dia and Faye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Moufid Mhamadi, bW91ZmlkLm1oYW1hZGlAcGFzdGV1ci5zbg==