
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Vet. Sci., 26 June 2024
Sec. Veterinary Emergency and Critical Care Medicine
Volume 11 - 2024 | https://doi.org/10.3389/fvets.2024.1376004
 Pierre-André Vidal1,2*
Pierre-André Vidal1,2* Søren R. Boysen3
Søren R. Boysen3 Julie Fordellone1
Julie Fordellone1 Alexandra Nectoux1,2Bernard Allaouchiche2,4
Alexandra Nectoux1,2Bernard Allaouchiche2,4 Céline Pouzot-Nevoret1,2
Céline Pouzot-Nevoret1,2Introduction: Motor vehicular trauma, bite wounds, high-rise syndrome, and trauma of unknown origin are common reasons cats present to the emergency service. In small animals, thoracic injuries are often associated with trauma. The objective of this retrospective study was to evaluate limits of agreement (LOA) between thoracic point-of-care ultrasound (thoracic POCUS) and thoracic radiography (TXR), and to correlate thoracic POCUS findings to animal trauma triage (ATT) scores and subscores in a population of cats suffering from recent trauma.
Methods: Cats that had thoracic POCUS and TXR performed within 24 h of admission for suspected/witnessed trauma were retrospectively included. Thoracic POCUS and TXR findings were assessed as “positive” or “negative” based on the presence or absence of injuries. Cats positive on thoracic POCUS and TXR were assigned 1 to 5 tentative diagnoses: pulmonary contusions/hemorrhage, pneumothorax, pleural effusion, pericardial effusion, and diaphragmatic hernia. When available ATT scores were calculated. To express LOA between the two imaging modalities a kappa coefficient and 95% CI were calculated. Interpretation of kappa was based on Cohen values.
Results: One hundred and eleven cats were included. 83/111 (74.4%) cats were assessed as positive based on thoracic POCUS and/or TXR. Pulmonary contusion was the most frequent diagnosis. The LOA between thoracic POCUS and TXR were moderate for all combined injuries, moderate for pulmonary contusions/hemorrhage, pneumothorax, diaphragmatic hernia, and fair for pleural effusion. Cats with positive thoracic POCUS had significantly higher median ATT scores and respiratory subscores compared to negative thoracic POCUS cats.
Discussion: The frequency of detecting intrathoracic lesions in cats was similar between thoracic POCUS and TXR with fair to moderate LOA, suggesting thoracic POCUS is useful in cats suffering from trauma. Thoracic POCUS may be more beneficial in cats with higher ATT scores, particularly the respiratory score.
Trauma is a common cause of mortality in cats that often results from motor vehicular trauma, bite wounds, high-rise syndrome, and unknown causes (1–3). In small animals, thoracic trauma is present in 39–60% of trauma cases (3, 4), with pneumothorax, lung contusions, pleural effusion, diaphragmatic hernia, and/or rib fractures being the most common thoracic injuries reported (1, 3–7). These lesions are not always evident on physical examination alone, stressing the importance of additional diagnostic modalities, particularly thoracic imaging (3).
Computed tomography (CT) is considered the reference standard to assess intrathoracic injury. However it often requires sedation or anesthesia, transport of the patient, may be cost prohibitive for owners and involves risk of patient and staff exposure to ionizing radiation (8). For these reasons, radiography is arguably the most widely used imaging modality to assess patients for thoracic injury in veterinary medicine, but has similar limitations to CT. Most recently, point-of-care ultrasound (POCUS) has gained acceptance in small animal medicine as it is relatively inexpensive, minimally invasive, radiation sparing, and can be performed patient-side with minimal stress, which is particularly important for low stress handling in cats. Point-of-care ultrasound is widely used and well described in human and canine trauma patients. Moreover, in human medicine, thoracic POCUS is more sensitive than TXR for the detection of many trauma related thoracic injuries, including lung contusions, pneumothorax, rib fractures and pleural effusion (9–12).
Four studies in small animals have compared POCUS to TXR, CT, and/or thoracocentesis for detection of trauma induced thoracic injuries. These studies found thoracic POCUS had good limits of agreement (LOA) for pulmonary contusions, slight to moderate LOA for pneumothorax and fair to moderate LOA for pleural effusion when compared to other diagnostic modalities (13–15). Unfortunately, although cats were sometimes enrolled with dogs, the combined number of cats included in any of these studies was small (n = 9) (5, 13–15).
In humans the likelihood of detecting thoracic injury correlates to the injury severity score. Several injury severity scores have been developed in small animals. In cats, the Animal Trauma Triage (ATT) score is probably the most widely applied and studied (2, 16–19). Several studies have shown a correlation between the ATT score and mortality in both dogs and cats (2, 16, 18–25). More recently, the American College of Veterinary Emergency and Critical Care Veterinary Committee on Trauma has also validated the use of the ATT score in a large population of cats (19). The ATT score is based on the evaluation of six independent equally weighted components: perfusion, cardiac, respiratory, eye/muscle/integument, skeletal, and neurologic, and is scored from 0 to 3 (0 for no or slight injuries and 3 for the most severe injuries) (17). No study has correlated the injury severity of trauma in cats with the likelihood of detecting pathology on thoracic POCUS.
The objectives of this study were to evaluate LOA between thoracic POCUS and TXR in a large population of cats with a recent history of trauma and to correlate thoracic POCUS findings to the ATT score. We hypothesized that the overall LOA between thoracic POCUS and TXR will be good for pulmonary contusions, fair to moderate for pleural effusion, slight to moderate for pneumothorax and moderate for all combined injuries. Furthermore, we hypothesized there will be a significant correlation between thoracic POCUS and the ATT score.
This retrospective clinical study enrolled cats presented to the intensive care unit (ICU) of VetAgro Sup (SIAMU) with suspected or witnessed trauma between February 2014 and April 2021.
A key word search of the electronic medical data base was performed using the terms “polytrauma,” “trauma,” “hit by car,” “fall,” “jump,” “high rise syndrome” and “bite.” Cats were included if thoracic POCUS and TXR were performed within 24 h of admission. Cats were excluded if thoracic POCUS or TXR findings were not recorded, if thoracocentesis was performed between imaging examinations, or if there was a delay of >24 h between imaging modalities.
The ICU admission date, breed, sex, age, weight, cause of trauma, and the approximate time between trauma and admission to the ICU were recorded. Vital signs including heart rate, respiratory rate, pulse quality, capillary refill time, mucous membrane color, respiratory effort and temperature were also recorded when available. When possible, the ATT score and subscores (perfusion, cardiac, respiratory, eye/muscle/integument, skeletal and neurologic) were calculated (16, 17). Finally, thoracocentesis and outcome (survival/dead) were also recorded.
Thoracic POCUS and TXR were categorically classified as positive or negative based on the presence or absence of detectable thoracic injuries. The following criteria, obtained from the medical records, was used to make a sonographic diagnosis of (1) pulmonary contusions: more than 3 B-lines/coalescent B-lines/pulmonary contusions/and or pulmonary hemorrhage, (2) pneumothorax: absence of lung sliding (glide sign) and/or pneumothorax, (3) pleural effusion: presence of anechoic fluid in the pleural space and or pleural effusion, (4) diaphragmatic hernia: presence of abdominal organs within the thoracic cavity and/or diaphragmatic hernia, and (5) pericardial effusion: anechoic fluid in the pericardial space and/or pericardial effusion. Radiology reports, written by board-certified radiologists, were reviewed to determine the final radiographic diagnosis. The diagnosis of several concomitant lesions was possible for both thoracic POCUS and TXR. Thoracic POCUS examinations were performed and interpreted within the ICU by house officers which included small animal rotating interns, emergency and critical care (ECC) interns, ECC residents and ECC specialists. In all cases, thoracic POCUS was performed on admission and TXR was performed after cats were sufficiently stable to allow radiographs to be safely obtained.
The thoracic POCUS exam was based on the 2008 TFAST protocol and included bilateral chest tube sites (CTS), bilateral pericardial site (PCS) and the diaphragmatico-hepatic site, with patients positioned in either lateral or sternal recumbency, or a standing position (26). However, this protocol was adapted by the attending clinician based on clinical patient assessment and the presence of life-threatening injuries which mandated immediate medical intervention. A microconvex ultrasound transducer with a frequency of 5–8 MHz (convexe SonoSite Edge II, Vet, FUJIFILM, Montigny Le Bretonneux, France) was used for all sonographic scans.
To determine the LOA between thoracic POCUS and TXR a Kappa coefficient and 95% CI were calculated using a commercial statistical software program (Graphpad–Dotmatics company). Statistical significance was set at p ≤ 0.05. Interpretation of kappa was based on Cohen values (27): a Kappa value greater than or equal to 0.81 was deemed to have the best agreement, between 0.61 and 0.80 was characterized as substantial agreement, between 0.41 and 0.60 as moderate agreement, between 0.21 and 0.40 as fair agreement, and between 0.00 and 0.20 as slight agreement. A Kappa <0 was characterized as no agreement. Descriptive statistics were calculated for signalment and presentation of variables. Categorical variables were expressed as frequencies or percentages. Quantitative parameters were expressed as mean and standard deviation (SD, normally distributed) or median and range (non-normally distributed). Normality was tested using the Shapiro–Wilk test. A Chi-square or Fisher’s exact test were used to compare categorical data. A Mann Whitney test was used to compare ATT score and thoracic POCUS findings and to compare the survival rate with the ATT score.
One hundred and twenty-two cases were included for review. Of these 122 cases, 11 cats were excluded; 6 because thoracocentesis was performed between thoracic POCUS and TXR, 3 because there was a lack of information in the record regarding thoracic POCUS findings, and 2 because a diagnosis of diaphragmatic hernia was based on TXR obtained by the referring veterinarian. Of the 111 remaining cats, 54 (48.6%) presented after witnessed or suspected motor vehicular trauma, 53 (47.8%) for high rise syndrome and 4 (3.6%) for canine induced bite wounds.
Mean age was 2.8 ± 2.3 years. There were 25 spayed females, 17 sexually intact females, 47 castrated males, and 22 sexually intact males. Represented breeds included domestic short hair (n = 97), four Siamese, three Bengal, two Main Coon, one British, one Chartreux, one Birman, one Norwegian Forest Cat and one Turkish Angora. Ninety-five cats (85.5%) were discharged, 11 cats (10.0%) were euthanized, and 5 cats (4.5%) died during hospitalization.
Thoracic injury was present on thoracic POCUS and/or TXR in 83/111 (74.4%) cats with 56/111 cats (50.4%) having thoracic injury detectable on both thoracic POCUS and TXR. Pulmonary contusions and pneumothorax were the most frequent injuries detected on thoracic POCUS and TXR. In the current study, no cats had pericardial effusion (Table 1).
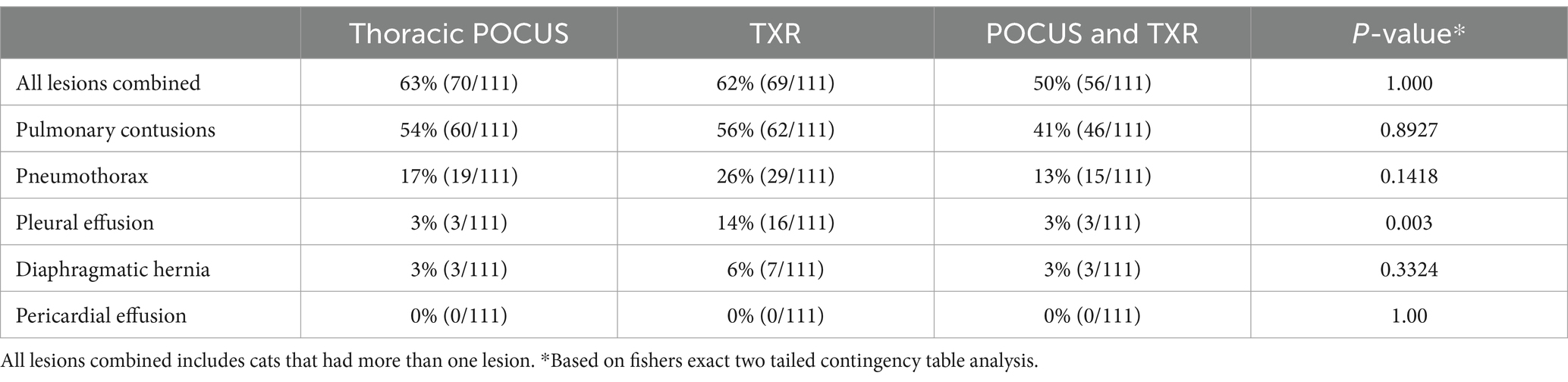
Table 1. Frequency of thoracic lesions found on thoracic point-of-care ultrasound (thoracic POCUS), thoracic radiography (TXR) and simultaneously on both modalities (POCUS and TXR) in a population of 111 cats presented for trauma.
The LOA between thoracic POCUS and TXR for the various thoracic lesions are reported in Table 2, with all agreements ranging from fair to moderate. Cats with and without signs of respiratory distress (n = 40 and 71, respectively) were subanalyzed to compare the overall LOA between POCUS and TXR for all lesions combined (Table 3). Samples size was too small in the subcategorized cats to compare values for individual pathologies.
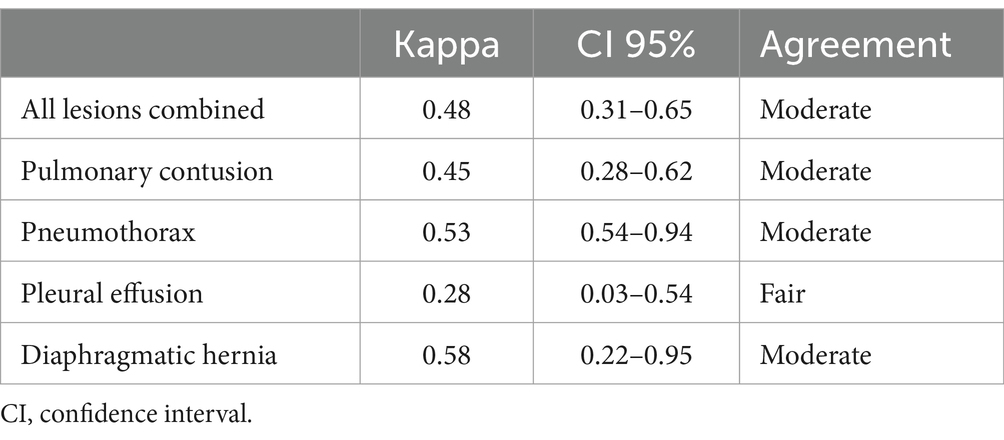
Table 2. Limit of agreement between thoracic point-of-care ultrasound (thoracic POCUS) and thoracic radiography (TXR) in a population of 111 cats presented for trauma.
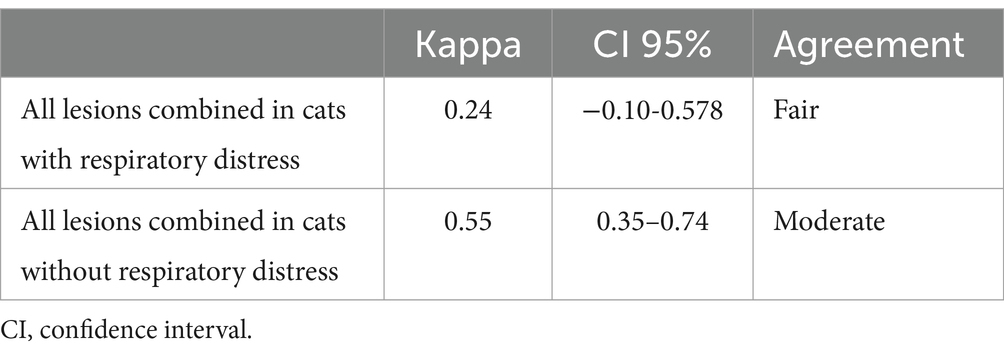
Table 3. Overall limit of agreement between thoracic point-of-care ultrasound (thoracic POCUS) and thoracic radiography (TXR) in a population of 111 cats presented for trauma with and without signs of respiratory distress.
The ATT score was calculated for 106/111 cats with a mean score of 3.66 (SD = 2.47). The ATT score was higher in cats that died (mean of 5.75, SD = 2.79) compared to cats that survived (3.29, SD = 2.22) which was statistically significant (p = 0.0008). There was a statistically significant difference between cats that were positive on thoracic POCUS and cats what were negative on thoracic POCUS (4 versus 3; p = 0.0428). For ATT subscores, only the respiratory subscore was statistically different between cats that were positive versus cats that were negative on thoracic POCUS (1 versus 0; p = 0.0028).
This is the first study to compare thoracic POCUS and TXR in cats presenting for trauma. Results confirm that thoracic POCUS is a valuable diagnostic modality in this study population, identifying injury in 63% of cases. However, the agreement between thoracic POCUS and TXR for all pathologies was only fair to moderate, suggesting the two imaging modalities are complementary in the feline trauma setting. In addition, cats with a positive thoracic POCUS had a significantly higher ATT score, suggesting thoracic POCUS may have greater application in more severely injured patients.
Thoracic injury was present on thoracic POCUS and/or TXR in 74.4% of cats in the current study. This percentage is close to the upper range previously reported in cats (10–90%) (1–3, 5–7, 20, 28, 29). However, due to the retrospective nature of this study and the inclusion/exclusion criteria, not all cases of cats with trauma were included. Therefore, the true frequency of trauma induced thoracic injury is probably lower than reported. Furthermore, the high prevalence of injury reported in the current study is likely due to the large number of cases that presented for high rise syndrome, which is reported to have the highest prevalence of thoracic injury among canine and feline trauma patients (up to 90%) (28). Similar to a prior feline study, pulmonary contusion and pneumothorax were the most frequent lesions identified (29). Given the high occurrence of thoracic injury reported in cats following trauma, thoracic evaluation with imaging should be standard of care, particularly given that cats with thoracic injury do not always show overt clinical signs of respiratory distress (3).
In the current study, pulmonary contusions had moderate LOA between thoracic POCUS and TXR, which is in line with what has been reported in human and canine trauma studies. Numerous human studies demonstrate a high sensitivity and specificity for thoracic POCUS to detect trauma related pulmonary contusions compared to TXR (11, 30). A canine study by Armenise et al. described similar results, demonstrating a more extensive thoracic POCUS protocol (VetFAST-ABCDE) detected pulmonary contusions in 47% of dogs presenting for trauma, compared to only 20% on TXR (15). Another canine study by Dicker et al. concluded that thoracic POCUS had a higher sensitivity (90.5%) and equal specificity (87.5%) compared to TXR (66.7 and 87.5%, respectively) for the diagnosis of pulmonary contusions when using CT as the reference standard (31) Direct comparison between the current and prior canine studies is difficult as lung ultrasound protocols varied between the TFAST protocol used in the current study and more extensive lung ultrasound protocols used in prior studies. It is possible that a higher percentage of pulmonary contusions would have been detected if a larger lung surface scanning protocol was used, which has been suggested by some authors (32).
The LOA between thoracic POCUS and TXR to detect pneumothorax was moderate in the current population of cats, which is similar to mixed results demonstrated in other small animal studies (13–15, 21, 33, 34). One canine study reported TFAST had a sensitivity of only 20% compared to TXR (21), while a second study showed an overall sensitivity of 78.1% and specificity of 93.4% with 7 false positives and 7 false negatives when compared to TXR (14). Comparing a mixed population of cats and dogs to CT in trauma patients, TFAST was shown to have a negative correlation with CT for the diagnosis of pneumothorax (13). A second mixed study population using the Vet BLUE protocol compared to CT in dogs and cats presenting to the emergency service showed that Vet BLUE was only 33% accurate for the diagnosis of pneumothorax (33). Finally, a canine study evaluating a horizontal sliding lung ultrasound protocol using thoracocentesis as the reference standard demonstrated that pleural and lung ultrasound has a higher sensitivity than TXR for detection of pneumothorax (15). There are several factors that likely explain these mixed results. The most widely used sonographic criterion to diagnose pneumothorax in both human and veterinary medicine is the absence of lung sliding. Although not clinically studied in small animals, other sonographic criteria have been described in both human and veterinary medicine to increase the likelihood of correctly ruling in (see-shore sign on M-mode, visualization of lung point, abnormal curtain sign) or ruling out the diagnosis (detection of B-lines, visualization of the lung pulse) (34–36). Because the current study only assessed lung sliding it may have underdiagnosed the presence of pneumothorax. Thoracic POCUS windows assessed may also have contributed to these results. The chest tube site was the most common site assessed for the presence or absence of pneumothorax in the current study, while larger lung surface areas were assessed in other studies (15, 33, 36). Moreover, the position of chest tube site can vary from operator to operator and the most gravity independent site for air to accumulate will vary depending on if the patient is in sternal or lateral recumbency (35). Although patient position was not specifically recorded in the current study, it is possible that assessing the more caudo-dorsal sites when cats were in a sternal or standing position, the widest point of the chest when cats were in a lateral position, and incorporating the curtain sign, may have increased the LOA between imaging modalities (34–36).
The sonographic detection of pleural effusion in the current study was low (3%) and had fair LOA with TXR, which is similar to what has been reported in other small animal studies following trauma (13, 15, 33). A trauma study in cats and dogs identified pleural effusion in 38% of cases using CT, and reported that TFAST had fair to moderate correlation to CT for detection of pleural effusion, depending on the operator performing the sonographic examination (13). Another study comparing TXR and CT in 59 dogs presenting with blunt motor vehicular trauma identified pleural effusion in 12% of cases using CT, compared to only 5% on TXR (37). Finally, a canine study identified pleural effusion in 6% of trauma patients using TFAST (14). The variation in detection of pleural effusion in small animals is likely a result of the imaging modality used, making it difficult to know the true prevalence of pleural effusion and therefore the sensitivity and specificity of thoracic POCUS to identify pleural effusion in cats. Indeed, based on a canine cadaver study and a small case study in dogs, Boysen et al. suggest that probe orientation and location, as well as patient position play an important role in pleural fluid detection. They suggest orientating the probe parallel to the ribs and scanning multiple sites along the ventral sternal border with the patient in a sternal or standing position, or scanning the widest gravity dependent site with the patient in lateral position, may increase the sensitivity and specificity of detecting pleural effusion (36–38). Due to the retrospective nature of the study, the exact probe orientation and location on the thoracic wall cannot be determined and small quantities of fluid may have been missed.
Diaphragmatic hernia is another traumatic injury well described in the veterinary literature (14, 15, 20, 28, 29, 39). Our study showed a moderate LOA between thoracic POCUS and TXR for diaphragmatic hernia, which has not previously been described in cats. However, these results should be interpreted with caution due to the low number of cases with diaphragmatic hernia. In the study by Armenise et al., thoracic POCUS was able to detect one case of diaphragmatic hernia which was not detected on TXR (15). Another study that compared the use of ultrasound with clinical signs of dyspnea and muffled heart sounds on auscultation to diagnose diaphragmatic rupture in dogs and cats compared to radiographs, surgery, or necropsy found the accuracy of ultrasonography was 93%. However, this study was conducted by imaging specialists in a controlled setting, and not by less experienced operators in the emergency setting, as was the situation in the current study (40).
Our study showed that cats with positive thoracic POCUS have significantly higher ATT scores, particularly the respiratory subscore. This is not surprising as the assessment of the respiratory subscore depends on clinical signs, which will be affected by intra-thoracic lesions. This clinical application of POCUS has also been highlighted in the McMurray et al. study in non-trauma patients, showing that the more unstable the patient is, the greater is the probability of finding POCUS lesions (41). Another study that enrolled 50 dogs suffering trauma demonstrated no significant association between ATT score and TFAST. However, only a small proportion of the population showed lesions on TFAST (21). When analyzing cats with and without respiratory distress the LOA between thoracic POCUS and TXR was higher in cats without respiratory distress which is likely explained by the higher number of true negative cases in this subgroup. Although POCUS is generally considered better at ruling in findings, many of the cats presenting without respiratory distress were likely true negative cases, which would tend to increase the LOA for negative findings in both thoracic POCUS and TXR (e.g., POCUS cannot miss lesions if there are no lesions to miss). By contrast, most cases with respiratory distress had pathology detected on thoracic POCUS and/or TXR, resulting in a very small number of cases without detectable pathology, increasing the likelihood that thoracic POCUS and/or TXR will miss some of these lesions. Larger studies using CT as the reference standard are required to corroborate this hypothesis.
This study has several limitations, mainly due to its retrospective nature. The interpretation of recorded data within the medical record required some subjective assessment to draw conclusions. Several operators performed thoracic POCUS with different levels of training and it is possible that lesions may have been missed by less experienced operators. The thoracic POCUS protocol used was initially based on the 2008 Lisciandro TFAST study, but was adapted by the clinician based on the clinical assessment of the patient, and likely evolved over the study duration as newer thoracic POCUS research findings in small animals became available. Although it is not possible to determine due to the retrospective nature, more recent cases enrolled in the study may have included more extensive thoracic POCUS protocols and therefore influenced findings. Another limitation is that the exact time between each imaging modality was not always possible to determine. Although both thoracic POCUS and TXR were performed within 24 h of admission, in some instances, lesions may have progressed, improved or resolved between imaging modalities, depending on the nature of the condition and time between diagnostics (42). Moreover, the results of TXR and thoracic POCUS have never been compared to the reference standard CT. As a result, some lesions may have been misclassified or misdiagnosed, making it impossible to know the true sensitivity, specificity, and accuracy of either modality. Finally, although the LOA between the two modalities was higher in cats without respiratory distress compared to cats with respiratory distress, LOA was not possible to calculate for individual pathologies due to the small sample size. This may have overestimated the LOA for the subcategories of cats with and without respiratory distress, as any finding was considered positive on thoracic POCUS and TXR, and individual discrepancies were not considered for the LOA calculation (e.g., thoracic POCUS may have identified only contusions in one cat and TXR identified pleural effusion in the same cat, but both would be considered positive).
Due to the retrospective nature of the study, it was not possible to determine if radiologists were blinded to the results of thoracic POCUS. It was also not possible to compare the localization of lesions between thoracic POCUS and TXR as the exact site of injury was not recorded during thoracic POCUS examination. Another limitation is that some cats were removed from the study if thoracocentesis was required following thoracic POCUS, and prior to TXR. This may have introduced a bias and decreased the coefficient of agreement for some injuries (e.g., pneumothorax). Finally, the ATT score was calculated retrospectively based on availability of information in the medical record, without specifically including the time the data was collected within a 24-h window. Therefore, these scores may have been different if they had been calculated at the time of admission.
Thoracic POCUS is a complementary and useful diagnostic imaging modality that can be used to detect trauma induced thoracic injury in cats. A higher ATT score, particularly the respiratory subscore, suggests a higher probability to identifying thoracic lesions, and particular attention should be paid to these cats when it comes to thoracic POCUS. Further prospective studies using CT as the reference standard and comparing different thoracic POCUS protocol is recommended.
This retrospective study was presented in part as oral abstract at the 2022 EVECC Congress in Ghent.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval is not required for studies involving animals in accordance with the local legislation and institutional requirements because only medical records were reviewed retrospectively. Written informed consent was not obtained from the owners for the participation of their animals in this study because ethical review and approval were not required because only medical records were reviewed retrospectively.
P-AV: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation. SB: Writing – review & editing, Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation. JF: Writing – original draft, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation. AN: Writing – review & editing, Conceptualization, Investigation, Methodology, Supervision, Validation. BA: Writing – review & editing, Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft. CP-N: Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
LOA, Level of agreement; TPOCUS, Thoracic point-of-care ultrasound; TXR, Thoracic radiographs; ATT, Animal trauma triage; CT, Computed tomography; ICU, Intensive care unit; ECC, Emergency and critical care.
1. Hernon, T, Gurney, M, and Gibson, S. A retrospective study of feline trauma patients admitted to a referral centre: retrospective study of feline trauma patients. J Small Anim Pract. (2018) 59:243–7. doi: 10.1111/jsap.12815
2. Lee, JA, Huang, C, and Hall, KE. Epidemiology of severe trauma in cats: an ACVECC VetCOT registry study. J Vet Emerg Crit Care. (2022) 32:705–13. doi: 10.1111/vec.13229
3. Zulauf, D, Kaser-Hotz, B, Hässig, M, Voss, K, and Montavon, PM. Radiographic examination and outcome in consecutive feline trauma patients. Vet Comp Orthop Traumatol. (2008) 21:36–40. doi: 10.3415/VCOT-07-01-0012
4. Sigrist, NE, Doherr, MG, and Spreng, DE. Clinical findings and diagnostic value of post-traumatic thoracic radiographs in dogs and cats with blunt trauma. J Vet Emerg Crit Care. (2004) 14:259–68. doi: 10.1111/j.1476-4431.2004.04024.x
5. Sepuya, RG, Dozeman, ET, Prittie, JE, Fischetti, AJ, and Weltman, JG. Comparing diagnostic findings and cost of whole body computed tomography to traditional diagnostic imaging in polytrauma patients. J Vet Emergen Crit Care. (2022) 32:334–40. doi: 10.1111/vec.13189
6. Conroy, M, O’Neill, D, Boag, A, Church, D, and Brodbelt, D. Epidemiology of road traffic accidents in cats attending emergency-care practices in the UK: RTA in cats attending emergency practice in the UK. J Small Anim Pract. (2019) 60:146–52. doi: 10.1111/jsap.12941
7. Gregory, CW, Davros, AM, Cockrell, DM, and Hall, KE. Evaluation of outcome associated with feline trauma: a veterinary committee on trauma registry study. J Vet Emergen Crit Care. (2023) 33:201–7. doi: 10.1111/vec.13277
8. Kaur, J, Bhoil, R, Kumar, R, Attri, PK, and Thakur, R. Diagnosis of traumatic pneumothorax: a comparison between lung ultrasound and supine chest radiographs. Indian J Crit Care Med. (2021) 25:176–80. doi: 10.5005/jp-journals-10071-23729
9. Battle, C, Hayward, S, Eggert, S, and Evans, PA. Comparison of the use of lung ultrasound and chest radiography in the diagnosis of rib fractures: a systematic review. Emerg Med J. (2019) 36:185–90. doi: 10.1136/emermed-2017-207416
10. Hyacinthe, AC, Broux, C, Francony, G, Genty, C, Bouzat, P, Jacquot, C, et al. Diagnostic accuracy of ultrasonography in the acute assessment of common thoracic lesions after trauma. Chest. (2012) 141:1177–83. doi: 10.1378/chest.11-0208
11. Vafaei, A, Hatamabadi, HR, Heidary, K, Alimohammadi, H, and Tarbiyat, M. Diagnostic accuracy of ultrasonography and radiography in initial evaluation of chest trauma patients. Emerg. (2016) 4:29–33. doi: 10.22037/emergency.v4i1.9251
12. Rainer, TH, Griffith, JF, Lam, E, Lam, PKW, and Metreweli, C. Comparison of thoracic ultrasound, clinical acumen, and radiography in patients with minor chest injury. J Trauma. (2004) 56:1211–3. doi: 10.1097/01.ta.0000075800.65485.48
13. Walters, AM, O’Brien, MA, Selmic, LE, Hartman, S, McMichael, M, and O’Brien, RT. Evaluation of the agreement between focused assessment with sonography for trauma (AFAST/TFAST) and computed tomography in dogs and cats with recent trauma. J Vet Emergen Crit Care. (2018) 28:429–35. doi: 10.1111/vec.12732
14. Lisciandro, GR, Lagutchik, MS, Mann, KA, Voges, AK, Fosgate, GT, Tiller, EG, et al. Evaluation of a thoracic focused assessment with sonography for trauma (TFAST) protocol to detect pneumothorax and concurrent thoracic injury in 145 traumatized dogs. J Vet Emergen Crit Care. (2008) 18:258–69. doi: 10.1111/j.1476-4431.2008.00312.x
15. Armenise, A, Boysen, RS, Rudloff, E, Neri, L, Spattini, G, and Storti, E. Veterinary-focused assessment with sonography for trauma-airway, breathing, circulation, disability and exposure: a prospective observational study in 64 canine trauma patients. J Small Anim Pract. (2019) 60:173–82. doi: 10.1111/jsap.12968
16. Ash, K, Hayes, GM, Goggs, R, and Sumner, JP. Performance evaluation and validation of the animal trauma triage score and modified Glasgow coma scale with suggested category adjustment in dogs: a VetCOT registry study: external validation of ATT score and mGCS. J Vet Emergen Crit Care. (2018) 28:192–200. doi: 10.1111/vec.12717
17. Rockar, RA, Drobatz, KS, and Shofer, FS. Development of a scoring system for the veterinary trauma patient. J Vet Emergen Crit Care. (1994) 4:77–83. doi: 10.1111/j.1476-4431.1994.tb00118.x
18. Hall, KE, Boller, M, Hoffberg, J, McMichael, M, Raffe, MR, Sharp, CR, et al. ACVECC-veterinary committee on trauma registry report 2013-2017: VetCOT trauma registry 2013-2017. J Vet Emergen Crit Care. (2018) 28:497–502. doi: 10.1111/vec.12766
19. Lapsley, J, Hayes, GM, and Sumner, JP. Performance evaluation and validation of the animal trauma triage score and modified Glasgow coma scale in injured cats: a veterinary committee on trauma registry study. J Vet Emergen Crit Care. (2019) 29:478–83. doi: 10.1111/vec.12885
20. Lux, CN, Culp, WTN, Mellema, MS, Rosselli, DD, Schmiedt, CW, Singh, A, et al. Factors associated with survival to hospital discharge for cats treated surgically for thoracic trauma. J Am Vet Med Assoc. (2018) 253:598–605. doi: 10.2460/javma.253.5.598
21. Parlak, K, Zamirbekova, N, Uzunlu, EO, Akyol, ET, and Yavru, N. Comparison of the focused assessment with sonography for trauma protocol and animal trauma triage scoring system in traumatized dogs. Kafkas Univ Vet Fak Derg. (2021) 27:439–44. doi: 10.9775/kvfd.2021.25457
22. Gottlieb, DL, Prittie, J, Buriko, Y, and Lamb, KE. Evaluation of acute traumatic coagulopathy in dogs and cats following blunt force trauma: acute traumatic coagulopathy in dogs and cats. J Vet Emergen Crit Care. (2017) 27:35–43. doi: 10.1111/vec.12525
23. Klainbart, S, Shipov, A, Madhala, O, Oron, LD, Weingram, T, Segev, G, et al. Dog bite wounds in cats: a retrospective study of 72 cases. J Feline Med Surg. (2022) 24:107–15. doi: 10.1177/1098612X211010735
24. Lyons, BM, Ateca, LB, and Otto, CM. Clinicopathologic abnormalities associated with increased animal triage trauma score in cats with bite wound injuries: 43 cases (1998–2009). J Vet Emergen Crit Care. (2019) 29:296–300. doi: 10.1111/vec.12831
25. Tinsley, AT, Oyama, MA, and Reineke, EL. Animal trauma triage score, modified Glasgow coma scale, age, and weight were associated with outcome in feline bite wounds (1,065 cases): a VetCOT registry study. J Am Vet Med Assoc. (2023) 261:1–887. doi: 10.2460/javma.22.11.0531
26. Lisciandro, GR . Abdominal and thoracic focused assessment with sonography for trauma, triage, and monitoring in small animals: AFAST and TFAST in small animals. J Vet Emergen Crit Care. (2011) 21:104–22. doi: 10.1111/j.1476-4431.2011.00626.x
27. Cohen, J . A coefficient of agreement for nominal scales. Educ Psychol Meas. (1960) 20:37–46. doi: 10.1177/001316446002000104
28. Lefman, S, and Prittie, JE. High-rise syndrome in cats and dogs. J Vet Emergen Crit Care. (2022) 32:571–81. doi: 10.1111/vec.13206
29. Dicker, SA . Lung ultrasound for pulmonary contusions. Vet Clin North Am Small Anim Pract. (2021) 51:1141–51. doi: 10.1016/j.cvsm.2021.07.001
30. Lewis, BT, Herr, KD, Hamlin, SA, Henry, T, Little, BP, Naeger, DM, et al. Imaging manifestations of chest trauma. Radiographics. (2021) 41:1321–34. doi: 10.1148/rg.2021210042
31. Dicker, SA, Lisciandro, GR, Newell, SM, and Johnson, JA. Diagnosis of pulmonary contusions with point-of-care lung ultrasonography and thoracic radiography compared to thoracic computed tomography in dogs with motor vehicle trauma: 29 cases (2017-2018). J Vet Emergen Crit Care. (2020) 30:638–46. doi: 10.1111/vec.13021
32. Rigot, M, Boysen, S, Masseau, I, and Letendre, J. Evaluation of B-lines with two point-of-care lung ultrasound protocols in cats with radiographically normal lungs. J Vet Emerg Crit Care. (2022) 34:143–52. doi: 10.1111/vec.13360
33. Cole, L, Pivetta, M, and Humm, K. Diagnostic accuracy of a lung ultrasound protocol (vet BLUE) for detection of pleural fluid, pneumothorax and lung pathology in dogs and cats. J Small Anim Pract. (2021) 62:178–86. doi: 10.1111/jsap.13271
34. Hwang, TS, Yoon, YM, Jung, DI, Yeon, SC, and Lee, HC. Usefulness of transthoracic lung ultrasound for the diagnosis of mild pneumothorax. J Vet Sci. (2018) 19:660–6. doi: 10.4142/jvs.2018.19.5.660
35. Boysen, SR . Lung ultrasonography for pneumothorax in dogs and cats. Vet Clin North Am Small Anim Pract. (2021) 51:1153–67. doi: 10.1016/j.cvsm.2021.07.003
36. Boysen, S, McMurray, J, and Gommeren, K. Abnormal curtain signs identified with a novel lung ultrasound protocol in six dogs with pneumothorax. Front Vet Sci. (2019) 6:291. doi: 10.3389/fvets.2019.00291
37. Dancer, SC, Le Roux, C, Fosgate, GT, and Kirberger, RM. Radiography is less sensitive relative to CT for detecting thoracic radiographic changes in dogs affected by blunt trauma secondary to a motor vehicle accident. Vet Radiol Ultrasound. (2019) 60:648–58. doi: 10.1111/vru.12795
38. Boysen, S, Chalhoub, S, and Romero, A. Abstracts from the veterinary emergency and critical care ultrasound society - veterinary point-of-care ultrasound probe orientation for detection of pleural effusion in dog cadavers by novice sonographers: a pilot study. Ultrasound J. (2020) 12:45. doi: 10.1186/s13089-020-00191-6
39. Schmiedt, CW, Tobias, KM, and Stevenson, MAM. Traumatic diaphragmatic hernia in cats: 34 cases (1991-2001). J Am Vet Med Assoc. (2003) 222:1237–40. doi: 10.2460/javma.2003.222.1237
40. Spattini, G, Rossi, F, Vignoli, M, and Lamb, CR. Use of ultrasound to diagnose diaphragmatic rupture in dogs and cats. Vet Radiol Ultrasound. (2003) 44:226–30. doi: 10.1111/j.1740-8261.2003.tb01276.x
41. McMurray, J, Boysen, S, and Chalhoub, S. Focused assessment with sonography in nontraumatized dogs and cats in the emergency and critical care setting: focused assessment with sonography in nontraumatized dogs and cats. J Vet Emergen Crit Care. (2016) 26:64–73. doi: 10.1111/vec.12376
Keywords: cats, trauma, point-of-care ultrasound, pulmonary contusions, pneumothorax, pleural effusion, lung ultrasound
Citation: Vidal P-A, Boysen SR, Fordellone J, Nectoux A, Allaouchiche B and Pouzot-Nevoret C (2024) Retrospective evaluation of the agreement between thoracic point-of-care ultrasound and thoracic radiographs in cats with recent trauma: 111 cats. Front. Vet. Sci. 11:1376004. doi: 10.3389/fvets.2024.1376004
Edited by:
Alex Lynch, North Carolina State University, United StatesReviewed by:
Sarah Malek, Purdue University, United StatesCopyright © 2024 Vidal, Boysen, Fordellone, Nectoux, Allaouchiche and Pouzot-Nevoret. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pierre-André Vidal, ZHIucGllcnJlYW5kcmV2aWRhbEBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.