 Diego Pulido Vega
Diego Pulido Vega Jérémie Ficheroulle
Jérémie Ficheroulle Mathieu Manassero
Mathieu Manassero Jeremy Mortier
Jeremy Mortier Christelle Maurey
Christelle Maurey- 1Service of Diagnostic Imaging, DEPEC, École Nationale Vétérinaire d’Alfort, Maisons-Alfort, France
- 2Teaching and Clinical Department of Companion Animal, Faculty of Veterinary Medicine, Fundamental and Applied Research for Animals and Health, University of Liège, Liège, Belgium
- 3Service of Small Animal Surgery, École Nationale Vétérinaire d’Alfort, Maisons-Alfort, France
- 4Laboratoire de Santé Animale, Service of Internal Medicine, École Nationale Vétérinaire d’Alfort, INRAE, ANSES, UMR Virology, Maisons-Alfort, France
Introduction: Prediction of renal recovery after surgical management of feline unilateral ureteral obstruction (UO) is crucial to guide therapeutic decisions, but predictors of this outcome are still lacking. Despite the functional importance of the contralateral kidney, there is currently no precise description of its ultrasonographic (US) features. In addition, US parameters of both the renal collecting system and the renal parenchyma have been identified in human medicine as prognostic factors in the case of UO but have not been described in veterinary medicine. The aim of this study was to evaluate an association between preoperative structural US renal parameters and long-term International Renal Interest Society (IRIS) stage after successful renal decompression with subcutaneous ureteral bypass (SUB) device in cats with unilateral UO.
Methods: This retrospective study included 60 cats with unilateral UO and evaluated preoperative US parameters of both kidneys, including measurements of parenchymal and pelvic areas as well as a renal score. Cats were divided according to their serum creatinine at 3 months postoperatively into group A (IRIS stages I and II) and group B (IRIS stages III and IV).
Results: A higher US chronic kidney disease (US-CKD) score of the kidney contralateral to the UO was associated with long-term IRIS stages III and IV. It also appeared as a fair discriminator of long-term IRIS stage IV, with an area under the curve of 0.74. The optimal cutoff value for accurately identifying cats with long-term IRIS stage IV was a US-CKD score > 7, with a specificity of 98%, a sensitivity of 25%, and a positive likelihood ratio of 12.75. No preoperative US parameters regarding the obstructed kidney, including parenchymal and pelvic areas, were significantly associated with long-term creatinine.
Conclusion: Ultrasonographic scoring of contralateral chronic kidney disease abnormalities is associated with IRIS stage following treatment of feline unilateral UO with a SUB device and serves as a specific indicator of cats presenting with long-term IRIS stage IV.
1 Introduction
Ureteral obstruction (UO) is a common cause of acute azotemia in cats, frequently occurring concurrently with chronic kidney disease (CKD) (1–3). Its most common etiology is ureterolithiasis, which is predominantly composed of calcium oxalate (4–11). Treatment of UO is challenging, and a subcutaneous ureteral bypass (SUB) device placement is considered an effective therapeutic strategy, with a low postoperative death rate and an excellent outcome (3, 12). However, this technique comes with high costs for the owners, a demanding follow-up, and a significant rate of long-term complications. In addition, postoperative renal function often remains impaired after the acute episode, reflecting not only the effects of concurrent CKD but also the sequelae of UO, with half of cats having a serum creatinine (SCr) greater than 3.2 mg/dL 6 months after surgery (3, 12–14).
In this context, the identification of prognostic factors is crucial to assist clinicians and pet owners in the surgical decision-making process. In two previous studies (9, 15), no preoperative clinical, biochemical, or ultrasonographic (US) finding was found predictive of long-term renal recovery, although the focus was on the imaging characteristics of the obstructed kidney alone. The McEntee et al. study (15) introduced a ratio of pelvic dilation to overall renal size which was not predictive of long-term SCr. Similar parameters assessing areas, rather than lengths, of both the renal parenchyma and the pelvic dilation have been described in human medicine. For instance, the parenchyma-to-hydronephrosis area ratio (PHAR) has proved to be predictive of renal function recovery after surgery in the context of ureteropelvic junction obstruction (16, 17), but it has not been studied in the context of UO in veterinary medicine.
To the best of the author’s knowledge, the US description of feline unilateral UO only focuses on the obstructed kidney, with no mention other than the size of the contralateral kidney (15, 18–22). Given that azotemia remains undetected until 75% of the renal function has been lost (23), unilateral UO does not result in azotemia if the contralateral kidney is functioning well. However, in cats, UO occurs in the course of a CKD, possibly fostered through repeated asymptomatic ureteral obstructive episodes (5), contributing to pre-existing renal damage within the contralateral kidney and explaining why UO becomes clinically relevant (24). This pathophysiological sequence underlines the need for a careful assessment of the contralateral kidney.
The aims of this study were (1) to assess the replicability of the research of McEntee et al. (15) performed on the obstructed kidney with a focus on additional novel US parameters and (2) to extend their work by evaluating ultrasonographically the contralateral kidney with the hypothesis that some parameters would show an association with the long-term renal recovery after pelvic decompression with a SUB device.
2 Materials and methods
2.1 Selection of cases
Medical and US records of all cats treated with a SUB device (Norfolk Vet Products) between December 2013 and January 2021 at the National Veterinary School of Alfort were retrospectively reviewed. Cats were included in the study if they presented a benign unilateral UO, renal preoperative US images and were followed for at least 3 months postoperatively with ultrasonographic evidence of renal pelvic decompression and patency of the device. Cats that died from renal causes during the 3-month follow-up were also included. Ureteral obstruction was diagnosed based on clinical signs, the presence of azotemia, and US findings such as pelvic dilation, diverticular dilation, ureteral dilation, intraluminal obstructive lesion, or some combination of these. Cats were treated in accordance with the standard surgical and perioperative management protocols, as previously described (3). Long-term follow-up was determined as the first follow-up occurring more than 3 months postoperatively. Additional data were collected and reviewed on a case-by-case basis, by a board-certified veterinary specialist in internal medicine (CM), to identify cats presenting with an acute or chronic kidney disease at the time of the long-term follow-up. This was based on a combination of criteria such as an increase in SCr higher than 20% above the last SCr measurement, acute onset of clinical signs (e.g., anorexia, lethargy, and vomiting), US images at the time of long-term follow-up compared with previous examinations, urine culture, and serum amyloid A protein (SAA) when available. For these cats, the long-term follow-up date was determined as the first follow-up in which the acute or chronic kidney event was resolved. Cats with bilateral UO, ureteral rupture, and UO of neoplastic origin, cats treated as part of a second surgery for UO, with incomplete medical records, lost to follow-up, or deceased from unknown or non-renal cause before long-term follow-up were excluded.
2.2 Clinical and biological data
Preoperative standardized clinical data were gathered from all cats including age, sex, breed, weight, nature, and duration of clinical signs. Blood samples and chemistry were collected. During surgery, pelvic urine from the obstructed kidney was collected for bacterial culture. Postoperative data included SCr follow-up for at least 3 months.
2.3 Ultrasonographic findings
The US examinations were performed using different ultrasound machines over the study time (IU22, Philips; Affinity 50, Philips) and by various experienced ultrasonographers. A multifrequency (5–8 MHz) microconvex or a multifrequency (5–18 MHz) linear transducer was used for ultrasound examination. Preoperative abdominal US still images were blindly reviewed by a veterinary radiology resident (JF). Measurements were performed for each kidney using the National Institutes of Health image software (Image J 1.53 k). Renal length was determined as the maximum longitudinal dimension in a sagittal plane. Pelvic diameter was measured in sagittal and transverse planes from one pelvic margin to another (Figure 1). Renal parenchymal thickness was defined as the distance between the renal sinus fat to the renal capsule in a sagittal plane. Renal cortical thickness was determined in a sagittal plane as the distance from the corticomedullary interface to the renal capsule. Cranial ureteral diameter was measured just caudally to the ureteropelvic junction, in the transverse plane. Ureteral diameter upstream of the obstruction site was measured in the sagittal plane, if an obstruction site was identified (Figure 2). The total renal area and pelvic area were determined by outlining the kidney and the pelvis on a sagittal plane as previously described (Figure 3) (25–28). The renal parenchymal area (RPA) was calculated by subtracting the pelvic area from the total renal area. Total RPA was defined as the sum of the RPA of both kidneys. Parenchyma-to-hydronephrosis area ratio (PHAR) was calculated by dividing the RPA by the pelvic area, only for obstructed kidneys.
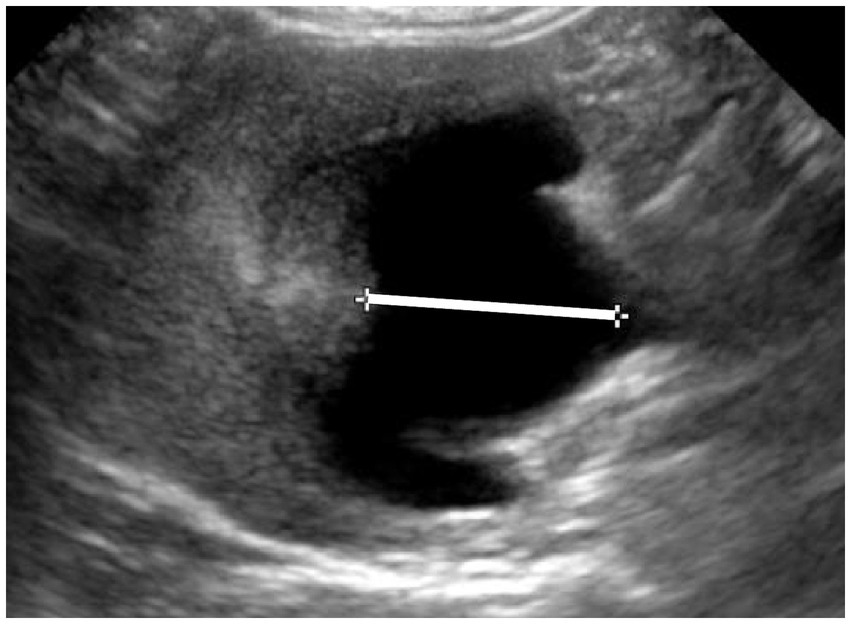
Figure 1. Ultrasonographic image of an obstructed kidney, in a transverse plane. The white line indicates the pelvic dilatation, spanning from one edge of the pelvis to the other, with a width of 7 mm.
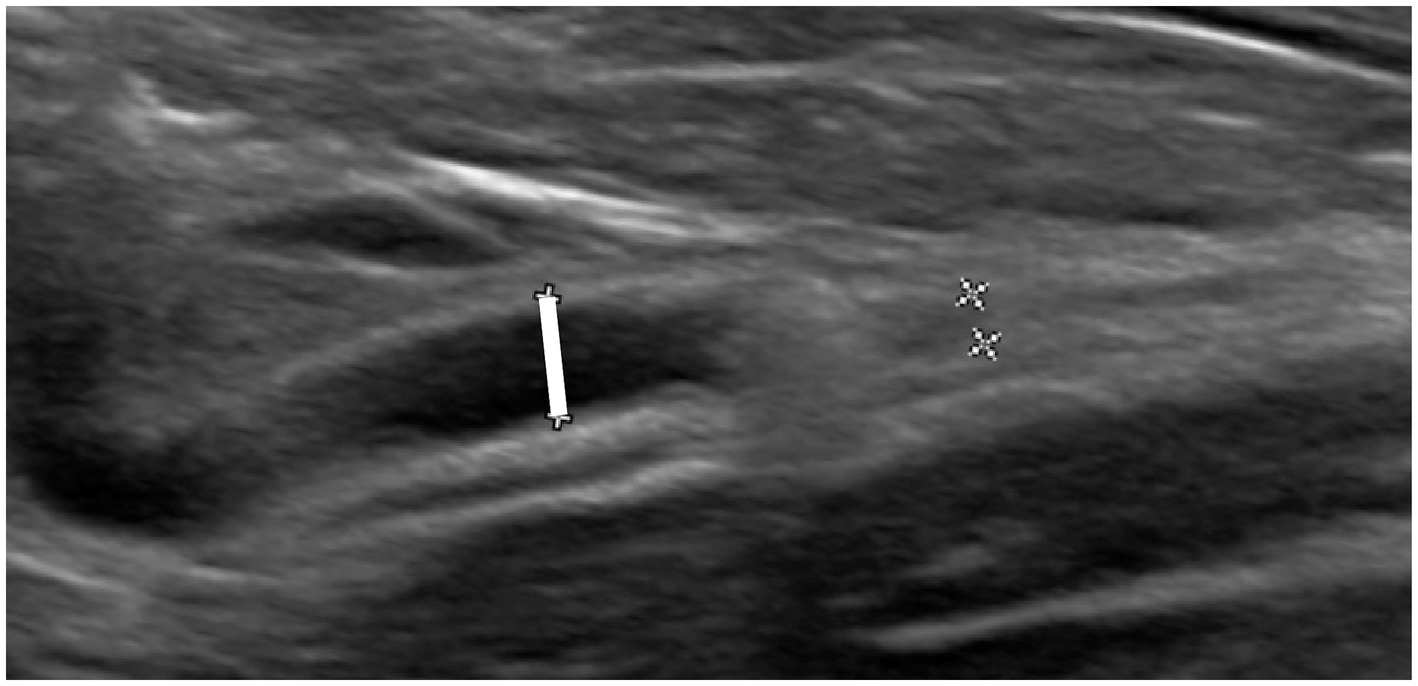
Figure 2. Ultrasonographic image of a ureter with intraluminal calculi. The ureter is dilated upstream of the calculi, and its diameter is indicated with the white line (measuring 2.3 mm), with no downstream dilation.
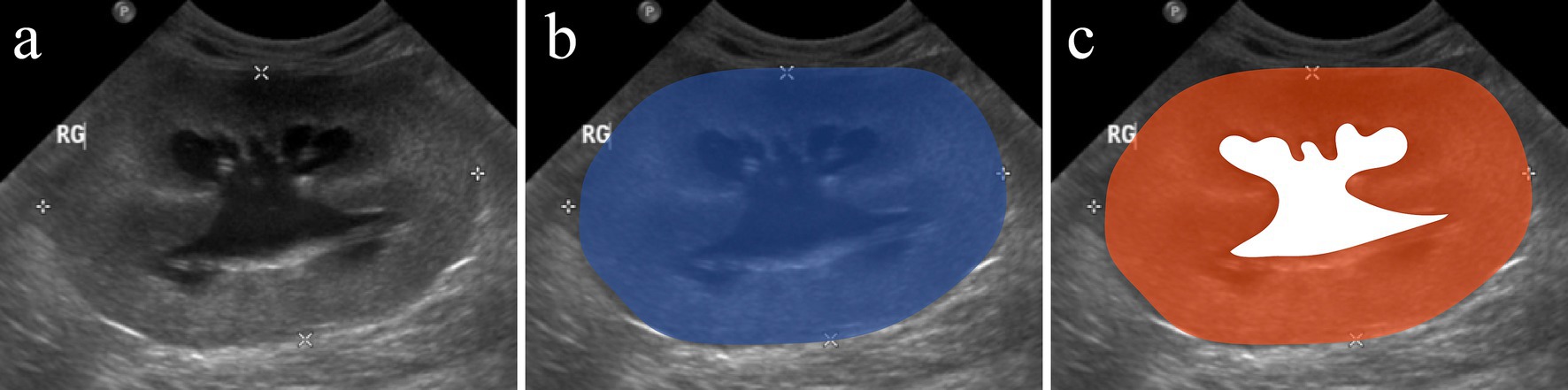
Figure 3. Parenchyma-to-hydronephrosis area ratio (PHAR) measurement on an ultrasonographic image of a kidney with hydronephrosis. Sagittal image of a hydronephrotic kidney (A). The blue area (B) corresponds to the total renal area. The white area (C) corresponds to the pelvic area. The renal parenchymal area (RPA) was calculated by subtracting the pelvic area from the total renal area and corresponds to the orange area (C). The PHAR was calculated by dividing the RPA by the pelvic area.
To grade the severity of the CKD on US images, we proposed a US-CKD score. This score allowed a semi-quantitative US description of the kidneys based on the presence of findings reportedly associated with CKD including corticomedullary differentiation attenuation, medullary rim sign, irregular renal margination, renal infarcts, and renal cysts (29–32). A sub-score was assigned to each US finding according to their presence or severity as described in Table 1. The ultrasonographic CKD score was defined as the sum of each sub-score for one kidney (ranging from 0 to 8), and the total US-CKD score was defined as the sum of the US-CKD score of both kidneys.
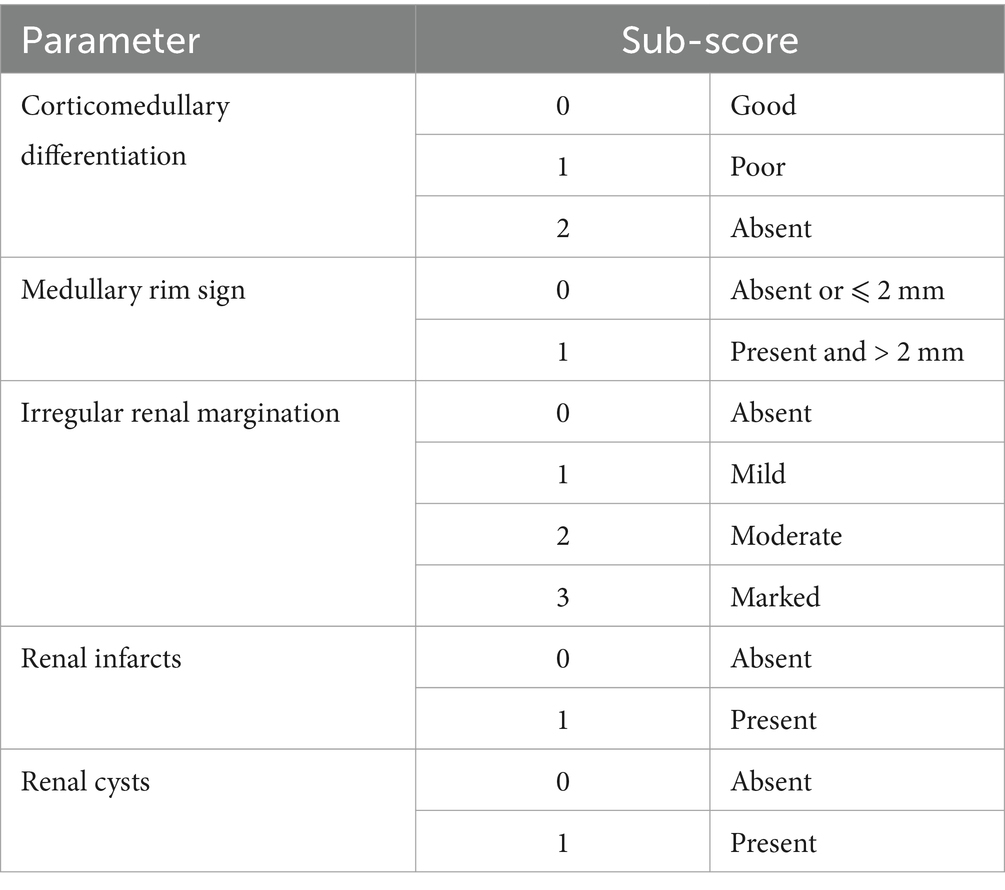
Table 1. Ultrasonographic characteristics assessed to calculate the ultrasonographic chronic kidney disease score (US-CKD score).
2.4 Groups
Cats were divided into two groups based on their long-term renal recovery. Group A included cats with SCr ⩽ 2.8 mg/dL, corresponding to stages I and II of the International Renal Interest Society (IRIS) classification (33). Group B included cats with SCr > 2.8 mg/dL and cats that died from renal causes during the 3-month follow-up period. The SCr cutoff was based on survival analysis of existing data: Median survival time was superior to 2,250 days in stage IRIS stages I and II cats, while it was 608 and 67 days in IRIS stages III and IV cats, respectively, based on their SCr measured 3 months postoperatively in one study (3).
2.5 Data analysis and statistics
Statistical analysis was performed using a statistical package (BiostaTGV, Pierre Louis Institute of Epidemiology and Public Health UMR S 1136). Quantitative descriptive results are presented as medians with ranges. Dichotomous variables are presented as percentages and associated with the number of cases included. Association between US features and groups was assessed using the Mann–Whitney U-test for continuous data and either the χ2 test or Fisher’s exact test for categorical data. The Wilcoxon signed-rank test was used for comparison between the change in SCr between the preoperative period and long-term follow-up. Receiver operating characteristic (ROC) curves were used to assess the diagnostic utility of quantitative US parameters that differed significantly between groups. The generalized Youden index was used to identify optimal cutoff values. An AUC of >0.9 was interpreted as excellent, 0.8 to 0.89 as good, 0.7 to 0.79 as fair, 0.6 to 0.69 as poor, and 0.5 to 0.59 as failure (34), and values are accompanied by their respective 95% confidence intervals (CIs). The level of statistical significance selected was set at a p-value of <0.05.
3 Results
3.1 Study population
Ninety-eight cats were treated with an SUB device between December 2013 and January 2021 and recruited for the study. Thirty-eight cats were excluded as follows: 25 due to admission criteria and 13 due to follow-up criteria (see Supplementary Figure S1). Fifteen cats presented a bilateral UO, six cats presented a ureteral rupture, and four cats were treated as part of a second surgery on UO. During the follow-up period, one cat presented a contralateral UO, two cats presented an obstruction of the SUB device, and four cats were lost to follow-up. One cat was excluded because of truncated US images. Three cats died of unknown reasons after discharge, and two cats died from non-renal causes: One presented with respiratory distress and signs of congestive heart failure, and the second presented a resolution of azotemia after treatment but died after a blood transfusion. The remaining 60 cats were included in the study, of which four cats died or were euthanized due to persistent marked azotemia and did not survive discharge (range 2–8 days postoperatively). These cats were part of group B, along with cats presenting a long-term SCr > 2.8 mg/dL.
3.2 Clinical data
Descriptive statistics on the study population are summarized in Table 2. Of the 60 cats, 38 (63%) were females and 22/60 (37%) were males, of which 31/38 (82%) and 19/22 (86%) were neutered. The median age at presentation was 6.1 years (range 1.5–15.7 years). On admission, median packed cell volume (PCV) was 30% (range 17–45%), and median SCr was 5.9 mg/dL (range 1.4–18.1) with 59/60 (98%) cats being azotemic. Other biochemical abnormalities included anemia (42%, n = 25/59), hyperphosphatemia (36%, n = 9/25), hyperkalemia (20%, n = 12/59), and ionized hypercalcemia (10%, n = 5/50). Urine culture obtained by pyelocentesis at the time of SUB placement was positive in 11/59 (18.6%) cats. The median long-term follow-up was 4 months (range 3–8 months). The median long-term SCr was 2.3 mg/dL (range 1.2–5.4 mg/dL), which was significantly lower than preoperative values (p < 0.001) and associated with a median decrease in SCr of 3 mg/dL (range 0.1–16.4 mg/dL). Among the 60 cats included, 43 (72%) presented a long-term SCr ⩽ 2.8 mg/dL and were part of group A. The remaining 17 cats (28%) were part of group B and included 12 cats with long-term SCr > 2.8 mg/dL and 5 cats that died of renal causes, as described above. Eleven cats presented bacteriuria on urine collected from the SUB device at the time of long-term follow-up. Of these cats, one presented an acute or chronic kidney disease suspected to be pyelonephritis, based on the elevation of SCr, bacteriuria, evocative US findings, and increased SAA. In this case, the long-term follow-up date was set 1.5 months later, when the acute or chronic kidney event had resolved (SCr = 2.5 mg/dL and normalization of SAA). The remaining cats were asymptomatic, and none were suspected of presenting an acute kidney injury at this time based on clinical signs, biological data, and evaluation of serial postoperative SCr values at follow-up. Female cats were significantly more frequent in group A than in group B (72% vs. 41%; p = 0.03). The remaining clinical data were not significantly different between groups (Supplementary Table S1).
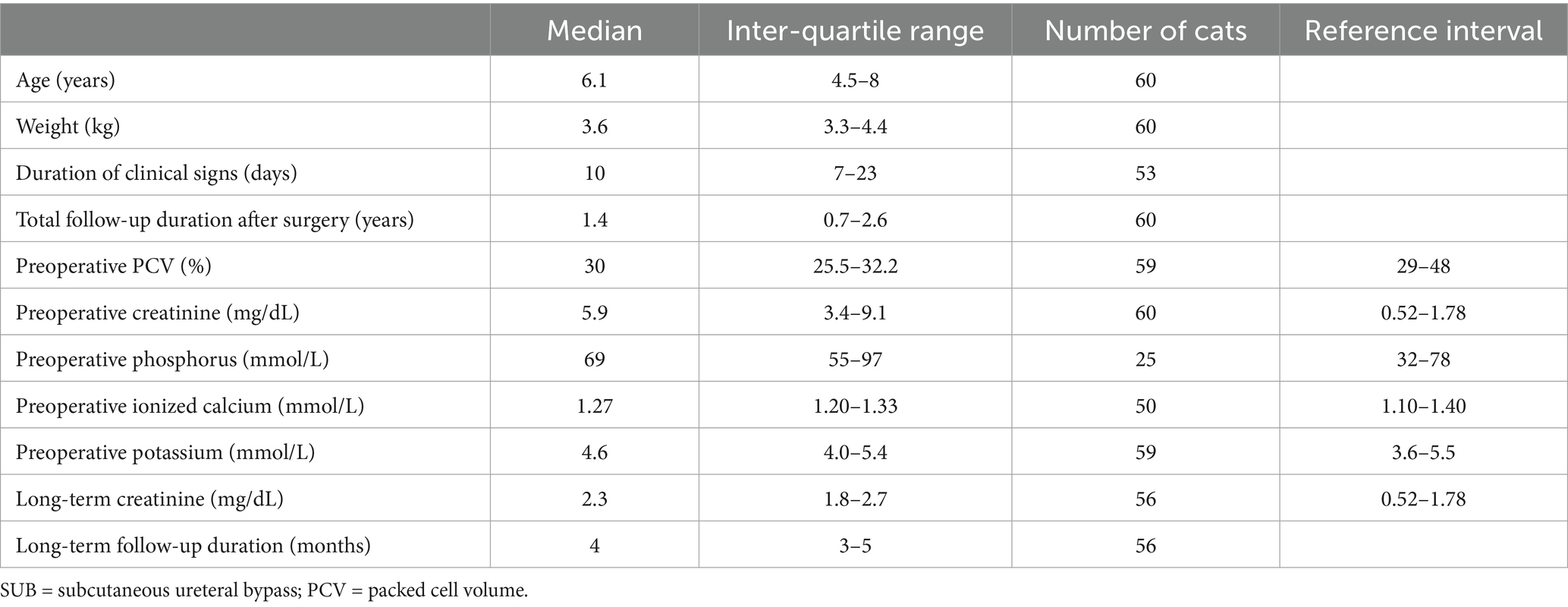
Table 2. Descriptive statistics in cats with unilateral ureteral obstruction treated with a SUB device.
3.3 Ultrasonographic findings
Preoperative US data are summarized in Tables 3, 4. Thirty-five cats were obstructed on the right side (58%) and 25 on the left side (42%). Obstructed kidneys had a median length of 4.4 cm (range 2.3–6 cm) and presented a median pelvic diameter in the transverse plane of 7.2 mm (range 1.4–20.1 mm). Ipsilateral nephroliths were identified in 35 (58%) cats. Peri-renal effusion, peri-renal fat hyperechogenicity, attenuation of the corticomedullary distinction, and renal infarcts were identified in 10 (17%), 14 (23%), 40 (67%), and 32 (53%) cats, respectively. The median US-CKD score was 3 (range 0–7). Median cranial ureteral diameter and upstream obstruction site were 4.8 mm (range 1.5–14 mm) and 3 mm (range 1.6–19.3 mm), respectively. The contralateral kidney had a median length of 3.1 cm (range 1.2–4.9 cm). The most frequent structural abnormalities of this kidney were attenuation of the corticomedullary distinction, renal infarcts, moderately to markedly irregular margination, and pelvic mineralization in 53 (90%), 49 (83%), 44 (75%), and 40 (68%) cats, respectively. The median US-CKD score was 5 (range 0–8) which was significantly higher than in the obstructed kidney (p < 0.01; n = 59). Nephroliths were identified in 40 (68%) contralateral kidneys.
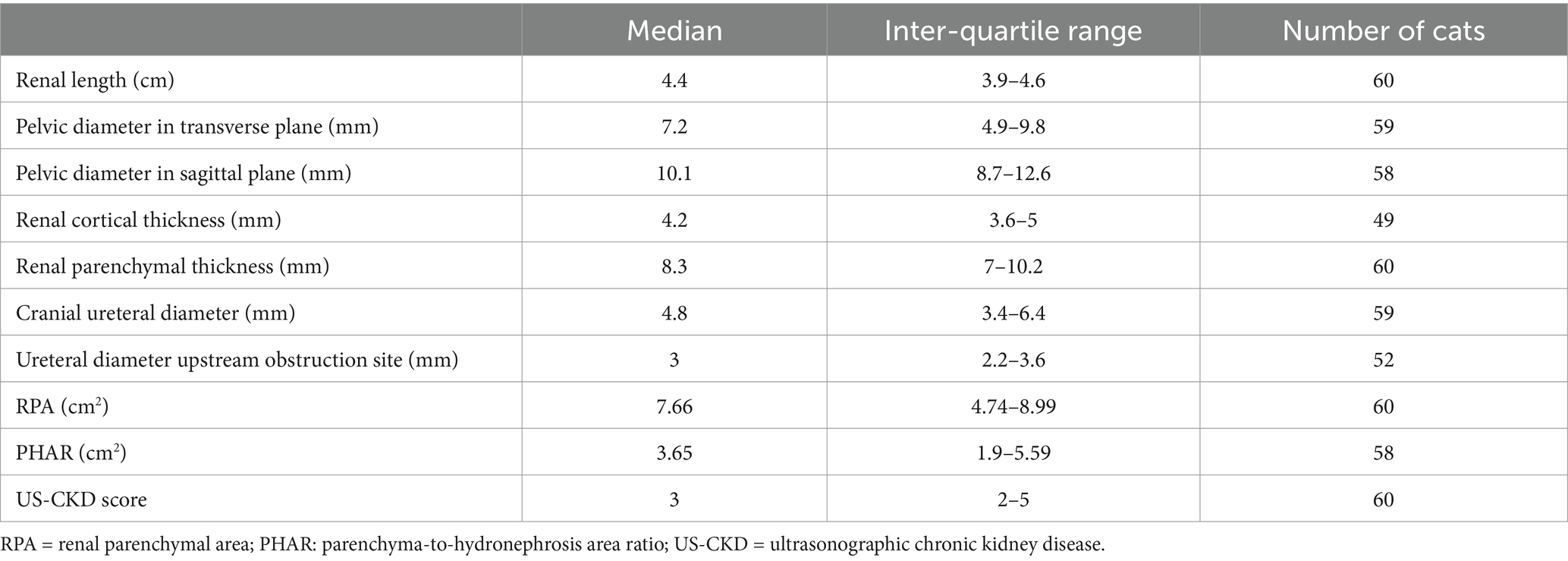
Table 3. Ultrasonographic parameters of the obstructed kidney in cats with unilateral ureteral obstruction.
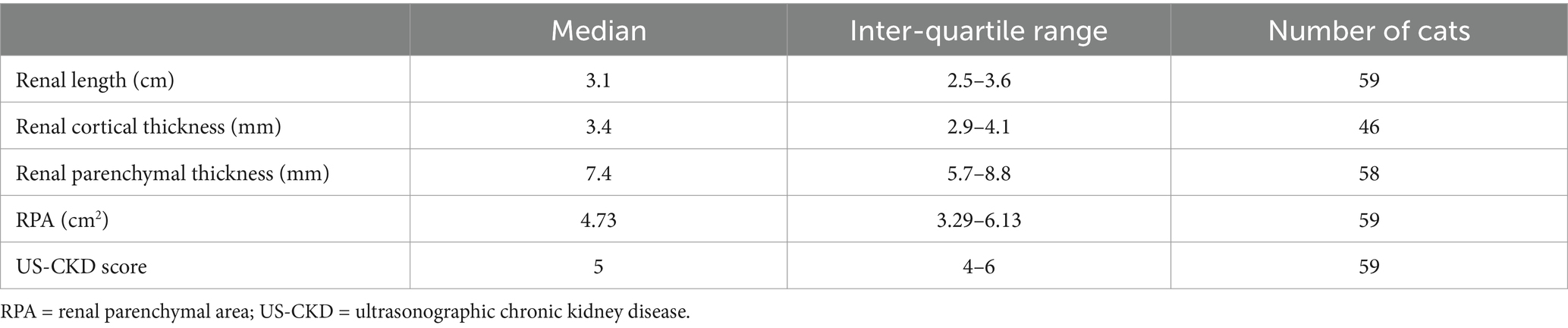
Table 4. Ultrasonographic parameters of the kidney contralateral to the ureteral obstruction in cats with unilateral ureteral obstruction.
The median US-CKD score of the contralateral kidney was significantly higher in group B (median, 5 in group A; median, 6 in group B; p = 0.01). Through ROC curve analysis, the US-CKD score of the contralateral kidney was a fair discriminator between groups A and B (AUC = 0.71, p < 0.01, 95% CI: 0.57–0.85). The optimal cutoff to correctly identify group B was a US-CKD score > 6 (specificity: 90.5%; sensitivity: 29.4%) and was associated with a likelihood ratio of 3.1 (95% CI: 0.94–4.94). Higher US-CKD score of the contralateral kidney was also significantly associated with cats presenting long-term CKD IRIS stage IV disease (median, 5 in IRIS stages I–III; median, 6 in stage IV; p = 0.028). The US-CKD score of the contralateral kidney was still a fair discriminator to distinguish cats presenting long-term CKD IRIS stage IV disease from others (AUC = 0.74; p = 0.02, 95% CI: 0.54–0.94). The optimal cutoff to correctly identify cats presenting long-term CKD IRIS stage IV disease was a US-CKD score > 7 (specificity: 98%; sensitivity: 25%) and was associated with a likelihood ratio of 12.75 (95% CI: 1.30–124.88). US-CKD score of the obstructed kidney was not significantly different among groups (median, 3 in each group; p = 0.56). Median total US-CKD score was higher in group B than in group A, but no statistical significance was reached (median, 8 in group A; median, 9 in group B; p = 0.08). No other preoperative US parameter, including RPA and PHAR, was significantly associated with long-term SCr (Table 5; Supplementary Table S2).
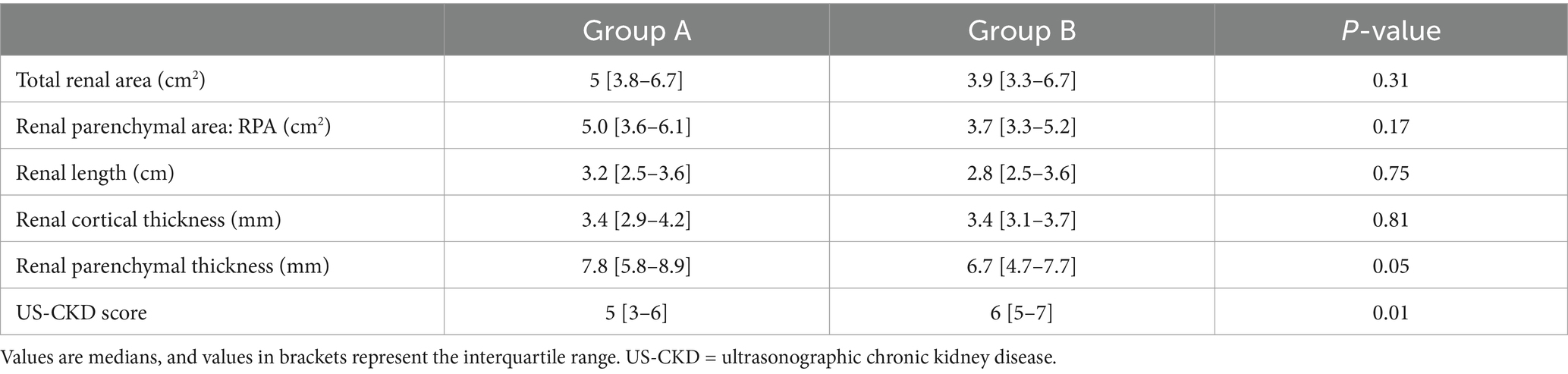
Table 5. Evaluation of the association between long-term serum creatinine and ultrasonographic parameters of the kidney contralateral to ureteral obstruction in included cats.
4 Discussion
This retrospective study is the first to focus on the preoperative US appearance of the contralateral kidney to predict renal function recovery after surgical treatment of feline unilateral ureteral obstruction. A higher US-CKD score of the contralateral kidney was significantly associated with a poor outcome (SCr > 2.8 mg/dL) at 3 months postoperatively. A cutoff score of >6 discriminated these cats with a specificity of 90.5% and a sensitivity of 29.4%. These results suggest that the potential for renal recovery after unilateral SUB device placement should be discussed with owners in light of the US aspect of the contralateral kidney.
Despite its importance, the ultrasonographic description of the kidney contralateral to unilateral UO is scarce (15, 18–21) and limited to its size, reported as a mean of 6 mm smaller than the obstructed kidney (22). This phenomenon is referred to as “big kidney, little kidney” and results from repeated subclinical obstructive episodes leading to nephron loss and fibrosis (5, 19). To further characterize the contralateral kidney and to grade the US abnormalities associated with CKD, a US-CKD score was proposed. This score is based on the semi-quantitative evaluation of US structural indicators that are reportedly associated with CKD (28–32). In the present study, a higher preoperative contralateral US-CKD score was associated with long-term IRIS stages III and IV (group B). This is likely to have clinical implications as the latter are associated with median survival times of 608 days and 67 days, respectively, compared to more than 2,250 days in stage IRIS stages I and II, based on SCr measured 3 months postoperatively in one study (3). However, there is still a significant difference in median survival time within cats in group B. Therefore, we decided to identify a specific cutoff value to discriminate cats with long-term IRIS stage IV from others, and the value of US-CKD >7 showed a specificity of 98% and a sensitivity of 25%. This cutoff was also associated with an excellent likelihood ratio of 12.75 (95% CI: 1.30–124.88). Assuming that the pre-test probability of reaching IRIS stage IV in the long-term is similar to its prevalence in our study population (15%), this means that identifying preoperatively a US-CKD >7 in the contralateral kidney would substantially raise its post-test probability from 15 to 69% (35). It should be noted that this cutoff value is not sensitive and is primarily intended to identify cats that are at a high risk of poor renal recovery following surgery. Further research is required to validate prospectively the use of the US-CKD score in alternative contexts and more specifically to correlate its value with basal SCr values. Among other US parameters studied, the median parenchymal thickness of the contralateral kidney was lower in cats of group B (7.8 mm in group A; 6.7 mm in group B) even though this parameter did not reach statistical significance (p = 0.05). This is in accordance with a previous study that reported a decrease in renal cortical thickness in cats with impaired renal function (36). These findings highlight the importance of the contralateral kidney in the overall renal function following surgical intervention and advocate for its preoperative US assessment to aid in the surgical decision-making process.
In human medicine, area measurements have been developed to provide a more accurate and objective assessment of hydronephrotic kidneys with ultrasonography. The renal parenchymal area is highly and positively correlated with the renal volume measured by magnetic resonance imaging, with no effect of hydronephrosis on this correlation (37, 38) and serves as an early marker to predict future renal deterioration in infants with posterior urethral valves (39). The parenchyma-to-hydronephrosis area ratio is another parameter that combines the value of the parenchymal area with an objective measure of hydronephrosis. It is used to identify patients who are more suitable for surgery in the context of ureteropelvic junction obstruction as it has been found to predict postoperative renal function in humans undergoing pyeloplasty (16, 17, 38). In this study, it was hypothesized that these preoperative US structural parameters would correlate with nephron mass and serve as surrogate markers of functional renal reserve in cats with ureteral obstruction. However, parenchymal and hydronephrosis area measurements did not allow to predict renal recovery in this study, and one explanation could be that feline UO occurs in the context of CKD, in contrast to humans. Similarly, other regularly measured US parameters of the obstructed kidney did not correlate with long-term SCr, which aligns with the previous results of a recent study (15). These data support the argument that identification of US features such as severe hydronephrosis or thin parenchyma on the obstructed kidney should not deter surgical decompression in cats presenting with unilateral UO as there is no evidence to suggest that these features adversely impact long-term renal recovery.
Our study has a number of limitations. The sample size is moderate owing to the exclusion of a large number of cases, and this might have underpowered the statistical analyses. The long-term follow-up was set at a minimum of 3 months, and a longer period could have helped to better characterize renal recovery. This may only have little impact as other studies suggested overall stability of SCr after 3 months postoperatively (9, 12, 40). As acute events on CKD are part of this disease and may impact long-term outcomes, such cases were included in the study to avoid selection bias. This happened for one case of suspected pyelonephritis, and the long-term follow-up SCr was set when the acute event had resolved. Bacteriuria was detected in 11 cats at the date of follow-up, including the case of suspected pyelonephritis. The remaining cases presenting bacteriuria showed no clinical signs and an overall stability of SCr concentration at the date of long-term follow-up. A previous study reported that postoperative asymptomatic bacteriuria was not associated with survival and that no increase of SCr was observed in these cats (12). In our population, there was no significant difference in the proportion of cats presenting with long-term bacteriuria between the two groups (p = 1; n = 48). Owing to the retrospective nature of the study, preoperative US was performed by different ultrasonographers. To limit inter-observer variability, all measurements were taken by a single observer. The assessment of some criteria (e.g., cortical thickness) was sometimes challenging as it relied on retrospectively acquired still US images. Standardized prospective evaluation of the US-CKD score, which may also be useful in the follow-up of CKD alone, is required in a larger cohort and with multivariable analysis to confirm our results and draw causal inferences.
5 Conclusion
Evaluation of US findings consistent with CKD on the kidney contralateral to UO is beneficial to assess the postoperative evolution of SCr in cats treated unilaterally with an SUB device. In particular, the identification of severe signs of CKD in the contralateral kidney is associated with long-term IRIS stage IV with high specificity. However, measurements of renal parenchymal and hydronephrosis areas were not useful in predicting long-term renal recovery in cats after surgical decompression.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving animals in accordance with the local legislation and institutional requirements because the study only involved retrospectively collected clinical data. Written informed consent was obtained from the owners for the participation of their animals in this study.
Author contributions
DP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. JF: Data curation, Investigation, Methodology, Resources, Writing – review & editing. MM: Methodology, Resources, Supervision, Writing – review & editing. JM: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – review & editing. CM: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fvets.2025.1518713/full#supplementary-material
References
1. Kopecny, L, Palm, CA, Drobatz, KJ, Balsa, IM, and Culp, WTN. Risk factors for positive urine cultures in cats with subcutaneous ureteral bypass and ureteral stents (2010-2016). J Vet Intern Med. (2019) 33:178–83. doi: 10.1111/jvim.15343
2. Kyles, AE, Stone, EA, Gookin, J, Spaulding, K, Clary, EM, Wylie, K, et al. Diagnosis and surgical management of obstructive ureteral calculi in cats: 11 cases (1993-1996). J Am Vet Med Assoc. (1998) 213:1150–6. doi: 10.2460/javma.1998.213.08.1150
3. Berent, AC, Weisse, CW, Bagley, DH, and Lamb, K. Use of a subcutaneous ureteral bypass device for treatment of benign ureteral obstruction in cats: 174 ureters in 134 cats (2009–2015). J Am Vet Med Assoc. (2018) 253:1309–27. doi: 10.2460/javma.253.10.1309
4. Wormser, C, Phillips, H, and Aronson, LR. Retroperitoneal fibrosis in feline renal transplant recipients: 29 cases (1998-2011). J Am Vet Med Assoc. (2013) 243:1580–5. doi: 10.2460/javma.243.11.1580
5. Cohen, L, Shipov, A, Ranen, E, Bruchim, Y, and Segev, G. Bilateral ureteral obstruction in a cat due to a ureteral transitional cell carcinoma. Can Vet J. (2012) 53:535–8.
6. Johnson, CM, Culp, WTN, Palm, CA, and Zacuto, AC. Subcutaneous ureteral bypass device for treatment of iatrogenic ureteral ligation in a kitten. J Am Vet Med Assoc. (2015) 247:924–31. doi: 10.2460/javma.247.8.924
7. Westropp, J, Ruby, A, Bailiff, N, Kyles, A, and Ling, V. Dried solidified blood calculi in the urinary tract of cats. J Vet Intern Med. (2006) 20:828–34. doi: 10.1111/j.1939-1676.2006.tb01793.x
8. Zaid, MS, Berent, AC, Weisse, C, and Caceres, A. Feline ureteral strictures: 10 cases (2007–2009). J Vet Intern Med. (2011) 25:222–9. doi: 10.1111/j.1939-1676.2011.0679.x
9. Horowitz, C, Berent, A, Weisse, C, Langston, C, and Bagley, D. Predictors of outcome for cats with ureteral obstructions after interventional management using ureteral stents or a subcutaneous ureteral bypass device. J Feline Med Surg. (2013) 15:1052–62. doi: 10.1177/1098612X13489055
10. Kyles, AE, Hardie, EM, Wooden, BG, Adin, CA, Stone, EA, Gregory, CR, et al. Clinical, clinicopathologic, radiographic, and ultrasonographic abnormalities in cats with ureteral calculi: 163 cases (1984-2002). J Am Vet Med Assoc. (2005) 226:932–6. doi: 10.2460/javma.2005.226.932
11. Cannon, AB, Westropp, JL, Ruby, AL, and Kass, PH. Evaluation of trends in urolith composition in cats: 5,230 cases (1985–2004). J Am Vet Med Assoc. (2007) 231:570–6. doi: 10.2460/javma.231.4.570
12. Wuillemin, F, Vachon, C, Beauchamp, G, and Dunn, M. Subcutaneous ureteral bypass device placement in 81 cats with benign ureteral obstruction (2013-2018). J Vet Intern Med. (2021) 35:2778–86. doi: 10.1111/jvim.16280
13. Vrijsen, E, Devriendt, N, Mortier, F, Stock, E, Van Goethem, B, and de Rooster, H. Complications and survival after subcutaneous ureteral bypass device placement in 24 cats: a retrospective study (2016–2019). J Feline Med Surg. (2020) 23:759–69. doi: 10.1177/1098612X20975374
14. Kulendra, NJ, Borgeat, K, Syme, H, Dirrig, H, and Halfacree, Z. Survival and complications in cats treated with subcutaneous ureteral bypass. J Small Anim Pract. (2020) 62:4–11. doi: 10.1111/jsap.13226
15. McEntee, EP, Berent, AC, Weisse, C, Le Roux, A, and Lamb, K. Evaluation of preoperative ultrasonographic parameters to predict renal recovery in long-term survivors after treatment of feline ureteral obstructions: 2012–2019. J Feline Med Surg. (2021) 24:328–36. doi: 10.1177/1098612X211023645
16. Han, JH, Song, SH, Lee, JS, Nam, W, Kim, SJ, Park, S, et al. Best ultrasound parameter for prediction of adverse renal function outcome after pyeloplasty. Int J Urol. (2020) 27:775–82. doi: 10.1111/iju.14299
17. Li, X-D, Wu, Y-P, Wei, Y, Chen, S-H, Zheng, Q-S, Cai, H, et al. Predictors of recoverability of renal function after Pyeloplasty in adults with Ureteropelvic junction obstruction. Urol Int. (2018) 100:209–15. doi: 10.1159/000486425
18. Lamb, CR, Cortellini, S, and Halfacree, Z. Ultrasonography in the diagnosis and management of cats with ureteral obstruction. J Feline Med Surg. (2018) 20:15–22. doi: 10.1177/1098612X17694253
19. Clarke, DL. Feline ureteral obstructions part 1: medical management. J Small Anim Pract. (2018) 59:324–33. doi: 10.1111/jsap.12844
20. Fages, J, Dunn, M, Specchi, S, and Pey, P. Ultrasound evaluation of the renal pelvis in cats with ureteral obstruction treated with a subcutaneous ureteral bypass: a retrospective study of 27 cases (2010-2015). J Feline Med Surg. (2018) 20:875–83. doi: 10.1177/1098612X17732900
21. Wormser, C, Reetz, JA, Drobatz, KJ, and Aronson, LR. Diagnostic utility of ultrasonography for detection of the cause and location of ureteral obstruction in cats: 71 cases (2010–2016). J Am Vet Med Assoc. (2019) 254:710–5. doi: 10.2460/javma.254.6.710
22. Bua, A-S, Dunn, ME, and Pey, P. Respective associations between ureteral obstruction and renomegaly, urine specific gravity, and serum creatinine concentration in cats: 29 cases (2006-2013). J Am Vet Med Assoc. (2015) 247:518–24. doi: 10.2460/javma.247.5.518
23. Braun, J-P, and Lefebvre, HP. Chapter 16—kidney function and damage In: JJ Kaneko, JW Harvey, and ML Bruss, editors. Clinical biochemistry of domestic animals. Sixth ed. San Diego: Academic Press (2008). 485–528.
24. Bartges, J, Polzin, D, and Segev, G. Diseases of the ureter In: Diseases of the ureter in nephrology and urology of small animals. Ames, Iowa, USA: John Wiley & Sons (2011). 583–90.
25. Cost, GA, Merguerian, PA, Cheerasarn, SP, and Shortliffe, LM. Sonographic renal parenchymal and pelvicaliceal areas: new quantitative parameters for renal sonographic followup. J Urology. (1996) 156:725–9. doi: 10.1016/S0022-5347(01)65798-7
26. Rodriguez, L, Lock, J, Kennedy, W, and Shortlife, L. Evaluation of sonographic renal parenchymal area in the management of hydronephrosis. J Urology. (2001) 165:548–51. doi: 10.1097/00005392-200102000-00066
27. Fischer, K, Li, C, Wang, H, Song, Y, Furth, S, and Tasian, GE. Renal parenchymal area growth curves for children 0 to 10 months old. J Urology. (2016) 195:1203–8. doi: 10.1016/j.juro.2015.08.097
28. Debruyn, K, Haers, H, Combes, A, Paepe, D, Peremans, K, Vanderperren, K, et al. Ultrasonography of the feline kidney: technique, anatomy and changes associated with disease. J Feline Med Surg. (2012) 14:794–803. doi: 10.1177/1098612X12464461
29. Pollard, R, and Philips, K. Diagnostic imaging of the urinary tract In: BSAVA manual of canine and feline nephrology and urology. Gloucester: British Small Animal Veterinary Association (2017)
30. Ferreira, A, Marwood, R, Batchelor, D, Maddox, T, and Mortier, JR. Prevalence and clinical significance of the medullary rim sign identified on ultrasound of feline kidneys. Vet Rec. (2020) 186:533–3. doi: 10.1136/vr.105619
31. Lamb, C, Dirrig, H, and Cortellini, S. Comparison of ultrasonographic findings in cats with and without azotaemia. J Feline Med Surg. (2018) 20:948–54. doi: 10.1177/1098612X17736657
32. Cordella, A, Pey, P, Dondi, F, Dunn, M, Caramazza, C, Cipone, M, et al. The ultrasonographic medullary “rim sign” versus medullary “band sign” in cats and their association with renal disease. Vet Int Med. (2020) 34:1932–9. doi: 10.1111/jvim.15878
33. IRIS Kidney—Guidelines—IRIS staging of CKD. Available at: http://www.iris-kidney.com/guidelines/staging.html (Accessed December 19, 2024)
34. Nahm, FS. Receiver operating characteristic curve: overview and practical use for clinicians. Korean J Anesthesiol. (2022) 75:25–36. doi: 10.4097/kja.21209
35. McGee, S. Simplifying likelihood ratios. J Gen Intern Med. (2002) 17:647–50. doi: 10.1046/j.1525-1497.2002.10750.x
36. Yan, G, Chen, K, Wang, H, Ma, T, and Chen, K. Relationship between ultrasonographically determined renal dimensions and international renal interest society stages in cats with chronic kidney disease. Vet Int Med. (2020) 34:1464–75. doi: 10.1111/jvim.15814
37. Wong, IY-Z, Copp, HL, Clark, CJ, Wu, H-Y, and Shortliffe, LD. Quantitative ultrasound renal parenchymal area correlates with renal volume and identifies reflux nephropathy. J Urol. (2009) 182:1683–7. doi: 10.1016/j.juro.2009.03.075
38. Rickard, M, Lorenzo, AJ, and Braga, LH. Renal parenchyma to Hydronephrosis area ratio (PHAR) as a predictor of future surgical intervention for infants with high-grade prenatal Hydronephrosis. Urology. (2017) 101:85–9. doi: 10.1016/j.urology.2016.09.029
39. Odeh, R, Noone, D, Bowlin, PR, Braga, LHP, and Lorenzo, AJ. Predicting risk of chronic kidney disease in infants and young children at diagnosis of posterior urethral valves: initial ultrasound kidney characteristics and validation of parenchymal area as forecasters of renal reserve. J Urol. (2016) 196:862–8. doi: 10.1016/j.juro.2016.03.137
Keywords: sub, ureterolithiasis, ureteral calculi, kidney, ureter
Citation: Pulido Vega D, Ficheroulle J, Manassero M, Mortier J and Maurey C (2025) Association of preoperative ultrasonographic parameters of the contralateral kidney with long-term serum creatinine in cats treated for unilateral ureteral obstruction. Front. Vet. Sci. 12:1518713. doi: 10.3389/fvets.2025.1518713
Edited by:
Hussein M. El-Husseiny, Tokyo University of Agriculture and Technology, JapanReviewed by:
Howard Dobson, Invicro, United StatesAdeline Decambron, Hopia Veterinary Clinic, France
Copyright © 2025 Pulido Vega, Ficheroulle, Manassero, Mortier and Maurey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego Pulido Vega, ZGllZ28ucHVsaWRvLXZlZ2FAdmV0LWFsZm9ydC5mcg==